TCM and Endocrinology - Khoo Teck Puat Hospital 2_TCM...TCM and Endocrinology -What a GP should...
54
TCM and Endocrinology -What a GP should know! Dr Anuradha Negi Associate consultant
Transcript of TCM and Endocrinology - Khoo Teck Puat Hospital 2_TCM...TCM and Endocrinology -What a GP should...

TCM and Endocrinology
-What a GP should know!
Dr Anuradha Negi
Associate consultant

Complementary and Alternative medicine
76% (95% C.I. 73.9—77.9%) used
CAM over a 12-month period
Females 2.1 times more likely than
males
Chinese (84%)
Malays (69%)
Indians (69%)
Complementary and alternative medicine use in multiracial Singapore M.K. Lim, Complement Ther Med. 2005 Mar

Popularity of different forms of CAM
Complementary and alternative medicine use in multiracial Singapore M.K. Lim, Complement Ther Med. 2005 Mar

• Adulteration of herbal medications is widely reported.
• In Malaysia, 18% of 1000 herbal medications tested were positive.
• Common adulterants include Lead, Mercury, Corticosteroids and Non
steroidal anti inflammatory drugs.
• Corticosteroids are widely used for treatment of eczema, skin allergies,
asthma, rheumatoid arthritis
• Favored adulterant due to its rapid onset of action
Achievements of drug control authority. Newsletter of Drug control Authority Malaysia; 2007;35(13):1-12

Overview
• Case histories
• When to suspect use of herbal medication
• How to investigate
• Managing complications

Case: All are supplements safe?
• 81 year old Chinese Lady, Walking frame ambulant
• Found sitting on the floor, complaining of severe lower limb weakness for 3-
4 days
• Chronic joint pains
• Recent worsening left hip pain


• Febrile, Tmax 38’C
• Blood pressure 90/50 mmHg , HR 100/min, Spo2 100% RA
• Pale, moon face, Central obesity
• Thin skin, proximal muscle weakness, Striae, Ecchymosis.

• Resting clawing of her hands-unable to grip.
• Decreased ROM left shoulder,
• Decreased extension right elbow
• Decreased ROM left hip
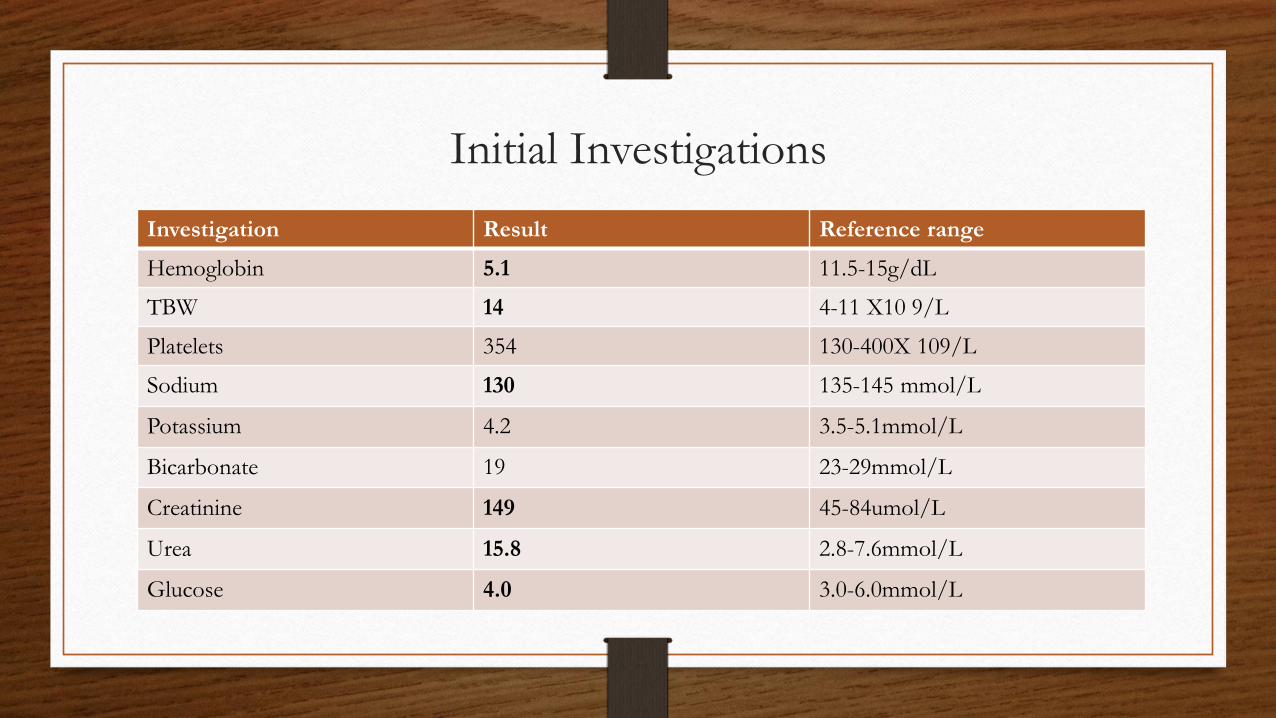
Initial Investigations
Investigation Result Reference range
Hemoglobin 5.1 11.5-15g/dL
TBW 14 4-11 X10 9/L
Platelets 354 130-400X 109/L
Sodium 130 135-145 mmol/L
Potassium 4.2 3.5-5.1mmol/L
Bicarbonate 19 23-29mmol/L
Creatinine 149 45-84umol/L
Urea 15.8 2.8-7.6mmol/L
Glucose 4.0 3.0-6.0mmol/L

