Technology Assessment in Kaiser Permanente NAIC Health Innovations (B) WG May 30, 2008 Brent...
36
Technology Assessment in Kaiser Permanente NAIC Health Innovations (B) WG May 30, 2008 Brent Barnhart Senior Counsel Kaiser Permanente
-
Upload
kathlyn-gwen-harrison -
Category
Documents
-
view
215 -
download
2
Transcript of Technology Assessment in Kaiser Permanente NAIC Health Innovations (B) WG May 30, 2008 Brent...

Technology Assessment in Kaiser Permanente
NAIC Health Innovations (B) WGMay 30, 2008
Brent BarnhartSenior Counsel
Kaiser Permanente
2
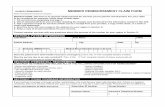
About Kaiser Permanente Nationwide
Nation’s largest nonprofit health plan
Integrated health care delivery system
8.5 million members14,000+ physicians140,000+ employees
8 regions in 9 states and D.C.32 hospitals and med centers430+ medical offices
$37 billion annually
Description:
People:
Facilities:
Revenue:
CO
OR
CA
GA
OH
VAMDDC
HI
WA
3
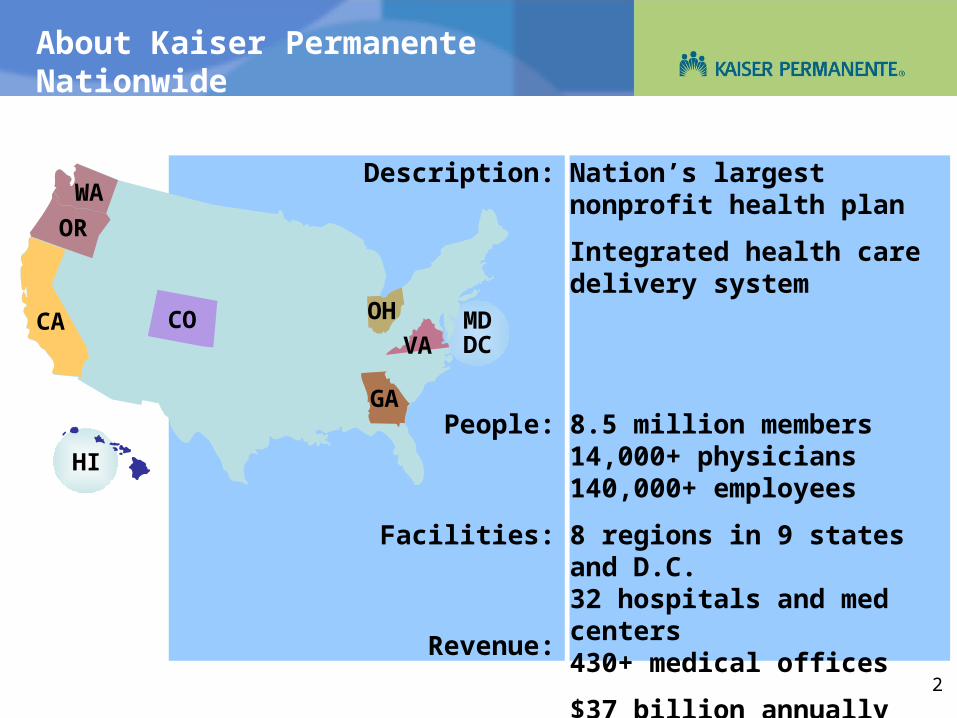
Social Purpose
Quality Driven
Shared Accountability for Program Success
Integration along Multiple Dimensions
Prevention & Care ManagementFocus
A Prepaid Integrated Delivery System With Aligned Incentives
Kaiser Foundation Hospitals
PermanenteMedicalGroup
KaiserFoundationHealth Plan
Health PlanMembers
ThePermanenteFederation

4
New
Medical Technology
Assessment
Drugs Biologics Devices, Equipment and Supplies Medical and Surgical Procedures Support Systems, Organizational and
Managerial Systems including IT
Systematic and comprehensive evaluation of the medical (safety, efficacy, and effectiveness), social, ethical and economic implications of development, diffusion, and use of health technology
Comparative Effectiveness
Entirely new technology New applications of existing technology

5
Comparative Effectiveness
Within Kaiser Permanente, the Interregional New Technologies Committee (INTC) is one of a group of national committees that review new technologies, products and pharmaceuticals:• INTC• National Product Council• Pharmacy and Therapeutics Committee
Kaiser Permanente is also helping to fund a new Institute for Comparative Effectiveness Research (ICER) that will disseminate information to patients, clinicians, and insurers.

