Technical White paper Healthy, wealthy and wise
10
Technical White paper Healthy, wealthy and wise Real-time intelligence helps match beds and patients—for better care, for more people, at less cost.
Transcript of Technical White paper Healthy, wealthy and wise
Technical White paper
Healthy, wealthy and wiseReal-time intelligence helps match beds and patients—for better care, for more people, at less cost.
2 | December, 2012
Table of contents
1 Fixed beds, moving patients•Urgency and quality of care•Financial and regulatory drivers
2 Better communication and coordination•Symptomsofpoorpatientflow
3 From bed management—to patient placement•The promise of all-digital technology
4 Transforming the hub of patient flow•Before•Now
5 Informing management decisions•Before•Now
6 The numbers tell the story
7 Real-time visibility and workflow considerations
8 Do no harm: Best practice patient placement principles
9 Ready-to-go real-time patient flow—from the leaders in healthcare technology•CentralLogicCore™bedmanagementsoftware•HPTouchSmart™workstations,PCs,tablets,and
interactive digital displays•3rd-generation Intel® Core™ vPro™ processor technology
10 Getting started•Financing•Consulting
11 Learn more•About HP•About Central Logic•About Intel
Technical White paper | Solution
3 | December, 2012
Better patient flow, better patient experience
Hospitalsarerecognizingthatbetterpatientflowmanagementimprovesqualityofcare,resourceutilization,andcost-efficiency.
The2012PatientFlowChallengesAssessmentsurveyconducted by American Hospital Association (AHA) Solutions andHospitalsinPursuitofExcellence(HPOE)findshospitalsinvestinginpatientflowimprovementinitiativesthatspanprocess,staffing,andsystems—andreportingpositive resultsfromtheirefforts.1AccordingtoTonyBurke,CEO ofAHASolutions,“Patientflowdirectlyimpactsahealthcarefacility’s overall performance and can also play a strong role inpatientsatisfaction.”2
Fixed beds, moving patients
Patientflowmanagementstartswiththeearliestpointinpatienttransport—whetherapatientcomesinthrough,ER,OR,Dialysis,oranotherhealthsystem—throughthepatient’sdischarge,whethertoanothercarefacilityortheirownhome.Ahospital’sabilitytomanagepatientflowdependsonitsabilitytobalanceboth“demand”(patientneeds)and“supply”(finitephysicalandhumancareresources).
Atthecoreofpatientflowisbedmanagement,orcapacitymanagement.Patienttransfer,forexample, is operationally inseparable from capacity management, because proper patient placementdependsonwhatbedsareavailable.Gaps,delays,ormistakesinplacingpatientsintherightbed,withtherightlevelofcare,canhaveseriousnegativeclinical,operational,andfinancialimpacts.
Makingthebestuseofexistinghospitalresourcesiscriticalinlightofeconomicuncertaintiescoupledwiththeanticipatedgrowthindemandfromanagingpopulationandthenewlyinsuredunderhealthcarereform.
Evenasmallimprovementinefficiencyinpatientplacementandflowcanhavesignificantimpact.Forexample,reducingaveragelength-of-staybyjustfourhoursina275-bedhospitalistheequivalenttoincreasingthefacility’sphysicalcapacityby10beds.3
Urgency and quality of care
Capacitymanagementismuchmorethanjustthetimelyallocationandprovisioningofphysicalbeds.Urgencyandqualityofcarerequiresthatpatientsbematchedwiththerightbed—withtherightlevelofnursingcareandaccesstotherightspecialists,diagnosticsandtreatments—asquicklyaspossible.
1 Source AHA Solutions and Hospitals in Pursuit ofExcellence(HPOE).“ResultsandReportofthe2012PatientFlowChallengesAssessment:HospitalsConsiderPatientFlowEssentialtoCareandCompetitiveness.”2012
2 Source AHA Solutions press release, January 26,2012.http://www.aha-solutions.org/press/01.26.12-pfca-report-launch.shtml?source=prindex
3 Source CSC calculation based on CDC data on U.S.averagesforinpatientcare(non-Federalshort-stayhospitals)http://www.cdc.gov
Technical White paper | Solution

Thetimelinessofdefinitivecareisthemostcritical—andcomplex—aspectofpatientplacement,directlyimpactingthequalityofcareandpatientexperience.AccordingtoState-ledinitiativeslikethenurse-to-patientratiosmandateinitiatedin1999inCalifornia,criticalcarebedsintheICUand“step-down”unitsrequirea1:1nurse/patientratio,whilestandardcareis1:3,andgeneralmedicalandsurgicalunitsonlyrequirea1:5ratio.4
Ifnosuitablebedisavailable—orthetransfercenterisunabletoseethatsuchabedisavailable—anadmittedpatientmayneedtobeplacedinanother,lesssuitableareaofthehospital,andsubjectedtomultiplemoves.Forexample,anoncologypatientmayfirstbetransferredtoabedinthepediatricsurgeryward,orviceversa.Inaworstcasescenario,admission may be delayed and critically ill patients are boarded in an emergency department orhallwayuntilabedopenswiththeproperlevelofcare.
