Technical Consultation on the role of Community Based ...
52
Technical Consultation on the role of Community Based Providers in improving Maternal and Newborn health Report August 2012 Maryse Kok Kathy Herschderfer Korrie de Koning
Transcript of Technical Consultation on the role of Community Based ...
Technical Consultation on the role of Community Based Providers
in improving Maternal and Newborn health
Report
August 2012
Maryse Kok
Kathy Herschderfer
Korrie de Koning

2
Table of Contents
Abbreviations .......................................................................................................................................... 4
Summary ................................................................................................................................................. 6
1. Introduction .................................................................................................................................... 9
1.1 Background of the Technical Consultation ............................................................................. 9
1.2 Objectives of the Technical Consultation ............................................................................. 11
1.3 Participants ........................................................................................................................... 12
1.4 Other initiatives .................................................................................................................... 12
2. Summary of plenary discussions ................................................................................................... 13
2.1 Introduction .......................................................................................................................... 13
2.2 Effectiveness and acceptability of CBP programmes ............................................................ 14
2.3 (Draft) task shifting guidelines WHO .................................................................................... 16
2.4 Postnatal care ....................................................................................................................... 18
2.5 Examples of CBP programmes (Jhpiego) .............................................................................. 19
3. Country case studies ..................................................................................................................... 20
3.1 Afghanistan ........................................................................................................................... 20
3.2 Bangladesh ............................................................................................................................ 22
3.3 Burkina Faso .......................................................................................................................... 25
3.4 Ethiopia ................................................................................................................................. 26
3.5 Ghana .................................................................................................................................... 28
3.6 India ...................................................................................................................................... 30
3.7 Malawi ................................................................................................................................... 31
3.8 Nepal ..................................................................................................................................... 33
3.9 Rwanda ................................................................................................................................. 36
3.10 Sierra Leone .......................................................................................................................... 38
4. Discussion, conclusions and next steps ........................................................................................ 39
4.1 Discussion of country case studies ....................................................................................... 39
4.2 Examples of innovation ......................................................................................................... 40
During the consultation, a number of innovative practices were identified. Some have shown
promise of impact and others have not been studied but they can be adapted for specific country
use and be added to Community Based Provider programmes where it is deemed appropriate. A
short summary of these innovations follows: .................................................................................. 40
4.3 Barriers and enablers to implementation of CBP programmes ............................................ 40
4.4 Knowledge gaps and policy challenges ................................................................................. 42
3
4.5 Summary of conclusions ....................................................................................................... 44
4.6 Next steps ............................................................................................................................. 45
ANNEX 1 PROGRAMME......................................................................................................................... 46
ANNEX 2 PARTICIPANT LIST .................................................................................................................. 48
ANNEX 3 COUNTRY MATRIX ................................................................................................................. 50

4
Abbreviations
AEC Area Executive Committee
AHW Auxiliary Health Worker
ANC Antenatal Care
ANM Auxiliary Nurse Midwife
ARI Acute Respiratory Infection
ASC Agent de Santé Communautaire
ASHA Accredited Social Health Activist
ASM Animatrice de Santé Maternelle
BCC Behavior Change Communication
BHW Basic Health Worker
CBA Community-based Agent
CBD Community Based Distribution
CBDA Community Based Distribution Agent
CBHC Community Based Health Care
CBO Community Based Organisation
CBP Community Based Provider
CBRHA Community Based Reproductive Health Agents
CCM Community Case Management
CHCP Community Health Care Provider
CHN Community Health Nurse
CHO Community Health Officer
CHP Community Health Post
CHS Community Health Supervisor
CHW Community Health Worker
C-SBA Community Skilled Birth Attendant
DHO District Health Officer
DHMT District Health Management Team
DMPA Depo Medroxy Progestrone Acetate
DOTS Directly Observed Treatment, Short-course
EmONC Emergency Obstetric and Neonatal Care
FCHV Female Community Health Volunteer
FHA Group Family Health Action Group
FHCI Free Health Care Initiative
FHH Family Health House
FHW Family Health Worker
FP Family Planning
FWA Family Welfare Assistant
GHWA Global Health Workforce Alliance
GHS Ghana Health Service
HA Health Assistant
HDA Health Development Army
HEP Health Extension Programme
HEW Health Extension Worker
5
HMIS Health Management Information System
HSA Health Surveillance Assistant
ICDS Integrated Child Development Service
IEC Information, Education and Communication
IMCI Community Integrated Management of Childhood Illnesses
IMR Infant Mortality Rate
IPC l’Initiative Privée et Communautaire
IRN Insecticide-treated bed nets
KMC Kangaroo Mother Care
LAM Lactational Amenorrhea Method
MCHP Maternal and Child Health Post
MCHW Maternal and Child Health Worker
MDG Millennium Development Goal
MMR Maternal Mortality Rate
MNCH Maternal, Newborn and Child Health
MNH Maternal and Newborn Health
NGO Non-Governmental Organisation
NID National Immunization Day
NMR Neonatal Mortality Rate
PBF Performance Based Financing
PHCU Primary Health Care Unit
PMTCT Prevention of Mother to Child Transmission
PNC Postnatal Care
PPH Postpartum Haemorrhage
SBA Skilled Birth Attendant
SDM Standard Days Method
SK Shasthya Kormis
SS Shasthyo Shebikas
TB Tuberculosis
TBA Traditional Birth Attendant
TT Tetanus Toxoid
vCHP voluntary Community Health Promoter
VDC Village Development Committee
VHC Village Health Committee
VHSC Village Health & Sanitation Committee
VHW Village Health Worker

6
Summary
On the 30th and 31th of May 2012, the Royal Tropical Institute organised a Technical Consultation on
the role of community based providers in improving maternal and newborn health. The meeting was
prepared in collaboration with Cordaid, the WHO, UNICEF, UNFPA and the University of North
Carolina and funded by Cordaid and the Dutch Ministry of Foreign Affairs. Forty-six participants
contributed to the consultation representing UN agencies, donor agencies, the academic
community, international and national NGOs and governments. Country representatives presenting
case studies from Afghanistan, Bangladesh, Burkina Faso, Ethiopia, Ghana, India, Malawi, Nepal,
Rwanda and Sierra Leone fed into the discussions.
The Technical Consultation focused on best practices and country experiences in improving the
quality and coverage of maternal and newborn health services involving community based
providers. For the purpose of the meeting, a community based provider was defined according to
the definition of “lay health worker” published by Lewin in 2010, as any health worker who performs
functions related to healthcare delivery; was trained in some way in the context of the intervention;
but has received no formal professional or paraprofessional certificate or tertiary education degree.
Plenary presentations highlighted the context of community based provider programmes within
health system strengthening, the evidence and acceptability of community-based provider
programmes, the role of task shifting to optimize the delivery of key interventions to attain
Millennium Development Goals 4 and 5, the role of postnatal home visits to improve maternal and
newborn health and the experiences from a multi-country programme implementing community
based providers of maternal and newborn health.
During the plenary sessions in which recent information was presented, it was shown that there is
evidence to support the implementation of promotional activities carried out by community based
providers (such as activities on immunization uptake and breastfeeding, improving tuberculosis
outcomes and reducing neonatal mortality and child morbidity and mortality) but there is still
insufficient evidence about the effectiveness of other tasks of community based health providers for
maternal and newborn health. Implementation of other tasks should be considered in the context of
rigorous research or targeted monitoring and evaluation. In terms of the acceptability of community
based provider programmes, the close relationship between community based providers and
recipients of their services is a major strength. Other factors that may be important to program
success include the development of services that are regarded as relevant by the recipients, regular
and visible support from other health workers and community leaders, and sufficient training,
supervision and incentives.
The roles and practices of the various types of community based providers in countries were
discussed. There were major variations seen in the nomenclature and definition of the health
workers, length and content of training and positioning within the health system (volunteer versus
professional; paid versus unpaid etc.), scope of work carried out (generalist versus specific health
issues) and the type of activities (health promotion and/or health care provision).
The main enablers (and in the absence of these enablers, they are barriers) to the implementation of
community based provider programmes were identified and included:

7
Policies: comprehensive policy framework and clarity of roles and tasks, continuity,
consistency and coordination in policy development and implementation, decentralization in
existing community structure;
Multi-stakeholder coordination and involvement: strong community ownership and
involvement, government coordination, NGO, bilateral and private sector involvement and
alignment and provider consultation;
Training and education: standardization of curriculum, fit for purpose, pre-service training
with in-service support and continuous education;
Recruitment and retention: community involvement in selection, clear criteria for
community based provider’s profile, incentives and motivation packages, recognition (i.e.
awards), career opportunities;
Enabling environment: political commitment, sufficient supplies and adequate working
conditions (including workload), teamwork and supervision, quality assurance mechanisms;
Community data collection and analysis to strengthen services.
The following knowledge gaps were identified for further research:
Impact of community based provider programmes in terms of equity of access and quality
and health outcomes and sustainability and how to assess this;
Packages, priorities and appropriate training for community based providers - which tasks
are needed and what is the most effective training and follow up strategy for a particular
task and type of community based provider?
Four main policy issues or constraints were identified:
How is policy operationalized and who is accountable?
How can activities of community based providers be regulated and supported within a legal
or professional framework?
In terms of human resources for health, how can an appropriate package of tasks for
community based providers be designed and applied and how can a pipeline for production
of health workers be developed to ensure coverage and professionalization and quality of
the workforce?
How can countries find the best balance and continue to invest in the training and
management of skilled birth attendants (such as midwives) and develop an effective
network of community based providers?
Five questions were formulated that could improve community based provider programme
implementation:
What areas should policy cover and what is in place already?
What lessons can be learned from other programmes on longer-term sustainability and key
policy debates?
What motivation and sustainable incentives are appropriate to different maturity levels and
objectives of programmes?
Which areas should be prioritised in a well-defined package to avoid multiple workloads?
What is the maximum/optimal package of services for community based providers?

8
The meeting closed with the announcement of actions from the participants. The organisers
promised to share the results of this consultation with other initiatives and meetings planned in the
following months that have similar objectives. Country representatives announced that they would
inform other stakeholders in their countries and pursue the discussions on barriers and enablers to
programme implementation in the local context. The Liverpool School of Tropical Medicine in
collaboration with the Royal Tropical Institute will integrate the results from this consultation in their
‘Reach Out’ programme starting this year in 6 countries. DFID is committed to supporting
coordination and follow up. UNFPA and other H4+ agencies and partners will collaborate to develop
a training manual for community health workers on reproductive, maternal and newborn health.
WHO will use the discussions from the Amsterdam meeting as input for the further development of
the task shifting guidelines and actions to improve postnatal care.
A dedicated website has been developed that contains relevant literature and documentation and all
the presentations given during the consultation: http://www.kit.nl/kit/Technical-consultation-
community-based-providers.

9
1. Introduction
This report presents the background, plenary sessions, discussions and conclusions of a two day
Technical Consultation on the role of Community Based Providers (CBPs) in improving Maternal and
Newborn health (MNH), held on the 30th and 31th of May 2012 in Amsterdam, the Netherlands.
1.1 Background of the Technical Consultation
Improving maternal health is one of the eight Millennium Development Goals (MDGs) adopted by
the international community in 2000. Under MDG5, countries have committed to reducing maternal
mortality but despite some reduction in worldwide maternal mortality, it is anticipated that most
countries will not meet the goal by 2015. The high number of maternal deaths reflects inequities in
access to health services and highlights the gaps between rich and poor, within and between
countries. Almost all maternal deaths occur in developing countries and most of these deaths are
preventable.1
One of the strategies adopted to combat maternal and newborn morbidity and mortality is ensuring
the involvement of skilled health personnel during pregnancy and in particular at childbirth.
Although these efforts have received increasing support from UN agencies and donors, about 40% of
the women in the world still give birth without the assistance of a skilled birth attendant. They
generally receive help from Community Health Workers (CHWs), Traditional Birth Attendants (TBAs)
or other lay persons2 (we call them Community Based Providers (CBPs)) who provide care and
support primarily in the community setting before, during and after childbirth.
In the 70’s, international organisations, including the WHO, promoted community-based care,
including antenatal care (screening of “at risk” women), the training of TBAs and the establishment
of referral mechanisms to deal with pregnancy and childbirth complications. This resulted in serious
investments made by governments, donors and non-governmental organisations (NGOs) in the
training of TBAs. Unfortunately, little attention was paid to a systematic analysis and evaluation of
the effects of TBA training programmes on maternal and newborn health outcomes. After two
decades without a marked improvement in maternal mortality, the international Safe Motherhood
partners3 withdrew support for further training and investments in TBAs. By 1997, international
attention had shifted to ‘skilled birth attendance’ and especially the presence of a Skilled Birth
Attendant (SBA) to assist delivering women. As efforts are being made to invest in training and
deployment of SBAs, there is growing emphasis on the need to keep on working with CBPs, to
ensure an unbroken chain of maternal and newborn health services from household to health facility
level.4
1 UNICEF, Levels and trends in child mortality; Report 2010 - Estimates developed by the UN Inter-agency Group
for Child Mortality Estimation. New York, United Nations Children's Fund, 2010. 2 WHO, 2005, “World Health Report 2005- Make every mother and child count, World Health Organisation
Geneva, Switzerland. 3 1997. Safe Motherhood Movement - Colombo Conference’s recommendations.
4 http://whqlibdoc.who.int/publications/2004/9241591692.pdf