Initial management
• Initial management : Bloods transfusion (5units).
• OGD: ulcer
• Colonoscopy : Inflamed caecal mucosa. Sigmoid diverticulum.
• Subsequent hemoglobin 10.4 g/L.
• No active bleeding noted.
• Patients blood pressure 100/80 mmHg with giddiness

Investigation Result Reference
Cortisol -0 min 183 Nmol/L
Cortisol- 30 min 314 Nmol/L
Cortisol- 60 min 330 Nmol/L
ACTH 1.0 1.6-13pmol/L
Tablets were obtained and sent to HSA for analysis
Patient reported consuming “black round pills” wrapped in cellophane for years for multiple
joint pains for more than 5 years. Stopped for 1 week due to poor appetite
In view of Cushingoid appearance and suspected Acute adrenal insufficiency from steroid
withdrawal, 250ug tetracosactide was performed.

Exogenous cushings syndrome
Adrenal insufficiency from steroid withdrawal

Treatment - Acute management
• Stabilizing patient
• Replace glucocorticoids
• Correct electrolyte disturbance: Rapid fluid administration D5% in isotonic Saline 1litre within first one hour and then as guided
• Hypoglycemia: Administer dextrose 0.5-1g/kg
• i.v Hydrocortisone 100 mg q 8 hourly X 3 days f/b
i.v Hydrocortisone 50mg q 8 hourly X 3 days f/b
PO. Hydrocortisone 20mg BD
Guidelines on Primary Adrenal Insufficiency. J Clin Endocrinol Metab 2016
Switched to 10 mg hydrocortisone OM and 5mg hydrocortisone ON
prior to discharge
Mineralocorticoid replacement and adrenal androgen is usually not
needed
To control joint pain:
• Hydroxychloroquine 200mg OM
• Methotrexate 10 mg per week
• Folic acid 5 mg daily
•Rheumatoid factor 24 (<14 IU/ml)
•ESR: 27 (1-20 mml/hr)
•XR: Periarticular joint erosions
along 2nd metacarpo phalangeal joint.

