Teaching acid base and electrolyte...
67
Teaching acid base and electrolyte problems Robert M. Centor, MD Director, and Professor DGIM UAB The importance of the topic Dawson-Saunders B, Feltovich PJ, Coulson RI, Steward DE. A survey of medical school teachers to identify basic biomedical concepts medical students should understand. Acad Med 1990 Jul;65(7):448-54 Acid-base electrolyte balance ranked #1 in importance (of 27 biomedical concepts). Serum sodium osmolarity and controls ranked 7.5. Acid-base ranked #1 in clinical difficulty, while serum sodium ranked #7 in clinical difficulty. This topic remains central to the care of inpatients, yet also pertains in outpatient medicine (while less frequently). Thoughts on teaching acid base and electrolytes Students and residents respond well to a logical physiologic approach to solving these clinical problems. Over the past decade I have collected (and continue to collect) classic cases which demonstrate these principles. I will focus on acid base and hyponatremia in this session, as these problems present most often. These problems lend themselves to a standard systematic approach. The classic principles of small group learning generally apply. I personally like asking students or residents questions. I “rescue” them when it is obvious that they are lost – moving on to the next learner. Often more than one learner is lost. I discourage pattern recognition, preferring the teaching of a standard approach. I teach first at a “101” level, but often add advanced concepts when appropriate. Repetition is necessary to learn these concepts. I present the standard approach repeatedly, and the residents (who have heard it often) tell me that they learn something new each time. We will start first with hyponatremia:
Transcript of Teaching acid base and electrolyte...

Teaching acid base and electrolyte problems
Robert M. Centor, MD Director, and Professor DGIM
UAB The importance of the topic
Dawson-Saunders B, Feltovich PJ, Coulson RI, Steward DE. A survey of medical school teachers to identify basic biomedical concepts medical students should understand. Acad Med 1990 Jul;65(7):448-54 Acid-base electrolyte balance ranked #1 in importance (of 27 biomedical concepts). Serum sodium osmolarity and controls ranked 7.5. Acid-base ranked #1 in clinical difficulty, while serum sodium ranked #7 in clinical difficulty. This topic remains central to the care of inpatients, yet also pertains in outpatient medicine (while less frequently). Thoughts on teaching acid base and electrolytes Students and residents respond well to a logical physiologic approach to solving these clinical problems. Over the past decade I have collected (and continue to collect) classic cases which demonstrate these principles. I will focus on acid base and hyponatremia in this session, as these problems present most often. These problems lend themselves to a standard systematic approach. The classic principles of small group learning generally apply. I personally like asking students or residents questions. I “rescue” them when it is obvious that they are lost – moving on to the next learner. Often more than one learner is lost. I discourage pattern recognition, preferring the teaching of a standard approach. I teach first at a “101” level, but often add advanced concepts when appropriate. Repetition is necessary to learn these concepts. I present the standard approach repeatedly, and the residents (who have heard it often) tell me that they learn something new each time. We will start first with hyponatremia:

Hyponatremia – a presentation with discussion A 47 year old man with empyema and hyponatremia HPI: A 47 year old man presented to the VA Hospital complaining of 10 days of progressive dyspnea. He also had lower extremity swelling. Right sided pleuritic chest pain started a few days prior to admission (which he blames on chopping down a tree in his yard). He complains of a chronic cough. His wife states that “he has not been himself” for the last month. He has had problems with weakness and difficulty walking. He has developed a productive cough, but denies fever, night sweats or chills PMH: unremarkable Meds: Aspirin Social History: 45 pack years of cigarettes, 1-2 cases of beer each week, no IV drug use, no HIV risk factors Review of Systems: Otherwise non-contributory PE: VS: T 98 P 96 BP 160/70 R 20 General: No acute distress, appears older than stated age HEENT: normal, anicteric Neck: supple, no thyromegaly Heart: S1, S2 normal, no murmurs rubs or gallops Lungs: decreased breath sounds right thorax, dull to percussion 2/3 of right chest, positive egophony, left sided crackles at the base Abdomen: good BS, no masses or organomegaly Extremities: 2+ peripheral edema to mid shin Neuro: 3/5 proximal muscle strength, sensation intact, deep tendon reflexes sluggish Laboratory data on admission: CBC: H/H 11.6/34 WBC 18,700 38s/54b/4l Platelets539,000 Electrolyte panel: Sodium 116 Potassium 4.1 Chloride 81 Bicarbonate 26 BUN 10 Creatinine 0.6 Glucose 92 Chest X-ray: large right sided effusion Thoracentesis: cloudy, foul smelling fluid Pleural fluid analysis: 116 nucleated cells, 60 RBCs. Total protein 500 mg/dl. pH 6.59 Questions: How do you evaluate his low serum sodium? What are the likely causes of hyponatremia in this man? Caveats: The most important feature of this case is an understanding of a logical approach to the low serum sodium. The diagnosis is not as important, if you do everything correctly, you will make the right diagnosis, even if it did not initially occur to you.