6
Interregional New Technologies Committee
Monitors and evaluates new, and new applications of existing, medical and behavioral technologies
Evaluates the medical appropriateness based on demonstrated safety, efficacy and comparative utility
Tracks and analyzes emerging technologies as evidence becomes available.
Compares the new technology to existing alternative technologies
Recommendations, not coverage decisions; never patient-specific
Under The Permanente Federation – the national physician Under The Permanente Federation – the national physician arm of Kaiser Permanentearm of Kaiser Permanente
INTC
7
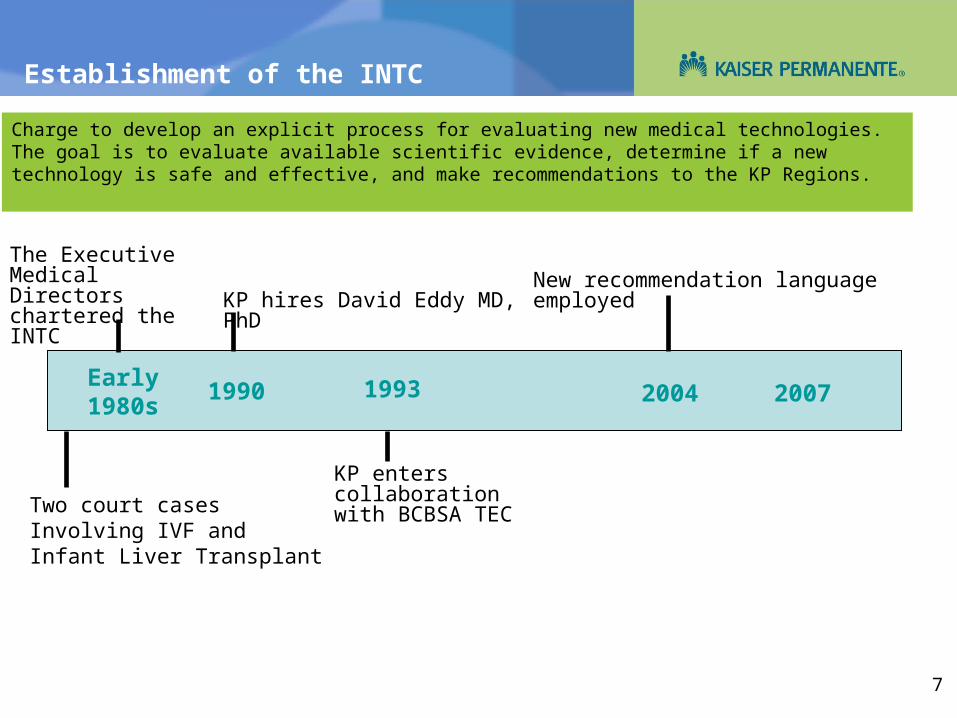
Establishment of the INTC
Early 1980s 2004 2007
The Executive Medical Directors chartered the INTC
Two court cases Involving IVF and Infant Liver Transplant
Charge to develop an explicit process for evaluating new medical technologies. The goal is to evaluate available scientific evidence, determine if a new technology is safe and effective, and make recommendations to the KP Regions.
19931990
KP hires David Eddy MD, PhD
KP enters collaboration with BCBSA TEC
New recommendation language employed

8
18 members, all regions represented Inter-regional Inter-entity 10/18 members are physicians Quarterly meetings with approx. 8 topics each Internal and external evidence reviews PMG experts as clinical guests for select topics PMG expert opinion gathered for all topics
INTC

