
Teaching Excellency in Competency-Based Education David L ...
25
David Lee Gordon, M.D., FAAN, FAHA OUHSC Neurology Teaching Excellence in Competency-Based Education (for Medical Students) 1 Teaching Excellency in Competency-Based Education David L. Gordon, M.D., FAAN, FAHA Professor & Chair, Department of Neurology University of Oklahoma Health Sciences Center Please turn your cell phones and pagers to silent or off. Thank you! OU Neurology TEACHING EXCELLENCE IN COMPETENCY-BASED EDUCATION for Medical Students David Lee Gordon, M.D., FAAN, FAHA Professor, Chair, & Clerkship Director Department of Neurology The University of Oklahoma Health Sciences Center
Transcript of Teaching Excellency in Competency-Based Education David L ...
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
1
OU Neurology
Teaching Excellency in Competency-Based Education
David L. Gordon, M.D., FAAN, FAHA
Professor & Chair, Department of Neurology
University of Oklahoma Health Sciences Center
Please turn your cell phones and pagers to silent or off.
Thank you!
OU Neurology
TEACHING EXCELLENCE IN
COMPETENCY-BASED
EDUCATION for Medical Students
David Lee Gordon, M.D., FAAN, FAHA
Professor, Chair, & Clerkship Director
Department of Neurology
The University of Oklahoma Health Sciences Center

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
2
OU Neurology
DISCLOSURES
FINANCIAL DISCLOSURE
DLG has nothing to disclose
UNLABELED/UNAPPROVED USES
DISCLOSURE
DLG has nothing to disclose
OU Neurology
LEARNING OBJECTIVES
Describe a competency-based, objectives-
driven clinical curriculum and how it differs
from a traditional clinical curriculum
List and describe the 10 essential features
(ABCs) of competency-based education
Name three key factors in creating an
optimal clinical-learning environment
within a competency-based curriculum

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
3
OU Neurology
TEACHING IS AN ART,
EDUCATION IS A SYSTEM
Definitions per Merriam-Webster Dictionary
Teaching = the act, practice, or profession of a teacher (#1)
Education = the field of study that deals mainly with methods
of teaching and learning in schools (#2)
Essential Qualities per DLG
Teaching excellence
Ability to convey enthusiasm & make material accessible
Education excellence
Ability to develop and implement consistently effective
systems of teaching and learning
OU Neurology
WHAT IS THE CORRECT ANSWER?
Experts are the best instructors.
A.True
B.False
“Evidence from cognitive science, organizational
behavior, and educational psychology suggests
that experts are not always the best teachers.”
Huston T. Teaching What You Don’t Know (2009)
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
4
OU Neurology
WHAT IS THE CORRECT ANSWER?
Superior performance correlates best with: A. Deliberate practice
B. Domain-related knowledge
C. Extensive experience
D. General education
“Superior performance does not automatically develop from
extensive experience, general education, and domain-related
knowledge.”
“Observed performance does not necessarily correlate with
greater professional experience.”
“Expert performance can, however, be traced to active
engagement in deliberate practice.”
Ericsson KA. Acad Emerg Med 2008;15:988-994
OU Neurology
WHAT IS THE CORRECT ANSWER?
Professional expertise correlates best with: A. Deliberate practice
B. Perceived mastery of knowledge and skill
C. Reputation
“Traditionally, professional expertise has been judged by length of
experience, reputation, & perceived mastery of knowledge & skill.”
“Unfortunately, recent research demonstrates only a weak relationship between these indicators of expertise & actual, observed performance.”
“Expert performance can, however, be traced to active engagement in deliberate practice.”
Ericsson KA. Acad Emerg Med 2008;15:988-994
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
5
OU Neurology
WHAT IS THE CORRECT ANSWER?
You should teach to the test.
A. True
B. False
“When educational evaluation data are seen and used
as a tool, not a weapon, the outlook becomes
improvement and mastery rather than enforcement.”
McGaghie WC. Guidebook for Clerkship Directors (2005)
OU Neurology
WHAT IS THE CORRECT ANSWER?
External standardized tests such as the USMLE are valid measures of clinical performance.
A. True
B. False
“USMLE Step 1 & 2 scores do not correlate with reliable measures of clinical skill acquisition by medical students, residents, & fellows.”
“The validity argument about using USMLE Step 1 & 2 scores for postgraduate residency selection decisions is not structured, coherent, or evidence based.”
“Continued use of USMLE Step 1 & 2 scores for postgraduate medical residency selection is discouraged.”
