TAVR in Intermediate & Low Risk Patients 643 628 604TF Surgery 595 577 569 557 538 TF TAVR p (log...
19
TAVR in Intermediate & Low Risk Patients Prakash Balan, MD, JD, FACC, FSCAI Assistant Professor Interventional Cardiology The University of Texas Health Science Center Houston
Transcript of TAVR in Intermediate & Low Risk Patients 643 628 604TF Surgery 595 577 569 557 538 TF TAVR p (log...

TAVR in
Intermediate & Low Risk Patients
Prakash Balan, MD, JD, FACC, FSCAI
Assistant Professor
Interventional Cardiology
The University of Texas Health Science Center Houston

McGovern Medical School
Disclosures • Member PARTNER Case
Review Board
• No relevant financial
interests

McGovern Medical School
TAVR High Risk
(STS > 8%)
PARTNER
+
COREVALVE US
PIVOTAL
SAVR/TA
VR
Intermediate Risk
(STS 4-8%)
PARTNER 2
+
SURTAVI
SAVR
Low Risk
(STS < 4%)
PARTNER 3
+
COREVALVE EVOLUT
LOW RISK
TAVRinPerspective
EarlyTAVRPioneers
-PhilippBonhoeffer-
2000:Firsthumanimplant(RVtoPAconduit)
-HeningRudAndersen-
1989:Firstporcineimplant
Valve
Technology
SAPIEN
SAPIEN XT
SAPIEN 3
Sheath
Compatibility
Available
Valve Sizes
23 mm 26 mm 20 mm 23 mm 26 mm 29 mm
PARTNER SAPIEN Platforms Device Evolution
22-24F 16-20F 14-16F
23mm 26mm
*First Implant Oct 30, 2012
29mm*
April 16, 2002; FIM-TAVI, Transseptal
15 min Post-TAVI

McGovern Medical School
Primary Endpoint: All-Cause Mortality or Disabling Stroke at Two Years
Randomized Patients n = 2032
Symptomatic Severe Aortic Stenosis
ASSESSMENT by Heart Valve Team Operable (STS ≥ 4%)
The PARTNER 2A Trial Study Design
TF TAVR (n = 775)
Surgical AVR (n = 775) VS. VS.
ASSESSMENT: Transfemoral Access
Transapical (TA) / TransAortic (TAo) Transfemoral (TF)
1:1 Randomization (n = 482) 1:1 Randomization (n = 1550)
TA/TAo TAVR (n = 236)
Surgical AVR (n = 246)
Yes No
From Craig R. Smith on behalf of PARTNER Trial Investigators, ACC, April 2, 2016, Chicago, IL.
McGovern Medical School
Purpose—PARTNER 2A
To compare the safety and effectiveness of the
second generation
SAPIEN XT TAVR system
with conventional surgery
in intermediate-risk patients using rigorous
clinical trial methodologies.
From Craig R. Smith on behalf of the PARTNER Trial Investigators, ACC, April 2, 2016, Chicago, IL.
Primary Endpoint: All-Cause Mortality or Disabling Stroke at Two Years
Characteristic TAVR
(n = 1011)
Surgery
(n = 1021) p-value
Age - yrs 81.5 ± 6.7 81.7 ± 6.7 0.63
Male - % 54.2 54.8 0.79
STS Score - % 5.8 ± 2.1 5.8 ± 1.9 0.29
NYHA Class III or IV - % 77.3 76.1 0.53
CAD - % 69.2 66.5 0.20
Prior CABG - % 23.6 25.6 0.33
Cerebrovascular Disease - % 32.1 31.0 0.60
PVD - % 27.9 32.9 0.02
Baseline Patient Characteristics Demographics and Vascular Disease

McGovern Medical School
1011 918 901 870 842 825 811 801 774
1021 838 812 783 770 747 735 717 695
Number at risk:
TAVR
Surgery
p (log rank) = 0.253
HR [95% CI] = 0.89 [0.73, 1.09]
TAVR
Surgery
0
10
20
30
40
50
19.3%
21.1%
14.5%
16.4%
0 3 6 9 12 15 18 21 24
6.1%
8.0%
Primary Endpoint (ITT) All-Cause Mortality or Disabling Stroke
Months from Procedure
All-
Cau
se M
ort
alit
y o
r D
isab
ling
Stro
ke (
%)
From Craig R. Smith on behalf of the PARTNER Trial Investigators, ACC, April 2, 2016, Chicago, IL.