9
FDA and INTC Scope Compared
Safety
Efficacy • Benefit of using a technology
for a particular health problem in ideal conditions
Substantial equivalence or comparison to placebo
Intermediate, short-term outcomes
Everything in the left column plus
Effectiveness• Benefit of using a
technology for a particular health problem in general or routine conditions
Comparisons to standard of care and experience relevant to members
Long-term health outcomes
Operational impact
FDA’s Scope INTC Scope
9

10
FDA: Medical Devices
Class ILow RiskScalpels, tongue depressors
Class IIModerate RiskAerosol holding chambers, oxygen generators
Class IIIHigh RiskImplantable electric urinary continence devices
General Controls General Controls General Controls
Special Controls Premarket Application (PMA)
General controls sufficient to provide reasonable assurance of safety and efficacy
510(k) process results in determination of whether a device is substantially equivalent (SE) to a predicate device. If not SE, risk determines if process is PMA or 510(k).
PMA approval is based on a determination that there is sufficient valid scientific evidence to reasonably assure that the device is safe and effective for its intended use.
Exempt from 510(k) except…
510(k) required except… PMA required except …
11
By Applying Principles of Evidence-based Medicine
Base clinical and policy decisions on evidence of effectiveness & benefit. David Eddy, MD, PhD
Evidence of benefit Do it
Evidence of no benefit/harm Don’t do it
Insufficient evidence Be conservative
• Use discretion• If it is new, recommend only within well designed trials
Do things that work, don’t do things that don’t, use resources wisely.
Guiding Principles

12
Topic Selection
Needs and ideas from INTC members Feedback on meeting minutes Feedback from regions as they make operational decisions Inquiry line database Internal and external assessment topics New evidence: medical journals and professional meetings FDA approvals, panel meetings, minutes, reviews Member and physician demand Open agenda planning calls including non-KP colleagues
Strict criteria are NOT used to select topics.
Generous input and judgment are used to determine topic priority.

13
2007 INTC Topics
Surgery for morbid obesity CT colonography Wearable cardiodefibrillator vest CAD Mammography Artificial cervical discs Hip resurfacing Remote electronic telemonitoring for CHF Robot-assisted laparoscopic prostatectomy
Topic Selection
14
Preparing a Topic
Determine interest level in new technology Gauge potential operational impact and demand Raise relevant benefit, media, legal and ethical issues Learn how the technology might fit into PMG practice Gather PMG input Determine source of assessment
• Consider internal and external resources, public and private Supplement most current assessment, as needed Select a speaker and prepare a presentation Assist speaker in drafting a recommendation

15
Anatomy of a Technology Assessment
Background Problem Formulation Literature Search Strategy Evidence Summary/Tables Regulatory Information including FDA External assessments, all sectors Conclusion/Rationale Bibliography
Supplemented with PMG expert opinion and professional societies

16
INTC
Sources of Information
Internal Input:Internal Input:
Permanente MedicalGroups
Primarily SCPMGAlso TPMG, TPF
BCBSATECECRI Hayes
Internal Assessments External Assessments
NICE Cochrane
AHRQFDA
CCOHTA
The PermanenteFederation
(TPF)
Inter-entityInterregional
InitiativesRegional Initiatives
EPCs
The INTC manages the national agenda for new medical technology assessment with the input of numerous
collaborators and resources.
Others: AdvisoryBoard, HTC, etc.
Inquiry LineInquiry Line

17
New Technology Inquiry Line
Supports the needs of PMG physicians throughout all KP regions for evidence-based information on new technologies
Volume of Inquiries . . . • Total inquiries (1999-2006) – 4,531• In 2006, the average number inquiries per day was 2.2
In 2006, clients used the inquiry line for . . .• Patient-specific inquiry – 44%• General technology inquiry – 46%

