
Técnicas microbiológicas rápidas para dirigir el ...©cnicas microbiológicas rápidas para...
47
1 Técnicas microbiológicas rápidas para dirigir el antibiótico empírico precozmente Patricia Muñoz, MD. Ph.D. Microbiología Clínica-Enf. Infecciosas Hospital General Universitario Gregorio Marañón Universidad Complutense of Madrid. Spain Jueves. NOV 10, 2011 19:15 - 19:35 h
Transcript of Técnicas microbiológicas rápidas para dirigir el ...©cnicas microbiológicas rápidas para...

1
Técnicas microbiológicas rápidas para dirigir el antibiótico empírico precozmente
Patricia Muñoz, MD. Ph.D.
Microbiología Clínica-Enf. Infecciosas
Hospital General Universitario Gregorio Marañón Universidad Complutense of Madrid. Spain
Jueves. NOV 10, 2011 19:15 - 19:35 h

2
Presentation and Disclaimer
Presentation Clinical Microbiology and Infectious Diseases
how molecular methods are used today in sepsis management
Disclaimer Advisory boards and Conference honoraria: Pfizer, MSD,
Novartis, Astellas, Biomerieux Research funds: Novartis, Astellas

3
Molecular methods (MS) in the Diagnosis of Sepsis
I. Sepsis challenges
II. Role of MM in blood samples
III. Role of MM in positive blood cultures
IV. Role of MM in other samples

4
I. Is diagnosis of sepsis still challenging?

Evolution of significant BSI episodes/1000 admissions H. General Universitario Gregorio Marañón
1615,3
16,417,3
21
23,1
21,422,8 23,3
21,8
26,427,9
25,7 25,9 25,726,8 26,7
29,4 29,4
26,8
28,5
31,2
32,8 3334,1
29,8
0
5
10
15
20
25
30
35
40
85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10
Gentileza de Dra. Marta Rodríguez-Creixéms
Total number BSI episodes: 35,161
28,414 patients

10
7,76,8
13 12,8
11,6
9,7 9,58,5 8,5
12,511,5
10,9
12,611,711,6
13
10,5
12,711,8
8,59,5 9,3
8
10,4
12,4
0
15
85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10
Gentileza de Dra. Rodriguez Créixems
% polymicrobial BSI episodes

7
Microorganism Nº BC Median IQR*
Gram (-) 1,089 8.8 h 4.3 – 15.5
Gram (+) 1,114 11.02 h 6.2 – 17.2
Anaerobes 67 27.8 h 17.7-56.4
Candida sp 88 33.3 h 19.9-47.4
Time to growth of different microorganisms
Gentileza de Dra. Marta Rodríguez-Creixéms

8
CHALLENGE FOR MM
We know that
>30% empiric Abs are incorrect
Mortality 7.6% > /hr delay after hypotension
We do not want to answer the question
Did the physician choose the correct empiric therapy?
We want to answer the question
Which antimicrobial agent is best for treating this patient ‘s infection now?
Tenover FC. Ann NY Acad Sci 2010

9
Challenges for MM
1. Is this sepsis?
2. Is it caused by a resistant pathogen?
3. Which pathogen?
4. Are there any complications?
Dickermann Am Heart J 2007; Bouza E CID 2004:39;