10
Community-based strategies associated with health systems strengthening have been implemented
that aim to improve childbirth care for the rural poor, help reduce inequities in maternal and
newborn survival and stillbirth rates, and provide an effective transition to higher coverage for
facility births. The role of CHWs has been revitalized with more attention to maternal and newborn
health in their activities. A systematic review concluded that “CHWs may play a promising role in
providing pregnancy and childbirth care, mobilising communities, and improving perinatal outcomes
in low-income settings” 5. A recent Cochrane review studying the effects of maternal and child health
interventions provided by CHWs show promising benefits in maternal and newborn health6. These
benefits are related solely to the CHW role in health promotion, in particular Family Planning (FP)
and in antenatal and postnatal care as they generally do not provide assistance at birth.
Despite the paradigm shift to SBAs in the late 90’s, some countries have continued to invest in TBAs,
with varying results according to anecdotal evidence. A Cochrane Review from 2009 concluded that
“after more than three decades of experience, the evidence to support TBA training has been limited
and conflicting”. TBA training may contribute to a reduction in peri-neonatal mortality but there is
no conclusive evidence showing an improvement in maternal health. An important point brought up
by the authors of the review is that TBAs, besides assisting during deliveries, also fulfil an important
role in supporting and referring women during pregnancy and childbirth7. A recent systematic review
on the integration of TBAs with formal health services concluded that TBA integration can lead to an
increase of the facility use and skilled delivery.8 There is more emerging country specific qualitative
data that supports this, including the results from a study in Sierra Leone showing that TBAs are the
first point of contact for women when seeking care during pregnancy and delivery and are influential
in promoting facility delivery.9 There is sufficient evidence and experience to support the shift made
in the 90’s not to promote TBAs as birth attendants and there are an increasingly number of country
experiences documented that support the transitioning of TBAs from the role of birth attendant to
the role of community based promoter of facility based birth.
There is sufficient evidence on packages of interventions for maternal and newborn health that can
be implemented from the household and community levels to facility level.10 A high quality and
5 Darmstadt GL, Lee AC, Cousens S, Sibley L, Bhutta ZA, Donnay F et al. 60 Million non-facility births: who can
deliver in community settings to reduce intrapartum-related deaths? Int J Gynaecol Obstet 2009; 107 Suppl 1:S89-112. 6 Lassi ZS, Haider BA, Bhutta ZA. Community-based intervention packages for reducing maternal and neonatal
morbidity and mortality and improving neonatal outcomes. John Wiley & Sons, LTd; The Cochrane Library 2010, Issue 11. 7 Sibley LM, Sipe TA, Brown CM, Diallo MM, McNatt K, Habarata . Traditional birth attendant training for
improving health behaviours and pregnancy outcomes. Cochrane Database of Systematic Reviews 2007, Issue
3 Art. No.: CD005460. DOI 10.1002/14651858. CD005460.pub2. 8 Byrne A, Morgan A. How the integration of traditional birth attendants with formal health systems can
increase skilled birth attendance. Int J of Gyn nad Obst 115 (2011): 127-134 9 Herschderfer K, de Koning K, Sam-M’Balu E., Walker P, jalloh-Vos H, Detmar Symone. Barriers and Promising
Interventions for Improving Maternal and Newborn health in Sierra Leone. KIT 2011. 10
The Partnership for Maternal, Newborn & Child Health. 2011. A Global Review of the Key Interventions Related to Reproductive, Maternal, Newborn and Child Health (Rmnch ). Geneva, Switzerland: PMNCH.
11
coverage of integrated service delivery packages with functional linkages between the levels of care
are essential in improving maternal health11. Community based providers such as CHWs and TBAs
play an important role in promoting healthy behaviours and preventive actions, and in promoting
facility utilization.
There are currently many country initiatives that address the need for better quality and coverage of
maternal and newborn health services involving CBPs. These involve existing cadres and new cadres
that vary greatly in nomenclature, training, competencies, scope of work and positioning in
relationship to the formal health system. Lessons learned from these different initiatives can
contribute to identifying what works and under which circumstances and what are the remaining
challenges regarding quality and scaling up of community based maternal and newborn health
service delivery.
The focus of this Technical Consultation was to link the results from recent global initiatives, best
practices and country experiences in improving quality and coverage of MNH services, involving
CBPs. It looked in particular at the role of CBPs in remote and rural areas and in the poorest
developing countries. The consultation also addressed what is needed to make community based
maternal health services effective. Strengths and weaknesses of interventions and programmes
were discussed, informed by country case studies. Directions for further implementation were
formulated, including implications for policy.
1.2 Objectives of the Technical Consultation
The main questions addressed in the Technical Consultation were:
What do CHWs, TBAs and other community based cadres contribute to improved maternal
and newborn care?
What are their tasks and responsibilities?
What are enablers and barriers to implementation of programmes to improve MNH along
the continuum of care?
What are major knowledge gaps (research questions) that need to be addressed?
The objectives of this technical consultation were:
To identify and synthesize current knowledge and best practices on the roles and scale up of
CBPs of maternal and newborn care;
To identify gaps in adequate quality and coverage of community based maternal and
newborn health services;
To develop directions for research, policy and practice;
To agree, among the participants, to further joint action.
11
Kerber, K et al. Continuum of care for maternal, neonatal and child health, from slogan to service delivery. Lancet 370; 1358-69.

12
1.3 Participants
Representatives from Afghanistan, Bangladesh, Burkina Faso, Ethiopia, Ghana, India, Malawi, Nepal,
Rwanda and Sierra Leone participated and presented on the roles and responsibilities of CBPs in
MNH in their particular country. In addition, UN organisations responsible for policy development in
this area and researchers and experts in this field also attended the meeting. The meeting was
chaired by a freelance consultant with longstanding experience in international health. In total 46
participants attended the meeting. See Annex 1 for the programme of the Technical Consultation
and Annex 2 for the participants list.
1.4 Other initiatives
This Technical Consultation was not the only meeting on the role and contribution of CBPs that took
place in the first half of 2012. Other relevant meetings recently convened included:
Evidence Summit on Community and Formal System Support for Enhanced Community
Health Worker Performance, May 31 and June 1 2012 (convened by USAID Global Health
Bureau).
Community Health Worker Regional Meeting in Ethiopia, June 19 – 21 2012 (convened by
USAID-funded Health Care Improvement Project).
Health workers at the Frontline – Acting on what we know: consultation on how to improve
front line access to evidence-based interventions by skilled health care providers, 25-27 June
2012, Nairobi (convened by NORAD and coordinated by EQUINET).
These meetings were organised independently of each other, but they have certain commonalities in
the themes, target audience and participants. The Global Health Workforce Alliance (GHWA) is
playing a role in coordinating between these meetings in order to make sure that outcomes are
shared and further actions are coordinated.

13
2. Summary of plenary discussions
A number of plenary presentations were held during the first morning that aimed to set the stage for
the consultation by contextualizing the term Community Based Providers (CBPs) and showcasing
current knowledge, evidence and programmes to ensure common understanding and shared
knowledge about the current state of CBPs and CBP programming in the world.
2.1 Introduction
Kathy Herschderfer (KIT) kicked off the plenary sessions by sharing the background to the
consultation and contextualizing the term Community Based Provider by defining it according to the
definition of “lay health worker”. For the purpose of the Technical Consultation, a Community Based
Provider was defined as adapted from Lewin et al. 201012 as any health worker who performs
functions related to healthcare delivery; was trained in some way in the context of the intervention;
but has received no formal professional or paraprofessional certificate or tertiary education degree.
Issues relating to CBP programmes were framed in relation to the WHO Health System building
blocks to provide a reference and structure for the group discussions that would take place later.
These blocks are shown in the table below.
Table 1. Issues relating to CBP programmes and the WHO Health System building blocks
Leadership/ governance Regulation
Accountability mechanisms
Discrepancies between policy and practice
Stakeholder involvement
Stewardship
Health information
systems
Monitoring and Evaluation
Research
Financing Sustainability
Service delivery Communication between cadres and community
Referral
Supervision
Performance evaluation
Quality of care
Health seeking behaviour
Health workforce Recruitment
Training
Retention
Clarity of role
Motivation (incentives, salaries, career perspectives, respect, authority)
12
Lewin SA, Babigumira SM, Bosch-Capblanch X, Aja G, van Wyk B, Glenton C, Scheel I, Zwarenstein M, Daniels K, 2010, The effect of lay health workers on mother and child health and infectious diseases, The Cochrane Library, 2010, Issue 3, http://www.thecochranelibrary.com

14
Enabling environment Medicines
Supplies
Transportation
2.2 Effectiveness and acceptability of CBP programmes
Claire Glenton (Norwegian Knowledge Centre for the Health Services) presented “what is known
about the effectiveness and acceptability of lay health worker (CBPs) programmes for maternal and
child health”. This presentation was mainly based on two recently undertaken systematic reviews, a
specific study on uniject use by CBPs and five country case studies of national CBP programmes.
One of the reviews is an update of an earlier Cochrane review on the effectiveness of lay health
worker interventions that is in the process of being published. The second review was qualitative in
nature and covered the barriers and facilitators to the implementation of lay health worker
programmes for maternal and child health. Both reviews were prepared in connection with and
helped to inform the expert meeting held by the WHO in April 2012 to develop guidelines on task
shifting in maternal and newborn health. Pending the publication of these reviews and with
permission of the authors, brief summaries of the findings are presented in this report.
Effectiveness study
107 studies (all randomized controlled trials) were included in the review. The majority were
conducted in high income countries (n=65) but many of these focused on low income and minority
populations. The rest of the studies (n=42) were from middle and low income countries. The
following results were presented:
There is evidence of moderate quality (when comparing CBP programmes with usual care) that:
• CBPs probably increase immunization uptake in children
• CBPs probably increase the number of women initiating breast feeding
• CBPs probably increase the number of women who breastfeed their child at all
• CBPs probably reduce neonatal mortality
• CBPs probably improve pulmonary Tuberculosis (TB) cure rates
• CBPs probably have little or no effect on TB preventive treatment completion
There is evidence of moderate quality (when comparing CBP programmes with usual care) that:
• CBPs may reduce child morbidity and mortality
• CBPs may reduce maternal mortality
• CBPs may increase the likelihood of seeking care for childhood illness
CBPs provide promising benefits in promoting immunization uptake and breastfeeding, improving TB
outcomes, and reducing neonatal mortality and child morbidity and mortality, when compared to
usual care. For other health issues, evidence is insufficient to draw conclusions about the effects of
CBPs. Partly, this is because there were too few studies available that fulfilled the criteria for the
review. For example, there are not many randomized controlled trials measuring the effect of the
role of CBPs in distributing contraceptives.

15
Acceptability study
In this review, 53 studies were included, 17 from low income countries, 19 from middle income
countries and 17 from high income countries. First of all, great diversity was observed in CBP
programmes regarding CBP selection, tasks, supervision, training and incentives. In many available
studies these aspects are poorly described.
Selection. CBPs are often women that are selected by the community based on criteria such as
specific (communication) skills they have and respect in the community. Some CBPs are former TBAs
that have received training. Sometimes, they are required to have a specific level of education, but
this is not always the case.
Tasks. The services that CBPs offer range from simple to complex and from purely promotional to
curative. In low income countries, they more often perform curative tasks than in high income
countries.
Training of CBPs varied among the 53 studies included from a few days to 4 months. A lot of CBPs
had complaints about training: there is insufficient training, poor quality training, irrelevant training,
unskilled trainers and inflexible schedules (that are unable to respond to CBP turnover).
Supervision is usually provided by nurses. Supervision and regular field visits are seen as very
important, but often supervision is lacking, because of lack of skills, time and transportation.
CBP’s motivation and incentives. Various types of incentives are used for CBPs: from fixed salaries
to income out of the sale of drugs or supplements to monetary or non-monetary incentives (such as
food, drinks, and bicycles). CBPs had multiple motives to do their job: altruism, social recognition,
knowledge gain and career development. In some cases, CBPs with a fixed salary are not content
with it and CBPs that get income from selling drugs or supplements have sometimes problems with
recipients buying on credit. CBPs without a fixed salary sometimes ask for that, but sometimes not
as they believe that they will lose credibility if they receive a fixed salary. Incentives are highly
appreciated among CBPs, but most of the times sustainability is a problem.
CBP – recipient relationship. Most of the studies included presented the views on the CBP
programmes from the point of view of the CBPs themselves or their recipients. Sometimes, the
views of other actors like health professionals, community leaders, policy makers and supervisors
were also presented. The studies showed that recipients are generally positive about the CBP. Both
CBPs and recipients emphasised the nature of the relationship between them: the importance of
similarities between CBP and community, trust, respect, kindness and empathy. For recipients at
community level, accessibility of CBPs is very important. For CBPs on the other hand, flexibility of the
work is appreciated. Doctors and nurses were described by recipients as less accessible, less friendly,
more intimidating, and less respectful.
Closeness and confidentiality are sometimes a problem for recipients. Some concern was expressed
that home visits might lead CBPs to observe and share sensitive information or might lead
neighbours to suspect HIV+. Closeness is also sometimes a problem for the CBPs as they are exposed
to social and personal problems which can be, at times, emotionally draining and for which they