18
INTC Website

19
The BCBSA TEC/KP Collaboration
TEC's collaborative relationship with Kaiser Permanente began in 1993. This relationship has given TEC staff ready access to Kaiser's clinical experts on a wide range of topics. As a result of TEC's collaboration with Kaiser, David M. Eddy, M.D., Ph.D., Senior Advisor for Health Policy and Management, served for over 10 years as TEC's Scientific Advisor, until his retirement from the position in 2004. In addition, one Permanente physician, Jed Weissberg, M.D., is a voting member of TEC's Medical Advisory Panel.
TEC Assessments and other publications are provided to Kaiser Permanente staff as drafts. Dr. Weissberg participates actively in the MAP discussions, sharing clinical opinion from Permanente physicians on the draft TEC products. TEC staff works with Kaiser Permanente's Technology Assessment staff to obtain input on topic selection and to gain access to Permanente's physician experts on a wide range of topics. Permanente clinical expertise may be used to help shape the actual research questions in TEC Assessments. In many cases, these are the same physicians that either chair or sit on committees that are responsible for developing practice guidelines at Kaiser Permanente.

20
More on BCBSA TEC
Founded in 1985 and pioneered the development of scientific criteria for assessing medical technologies through comprehensive reviews of clinical evidence.
TEC provides comprehensive evaluation of the clinical effectiveness and appropriateness of a given medical procedure, device or drug, averaging 20 to 25 assessments a year. TEC serves a wide range of clients in both the private and public sectors, including KP and CMS.
TEC Assessments are scientific opinions, provided solely for informational purposes and should not be construed to suggest that BCBSA, KP or the TEC Program recommends, advocates, requires, encourages, or discourages any particular treatment, procedure, or service; any particular course of treatment, procedure, or service; or the payment or non-payment of the technology or technologies evaluated.
TEC is headed by Executive Director, Naomi Aronson, Ph.D. Its core staff of research scientists consists of experienced physicians and doctorate-level scientists with a history of academic and primary research affiliations.
A Medical Advisory Panel, comprising independent, nationally recognized experts in technology assessment, clinical research and medical specialties, has scientific accountability for all TEC assessments.
BCBSA TEC content is available at: http://www.bcbs.com/betterknowledge/tec/

21
BCBSA TEC Criteria
TEC Assessments routinely use the five TEC criteria to evaluate whether drugs, devices, procedures and biological products improve health outcomes such as length of life, quality of life and functional ability.
1. The technology must have final approval from the appropriate governmental regulatory bodies. 2. The scientific evidence must permit conclusions concerning the effect of the technology on health outcomes. 3. The technology must improve the net health outcome. 4. The technology must be as beneficial as any established alternatives. 5. The improvement must be attainable outside the investigational settings.
22
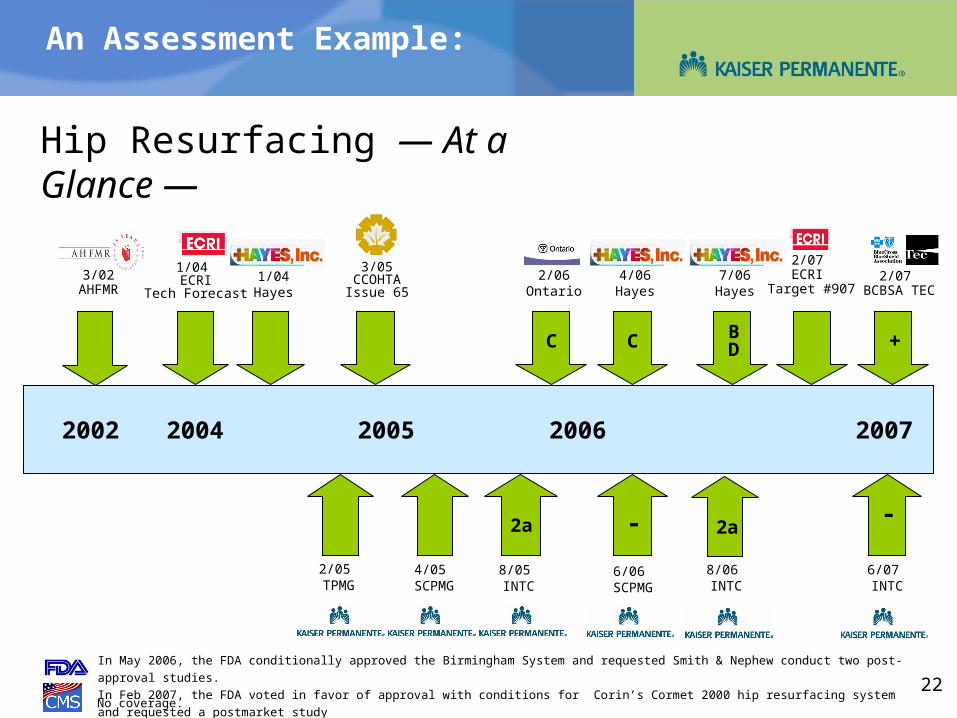
In May 2006, the FDA conditionally approved the Birmingham System and requested Smith & Nephew conduct two post-approval studies.
In Feb 2007, the FDA voted in favor of approval with conditions for Corin’s Cormet 2000 hip resurfacing system and requested a postmarket study
No coverage.
2002
1/04 ECRI
Tech Forecast
2004 2005 2006 2007
8/05 INTC
4/05 SCPMG
3/05 CCOHTAIssue 65
3/02 AHFMR
1/04Hayes
7/06Hayes
2a
8/06 INTC
2a
6/06 SCPMG
2/05 TPMG
2/07 BCBSA TEC
6/07 INTC
- -
4/06Hayes
C BD
2/07 ECRI
Target #9072/06
Ontario
C +
An Assessment Example:
Hip Resurfacing — At a Glance —
23
What the INTC Produces
The INTC Recommendations:1. There is sufficient evidence to determine that the technology is
medically appropriate (or is a medically appropriate treatment/diagnostic option) for select patients.
2. There is insufficient evidence to determine whether the technology is medically appropriate for any patient. OR There is insufficient evidence to determine whether the technology is a medically appropriate treatment/diagnostic option for any patient.
a) no evidenceb) insufficient quantity and/or insufficient qualityc) conflicting or inconsistent
3. There is sufficient evidence to determine that the technology is generally not medically appropriate (or is not a medically appropriate treatment/diagnostic option) for any patients.
What the INTC Does Not Do:Cost-effectiveness studies Operational decisions Clinical practice guidelines Coverage policiesConsultation for individual patient cases
Further describe characteristics of the evidence