10
IS THIS SEPSIS? Can MM help in the empirical phase of sepsis management?
11
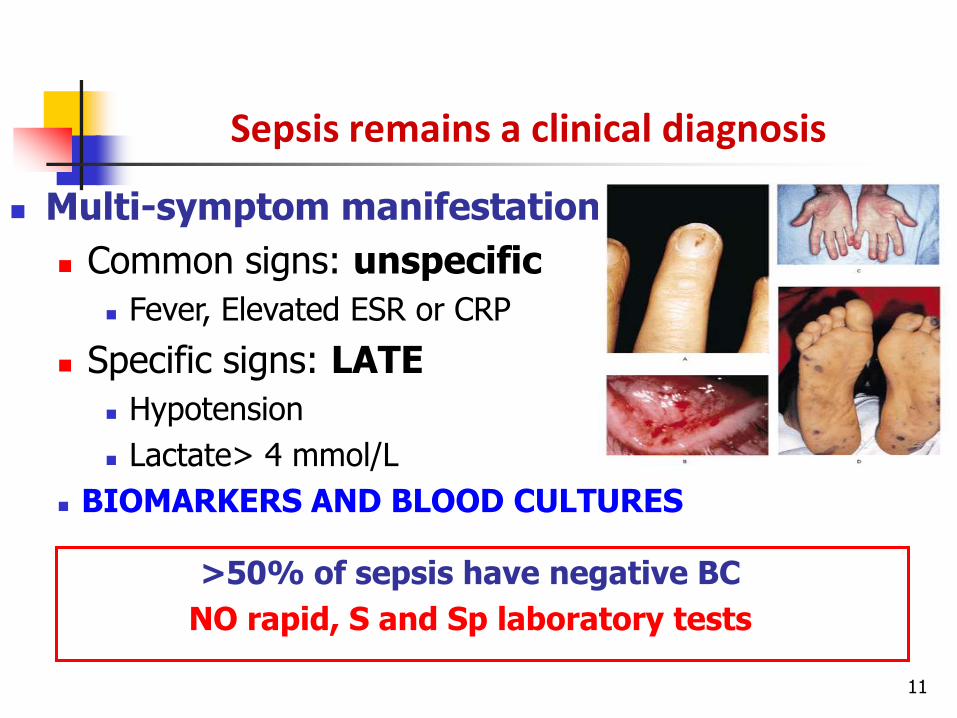
Sepsis remains a clinical diagnosis
Multi-symptom manifestation
Common signs: unspecific
Fever, Elevated ESR or CRP
Specific signs: LATE
Hypotension
Lactate> 4 mmol/L
BIOMARKERS AND BLOOD CULTURES
>50% of sepsis have negative BC
NO rapid, S and Sp laboratory tests

Blood cultures usually the base of Dx
PROS
Available in most laboratories
Efficacious and well-known technology
Etiology and susceptibility
Strains storage
Cheap
CONS
30-50% of negative BC
Diagnosis delay may increase mortality

Blood cultures
<50% of the etiological diagnosis of sepsis
+3-4d
Identification and susceptibility
+ 2d
Culture and preliminary data
Bouza, Sousa et al. (2004). CID 39:1170-3
~7h-5d
BC + Gram stain
G- 8.8h ; G+ 11 h

Molecular methods
Different microorganisms Resistance genes Fastidious microorganisms
PCR
Typing
Identification
Resistance genes
Rapid identification Resistance genes
Commercial or in-house methods Pathogen specific, Broad range , Multiplex Different post PCR detection methods
Universal PCR + sequencing
Specific PCRs
Dr. Marin

Molecular methods: blood samples
PCR
Septifast® (Roche)
SepsiTest® (Molzym)
VYOO® (Sirslab)
BlacKLight Sepsis® (Blackbio)
Plex-ID® (Abbott)
Low concentration of microbial DNA High concentration of inhibitors Do not detect fastidious m.s. Detect DNAemia (contaminating?)
Limited susceptibility information No storage of strains
Contamination risk Laborious. Trained personnel Special equipment. Expensive
Rapid results Theoretical high sensitivity Multiple + difficult pathogens Diagnosis in treated patients
PROS
CONS
Dr. Marin