Exogenous Cushing’s Syndrome
• Iatrogenic – glucocorticoids used for neoplastic, inflammatory and
autoimmune disorders.
• Topical, Intra articular , aerosol- allow targeted therapy yet implicated in
development of CS
• Herbal remedies containing steroids.
• Megestrol acetate, a progestational agent for AIDS has glucocorticoid activity

Exogenous Cushing’s Syndrome secondary to Herbal
medication
• Incidence of hypertension increased but relatively less hypertension and
hypokalemia compared with spontaneous Cushing’s syndrome
• Less hirsutism and virilization than spontaneous disease.
• Higher incidence of glaucoma and posterior subcapsular cataract.
• Avascular necrosis is more common
• Osteoporosis-bone loss at trabecular bone as opposed to cortical bone

Diagnosing Exogenous Cushing’s syndrome…
• Clinical suspicion
• Suppressed endogenous cortisol
• Suppressed ACTH levels
• Decreased plasma cortisol response to cosyntropin
• Hydrocortisone interferes with the measurement of endogenous cortisol
Exogenous Cushing’s Syndrome and Glucocorticoid Withdrawal Endocrinol Metab Clin N Am 2005

Management of HPA axis suppression and steroid tapering
STEP 1. Decrease glucocorticoid dose from supraphysiologic to physiologic
STEP 2. Switch to a.m hydrocortisone or consider alternate day therapy
STEP 3. Measure morning cortisol
Exogenous Cushing’s Syndrome and Glucocorticoid Withdrawal Endocrinol Metab Clin N Am 2005

Morning cortisol level
<3 ug/dl (82nmol/L)
• Adrenal insufficiency.
• Continue glucocorticoids
• Retest 4-6 wk
3-20 ug/dl
(82-550nmol/L
• Needs further testing:
• Synacthen
• ITT
>20ug/dl
(550nmol/L)
• Recovered HPA axis
• Withdraw glucocorticoids
Exogenous Cushing’s Syndrome and Glucocorticoid Withdrawal Endocrinol Metab Clin N Am 2005

Radiology
XR Left Hip: Flattening of the femoral
head consistent with changes of
underlying avascular necrosis with
secondary osteoarthritis
Left Humeral head deformity with
degeneration. Joint space loss and
subchondral sclerosis


• Decline in BMD within 3 months of glucocorticoid use and peaks at 6
months.
• Increased risk of both vertebral and non vertebral fractures at doses 2.5-7.5
mg/day of Prednisolone- controversial.
Grossman, J.M et al. (2010) American College of Rheumatology 2010 recommendations for the prevention and treatment of
glucocorticoid-induced osteoporosis. Arthritis Care and Research.

Assessment of bone mineral density
• Dual X-ray absorptiometry – Gold standard
• Site- Spine and Hip
• FRAX score :
- Low risk < 10% for 10 year risk major osteoporotic fracture
- Medium risk FRAX 10-20% for 10 year major osteoporotic fracture
- High risk FRAX >20% for 10 year major osteoporotic fracture
Grossman, J.M et al. (2010) American College of Rheumatology 2010 recommendations for the prevention and treatment of
glucocorticoid-induced osteoporosis. Arthritis Care and Research.

Factors that shift an individual to a greater risk category for
glucocorticoid induced osteoporosis
• Low body mass index
• Parental history of hip fracture
• Current smoking
• >3 alcohol drinks per day
• Higher daily glucocorticoid dose
• Intravenous pulse glucocorticoid usage
• Declining central bone mineral density measurement that exceeds the least significant change
Grossman, J.M et al. (2010) American College of Rheumatology 2010 recommendations for the prevention and treatment of
glucocorticoid-induced osteoporosis. Arthritis Care and Research.

