teaching (including multiple copies for classroom use ......Yanning XUE1 Hao CHEN2 Xuesi ZENG2 Yiqun...
4
2386 East Heritage Way, Suite B, Salt Lake City, Utah 84109 USA Phone +1-877-628-7300 • Email—[email protected] www.pachyonychia.org 15 March 2005 Use of Articles in the Pachyonychia Congenita Bibliography The articles in the PC Bibliography may be restricted by copyright laws. These have been made available to you by PC Project for the exclusive use in teaching, scholar- ship or research regarding Pachyonychia Congenita. To the best of our understanding, in supplying this material to you we have followed the guidelines of Sec 107 regarding fair use of copyright materials. That section reads as follows: Sec. 107. - Limitations on exclusive rights: Fair use Notwithstanding the provisions of sections 106 and 106A, the fair use of a copyrighted work, including such use by reproduction in copies or phonorecords or by any other means specified by that section, for purposes such as criticism, comment, news reporting, teaching (including multiple copies for classroom use), scholarship, or research, is not an infringement of copyright. In determining whether the use made of a work in any particular case is a fair use the factors to be considered shall include - (1) the purpose and character of the use, including whether such use is of a commercial nature or is for nonprofit educational purposes; (2) the nature of the copyrighted work; (3) the amount and substantiality of the portion used in relation to the copyrighted work as a whole; and (4) the effect of the use upon the potential market for or value of the copyrighted work. The fact that a work is unpublished shall not itself bar a finding of fair use if such finding is made upon consideration of all the above factors. We hope that making available the relevant information on Pachyonychia Congenita will be a means of furthering research to find effective therapies and a cure for PC.
Transcript of teaching (including multiple copies for classroom use ......Yanning XUE1 Hao CHEN2 Xuesi ZENG2 Yiqun...

2386 East Heritage Way, Suite B, Salt Lake City, Utah 84109 USA Phone +1-877-628-7300 • Email—[email protected]
www.pachyonychia.org
15 March 2005
Use of Articles in the Pachyonychia Congenita Bibliography
The articles in the PC Bibliography may be restricted by copyright laws. These have been made available to you by PC Project for the exclusive use in teaching, scholar-ship or research regarding Pachyonychia Congenita. To the best of our understanding, in supplying this material to you we have followed the guidelines of Sec 107 regarding fair use of copyright materials. That section reads as follows:
Sec. 107. - Limitations on exclusive rights: Fair use Notwithstanding the provisions of sections 106 and 106A, the fair use of a copyrighted work, including such use by reproduction in copies or phonorecords or by any other means specified by that section, for purposes such as criticism, comment, news reporting, teaching (including multiple copies for classroom use), scholarship, or research, is not an infringement of copyright. In determining whether the use made of a work in any particular case is a fair use the factors to be considered shall include - (1) the purpose and character of the use, including whether such use is of a commercial nature or is for nonprofit educational purposes; (2) the nature of the copyrighted work; (3) the amount and substantiality of the portion used in relation to the copyrighted work as a whole; and (4) the effect of the use upon the potential market for or value of the copyrighted work. The fact that a work is unpublished shall not itself bar a finding of fair use if such finding is made upon consideration of all the above factors.
We hope that making available the relevant information on Pachyonychia Congenita will be a means of furthering research to find effective therapies and a cure for PC.

142 EJD, vol. 21, n◦ 1, January-February 2011
A B C
D E F
Figure 1. A) At the age of 33 years: appearance of premature aging. B) Many lax papules and plaques on her abdomen. C)Red urticarial vasculitis-like plaques on the right forearm. D) elastic fibers were diffusely decreased in all layers of the dermis(elastic tissue strain, ×100). E) Elastic fibers are shortened and fragmented only within the inflammatory infiltrate of neutrophilsaround the vessels and between the collagen bundles (elastic tissue strain, ×200). F) At present: therapy after rhytidectomy andblepharoplasty.
the progression of cutis laxa. How to hold back progressionof the disease is still a challenge. �
Disclosure. Financial support: none. Conflict of interest:none.
1 Jiangsu Province hospital oftraditional Chinese medicine,155 Han-zhong Road,210029 Nanjing,Jiangsu Province,China2 Institute of Dermatology,Chinese Academy of MedicalSciences,12 Jiang-wang-miao Road,Nanjing city,210042 Jiangsu Province,China<[email protected]>
Yanning XUE1
Hao CHEN2
Xuesi ZENG2
Yiqun JIANG2
Jianfang SUN2
1. Marshall J, Heyl T, Weber HW. Postinflammatory elastolysis andcutis laxa. A report on a new variety of this phenomenon and a dis-cussion of some syndromes characterized by elastolysis. S Afr Med J1966; 40: 1016-22.2. Thomas WO, Moses MH, Craver RD, et al. Congenital cutis laxa:a case report and review of loose skin syndromes. Ann Plast Surg1993; 30: 252-6.