16
Some clinical experience with Septifast 23 microorganisms
Patients n +BC +PCR Combined Concordance % pts significant
improved Dx
Mancini N1 Neutropenic 34 20.4% 33% 34% 83% 5.8%
Varani S3 Neutropenic 100 29.2% 21.5% 33.8% 79.2% 4.6%
Louie RF7 General 200 18.5% 22.5% 30% 88.5% 25%
Westh H8 General 359 17% 26% 31.5% 79% 16.7%
Maubon D9 Malignancy 110 29% 25.4% 30% 70% 10%
Avolio M10 ER 144 29.9% 27.8% 37% 56.6% NR
Dierkes C11 General 101 21% 27.4% 35% 77% 8%
Lehman LE12 General 436 21.2% 28% 36.4% 58.2% 29%
Wallet F 13 ICU 72 10% 15% 21% 83.3% 5.5%
Lamoth F14 Neutropenic 86 25% 25% 43% 65% 37%
Tsalik EL15 General ER 306 25% 17.3% 34.2% 82.6% NR
Lilienfeld16 Neutropenic 70 28.5% 21% 38.6% 71% NR
1.JCM 09; 2 Steinmann J. TID 09; 3 J Infect 09; 4. Mussap M. J Chemother 07; 5. Paolucci M. J Med Microb 09; 6. Vince A. J Med Microb 08; 7. CCM 08. 8. JCM 09; 9. J Infect 10. 11. BMC Infect Dis 09; 12. CCM 09; 13. CMI 09. 14. JCM 10; 15. JCM 10; 16. von Lilienfeld-Toal M. JCM 2009
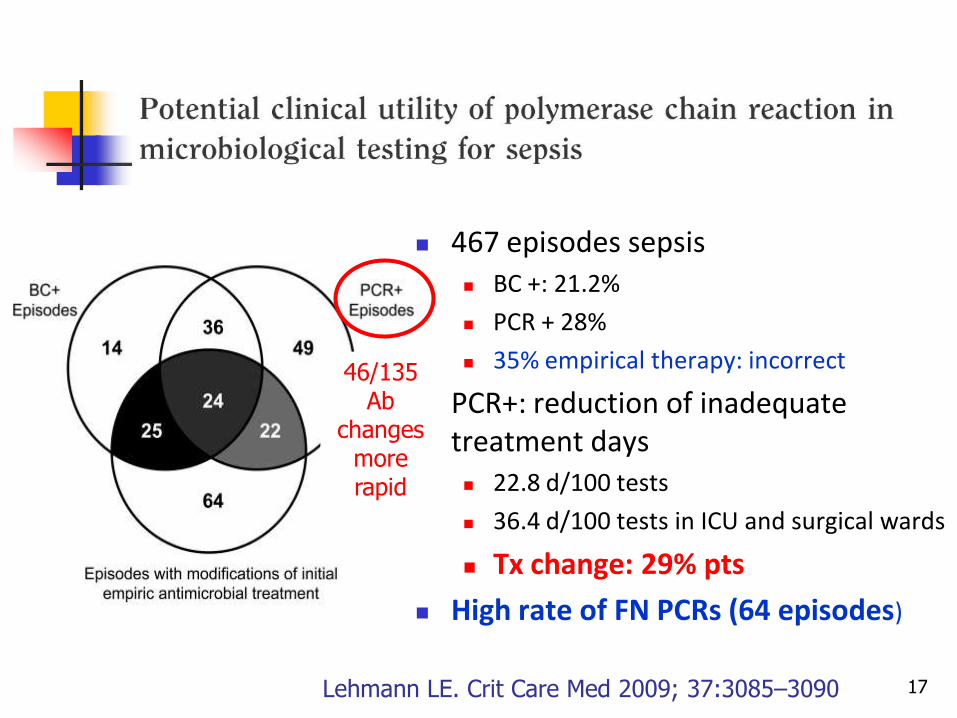
467 episodes sepsis BC +: 21.2%
PCR + 28%
35% empirical therapy: incorrect
PCR+: reduction of inadequate treatment days 22.8 d/100 tests
36.4 d/100 tests in ICU and surgical wards
Tx change: 29% pts
High rate of FN PCRs (64 episodes)
17 Lehmann LE. Crit Care Med 2009; 37:3085–3090
46/135 Ab
changes more rapid