Treatment of glucocorticoid induced osteoporosis
Low risk
If gluco<7.5 mg/d: No pharmacologic treatment
recommended.
If gluco >7.5mg/d: Need bisphosphonate
Medium risk
If gluco <7.5 mg/day, use Alendronate or Residronate.
If gluco >7.5mg/day, use above or Zoledronate
High risk
If gluco <5 mg/d for < 1m Alendronate, Residronate or
Zoledronate
If gluco >5mg/day for <1 month or any other gluco > 1m
Alendronate, residronate, Zoledronate, Teriparatide
Grossman, J.M et al. (2010) American College of Rheumatology 2010 recommendations for the prevention and treatment
of glucocorticoid-induced osteoporosis. Arthritis Care and Research.
• Weight bearing exercise
• Smoking cessation
• Avoidance of excessive alcohol(>2 drinks per day)
• Nutritional counseling on Calcium 1200mg-1500mg/day and Vitamin D 800-1000 U /day.
• Fall risk assessment
• Baseline dual X ray absorptiometry
• Serum 25 –hydroxyvitamin D
• Baseline height
• Assessment of prevalent fragility fractures
Grossman, J.M et al. (2010) American College of Rheumatology 2010 recommendations for the prevention and
treatment of glucocorticoid-induced osteoporosis. Arthritis Care and Research.

Case 2.
• 58 Year old Male with history of hypertension, chronic tophaceous gout and
chronic kidney disease.
• Admitted for uncontrolled hypertension. Diagnosed with diabetes in the same
admission. HbA1c 8.2% ad fasting glucose 8.6mmol/L. Patient appeared clinically
Cushingoid 24 hour urine cortisol 9nmol/day (100-379 nmol/day).
• He claimed talking “Herbat” 2 pills/day for 2 years for general well being.
• He obtained these drugs from “ Pusat Rawatan Darul Ilaaj Centre”
• Omission of this medication will lead to feeling unwell with joint aches and pain.

Dexamethasone
Chlorpheniramine

Case : Increasing thyroxine requirement
• 60 Year old Chinese female
• Presented to ENT with chronic cough
• CT thorax :MNG with 4.4x2.1x1.4cm left lobe nodule and right mid pole
nodule measuring 2.9x 1.2 cm with calcification
• FNAC left nodule : Benign follicular nodule THY2
• Underwent Total thyroidectomy (Aug 2013). Histology : benign

Free T4 (12-
22pmol/L)
TSH (0.27-4.2
m iu/l)
Thyroxine dosage
Aug 2013 20 1.75 Thyroxine 50 mcg
Oct 2013 15.6 43 Thyroxine 100mcg
Nov 2013 26.6 0.963 Thyroxine 75mcg
Feb 2014 20.6 8.7 Thyroxine 75mcg
June 2014 24 5.08 Thyroxine 75 mcg
Sep2014 22 10 Thyroxine 50/75mcg
Dec 2014 18 32 Thyroxine 50/75mcg
Marc 2015 11.8 >100 Thyroxine 75mcg
Mar 2015 10 >100 Thyroxine 100mcg

Approach to patients requiring large dose of
L-T4
Optimal dose : 1.6-1.8ug/kg/day (Patients requirement 70mcg/day)
• Compliance
• Technique
-Absorption occurs in small intestine (60-80% )
-Maximal on empty stomach (within 3 hrs)
-Gastric acidity increases absorption
-Coffee decreases thyroxine absorption by 35%
-Fiber decrease absorption

Approach to patients requiring large doses of
L-T4
• Medications
Reduce absorption: Form insoluble complexes with Levothyroxine
Ferrous sulphate, Antacids, calcium carbonate, Phosphate binders, Proton
pump inhibitors.
Increase thyroxine metabolism: Antiepileptic, Rifampicin,
Herbal medications: Lemon balm, used in herbal tea. Anti TSH effect and
reduces intestinal thyroxine absorption

Suspect gastrointestinal condition if LT4> 2mcg/kg
Main gastrointestinal disorder that interfere with levothyroxine
absorption
Gastrointestinal disorders
Mechanism
Atrophic gastritis
Hypochlorhydria
H pylori
Ammonia production increased gastric pH
Celiac disease
Inflammation
Lactose intolerance
Inflammation
Bowel resection
Short bowel syndrome



• Compliant
• Technique
• Medications
• Reports chronic abdominal pain with bloating, weight 42-44 kg and
BMI 18.6 Kg/m2. No anemia, rash, oral ulcer, defects in tooth enamel,
arthralgia, osteoporosis.