16
receive little support. Many CBPs feel the need to draw boundaries between their own and
recipients’ lives, but sometimes this is difficult.
CBPs involved in offering interventions that involved medication or procedures feared blame if
interventions were (perceived as) unsuccessful. Some recipients perceived CBP services as not
relevant to their needs or not sufficient, particularly when services focused on promotional
activities. In these cases, CBPs described feelings of impotence and demotivation and sometime
expressed a need to offer “real healthcare”.
CBP credibility is heightened through visible ties to the health system and active support and
participation of community leaders. However, this depends on the extent to which health systems
and community leaders have legitimacy, authority and respect. CBPs are as good as the health
system itself!
CBP - health professional relationship. Health professionals were often positive to CBPs, as they
were seen as reducing the workload and their role in communicating with the community was seen
as important. Some health professionals were less positive: they referred to added workloads; there
sometimes was fear of loss of authority and tension because of multiple roles (partners, supervisors,
evaluators). CBPs described good relationships with health professionals as: respectful, supportive,
and egalitarian (where CBPs were regarded as possessing complementary and valuable skills). CBPs
described poor relationships with health professionals as overly hierarchical (where CBPs were
regarded primarily as an extra pair of hands).
More research is needed on the following subjects:
Effectiveness of some interventions: more research, better quality research, and more
research in low and middle income countries
CBPs as direct substitutes for health professionals
“Generalist” CBPs
Resource use and cost-effectiveness of CBP programmes
The views of policy makers, NGOs, professional organisations
Different approaches to selecting, training and supporting CBPs
Different approaches to incentivizing and motivating CBPs, including impacts on attrition
Community engagement and involvement in CBP programmes
2.3 (Draft) task shifting guidelines WHO
Mario Merialdi (WHO Geneva) gave a presentation about “Optimizing the delivery of key
interventions to attain MDGs 4 & 5 through task shifting (Optimize4MNH)”. Currently, the WHO is
developing these guidelines with the aim of identifying and making recommendations about cadre(s)
of workers who can increase access to effective practices in a safe way. For many countries, task
shifting (a cadre that does not normally have the competency for a specific task is trained to deliver
these tasks, thereby increasing access) is much needed because of the lack of human resources for
health. Currently, there are some controversies in the field of MNH where guidance from WHO may
be helpful:

17
Misoprostol use by CBPs
TBA training to improve maternal and newborn outcomes
Non-physician clinicians performing caesarean sections
MgSO4 use by midwives
Provision of contraceptives by CBPs
For this Technical Consultation, only task shifting related to CBPs was discussed. These were still
draft recommendations, which were being developed as the result of an extensive process within
WHO and after consultation with international experts. Separate expert meetings were scheduled to
take place on abortion, contraception and Prevention of Mother to Child Transmission of HIV
(PMTCT) to feed into the final task shifting guidelines.
The table below shows draft recommendations for CBPs in MNH. (Arrow up means: task
recommended, arrow down means: task not recommended, arrow up as well as down means: task
could be considered but only in the context of rigorous research (RR) or strong monitoring and
evaluation (ME).
Table 2. Draft WHO recommendations for CBPs in MNH
Draft recommendations for CBPs
Promotional interventions for maternal and newborn health
Distribution of oral supplements to pregnant women ME, RR (aspirin)
Initiation and maintenance of antiretroviral treatment or
antiretroviral prophylaxis for pregnant women and for prevention
of HIV infection in infants
, RR
Continuous support during labour
Prevention and treatment of postpartum haemorrhage , RR
Delivery of neonatal resuscitation RR
Management of puerperal sepsis using parenteral antibiotics
before referral
RR
Initiation and maintenance of kangaroo mother care RR
Delivery of antibiotics for neonatal sepsis RR
Regarding antiretroviral treatment or prophylaxis for pregnant women and for prevention of HIV in
infants, the initiation of treatment or prophylaxis is recommended against while maintenance of
antivirals use is seen as an option in the context of rigorous research. The distribution of misoprostol
by CBPs for the prevention of postpartum haemorrhage is recommended. The above overview
18
shows once again that there is a lack of evidence on effectiveness of certain tasks performed by
CBPs in MNH. The WHO guidelines are expected to be published within a few months.
2.4 Postnatal care
Severin von Xylander (WHO Geneva) presented the outcomes from the Informal Meeting held this
year on provision of home-based care to mother and child in the first week after birth. In 2009, the
WHO and UNICEF published a joint statement on home visits for the newborn child that addressed
the utilization of community based providers. Home visits after birth are both for newborn and
maternal care (although maternal care is more variable than the newborn care component).
There is good evidence for home visits:
Home visits, in combination with community promotion practices, reduce Neonatal
Mortality Rate (NMR) by about 21%
Larger impact is likely in settings with high NMR and where most births occur at home
Data from India indicate that the impact extends to the post neonatal period
All studies show impressive improvements in newborn care practices
A postnatal care policy and practice survey was done in 47 countries. 62% of all countries had a
policy on postnatal care home visits (19/36 in Africa, 53% and 11/11 in Asia, 100%). The
implementation and coverage of postnatal care home visits was better in Asia than in Africa. The
content of home visits were mainly: promotion of appropriate care, identification of danger signs
and feeding support. The providers of the home visits were CBPs and/or health professionals
(nurses, midwives) and some of them got salary and others only incentives (monetary or non-
monetary). Difficulties of home visit programmes that were identified were:
Maintaining competencies and motivation of the care provider
Health systems support
Recruitment and training
Community participation
Policy adoption
In order to have an effective system of home visits for the postnatal period, the following health
systems issues need to be in place:
A human resources plan: category of health workers, workload, population deployment,
regulations, job descriptions, remuneration
An implementation plan: stakeholder involvement, district based planning, targeting high-
risk populations and planning for scale-up
A national and district monitoring plan: targets, indicators, data drive decision making
Also, demand creation and community participation are essential for increasing coverage and
sustainability. Home visit programmes create demand for services at first level facilities and referral
hospitals, so they shouldn’t work in isolation.
WHO will organise an Expert Meeting on postnatal interventions in general, which will result in
technical guidance for countries on postnatal care.
19
2.5 Examples of CBP programmes (Jhpiego)
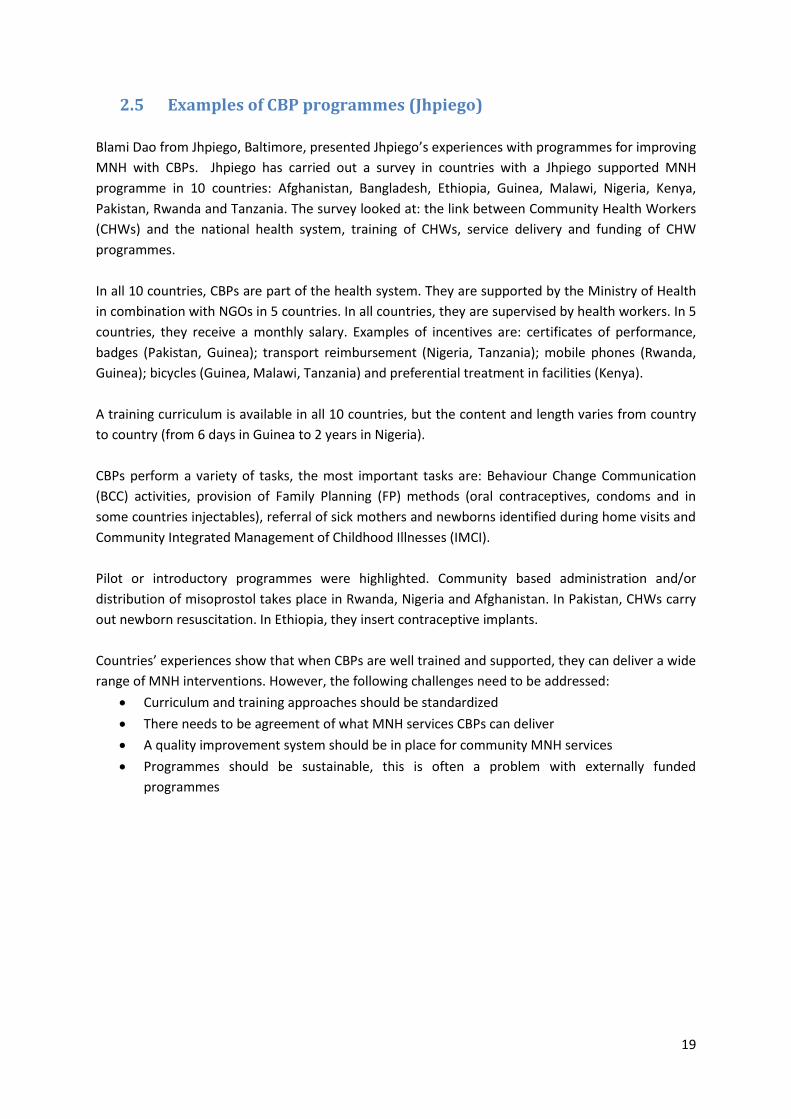
Blami Dao from Jhpiego, Baltimore, presented Jhpiego’s experiences with programmes for improving
MNH with CBPs. Jhpiego has carried out a survey in countries with a Jhpiego supported MNH
programme in 10 countries: Afghanistan, Bangladesh, Ethiopia, Guinea, Malawi, Nigeria, Kenya,
Pakistan, Rwanda and Tanzania. The survey looked at: the link between Community Health Workers
(CHWs) and the national health system, training of CHWs, service delivery and funding of CHW
programmes.
In all 10 countries, CBPs are part of the health system. They are supported by the Ministry of Health
in combination with NGOs in 5 countries. In all countries, they are supervised by health workers. In 5
countries, they receive a monthly salary. Examples of incentives are: certificates of performance,
badges (Pakistan, Guinea); transport reimbursement (Nigeria, Tanzania); mobile phones (Rwanda,
Guinea); bicycles (Guinea, Malawi, Tanzania) and preferential treatment in facilities (Kenya).
A training curriculum is available in all 10 countries, but the content and length varies from country
to country (from 6 days in Guinea to 2 years in Nigeria).
CBPs perform a variety of tasks, the most important tasks are: Behaviour Change Communication
(BCC) activities, provision of Family Planning (FP) methods (oral contraceptives, condoms and in
some countries injectables), referral of sick mothers and newborns identified during home visits and
Community Integrated Management of Childhood Illnesses (IMCI).
Pilot or introductory programmes were highlighted. Community based administration and/or
distribution of misoprostol takes place in Rwanda, Nigeria and Afghanistan. In Pakistan, CHWs carry
out newborn resuscitation. In Ethiopia, they insert contraceptive implants.
Countries’ experiences show that when CBPs are well trained and supported, they can deliver a wide
range of MNH interventions. However, the following challenges need to be addressed:
Curriculum and training approaches should be standardized
There needs to be agreement of what MNH services CBPs can deliver
A quality improvement system should be in place for community MNH services
Programmes should be sustainable, this is often a problem with externally funded
programmes

20
3. Country case studies
This chapter presents a detailed overview of the country case studies, highlighting the key points
that emerged from the country group discussions in which countries presented the role of CBPs in
MNH and enablers and barriers, knowledge gaps and research questions. For an overview of CBP
programmes in the various participating countries, see Annex 3.
3.1 Afghanistan
Current situation
Afghanistan presented its Community Based Health Providers Programme. The current cadres in
Community Based Health Care (CBHC) are:
CHWs. They serve between 1,000 and 15,000 population. Scope of services: health
education, promotion of the appropriate use of health services, treatment and referral for
common illnesses and establishment and support of Family Health Action Groups (FHA
Groups, see below).
Community Health Supervisors (CHSs). They supervise the CHWs.
Shura-e-Sehi. These are community health committees, consisting of representatives of the
community. There are 2 types: 1) health facility level and 2) health post level. They support
CHWs and other health staff.
FHA Groups: groups of 10-15 women established by female CHWs in their catchment areas
in order to support them in promoting healthier homes, lifestyle and increase the use of
available health services. Selection criteria: women with young children, who are respected
in the community, trusted by the female CHW, willing to volunteer, basic literacy/ education
is an advantage but not necessary. These FHA Groups are implemented in 9 districts, but are
going to be expanded all over the country.
Family Health Worker (FHW): volunteers that give health education in secondary schools.
There were also 2 midwives at the Technical Consultation who shed more light on the community
midwifery programme and their relationship with CBPs. Community midwives work in Family Health
Houses (FHHs) in rural areas, where deliveries take place, but also antenatal care and health
education. The FHHs are part of a pilot project in 3 districts.
The main tasks of CHWs in Afghanistan are:
Health education (different topics, including MNH)
Referral (encouraging skilled birth attendance, identification of women with danger signs)
First aid
Treatment of common diseases (including administering certain types of antibiotics)
Family Planning (66% of the provision of FP methods is carried out by CHWs who provide
condoms, pills and Depo Medroxy Progestrone Acetate (injectable, DMPA) and they
promote natural FP (Lactational Amenorrhea Method, LAM)
Antenatal care and referral for postnatal care