McGovern Medical School
1
775 718 709 685 663 652 644 634 612
775 643 628 604 595 577 569 557 538
TF TAVR
TF Surgery
p (log rank) = 0.05
HR: 0.79 [95% CI: 0.62, 1.00]
16.8%
20.4%
0 3 6 9 12 15 18 21 24
0
10
20
30
40
50
15.9%
7.7%
12.3%
4.9%
TF Primary Endpoint (ITT) All-cause Mortality or Disabling Stroke
TF TAVR
TF Surgery
Months from Procedure Number at risk:
All-
Cau
se M
ort
alit
y o
r D
isab
ling
Stro
ke (
%)
From Craig R. Smith on behalf of the PARTNER Trial Investigators, ACC, April 2, 2016, Chicago, IL.

McGovern Medical School
Intermediate Risk Operable
(PII S3i)
High Risk Operable / Inoperable
(PII S3HR)
Symptomatic Severe Aortic Stenosis
ASSESSMENT by Heart Valve Team
n = 1076 Patients
n = 583 Patients
ASSESSMENT: Optimal Valve Delivery Access
ASSESSMENT: Optimal Valve Delivery Access
SAPIEN 3
2 Single Arm Non-Randomized Historical-Controlled Studies
Transfemoral (TF)
TF TAVR SAPIEN 3
TAA TAVR SAPIEN 3
Transapical / Transaortic (TA/TAo)
TF TAVR SAPIEN 3
PI A SAPIEN
PII A SAVR
Transfemoral (TF)
TAA TAVR SAPIEN 3
Transapical / Transaortic (TA/TAo)
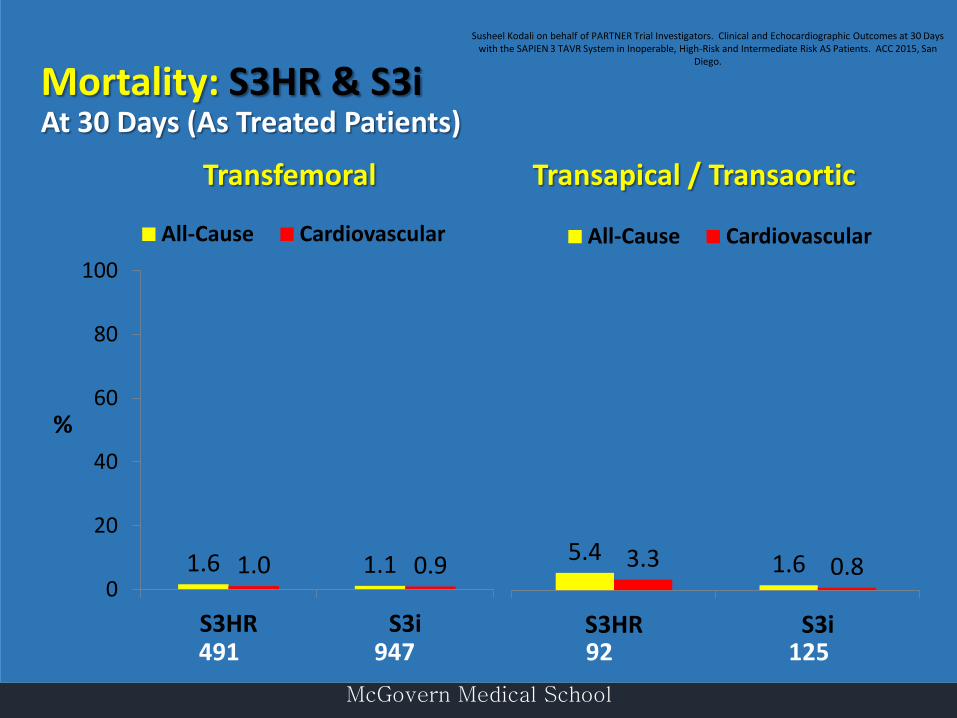
Susheel Kodali on behalf of PARTNER Trial Investigators. Clinical and Echocardiographic Outcomes at 30 Days with the
SAPIEN 3 TAVR System in Inoperable, High-Risk and Intermediate Risk AS Patients. ACC 2015, San Diego.
The PARTNER II S3 Trial Study Design

