Techniques of Tooth Surface Assessment- Indications for Sealant Placement Margherita Fontana, DDS,...
51
Techniques of Techniques of Tooth Surface Tooth Surface Assessment- Assessment- Indications for Indications for Sealant Placement Sealant Placement Margherita Fontana, DDS, PhD Margherita Fontana, DDS, PhD Domenick Zero, DDS, MS Domenick Zero, DDS, MS Indiana University School of Indiana University School of Dentistry Dentistry Department of Preventive and Department of Preventive and Community Dentistry Community Dentistry Caries? Active? Arrested? How big? To Seal or Not To Seal?
-
Upload
colt-stacy -
Category
Documents
-
view
213 -
download
0
Transcript of Techniques of Tooth Surface Assessment- Indications for Sealant Placement Margherita Fontana, DDS,...

Techniques of Tooth Techniques of Tooth Surface Assessment- Surface Assessment-
Indications for Indications for Sealant PlacementSealant Placement
Margherita Fontana, DDS, PhDMargherita Fontana, DDS, PhDDomenick Zero, DDS, MSDomenick Zero, DDS, MS
Indiana University School of DentistryIndiana University School of DentistryDepartment of Preventive and Community Department of Preventive and Community
DentistryDentistry
Caries?
Active? Arrested?
How big?
To Seal or Not To Seal?

““Prevention works”Prevention works”
Professional dental care Community water fluoridation School-based dental sealant
programs Role of “non-dentists”
– Physicians, NPs, RNs, PAs– Social workers– WIC counselors– HeadStart teachers – and others…

Presentation OutlinePresentation Outline Overview of Caries Detection/Diagnosis
Traditional Caries Detection Methods
Hidden Caries
New Methods of Caries AssessmentVisual
Technology-based
Caries Lesion Activity Status
Diagnostic Thresholds for Placing SealantsSound
Carious
Incipient
Cavitated

What is the accuracy (sensitivity, specificity) of visual or visual-tactile techniques with and without the use of other adjunctive diagnostic techniques, such as radiographs, dyes, and lasers. What degree of accuracy in assessing caries is necessary before sealants can be placed?
How important are missed diagnoses, e.g. “hidden” caries? What do we know about “hidden” caries? What should we do about “hidden caries”?
What visual signs (color, opacity, stain, translucency or other physical characteristics structure) determine dental caries status of the surface and classification into established categories of disease state (sound/caries-free, questionable, enamel caries, and dentin caries)?

•“Improved caries detection and diagnostic methods would help determine the appropriate cutpoint or threshold separating the clinical decisions to do nothing or preventively seal, or to therapeutically seal or surgically treat and restore”
•“Theoretically, laser fluorescence could be useful for determining whether a tooth is sound and does not require intervention, has evidence of a low level of caries ACTIVITY and is appropriate candidate for a sealant application, or has a higher degree of disease severity that requires surgical intervention. Ideally it could subsequently be used to monitor sealant effectiveness…”
(Weintraub, 2001)

“At this time the panel senses a paradigm shift in the management of dental caries toward improved diagnosisdiagnosis of early non-cavitated lesionsearly non-cavitated lesions and treatment for prevention and arrest of such lesions.
NATIONAL INSTITUTES OF HEALTHCONSENSUS DEVELOPMENT CONFERENCE
Diagnosis and Management of Dental Caries Diagnosis and Management of Dental Caries Throughout Life (March 26-28, 2001)Throughout Life (March 26-28, 2001)
http://odp.od.nih.gov/consensus/cons/115/115_statement.htm
Restorations repair the tooth structure, do not stop caries, and have a finite life span. They are themselves susceptible to disease.”