McGaghie WC et al. Acad Med 2011;86:48-52
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
6
OU Neurology
TRADITIONAL CURRICULUM
IS TEACHER & PATIENT CENTERED
Ward teaching Difficult to standardize (variable patients & faculty)
Inefficient time (limited teaching, feedback, deliberate practice)
Not highest priority (secondary to patient care & safety)
Increasingly inadequate for training due to time constraints induced by changes in healthcare delivery & duty-hour limitations
Didactic teaching Lecture format (passive with limited long-term retention)
Based on faculty expertise (not student need)
Assessments Ward assessment—high validity, but low reliability, inconsistent
implementation, & often inconsistent with declared curriculum
Independent MCQ exam (e.g., “shelf”)—not linked to objectives or student experiences & does not assess skills, attitudes, behavior
Local expertise drives learning
& assessments do not reflect or drive performance
OU Neurology
COMPETENCY-BASED CURRICULUM
IS LEARNER CENTERED
Emphasizes learner needs, not teacher needs or knowledge
Objectives are not superfluous—they drive the process (“Begin with the end in mind” – Steven Covey)
Standardized learning and assessment for all learners, regardless of ward experiences
Assesses what is learned, not what is taught
Requires major changes in: Traditionally-held tenets of education (buy-in of key faculty)
Learner and institution schedules (buy-in of chair & deans)
Preferred by vast majority of learners
Most like structure & direction—everyone learns
Consensus guidelines & course objectives drive learning
& assessments reflect & drive performance

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
7
OU Neurology
COMPETENCY-BASED EDUCATION:
THE PROCESS GUARANTEES SUCCESS
1. Define “fundamental
knowledge”
2. Teach fundamentals
3. Test knowledge
4. Hope for best
3. Develop learning
experiences
2. Design measures and
standards of performance
1. Define successful graduate
Traditional / Flexnerian
“Planning Forwards”
Competency / Outcome-Based
“Planning Backwards”
Stephen R. Smith, M.D., MPH
A Practical Guide for Medical Teachers, 3rd ed. (2009)
Models for Curriculum Development
OU Neurology
THE LOGIC BEHIND
COMPETENCY-BASED EDUCATION
1. Competent physicians demonstrate certain knowledge, skills, attitudes, & behaviors (KSAB)
2. Graduating students & residents must demonstrate core KSAB
3. Assessment of core KSAB requires setting specific, measurable standards (= objectives or competencies), i.e., establishment of a competency-based curriculum
4. Learning core KSAB requires deliberate practice with feedback in a standardized curriculum
5. Demonstration of competence is an all-or-none phenomenon
6. Assessment of competence requires mastery testing with criterion-referenced grading
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
8
OU Neurology
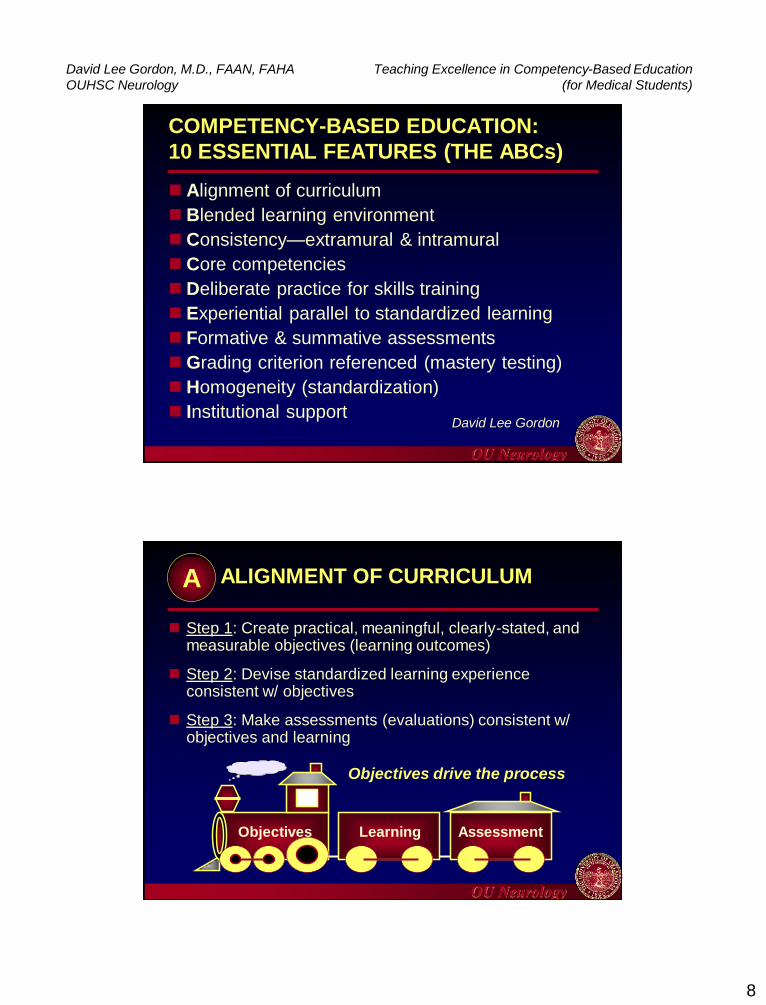
COMPETENCY-BASED EDUCATION:
10 ESSENTIAL FEATURES (THE ABCs)