Gettingpatientsintotherightbed,thefirsttime,improveshealthoutcomesandpatientexperience,andreducesoveralllengthofstay.Theabilitytomakefast,informeddecisionsaboutpatientplacement—fromtransfer,admission,andinternaltransport,todischarge—isanimportantfactorinachievingmanyhospitalobjectives,includinghigherHospitalConsumerAssessment of Healthcare Providers Systems (HCAHPS) survey ratings, reducing unnecessary re-admissions,andmakingthemostefficientuseofallhealthsystemresources.
Financial and regulatory drivers
Properandefficientpatientplacementalsocontributestolowercostsforpatients,payors,andhospitals.Medicare,Medicaid,andprivateinsurerscloselymonitor“rightpatientstatus”asdesignatedbythepatient’sphysicianandcompare“intensityofservice”and“severityoforder”todefinereimbursablepatientstay.If,forexample,apatientcomestotheERwithabdominalpain,itcouldbeappendicitis,butinitiallabworkandsymptomsarenotdefinitive.Theinsurerwilltypicallypaythefullcostofovernightobservation.However,ifthepatientisunnecessarilyadmitted the next day due to inappropriate communications to the care team to ascertain status,theinsurermaynotpaythefullcost,leavingthehospitaltoabsorbthedifference.
HealthcarereformwillincreasinglytiereimbursementtohospitalqualityofcaremetricssuchasHCAHPSandotherstill-to-bedefinedefficiencymeasures.BeginningOctober2012,hospitalsfacedmaximumfinancialpenaltiesofupto1%ofMedicare/Medicaidreimbursementforexcessivereadmissionofpatientsinlessthan30days.In2014,themaximumfinancialpenaltiesdoubleto2%ofMedicare/Medicaidreimbursement.5
Thefinancialbenefitsofbeingabletoquickly,efficientlyplacepatientsintherightbedthefirsttimearecompelling.Theyinclude:
• Added capacity—Withoutphysicallyexpanding,throughmoreefficientutilizationandfasterturnoverofexistingcapacityandless“bedhiding”fromdelayedupdatingofavailability
• Increased revenue—Byprovidingcareformorepatients,withoutaddingresources
• Reduced costs—By optimizing use of hospital resources and proactively managing length-of-stay
• Improved staff productivity—By cutting the time teams (transport, emergency, transfer, nursing,EVS)spendlookingfordataandminimizing“workqueuing”
• Improved patient health and satisfaction—Byreducingwaittimesandtimelinessofdefinitivecare
• Shorter length-of-stay / Fewer readmissions—Through right level of care and coordinated discharge processes
4 | December, 2012
Technical White paper | Solution
4 SourceHealthAffairsSeptember2002vol.21no.553-64:http://content.healthaffairs.org/content/21/5/53.long
5 Sourcehttp://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html
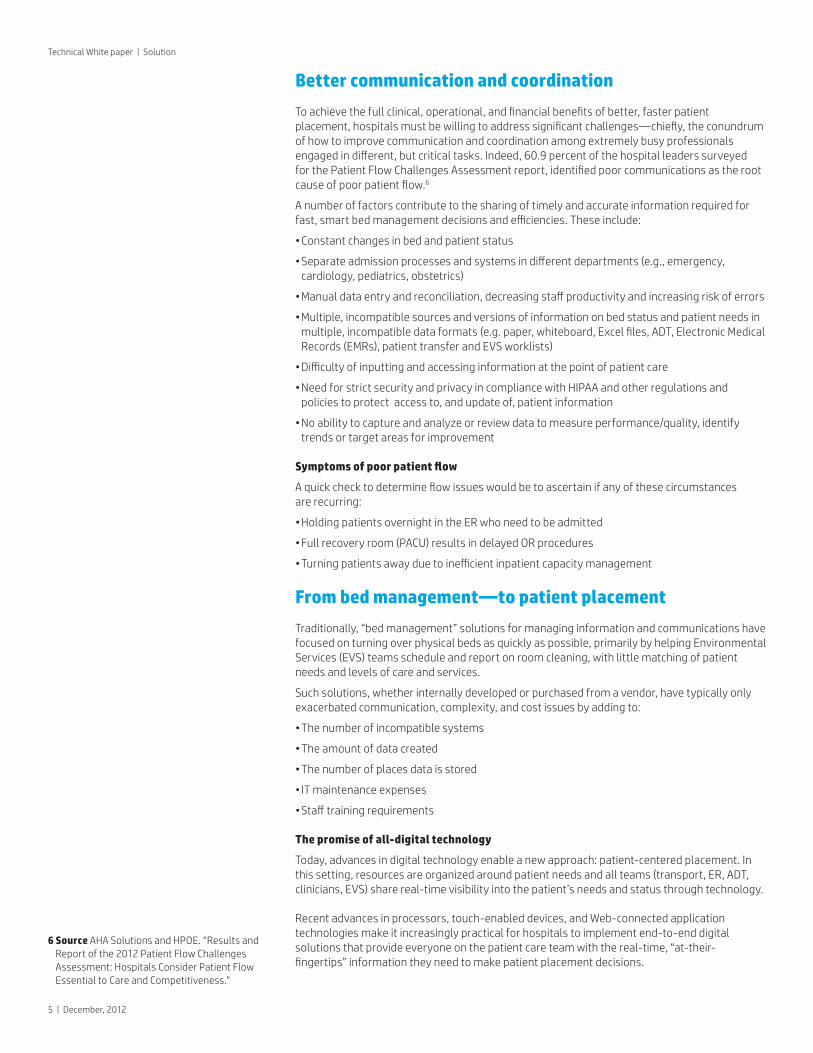
Better communication and coordination