Management of Dental CariesManagement of Dental Caries
Diagnosis
Risk Assessment
Preventive + Non-Surgical Intervention
(Medical Model)
Restorative (Surgical) Intervention
Oral Health Outcome
Assessment
Detection
mfontan
DIagnosis and risk assessment should drive the treatment decisions
mfontan
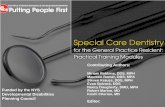
Discussion of cavitated lesions is beyond the scope of this presentation

+ clinically detectable"cavities" limited to enamel
+ clinically detectable enamel lesions with “intact” surfaces
+ lesions detectable only with traditionaldiagnostic aids
+ sub-clinical initial lesions in a dynamic state ofprogression/ regression
Mis-labelled"cariesfree" atthe Dthreshold
3
+ clinically detectablelesions in dentine
lesions into pulp
D4
D3 + enamel=
D3
D1
DHSRU/2002
Diagnosticthreshold
determines whatis recorded as“diseased” or
“sound” D3
D2
D1
Nigel Pitts
The “iceberg of dental caries” Diagnostic thresholds
in surveys, research & practice

Progress of Mineral Loss/DetectionProgress of Mineral Loss/Detection
(White Spot)
DiseaseDisease
Treatment?Treatment?DiseaseDisease
TreatmentTreatment
mfontan
White spots can also be in dentin....

White Spot Lesion:
It is a subsurface lesion
External (outer) surface
Internal loss of minerals

To DiagnoseDiagnose implies not only finding a lesion (DetectionDetection), but, most importantly, to decide if it is active, progressing rapidly or active, progressing rapidly or slowly, or already arrestedslowly, or already arrested.. Without this information a logical decision about treatment is impossible (Kidd, 2001)

Visual ExaminationVisual Examination Most widely used method, in dental offices, in clinical
research and in epidemiological studies. Quick, cheap and easy.
Should be performed on a dry, clean toothdry, clean tooth, with good light, with a mirror.
Useful on all surfaces and on all types of caries.
The basis of most other detection, and most often compared to new methods.
Standard on occlusalocclusal, smooth surface and root caries.
Mostly dichotomous decisions: presence or absence.
Usually no quantification of lesions and therefore difficult to monitor lesions.

Wet
Dry

Detection of LesionsDetection of Lesions
Sturdevant’s (1985) textbook in Operative Dentistry: – Defects are best detected when an explorer placed into a pit or fissure provides
tug-back or resistance to removal.
Subject of controversy:– Use of the explorer does not add anything to the detection yield of the
examination.– The use of the explorer may at best be misleading and at worst be potentially
damaging.– Use a BLUNT probe, proper lighting, dry, clean teeth and sharp eyes

Probing with Sharp Explorer…Probing with Sharp Explorer…
Ekstrand et al., 1987
Traditional probing with a sharp explorer has come into question as the ultimate determinant of caries activity. The exclusive use of a “catch” by the sharp explorer to diagnose caries in pit and fissure sites should be discontinued and clinicians are being called upon to use “sharp eyes and a blunt explorer.” Also non-cavitated lesions can become cavitated simply through pressure from the explorer during the typical examination. Thus, penetration by a sharp explorer can actually cause cavitation in areas that are remineralizing or could be remineralized.
Treating caries as an Treating caries as an infectious disease. JADA infectious disease. JADA 125 (June): 2-S to 15-S 125 (June): 2-S to 15-S (1995)(1995)

ValidationValidation methodmethod
Detection methodDetection method CariesCaries
N=50N=50
No CariesNo Caries
N=950N=950
TotalsTotals
N=1000N=1000
Caries PresentCaries Present
TPTP
True PositiveTrue Positive
N=20N=20
FPFP
False Positive-False Positive-OvertreatmentOvertreatment
N=57N=57
N=77N=77
Caries Not presentCaries Not present
FNFN
False Negative-False Negative-UndertreatmentUndertreatment
N=30N=30
TNTN
True NegativeTrue Negative
N=893N=893
N=923N=923
Specificity: Specificity: 94%94%
Sensitivity of Visual ExaminationSensitivity of Visual Examination
Sensitivity: 40%Alwas-Danowska
et al., 2002
Occlusal surfaces:Occlusal surfaces:Typically low sensitivity, ~ 0.30, and high specificity

Appropriate Ways to Use the Appropriate Ways to Use the Explorer for Sealant Placement Explorer for Sealant Placement
• Clean debris from fissures and interproximal spaces• Confirm and assess cavitations (breaks in the
continuity of the surface)• Feel the texture (roughness) of non-cavitated
lesions, if they extend well beyond the opening of the fissure (if the program desires to consider surface activity in their risk decision making process)
• Once sealed, help assess the quality and integrity of the sealant.