142 Severe Sepsis
BC +: 16.5%
PCR + 34.7%
Only PCR+ vs PCR-
Higher disease severity
Higher + biomarkers
Higher mortality
PCR- no withdrawal of ABS
18 Blood F. Intensive Care Med 2010
BC+: 70% PCR+
PCR+: 21% BC+

SepsiTest (Molzym Co.)
Universal 16S/18S rRNA Gene-Based PCR and sequence analysis
Time-consuming
Bacteria and yeasts
217 Euros
Wellinghausen N. J Clin Microbiol 2009; Lehman Med Microbiol Immunol
187 patients
BC +:18% PCR+: 31.5%
S 87% Sp 85.8%. Concordance 86%
20
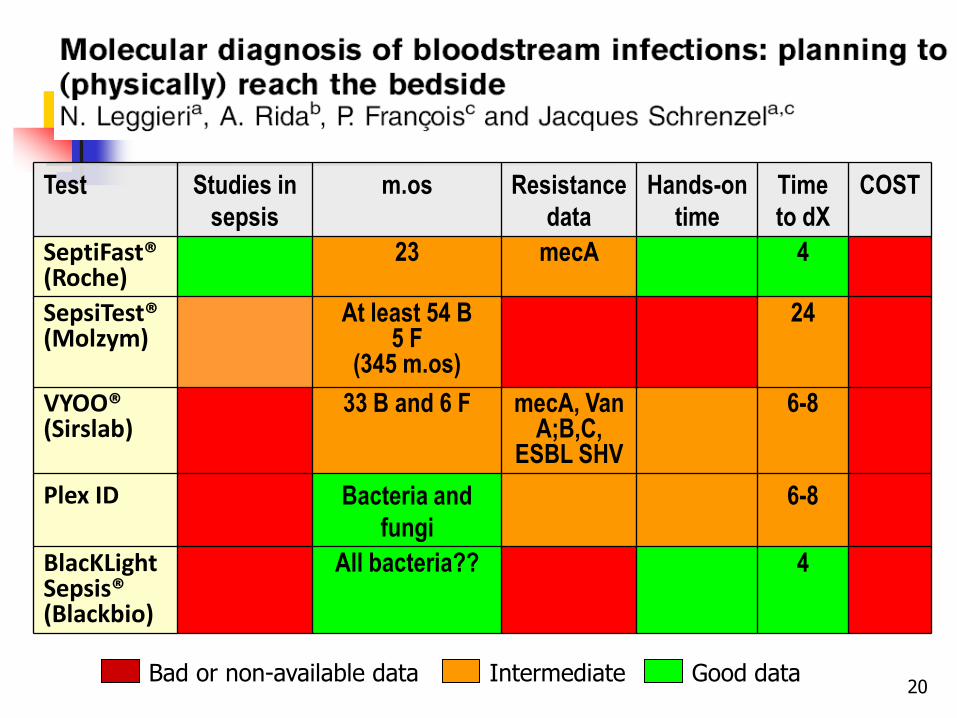
Test Studies in