21
CHWs are selected by the community and do not receive a salary. Seventy percent of the CHWs in
Afghanistan are illiterate. All receive 6 months of training using adapted materials and working with
images and checklists. The training consists of 3 months theory, 2 months of practice and a final
month of theory. After completion of the training and as reflected in CBHC national package, they
receive 6 days of refresher training every 6 months.
CHWs are selected from the community and they participate in all events at community level,
conduct family visits and have close relationships with community members. As they are responsible
to report to the health facility, they have monthly meetings at the health facility level and are
supervised by the CHS. Each health post has 2 CHWs, one male and one female.
Enablers and barriers
The following enablers were identified during the session:
CHWs are seen as very important by the Ministry and will be scaled up from 23,663 to
40,000. There is political will for CHWs.
CHWs are selected by the community.
The utilization of community mapping contributes to better services at the community level.
CHWs are accountable to FHA Groups and other community based committees (the Shura e
Sehi).
Although CHWs are volunteers and do not receive a salary, they are provided with
transportation reimbursements and receive a per diem during training days and community
campaigns. They also receive in kind donations from community members.
CHWs are supervised by CHSs, who are responsible for a certain facility and also responsible
for the supply of drugs and health education materials.
The CBHC is a government programme. It was concluded that good coordination and partnership
between government, community, NGOs and UN agencies is crucial for success as the involvement
of different parties can be challenging.
Knowledge gaps and research needs
In Afghanistan, rural areas have a better uptake of the Community Based Health Providers
Programme. This is an issue to look into; what can be done to improve community health in urban or
semi-urban areas?
In many districts, community midwives form an important cadre in MNH service provision. Referral
from CHWs to community midwives needs to be looked at; how can the referral system be improved
and how can CHWs and community midwives coordinate their activities and work together?
In general, there is a need for a formal evaluation of the Community Based Health Providers
Programme. This has not been done yet and is needed before going to scale. It is important to know
what the impact is of CHWs on MNH in Afghanistan.

22
3.2 Bangladesh
Current situation
Bangladesh has a high number of CBPs, called Basic health workers (BHWs) who are supported by
the government as well as NGOs. They have different names, tasks, responsibilities and skills and
they are not equally distributed throughout the country. In the table below, the various types of
CBPs are presented.
Table 3. CBPs in Bangladesh
Category of CBP Organisation Major roles/
responsibilities
Knowledge and skills Training
HA (Health
Assistant) and
FWA (Family
Welfare Assistant)
(>38,000)
Government Registration of women
and children, service
delivery at community
clinics, immunization,
satellite clinics for MNH
care, case detection for
communicable and
non-communicable
diseases, geographical
reconnaissance, health
care during disasters,
conduction of delivery
at community clinics,
community case
management of under
5 children.
Class 12, able to
vaccinate, identify
danger signs and case
detection, management
of pneumonia/
diarrhoea/ malaria,
knowledge of FP
methods, referral
knowledge, counselling
and health education,
nutrition counselling.
HA and FWA receive 21 days
basic training by the
government on essential
service package primarily
focusing on primary health
care. In addition HA and
FWA also get separate
training from different
programmes (malaria
detection and management,
FP methods, immunization,
counselling on ANC, PNC
etc.) There are also
refreshers training on
different programme
components, however there
is no national plan for
refresher training of these
cadres of CHWs.
CHCP (Community
Health Care
Providers)
(12,500)
Government Supervision of the
community clinic,
service delivery
especially for mother
and children, referral,
FP service delivery,
record keeping and
reporting.
Class 12, computer
skills, communication
skills, treatment of
minor illness, case
detection and referral.
CHCP receive 12 weeks (6
weeks theoretical and 6
weeks practical) basic
training by the government.
This training covers all
primary care components
including treatment of
minor illness, Community
Case Management (CCM)
etc. There is no planned
refresher training for
CHCPs.
C-SBA (Community
Skilled Birth
Attendant)
(> 13,000)
Government Provide ANC/PNC
(antenatal and
postnatal care),
conduct normal
delivery at
home/community clinic
level, identification of
complicated delivery
and referral,
resuscitation for
Conducting delivery,
assess and identify
complicated cases and
referral, resuscitation
for asphyxia.
C-SBAs receive 6 months C-
SBA training by the
government. No planned
structured refresher training
is in place for the C-SBA.

23
asphyxia, counselling
on MNH and nutrition.
SS (Shasthyo
Shebikas) (8,500),
SK (Shasthya
Kormis, supervisor
of SS) (91,000),
BRAC Pregnancy registration,
ANC, PNC,
immunization, iron-folic
acid, de-worming,
referral of
complications, iodized
salt, early initiation of
breast feeding,
exclusive breast feeding
up to 6 months,
micronutrients:
sprinkles, vitamin A,
diagnosis and
management of ARI
(Acute Respiratory
Infection), diarrhoea
and malnutrition, water
and sanitation, FP,
health education, basic
curative services,
sputum collection,
DOTS (Directly
Observed Treatment,
Short-course), malaria
treatment, ITN
(Insecticide-treated bed
nets) distribution.
Class 5-8 grade or less,
able to vaccinate,
identify danger signs
and case detection,
management of
pneumonia/ diarrhoea/
malaria, knowledge on
FP methods, referral
knowledge, counselling
and health education,
nutrition counselling.
Shasthyo Shebika receive 15
days training and Shasthya
Kormi receive 3 weeks
training by BRAC. Apart from
this basic training, BRAC
CHWs also receive special
training on different MNCH
issues over the years.
Other NGO CBPs CARE, PLAN,
SSFP and
other NGOs
Pregnancy registration,
ANC, PNC,
immunization, iron-folic
acid, de-worming,
referral of
complications, iodized
salt, early initiation of
breast feeding,
exclusive breast feeding
up to 6 months,
micronutrients:
sprinkles, vitamin A,
diagnosis and
management of ARI,
diarrhoea and
malnutrition, water and
sanitation, FP, health
education, basic
curative services,
sputum collection,
DOTS, malaria
treatment, insecticide-
treated bed nets
distribution.

24
HAs, FWAs and CHCPs are government recruited health workers who receive a monthly salary from
the government. C-SBAs are also government workers (FWA and female HA) and get a monthly
salary as well. Regarding the BRAC supported SSs and SKs, the SKs receive a monthly salary but the
SSs do not. SSs act as depo-holder and receive some benefits out of the sale of commodities to the
community. Some of the NGO CHWs receive monthly honorarium but not all. Some project based
MNCH programmes provide incentives for the CHWs.
HAs, FWAs, CHCPs and C-SBAs are supervised through the existing government supervisory
mechanism. There is a first line supervisory structure (including a Health Inspector, Assistant Health
Inspector and Family Planning Inspector) within the government to supervise the front-line workers.
NGO CHWs are supervised by the NGO’s own supervisory mechanism.
The NGO CHWs are selected from the community; they belong to and are very much embedded
within the community. CHWs of different NGOs who are working in different MNCH interventions,
covering more than 30 districts (out of 64 districts) supported by UN agencies and other
development partners, are closely linked with the local health system. They are mainly responsible
for household counselling on nutrition, ANC, PNC, essential newborn care, CCM of pneumonia and
diarrhoea, identification of complicated cases and referral, facilitating community support group
activities for demand creation and increasing care seeking from trained providers etc. However in
some of the districts, BRAC CHWs are working parallel to the government system and are not very
much linked with the formal health system, except those CHWs who are working under the TB
programme.
In Bangladesh, CBPs are also involved in distribution of Misoprostol for the prevention of
Postpartum Haemorrhage (PPH). They are also involved in maternal and perinatal death reviews.
Enablers and barriers
UNICEF has supported the Maternal, Neonatal and Child Health Intervention programme
implemented by the Ministry of Health and Family Welfare of Bangladesh. One of the strengths of
the programme was that the focus was on multiple levels: community (mobilization), health systems
(strengthening) and local government (involvement), with effective linkages between these 3 levels.
One difficulty addressed was retaining appropriate skills (and quality of service delivery) as training
of new staff and continuous education is not often carried out. Furthermore, it was noted the CBPs
need more acknowledgement and recognition.
The distribution and coverage of CBPs, especially in hard to reach areas as in Chittagong Hill Tracts, is
another issue of concern. It is difficult to recruit CBPs due to a low level of education and lack of
adequate incentives or remuneration. Furthermore, government and NGOs should look at the
uniformity of the skills and service delivery modalities for all the different CBPs. Currently there is no
standardization of roles, tasks and job description.
Knowledge gaps and research needs
Performance appraisal of CBPs functions could be looked into. Strategies to promote retention of
CBPs should also be researched. Issues on incentives and motivation must be included. There should

25
be more research on performance tracking, monitoring and supervision. What is working and what
will improve the effectiveness of CBP programmes? The main research gaps that were identified
during the Bangladesh session were:
What is the attribution factor of the CBP to the success in the reduction of the Maternal
Mortality Rate (MMR) and Infant Mortality Rate (IMR)?
What are the services, roles and skills that a CBP needs and how can it be standardized?
3.3 Burkina Faso
Current situation
The presentation from IPC (l’Initiative Privée et Communautaire contre le VIH et le SIDA au Burkina
Faso), an HIV & AIDs NGO) described an innovative “social mapping” pilot project, supported by the
Ministry of Health and UNFPA. IPC covers a population 900,000 (6 districts). The social map is a
planning, implementation, monitoring and evaluation tool which ensures that all social groups are
taken into account and real-time data on population and services are available.
The project implementation process is as follows:
A baseline survey is conducted to set up an extended family register – intensive
collaboration/negotiation/awareness raising with community stakeholders to get buy-in –
targets children (<5) and all women of childbearing age.
Identification, selection and training of 1 moderator for every 2-3 villages and an ASC (Agent
de Santé Communautaire, a CHW), 1 or 2 per village, in collaboration with community.
Moderators hold monthly meetings with the ASCs (opportunity to provide training). They are
supervisors of the ASC.
Data collected quarterly and validated with village chief – village database established
(population number, number of pregnant women, burden of disease, common diseases,
contraceptive supplies distributed, births, deaths).
ASCs and health workers at the health centre review data monthly for planning of health
services.
Annual general village meetings are held to share data and discuss them.
The roles and responsibilities of ASCs are primarily promotional:
Malaria: home based care of uncomplicated cases of malaria, monitoring the use of ITNs,
conducting awareness sessions on malaria.
Malnutrition: raise awareness on exclusive breast feeding during the first 6 months after
birth, raise awareness on complementary foods made of local products after 6 months up till
24 months of age, micronutrient supplementation – pregnant women and children under 5
and care and support for moderate malnutrition.
Immunization promotion (not conducting the vaccination itself).
Promotion of reproductive health – promotion of ANC and health facility birth, identification
of pregnant women at village level, raise awareness on essential obstetric care and danger
signs during pregnancy, labour and postpartum, promote voluntary testing, distribution of
FP supplies, PNC visiting, breastfeeding promotion.
Prevention and community care of diarrheal diseases, promotion of good hygiene practices,

26
Raise awareness on danger signs for ARI.
The moderators get a salary of 30 USD quarterly and ASCs are volunteers but get results-based
stipend of about 6 USD per month. ASCs get a general 1 week training and subsequent 1 week
trainings for different themes (like malaria, TB). There is no entrance level, they have to be able to
read and write. The training is given in the local language. After 2 years, they get a refresher course.
Enablers and barriers
An enabler of this CBP programme is the community participation: the community is very involved
and their involvement drives the process. The community determines health priorities and meets
regularly. This is done in cooperation with health workers and health centres. The Ministry of Health
predicted that communities would not provide “sensitive” information, but they even shared
abortion data.
A challenge is to find enough literate community moderators. The original plan was to primarily
recruit women in the age range 25-49 and who were married and literate. But because it was hard to
find sufficient recruits who met these criteria some illiterate women (40%) were recruited and some
male moderators were recruited as well. The data collection tools were sometimes too difficult for
the moderators. Other challenges were the supply of commodities, weak referral systems, the
quality of care at health centre level, low involvement of some health workers at health centres
(they perceived social mapping as an added workload) – generally there was a need for more
commitment to this process from formal health sector. Furthermore, it was difficult to involve men.
Lastly, the financial sustainability of this programme is not guaranteed yet.
Knowledge gaps and research needs
There is a need for better evidence on effectiveness of this programme. This evidence is needed in
order to decide on the feasibility of scale-up.
3.4 Ethiopia
Current situation
In 2004, Ethiopia launched its Health Extension Programme (HEP), as a national health policy priority
to include community-based health service provision as a core component of the broader health
system. This had the overall goal of creating a healthy society and reducing maternal and child
mortality and mortality. A cadre of largely female Health Extension Workers (HEWs) have been
trained for one year and they receive government salaries. They work in the community delivering
primary health care services, falling under sixteen overall health extension packages – maternal and
child health falls under Family Health Service. Two HEWs function out of a health post covering an
average population of five thousand and were initially intended to be spending 75% of their time in
the community. They are supported by voluntary Community Health Promoters (vCHPs) and model
families. Their role is to support the delivery of the HEP to the community. The vCHPs train model
families who implement the HEP packages and serve as role models to show the benefits of the
system within their village. The Health Development Army (HDA) is a new initiative that further
expands best practices in the HEP. This links one model family household to 5 other households.