Core ICDAS Criteria ••For use on coronal and root surfaces, as well as caries adjacent to restorations and sealants••These unifying, predominantly visual, criteria code a range of the characteristics of clean, dry teeth in a consistent way that promotes the valid comparison of results between studies, settings & locations• ICDAS criteria record both enamel and dentine caries and explore the measurement of caries activity in all three of the domains below
Epidemiology /
Public Health
Clinical Research
Clinical Practice
The ICDAS Detection codes are in use now and are recommendedThe ICDAS Assessment codes are part of a developing research agendaThe ICDAS System provides an evidence based framework to validate and explore the impact of existing and new-technology aids to caries “diagnosis”

2 A. VISUAL APPEARANCE
ICDAS-2ICDAS-2
Score5
DISTINCT CAVITY
Score6
EXTENSIVE CAVITY
SOUND
Score0
2. ACTIVITYDETECTION AND SEVERITY OF
THE LESION
SURFACE INTEGRITY
LOSS
Score3
OPACITYwithout
air-drying: WHITE,BROWN
Scores2W,2B
Ekstrand et al., modified by ICDAS (Ann Arbor), 2002; further modified by ICDAS (Baltimore) 2005
OPACITYwith air-drying:
WHITE, BROWN
Scores1W,1B
UNDERLYING GREY
SHADOW
Score4
Lesion in Dentin Lesion in Enamel
Lesion in
Enamel/Dentin
http://www.dundee.ac.uk/dhsru/news/icdas.htm

It must be emphasized that cleaning of the tooth surface and use of air are essential components in the use of these criteria, especially if differentiation between the lower categories (e.g., 0, 1 and 2) is considered necessary. – If cavitation is the threshold for sealant placement, then for surface
assessment teeth can be dried with cotton rolls, gauze, or compressed air
No magnification is required to make these calls. – Magnification may be useful for surface assessment; sealant
application; and retention checks; however, there is limited evidence in the scientific literature to support the adoption of magnification for visual assessment of tooth surfaces for sealant placement

Lussi (1993) compared unaided VE with that using 2x magnification, VE with bitewings, bitewings alone, and visual/tactile with gentle probing, and found that magnification did NOT significantly improve sensitivity.
Forgie et al. (2002) found that using 3.25x loupes for occlusal and interproximal assessment sensitivity was significantly higher than unaided vision. Specificity and PPV were similar to unaided vision .
However, although magnification is not necessary to detect lesions using the ICDAS-2 criteria, its use may affect the interpretation of the histological findings in relation to the criteria developed to correlate with it. -For example, a category 2 tooth could be viewed as a category 3 under magnification, and this would result in more teeth being eliminated from consideration of sealants.

Role of Magnification in Determining Role of Magnification in Determining CavitationCavitation

Hidden Caries or Mis-Diagnosis?Hidden Caries or Mis-Diagnosis? When no lesion is detected by visual examination, but
radiographic methods reveal a lesion into the dentin.
Noted in several reports in the 1980’s and 90’s (changes in histopathology of disease, slower progression, increased use of fluoride). Most studies at that time (that report a criteria) use cavitation as a threshold for caries.
Prevalence: Ranges from 3% to 50% of lesions only detected on radiographs, usually 8-15% in adolescent population (Ricketts et al, 1997)
Hidden caries does not seem to be a major problem when the clinical caries diagnostic criteria include non-cavitated diagnoses (Machiulskiene et al., Caries Res 1999)

Hidden Caries:Hidden Caries:
Of the clinically ‘sound’ surfaces, between 26%-50% in 14-20 year olds showed a radiolucency in the radiograph (Weerheijm et al., 1992)
Should we use other methods to aid in the visual detection?
Note: Sound teeth included everything except those with dentine caries clearly present-cavitation
“decalcification at the entrance of a discolored fissure or a dim white aspect in enamel”: Sound

Radiographic ExaminationRadiographic Examination
Radiographs show that demineralization is present, but when looked at in one period of time they cannot determine ACTIVITY
Sealants can arrest active lesions and prevent further demineralization. However, the radiolucency will remain.
<2% of sound surfaces diagnosed with dentin lesions on radiographs when non-cavitation was used as a threshold (Machiulskiene et al, 1999).

