T VIEW - Informa Marketsimages2.advanstar.com/PixelMags/vetmedicine/pdf/2014-11.pdf · development...
36
Social media INCLUDES THE November 2014 | Volume 109 | Number 11 | PEER-REVIEWED | dvm360.com Don’t forget to count! The consequences of a preventable surgical complication 346 Journal Scan Why you should be looking harder for CKD in cats 342 Feline diabetes What factors influence spontaneous clinical remission? 344 Idea Exchange ▸ A measured way to keep an eye on skin masses 360 ▸ A super approach to getting cats into carriers 360 p351 Te VIEW from BOTH SIDES
Transcript of T VIEW - Informa Marketsimages2.advanstar.com/PixelMags/vetmedicine/pdf/2014-11.pdf · development...

Social media
INCLUDES THE
November 2014 | Volume 109 | Number 11 | PEER-REVIEWED | dvm360.com
Don’t forget to count!The consequences
of a preventable
surgical complication 346
Journal ScanWhy you should be
looking harder for
CKD in cats 342
Feline diabetesWhat factors infl uence
spontaneous clinical
remission? 344
Idea Exchange▸ A measured way
to keep an eye
on skin masses 360
▸ A super approach
to getting cats
into carriers 360
p351
T e
VIEWfrom
BOTH SIDES
ES519833_vetm1114_CV1.pgs 10.27.2014 20:01 ADV blackyellowmagentacyan

© 2014 Abbott Laboratories. AlphaTRAK is a trademark of Abbott Group of companies in various jurisdictions. AT2-2109
Humans sharea lot of things with their pets.Blood glucose meters shouldn’t be one of them.
Portable blood glucose meters designed for blood glucose monitoring in humans are not validated for veterinary use on pets.
AlphaTRAK is specifi cally calibrated and validated for dogs and cats for accurate readings.
Now with a reduced price, accuracy is affordable for your practice and your clients. With a recommended Starter Kit price of just $70 to pet owners, there is no better time than now to upgrade to AlphaTRAK.
For more information call 866-257-8807 or visit www.AlphaTRAKmeter.com
NOW AT A REDUCED
PRICE
ES521303_VETM1114_CV2_FP.pgs 10.29.2014 00:27 ADV blackyellowmagentacyan

dvm360.com | Veterinary Medicine | November 2014 | 341
Subscriber Services: Call (800) 815-3400 in the United States, or (888) 527-7008 or (218) 740-6477 in Canada; fax (218) 740-6417; or write to: Veterinary Medicine, 131 W. 1st St., Duluth, MN 55802-2065. If you are un-able to connect with the 800 numbers, email [email protected]. Reprint Services: Call 1-877-652-5295 ext. 121 or email [email protected]. Outside US, UK, direct dial: 281-419-5725. ext. 121 Back Issues: Individual copies are available for one year; to order, call (800) 598-6008. Permissions/International Licensing. Call Maureen Cannon at (440) 891-2742. List Sales: Please contact List Account Executive Renée Schuster at (440) 891-2613. Editorial Offices: Write to 8033 Flint, Lenexa, KS 66214; or call (913) 871-3800. Visit our websites: dvm360.com; thecvc.com; industrymatter.com.
MissionVeterinary Medicine is a peer-reviewed journal dedicated
to providing concise, credible, and essential information
on the most common and crucial clinical problems seen
in companion-animal practice.