27
The most important cadres and their characteristics are presented below.
Health Extension Workers (HEWs):
High school graduate females
One year of training
2 serving 5,000 people
Provide basic curative and preventive health services in every rural community, including
delivery services
On the government payroll
Each HEW is supported by 10 vCHPs and model families
The HEW is supported by the nearest health facility. There is a structure called Primary
Health Care Unit (PHCU) that comprises one health centre and it’s surrounding five health
posts. The health centre provides technical and administrative support to the 5 health posts
under it.
Voluntary Community Health Promoters (vCHPs):
Recruited by the District Health Officer (DHO), HEWs and community members
Support the HEWs
Implement full HEP packages
Each vCHP is expected to have 30 to 50 households
40.2% of them served as TBAs/ Community Based Reproductive Health Agents (CBRHAs) or
other CBPs
Not paid
Model families are expected to:
Practice health actions for themselves
Show the benefit they gained for neighbours/relatives/peers
Communicate health actions to the community
Refer to health facility/HEW
Be role models for change
Enablers and barriers
Ethiopia has benefited from political commitment and a conducive policy environment. The health
extension programme is considered by the government of Ethiopia as a flagship programme and is
fully supported. The structure of the system is another enabling factor. The Ethiopian model of
linking HEWs with vCHPs and model families has been evaluated as a promising model in many areas
(immunization etc.). The teamwork between HEWs and vCHPs is an enabler.
The main problems can be categorized as lack of capacity at individual CBP’s level (e.g. inadequate
technical skills), institutional (e.g. poor training and supervision, inadequate M&E mechanisms and
shortage of equipment and supplies) and systems (e.g. unclear referral systems) level. Also, it could
be that HEWs have a too heavy workload. Although the HEWs were expected to spend about 75% of
their time in the communities and only 25% of their time in the health post, the reality is that they
28
are given more assignments to be implemented at the health post including basic curative services,
family planning and community case management of common childhood illnesses.
If recruitment of HEWs is not done locally (because the education level is not high enough), they
tend to stay shorter in that particular area. This indicates that it might be better to recruit HEWs
locally. HEWs get de-motivated mainly due to their career perspectives and staying for a long time in
remote kebeles (neighbourhoods). The turnover of HEWs is high. Health care at the referral site can
be a problem: sometimes referred patients find no health worker around.
There was also discussion about the role of HEWs in maternal and newborn health and especially at
the time of delivery. Out-of-facility births in Ethiopia are high (90%) along with maternal mortality.
The distribution of misoprostol to women after birth to reduce the risk of postpartum haemorrhage
is part of the work package of HEWs, but they are not always at the place of birth timely enough for
the misoprostol to make an impact. This has stimulated a pilot study where women are given
misoprostol to take after delivery (at home) and don’t have to wait for the HEW.
Knowledge gaps and research needs
More understanding of barriers to institutional delivery (which is still very low) is needed, since this
is the target area for improvement by the government.
3.5 Ghana
Current situation
In Ghana, there different types of CBPs:
TBAs
Community-based Agents (CBAs) (mother support groups/ mothers’ clubs, distributers)
Health Aids
Health Extension Workers
There are supervised by other (paid and skilled) community level providers: midwives, nurses,
Community Health Nurses (CHNs) and Community Health Officers (CHOs, they got a basic training
for nursing but are not full nurses).
The roles and tasks of CBPs are:
Health promotion activities
Mobilizing communities for health activities
Growth promotion (weighing, counselling and referral)
Assisting with National Immunization Days (NIDs)
Accompanying referrals to the health facility
Breastfeeding mother support
Management of common ailments
Vital events registration
Surveillance

29
CBPs are selected through community processes and are trained according to standard modules by
the Ghana Health Service (GHS) or by NGOs. The duration of training depends on the activities they
are involved in. The average duration is 5 days for most programmes, with a range of 1 day to 10
days. Refresher trainings are available. CBPs tend to perform multiple functions and are likely to
undergo a series of trainings with a total duration of over 3 weeks depending on their functions.
They do not receive a salary, but they are given incentives like t-shirts, bicycles, certificates and
monthly/ quarterly meetings. Most of them are female and they are selected by communities based
on criteria such as residence within the community and possession of immovable property such as a
farm or house. They answer to community leaders like chiefs and other opinion leaders who assist
with planning for health activities and providing a venue for CBPs to operate from. They are
supervised technically by health workers starting from Community Health Officers who are resident
in the community to staff at the sub-district (health centres) to the district level. They work together
with health workers when they conduct outreaches. Their logistics are supplied through the health
facilities closest to them.
Enablers and barriers
Community acceptance of CBPs is a major enabler. CBPs are accountable to the community that
selected them. Technically and programmatically they are accountable to the health service or the
health organisation that recruited them. Technical supervision is another enabler: maintaining
contacts with health workers on a regular basis gives CBPs credibility in the community. After a
structured initial training, refresher courses and updates of knowledge and skills are important, even
as incentives to improve motivation. According to the country team, recognition by health
professional is also very important and CBPs should be linked to a health facility. Reporting of health
data is done from the community level to the district; even data from trained TBAs are included.
Barriers could be interrupted supply of commodities for service delivery. There is a high attrition rate
of both skilled and trained community health workers. This is partly due to motivation issues and
inadequate supervision.
There is inequity in coverage of health insurance and the insurance doesn’t cover community based
services and FP. The main areas of the country that are covered by health insurance are rural.
However, the poor (whether urban, rural, or indigenous) are not covered. All deliveries are free in
principle, but to access that care people have to register. People don’t register because of the
registration fee. Some are given a stipend and made to register for care before they can use the
stipend.
The link between community and facility services is not strong enough to deal with all referrals. It is
seen to be time to strengthen Emergency Obstetric and Neonatal Care (EmONC) facilities to address
MDG5; therefore an MDG5 Acceleration Framework has been developed. This should help to
increase capacity to deal with referrals from the community.
Knowledge gaps and research needs
One of the big issues to address is the increasing number of urban poor. There are a few realities
that influence this:
Often urban populations have access to health facilities, while the rural populations have to
make do with volunteers.

30
Urban areas generally do not consist of well-organised communities that oversee and
influence the services they receive.
Special approaches are needed to serve the urban deprived.
The key research questions that emerged are:
How do you use community based workers in deprived urban communities?
Is volunteerism in community service delivery sustainable?
3.6 India
Current situation
In India, there is a range of CBPs:
Auxiliary nurse midwife (working in communities but not CBPs by definition).
Accredited Social Health Activist (ASHA), a voluntary position for women who form the
foundations of the health services in India. The ASHA is acting as the interface between the
community and the public health system in the country. Each village has an ASHA to provide
health services, particularly for the mother and child, to the community. ASHAs receive 23
days of training in 5 different modules. Government health officials are the resource persons
and the logistics are arranged by NGOs. The entry level for ASHA is 8th standard. However in
many states the entry level has reduced up to 5th standard. ASHAs also are given refresher
training.
TBAs (now officially out of the system, and replaced by ASHAs).
Anganwadi workers. In 1975, the Government of India initiated the Integrated Child
Development Service (ICDS) scheme which operates at the state level to address the health
issues of small children all over the country. It is one of the largest child care programmes in
the world aiming at child health, hunger, malnutrition and related issues. Under the ICDS
scheme, one trained Anganwadi worker is allotted to a population of 1,000, to bridge the
gap between the person and organised healthcare, and to focus on the health and
educational needs of children aged 0-6 years.
The ASHA acts as the interface between the community and the public health system. They play a
central role in achieving national health and population policy goals. They are not civil servants, but
community based volunteers, receiving performance based incentives. Their main tasks are health
promotion, reporting, medicine distribution and accompanying women to the facility for birth (they
are not supposed to conduct deliveries). The drugs provided in the ASHA kit include: disposable
delivery kit for clean deliveries at home, Iron Folic Acid, Punarvadu Mandur (preparation of iron),
oral rehydration salt packets, paracetamol, dicyclomine, povidine ointment tube, thermometers,
cotton absorbent roll, bandages, chloroquine, condoms, and oral pills.
The ASHA is considered to be the daughter-in-law of the village and is selected by the community
after which this selection is endorsed by the health administration. They are not employees of the
health system. However, they receive payment in the form of incentives for services rendered to the
community following the norms of the National Rural Health Mission.

31
In addition to the above mentioned CBPs, there are community level institutions:
Village Health & Sanitation Committees (VHSCs)
Self-Help Groups
Community Based Organisations (CBOs)
Enablers and barriers
The case study of India involved a project on community based distribution of non-clinical
contraceptives by ASHAs, supported by their spouses in Odisha State. The Community Based
Distribution (CBD) programme emphasizes on ensuring access to information and services pertaining
to contraceptives to promote health of mother and child through spacing method and limiting the
number of births. Supported by UNFPA, this project has had positive results. It has been successful in
promoting the spirit of volunteerism among the ASHAs and their spouses in the district. Sociocultural
barriers relating to contraceptives have become flexible. Availability, accessibility and acceptance of
nonclinical contraceptives have increased. This project has bridged the gap between user and service
provider.
An independent study showed that the ASHAs that were involved in the project increased their
knowledge of family planning. Enabling factors were:
Integration on supply and demand side (to ensure that the health system is more
responsive)
Continuous in-service education and training
Social mobilization among the eligible couples, especially the young and newly married
couples, to address the myths and misconception about contraception and family planning
Strengthening community institutions and more community involvement
Complimentary role of spouse for workload reduction, motivation and retention (proven by
a study)
Barriers that were observed were the incentives: Some people expect salaries. Sometimes, there
was a mismatch between expectations of the community or management on ASHAs and their
capabilities. Furthermore, despite in-service education, the attitudes of ASHAs were shown to need
improvement.
Knowledge gaps and research needs
The research questions identified were:
How to expand the scope of work of ASHA nationally (family planning)?
What is the optimal work package for ASHAs?
What is the community perception on quality of care?
3.7 Malawi
Current situation
There are two main categories of community health workers In Malawi: 1) Health Surveillance
Assistants (HSAs) and 2) community volunteers, including TBAs. The Malawi government has a target
of one HSA for every 1,000 population. HSAs receive 8-10 weeks initial training. The refresher course

32
that is part of their programme is often not given because of lack of resources. HSAs are salaried
and employed by the Ministry of Health and there are currently 11,000 of them. This cadre
constitutes a formal link between the communities and the health facilities and supervises all
community-based health initiatives and volunteers within their communities (such as community
home-based care volunteers, health promoters, Village Health Committees (VHCs) and expert
patients among others). Many programmes are turning to the HSA in an effort to improve access,
coverage and basic health outcomes. In terms of MNH, the official roles of HSAs include promotion,
growth monitoring, Information, Education and Communication (IEC), vaccinations, and assisting in
referrals. In addition, they carry out community data collection, treatment of minor ailments and
report on disease outbreaks and sanitation and disease surveillance. HSAs are generally supervised
by Environmental Health Officers and Assistants who work at district level. HSAs are well embedded
in the community and linked to the health system. This is the only Ministry of Health cadre at the
community level. Each HSA is responsible for two villages or more, in this way they are in close
contact with the community. Every health related activity in the village goes through an HSA,
likewise every health related issue (including outbreaks) from the village is reported to a health
facility by an HSA. In each village there is a Village Development Committee (VDC) and a VHC that
reports to the HSA. The HSA is a member of the Area Executive Committee (AEC). According to
policy, TBAs are not supposed to provide delivery services. There are also community based
distribution agents who sometimes provide Family Planning supplies.
Enablers and barriers
The country case study of Malawi presented a Safe Motherhood project in Mangochi district. Within
this project, TBAs were trained to refer patients to the health facility. They were rewarded for best
practice. Community maternal death audits were introduced and community empowerment
through local IEC groups who disseminate safe motherhood information was established. There
were bicycle ambulances introduced to address the second delay (the delay in reaching the facility).
Voluntary Safe Motherhood Field Assistants (who act as HSA but are focused on MNH) were
introduced and Community Based Distribution Agents (CBDAs) trained by Save the Children were
also incorporated in the district programme. The project led to increased referrals, better
community empowerment, more deliveries by skilled personnel and the number of maternal deaths
went down. The enables that were identified are the following:
Good health and Sexual and Reproductive Health and Right Policies.
Decentralized system with community structures in place.
Recognition of HSAs, CBDAs, volunteers.
Up grading, locum (payments for overwork), transport and housing for staff in rural areas.
Award system, training, exchange visits-learning by living approach.
The community selected the TBAs for training – the criteria for selection were: living locally,
years of experience, and community trust in their discretion. They were seen as trusted and
“disciplined women” who would not ask for high incentives. The training criteria were also
decided at community level.
Active involvement of community leaders.
Barriers are:
Persistent shortage of skilled health care professionals (up to 50% vacant establishment
posts).