Alignment of curriculum
Blended learning environment
Consistency—extramural & intramural
Core competencies
Deliberate practice for skills training
Experiential parallel to standardized learning
Formative & summative assessments
Grading criterion referenced (mastery testing)
Homogeneity (standardization)
Institutional support David Lee Gordon
OU Neurology
ALIGNMENT OF CURRICULUM
Step 1: Create practical, meaningful, clearly-stated, and measurable objectives (learning outcomes)
Step 2: Devise standardized learning experience consistent w/ objectives
Step 3: Make assessments (evaluations) consistent w/ objectives and learning
Assessment Learning Objectives
Objectives drive the process
A
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
9
OU Neurology
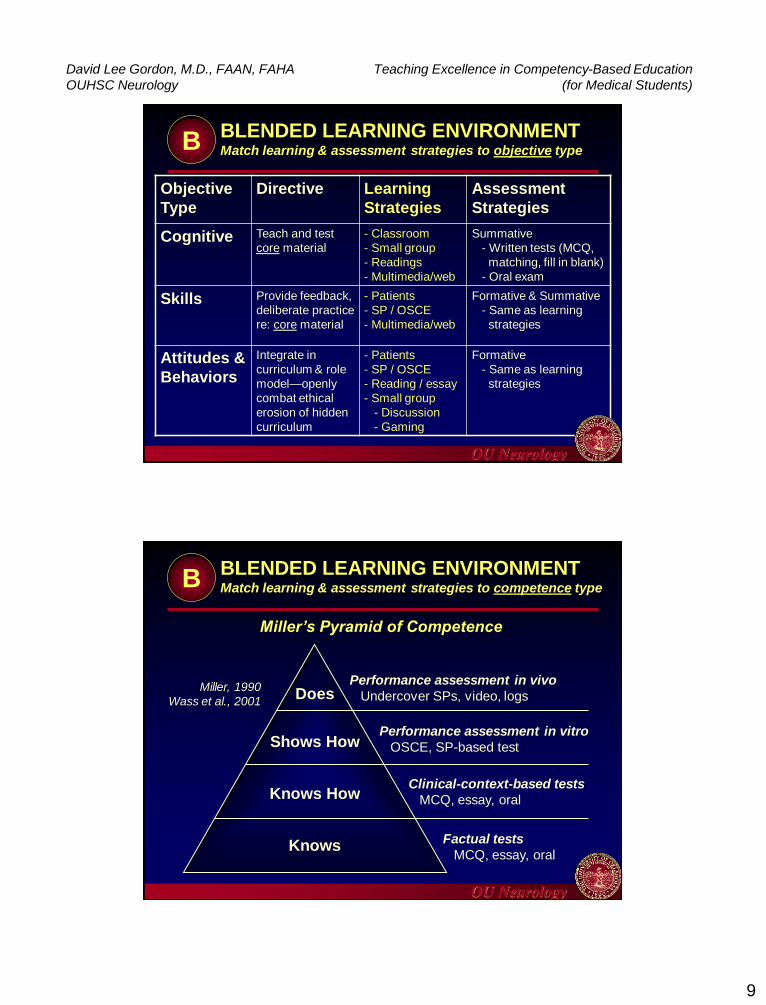
BLENDED LEARNING ENVIRONMENT Match learning & assessment strategies to objective type
Objective
Type
Directive Learning
Strategies
Assessment
Strategies
Cognitive Teach and test
core material
- Classroom
- Small group
- Readings
- Multimedia/web
Summative
- Written tests (MCQ,
matching, fill in blank)
- Oral exam
Skills Provide feedback,
deliberate practice
re: core material
- Patients
- SP / OSCE
- Multimedia/web
Formative & Summative
- Same as learning
strategies
Attitudes &
Behaviors
Integrate in
curriculum & role
model—openly
combat ethical
erosion of hidden
curriculum
- Patients
- SP / OSCE
- Reading / essay
- Small group
- Discussion
- Gaming
Formative
- Same as learning
strategies
B
OU Neurology
OU Neurology
BLENDED LEARNING ENVIRONMENT Match learning & assessment strategies to competence type
Does
Shows How
Knows How
Knows
Performance assessment in vivo
Undercover SPs, video, logs
Performance assessment in vitro
OSCE, SP-based test
Clinical-context-based tests
MCQ, essay, oral
Factual tests
MCQ, essay, oral
Miller, 1990
Wass et al., 2001
Miller’s Pyramid of Competence
B

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
10
OU Neurology
BLENDED LEARNING ENVIRONMENT The support-challenge model of learning (Bower, 1998)
SUPPORT
Core competencies /
Pre-identified objectives
Curricular alignment
Private formative
assessment (1-on-1
feedback)
CHALLENGE
Public formative
assessment (feedback
before or by peers)
Summative assessment
high
SUPPORT
CH
AL
LE
NG
E
RETREAT GROWTH
STASIS CONFIRMATION
high
B
“Rule with an iron fist & a heart of gold”
OU Neurology
CONSISTENCY
Extramural consistency Base course on consensus statement
Obtain external review
Intramural consistency Longitudinal
M1 through M4
KSAB (knowledge, skills, attitudes, behaviors)
Horizontal Intracurriculum / Intradepartment / Interdepartment
Hidden / informal curriculum
Across multiple clinical sites
Requires extensive communication and cooperation among course directors and faculty—and is most effective with institutional direction and oversight
C1

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
11
OU Neurology
CORE COMPETENCIES Required Characteristics