Editorial Advisory Board
Leading specialists who direct our content and ensure
our editorial quality and integrity
Joseph W. Bartges, DVM, PhD, DACVIM, DACVN
David S. Bruyette, DVM, DACVIM
Barret Bulmer, DVM, MS, DACVIM
John Ciribassi, DVM, DACVB
Timothy M. Fan, DVM, DACVIM
Juliet R. Gionfriddo, DVM, MS, DACVO
Karen A. Moriello, DVM, DACVD
Jennifer Wardlaw, DVM, MS, DACVS
Practitioner Advisory Board
Progressive practitioners who keep our content
practical, timely, and relevant
Mili Bass, DVM, DABVP
Robin Downing, DVM
Corey Entriken, DVM
Wayne L. Hunthausen, DVM
Thomas McCoy, DVM
Melissa M. Mckendry, DVM, DABVP
Fred L. Metzger Jr., DVM, DABVP
Robert M. Miller, DVM
Gary D. Norsworthy, DVM, DABVP
R. Wayne Randolph, VMD
Michael H. Riegger, DVM, DABVP
David Robbins, DVM
Philip VanVranken, DVM
Laura L. Wade, DVM, DABVP
Content Group
Editor/Medicine Channel Director | Mindy Valcarcel
Medical Editor | Heather Lewellen, DVM
Content Manager | Adrienne Wagner
Senior Content Specialist | Alison Fulton
Assistant Content Specialist | Katie James
Technical Editor | Jennifer Vossman, RVT
Consulting Technical Editor | Avi Blake, DVM
Digital Channel Director | Jessica Zemler
Senior Designer/Web Developer | Ryan Kramer
Art Director | Shawn Stigsell
Multimedia Contributor | Troy Van Horn
Advanstar Veterinary
Vice President/General Manager | Becky Turner Chapman
Group Content Director | Marnette Falley
Medical Director | Theresa Entriken, DVM
Director, Electronic Communications | Mark Eisler
Director, The CVC Group | Peggy Shandy Lane
Sales Group
Sales Director | David Doherty
Senior Account Managers, Advertising
Terry Reilly | Chris Larsen
Account Manager, Advertising | Angela Paulovcin
Senior Account Manager, Projects | Jed Bean
Sales and Projects Coordinator | Anne Belcher
Books/Resource Guides | Maureen Cannon(440) 891-2742
List Rental Sales | Renée Schuster(440) 891-2613, [email protected]
Chief Executive Officer | Joe Loggia
Chief Executive Officer Fashion Group,
Executive Vice-President | Tom Florio
Executive Vice President, Chief Administrative Officer
& Chief Financial Officer | Tom Ehardt
Executive Vice President | Georgiann DeCenzo
Executive Vice President | Chris DeMoulin
Executive Vice President, Business Systems | Rebecca Evangelou
Executive Vice President, Human Resources | Julie Molleston
Senior Vice President | Tracy Harris
Vice President, Legal | Michael Bernstein
Vice President, Media Operations | Francis Heid
Vice-President, Treasurer & Controller | Adele Hartwick
Veterinary Medicine (ISSN 8750-7943 print; ISSN 1939-1919 online) is published monthly by Advanstar Communications Inc., 131 West First St., Duluth, MN 55802-2065. One year subscription rates: $60 in the United States and Possessions; $72 in Canada and Mexico; $97 in all other countries. Single issue orders: $18 in the United States and Possessions; $22 in Canada and Mexico; $24 in all other countries. Periodicals postage paid at Duluth, MN 55806 and additional mailing offces. POSTMASTER: Please send address changes to Veterinary Medicine, P.O. Box 6087, Duluth, MN 55806-6087. Canadian GST Number: R-124213133RT001. Publications Mail Agreement Number: 40612608. Return undeliverable Canadian addresses to: IMEX Global Solutions, P.O. Box 25542, London, ON N6C 6B2, Canada. Printed in the U.S.A. © 2014 Advanstar Communications Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission in writing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specifc clients is granted by Advanstar Communications Inc. for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: [email protected]. Advanstar Communications provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities which may be of interest to you. If you do not want Advanstar Communications to make your contact information available to third parties for marketing purposes, simply call toll-free (866) 529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from Advanstar’s lists. Outside the United States, please call (218) 740-6477. Veterinary Medicine does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance on such content. Publisher assumes no responsibility for unsolicited manuscripts, photographs, art, and other material. Unsolicited material will not be returned. Address correspondence to Veterinary Medicine, 8033 Flint, Lenexa, KS 66214; (913) 871-3800; e-mail [email protected]. To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
ES519837_vetm1114_341.pgs 10.27.2014 20:03 ADV blackyellowmagentacyan

JOURNAL SCAN from the literature to your exam room
342 | November 2014 | Veterinary Medicine | dvm360.com GETTY IMAGES/BANANASTOCK
Why they did itEarly intervention for cats with
chronic kidney disease (CKD)
allows an opportunity to slow
disease progression. Identifying
risk factors for disease devel-
opment before the onset
of clinical signs would
provide clinicians
with clues of an
emerging prob-
lem and facilitate
discussion with
owners about the
need for preemp-
tive screening.