• Further investigations:
• Endomysial IgA antibody negative
• OGD and Colonoscopy negative
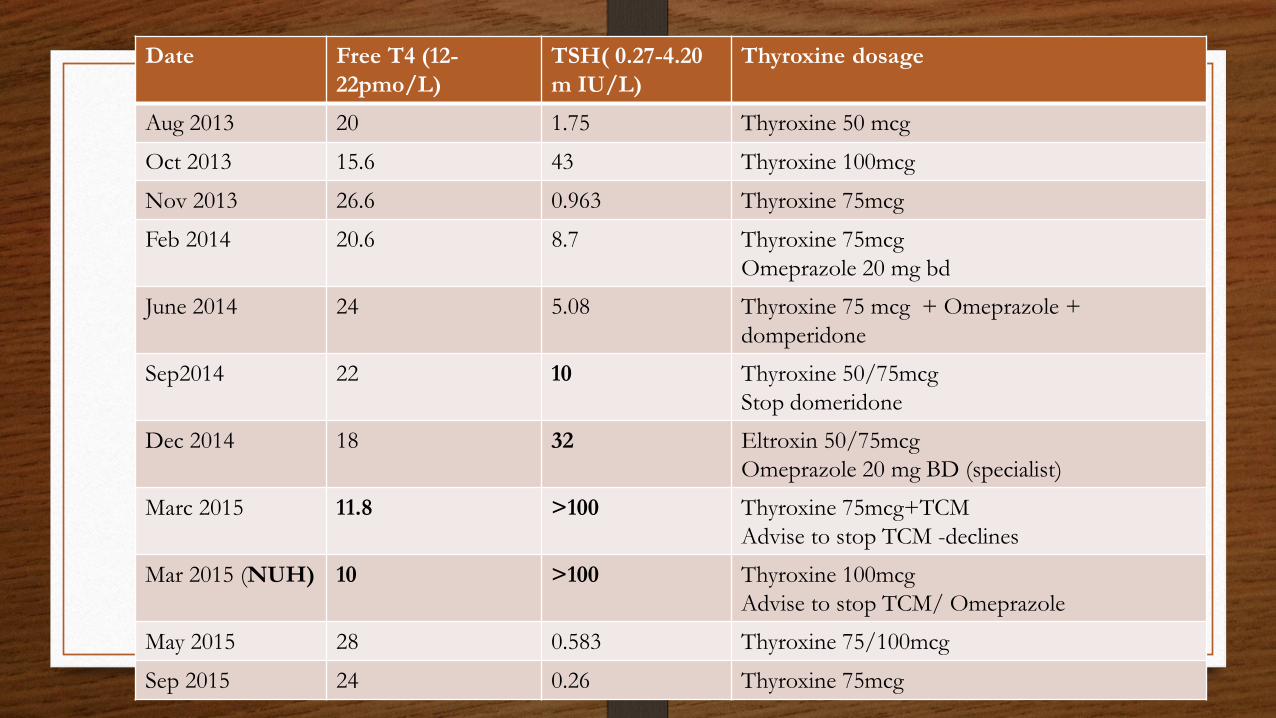
Date Free T4 (12-
22pmo/L)
TSH( 0.27-4.20
m IU/L)
Thyroxine dosage
Aug 2013 20 1.75 Thyroxine 50 mcg
Oct 2013 15.6 43 Thyroxine 100mcg
Nov 2013 26.6 0.963 Thyroxine 75mcg
Feb 2014 20.6 8.7 Thyroxine 75mcg
Omeprazole 20 mg bd
June 2014 24 5.08 Thyroxine 75 mcg + Omeprazole +
domperidone
Sep2014 22 10 Thyroxine 50/75mcg
Stop domeridone
Dec 2014 18 32 Eltroxin 50/75mcg
Omeprazole 20 mg BD (specialist)
Marc 2015 11.8 >100 Thyroxine 75mcg+TCM
Advise to stop TCM -declines
Mar 2015 (NUH) 10 >100 Thyroxine 100mcg
Advise to stop TCM/ Omeprazole
May 2015 28 0.583 Thyroxine 75/100mcg
Sep 2015 24 0.26 Thyroxine 75mcg