Pertinent (learner-population specific)
Integrated (defined first & as guide for rest of curriculum)
Comprehensive (KSAB, all 6 ACGME competencies)
Consistent (extramurally & intramurally)
Standardized (uniformly taught in curriculum)
Assessable (varied methods, matched to objective type)
(1) Patient care
(2) Medical knowledge
(3) Practice-based learning & improvement
(4) Interpersonal & communication skills
(5) Professionalism
(6) Systems-based practice
C2
OU Neurology
CORE COMPETENCIES Keys to Successful Implementation
Base all assessments on core competencies only
Publicize this fact to learners & teachers
Discourage teaching contrary to core competencies
Encourage teaching supplemental to core
competencies—but do not assess students on
supplemental information or skills
Assessing only core competencies leads to improved:
Retention of knowledge & skills
Learner confidence
Enthusiasm for the topic
Comprehension of supplemental learning
C2

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
12
OU Neurology
DELIBERATE PRACTICE FOR
SKILLS TRAINING…Evolution of a Concept
The value of experience is not in seeing much but in seeing wisely—Sir William Osler 1849-1919
Know that by practice alone can you become an expert—Sir William
Osler 1849-1919
Practice does not make perfect. Only perfect practice makes
perfect—Vince Lombardi 1913-1970
Expert performance can be traced to active engagement in
deliberate practice, where training (often designed and arranged by
teachers and coaches) is focused on improving particular tasks—K
Anders Ericsson 2008
D
“Experience” & “practice” are equally important to achieve
competence & expertise. This is true for all skill-based
professionals (e.g., athletes, musicians, dancers, pilots,
chess masters—and health professionals).
OU Neurology
DELIBERATE PRACTICE FOR
SKILLS TRAINING…Definition & Components
Focused, repetitive practice consisting of domain-related activities necessary for improving performance & advancement to the level of expert
Essential components include: Motivated & attentive learner
Well-defined task and goals
Appropriate level of difficulty
Informative feedback from educational sources
Opportunities for repetition & refinements Modified from
Ericsson KA et al. Psychol Rev. 1993;100 (3):363-406
Ericsson KA Acad Emerg Med. 2008;15:988-94
McGaghie et al. Acad Med. 2011;86:706-11
D
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
13
OU Neurology
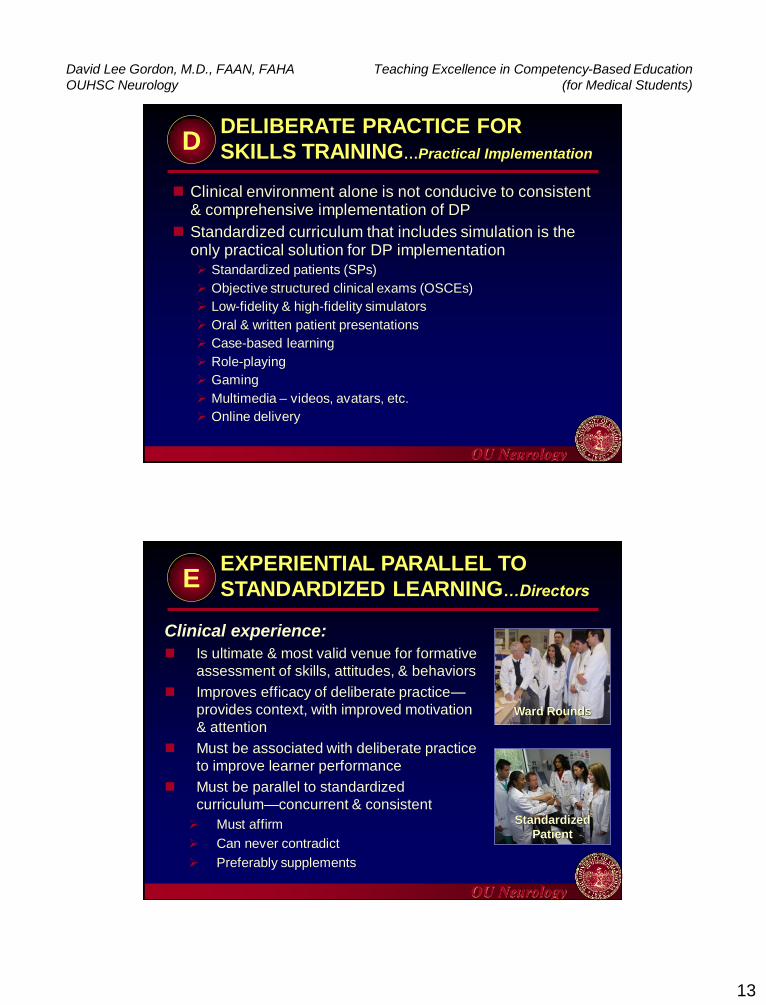
DELIBERATE PRACTICE FOR
SKILLS TRAINING…Practical Implementation
Clinical environment alone is not conducive to consistent & comprehensive implementation of DP
Standardized curriculum that includes simulation is the only practical solution for DP implementation
Standardized patients (SPs)
Objective structured clinical exams (OSCEs)
Low-fidelity & high-fidelity simulators
Oral & written patient presentations
Case-based learning
Role-playing
Gaming
Multimedia – videos, avatars, etc.