Hyponatremia Solution: 1. How do you evaluate his low serum sodium? I have a standard method for evaluating serum sodium. I will present a stepwise system that I encourage you to use. Internal medicine requires some compulsivity – and electrolyte disorders clearly require you to work through the possibilities carefully. We should remember that hyponatremia represents a problem of water, not sodium. Hyponatremia occurs either because of excess water intake (very rare) or inability to excrete free water.
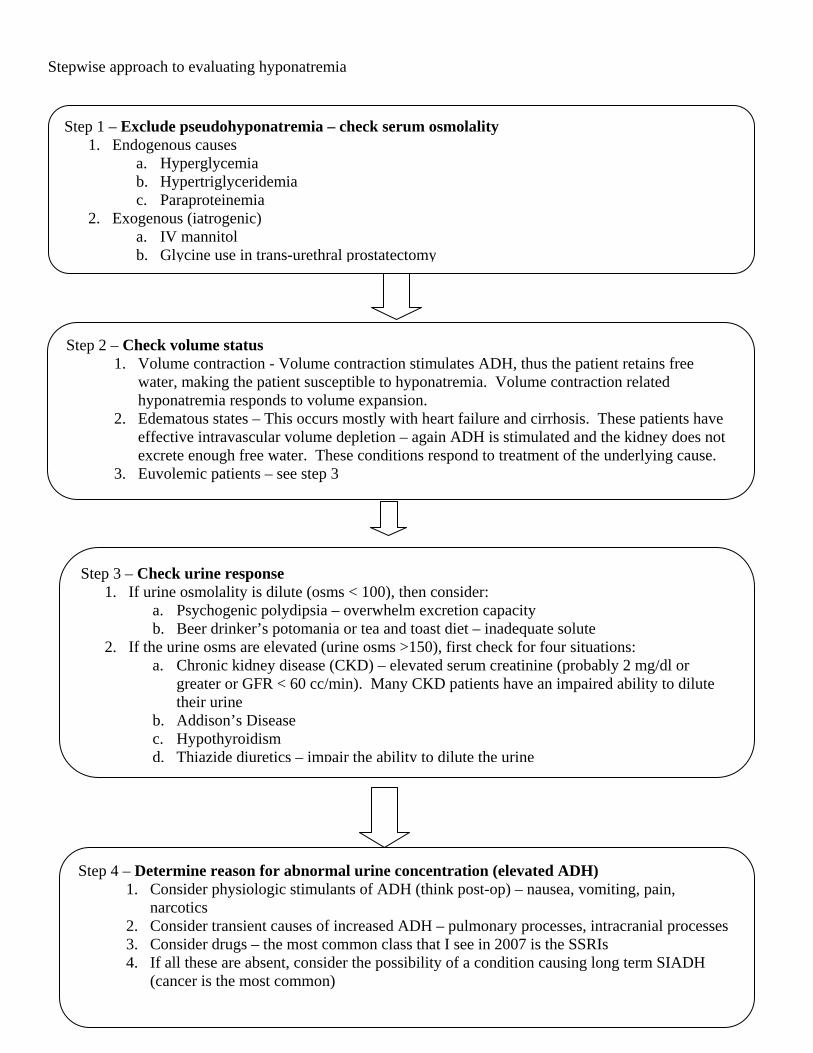
Stepwise approach to evaluating hyponatremia
Step 1 – Exclude pseudohyponatremia – check serum osmolality 1. Endogenous causes
a. Hyperglycemia b. Hypertriglyceridemia c. Paraproteinemia
2. Exogenous (iatrogenic) a. IV mannitol b. Glycine use in trans-urethral prostatectomy
Step 2 – Check volume status 1. Volume contraction - Volume contraction stimulates ADH, thus the patient retains free
water, making the patient susceptible to hyponatremia. Volume contraction related hyponatremia responds to volume expansion.
2. Edematous states – This occurs mostly with heart failure and cirrhosis. These patients have effective intravascular volume depletion – again ADH is stimulated and the kidney does not excrete enough free water. These conditions respond to treatment of the underlying cause.
3. Euvolemic patients – see step 3
Step 3 – Check urine response 1. If urine osmolality is dilute (osms < 100), then consider:
a. Psychogenic polydipsia – overwhelm excretion capacity b. Beer drinker’s potomania or tea and toast diet – inadequate solute
2. If the urine osms are elevated (urine osms >150), first check for four situations: a. Chronic kidney disease (CKD) – elevated serum creatinine (probably 2 mg/dl or
greater or GFR < 60 cc/min). Many CKD patients have an impaired ability to dilute their urine
b. Addison’s Disease c. Hypothyroidism d. Thiazide diuretics – impair the ability to dilute the urine
Step 4 – Determine reason for abnormal urine concentration (elevated ADH) 1. Consider physiologic stimulants of ADH (think post-op) – nausea, vomiting, pain,
narcotics 2. Consider transient causes of increased ADH – pulmonary processes, intracranial processes 3. Consider drugs – the most common class that I see in 2007 is the SSRIs 4. If all these are absent, consider the possibility of a condition causing long term SIADH
(cancer is the most common)

2. What are the likely causes of hyponatremia in this man? The patient had a serum osm = 234 mOsm/kg confirming true hyponatremia. Despite his mild edema, his exam was consistent with a euvolemic state. (note that SIADH causes a mild volume expansion) When the patient was first admitted we assumed that he had ADH release related to his empyema. However, we proceeded with the evaluation. First, we obtained a urine osm = 332 mOsm/kg. This is in fact inappropriately high for his serum sodium. This result was consistent with our presumed diagnosis. However, like a runner who hits a home run, we touched all the bases and found: TSH = 26.8 (normal range 0.6-4.7) Free T4 < 0.023 (normal range 0.8-1.6) Free T3 = 1.16 (normal range 2.3-4.2) This confirmed a laboratory diagnosis of hypothyroidism. We went back to the bedside and discovered:
1. His energy level had decreased dramatically 4-5 years previously. 2. His antecubital fossa revealed dry coarse skin 3. As mentioned in the previous physical exam, his reflexes were sluggish (especially the relaxation
phase). He had a prolonged hospital course because of the empyema (he required over 2 weeks of chest tube drainage). We started synthetic thyroid with dramatic clinical results. He expressed amazement at how much better he felt. 2 years later he is doing well, euthyroid and normal sodium on daily synthetic thyroid supplementation. Key points from this patient:
1. Even though this patient most likely had ADH release secondary to his empyema, going through the evaluation compulsively allowed us to diagnose hypothyroidism.
2. Because we focused all of our attention on his empyema, we missed the opportunity to make a clinical diagnosis of hypothyroidism. This happens often in medicine – we focus on the most life threatening problem, and miss a second problem.