Lemon Balm
Melissa officinalis
-Often used herbal teas and essential oils
-Anxiolytic, calming and sedative
-Used for the treatment of disorders of
Gastrointestinal, nervous system and liver
disorders
-Antithyrotropic activity by forming adducts
with TSH that bind weakly with
TSH receptor

Case 4: Excess of everything is bad
• 65 year old female
• Type 2 DM (HbA1c 7.4%)
• Hyperlipidemia
- Presented with a fall and back pain.
-Blood cultures : MSSA
-CT Abdomen : psoas Abscess
-Undergoing Rehab in CH

• Transferred from CH for Patient reports nausea, vomiting and epigastric
discomfort.
• She reported poor appetite
• BP 160/110mm Hg
• Lower limb weakness (power 4/5 bilateral)

Date baseline April 2016 Value Reference
Sodium 139 135-145mmol/L
Potassium 4.5 3.5-5.0mmol/L
Urea 5.8 2.8-7.7mmol/L
Creatinine 28 50-90umol/L
Bicarbonate 23 9-31mmol/L
Date June 2016 Value Reference
Sodium 146 135-150mmol/L
Potassium 2.4 3.5-5mmol/L
Urea 2.1 2-6.5mmol/L
Creatinine 53 50-90umol/L
Chloride 102 95-110mmol/L
Bicarbonate 31 23-29mmol/L
lactate 1.4 <2.2 mmol/L
Ketone 0.4 <0.6mmol/L

T wave
amplitude
ST T wave
PR prolonged
U waves > T waves
Giant U waves
PseudoQT
prolongation
VT VF AV block
Treated with IV KCL 10mmol x3 and Tablet KCL 1200mg BD
Monitor K every 2-4 hour
Continuous cardiac monitoring