Online delivery
D
OU Neurology
EXPERIENTIAL PARALLEL TO
STANDARDIZED LEARNING…Directors
Clinical experience:
Is ultimate & most valid venue for formative
assessment of skills, attitudes, & behaviors
Improves efficacy of deliberate practice—
provides context, with improved motivation
& attention
Must be associated with deliberate practice
to improve learner performance
Must be parallel to standardized
curriculum—concurrent & consistent
Must affirm
Can never contradict
Preferably supplements
Ward Rounds
Standardized
Patient
E

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
14
OU Neurology
EXPERIENTIAL PARALLEL TO
STANDARDIZED LEARNING…Attendings
Clinical preceptors can optimize student
skill acquisition and performance by
providing an environment:
1. Consistent with core competencies
established by the course director
2. Conducive to deliberate practice
3. With optimal balance of support & challenge
E
OU Neurology
FORMATIVE & SUMMATIVE
ASSESSMENTS…Principles & Definitions
General principles
Validity (appropriateness)
Reliability (consistency)
Feasibility (practicality)
Formative assessment (feedback—without grade)
Summative assessment (graded testing)
Make tests pertinent, assess core competencies
Set appropriate standards (minimal competence)
Overall course
Specific competencies
Use criterion-referenced (not norm-referenced) grading
Monitor results for course QI (curriculum evaluation)
Wass et al., 2001
Assessment drives learning—
accept & embrace it!
You should teach to the test.
F

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
15
OU Neurology
GRADING CRITERION REFERENCED
(MASTERY TEACHING)…vs. Norm Referenced
Criterion-Referenced (Absolute)
Individual vs. fixed standard (criterion)
Standard
Absolute—knowledge or skill learner
must have in order to pass
Based on instructor’s judgment
Known in advance (objectives)
Purpose is to assess competence
Mastery testing/assumption
Most students should perform well
(common mastery level 85%)
Bell-shaped curve skewed to right
Items assess core competencies,
linked to objectives
Diagnostic feedback relative to
performance is clear
Norm-Referenced (Relative)
Individual vs. others
Standard
Relative—based on class test
results (mean/standard deviation)
Influenced by examinees’ abilities
Not known in advance
Purpose is to discriminate
Normative assumption
Guaranteed some will fail
Bell-shaped curve, variable scores
Items assess broad content, not
linked to local objectives
Diagnostic feedback relative to
performance unclear
G
OU Neurology
GRADING CRITERION REFERENCED
(MASTERY TEACHING)…Sample Curves G
Mean SD SD CP Minimal 100%
CRITERION-REFERENCED
GRADING
NORM-REFERENCED
GRADING
Comparison to fixed standards Comparison to other students
HP
CP = Competent performer
HP = High performer
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
16
OU Neurology
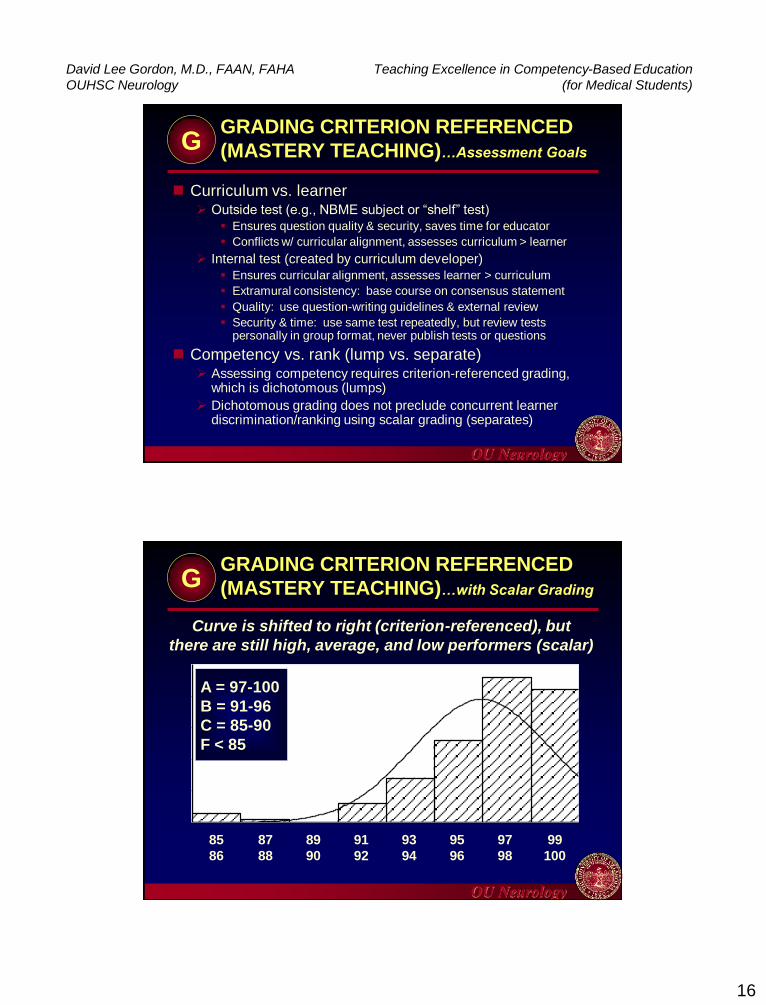
GRADING CRITERION REFERENCED