Toachievethefullclinical,operational,andfinancialbenefitsofbetter,fasterpatientplacement,hospitalsmustbewillingtoaddresssignificantchallenges—chiefly,theconundrumofhowtoimprovecommunicationandcoordinationamongextremelybusyprofessionalsengagedindifferent,butcriticaltasks.Indeed,60.9percentofthehospitalleaderssurveyedforthePatientFlowChallengesAssessmentreport,identifiedpoorcommunicationsastherootcauseofpoorpatientflow.6
A number of factors contribute to the sharing of timely and accurate information required for fast,smartbedmanagementdecisionsandefficiencies.Theseinclude:
•Constant changes in bed and patient status
•Separateadmissionprocessesandsystemsindifferentdepartments(e.g.,emergency,cardiology, pediatrics, obstetrics)
•Manualdataentryandreconciliation,decreasingstaffproductivityandincreasingriskoferrors
•Multiple, incompatible sources and versions of information on bed status and patient needs in multiple,incompatibledataformats(e.g.paper,whiteboard,Excelfiles,ADT,ElectronicMedicalRecords(EMRs),patienttransferandEVSworklists)
•Difficultyofinputtingandaccessinginformationatthepointofpatientcare
•NeedforstrictsecurityandprivacyincompliancewithHIPAAandotherregulationsandpolicies to protect access to, and update of, patient information
•Noabilitytocaptureandanalyzeorreviewdatatomeasureperformance/quality,identifytrends or target areas for improvement
Symptoms of poor patient flow
Aquickchecktodetermineflowissueswouldbetoascertainifanyofthesecircumstances arerecurring:
•HoldingpatientsovernightintheERwhoneedtobeadmitted
•Full recovery room (PACU) results in delayed OR procedures
•Turningpatientsawayduetoinefficientinpatientcapacitymanagement
From bed management—to patient placement
Traditionally,“bedmanagement”solutionsformanaginginformationandcommunicationshavefocusedonturningoverphysicalbedsasquicklyaspossible,primarilybyhelpingEnvironmentalServices(EVS)teamsscheduleandreportonroomcleaning,withlittlematchingofpatientneedsandlevelsofcareandservices.
Suchsolutions,whetherinternallydevelopedorpurchasedfromavendor,havetypicallyonlyexacerbatedcommunication,complexity,andcostissuesbyaddingto:
•The number of incompatible systems
•The amount of data created
•The number of places data is stored
•IT maintenance expenses
•Stafftrainingrequirements
The promise of all-digital technology
Today,advancesindigitaltechnologyenableanewapproach:patient-centeredplacement.Inthis setting, resources are organized around patient needs and all teams (transport, ER, ADT, clinicians,EVS)sharereal-timevisibilityintothepatient’sneedsandstatusthroughtechnology.
Recent advances in processors, touch-enabled devices, and Web-connected application technologiesmakeitincreasinglypracticalforhospitalstoimplementend-to-enddigitalsolutionsthatprovideeveryoneonthepatientcareteamwiththereal-time,“at-their-fingertips”informationtheyneedtomakepatientplacementdecisions.
5|December,2012
6 SourceAHASolutionsandHPOE.“ResultsandReportofthe2012PatientFlowChallengesAssessment:HospitalsConsiderPatientFlowEssentialtoCareandCompetitiveness.”