Some additional key teaching points in hyponatremia
1. Who with hyponatremia deserves aggressive (3% saline) treatment? a. Patient with acute hyponatremia and significant neurologic symptoms, especially seizures.
2. How fast should we correct hyponatremia? a. ~1 mEq/hour when treating seizures until seizures stop and/or sodium reaches 125 me/L b. Otherwise 0.3-0.5 mEq/hr (faster rates put patients at risk for central pontine myelinolysis) –
highest risk are patients with chronic hyponatremia, especially alcoholics and those who are malnourished
3. Does urine sodium help? a. If you are having difficulty deciding whether the patient has volume contraction, then a low urine
sodium gives supporting evidence for volume contraction 4. How do we treat SIADH?
a. Acutely we try water restriction. This is difficult and not always successful. b. We have a new expensive medication – conivaptan (Vaprisol) which is an ADH inhibitor– which
we can use IV to create a nephrogenic diabetes insipidus. I would reserve that medication for severe, difficult to treat hyponatremia secondary to SIADH. Currently, it does not have an indication in CHF or cirrhosis, but we may see these indications in the future.
c. Chronically, we can use democlocycline which also causes a nephrogenic diabetes insipidus. This allows the patient to liberalize their water intake.
d. In the near future we will probably use tolvaptan – an oral ADH antagonist. A recent NEJM study - Schrier RW, Gross P, Gheorghiade M, et al. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N Engl J Med 2006;355:2099-2112 – describes a study of this drugs effectiveness both in SIADH and in edematous states (CHF and cirrhosis). I suspect this drug will receive FDA approval sometime in 2007.

Thoughts on metabolic acidosis The most common diagnostic acid-base problems include metabolic acidosis. The steps that I use:
1. Check the electrolyte panel and the arterial blood gas 2. Calculate the anion gap 3. Calculate the delta gap 4. Check the respiratory compensation
The steps in normal gap acidosis
1. Determine whether the patient has a buffering problem or bicarbonate loss. 2. Consider the urine anion gap
Teaching points on normal gap acidosis
The measured cations and anions in the urine are Na+, K+, and Cl- ; thus the urine anion gap is equal to: Urine anion gap = [Na ] + [K ] - [+ + Cl-] Urine anion gap = unmeasured cations – unmeasured anions
In normal subjects, the urine anion gap is usually near zero or is positive. In metabolic acidosis, the excretion of the NH4
+ (which is excreted with Cl-) should increase markedly if renal acidification is intact. Because of the rise in urinary Cl-, the urine anion gap which is also called the urinary net charge becomes negative, ranging from -20 to more than -50 meq/L. The negative value occurs because the Cl- concentration now exceeds the sum total of Na+ and K+.
In contrast, if there is impairment in kidney function resulting in an inability to increase ammonium excretion (i.e. Renal Tubular Acidosis), then Cl- ions will not be increased in the urine and the urine anion gap will not be affected and will be positive or zero.
In a patient with a hyperchloremic metabolic acidosis: A negative UAG suggests GI loss of bicarbonate (e.g. diarrhea), a positive UAG suggests impaired renal acidification (i.e. renal tubular acidosis).
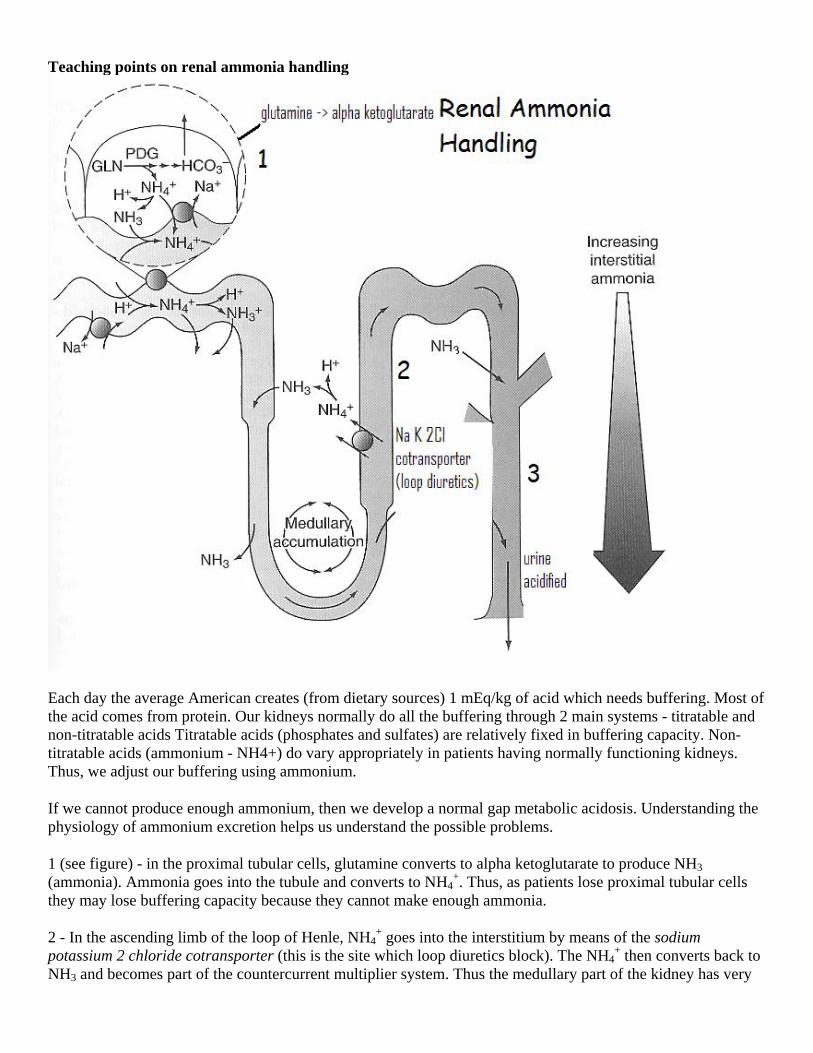
Teaching points on renal ammonia handling
Each day the average American creates (from dietary sources) 1 mEq/kg of acid which needs buffering. Most of the acid comes from protein. Our kidneys normally do all the buffering through 2 main systems - titratable and non-titratable acids Titratable acids (phosphates and sulfates) are relatively fixed in buffering capacity. Non-titratable acids (ammonium - NH4+) do vary appropriately in patients having normally functioning kidneys. Thus, we adjust our buffering using ammonium.
If we cannot produce enough ammonium, then we develop a normal gap metabolic acidosis. Understanding the physiology of ammonium excretion helps us understand the possible problems.
1 (see figure) - in the proximal tubular cells, glutamine converts to alpha ketoglutarate to produce NH3 (ammonia). Ammonia goes into the tubule and converts to NH4
+. Thus, as patients lose proximal tubular cells they may lose buffering capacity because they cannot make enough ammonia.
2 - In the ascending limb of the loop of Henle, NH4+ goes into the interstitium by means of the sodium
potassium 2 chloride cotransporter (this is the site which loop diuretics block). The NH4+ then converts back to
NH3 and becomes part of the countercurrent multiplier system. Thus the medullary part of the kidney has very
high concentrations of NH3. In the distal tubule, we acidify the urine. Here NH3 diffuses into the distal tubule, converts back to NH4
+, creating the desired buffer effect.
Renal acidosis (normal gap) can occur for 3 major reasons.
1. Distal RTA - inability to acidify the urine - cannot excrete the ingested acid if we cannot make mEq of NH4+
(which requires acid urine)
2. Type IV RTA - this one is interesting. The problem in type IV RTA is primarily hyperkalemia (most commonly called hyporenin/hypoaldo). Increased potassium levels inhibit the enzyme glutaminase which is responsible for the production of ammonia (see 1 in the figure). Thus if we correct the hyperkalemia, we usually resolve the acidosis.
3. The acidosis of CKD - two problems for these patients - decreased production of ammonia and decreased concentration in the medulla. As CKD worsens, the countercurrent mechanism does not function as efficiently, decreasing the concentrations of solutes in the medulla. Thus, less ammonia is available to enter the distal tubule for buffering.