sepsis
m.os Resistance
data
Hands-on
time
Time
to dX
COST
SeptiFast® (Roche)
23 mecA 4
SepsiTest® (Molzym)
At least 54 B 5 F
(345 m.os)
24
VYOO® (Sirslab)
33 B and 6 F mecA, Van A;B,C,
ESBL SHV
6-8
Plex ID Bacteria and
fungi
6-8
BlacKLight Sepsis® (Blackbio)
All bacteria?? 4
Bad or non-available data Intermediate Good data
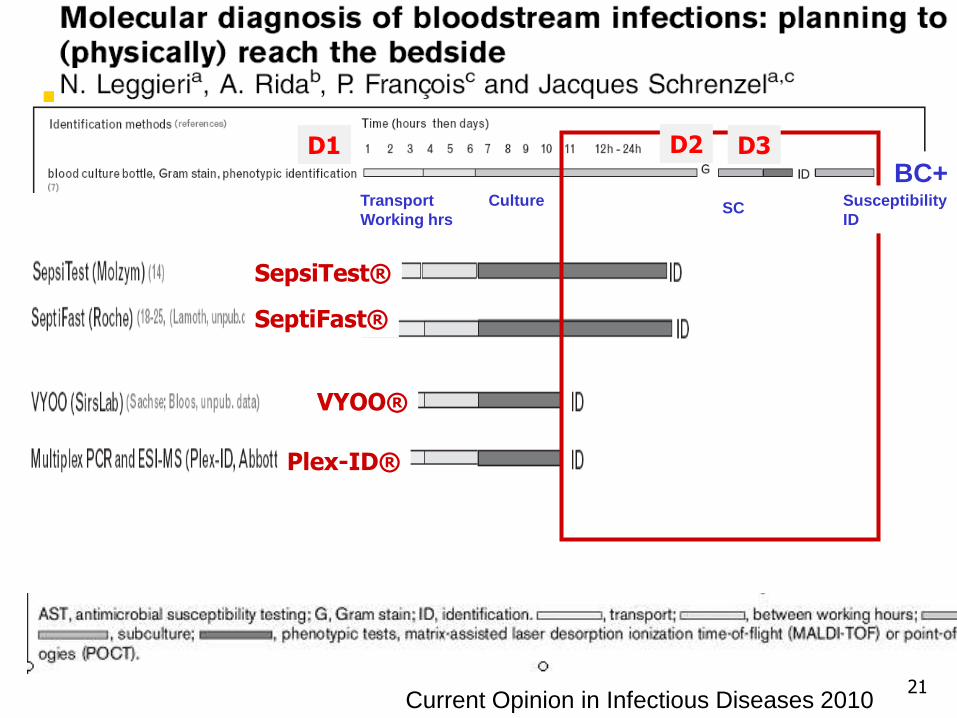
21 Current Opinion in Infectious Diseases 2010
BC+
18 h
Transport
Working hrs SC
Culture
SepsiTest®
SeptiFast®
VYOO®
Plex-ID®
Susceptibility
ID
D2 D3 D1