(MASTERY TEACHING)…Assessment Goals
Curriculum vs. learner Outside test (e.g., NBME subject or “shelf” test)
Ensures question quality & security, saves time for educator
Conflicts w/ curricular alignment, assesses curriculum > learner
Internal test (created by curriculum developer)
Ensures curricular alignment, assesses learner > curriculum
Extramural consistency: base course on consensus statement
Quality: use question-writing guidelines & external review
Security & time: use same test repeatedly, but review tests personally in group format, never publish tests or questions
Competency vs. rank (lump vs. separate) Assessing competency requires criterion-referenced grading,
which is dichotomous (lumps)
Dichotomous grading does not preclude concurrent learner discrimination/ranking using scalar grading (separates)
G
OU Neurology
GRADING CRITERION REFERENCED
(MASTERY TEACHING)…with Scalar Grading
46.044.042.040.038.036.034.032.0
50
40
30
20
10
0
Std. Dev = 2.82
Mean = 43.0
N = 138.00
99
100
97
98
95
96
93
94
91
92
89
90
87
88
85
86
A = 97-100
B = 91-96
C = 85-90
F < 85
Curve is shifted to right (criterion-referenced), but
there are still high, average, and low performers (scalar)
G
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
17
OU Neurology
HOMOGENEITY
(STANDARDIZATION)
Curriculum based on mastering core competencies
and deliberate practice requires that ALL students
receive an equivalent—homogeneous or
standardized—learning experience
“Standardized” curriculum:
Is highly structured
Requires punctual & mandatory attendance
Takes precedence over ward responsibilities
Requires full attention of learners (pagers & phones off)
Accounts for majority of grade, but not student time
Requires strong, well-organized course director
H
OU Neurology
INSTITUTIONAL SUPPORT Leadership commitment
Curriculum champion
Faculty member delegated (not relegated) as director with mettle, motivation, authority, & protected time
Buy-in ability and bypass authority
Schedule 100% learner attendance
Cooperation of dept. (chair/faculty) & school (deans)
Simulation exercises, e.g., SPs, OSCEs, skills center
Resources Director > 50% FTE, coordinator > 50% FTE
Simulation / SP costs
Instructors (faculty / residents / nurses)
I
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
18
OU Neurology
COMPETENCY-BASED EDUCATION:
10 ESSENTIAL FEATURES (THE ABCs)
Alignment of curriculum
Blended learning environment
Consistency—extramural & intramural
Core competencies
Deliberate practice for skills training
Experiential parallel to standardized learning
Formative & summative assessments
Grading criterion referenced (mastery testing)
Homogeneity (standardization)
Institutional support David Lee Gordon
OU Neurology
OPTIMAL CLINICAL-LEARNING ENVIRONMENT
IN COMPETENCY-BASED CURRICULUM
Three key factors:
1. Consistent with core competencies
established by the course director
2. Conducive to deliberate practice