33
Inequitable deployment of health personnel, which favours urban areas.
Communication and transport systems remain inadequately developed.
Shortage of resources in the rural facilities.
Health care (perceived) as being too expensive for the rural poor.
Poor access /availability of EmONC services.
TBA ban from providing deliveries. TBAs were recently banned at policy level from assisting
deliveries, but at project level they were first trained to conduct deliveries in a limited scope
(deliver only gr 2-4 with no past history of complications), and to refer to a facility timely
facilitated with donated bicycle ambulances. Later, in line with the ban, they were trained as
sign posts for maternal health services (referral points in the village). The ban has led to a
shift in focus to referral.
Geographical barriers.
Low illiteracy levels/risky cultural practices.
Too many responsibilities for CBPs, they are overburdened.
Not many bottom up approaches.
Resources are still an issue. Only three quarters of the HSAs nationally are salary-supported
by the Ministry of Health. Some organisations, like Save the Children, and the WHO have
employed them on a project basis. This can be a problem for them to be taken over. The
VHCs are volunteers. The incentives for them are award systems and recognition of their
services, plus involving them when there is a project (at that time they get things like t-
shirts, umbrellas or allowance).
Knowledge gaps and research needs
In Malawi there is a need to focus on the human resource management aspects (supervision,
training, motivation) that contribute to successful CBP programmes. In addition, research should be
done on task-shifting structures in place and the extent to which multiple responsibilities put
pressure on HSAs that prevents them from delivering equitable, effective and efficient services and
adequate referral of patients. So far research projects and NGOs have been putting in extra human
resources, but it is not clear whether addition of external people (safe motherhood assistants)
influences the success of the project vis-à-vis the normal services available in an area. What is
needed to strengthen the facility level? How will demand creation by better referral from CBPs
influence the whole health system?
Many projects are pilots, there is a need to document processes and develop a standard model for
rural areas and scaling up of pilot projects. Most of the time, research is difficult to conduct if a
project only lasts for 1 or 2 years. This problem exists in more countries.
3.8 Nepal
Current situation
In Nepal, there is a system with different types of CBPs:
Maternal and Child Health Workers (MCHWs): this cadre was introduced nearly 20 years
back by the National Health Policy 1991. It took nearly 4 years to bring on board the 3,134
MCHWs. This cadre’s main responsibility is maternal and child health. One of the selection

34
criteria includes that the candidate should be considered as the daughter-in-law of the
community to ensure sustainability of the programme. They get a salary from the Ministry of
Health. The roles of MCHWs are:
o Conduct ANC
o Conduct delivery
o Conduct PNC
o Care of newborn
o Supply FP commodities: pills, condoms and injectable (Depo)
o BCC
o Conduct outreach clinics in the community
o Management of diarrhoea and pneumonia in the community under community
based IMCI
o Supervision of FCHVs
o Referral Services
Village Health Workers (VHWs). This cadre was introduced 32 years ago and there are 4,015
VHWs currently. They receive a salary from the Ministry of Health. Their roles and
responsibilities include:
o Immunization services, including Tetanus Toxoid (TT) for pregnant women
o Management of Newborn Infections
o Supervision of FCHVs (see below)
Female Community Health Volunteers (FCHVs): There are currently 48,549 FCHVs present in
Nepal. They are volunteers and one FCHV serves 500 people at village level. They are
involved in maternal and neonatal health (FP programmes, vitamin A and iron tablet
distribution, awareness raising and provision of essential neonatal care during birth and
postnatal) and child health (vitamin A distribution and de-worming, community based
management of pneumonia and diarrhoea and awareness ion immunization programmes).
Their activities include:
o Demand generation in the community for Maternal, Newborn and Child Health
(MNCH) services
o Counselling pregnant women and family on birth preparedness (identifying and
timely referral for danger signs during pregnancy, delivery and postnatal, promotion
of institutional delivery, ensuring availability of transport money)
o Community based management of pneumonia & diarrhoea
o Management of newborn infections in the community under the community based
Newborn Care Programme
o Behaviour Change and Communication activities
o Distribution of FP commodities (condom and pills)
o During NIDs: administration of Polio drops
o Referral services
o Coordination of mother groups
MCHWs and VHWs receive 6 months of training and are supervised by Auxiliary Nurse Midwives
(ANMs) at the health facility level. The government stopped recognizing trained TBAs in 2004. At the
moment, the FCHVs are extensively counselling and raising awareness in the community for
institutional delivery. FCHVs receive an 18 days basic training which is carried out in two phases: 9
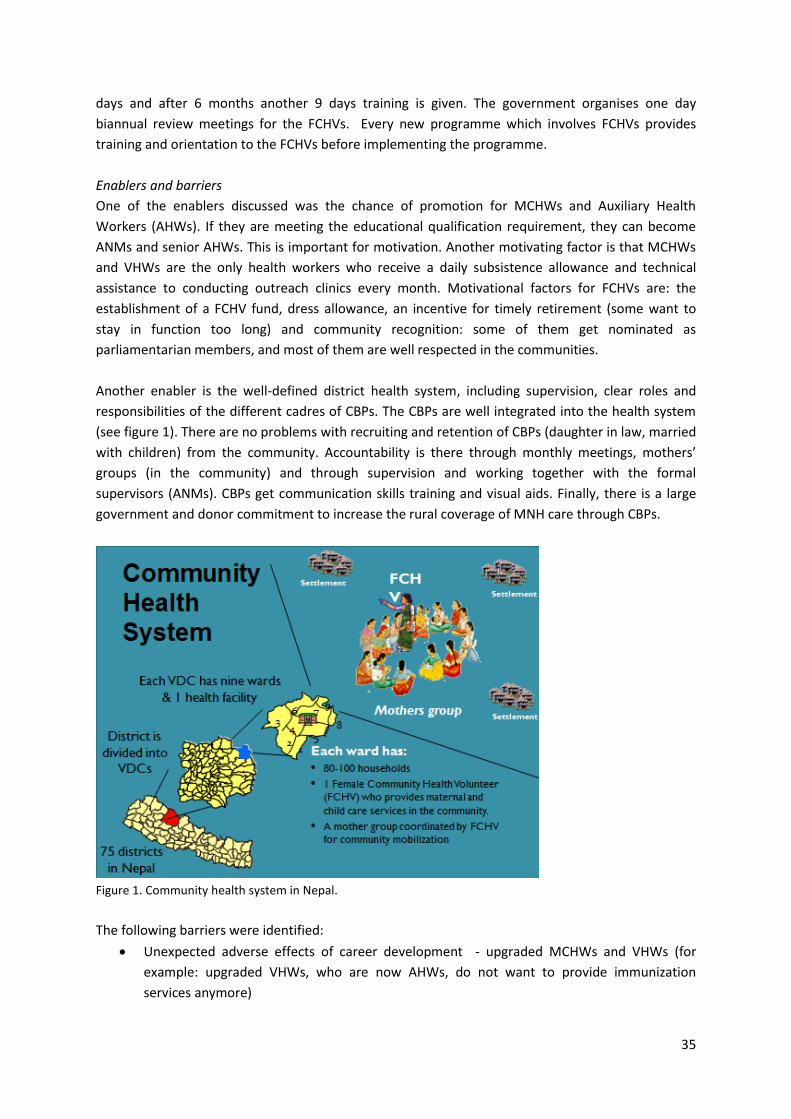
35
days and after 6 months another 9 days training is given. The government organises one day
biannual review meetings for the FCHVs. Every new programme which involves FCHVs provides
training and orientation to the FCHVs before implementing the programme.
Enablers and barriers
One of the enablers discussed was the chance of promotion for MCHWs and Auxiliary Health
Workers (AHWs). If they are meeting the educational qualification requirement, they can become
ANMs and senior AHWs. This is important for motivation. Another motivating factor is that MCHWs
and VHWs are the only health workers who receive a daily subsistence allowance and technical
assistance to conducting outreach clinics every month. Motivational factors for FCHVs are: the
establishment of a FCHV fund, dress allowance, an incentive for timely retirement (some want to
stay in function too long) and community recognition: some of them get nominated as
parliamentarian members, and most of them are well respected in the communities.
Another enabler is the well-defined district health system, including supervision, clear roles and
responsibilities of the different cadres of CBPs. The CBPs are well integrated into the health system
(see figure 1). There are no problems with recruiting and retention of CBPs (daughter in law, married
with children) from the community. Accountability is there through monthly meetings, mothers’
groups (in the community) and through supervision and working together with the formal
supervisors (ANMs). CBPs get communication skills training and visual aids. Finally, there is a large
government and donor commitment to increase the rural coverage of MNH care through CBPs.
Figure 1. Community health system in Nepal.
The following barriers were identified:
Unexpected adverse effects of career development - upgraded MCHWs and VHWs (for
example: upgraded VHWs, who are now AHWs, do not want to provide immunization
services anymore)
36
FCHVs still conducting home deliveries (40% “recycled” TBAs)
Health facility birth rates have increased but at still only at 36%
Problem of increasing demand without increasing supply
Maternal death review data not filtering down to community
Overload - FCHVs are utilized by many programmes. This might hamper the overall spirit of
volunteerism in the future
Political manipulation of FCHVs – vote banks
Increased service utilization rates not a measure of quality
Knowledge gaps and research needs
Nepal will be a good country to include in impact studies on the implementation of CBPs, as there
are different cadres that seem to be well integrated in the health system. More research should be
conducted into the above mentioned enablers and barriers and their effect on CBP programme
implementation and improvement of MNH.
3.9 Rwanda
Current situation
In Rwanda, each village has 3 CHWs: 2 dealing with child health and Family Planning (FP) and one
dealing with MNH: the Animatrice de Santé Maternelle (ASM). They are all supervised by the CHW
coordinator (at the cell level) and the community supervisor (at the health centre level, where there
is basic EmONC services).
The ASM:
Identifies and registers all women of reproductive age in the community (and encourages
FP)
Identifies pregnant women in the community and encourages ANC attendance and facility
based delivery
Promotes health behaviours during pregnancy and the postnatal period (nutrition, use of
ITNS, early breastfeeding, use of FP, information about PPH etc.)
Accompanies women in labour to the health facility
Provides misoprostol to women who deliver unexpectedly at home
Makes early home visits and identifies women and newborns with danger signs and refers to
health facility for care
Encourages early postnatal facility checks for both newborn and the mother
The requirements for becoming an ASM are: female, primary education (or higher), literacy, age
between 25-30, living in the village where they work, availability to conduct home visits and
respected by the community. They are selected by the community.
ASMs receive training to increase their knowledge and skills. The training lasts for 6 days and there is
a 3 day refresher planned after 6 months. ASMs are organised in cooperatives to ensure income
generation (they are not paid) and accountability of expected results. They are part of a PBF system,
which is good for motivation. They also have an ASM kit, including registers, counselling and
screening cards, demonstration cloths for dry wrap and Kangaroo Mother Care (KMC), a