• History :
Reported vomiting.
• Drug history : No diuretics and no TCMs
• Stopped Tramadol and Metformin
DRUG HISTORY
Tramadol 50 mg TDS Omeprazole 40 mg OM
Metformin 850 mg TDS Gabapentin 300mg ON
Ergocalceferol 50,000 Units/wk Simvastatin 20 mg ON
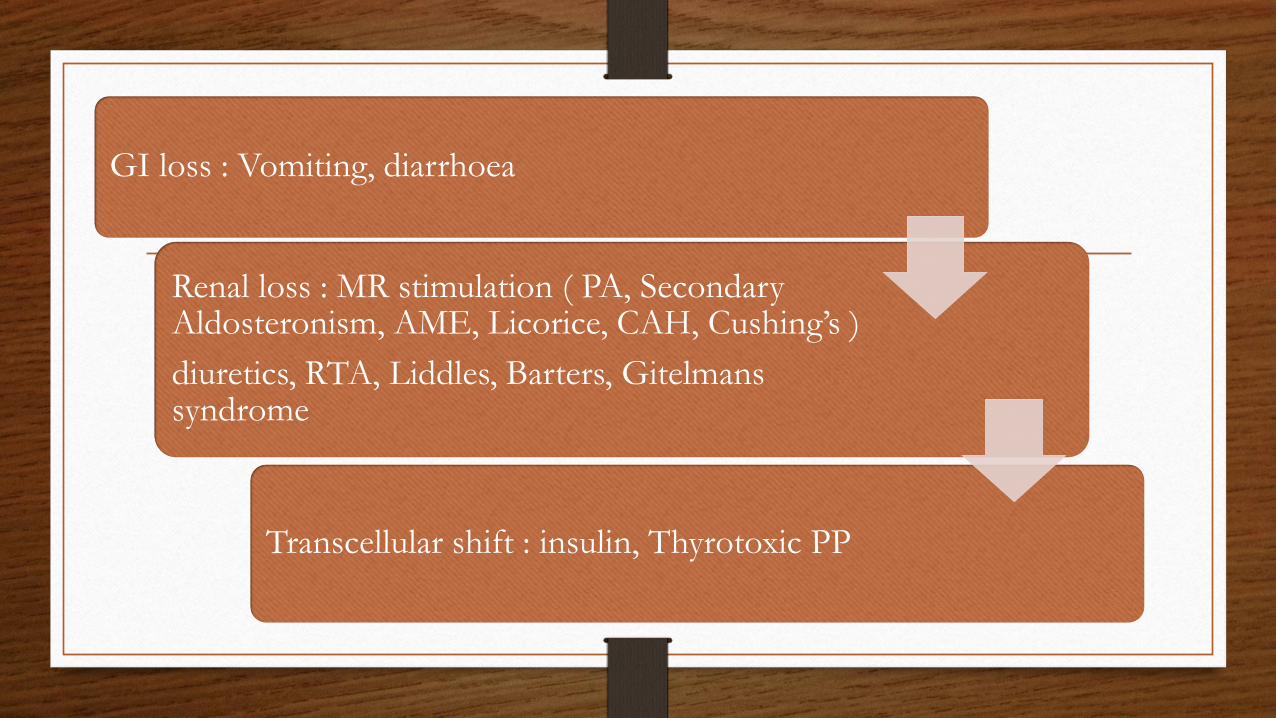
GI loss : Vomiting, diarrhoea
Renal loss : MR stimulation ( PA, Secondary Aldosteronism, AME, Licorice, CAH, Cushing’s )
diuretics, RTA, Liddles, Barters, Gitelmans syndrome
Transcellular shift : insulin, Thyrotoxic PP
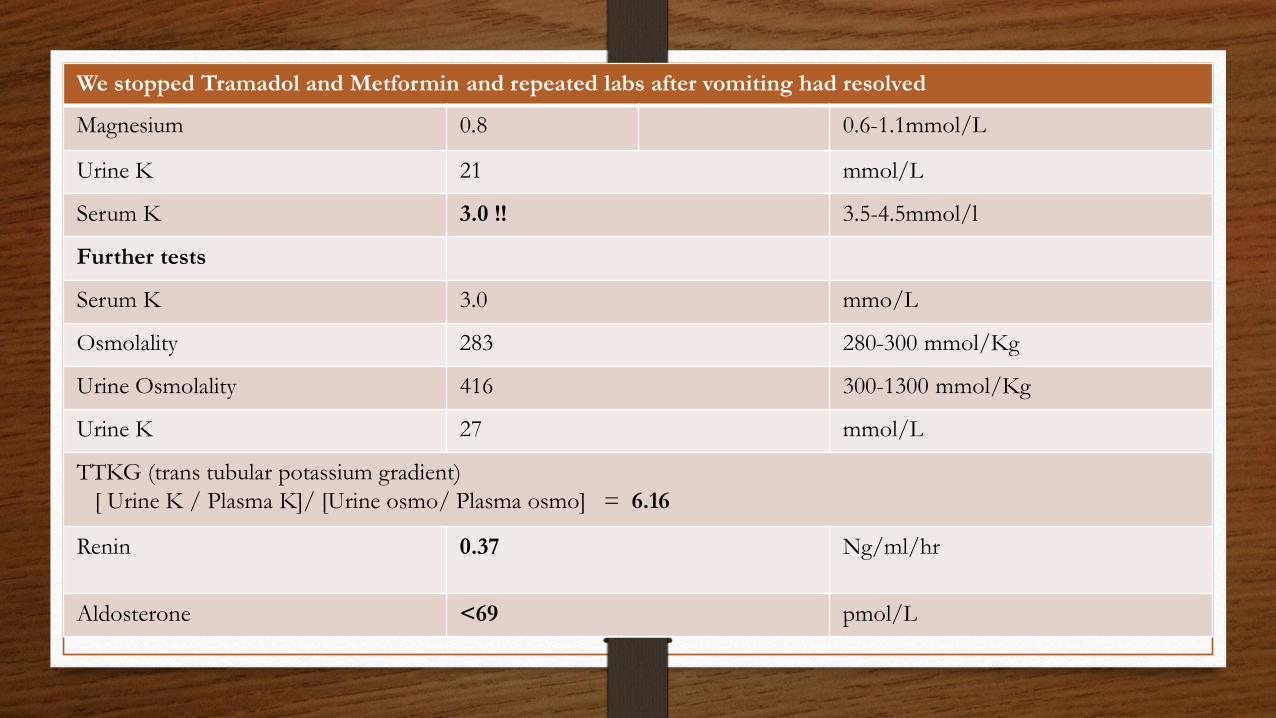
We stopped Tramadol and Metformin and repeated labs after vomiting had resolved
Magnesium 0.8 0.6-1.1mmol/L
Urine K 21 mmol/L
Serum K 3.0 !! 3.5-4.5mmol/l
Further tests
Serum K 3.0 mmo/L
Osmolality 283 280-300 mmol/Kg
Urine Osmolality 416 300-1300 mmol/Kg
Urine K 27 mmol/L
TTKG (trans tubular potassium gradient)
[ Urine K / Plasma K]/ [Urine osmo/ Plasma osmo] = 6.16
Renin
0.37
Ng/ml/hr
Aldosterone <69 pmol/L