Fluorescence methods– QLF– Infra-red Fluorescence
Transillumination– FOTI– DiFOTI
Electrical Conductance– ECM
Digital Radiography– DDR
A New Way to “Look” at Dental A New Way to “Look” at Dental CariesCaries

Why new methods Why new methods
Goals: Detect lesions early More reliably than
before Quantification
Lesion Progression: Occlusal surface at 0, 4, 8, 12 months (QLF)

Fluorescence ExampleFluorescence Example
White Spot
Reflections obscuring image

QLF QLF in Vivoin Vivo System System
Light
CCD camerawith Filter
Dental mirror

QLF; scattering, absorption and QLF; scattering, absorption and fluorescence in sound and carious enamel fluorescence in sound and carious enamel
with sound dentin underneathwith sound dentin underneath
Van der Veen and de Josselin de Jong‘00Van der Veen and de Josselin de Jong‘00

QLF ExaminationQLF Examination

At a follow-up visit a second image it taken with an innovative At a follow-up visit a second image it taken with an innovative repositioning software, specifically made for this technique. repositioning software, specifically made for this technique.

Images can be taken and analyzed Images can be taken and analyzed over time to monitor non-cavitated over time to monitor non-cavitated
lesionslesions

QLF, summary of studiesQLF, summary of studies
Studies of natural caries on extracted teeth:
Sensitivity Specificity
Smooth Surfaces 0.94 0.80
Occlusal 0.77 0.74
Root caries 0.59 – 0.84 0.77 – 0.88
Secondary Caries 0.87 0.21

Infra-Red Infra-Red Fluorescence:Fluorescence: DiagnodentDiagnodent®®
Values Interpretation Recommendation
0-13 Sound no treatment
14-20 Enamel lesion preventive treatment
>20 Dentin Lesion preventive or restorative treatment depending upon risk
>30 Dentin Lesion restorative treatment
Lussi et al, 2001Note: As you lower the threshold, you increase Sens. and decrease Spec.(more false positives-more overtreatment)

ValidationValidation methodmethod
Detection methodDetection method CariesCaries
N=50N=50
No CariesNo Caries
N=950N=950
TotalsTotals
N=1000N=1000
Caries PresentCaries Present
TPTP
True PositiveTrue Positive
N=46N=46
FPFP
False Positive-False Positive-OvertreatmentOvertreatment
N=133N=133
N=179N=179
Caries Not presentCaries Not present
FNFN
False Negative-False Negative-UndertreatmentUndertreatment
N=4N=4
TNTN
True NegativeTrue Negative
N=817N=817
N=821N=821
Specificity: Specificity: 86%86% Lussi Lussi et al.,et al., 2001 2001
Sensitivity of a Detection System-Sensitivity of a Detection System-Low Caries Prevalence PopulationLow Caries Prevalence Population
Sensitivity: 92%

Limitations Stain in fissures (e.g., tea) Calculus and plaque Some dental materials, e.g. some sealants Adjacent to fillings, some resin materials give signal
Not a good correlation between high score and depth of lesion
Irresponsible to let a machine do the diagnosis (“It is not a stand alone diagnostic tool” http://www.kavousa.com/download/diagnodent.pdf)
Bader and Shugars (2004): Systematic review conclusions for dentinal caries:Sensitivity is almost always higher than traditional visual methods (range 0.19-1)Specificity is almost always lower (range 0.52-1).“The increased likelihood of false positives compared with visual methods limits is usefulness as a principal diagnostic tool”
Performance of Infra-Red FluorescencePerformance of Infra-Red Fluorescence

ACTIVITY: How to assess over time?ACTIVITY: How to assess over time?Increase in number of lesions in a certain time period (incidence, increment)Increase or change in certain lesions (size, etc)…
How to assess the caries lesion activity in How to assess the caries lesion activity in one appointment?one appointment?Relate to appearance of lesion (chalky white, rough, dull, high surface porosity)Relate to other patient factors (e.g., presence of plaque, closeness to gingival margin, presence of other lesions)(Ekstrand et al., 1998; Nyvad et al., 1999)
We do not have yet a way/tool to do this reliably in “real-time”We do not have yet a way/tool to do this reliably in “real-time”
Thylstrup and Fejerskov, 1994
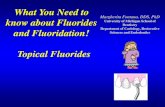
““WATCH”WATCH”