False negatives
Inhibition with WBC >30000/mm3
Specificity of primers and probes
Genetic variability of target site
Sample volume
Not in the list
22
False negative PCR

Which should be the ‘gold standard’? BC??
MM positive/ BC negative FP?
Clinically relevant? Many, later confirmed in other samples.
Non viable organisms? Cell-free DNA released from remote infection sites? Antibiotic interference?
MM neg/ BC neg. Unculturable pathogens? Not sepsis???
Refence method should include multiple data 23
Ecker DJ. Expert Rev Mol Diagn 2010

24
Are molecular methods of any benefit when BC are already
positive?

Molecular methods from + BC
PCR
+
MALDI-TOF MS (Bruker, Shimadzu, Vitek-MS)
PCR/ESI-MS (Plex-ID®)
PCR and microarray hybridization (Prove-it®)
RealT- specific PCR (Genexpert®, GenOhm®)
Peptide Nucleic Acid FISH (PNA FISH®)
PCR- reverse hybridization (Genotype®)
2-6 h
From POS BC
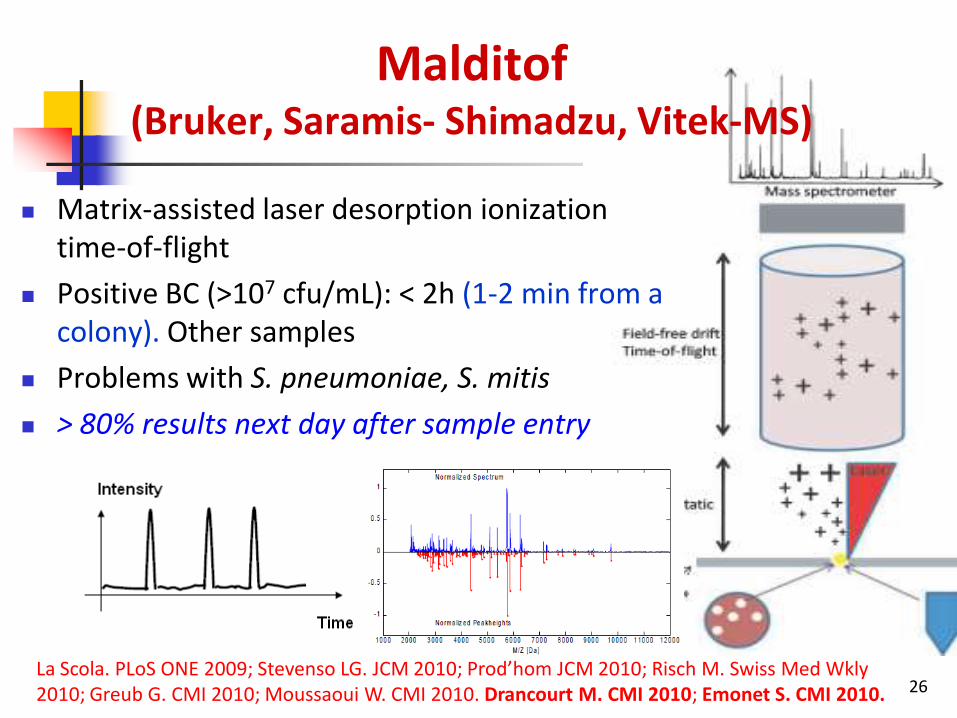
Malditof (Bruker, Saramis- Shimadzu, Vitek-MS)
Matrix-assisted laser desorption ionization time-of-flight
Positive BC (>107 cfu/mL): < 2h (1-2 min from a colony). Other samples
Problems with S. pneumoniae, S. mitis
> 80% results next day after sample entry
26 La Scola. PLoS ONE 2009; Stevenso LG. JCM 2010; Prod’hom JCM 2010; Risch M. Swiss Med Wkly 2010; Greub G. CMI 2010; Moussaoui W. CMI 2010. Drancourt M. CMI 2010; Emonet S. CMI 2010.

27
Clinical experience with Malditof
Samples n Correct
identification Comments
La Scola B. 2009 BC - Bactec 9240 562 76 G +/- 67%/94%
Stevenson LG. 2010 BC - Bactec 9240 212 80 Poor S mitis
Prod’hom G. 2010 BC - Bactec Plus 126 78.7 Poor S pn
Ferroni A. JCM 10 BC - Bact/Alert 312 91 S.a. vs CNS 100%
Christner M JCM 10 BC - Bactec Plus 304 95 S.a better AN bottles
Risch M. 2010 BC, urine, genital, wounds,
etc 204 87 Poor S pn
Moussaoui W. 2010 BC- Bactec 9240 503 90 G +/- 89%/91%
Ferreira L. 2011 BC- Bactec 9240 330 NR G +/- 31.8%/83%
Candida

Malditof potential
Different samples Fungus, virus, parasites Genotyping (nucleic acids)
Resistance R marker protein Degradation of Ab Induced R marker
Virulence Quantification?
28
RESEARCH IS ONGOING
Malditof
Some problems to solve
Poor detection of mixed populations
22 cases: only 1 species detected in 18
Sometimes lack of identification or false species
Poor detection of S. pneumoniae (4/20)
Agglutination test in all viridans strep identification (Bruker)
29 La Scola B. PLoS ONE 2009

PCR of several genes • Broad range primers • Polymicrobial inf
4-6 hours Different samples Quantification (sputum)
Typing, virulence, resistance
Biowarfare agents, infection control, syndromic panels
Ecker DJ. Expert Rev Mol Diagn 2010; Emonet S. CMI 2010; Kaleta EJ. JCM 2011.
Electrospray ionization mass Spectrometry
(PCR/ESI-MS) Plex ID® (Abbot)