What they didAs part of a retrospective review,
researchers evaluated the medi-
cal records of 1,230 cats from
Banf eld clinics across the United
States that were diagnosed with
CKD between Jan. 1, 2010, and
Dec. 31, 2010. Cats included
in the study had to have been
seen at least once before the
qualifying 2010 visit. CKD was
diagnosed based on a creatinine
concentration > 1.6 mg/dl and
urine specif c gravity (USG).
What they foundBeing a neutered male; having
a thin body condition; having a
history of previous periodontal
disease or cystitis, anesthesia,
or documented dehydration
in the preceding year; or living
anywhere in the United States
other than the northeast were
all found to be risk factors for
the development of CKD. T e
reason for the regional dif er-
ence was not elucidated in the
study. Cats with a previous
history of diabetes mellitus ap-
peared to have a decreased risk
of CKD development.
Body condition and diet were
recorded for a subset of cats.
Among CKD cats and control
cats, thin body condition was
identif ed in 66.3% (396/597)
and 38.4% (167/435), respec-
tively. Pyuria (which was used
as a surrogate marker for the
presence of a bacterial urinary
tract infection) was identif ed in
72% (175/243) of cats with CKD
and 35.8% of control cats, con-
sistent with the known associa-
tion between CKD and bacterial
urinary tract infections. T e
exact cause of the pyuria, how-
ever, was not determined.
Median weight loss in the
preceding six to 12 months
was 10.8% and 2.1% among the
CKD and control cats, respec-
tively, and was associated with
a diagnosis of CKD. Interest-
ingly, there appeared to be no
association between type of
diet (wet or dry) and the de-
velopment of CKD despite the
belief that a dry diet is more
taxing on the kidneys.
Take-home messageT ese early indicators may
provide subtle hints of the need
for increased screening for
CKD before the development
of overt clinical signs. T ese
f ndings are not evidence of a
cause-and-ef ect relationship;
rather they provide a sound
basis for recommending more
aggressive screening among the
older cat population. Specif -
cally, evidence of weight loss
> 10%, which may have previ-
ously simply been attributed to
aging, should now prompt more
aggressive screening for emerg-
ing disease such as CKD. In
older cats, the presence of pyuria
should also prompt bacterial cul-
ture to rule out occult infection.
In cases of asymptomatic
CKD, early intervention with
a therapeutic diet may delay
the onset of uremic signs, may
prolong survival time, and
would be easier to implement
before the development of
CKD-associated gastrointesti-
nal problems.
Greene JP, Lefebvre SL, Wang M, et al. Risk factors associated with the development of chronic kidney dis-ease in cats evaluated at primary care veterinary hospitals. J Am Vet
Med Assoc 2014;244:320-327.
Early signs of chronic kidney disease:
Are we looking hard enough?
T ese “Journal Scan”
summaries were
contributed by Jen-
nifer L. Garcia, DVM,
DACVIM, a veterinary
internal medicine spe-
cialist at Sugar Land
Veterinary Specialists
in Houston, Texas.
Read more summaries
at dvm360.com
/JournalScan.
ES519841_vetm1114_342.pgs 10.27.2014 20:05 ADV blackyellowmagentacyan

ES521254_VETM1114_343_FP.pgs 10.29.2014 00:06 ADV blackyellowmagentacyan

Hear all
about it!Listen to Dr. Scott-
Moncrieff explain
why monitoring for
diabetic remission is
crucial by scanning
the QR code
below or by visiting
dvm360.com/
CVC14remission.