Technical White paper | Solution
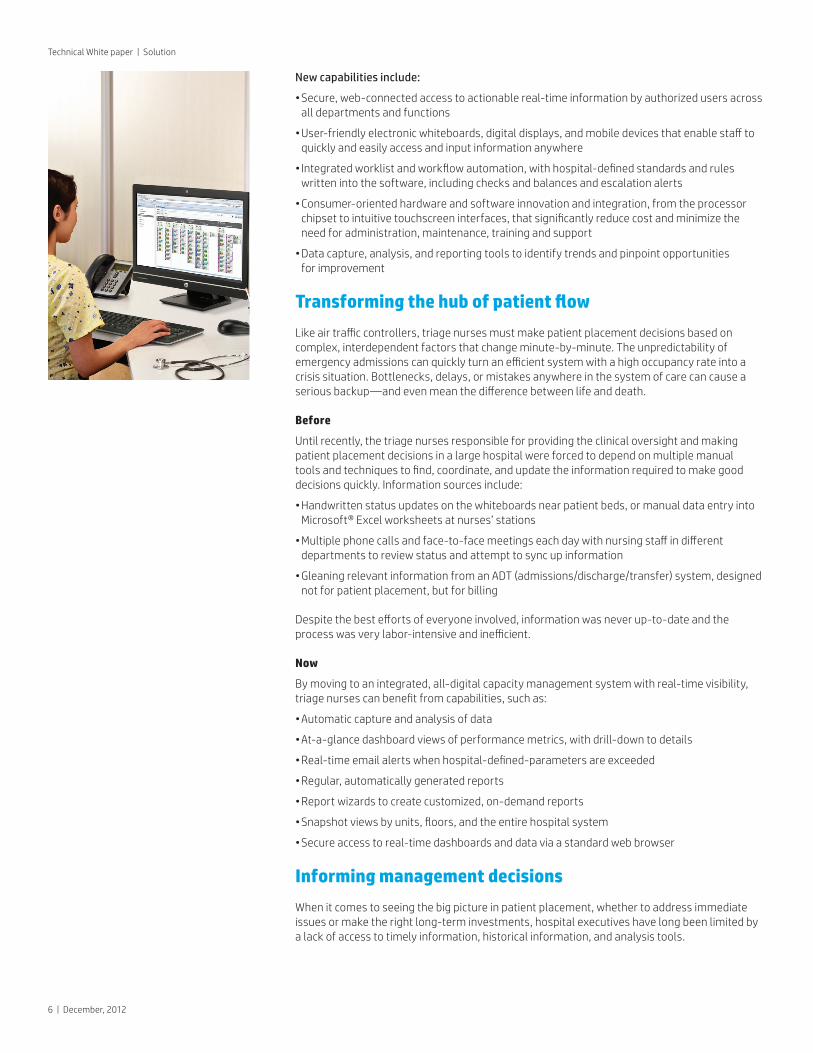
New capabilities include:
•Secure,web-connectedaccesstoactionablereal-timeinformationbyauthorizedusersacrossall departments and functions
•User-friendlyelectronicwhiteboards,digitaldisplays,andmobiledevicesthatenablestafftoquicklyandeasilyaccessandinputinformationanywhere
•Integratedworklistandworkflowautomation,withhospital-definedstandardsandruleswrittenintothesoftware,includingchecksandbalancesandescalationalerts
•Consumer-orientedhardwareandsoftwareinnovationandintegration,fromtheprocessorchipsettointuitivetouchscreeninterfaces,thatsignificantlyreducecostandminimizetheneed for administration, maintenance, training and support
•Data capture, analysis, and reporting tools to identify trends and pinpoint opportunities for improvement
Transforming the hub of patient flow
Likeairtrafficcontrollers,triagenursesmustmakepatientplacementdecisionsbasedoncomplex,interdependentfactorsthatchangeminute-by-minute.Theunpredictabilityofemergencyadmissionscanquicklyturnanefficientsystemwithahighoccupancyrateintoacrisissituation.Bottlenecks,delays,ormistakesanywhereinthesystemofcarecancauseaseriousbackup—andevenmeanthedifferencebetweenlifeanddeath.
Before
Untilrecently,thetriagenursesresponsibleforprovidingtheclinicaloversightandmakingpatientplacementdecisionsinalargehospitalwereforcedtodependonmultiplemanual toolsandtechniquestofind,coordinate,andupdatetheinformationrequiredtomakegooddecisionsquickly.Informationsourcesinclude:
•Handwrittenstatusupdatesonthewhiteboardsnearpatientbeds,ormanualdataentryintoMicrosoft®Excelworksheetsatnurses’stations
•Multiplephonecallsandface-to-facemeetingseachdaywithnursingstaffindifferentdepartmentstoreviewstatusandattempttosyncupinformation
•GleaningrelevantinformationfromanADT(admissions/discharge/transfer)system,designednot for patient placement, but for billing
Despitethebesteffortsofeveryoneinvolved,informationwasneverup-to-dateandtheprocesswasverylabor-intensiveandinefficient.