3. de Schepper S, Loeys B, de Paepe A, et al. Cutis laxa of theautosomal recessive type in a consanguineous family. Eur J Dermatol2003; 13: 529-33.4. Riveros CJP, Gavilán MFB, Francxa LFS, et al. Acquired cutis laxaconfined to the face: case report and review of the literature. Int JDermatol 2004; 43: 931.5. Lewis KG, Bercovitch L, Dill S, et al. Acquired disorders of elas-tic tissue: part II. Decreased elastic tissue. J Am Acad Dermatol2004; 51: 165-85.6. Fisher BK, Page E, Hanna W. Acral localized acquired cutis laxa.J Am Acad Dermatol 1989; 21: 33-40.
doi:10.1684/ejd.2010.1206
A novel mutation (p.Arg94Gly) of keratin17 in a Chinese family with steatocystomamultiplex
Steatocystoma multiplex (SM) is an uncommon, autosomaldominant disorder affecting the pilosebaceous unit, charac-terized by widespread sebum-containing dermal cysts thatmay occasionally rupture, become inflamed, and heal withscarring (SM suppurativum) [1]. SM was demonstrated to

EJD, vol. 21, n◦ 1, January-February 2011 143
1 2
1
1 2 3 4 5 6 7 8
2 3 4 5
prob
and
cont
rol
*****
* * * * *
I
II
III
c.280C>G
ED
B CA
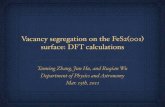
Figure 1. Clinical features of the patients and mutation analysis of KRT17. A) Lesions of Steatocystoma multiplex located onthe chest and abdomen of the proband. B) Lesions were found only in the axilla in a female patient (III-3, 36-year-old). C) Asteatocystoma with sebaceous gland lobules in the cyst wall were present on histology (Haematoxylin and eosin staining; originalmagnification ×40). D) Pedigree of the steatocystoma multiplex family, consistent with autosomal dominant inheritance. Arrowindicates the proband, asterisks denote individuals from whom DNA was obtained. E) KRT17 sequence in exon 1 from theproband and normal, showing codons 92–95. Missense mutation c.280C>G of KRT17 was found in patients that led to aminoacid substitution p.Arg94Gly.
be caused by mutations in the keratin 17 (KRT17) gene,which is also associated with pachyonychia congenital type2 (PC-2) [1, 2]. Here, we report a Chinese SM family witha novel mutation in KRT17.The proband was a 28-year-old Chinese man who wasreferred to our clinic for multiple cysts. When he was 17,multiple papules and cysts developed on his face, chest andaxilla. These cysts gradually grew larger and more exten-sive, varying in size from 0.1 to 5 cm in diameter. Somecysts were repeatedly infected and discharged yellowish,oily material. Physical examination showed multiple softcysts and nodules on his face, nape, trunk, groin, and thighs(figure 1A) with atrophic scars. The nail, palmoplantarareas, mouth, tongue and teeth were normal. Histologicexamination of a subcutaneous cyst revealed that the cystwall was composed of several layers of epithelial cellsaccompanied by sebaceous gland lobules (figure 1C). Therewere 7 affected members among 15 people in the pedigree(figure 1D). Other patients in this family had similar symp-
toms, the females were less affected and their lesions werefound only in the axilla (figure 1B).After informed consent, genomic DNA was extracted fromall available family members. Exon 1 of the KRT17 genewas amplified by polymerase chain reaction (PCR) withspecific primers, to avoid pseudogene contamination, asdescribed previously [3]. The amplified products were puri-fied and directly sequenced. A novel heterozygous mutation(c.280C>G) in the helix initiation motif of the KRT17 genewas found, which resulted in a predicted substitution muta-tion, R94G (figure 1E). This mutation was verified throughthe same PCR and sequencing in other family members and50 unrelated controls.The keratin pairs K17 and K6B are expressed innail bed, palmoplantar epidermis (restricted), epidermalappendages, sebaceous glands, hair shafts, other epitheliaand wound healing [3]. Keratins consist of an alpha-helical rod domain with four helical segments (1A, 1B, 2A,2B). To date, almost all mutations in PC-2 and SM have

144 EJD, vol. 21, n◦ 1, January-February 2011
been reported within the highly conserved helix boundarydomains at either end of the alpha-helical rod domain ofkeratin [4].In total, 18 mutations in KRT17 have been reported(http://www.interfil.org). Most KRT17 mutations werefound in PC-2 families and only 4 mutations were reportedin SM families without nail changes. In PC-2 and SM, themajority of the mutations were found in the helix initiationmotif of K17 with mutations at two codons, N92 and R94,accounting for more than 50% cases. This area is highlyconserved and even subtle amino acid changes are thoughtto disrupt intermediate filament formation and assembly[2, 3].Although SM and PC-2 patients share the same K17 muta-tion, R94C and R94H, some have the typical PC-2 naildystrophy and epidermal cysts, whereas others have onlySM without nail changes [1, 2, 4, 5]. It is suggested that thevariable phenotype is not due to the specific K17 mutationalone, but also depends on a combination of other fac-tors, e.g. androgenic stimulation. Sebum synthesis couldbe stimulated by androgen. Androgen could also increasedownstream PPAR expression, which in turn transduces theterminal differentiation of sebocytes [6]. In this study, thefemale patients had mild SM lesions, only in their axilla,which supports that androgenic stimulation might be animportant factor in SM.In summary, we report a novel missense mutation of K17in a Chinese SM family. This may help in expanding themolecular mutation spectrum of K17 in SM. �
Disclosure. Financial support: none. Conflict of interest:none.