Teaching points about increased anion gap acidosis This case discussion highlights my favorite teaching points on increased anion gap acidosis:
Presentation:
A 42-year-old white man comes to the ER after a motor vehicle accident in which he was ejected from his car into a lake. He is confused and only remembers trying to swim. The emergency medical technician (EMT) reports nausea, vomiting, and agitation.
PE:
VS: T 98, BP 169/78, RR 24, SaO2, 100% RA GEN: Thin, barrel-chested man in acute distress. He is flushed, diaphoretic, and tachypneic, demonstrating Kussmaul respirations and accessory muscle use. Breath has a sweet odor. HEENT: Pupils equal, round, and reactive. Extraocular muscles intact. Anicteric. CV: Regular rate and rhythm, no murmurs, rubs, or gallops. PULM: Clear to auscultation bilaterally. ABD: Scaphoid. Soft. Good bowel sounds. 4-cm laceration across right midclavicular line. EXT: Bruise on right shin.
Labs are as follows:
• Electrolyte panel: sodium 140, potassium 4.6, chloride 102, bicarbonate 5, BUN 7, creatinine 1.2, glucose 118
• ABG: pH 7.06; pO2 130; pCO2 8; calculated HCO3 2
His trauma evaluation and x-rays are entirely unremarkable.
The Problem
Define the acid-base disorder and develop a differential diagnosis.
What additional tests would you order?

Solution:
The patient has an increased anion gap acidosis.
Calculations:
1. Anion gap = 33
2. Delta gap calculation = (observed gap - expected gap) + observed bicarbonate = (33 - 12) + 5 = 26.
Thus, the patient started out with a normal bicarbonate (this excludes an underlying metabolic acidosis or alkalosis).
3. Winter's equation = 1.5 (calculated bicarbonate) + 8 (+ or -) 2 [expected pCO2] = 1.5 (2) + 8 = 11.
This suggests that the hyperventilation is appropriate for the degree of metabolic acidosis.
We use the mnemonic KILU for remembering the differential of anion gap acidosis:
Ketoacidoses (diabetic, alcoholic, starvation)
Ingestions (salicylates, ethylene glycol, methanol – and, less commonly, iron and isoniazid)
Lactic acidosis (hypoperfusion, tumors, medications or d-lactic acidosis)
Uremia
Anion gaps > 25 occur primarily with diabetic ketoacidosis, lactic acidosis, ethylene glycol, and methanol.
In consideration of the stable vital signs and normal blood sugar, the physicians appropriately considered an ingestion. They ordered a serum osmolality.
Lab values:
Serum osmolality = 395
Calculated osmolality = 289
Thus, osmolal gap = 96
This supports a likely ingestion with either ethylene glycol or methanol.
Brief bibiography 1. Adrogue HJ, Madias NE. Hyponatremia. NEJM 2000;342:1581-1589. Classic review article on hyponatremia 2. Milionis HJ, Liamis GL, Elisaf MS. The hyponatremic patient: a systematic approach to laboratory
diagnosis. CMAJ 2002;166:1056-62. Useful summary of evaluating hyponatremic patients 3. Gabow PA, Kaehny WD, Fennessey PV, et al. Diagnostic Importance of an Increased Serum Anion Gap.
NEJM 1980;303:854-8. Gives information on how the size of the anion gap matters 4. Oh MS, Carroll HJ. Current Concepts – The Anion Gap. NEJM 1977; 297:814-817. Old, but still relevant article on the anion gap 5. Batlle DC, Hizon M, Cohen E, et al. The Use of Urinary Anion Gap in the Diagnosis of Hyperchloremic
Metabolic Acidosis. NEJM 1988;318:594-599. Explains the urine anion gap concept 6. Orringer CE, Eustace JC, Wunsch CD, et al. Natural History of Lactic Acidosis After Grand-Mal Seizures.
A Model for the Study of an Anion-Gap Acidosis Not Associated with Hyperkalemia. NEJM 1977;297:796-799.
Explains a common cause of transient lactic acidosis 7. Albert MS, Dell RB, Winters RW. Quantitative Displacement of Acid-Base Equilibrium in Metabolic
Acidosis. Ann Intern Med 1967;66:312-322. The original Winter’s equation publication