Now
Bymovingtoanintegrated,all-digitalcapacitymanagementsystemwithreal-timevisibility,triagenursescanbenefitfromcapabilities,suchas:
•Automatic capture and analysis of data
•At-a-glancedashboardviewsofperformancemetrics,withdrill-downtodetails
•Real-timeemailalertswhenhospital-defined-parametersareexceeded
•Regular, automatically generated reports
•Reportwizardstocreatecustomized,on-demandreports
•Snapshotviewsbyunits,floors,andtheentirehospitalsystem
•Secureaccesstoreal-timedashboardsanddataviaastandardwebbrowser
Informing management decisions
Whenitcomestoseeingthebigpictureinpatientplacement,whethertoaddressimmediateissuesormaketherightlong-terminvestments,hospitalexecutiveshavelongbeenlimitedbyalackofaccesstotimelyinformation,historicalinformation,andanalysistools.
6 | December, 2012
Technical White paper | Solution
Before
Gainingaccesstopatienttransferandbedmanagementinformationtypicallymeanthiringanoutside consultant or adding to the burden of already-busy professionals to collect and enter informationintoMicrosoft®Excelspreadsheets.Management-by-walking-aroundwasanotheroption.Unfortunately,problemswithpatientplacementandcapacitymanagementtypicallyonlybecameevidentduringacrisis,suchabedshortageorERboarding.
Now
Bymovingtoanintegrated,all-digitalcapacitymanagementsystemwithreal-timevisibility,hospitalexecutivescanbenefitfromcapabilities,suchas:
•Automatic capture and analysis of data
•At-a-glancedashboardviewsofperformancemetrics,withdrill-downtodetails