24
Current Example: Cervical Arthroplasty
Anterior Cervical Discectomy with Fusion (ACDF)
The goal is to decompress the disc space and stabilize the vertebrae, relieving pressure on the nerve to reduce back, neck and shoulder pain.
Disadvantages: complications associated with grafting loss of cervical mobility growing evidence that fusion may contribute to
adjacent-level degenerative disease
Uses the same anterior surgical approach as cervical fusion Eliminates need for donor bone Aims to maintain motion of cervical vertebrae hoping to reduce
future problems and not hasten DDD in adjacent discs
Cervical Arthroplasty
versus
Implanted Bryan Disc
25
Prestige-ST® by MedtronicOn July 17, 2007, the FDA approved the Prestige-ST® for the treatment in skeletally mature patients for reconstruction of the disc from C3-C7 following single-level discectomy for intractable radiculopathy and or myelopathy. Intractable radiculopathy and or myelopathy should be present with at least one of the following items producing symptomatic nerve root and/or spinal cord compression which is documented by patient history (e.g., pain [neck and/or arm], functional deficit, and/or neurological deficit), and radiographic studies (e.g., CT, MRI, x-rays, etc.): 1) herniated disc, and/or 2) osteophyte formation. The Prestige® is implanted via an open anterior approach.
Cervical Discs and the FDA
The FDA’s Panel recommended Medtronic be barred from claiming preservation of ROM could protect adjacent discs.
The FDA recommended a post-approval study of a min. of 200 pts. with data collection at 5 and 7 years post-op.