PROVE-IT™ SEPSIS (MobiDiag)
PCR and microarray (gyrB, parE, mecA, 50 bacterial species, Fungi)
3318 BC / 2107 + (14% non detectable by Prove-It)
S 94.7 %; Sp 98.8% (100% MRSA)
1.6% FP, really FP?
18 h faster than BC
Tissari P. Lancet 2010; 375
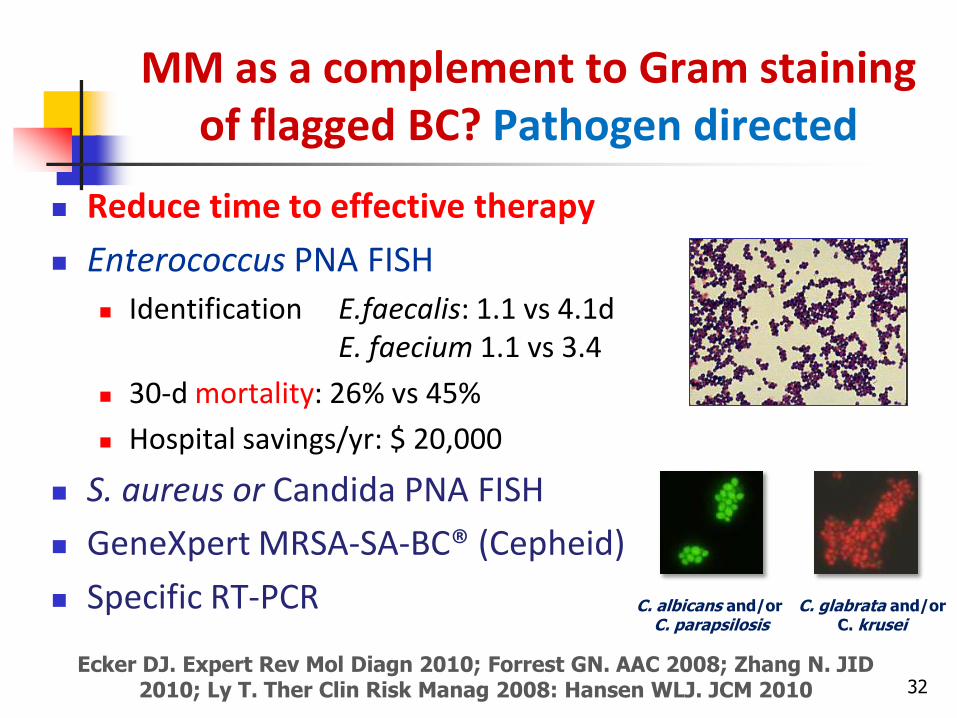
MM as a complement to Gram staining of flagged BC? Pathogen directed
Reduce time to effective therapy
Enterococcus PNA FISH
Identification E.faecalis: 1.1 vs 4.1d E. faecium 1.1 vs 3.4
30-d mortality: 26% vs 45%
Hospital savings/yr: $ 20,000
S. aureus or Candida PNA FISH
GeneXpert MRSA-SA-BC® (Cepheid)
Specific RT-PCR
32
Ecker DJ. Expert Rev Mol Diagn 2010; Forrest GN. AAC 2008; Zhang N. JID 2010; Ly T. Ther Clin Risk Manag 2008: Hansen WLJ. JCM 2010
C. glabrata and/or C. krusei
C. albicans and/or C. parapsilosis

Molecular detection in Positive blood cultures GeneXpert MRSA-SA-BC® (Cepheid)
406 blood cultures with clusters G + cocci Identification of MSSA and MRSA in 1h Simple. No special requirements
Wolk DM. J.Clin.Microb.2009
Sen 98.3% Spec 99.4% PPV 96.6% NPV 99.7% Contaminants CNS increase cost

34
Test Clinical
data
m.os Resistance
data
Hands-on
time
Time To
dX
COST
GENEXPERT aureus ® , Staph Plex
S. aureus MS and MR
PNA FISH
GENOTYPE® 15G+, 17G-, mecA, VanA,B
PROVE IT® 60 B mecA
MALDITOF B, Fung, Micob
Bad or non-available data Intermediate Good data