CVC highLight
344 | November 2014 | Veterinary Medicine | dvm360.com
A look at which factors might make spontaneous normalization of glycemic control more likely in one of your feline patients. By J. Catharine Scott-Moncrief, MA, Vet MB, MS, DACVIM, DECVIM
A unique feature of
diabetes mellitus in
cats is that some cats
become non-insulin-dependent
after treatment has been initi-
ated. From 17% to 67% of cats
with diabetes mellitus have been
reported to go into spontaneous
clinical remission after insulin
treatment is initiated.1-4
Diabetic remission is usu-
ally defned as normoglycemia
that persists for more than
four weeks without the use of
exogenous insulin,2 although
some studies have defned it as
euglycemia for only two weeks.5,6
Te duration of remission var-
ies, with some cats requiring
insulin treatment again within a
few weeks to months and other
cats remaining in remission for
months to years.
Factors that have been
hypothesized to infuence the
likelihood of diabetic remission
include the duration of diabetes
mellitus, whether the cat initially
presented in a ketoacidotic crisis,
the carbohydrate content of the
diet, the type of insulin used for
treatment, the cat’s breed, the
presence of underlying disease,
and how closely the blood glu-
cose concentration is maintained
within the normal range with
insulin treatment. Stimulation
tests with secretagogues such as
glucagon and arginine have also
been investigated to identify cats
that have residual insulin secre-
tion from the pancreas, but the
presence of glucose toxicosis in
cats complicates the interpreta-
tion of these tests, and they have
not proved useful in predicting
the likelihood of remission.7,8
In a study of factors infuenc-
ing diabetic remission in cats,
remission was found to be more
likely with increasing age and
increasing cholesterol concen-
tration.2 Overall, 21 cats treated
with insulin glargine and 23 cats
treated with Lente insulin went
into remission. A slightly higher
percentage of cats (53%) treated
with insulin glargine went into
remission than cats treated with
Lente insulin (47%).
Influence of dietIt has been proposed that low-
carbohydrate diets increase the
chance of diabetic remission in
newly diagnosed diabetic cats.
A prospective study comparing
a low-carbohydrate, low-fber
diet to a moderate-carbohy-
drate, high-fber diet in 63
diabetic cats showed improve-
ments in glycemic control in
both groups, but there was a
higher rate of remission of dia-
betes mellitus in the low-carbo-
hydrate, low-fber diet.6 Tese
fndings support the clinical
opinion that low-carbohydrate
diets in conjunction with good
glycemic control increase the
likelihood of diabetic remission.
If diabetic remission occurs in
cats, it is most commonly in the
frst few months of treatment.
Influence of insulinIt has been shown that strict
glycemic control is important
in achieving diabetic remission,
and it is clear that diabetic cats
can go into remission with any
insulin (e.g. Lente, protamine
zinc [Prozinc—Boehringer
Ingelheim Vetmedica], insulin
glargine) if good glycemic con-
trol is achieved. Many clinicians
What infuences
in catsdIabetIC remIssIon
ES519846_vetm1114_344.pgs 10.27.2014 20:16 ADV blackyellowmagentacyan

CVC highLight
Getty ImAGes/DsGpro dvm360.com | Veterinary Medicine | November 2014 | 345
believe that cats have better
glycemic control with long-act-
ing insulins (protamine zinc or
insulin glargine), so most clini-
cians recommend these insulins
as the initial insulin choice for
treatment in diabetic cats.