Additional discussion of acid-base electrolyte cases (blog and Medscape) http://medrants.com/index.php/archives/3095 An iatrogenic cause of increased anion gap acidosis http://medrants.com/index.php/archives/3084 and http://medrants.com/index.php/archives/3085 These two entries discuss an unusual normal gap acidosis http://www.medscape.com/index/section_2682_0 My interesting cases section on Medscape The following cases have acid-base electrolyte issues: A 42-Year-Old Man With HIV An Ileal Bypass Patient With Watery Diarrhea A 60-Year-Old Woman With New Seizures A 58-Year-Old Disoriented, Schizophrenic Man A 41-Year-Old Woman With Back Pain A 47-Year-Old Man With Empyema and Hyponatremia A Disoriented, Nauseated Car-Wreck Victim Many of these cases are included in the PowerPoint slides. These links give more complete discussions of the solutions.
Acid Base and Electrolyte Problems 2007
Robert M. Centor, MD Professor and Director, Division of GIM
Assoc Dean, HRMCUniversity of Alabama at Birmingham

Importance of the topicDawson-Saunders B, Feltovich PJ, Coulson RI, Steward DE. A survey of medical school teachers to identify basic biomedical concepts medical students should understand. Acad Med 1990 Jul;65(7):448-54Acid-base electrolyte balance ranked #1 in importance (of 27 biomedical concepts). Serum sodium osmolarity and controls ranked 7.5. Acid-base ranked #1 in clinical difficulty, while serum sodium ranked #7 in clinical difficulty.
Some teaching thoughts
Focus on a physiologic approachUse of actual cases and a Socratic method (cause mild anxiety)Discourage pattern recognitionEncourage a repeatable systematic approachRepetition, repetition, repetition

Goals of the workshop
1. Develop a systematic approach to diagnosing hyponatremia
2. Develop a systematic approach to diagnosing metabolic acidosis
3. Have a systematic process for analyzing complex acid base problems

Case # 1
A 47 year old man presents with an empyema, weakness and low serum sodium.Patient presents with progressive dyspnea of 10 days duration. He had mild low extremity swelling. He had right sided pleuritic chest pain and a chronic cough Chest x- ray revealed pneumonia with pleural effusion. Thoracentesis showed an empyema which required a chest tube.

Laboratory – Case #1
116 81 10
4.1 26 0.6 92
Stepwise approach to hyponatremia
Look for pseudohyponatremia
If patient has true hyponatremia
Check volume statusIf euvolemic check urine osms

Pseudohyponatremia
Endogenous HyperglycemiaHypertriglyceridemiaParaproteinemia
Exogenous (iatrogenic)IV MannitolGlycine (TURP)
Volume Status
Volume contraction – ADH stimulated
Edematous states – effective intravascular volume depletion > ADH stimulated
Euvolemic patients
Euvolemic Patients
Dilute urine (urine osms < 100) Psychogenic polydipsiaBeer drinker’s potomaniaTea & Toast Diet
Urine osms inappropriately elevated (> 150) – first exclude
Chronic kidney disease Addison’s disease Hypothyroidism Thiazide diuretics

Urine mOsm elevated and 4 conditions excluded
Physiological stimulation of ADH (think post-op)Nausea Vomiting Pain Narcotics
Transient causes of increased ADH Pulmonary processes Intracranial processes Medications (especially SSRI’s)
If all above absent consider possibility of chronic SIADH
Solution Case #1
Serum osms = 234 - confirms true hyponatremia
Exam was consistent with euvolemia
Urine osms 332 kg
Screening for thyroid and cortisolTSH = 27, free T4 <0.023, free T3 = 1.16Cortisol – normal
Solution Case #1
Solution – the laboratory data confirmed the diagnosis of hypothyroidism
On repeat focused examination the patient admitted to a marked decrease in energy level for 5 years, his antecubital fossa revealed dry course skin
The patient had sluggish reflexes
Hyponatremia Case #2
A 70 year old man with non small cell lung cancer presents with fatigue and dizziness for one monthA 5-10 lb weight loss and anorexia
Wife states that he is forgetfulBP – 95/47 (but neither orthostasis or tachycardia)
No peripheral edema

Laboratory Data
115 83 28
6.1 20 1.4 72
Solution in Case #2
Serum Osm 243 – confirms true hyponatremia
Physical examination – consistent with euvolemia
Urine Osm 343

Solution #2 continued….
TSH level normal
ACTH stimulation test – low cortisol level (3.1 with no response to ACTH stimulation)
Abdominal CT Scan revealed bilateral adrenal metastasis.
Hyponatremia Case #3
Known paranoid schizophrenia and major depressive disorder, presents to ER after having seizure at home
Patient has another witnessed seizure in the ER
She provides no history but her sisters state that she seems to have been drinking water excessively all day

Laboratory Data
116 80 7
3.9 15 0.4177
Medications AtivanNexiumGeodonZoloft
Physical Examination – unremarkable
Solution to Hyponatremia Case #3
The patient’s seizures are likely due to sudden onset hyponatremia
When hyponatremia presents with seizures, they need rapid correction to a goal sodium of 125 and a reversal of neurological abnormalities.
Solution to Case #3 continued..
Where as we usually recommend slow increases in sodium for hyponatremia (0.3-0.5 mEq/hr)
Rapid correction can go as fast as 1 to 1.5 mEq/hr until goal sodium and end of seizures
We treated this patient with hypertonic (3%) saline at a rate of 42cc/hr