Caries Detected?
Caries Active Lesion?
InitialDiagnosis
(Based on physical appearance and location)
Changes Present?
Low Risk
Yes
No
No
At Risk No
Yes
Yes
High Risk Moderate Risk
Transmission

Once a pit and fissure surface is assessed and determined to be sound, questionable or carious (Incipient/enamel to frank/dentin caries), which categories are indicated for sealants?
What are the potential benefits and risks of sealing or not sealing sound, questionable or carious surfaces??
Does it really matter?Does it really matter?

“Clearly, since our diagnostic methods for assessing pit and fissure caries have been up to this time basically an educated guess, we must be placing sealants almost routinely over undetected incipient lesions” (Simonsen, 2002)
When we view the low sensitivity of current methods, we have always misdiagnosed a significant number of fissures calling them sound when they are carious (Fiegal, 2002).

Indications for Occlusal SealantsIndications for Occlusal Sealants (Siegel, 1995)
On sound, at risk surfaces
To arrest enamel lesions
Should the threshold be questionable or non-cavitated (incipient) caries lesions?

32
Diagnodent score used to find lesions underneath sealants:
Takamori et al., 2001: Diagnodent could find 53.5% of lesions under white sealants). False positives?
Is that lesion active or not? Was it there to begin with?
Do not use it to
diagnose secondary
caries http://www.kavousa.com/download/di
agnodent.pdf

Handelman, 1991 review of radiographic and bacteriologic studies (several years of follow up) on the therapeutic use of sealants
Concluded that “caries is inhibited and may in fact regress under intact sealants”. (Handelman et al. 1976; Handelman 1982; Mertz-Fairhurst et al., 1986, 1995).
Even with partially lost sealants no radiographic evidence of caries progression after 2 years (Handelman et al., 1986; Messer et al., 1997)

Heller et al. (1995) found in a fluoridated community that
initially sound surfaces were unlikely to become carious in 5 years and did not benefit greatly from the application of sealants (caries rate: 13% if not sealed vs. 8% if sealed).
There were, however, clear benefits in sealing incipient caries (52% if not sealed vs. 11% if sealed):
Incipient if dark staining; chalky appearance, or if explorer sticks, but no frank caries (cavitation). When in doubt used this classification.
Is it ethical to allow disease to occur before instituting a proven, effective preventive procedure?

Professional leadership has advocated that any fissure lesion judged to be limited to enamel is a candidate for sealant
therapy (Siegal, 1995, 2002)
Can we judge when caries is in enamel?
Is it necessary that it be limited to enamel, or is the question whether it is cavitated or not and in need of operative intervention?

The concern with sealing more advanced lesions is that it is believed that the potential for caries to advance when sealants are lost is greater than with incipient lesions
(Dentistry for the Child and Adolescent, 2004)

A 10-year clinical study evaluated bonded and sealed composite restorations placed directly over frank cavitated lesions extending into
dentin vs. sealed conservative amalgam restorations and conventional unsealed amalgam
restorations (Mertz-Fairhurst et al., 1998).
Time
Susceptibl
e Host
Carbohydrat
e-rich diet
Cariogenic Microflora Caries
X


How do we assess cavitated vs. non-cavitated lesions?How do we assess cavitated vs. non-cavitated lesions?– Visual assessment is appropriate– Teeth can be dried with cotton rolls, gauze, or compressed
air– Explorer may be used to clean the fissures and “gently”
confirm cavitations (i.e., breaks in the continuity of the surface); do not use sharp explorer under force
– Magnification (2x-4x) can be used, but is not required due to insufficient evidence on its effect in assessing cavitation
– Radiographs are unnecessary, especially in programs targeting children in grades 2 – 3
– Insufficient evidence to recommend other technologies to determine presence or absence of cavitation
SummarySummaryJ Pub Health Dent, 1995
* * *Non-Cavitated Cavitated

Thank you…Thank you…