3. With optimal balance of support & challenge
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
19
OU Neurology
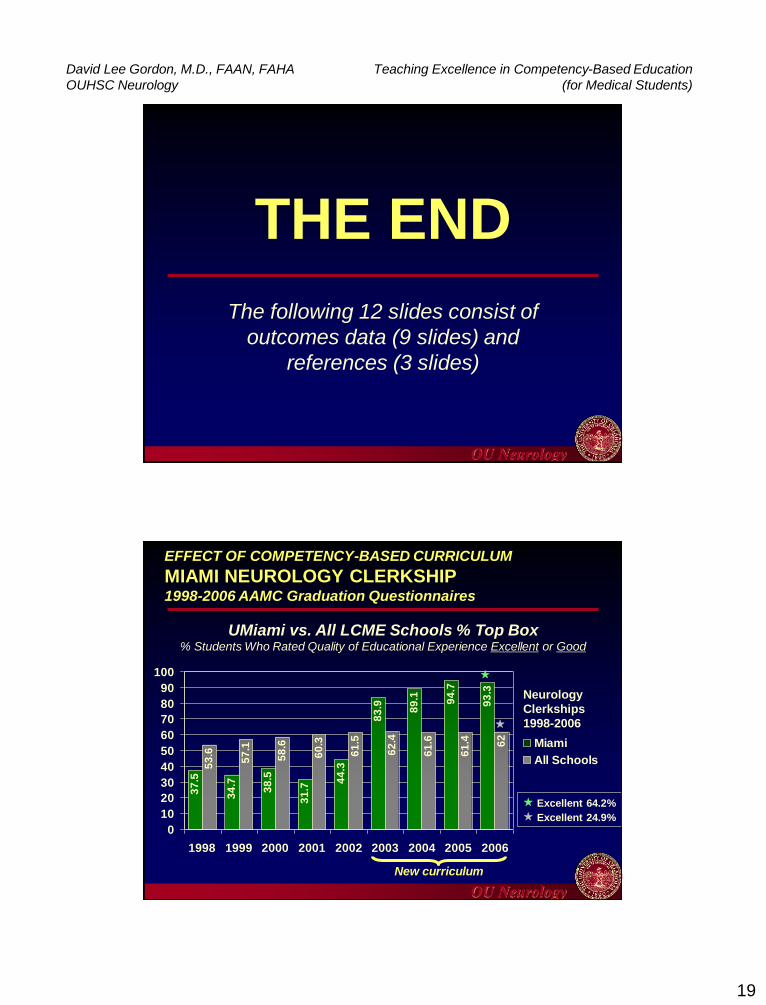
THE END
The following 12 slides consist of
outcomes data (9 slides) and
references (3 slides)
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM
MIAMI NEUROLOGY CLERKSHIP 1998-2006 AAMC Graduation Questionnaires
93
.3
53
.6
57
.1
58
.6
60
.3
61
.5
62
.4
61
.6
61
.4 62
37
.5
34
.7
38
.5
31
.7
44
.3
83
.9 89
.1 94
.7
0
10
20
30
40
50
60
70
80
90
100
1998 1999 2000 2001 2002 2003 2004 2005 2006
Miami
All Schools
New curriculum
UMiami vs. All LCME Schools % Top Box % Students Who Rated Quality of Educational Experience Excellent or Good
Neurology
Clerkships
1998-2006
Excellent 64.2%
Excellent 24.9%

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
20
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM
OU-OKC NEUROLOGY CLERKSHIP 2005-2011 AAMC Graduation Questionnaires
37
.5
48
.7
31
.4
31
.7
94
.5
95
.3 97
61
.4 62
61
.2
61
.3
63
.3
73
.1
73
.4
0
10
20
30
40
50
60
70
80
90
100
2005 2006 2007 2008 2009 2010 2011
OU-OKC
All Schools
New curriculum
OU-OKC vs. All LCME Schools % Top Box % Students Who Rated Quality of Educational Experience Excellent or Good
Excellent 82.1%
Excellent 34.1%
Neurology
Clerkships
2005-2011
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM
OU-OKC CLERKSHIPS 2007-8 2009 AAMC Graduation Questionnaire (n = 73)
25
6.9
32.9
50.7
61.6 60.757.5
76.7
70.8
26.3
79.5
91.8
83.587.7 87.6
94.5
0
10
20
30
40
50
60
70
80
90
100
A B C D E F G NEURO
Excellent %
Top Box %
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
21
OU Neurology
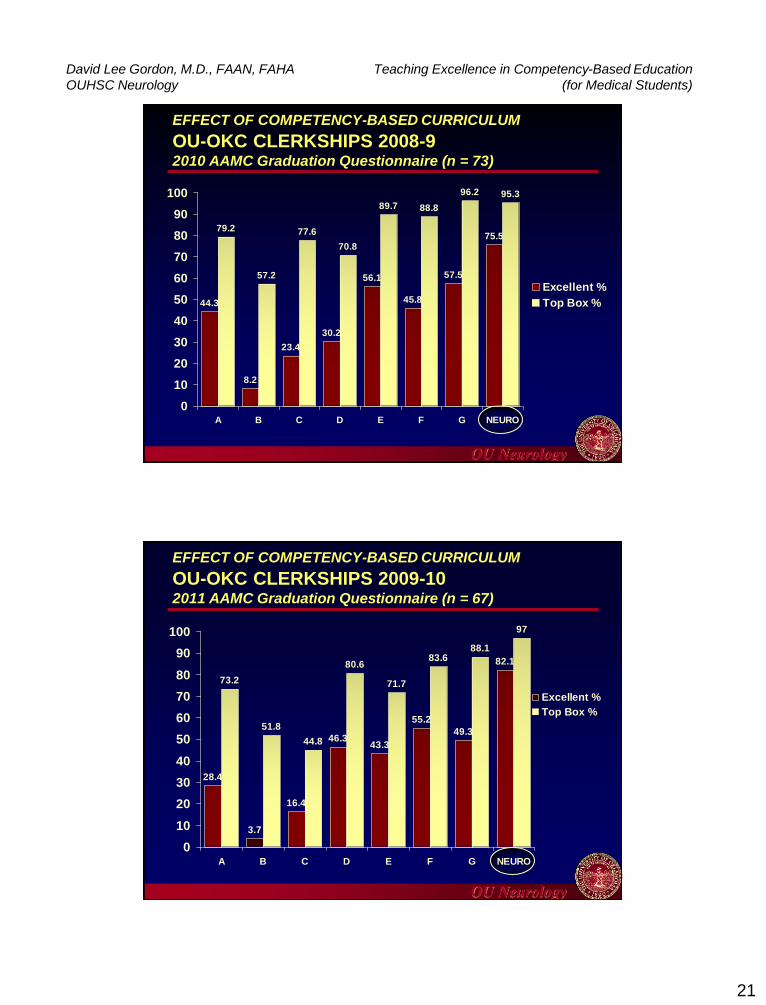
EFFECT OF COMPETENCY-BASED CURRICULUM
OU-OKC CLERKSHIPS 2008-9 2010 AAMC Graduation Questionnaire (n = 73)
44.3
8.2
23.4
30.2
56.1
45.8
57.5
75.579.2
57.2
77.6
70.8
89.7 88.8
96.2 95.3
0
10
20
30
40
50
60
70
80
90
100
A B C D E F G NEURO
Excellent %
Top Box %
OU Neurology
28.4
3.7
16.4
46.343.3
55.2
49.3
82.1
73.2
51.8
44.8
80.6
71.7
83.688.1
97
0
10
20
30
40
50
60
70
80
90
100
A B C D E F G NEURO
Excellent %
Top Box %
EFFECT OF COMPETENCY-BASED CURRICULUM
OU-OKC CLERKSHIPS 2009-10 2011 AAMC Graduation Questionnaire (n = 67)

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
22
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM
OU-OKC TOP TWO RATED CLERKSHIPS 2009-2011 AAMC Graduation Questionnaires
3.4
3.5
3.4
3.8
3.7
3.7
3.2 3.4 3.6 3.8 4
2011
2010
2009
Neurology
Next HighestOU-OKC
Clerkship
2 wks
2 wks
4 wks
Length of
Neurology Clerkship
OU-OKC Clerkship Mean Scores 1 Poor, 2 Fair, 3 Good, 4 Excellent
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM UM STUDENTS CHOOSING NEUROLOGY CAREER
1
3 3 3
5
3 3
7 7
10
0
2
4
6
8
10
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
UMiami Students Choosing
Neurology or Child
Neurology as a Career
Graduates of new
curriculum

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
23