Diagnosis
We ruled out pseudohyponatremia which we did not expect since the patient was symptomatic
We established that she had normal volume status and sent off a screening test for hypothyroidism and adrenal insufficiency
Both of those were found to normal
We obtained urine osmolality which was 407 mOsm/kg

Probable explanation
Medication induced SIADH probably secondary to her antidepressant which was an SSRI. This probably caused a chronic SIADH which was exacerbated by acute psychogenic polydipsia causing a rapid decrease in sodium Note that the patient has an increased anion gap of 21 likely secondary to the seizure caused by the hyponatremia Her anion gap returned to normal within 2 hours consistent with a transient lactic acidosis
Complex Acid Base Problems

Complex Acid Base Case #1
52 yo man with h/o PVD (s/p aortofembypass), hep C and infected sacral decubitus ulcerAdmitted to ICU with hypotension, weakness and acute renal failureTransferred to ward 2 days later
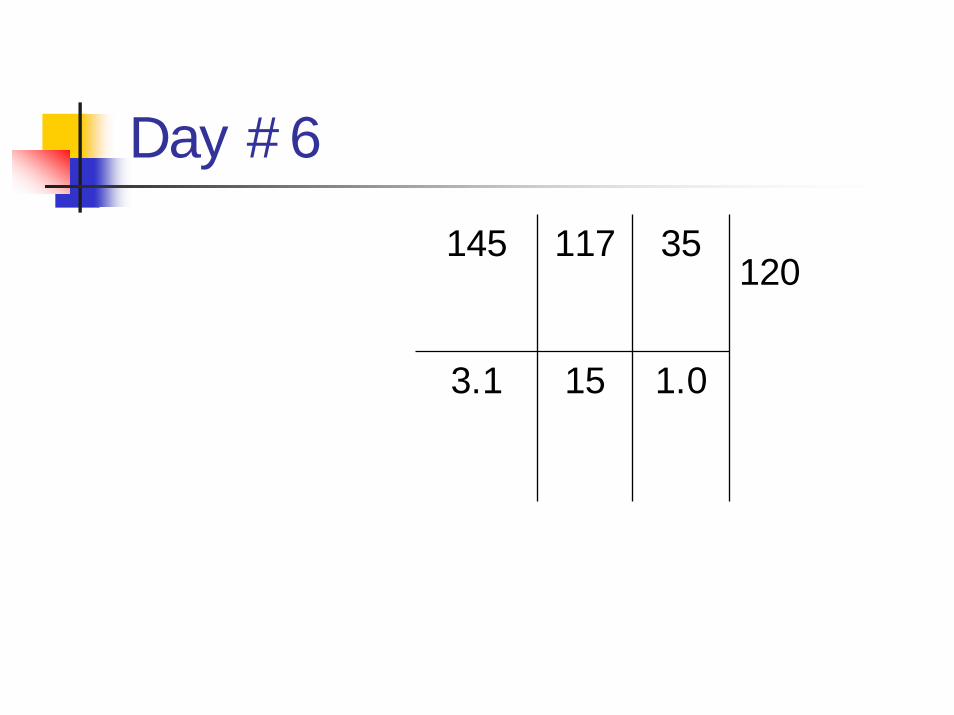
Day #6
145 117 35
3.1 15 1.0
120
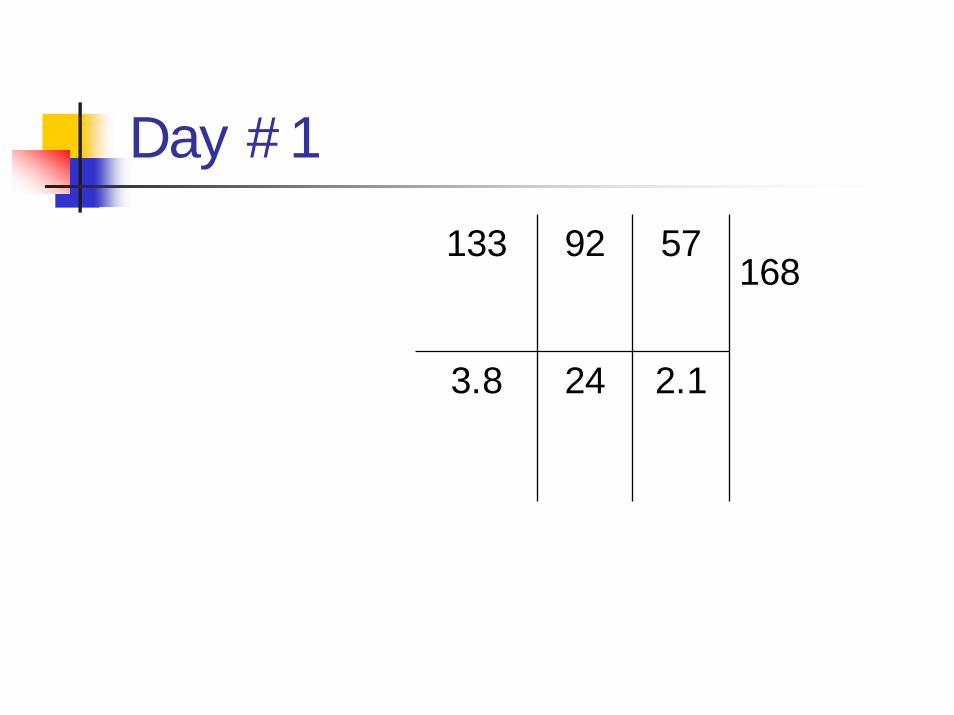
Day #1
133 92 57
3.8 24 2.1
168

Why a bicarb of 15?