Urinary potassium excretion :
-24 hour urine potassium >25-30 mmol/day indicates renal loss
-Spot urine K to creatinine ratio (<13 meq/g creat or 1.5meq/mmol)
-Fractional K excretion (<7% in hypokalemia)
-Transtubular K gradient (<3 in hypokalemia)

• Evidence of its use in ancient China dates back to the 1st century AD
• Referenced in the book Shen nung Pen Tsao Ching ( Divine Husbandman’s Classic
of Materia Medica )and believed to have been written by the Chinese emperor
Shen Nung, considered to be the father of Chinese medicine
• Reduces “fire poison” and diminishes “heat”
• Used for gastric and duodenal ulcer, acute abdomen pain,
sore throat, cough, asthma
The licorice plant- Glycyrrhizia

-Sweet taste x 30 times sweeter than sucrose
-“Generally recognized as safe” flavoring by FDA
- Upper limit is 100mg/day of glycyrrhizin intake-EU
(Same amount= 60 gm of licorice candy)
-“Asam boi” or “Sng Buay” is used locally. It is richly
flavored with sweetener and preservatives and
contains glycyrrhizic acid.
The licorice plant- Glycyrrhizia

Physiological effects of Licorice
• Hypertension
• Hypokalemia
• Metabolic
alkalosis
• Sodium and water
retention

Licorice Toxicity
• Hypertension
• Fluid and salt retention, edema, weight gain
• Muscle weakness and paralysis
• Rhabdomyolysis
• Acute renal failure
• EKG changes and ventricular tachycardia

Sample Analyte Effect
Blood Potassium Decreased
pH Increased
Hco3 or CO2 Increased
Aldosterone Decreased
Renin Decreased
Creatinine Kinase, Myoglobin Increased
Urine Cortisol : cortisone ratio Increased
Urine TTKG Increased