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM OU STUDENTS CHOOSING NEUROLOGY CAREER
1
2
0 0 0
1
0
8
7
10
6
0
2
4
6
8
10
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Graduates of new
curriculum
OU Students Choosing
Neurology or Child
Neurology as a Career
OU Neurology
EFFECT OF COMPETENCY-BASED CURRICULUM NEUROLOGY DEPARTMENT TEACHING AWARDS
TEACHING AWARD Before 2007 After 2007
Stanton L. Young Master
Teacher Award (f. 1984) Peggy W. Wisdom 1996
Herman E. Jones 2009
David Lee Gordon 2011
Edgar W. Young Lifetime
Achievement Award (f. 1987) Herman E. Jones 2011
M2 Aesculapian Award –
To Faculty (f. 1962) Herman E. Jones 2006
M3 Aesculapian Award –
To Resident (f. 1975) AJ Vaughn 2011
M4 Aesculapian Award –
To Faculty (f. 1962) Gunter Haase 1964 Herman E. Jones 2009

David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
24
OU Neurology
SELECT TEXTBOOK REFERENCES
Dent JA, Harden RM. A Practical Guide for Medical Teachers. 3rd ed.
Edinburgh: Churchill Livingstone; 2009
Fincher RME, Cox S, DaRosa DA, Lynn DJ, Margo K, Morgenstern BZ,
Pangaro LN, Sierles FA. Guidebook for Clerkship Directors, 3rd edition.
Omaha: Alliance for Clinical Education; 2005
Huston T. Teaching What You Don’t Know. Cambridge, Mass.: Harvard
University Press; 2009
Kern DE, Thomas PA, Howard DM, Bass EB. Curriculum Development
for Medical Education. A Six-Step Approach. Baltimore: The Johns
Hopkins University Press; 1998
Norman GR, van der Vleuten CPM, Newble DI. International Handbook
of Research in Medical Education. Dordrecht: Kluwer Academic
Publishers; 2002
OU Neurology
SELECT ARTICLE REFERENCES, 1 of 2
Bower DJ. Support-challenge-vision: a model for faculty
mentoring. Medical Teacher 1998;20:595-597
Ericsson KA, Krampe RT, Tesch-Römer C. The role of
deliberate practice in the acquisition of expert
performance. Psychological Review 1993;100:363-406
Ericsson KA. Deliberate practice and acquisition of expert
performance: a general overview. Acad Emerg Med
2008;15:988-994
McGaghie WC, Issenberg SB, Cohen ER, Barsuk JH,
Wayne DB. Does simulation-based medical education
with deliberate practice yield better results than traditional
clinical education? A meta-analytic comparative review of
the evidence. Acad Med 2011;86:706-711
David Lee Gordon, M.D., FAAN, FAHA
OUHSC Neurology
Teaching Excellence in Competency-Based Education
(for Medical Students)
25
OU Neurology
SELECT ARTICLE REFERENCES, 2 of 2
McGaghie WC, Cohen ER, Wayne DB. Are USMLE step
1 & 2 scores valid measures for postgraduate medical
residency selection decisions? Acad Med 2011;86:48-52
Miller GE. The assessment of clinical skills / competence /
performance. Acad Med 1990;65:S63-S67
Smith SR, Dollase RH, Boss JA. Assessing students’
performance in a competency-based curriculum. Acad
Med 2003;78:97-107
Wass V, van der Vleuten C, Shatzer J, Jones R.
Assessment of clinical competence. Lancet
2001;357:945-949
OU Neurology
THE END


















