TC's emergency medicine wrap up 4
48
TC’S POTPOURRI THE MEME EDITION
-
Upload
scgh-ed-cme -
Category
Health & Medicine
-
view
221 -
download
1
Transcript of TC's emergency medicine wrap up 4

TC ’ S P O T P O U R R ITHE M E ME ED I T I ON

W H AT I S A M E M E ?

F E A ST ST U DY
• I’ve mentioned it before• Essentially found shocked
septic kids in Africa did worse with fluid boluses over maintenance fluid
• Comment from the floor was “yeah but they’ll all have malaria and the fluid will make their cerebral oedema worse”
• Fair enough

SH UT U P F E R G I E
• The non-anaemic and non-malaria patients were analysed
• Found to have the same poor outcomes with fluid boluses over maintenance fluids as the anaemia and malaria kids
• Regardless of whether albumin or crystalloids given



SG A R BO S S A C R I T E R I A
• Smith modified Sgarbossa rule:
• At least one lead with concordant STE (Sgarbossa criterion 1) or
• At least one lead of V1-V3 with concordant ST depression (Sgarbossa criterion 2) or
• Proportionally excessively discordant ST elevation in V1-V4, as defined by an ST/S ratio of equal to or more than 0.20 and at least 2 mm of STE. (this replaces Sgarbossa criterion 3 which uses an absolute of 5mm)


SE V E R E C U TA N E O U S A DV E R SE R E AC T I O N S• Drug hypersensitivity syndrome is the same as DRESS
• SJS/TEN
• Acute generalised exanthematous pustulosis (AGEP)
• drug induced erythroderma
• Severe, unexpected reaction to a medicine(s)
• high fever, a morbilliform skin rash
• inflammation of one or more internal organs including the liver, kidneys, lungs and/or heart
• It generally starts two to eight weeks after taking the responsible medicine.

C U L PR I T S
• Allopurinol
• AEDs esp. carbamazepine, phenobarbitol, phenytoin
• Sulfonamides
• But really anything


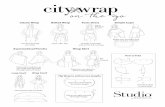
M E A C U L PA




wire left in
Individual Factors
Patient Factors
Task Factors
Education and
Training
Team and
Social Factors
Working Condition
s
Equipment and
resourcesCommunication
Organisational and
strategic Factors



CH O I CE S RANK RATE18 G I VC 8 . 5F R R I C 00 : 46
6F R SH EATH 7F R R I C 1 : 008 . 5F R R I C 8 . 5F R S HE ATH 1 : 05
14G LU MEN CVC 14G I VC 1 : 307F R R I C 6F R S HE ATH 2 : 1016 G I VC 14G 13 .3 CM I VC 2 : 1020 G I VC 16G I VC 2 : 2014 G I VC 18G I VC 4 : 23
8 . 5F R SH EATH 14 G LU MEN CVC 5 : 2014G 13 .3 CM I VC 20G I VC 6 : 47

C O U N T RY W E E K
• 13yo playing football, someone stepped on his foot while trying to spin round
• pain


T I LL A U X F RAC T U R E
• Salter Harris III distal tibia epiphysis
• Caused by an avulsion of the anterior inferior tibiofibular ligament
• Mechanism of injury is thought to be due to an external rotation force
• 12-14yo
• A period of time exists when the lateral physis is the only portion not fused
• An additional fracture in the posterior distal tibial metaphysis in the coronal plane would result in a…?


BA R BA RA
• 70yo lady
• sore right knee
• normal XR with GP
• moderate effusion, ROM ~70º
• No PMHx

P L A N ?


WH AT A RE YOU LOO K I NG FOR I N T HE SYN OV I AL FLU I D?




C O U R S E
• D/C with NSAIDS and Dx with pseudogout
• Recalled 2 days later after bacteria grown
• Sent home by ED as patient feeling ok
• No bloods done
• Back 5 days after initial presentation with obvious septic joint



• Unwitnessed arrest
• Initial non-VF Rhythm
• Lack of bystander CPR
• >30 min to ROSC
• >30 min of CPR
• Evidence of unresponsive hypoperfusion and microcirculatory failure:
• pH <7.2 and Lactate >7
• Age >85
• End-Stage Renal Disease (ESRD
• Non-Cardiac Causes: Cardiac arrest due to drugs, drowning, acute stroke, terminal cancer and trauma, just to name a few non-cardiac causes, are likely to result in poor outcomes post-resuscitation.
Unfavourable for Cath



AVO I D
• All STEMI criteria patients
• excluded if sats <94%
• There was an increase in the rate of recurrent myocardial infarction in the oxygen group compared with the no oxygen group (5.5% versus 0.9%; P=0.006)
• An increase in frequency of cardiac arrhythmia (40.4% versus 31.4%; P=0.05).
• At 6 months, the oxygen group had an increase in myocardial infarct size on cardiac magnetic resonance (n=139; 20.3 versus 13.1 g; P=0.04).


PLU G F O R A C H A R I TY
• I’ve belonged for ~5years
• “Medics Beyond Medicine”
• For doctors who want to connect with people with mental and physical disabilities rather than just see them in a clinical setting
• Generally revolves around outings
• Recently featured on channel 9 news



• Emma and Dave volunteered their time
• “Daniel” here has myotonic dystrophy as seen by the tell tale baldness pattern
• “Chris” has a rare chromosomal abnormality that means he has a compulsion to wear a cap in an inappropriate setting

AG E A D J US T E D D - D I M E R
• Wells score ≤4
• Age ✷ D-dimer (0.01mg/L)
• ie a 70yo will have an acceptable D-dimer <0.7mg/L
• Validated in multiple studies
• I think we should use it

C E N TO R• History of fever• Tonsillar exudates• Tender anterior cervical adenopathy• Absence of cough• The Modified Centor Criteria add the patient's age to
the criteria• Age <15 add 1 point• Age >44 subtract 1 point• -1, 0 or 1 points - No antibiotic or throat culture
necessary (Risk of strep. infection <10%)• 2 or 3 points - Should receive a throat culture and treat
with an antibiotic if culture is positive (Risk of strep. infection 32% if 3 criteria, 15% if 2)
• 4 or 5 points - Treat empirically with an antibiotic (Risk of strep. infection 56%)
• The presence of all four variables indicates a 40 - 60% positive predictive value for a culture of the throat to test positive for Group A Streptococcus bacteria. The absence of all four variables indicates a negative predictive value of greater than 80%

W H AT A N T I B I O T I C
• Phenoxymethylpenicllin
• Cheap, proven
• Never been a resistant GABHS to penicillin
• Good anaerobic cover just in case the patient has…


F U S O B AC T E R I U M N E C R O P H O NU M
• lemierre’s syndrome
• Thrombus of the internal jugular
• Sepsis
• Mortality of ~5%
• Not sensitive to macrolides