26
Bryan by MedtronicOn July 17, 2006, the Orthopaedic and Rehabilitation Devices Panel of the FDA recommended approval of the Bryan Cervical Disc but has not received final marketing approval at this time. The Bryan disc is indicated for use in patients similar to those for whom the Prestige device is indicated.
Cervical Discs and the FDA
27
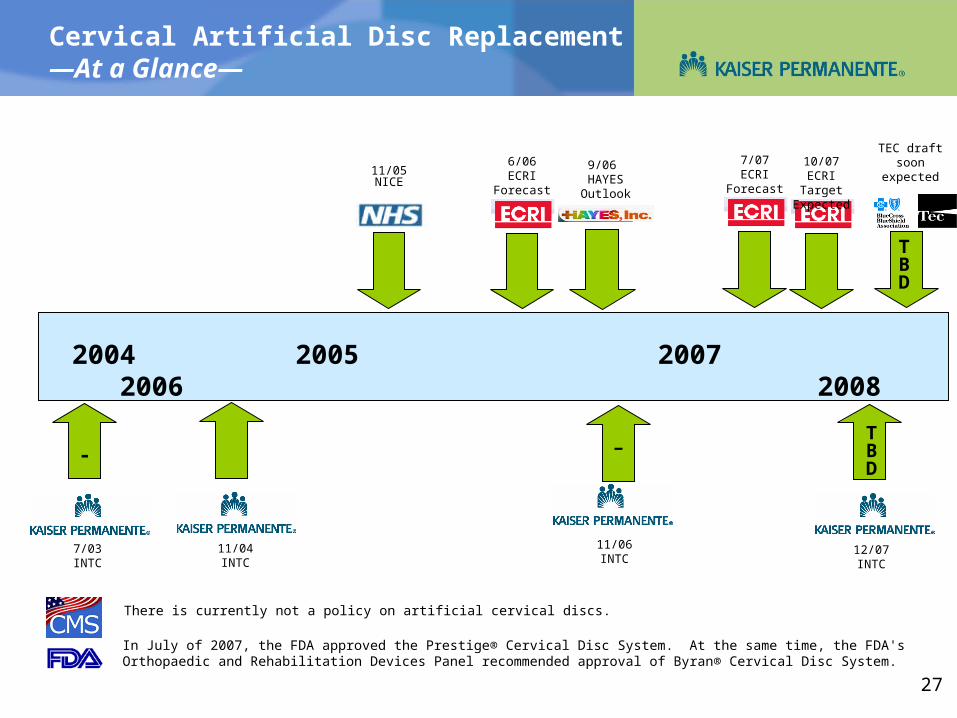
Cervical Artificial Disc Replacement—At a Glance—
2007 2008
11/04 INTC
There is currently not a policy on artificial cervical discs.
7/03INTC
In July of 2007, the FDA approved the Prestige® Cervical Disc System. At the same time, the FDA's Orthopaedic and Rehabilitation Devices Panel recommended approval of Byran® Cervical Disc System.
2004 2005 2006
11/06 INTC
11/05NICE
6/06ECRI
Forecast
9/06 HAYES Outlook
-
7/07ECRI
Forecast
12/07 INTC
TBD
10/07ECRI Target
Expected
TEC draft soon
expected
-
TBD

28
Selective Evidence by Disc Type
Lind (2007), Bryan, n=11, Sears (2007and 2007b), Bryan, n=67Shim (2006), Bryan, n=61
Coric (2006), Bryan, n=33, RCTLafuente (2005), Bryan, n=46, prosp. series
Hacker (2005), Bryan, n=46, RCT
Goffin (2002, 2003), Bryan, n=146, prosp. series
Duggal (2004), Bryan, n=26, prosp. Series
Bertagnoli (2005), ProDisc-C, n=27, prosp. Series
Pimenta (2004), PCM, n=53, prosp. Series
Mummaneni (2007), Prestige, n=541, RCTPorchet (2004), Prestige II, n=55, RCT

29
Coric (2006), Bryan, n=33, RCT
Hacker (2005), Bryan, n=46, RCT
(2005), Bryan, n=550 (not published)
Mummaneni (2007), Prestige, n=541, RCT
Sawin (2005), Prestige ST, n=118, RCT (not publ.)
Porchet (2004), Prestige II, n=55, RCT
Even More Selective: RCTs by Disc Type