Adding a blood gas
pH 7.43 145 117 35
pC02 20 3.1 15 1.0
pO2 59
Urine Na 65, Urine K 70, Urine Cl 116
120

Clinical outcome
We confirmed CHF secondary to overly aggressive IV fluidsPatient weighed 40 kg and was receiving 100 cc NS/ hrBNP was markedly elevatedPatient spontaneously diuresed and recovered from this acute insult

Complex Acid Base Case #2
42 yo man, known HIV infection admitted with headache and fever
Cryptococcal meningitis diagnosed, patient started on amphotericin B and 5-FC
One week later he is found confused during rounds
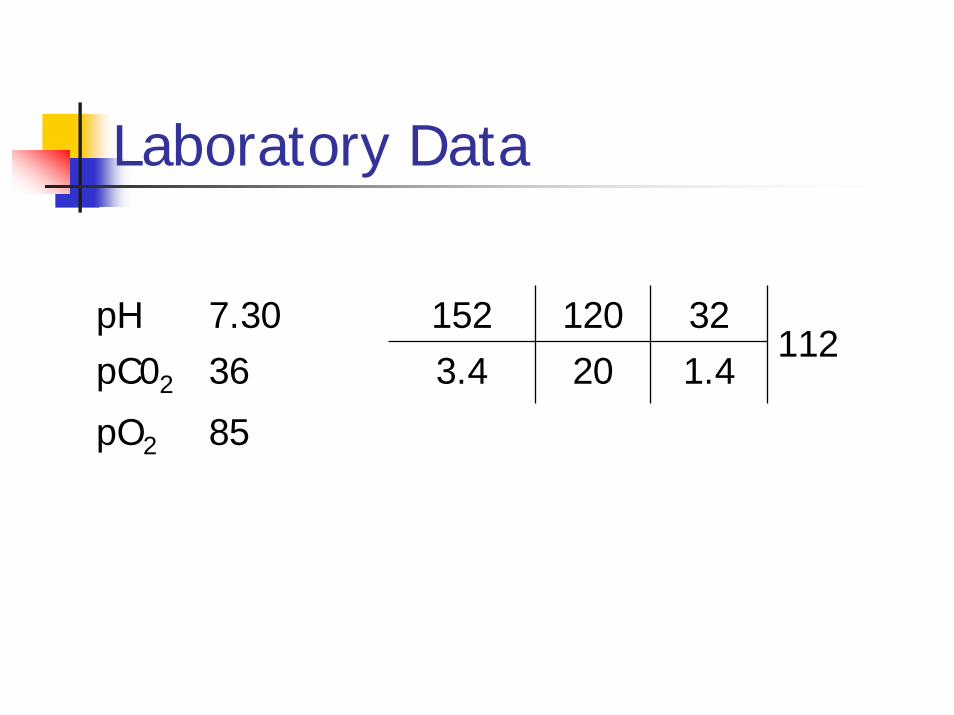
Laboratory Data
pH 7.30 152 120 32pC02 36 3.4 20 1.4
pO2 85
112

Additional Laboratory Data
Plasma osm - 315Urine osm - 150Urine NA - 25Urine K - 45Urine Cl – 38Urine pH – 6.2

Note dilute urine despite hypernatremia
This suggests strongly the diagnosis of central diabetes insipidus
The patient did respond to exogenous ADH with increased urine concentration
Hypernatremia

Normal gap Acidosis
The patient has a normal gap Acidosis

Bicarbonate wasting
Proximal RTAAcetazolamide
Diarrhea

Incomplete buffering
Chronic renal insufficiency
Type IV RTA
Distal RTA
Urine-bowel connections

Solution CAB #2
Urine Anion gap = 25 + 45 – 38 = 32
This is a positive value consistent with a very low urine ammonium
This tells us that we have a buffering problem
Further review of his laboratory data shows a relatively alkaline urine despite a significant normal gap metabolic acidosis
This supports a diagnosis of distal RTA
Amphotericin B is known to cause a distal RTA
Complex Acid-Base Case # 3
A 42yo white male comes to the ER after a motor vehicle accident
He was ejected into the lake. He is found confused and only remembers trying to swim
The EMT reports nausea, vomiting and agitation.
The patient is flushed, diaphoretic, tachypneic, and has Kussmaul respirations

Laboratory Data
pH 7.06 140 102 7
pC02 8 4.6 5 1.2
pO2 130
118

Solution CAB #3
Anion gap = 33
Delta gap (observed gap minus expected gap plus observed bicarbonate) = 33 – 12 + 5 = 26 (patient started with a normal bicarbonate)
Winter’s equation (1.5 times calculated bicarbonate plus 8 plus or minus 2 equals expected pCO2)

Differential Diagnosis of elevated anion gap metabolic acidosis
KetoacidosisIngestions Lactic acidosis Uremia