•Real-timeemailalertswhenhospitaldefinedparametersareexceeded
•Regular, automatically generated reports
•Reportwizardstocreatecustomized,on-demandreports
•Snapshotviewsbyunits,floors,andtheentirehospitalsystem
•Secureaccesstoreal-timedashboardsanddataviaastandardwebbrowser
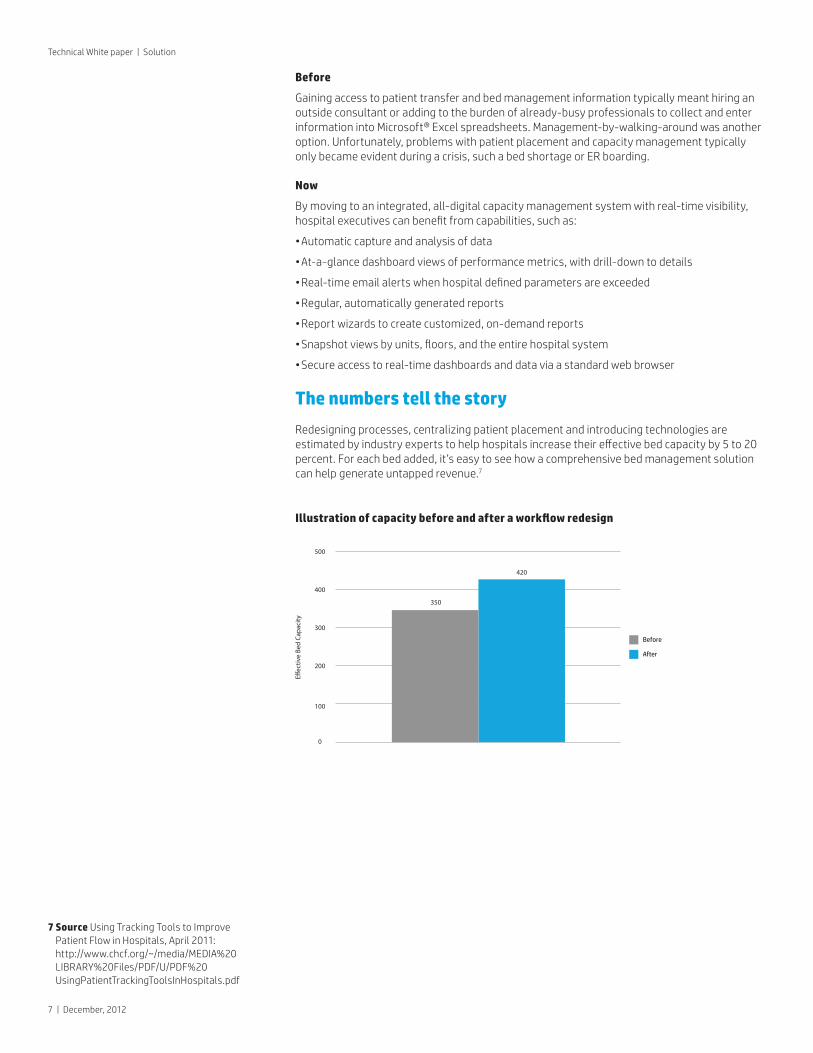
The numbers tell the story
Redesigning processes, centralizing patient placement and introducing technologies are estimatedbyindustryexpertstohelphospitalsincreasetheireffectivebedcapacityby5to20percent.Foreachbedadded,it’seasytoseehowacomprehensivebedmanagementsolutioncanhelpgenerateuntappedrevenue.7
Illustration of capacity before and after a workflow redesign
7|December,2012
Technical White paper | Solution
7 SourceUsingTrackingToolstoImprovePatientFlowinHospitals,April2011:http://www.chcf.org/~/media/MEDIA%20LIBRARY%20Files/PDF/U/PDF%20UsingPatientTrackingToolsInHospitals.pdf
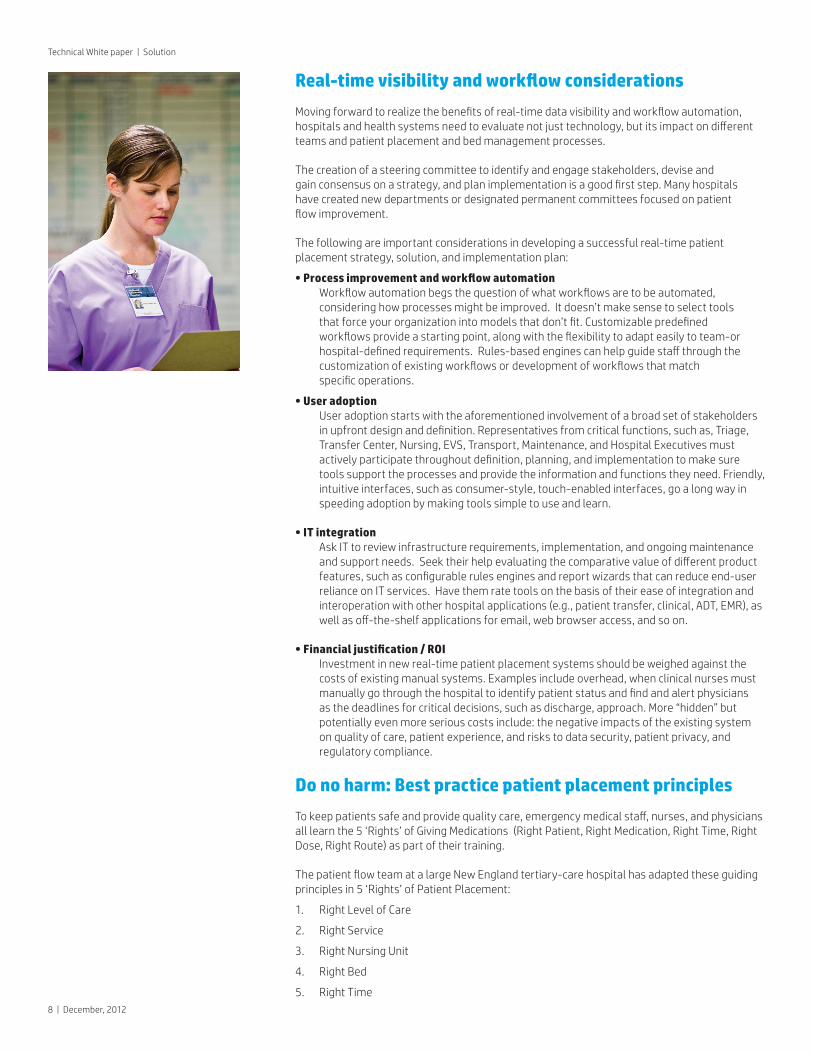
Real-time visibility and workflow considerations
Movingforwardtorealizethebenefitsofreal-timedatavisibilityandworkflowautomation,hospitalsandhealthsystemsneedtoevaluatenotjusttechnology,butitsimpactondifferentteamsandpatientplacementandbedmanagementprocesses.
Thecreationofasteeringcommitteetoidentifyandengagestakeholders,deviseand gainconsensusonastrategy,andplanimplementationisagoodfirststep.Manyhospitals havecreatednewdepartmentsordesignatedpermanentcommitteesfocusedonpatient flowimprovement.