McGovern Medical School
Baseline Patient Characteristics S3i Patients
Average STS =
5.3% (Median 5.2%)
TF, 89%
TA, 7%
TAo, 4%
N = 1076
4.1%
32.2% 43.7%
20.0%
20 mm 23 mm 26 mm 29 mm
Average Age =
81.9yrs
Male 62%
Female 38%
Susheel Kodali on behalf of PARTNER Trial Investigators. Clinical and Echocardiographic Outcomes at 30 Days with the SAPIEN 3 TAVR System in Inoperable, High-Risk and Intermediate Risk AS Patients. ACC 2015, San Diego.
McGovern Medical School
1.6 1.1 1.0 0.9 0
20
40
60
80
100
S3HR S3i
All-Cause Cardiovascular
5.4 1.6 3.3 0.8
S3HR S3i
All-Cause Cardiovascular
Transfemoral Transapical / Transaortic
%
Mortality: S3HR & S3i At 30 Days (As Treated Patients)
491 947 92 125
Susheel Kodali on behalf of PARTNER Trial Investigators. Clinical and Echocardiographic Outcomes at 30 Days with the SAPIEN 3 TAVR System in Inoperable, High-Risk and Intermediate Risk AS Patients. ACC 2015, San
Diego.

McGovern Medical School
Pre-sp
ecified
non-inf
eriority
margin
= 7.5%
-10 -8
-6 -4
-2 0
2 4
6 8
10
Primary
Non-In
feriorit
y Endpo
int Met
Weight
ed Differ
ence
-9.2%
Upper 1
-sided 9
5% CI
-6.0%
Non-Inf
eriority
p-value
< 0.001
Favors
TAVR
Favors
Surgery
Primary
Endpo
int - No
n-inferi
ority
Death, Stroke, or AR ≥ Mod at 1 Year (VI)
From Vinod H. Thourani on behalf of the PARTNER Trial Investigators, ACC, April 3, 2016, Chicago, IL.

McGovern Medical School
From Vinod H. Thourani on behalf of the PARTNER Trial Investigators, ACC, April 3, 2016, Chicago, IL.

McGovern Medical School
PatientFlow
9
ContinuedAccessStudy(CAS)290patients
15notattempted:-1died- 2withdrewconsent- 11physicianwithdrew- 1pendingprocedure
TAVRattemptedimplant:N=275
TAVRimplantedgroup:N=274
1notimplanted
TAVRITTgroup:N=879
TAVRimplantedgroup:N=863 SAVRimplantedgroup:N=794
*Themodifiedintention-to-treat(mITT)populationincludesallsubjectswithanattemptedprocedure
SAVRITTgroup:N=867
2notimplanted1wenttoSAVR
2surgicalpatientsreceivedTAVR
TAVRmITT*group:N=864
15notattempted:-4died- 6withdrewconsent- 5physicianwithdrew
71notattempted:-4died- 43withdrewconsent- 23physicianwithdrew- 1losttofollow-up
SAVRmITT*group:N=796
1notimplanted2wenttoTAVR
1TAVRpatientreceivedSAVR
RandomizedControlledTrial(RCT)1746patients
Age,years 79.7± 6.1 79.9± 6.2 79.0± 6.1
STSPROM,% 4.5± 1.6 4.4± 1.5 4.1± 1.5
n(%)ormean±SD RCT* CAS
SAVR(N=796) TAVR(N=864) TAVR(N=275)
Malesex 438(55.0) 498(57.6) 127(46.2)
Bodysurfacearea,m2 1.9± 0.2 1.9± 0.2 1.9± 0.2
LogisticEuroSCORE,% 11.6± 8.0 11.9± 7.6 9.1± 6.5
Diabetesmellitus 227(34.8) 295(34.1) 100(36.4)
Serumcreatinine>2mg/dl 17(2.1) 14(1.6) 2(0.7)
Priorstroke 57(7.2) 57(6.6) 16(5.8)
PriorTIA 46(5.8) 58(6.7) 8(2.9)
Peripheralvasculardisease 238(29.9) 266(30.8) 71(25.8)
Pre-existingIPG/ICD 72(9.9) 87(10.1) 19(6.9)
BaselineCharacteristics
10*mITTpopulation;nosignificantdifferenceinanybaselinecharacteristics
From VanMeighem VM. Transcathether Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in
Intermediate Risk Patient. TCT 2017.

McGovern Medical School
796 723 678
864 813 772
All-CauseMortalityorDisablingStroke
15%
10%
5%
20%
25%
30%
All-CauseM
ortalityor
DisablingStroke TAVR
SAVR
0%
0 2 4 6
MonthsPost-Procedure
8 10 12
No.atRiskSAVR
TAVR13
P-value(log-rank)=0.55
8.5%7.8%
From VanMeighem VM. Transcathether Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in
Intermediate Risk Patient. TCT 2017.