Further Laboratory Data
Serum Osmolality - 395 Calculated Osmolality – 289Osmolal gap – 96 Urinalysis – showed calcium oxalate crystals This makes the diagnosis of ethylene glycol toxicity
Complex Acid-Base Case #4
50 yo female presents with watery diarrhea She has a history of ileal bypass for morbid obesity She has 10-15 watery stools of high volume each day Patient’s intern gives her a high dose of narcotics to decrease the diarrhea
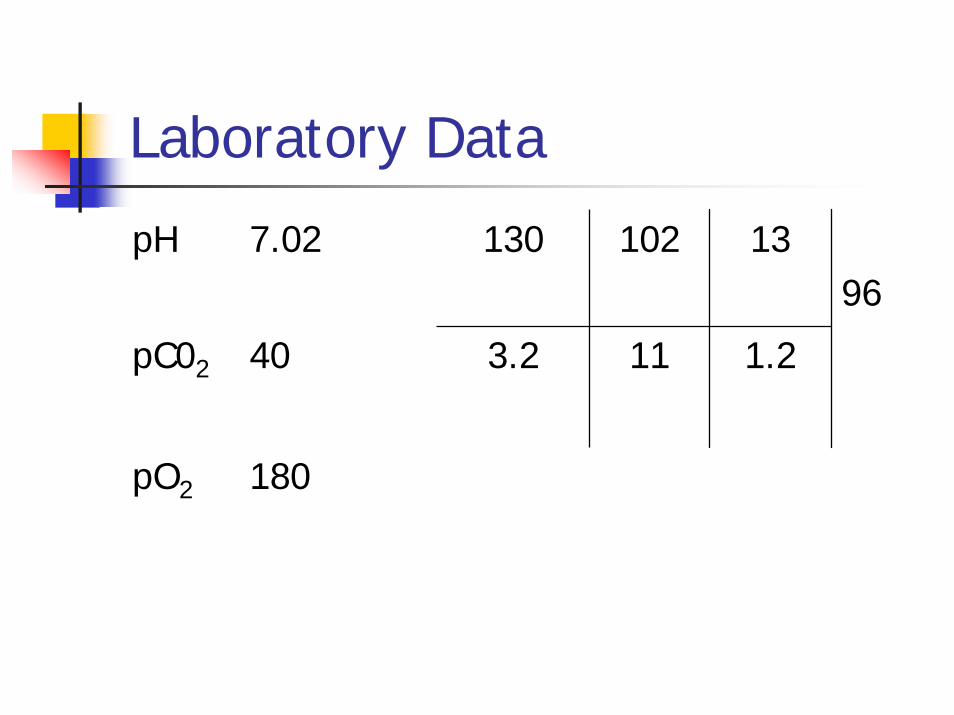
Laboratory Data
pH 7.02 130 102 13
pC02 40 3.2 11 1.2
pO2 180
96
Solution CAB #4
Anion gap = 18 Delta gap calculation (18 - 12 + 10 = 16)This confirms an underlying normal gap acidosis
Winter’s Equation – expected pCO2 = 14.5 This suggests hypoventilation inappropriate for the degree of metabolic acidosis
Thus this patient represents the rare triple acidosis – an increased Anion gap Acidosis, a Normal gap metabolic acidosis and a respiratory acidosis
CAB #5
83 yo man brought from his nursing home for nausea and vomiting for 5 days. He has a history of esophageal dysmotility, but this episode is dramatically different.PMH includes a previous stroke and neurogenic bladder which requires an indwelling catheter
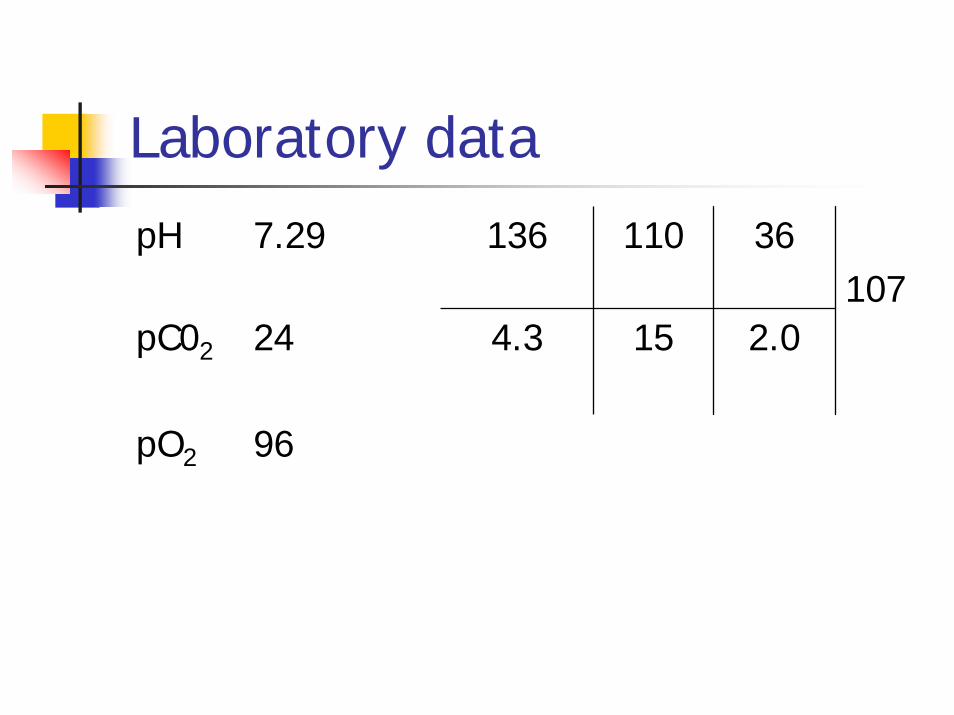
Laboratory datapH 7.29 136 110 36
pC02 24 4.3 15 2.0
pO2 96
107
Unexpected labs
Given 5 days of nausea and vomiting we expected to find a hypokalemic metabolic alkalosisHe additionally had a poorly draining indwelling catheter with mild obstructionHis previous electrolyte panels had no evidence of significant CKD or acid base disorderWe obtained additional labs:

Additional labs
Urine pH = 6.5Urine chemistries
Na 71K 28Cl 73

Postulation CAB #5
The high urine pH in the face of a normal gap metabolic acidosis makes the diagnosis of a distal RTAWe suspected that his distal RTA occurred secondary to his obstructive uropathyHowever, that distal RTA usually has hyperkalemiaWe suspect that his vomiting prevented the expected hyperkalemia

Resolution
He responded appropriately to bicarbonate repletion with correction of his acidosisHis renal function also returned to baseline (creat 1.4)We discharged him on Shohl’s solution

CAB #6
A 58 YO schizophrenic male was brought to the hospital because of strange behavior.
Laboratory data:
pH 7.49 139 90 18
pC02 15 4.7 14 1.0
pO2 169 on 2 liters
100
Summary of Concepts
Systemic approach to diagnosing cause of hyponatremia
Steps need for complex acid base casesAnion gapDelta gapWinter’s equation