37
thermometer to identify hypothermia, a timer to identify newborns with breathing problems, a scale
to identify low birth weight, a cell phone, a solar torch and soap for hand washing.
Monitoring and evaluation of ASMs takes place through monthly reports submitted to health centre
staff. Indicators have been defined and linked to the Health Management Information System
(HMIS). The supervision by the community health coordinator is also monthly, and in addition, there
are monthly meetings at health centre level. Innovations are e-ubuzima (e-health) and on-going
training via radio.
ASMs are well integrated to their community as they are part of them. They are trusted by the
community and play a huge role in linking the community to the health system and vice versa. They
meet monthly with health providers and activity reports are shared with them. In return they receive
support and supervision.
Enablers and barriers
A large enabling factor is the strong political commitment (16% of the national budget expenditure is
for health). There is an innovative financing system (PBF) with 95% coverage. This PBF system
appears to work as an incentive mechanism for ASMs. Furthermore, there is a clear and
comprehensive policy framework and good health sector coordination.
Dedicated community coordinators and community supervisors have been essential to the planning
and training and support of ASMs (at the local level). At central level, a Community Health Desk and
Committee played an important role in coordination. Equipment and supply kits have proven to be
essential to enable ASMs to conduct home visits. The high mobile phone coverage has made a rapid
SMS alert system possible.
The selection by the community and the fact that ASMs are supposed to live in the community
where they serve makes ASMs well respected in their community.
There are also challenges: Community MNH activities are mainly financed by development partners
and not yet incorporated into routine district plans. There are no data on the costs of
implementation, and this is much needed for further expansion of the programme. Routine
supervision of ASMs is difficult to maintain. Follow-up after trainings (refresher courses) is needed
but not realized because of financial constraints.
Knowledge gaps and research needs
A cost analysis of the whole community MNH programme is needed, in order to quantify total
resources required for implementation – at all levels. Future programme activities should have
costing mechanisms built in at the start to ensure that costing information is collected and analysed.
In addition, more research should be done into the mechanisms to maintaining community MNH
performance and motivation.
38
3.10 Sierra Leone
Current situation
In Sierra Leone, the health facilities closest to the community are the Maternal and Child Health
Posts (MCHPs) and the Community Health Posts (CHPs). Most of these are staffed by MCH Aides,
who are supported by CBPs, such as TBAs and community volunteers. It is estimated that there are
24,000 CHWs in the country. The exact number is not known as they as most of them are involved in
specific NGO programmes. They do not receive salaries, but get incentives. The government has
decided to support this cadre and has starting action to coordinate the implementation of CHWs in
Sierra Leone. The proposed package of tasks for CHWs includes:
Promotion of healthier life-styles and environmental control
Promotion of appropriate use of health services
Promotion of health services like ANC, vaccination and FP
Provision of more accessible preventive services in the community
Being an advocate for the community linking community and the formal health system.
At this moment, the CHW – population ratio, the training, workload and incentive package is all
under discussion. The current training package is 10 weeks and covers MNH, childhood diseases,
acute malnutrition and total sanitation.
The largest group of community based providers currently in Sierra Leone are TBAs. The Free Health
Care Initiative (FHCI) made deliveries in health facilities free for all pregnant women. As a result,
TBAs have found themselves without a livelihood. Their role in the system is disputed and how they
are integrated into the health system depends largely on the District health Management Team
(DHMT) and/or NGOs in their area. The current Government policy is to concentrate on the changing
role of TBAs; not conducting deliveries but more involved in health education and referral and
monitoring the use of ITNs by pregnant women and under 5 children.
Enablers and barriers
The government is in the process of finalizing a Community Health Worker policy. The guiding
principles for this include community ownership, equity and access, support of the CHW by
communities and the health system, multi-sectoral partnerships and coordination. Much can be
learned from other countries. The participation and engagement of all partners (national and local
governments, NGOs and UN agencies) will contribute to this.
The current challenge in Sierra Leone is providing maternity services in remote areas where TBAs are
the only health providers available. Currently TBAs still widely conduct out-of facility deliveries (50%
of all births take place out-of-facility). A key question is how to change the current TBA role.
Furthermore, the financial sustainability of the CHW programme has to be looked at, as
remuneration for volunteers is still a debate in Sierra Leone.
Knowledge gaps and research needs
Research is needed to make recommendation on how the role of TBAs can be changed in Sierra
Leone. Furthermore, much knowledge and evidence is needed on training, incentive packages and
task packages for CHWs before CHWs are scaled up.

39
4. Discussion, conclusions and next steps
The first section of this chapter covers common issues that came out of the country case studies and
the second section lists innovative practices that were shared during the meeting. The following two
sections cover the outcomes of the two group discussions that were held: 1) on barriers and
enablers to the implementation of CBP programmes and 2) on knowledge/ research gaps and key
policy challenges. Finally, a summary of the conclusions and future actions is given in the last two
sections.
4.1 Discussion of country case studies
CBPs form a link between the formal health system and the community. Examples from all countries
show that CBPs play an important role in improving accessibility of care, especially in settings with a
shortage or lack of human resources for health.
The various CBP programmes discussed during the Technical Consultation showed to be in
accordance with policies and guidelines developed by the Ministry of Health.
In many country case studies, the success of the CBP programme depended on the degree of
involvement of different stakeholders and their links with each other. The role of the community in
relation to selection, ownership, action and support of CBPs is also crucial. The health system is
indispensable and it is essential that it functions adequately and has the human resources and
facilities to deal with referrals. The role of national and local government in providing, managing and
supporting the system is crucial. CBP programmes should not be set up in isolation.
The way in which CBPs are embedded in the community is reported as very important in all country
case studies. In Ethiopia, there are model families, supervised by the CBPs. In Nepal, there is good
integration in the community via mothers’ groups. Such structures improve the credibility of the CBP
and reduce their workload. Recruitment by the community of CBPs that come from, and stay in, the
community is reported as important for the sustainability of the programme.
In most countries, CBPs had a link with the community and also with the formal health system. In
many countries, NGOs play an important role in the training and provision of incentives for CBPs.
There are differences in the tasks performed by the CBPs: some are trained for specific tasks (vertical
programmes), but most CBP training programmes entail broad packages of tasks that include health
promotion, prevention, distribution and in some cases, actual hands on care.
There is a wide diversity in the background and training that CBPs receive between countries and
between programmes within countries. Some CBPs receive between 8-10 weeks training and others,
such as Health Extension Workers in Ethiopia, receive a full year’s training. The more training and
tasks CBPs fulfil, the more they come to resemble a cadre of auxiliary staff. The length of training
and variety of tasks to perform as well as the issue of salaries also influences the notion of
voluntarism versus professionalism.

40
This issue of voluntarism versus professionalism was raised at various points during the case studies
and in subsequent plenary discussions. There is considerable variation between countries on the
remuneration of CBPs. In some countries, they are volunteers who receive incentives in kind, or are
rewarded by the increased respect and status they acquire in the community. In other countries
CBPs are more of a “cadre”, and sometimes they are on the pay role of the Ministry of Health. Some
CBPs have been given more and more tasks, partly as a result of task shifting. In some cases the CBPs
seem to becoming gradually professionalized. Questions on remuneration are often raised and
different countries have adopted varied ways of dealing with it reflecting not only available
resources but also cultural differences. Some CBPs want a fixed salary as acknowledgment of their
efforts and status; but in Nepal for example, FCHVs do not want a fixed salary, because they think
they will lose credibility within their community. They want to keep their voluntary status and a
degree of independence from the central government. These differences in attitude will be one of
the factors that determine how best CBPs can be organised and supervised but it seems clear that
some degree of professionalization is necessary to regulate the way in which CBPs work and to
ensure that they are protected by an appropriate legal framework.
4.2 Examples of innovation
During the consultation, a number of innovative practices were identified. Some have shown
promise of impact and others have not been studied but they can be adapted for specific country
use and be added to Community Based Provider programmes where it is deemed appropriate. A
short summary of these innovations follows:
The ASM in Rwanda is one of the few CBPs with a specific mandate for maternal and
newborn health as part of a community team of CBPs.
A small pilot study in India that has included the recruitment of the spouse of the ASHA
suggests that motivation of the ASHA is improved because she has more support from home
and is able to hand over some of the more difficult work (dealing with male community
members) to her husband.
The so-called ‘recycling’ of TBAs in Nepal to FCHVs may provide an example of how to
change TBA’s role and practices while making use of their strong ties with communities once
they transition themselves to stop conducting out of facility births.
Community data collection spearheaded by CBPs as in Afghanistan and Ethiopia could
contribute greatly to more valid data and better disaggregated data sets that would be
extremely helpful in understanding differences and inequities.
There is a global increase of interest in CBP distribution of misoprostol in order to help
prevent postpartum haemorrhage and some of the country teams (Ethiopia, Nepal, Rwanda)
spoke to this issue sharing their experiences, especially as country policies often do not
match this practice.
4.3 Barriers and enablers to implementation of CBP programmes
During the discussions enablers and barriers to the implementation of CBP programmes were
discussed. It was noted that the barriers are often the same as the absence of enablers. For instance:
a consistent policy framework was identified as an enabler. The absence of a consistent policy

41
framework was identified as a barrier. For this reason enablers and barriers were discussed together
as critical factors in the plenary sessions and the country workshops. An overview is given below of
all factors. For the purposes of the report they have been categorized according to the WHO Health
Systems building blocks framework.
Leadership/ governance
First of all, policy is an enabling factor or barrier. CBPs need to be embedded in the formal health
system, with good regulation on referral and supervision and clarity on roles and tasks of CBPs.
Sometimes, discontinuity of policies poses a problem (new or adjusted policies after election can
cause confusion regarding the direction of health programmes). Also, policies need to be consistent:
within the same country, different policies can conflict with each other. Policy and practice change
can have consequences at multiple levels which may in turn be enablers, e.g. the free health care
initiative in Sierra Leone made maternal health care better accessible to women.
Secondly, stakeholder involvement is very important. The Ministry of Health, NGOs, bilateral
organisations, the private sector (e.g. in Bangladesh) and most importantly the community should be
involved and work together. Community involvement, acceptance and ownership are very
important, as the community is the target group of the CBP.
Health information systems
Monitoring and evaluation of CBP programmes should be fed back to the implementation level.
Social mapping can be an enabling factor for effective CBP programmes, as they are always part of
other organisations and systems that are in place in a certain area. Community maternal death
audits are an example of a specific community based activity (involving CBPs, community and health
professionals) that seem to be effective in evaluation and improving maternal health services. The
upcoming use of mobile technology can also improve monitoring and evaluation, enabling the good
implementation of CBP programmes.
Financing
On financing, the sustainability of CBP programmes was discussed, as well as donor influence.
Sometimes, CBP programmes are established dependent on temporary incentives and this creates
risks in terms of sustainability. In countries where health insurance is available, many community
based services are not included in the scheme and this can be an important barrier for CBP
programmes.
Service delivery
Regarding service delivery, it is most important that CBP programmes are not implemented in
isolation but are embedded in the health system with collaboration between CBPs and health
workers. CBPs play a major role in stimulation and encouraging the community to utilize facility
health services. It is essential that this increase in demand can be met and more specifically that
health facilities are able to absorb the increase in clients by ensuring sufficient numbers of facility
staff and having enough supplies and medicines. Service quality at the referral point can also be seen
as an enabling environment (for CBP programmes). Referral systems themselves should be in place:

42
from the community level to the first level health facility, facilitated by the CBP, and, if needed, from
a first level health facility to a higher level facility.
The supervision of CBPs needs to be clearly described and regular. CBPs need technical supervision
but they also need support. Some aspects of the supervision need to be done by health
professionals, others can be provided by peers.
Health workforce
Many of the country case studies showed that recruitment or selection by the community is an
enabling factor. Clear criteria for the profile of a CBP can be enablers (for example: gender, literacy
level, having no more than 2 children as a role model, model families).
Sufficient and appropriate training is another enabling factor. There should be a national level
standard curriculum for pre-service training. There should be a system for in-service/ on-going
training.
Motivation of CBPs is a factor that influences the implementation of programmes. Motivation is
influenced by a number of factors including remuneration and incentives, teamwork, status and
recognition, and community and family support. Remuneration in the form of salary, incentives,
performance based financing can be effective mechanisms. Motivation packages include housing,
transport money, awards. Recognition by health professionals seems to be a very important factor
affecting CBP’s motivation. There is a risk that CBPs become overburdened with the large work
packages they are expected to carry out and become de-motivated when more tasks are added to
their workload. Some innovative new approaches were highlighted; for instance in India spouses of
the CBPs have been actively involved and this has increased the motivation and support for the work
of the CBP.
For many CBPs, career opportunities are limited, which may lead to attrition. In many countries,
CBPs have a big work load and find this a burden and in some of the cases discussed it was reported
that the major responsibilities they carry are not reflected in the status that they are accorded.
Enabling environment
Often, policies are present, but the implementation of the policies is not sufficient. Political
commitment is very important. In addition, sufficient supplies, drugs and good working conditions
(including safety in the field) form the “enabling environment” for a CBP.
4.4 Knowledge gaps and policy challenges
Knowledge gaps
During the meeting, attention was drawn to the fact that there is not a common or accepted
terminology in use to describe this area of work. Whilst uniformity is not necessarily desirable it
would be very helpful if there is some standardization of terms and definitions so that comparisons
across systems and between countries are more feasible. Currently it is a challenge to find a
common language to discuss research needs and knowledge gaps.