McGovern Medical School
The PARTNER 3 TrialStudy Design
1:1 Randomization
(n=1228)
TF - TAVR
(SAPIEN 3)
Surgery
(Bioprosthetic Valve)
Follow-up: 30 days, 6 mos, 1 year and annually through 10 years
CT Imaging Sub-Study (n=200)
Low Risk ASSESSMENT by Heart Team(STS < 4%, TF only)
Symptomatic Severe Calcific Aortic Stenosis
PRIMARY ENDPOINT:
Composite of all-cause mortality, all strokes,
or re-hospitalization at 1 year post-procedure
Bicuspid Valves
(n=100)
ViV (AV and MV)
(n=100)
PARTNER 3
Registries
Alternative Access
(n=100)
(TA/TAo/Subclavian)
Actigraphy/QoL Sub-Study (n=200)
CT Imaging Sub-Study (n=200)
Actigraphy/QoL Sub-Study (n=200)

McGovern Medical School

McGovern Medical School
Trial Flow
All randomized n=280
ITT SAVR n=135
ITT TAVR n=145
Died prior to procedure n=1
IMPLANTED TAVR n=139
IMPLANTED SAVR n=135
AT TAVR n=142
AT SAVR n=134
Crossover
SAVR to
TAVR
n=1
Crossover
TAVR to
SAVR
n=1
Crossover
TAVR to
SAVR
n=3
Not implanted n=2
Died prior to procedure n=3
Thyregod HGH. An All Comers Randomized Clinical Trial Comparing Transcatheter with Surgical Aortic Valve Replacement in Patient
with Aortic Valve Stenosis. ACC 2015.
Nordic Aortic Valve Intervention (NOTION) Trial
Objective: Compare TAVR vs. SAVR in patients > 70 years eligible for
surgery (all-comers population)
Primary outcome: Composite rate of death from any cause, stroke or myocardial
infarction at 1 year (VARC II-defined)
Secondary outcomes: Safety and efficacy (NYHA), echocardiographic outcomes
(VARC II-defined)
Design: Prospective, multicenter, non-blinded, randomized trial
Enrollment period: December 2009 - April 2013
Baseline Characteristics
Characteristic, % or mean ± SD
TAVR n=145
SAVR n=135
p-value
Age (yrs) 79.2 ± 4.9 79.0 ± 4.7 0.71
Male 53.8 52.6 0.84
Society of Thoracic Surgeons (STS) Score 2.9 ± 1.6 3.1 ± 1.7 0.30
STS Score < 4% 83.4 80.0 0.46
Logistic EuroSCORE I 8.4 ± 4.0 8.9 ± 5.5 0.38
NYHA class III or IV 48.6 45.5 0.61

McGovern Medical School
Death from Any Cause, Stroke or Myocardial Infarction
at 1 Year in As-Treated Population
Thyregod HGH. An All Comers Randomized Clinical Trial Comparing Transcatheter with Surgical Aortic Valve Replacement in Patient
with Aortic Valve Stenosis. ACC 2015.

McGovern Medical School
Garg A et al. Transcatheter Aortic Valve Replacement versus Surgical Valve
Replacement in Low-Intermediate Surgical Risk Patients. J Invasive Cardiol
2017; 29 (6): 209-216.
Witberg G et al. Transcatheter versus Surgical Aortic
Valve Replacement in Patients at Low Surgical Risk: A
Meta-Analysis of Randomized Trials and Propensity
Score Matched Observational Studies. Cardiac Cath &
Interven. Published online 2/8/18.

McGovern Medical School
CONCLUSION
• Await RCT data among low risk
• TAVR appropriate in intermediate risk patients
• Each with advantages and disadvantages:
• SAVR: AFib, AKI
• TAVR: PPM, PVL
• Heart Team
McGovern Medical School
“The management of patients with complex severe VHD is best
achieved by a Heart Valve Team composed primarily of…”
• Cardiologists
• Surgeons
• Structural valve interventionalists
• Cardiovascular imaging specialists
• Cardiovascular surgeons
• Anesthesiologists
• Nurses
Old Paradigm Emerging Paradigm
Interventionalist
Patient
Cardiologist Surgeon
Patient
Interventionalist
Cardiologist Surgeon
NishmuraRA,etal.Circulation.2014;129.
Multidisciplinary Heart Valve Team AHA/ACC 2014
Guidelines