Thefollowingareimportantconsiderationsindevelopingasuccessfulreal-timepatientplacementstrategy,solution,andimplementationplan:
• Process improvement and workflow automation Workflowautomationbegsthequestionofwhatworkflowsaretobeautomated,consideringhowprocessesmightbeimproved.Itdoesn’tmakesensetoselecttools thatforceyourorganizationintomodelsthatdon’tfit.Customizablepredefined workflowsprovideastartingpoint,alongwiththeflexibilitytoadapteasilytoteam-orhospital-definedrequirements.Rules-basedenginescanhelpguidestaffthroughthe customizationofexistingworkflowsordevelopmentofworkflowsthatmatch specificoperations.
• User adoption Useradoptionstartswiththeaforementionedinvolvementofabroadsetofstakeholdersinupfrontdesignanddefinition.Representativesfromcriticalfunctions,suchas,Triage,Transfer Center, Nursing, EVS, Transport, Maintenance, and Hospital Executives must activelyparticipatethroughoutdefinition,planning,andimplementationtomakesuretoolssupporttheprocessesandprovidetheinformationandfunctionstheyneed.Friendly,intuitiveinterfaces,suchasconsumer-style,touch-enabledinterfaces,goalongwayinspeedingadoptionbymakingtoolssimpletouseandlearn.
• IT integration AskITtoreviewinfrastructurerequirements,implementation,andongoingmaintenanceandsupportneeds.Seektheirhelpevaluatingthecomparativevalueofdifferentproductfeatures,suchasconfigurablerulesenginesandreportwizardsthatcanreduceend-userrelianceonITservices.Havethemratetoolsonthebasisoftheireaseofintegrationandinteroperationwithotherhospitalapplications(e.g.,patienttransfer,clinical,ADT,EMR),aswellasoff-the-shelfapplicationsforemail,webbrowseraccess,andsoon.
• Financial justification / ROI Investmentinnewreal-timepatientplacementsystemsshouldbeweighedagainstthecostsofexistingmanualsystems.Examplesincludeoverhead,whenclinicalnursesmustmanuallygothroughthehospitaltoidentifypatientstatusandfindandalertphysiciansasthedeadlinesforcriticaldecisions,suchasdischarge,approach.More“hidden”butpotentiallyevenmoreseriouscostsinclude:thenegativeimpactsoftheexistingsystemonqualityofcare,patientexperience,andriskstodatasecurity,patientprivacy,andregulatorycompliance.
Do no harm: Best practice patient placement principles
Tokeeppatientssafeandprovidequalitycare,emergencymedicalstaff,nurses,andphysiciansalllearnthe5‘Rights’ofGivingMedications(RightPatient,RightMedication,RightTime,RightDose,RightRoute)aspartoftheirtraining.
ThepatientflowteamatalargeNewEnglandtertiary-carehospitalhasadaptedtheseguidingprinciplesin5‘Rights’ofPatientPlacement:
1. Right Level of Care
2. Right Service
3. Right Nursing Unit
4. Right Bed
5. Right Time
8 | December, 2012
Technical White paper | Solution
Ready-to-go real-time patient flow—from the leaders in healthcare technology
Together,Intel,HP,andCentralLogicofferintegrated,easy-to-usesolutionsthatreducethetime,cost,andcomplexityofimplementingend-to-enddigitalpatientflow.
Thereal-timecapacitymanagementsolutioncombines:
Central Logic Core™ bed management software Intuitive,web-enabled,Coresoftwareprovidessecure,real-timecommunication,tracking, andupdatingofpatientandbedstatustooptimizequalityofcareandexperience. Featuresinclude:
•Multipleviewsof/andaccesstoactionabledata—authorizeduserssimplyclickonaroomorpatienttochangeastatusormakearequest
•SeamlessintegrationwithCentralLogicForeFront,theindustry’smostpopularpatienttransfersoftware
•Easyintegrationwithotherhospitalsystems,suchasADTandEMR
•Customizableautomatedworkflowtemplatesandrules-basedengine
•Real-time dashboards and reports
•Integratedworklistsfornursing,transport,transfer,EVSandmaintenancewithautomaticprioritization based on urgency of care and location
•Predictivereasoningtohelpoptimizecapacityutilizationandforecastwhenbedswill become available
•Assistedmatchingofpatientneedstohospital-definedbedattributes
HP TouchSmart Elite All-in-One PCs, HP Workstations, HP Business PCs, HP EliteBook Tablet PCs, and HP Interactive Digital Signage Displays
CentralLogicsoftwareonHPsystemsmakesiteasyforauthorizedpersonneltosecurelyaccessandupdatepatientandbedinformationonthespot.Forexample:
•HPTouchSmart8300All-in-OnePCfeaturingIntel®Core™vPro™processorswith23inchdiagonaltouchscreenmonitorofferacompact,ergonomicworkstationatthenurses’station