Department of Dermatology,Peking University People’s hospital,#11 Xi Zhi Men Avenue South,Beijing 100044,China<[email protected]>
Dongjie ZANGCheng ZHOU
Meili HEXiaolei MA
Jianzhong ZHANG
1. Smith FJ, Corden LD, Rugg EL, et al. Missense mutations in keratin17 cause either pachyonychia congenita type 2 or a phenotype resem-bling steatocystoma multiplex. J Invest Dermatol 1997; 108: 220-3.2. Covello SP, Smith FJ, Sillevis Smitt JH, et al. Keratin 17 mutationscause either steatocystoma multiplex or pachyonychia congenita type2. Br J Dermatol 1998; 139: 475-80.3. Smith FJ, Liao H, Cassidy AJ, et al. The genetic basis of pachyony-chia congenita. J Investig Dermatol Symp Proc 2005; 10: 21-30.4. Wang JF, Lu WS, Sun LD, et al. Novel missense mutation of keratinin Chinese family with steatocystoma multiplex. J Eur Acad DermatolVenereol 2009; 23: 723-4.5. Wang X, Shi Y, Ye Y, et al. Keratin 17 gene mutation in patients withsteatocystoma multiplex. Zhonghua Yi Xue Za Zhi 2001; 81: 540-3 (inChinese).6. Rosenfield RL, Deplewski D, Kentsis A, et al. Mechanismsof androgen induction of sebocyte differentiation. Dermatology1998; 196: 43-6.
doi:10.1684/ejd.2011.1207
Lipedematous scalp with heterochromia ofscalp hair in a boy
Lipedematous scalp (LS) is a rare condition characte-rized by a thickened and boggy scalp, due to hyperplasiaof the subcutaneous fat layer, without any hair loss. Todate, twenty-two cases have been reported in English witha predilection for middle-aged women [1-4]. Herein, wereport a case of LS with heterochromia of scalp hair in aboy.An 11-year-old Chinese boy presented with an eight-monthhistory of a circumscribed area of lighter hair on the vertexwith gradually asymptomatic thickening of the underlyingscalp. There was no history of trauma or hair dyeing. Thefamily history was also unremarkable. Physical examina-tion revealed a circumscribed, round patch (4 cm × 4 cmin size) of lighter hair on the vertex without shortening orloss of hair (figure 1A). On palpation, the underlying scalpwas found to be thickened, soft and boggy compared tothe unaffected areas. No inflammation or color change wasobserved. Histopathological examination of a punch biopsyspecimen from the affected scalp revealed unremarkableepidermis, a mild perivascular lymphocytic inflammatoryinfiltrate in the dermis and marked hyperplasia of the sub-cutaneous fatty tissue. The number and distribution ofterminal hair follicles were normal. No mucinous mate-rial was observed (figure 1B). Magnetic resonance imaging(MRI) displayed diffuse thickening of the subcutaneous fatlayer at the vertex with a maximum thickness of 11 mm,whereas unaffected scalp measured 5 mm (figure 1C).
1mm
0
A
C
A
Se:3
SS:SESag T2 FRFSE
12341234
IM:6
10
46
8cm2
0
10
0 2 6 8 cm
H
B
Figure 1. A) A circumscribed patch of lighter hair emerg-ing from the vertex whorl. B) Scalp biopsy from the affectedarea shows a mild perivascular lymphocytic inflammatory infil-trate in the dermis and marked hyperplasia of the subcutaneousfatty tissue and normal morphology of the hair follicles (HEstain). C) Sagittal T2-weighted MR image shows thickeningof the subcutaneous fat tissue at the vertex (arrows indicate theaffected area).