35 Current Opinion in Infectious Diseases 2010
BC+ Transport
Working hrs SC
Culture Susceptibility
ID
MALDI-TOF®
Prove-It®
MolYsis®

36
Does MM help in providing diagnosis of septic patients from
other samples?

37
MM in heart valve tissue FIRST-CHOICE technique
Broad-range bacterial or fungal PCR + sequencing Always confirm a positive result (PCR in different sample,
specific PCRs)
Organism-specific PCRs Tropheryma whipplei, B. quintana, B. henselae, C. burnetti
MRSA, S. pneumoniae, Generic PCR sodA for Streptococcus and Staphylococcus
Tang. JCM 2009; Raoult JCM 2005; Fournier CID 2010
38
S 96%, Sp 95.3%, NPV 98.4%, PPV 88.5%
Median response time
PCR result (pos or neg): 6 h from the reception of the sample
Hands-on time: 1.5 h
Species level: 24-48 h (6 hrs if targeted PCR used)
Medicine 2007;86:195–202

39
Embolus and clots
Vegetations that have embolized to peripheral arteries
Septic metastases
Pleural fluid
International Journal of Infectious Diseases (2009)

40
Culture 16S PCR p
Sensitivity 56.1% 81.7% <0.001
Specificity 97.4% 99.1% 0.057
Positive predictive value 76.7% 94.4% 0.004
Negative predictive value 92.8% 96.8% 0.008
Gram stain
Sensitivity
Specificity
24.4%
99.5%
723 pleural fluids
S. Insa, E. Bouza. Medicine (Baltimore) 2011.

41
Challenges for MM
1. Is this sepsis?
2. Is it caused by a resistant pathogen?
3. Which pathogen?
4. Are there any complications?
Dickermann Am Heart J 2007; Bouza E CID 2004:39;

42
Etiologic Dx of endocarditis LightCycler SeptiFast ®
63 IE
41 + BC: 11 positive SF (26.8%)
5/9 S. aureus, 0/9 CNS
1/7 Enterococcus
5/12 Streptococcus
0/4 other microorganisms (2 E. coli, 1 P. mirabilis, 1 C.
parapsilosis)
3 + in 22 BC – endocarditis S. gallolyticus, S. aureus, and E. faecalis
J. P. Casalta. Eur J Clin Microbiol Infect Dis (2009)

43
IE: specific etiology
Gram neg
40%Gram pos
53%
Anaerobes
3%
Fungi
4%
HOSPITAL GENERAL UNIVERSITARIO GREGORIO MARAÑÓN.
1,826 EPISODES OF BSI IN 2009
Fungi
1.9%
Gram neg
5.5%
CNS
17%
Enterococcus
12.1%
Streptococcus
spp
23.8%
S. aureus
26.5%
Unknown
9.9%
ENDOCARDITIS

44
Let’s imagine ….
1000 pts with SS
400 BC+ MM in blood 75% S 1-3 d more rapid ID
600 BC-
Septifast 30%S
20% Qx or other fluids
Specific PCR in blood <1%
>800 patients would benefit from MM methods For 300 the impact would be very major
180 pts
>300 pts?
120 pts
6 pts

45
Resistance in clinical samples Too many different techniques. Which is the best? Indications for specific populations. Complement to
BC and in selected high risk patients ? More microorganisms should be detected, more
information on resistance provided Quantification?
Evaluation in different clinical settings and cost-efficiency studies are warranted
Wishes for the future

46
Challenges for MM
1. Is this sepsis? Partially yes, if positive
2. Is it caused by a resistant pathogen? Not enough yet
3. Which pathogen? Partially yes
4. Are there any complications? Not enough yet
May not yet be the definite solution, but I think they are already helping…!!!

47
Will New Diagnostic Solutions Help Meet the Challenges of Sepsis?
I think so!


