43
The type of task package for CBPs needs to be defined, based on research. Which tasks could be
conducted by CBPs against which skills base? What is the minimum package and what is the
maximum package? What is the generalist and what can be a specific package? How does workload
relate to coverage (i.e. less tasks, more coverage). And what specific tasks are appropriate to be a
task for a CBP, based on evidence (task shifting guidelines WHO)? Regarding certain tasks, where
does service provision by the CBP stop and when should be referred? For which tasks do CBPs need
extra training? There is also research needed to find out what supervision is appropriate. Who, how
and where to supervise in a way that appropriately captures the range of tasks the CBP is
conducting?
The training of CBPs is also a research gap. The focus (skills base and competency) and length of the
training varies from country to country, and research should be done to see what kind of training
can contribute best to effective CBP programmes in a specific setting. Research should be done on
what minimum education and literacy requirements should be met before entering a training to
become CBP.
There is a debate on volunteerism against professionalizing. If you give CBPs training, is this
influencing to distract CBPs from their social embedding in communities? Is volunteerism
sustainable?
For motivation of CBPs, research should be conducted on what incentives are appropriate. This will
always depend on the setting. There should be research done to see if there is any resistance to task
shifting.
Another field of research is experiences of CBPs and communities themselves. What are their
perceptions on how CBP programmes can be effective? Furthermore, models that give a voice to
CBPs within the health systems should be identified.
A large focus for research could concentrate on the question how to simultaneously strengthen
health systems (quality of care) and build CBP programmes (CBPs are only as good as the system
they refer to). What is the functionality of the referral system of CBPs? How do we ensure that there
is no duplication and what are the barriers to service utilization? What factors in the enabling
environment (see above) should be addressed to improve quality of care and what is the influence
of PBF on the quality of care?
In some countries, research could focus on the mix of private and public services and providers that
work with CBPs.
We should also know more about geographical factors. How do we use CBPs in urban areas? What
works well in very remote, rural areas? And where do we prioritize the use of CBPs?
Community participation and the link to the health system is another area of research. How to
better encourage community participation? What are criteria for selecting CBPs and how does
community selection affect community ownership? Do we know if the expectations from community

44
and health management and CBPs match? How do we define quality from a client perspective?
What is the role and potential of community based audits and social mapping in linking community
perspectives/ equity concerns to health systems? How do we feedback on outcomes of community
based monitoring mechanisms to influence policy? And the other way around, do policy priorities
reflect community needs and realities?
There is a need for cost effectiveness analyses of CBP programmes. What is the contribution of CBPs
towards progress on certain health indicators, what is their impact? What is the contribution of the
community to their own health, as promoted by the CBP? How do we measure this? In general, we
need more research on effectiveness, equity and sustainability of CBP programmes. Given the
importance of context, how can we best share and learn from each other across multiple contexts?
Policy challenges
Policy challenges are already partly discussed in the above section on enablers and barriers. In many
cases policies are in place, but implementation is incomplete or lacking. It should be clear who is
responsible for the monitoring of the operationalization and who is accountable for the
operationalization itself.
All aspects that can be enablers and barriers should preferably be addressed in the existing and new
policies on CBP programmes. It should be clear how activities with CBPs are to be regulated and
supported within a legal framework (also to protect CBPs). There needs to be attention for an
appropriate task package, training and continuously support and embedding in the health system.
CBP programmes should be linked to programmes that improve the health system as a whole.
Regarding MNH, not only CBPs, also policies on nurses an midwives should be improved and linked
to those making use of CBPs.
4.5 Summary of conclusions
The main enablers and barriers to the implementation of community based provider programmes
identified were:
Policies: comprehensive policy framework and clarity of roles and tasks, continuity,
consistency and coordination in policy development and implementation, decentralization in
existing community structure;
Multi-stakeholder coordination and involvement: strong community ownership and
involvement, government coordination, NGO, bilateral and private sector involvement and
alignment and provider consultation;
Training and education: standardization of curriculum, fit for purpose, pre-service training
with in-service support and continuous education;
Recruitment and retention: community involvement in selection, clear criteria for
community based provider’s profile, incentives and motivation packages, recognition (i.e.
awards), career opportunities;
Enabling environment: political commitment, sufficient supplies and adequate working
conditions (including workload), teamwork and supervision, quality assurance mechanisms;
Community data collection and analysis to strengthen services.

45
The following knowledge gaps were identified for further research:
Impact of community based provider programmes in terms of equity of access and quality
and health outcomes and sustainability and how to assess this;
Packages, priorities and appropriate training for community based providers - which tasks
are needed and what is the most effective training and follow up strategy for a particular
task and type of community based provider?
Four main policy issues or constraints were identified:
How is policy operationalized and who is accountable?
How can activities of community based providers be regulated and supported within a legal
or professional framework?
In terms of human resources for health, how can an appropriate package of tasks for
community based providers be designed and applied and how can a pipeline for production
of health workers be developed to ensure coverage and professionalization and quality of
the workforce?
How can countries continue to invest in skilled birth attendants, such as midwives,
production and management and creating at the same time a sufficient network of
community based providers?
Five questions were formulated that could improve community based provider programme
implementation:
What areas should policy cover and what is in place already?
What lessons can be learned from other programmes on longer-term sustainability and key
policy debates?
What motivation and sustained incentives are appropriate to different maturity levels and
objectives of programmes?
Which areas should be prioritised in a well-defined package to avoid multiple workloads?
What is the maximum/optimal package of services for community based providers?
4.6 Next steps
The meeting closed with the announcement of actions from the participants. The organisers
promised to share the results of this Technical Consultation with other initiatives and meetings
planned in the following months that have similar objectives. Country representatives announced
that they would inform other stakeholders in their countries and pursue the discussions on barriers
and enablers to programme implementation in the local context. The Liverpool School of Tropical
Medicine in collaboration with the Royal Tropical Institute will integrate the results from this
consultation in their ‘Reach Out’ programme starting this year in 6 countries. DFID is committed to
supporting coordination and follow up. UNFPA and other H4+ agencies and partners will collaborate
to develop a training manual for community health workers on reproductive, maternal and newborn
health. WHO will use the discussions from the Amsterdam meeting as input for the further
development of the task shifting guidelines and actions to improve postnatal care.

46
ANNEX 1 PROGRAMME Wednesday 30 May 2012
8.30 - 9.00 Registration with coffee and tea Marble Hall
9.00 - 9.20
Opening
Mauritszaal Chair Catherine Hodgkin, welcome by: KIT, Korrie de Koning and
Ministry of Foreign Affairs, Marijke Wijnroks
9.20 - 9.45 Introduction contextualizing the role of community based providers
Mauritszaal KIT, Kathy Herschderfer
9.45 - 10.45
What is known about the effectiveness and acceptability of lay health worker
programmes for maternal and child health? Mauritszaal
NOKC, Claire Glenton
10.45 -
11.15
Coffee & Tea
Marble Hall
11.15 -
11.45
Optimizing the delivery of key maternal and newborn interventions through
task-shifting Mauritszaal
WHO, Mario Merialdi
11.45 -
12.15
Outcomes of the Informal Meeting on provision of home-based care to
mother and child in the first week after birth Mauritszaal
WHO, Severin von Xylander
12.15 -
13.45
Lunch
Marble Hall
13.45-
14.30
The role of community based providers in MNH: Jhpiego's experience Mauritszaal
Blami Dao
14.30 -
15.30
First round Country Cases, see attached overview
Break out Presentations and group discussions: choice between 1. India 2. Bangladesh 3.
Afghanistan 4. Nepal
15.30 -
16.00
Coffee & Tea Down the
stairs
16.00 -
17.00
Second round Country Cases, see attached overview
Break out Presentations and group discussions: choice between 1. Ghana 2. Ethiopia 3.
Rwanda

47
17.00 -
19.00 Reception Marble Hall
Thursday 31 May 2012
8.30 Welcome with Coffee & Tea Marble Hall
8.30 - 9.30
Third round Country Cases, see attached overview
Break out Presentations and group discussions: choice between 1. Malawi 2. Sierra Leone
3. Burkina Faso
9.30 - 10.45
Plenary feedback and discussion from Country Cases
Mauritszaal
Chair: Catherine Hodgkin, Reporter Maryse Kok
10.45 - 11.15 Coffee & Tea Marble Hall
11.15 - 12.00
Plenary feedback and discussion from Country Cases
Mauritszaal
Chair: Catherine Hodgkin, Reporter Maryse Kok
12.00 - 13.30 Lunch Marble Hall
13.30 -14.45
Group discussions on conditions for implementation, knowledge gaps,
research and policy agenda, see attached overview Break out
3 groups
14.45 - 15.15 Coffee & Tea Marble Hall
15.15 -16.15 Plenary feedback and discussion
Mauritszaal Chair: Catherine Hodgkin, Reporter Maryse Kok
16.15 - 16.45
Wrap up and further joint actions
Mauritszaal
Chair and representative of Ministry of Foreign Affairs

48
ANNEX 2 PARTICIPANT LIST
Name Email address Country Organisation
1 Abdul Hamnawozada, Saleha [email protected] Afghanistan Afghan Midwife Association
2 Ahmadi, Yalda [email protected] Afghanistan Afghan Midwife Association
3 Ansari, Nasrat [email protected] Afghanistan Student
4 Bernis, Luc de [email protected] UNFPA
5 Dao, Blami [email protected] Jhpiego
6 Das, Sudarsan [email protected] India Human Development Foundation (HDF)
7 Desta, Binyam Fakadu [email protected] Ethiopia MaNHEP
8 Dickson, Kim [email protected] UNICEF
9 Glenton, Claire [email protected] NOKC
10 Grebremariam, Abebe [email protected] Ethiopia MaNHEP
11 Habib Arwal, Said [email protected] Afghanistan Ministry of Public Health
12 Herschderfer, Kathy [email protected] Royal Tropical Institute
13 Hodgkin, Catherine [email protected] Chair, consultant
14 Hoope, P. ten [email protected] ICS Integrade
15 Hossain, Altaf Bangladesh MOH&FW
16 Kamara, Zainab Sierra Leone Ministry of Health and Sanitation
17 Kamphuis, Monique [email protected] Ministry of Foreign Affairs Netherlands
18 Kargbo, SAS [email protected] Sierra Leone Ministry of Health and Sanitation
19 Kok, Maryse [email protected] Royal Tropical Institute
20 Koning, Korrie de [email protected] Royal Tropical Institute
21 Kwast, Barbara [email protected] Consultant
22 Lawson, Ruth [email protected] DFID

49
Name Email address Country Organisation
23 Leemhuis, Elly [email protected] Ministry of Foreign Affairs Netherlands
24 Matin, Ziaul [email protected] Bangladesh UNICEF
25 Mensvoort, Geertje van [email protected] CORDAID
26 Merialdi, Mario [email protected] WHO
27 Moyo, Nester [email protected] ICM
28 Mugeni, Cathy [email protected] Rwanda Mchip
29 Musa, Syed Bangladesh MOH&FW
30 Naseem, Mohammed [email protected] Afghanistan Student
31 Ofosu, Anthony [email protected] Ghana Ghana Health Service
32 Pett, Celia [email protected] Engenderhealth
33 Portela, Annie [email protected] WHO
34 Pratap K.C., Naresh Through: [email protected] Nepal Ministry of Health and Population
35 Sagoe-Moses, Isabella [email protected] Ghana Ghana Health Service
36 Salam, Abdus Bangladesh Partners in Health and Development
37 Saloucou, Lydia [email protected] Burkina Faso Initiative Privée Communautaire ( IPC)
38 Sibande, Mary Kumwanje [email protected] Malawi College of Medicine
39 Stekelenburg, Jelle [email protected] NVTG Netherlands
40 Taegtmeyer, Miriam [email protected] Liverpool School of Tropical Medicine
41 Theobald, Sally [email protected] Liverpool School of Tropical Medicine
42 Vries, Christina de [email protected] CORDAID
43 Wardt, Sophia van der [email protected] Simavi
44 Wijnroks, Marijke [email protected] Ministry of Foreign Affairs Netherlands
45 Xylander, Severin von [email protected] WHO
46 Zoungrana, Jeremie [email protected] Rwanda Mchip and Jhpiego

50
ANNEX 3 COUNTRY MATRIX
Nomenclature Specific for MNH?
Scope of practice (PR=preventive, CU=curative
Remuneration Training Embedding in system Innovations
Afghanistan CHW No PR and CU (including misoprostol)
Voluntary, no incentives
6 months Government Experience with training illiterate people, social mapping
Bangladesh CHW, many types, called: Basic Health Workers (BHWs)
No PR (mainly) and CU
Varies Range: $10-12
For government BHWs it varies between 3-12 weeks. For NGO CHWs 5-10 days.
Government and NGO
Social mapping
Burkina Faso ASC: Agent de Santé Communautaire
No PR Voluntary, 6 USD per month
1 week per technical topic
Government Social mapping
Ethiopia HEW: Health Extension Worker and vCHP: Voluntary Community Health Promoters
No PR and CU (including misoprostol)
Salary (HEW) 1 year (HEW)
Government 21 days refresher trainings for HEW, supported by model families
Ghana TBA, CBA: Community-based Agent, Health Aids, HEW
No PR Voluntary, incentives
Average 5days (1day to 2weeks)
Government and NGO
Good data reporting system, including data from TBAs

51
Nomenclature Specific for MNH?
Scope of practice (PR=preventive, CU=curative
Remuneration Training Embedding in system Innovations
India ASHA: Accredited Social Health Activist
No PR and FP distribution
Voluntary, incentives
23 days Government Experience project with providing FP
Malawi HSAs: Health Surveillance Assistants, TBAs
No Mainly PR, some CU
Salary (HSA) 10 weeks (HSA)
Government TBAs are banned but on project basis they are trained for mainly referrals and health education
Nepal MCHWs: Maternal and Child Health Workers, VHW: Village Health Workers, FCHV: Female Community Health Volunteer
Yes PR and CU (including providing misoprostol) (MCHWs conduct deliveries), FCHVs only PR
Salary, only FCHV is volunteer
6 months for MCHWs and VHWs, 18 days for FCHV
Government System of different CBPs, 2 types paid and 1 type volunteer. MCHWs specifically responsible for MNH. FCHVs: majority of the FCHVs are illiterate, huge in number nearly 50,000, selected by the community and working closely with the community
Rwanda ASM: Animatrice de Santé Maternelle
Yes PR and providing misoprostol
Incentives 6 days per technical topic
Government PBF approach
Sierra Leone TBAs and CHWs No PR Incentives 10 weeks Mainly NGOs 24,000 are there, government is starting a programme, at the moment NGOs are leading
Organizing committee:
Royal Tropical Institute, Cordaid, WHO, UNFPA, UNICEF and the University of North Carolina.
Funded by Cordaid and the Ministry of Foreign Affairs