•PowerfulHPZ600WorkstationsfeaturingIntel®Xeon™processorsprovidebackendvirtualization and redundancy
•HP ElitePad tablets enable nurses, Environmental Services (EVS), and Transport teams to accessandenterthelatestinformationwheretheyworkastheycheckonpatients,cleanrooms, transfer patients
•HPDigitalSignageDisplayswithintegratedmulti-touchscreentechnologyreplaceantiquatedwhiteboardstoprovideup-to-the-minuteviewsofthefacility,units,bedstatus,assignedstaff, and patient status
3rd-generation Intel® Core™ vPro™ processor technology
HPhealthcaresystemstakeadvantageofadvancedIntelprocessortechnologyinnovations,whichbuildsecurity,self-maintenance,dataencryption,andotherfunctionalityintothechipsetandothersystemhardware,wheretheyarelessvulnerabletohackers,computerviruses,computerworms,andotherthreats.Forexample:
•Duringdeployment,securitycredentials,keys,andothercriticalinformationarestoredinprotectedmemory(notontheharddiskdrive)—anderasedwhennolongerneeded
•3rd-generationIntel®Core™processorswithvPro™technology8 support encrypted communicationwhileroaming
•Multi-layered,hardware-assistedmonitoring,security,management,reliability,andmaintenancecapabilitiesmakeiteasierforasys-admintomonitor,maintain,secure,andservice systems
9|December,2012
Technical White paper | Solution
8 Source Some functionality of this technology, such as Intel® Active management technology andIntel Virtualizationtechnology,requiresadditional3rdpartysoftwareinordertorun. Availabilityoffuture“virtualappliances”applications for Intel vPro technology isdependenton3rdpartysoftwareproviders. MicrosoftWindowsrequired.”
Rate this document
Sign up for updates hp.com/go/getupdated
Getting started
Integrated bed management solutions leveraging technologies from HP, Intel and Central Logic can help your organization optimize resources by providing real-time data visibilityandcustomized,automatedbedmanagementworkflows.Bettercommunicationsbenefitproviders,physicians,nurses,otherstaff,patients,andtheirfamilies.
Financing HPFinancialServicescanhelpyoutobegintotakeadvantageofend-to-enddigitalbedmanagementinyourhospitaltoday—withminimalimpacttocashflow.HPfinancingspecialiststakealifecycleapproachthathelpsyoutoconsidernotjustinitialpurchase,buttotalcost-of-ownershiptodevelopfinancingthatmakessenseforyourorganization.
Consulting CentralLogicconsultantsandauthorizedHPHealthSpecialistpartnerswithextensiveexpertiseindigitalpatientflowsolutionswillworkwithyourstafftointegratewithexistingworkflowsandprovideonsitetraining.
Learn more
About HP As a trusted supplier of information technology solutions to hospitals, clinics, and medical practicesaroundtheworld,HPisuniquelyequippedtosupportend-to-endpatientflowsolutionsinmajormedicalcenters,communityhospitals,andsmallcarecenters.TheHPHealthcareAllianceprogramcombinesofferingsfromindependentsoftwarevendorswithhardwarefromHPtodeliverintegrated,tailored,andtestedsolutionsthatwork.
Learn more about HP Healthcare solutions at: hp.com/go/healthcare
About Central Logic CentralLogicisthehealthcareindustry’sleadingproviderofinnovativepatientflowsoftwareandconsultativeexpertise.Since2005,thecompany’ssolutionshavetransformedpatienttransfer processes for some of the United States’ most respected medical systems and hospitals.CentralLogicworkscollaborativelywithphysicians,administrators,andstafftodesignanddeliverpatientflowsolutionsthatincreasepatientthroughputwhileconservinginternalresources.
Learn about Central Logic patient flow solutions at: centrallogic.com/solutions
About Intel Whereinformationandcaremeet:HPsolutionspoweredbytheIntel®vProprocessorfamilydeliversmart,long-lastingperformance.AdvancedandIndustrystandardtechnologiesfrom Intel help enable coordinated, customized care by contributing to the creation of an interoperablehealthITinfrastructure.
Learn about Intel and healthcare at: intel.com/about/companyinfo/healthcare/index.htm
Sharewithcolleagues
©2012Hewlett-PackardCompany,LP.Theinformationcontainedhereinissubjecttochangewithoutnotice. Intel,theIntellogo,IntelCore,CoreInside,IntelvPro,vProInside,andXeonaretrademarksofIntel CorporationintheU.S.and/orothercountries. CentralLogicisaregisteredtrademarkandCoreisatrademarkofCentralLogic,Inc..
4AA4-4658ENUS,December2012 ThisisanHPIndigodigitalprint.
Technical White paper | Solution