30
• 28% of surgeons (20/72) had financial interest in Medtronic and contributed a total of 187 of 541 patients with all centers contributing 1-49 patients each.
• A fixed non-inferiority margin of 10% was agreed upon in advance by Medtronic and the FDA (Hypothesis: The success rate of Prestige is not lower than control by 10%.)
• The interim Bayesian statistical analysis was planned when all patients reach 12-months and 250 pts. reach 24 mos. Primary endpoint is a composite of pain and functional disability, neurological status, adverse events, secondary surgical interventions and a radiographic functional spinal unit (FSU) height determination.
Mummaneni et al - Prestige IDE Trial

31
The Bayesian Interim Analysis
The FDA issued draft guidance on Bayesian statistics in medical device trials in May 2006 http://www.fda.gov/cdrh/osb/guidance/1601.pdf
“Bayesian statistics is a statistical theory and approach to data analysis that provides a coherent method for learning from evidence as it accumulates. Traditional (frequentist) statistical methods formally use prior information only in the design of a clinical trial. … In contrast, the Bayesian approach uses a consistent, mathematically formal method called Bayes’ Theorem for combining prior information with current information on a quantity of interest. …“
“When good prior information on clinical use of a device exists, the Bayesian approach may enable FDA to reach the same decision on a device with a smaller-sized or shorter-duration pivotal trial.”

32
Previous INTC Recommendation (11/06)
There is insufficient evidence to determine whether cervical arthroplasty is a medically appropriate treatment option for single-level cervical degenerative disc disease, including disc herniation and spondylosis.
• The existing evidence is of insufficient quantity and quality. The published evidence literature is limited to 3 small RCTs on two difference devices with less than 50 disc-patients with 24-month follow-up data reported.
KP INTC Discussion 12/07What’s Different Now?
• FDA approval and recommendation for approval • Access to new trial data (published & unpublished) • Additional perspectives on the evidence pending
– Internal, BCBSA TEC, ECRI Target• Evolving PMG opinion and growing consumer interest

33
Thoughts for December Discussion
Studies suggest comparable adverse events, maintenance of ROM, patient satisfaction and decreased pain and disability levels.
Risks appear to be small, although number of patients examined is small Protocols for the controls are not clear and may not represent current
practice. RCTs have not been blinded and are sponsored by device manufacturer Significant variability in success rate by centers and many surgeons and
most authors are financially tied to the manufacturers. In the Prestige IDE trial, only 185 patients had completed outcome
information including FSU. Inclusion of these patients without FSU into the overall success calculations was not consistent with the planned analysis.
In the Prestige IDE trial, 36 patients in the disc group and 48 in the control group declined surgery after randomization suggesting informed consent was not ideal.
In the Prestige IDE trial, the device used is not the device intended for market. Design modifications are being made in anticipation of FDA approval.
There are some reports regarding heterotopic ossification. Marketing to physicians and consumers is increasing along with surgeon
training programs. The INTC’s previous recommendation regarding artificial lumbar discs may
resurface.
34
Cervical Arthroplasty: The Strategy
Early Review Iterative Reviews Stay in touch with PMG practice and consumer interest Monitor ongoing trials and unpublished data Track FDA Advisory Panel meetings Provide Spine Surgeons with evidence
• Assists in early discussion of potential indications• Supports product discussions
– Information regarding FDA recommendations and approvals, products in development, differences in design, tracking of literature and adverse events, etc.
• Informs decision makers regarding potential deployment considerations including surgeon training and volume expectations

35
Cervical Disc Arthroplasty
7/07 9/07 10/07 11/07 12/07
Spine SST
Meeting
INTC
In July of 2007, the FDA approved the Prestige® Cervical Disc System. At the same time, the FDA's Orthopaedic and Rehabilitation Devices Panel recommended approval of Byran® Cervical Disc System.
10/07ECRI Target
Expected
TEC draft soon expected
TBD
TBD
+
Immediately upon FDA approval, Medtronic approaches KP about training

36
What You Need To Make It Work
Evidence-based culture, or the makings of one Supportive medical group leadership Respected source of technology assessments Effective physician/analyst partnerships Resources and process that enable timely and relevant
information and recommendations Courageous physician opinion leaders Realization that this is the grey-zone and uncertainty is the
norm and decisions have to be made Willingness to start somewhere and be persistent