It is currently unclear wheth-
er some long-acting insulin
formulations are more likely to
result in remission than others,
or whether the critical factor is
the glycemic control itself. In
a study of 24 newly diagnosed
diabetic cats treated with either
glargine, protamine zinc, or
Lente insulin and fed a low-
carbohydrate, high-protein diet,
a higher rate of diabetic remis-
sion occurred in the cats treated
with insulin glargine than in
the cats treated with protamine
zinc or Lente insulin. However,
because of the limitations of this
study, further studies in larger
groups of diabetic cats are re-
quired to confrm this fnding.5
Influence of clinical presentationAlthough presentation in a
diabetic ketoacidotic crisis was
thought to occur predominant-
ly in cats with type I diabetes
mellitus, suggesting that cats
with diabetic ketoacidosis
should not go into remission, a
recent study documented that
some cats that initially pre-
sented with ketoacidosis can go
into remission with adequate
glycemic regulation and control
of concurrent illness.9
other factorsOther factors that have been
documented to increase the
likelihood of diabetic remission
in cats include1,2
> A short duration of diabetes
mellitus (< 180 days)
> Administration of glucocorti-
coids before diagnosis
> A low insulin dose required
to achieve glycemic control
> A lack of polyneuropathy
> An older age
> A lower cholesterol
concentration.
Sex, body weight, presence
of renal failure, presence of
hyperthyroidism, or presence
of obesity at diagnosis have not
been shown to infuence the
likelihood of remission.1
Diabetic remission tends
to last longer in cats of higher
body weight.2 Serum concen-
trations of glucose, fructos-
amine, insulin, glucagon, and
insulin growth factor 1 are not
diferent between cats that do
and do not achieve remission,
but cats achieving remission
have a higher glucagon-to-
insulin ratio.7,10Vm
reFerenCes
1. roomp K, rand J. Intensive blood
glucose control is safe and effective in
diabetic cats using home monitoring and
treatment with glargine. J Feline Med
Surg 2009;11(8):668-682.
2. Zini e, Hafner m, osto m, et al. predic-
tors
of clinical
remission in cats with
diabetes mellitus. J Vet Intern
Med 2010;24(6):1314-1321.
3. michiels L, reusch Ce, Boari A, et al.
treatment of 46 cats with porcine lente
insulin—a prospective, multicentere study.
J Feline Med Surg 2008;10(5):439-451.
4. roomp K, rand J. evaluation of detemir
in diabetic cats managed with a protocol
for intensive blood glucose control. J
Feline Med Surg 2012;14(8):566-572.
5. marshall rD, rand Js, morton Jm.
treatment of newly diagnosed dia-
betic cats with glargine insulin improves
glycaemic control and results in higher
probability of remission than protamine
zinc and lente insulins. J Feline Med Surg
2009;11(8):683-691.
6. Bennett N, Greco Ds, peterson me, et
al. Comparisons of a low carbohydrate-low
fiber diet and a moderate carbohydrate-
high fiber diet in the management of
feline diabetes mellitus. J Feline Med Surg
2006;8(2):73-84.
7. tschuor F, Zini e, schellenberg s,
et al. remission of diabetes mellitus
in cats cannot be predicted by the
arginine stimulation test. J Vet Intern Med
2011;25(1):83-89.
8. Nelson rW, Griffey sm, Feldman eC,
et al. transient clinical diabetes in cats:
10 cases (1989-1991). J Vet Intern Med
1999;13(1):28-35.
9. sieber-ruckstuhl Ns, Kley s, tschuor F,
et al. remission of diabetes mellitus in cats
with diabetic ketoacidosis. J Vet Intern Med
2008;22(6):1326-1332.
10. Alt N, Kley s, tschuor F, et al. evalua-
tion of IGF-1 levels in cats with transient
and permanent diabetes mellitus. Res Vet
Sci 2007;83(3):331-335.
J. Catharine Scott-Moncrief, MA,
Vet MB, MS, DACVIM, DECVIM
Department of Veterinary
Clinical Sciences
School of Veterinary Medicine
Purdue University
West Lafayette, IN 47907
ES519847_vetm1114_345.pgs 10.27.2014 20:16 ADV blackyellowmagentacyan

Gossypiboma-induced tumor peer-reviewed
346 | November 2014 | Veterinary medicine | dvm360.com
This potentially deadly surgical complication is preventable. Let this case report remind you about—and reinforce the importance of—counting surgical sponges. By A. Catherine Peace, DVM, and Michael W. Riggs, DVM, PhD, DACVP
A5-year-old 82.3-lb
(37.3-kg) spayed Ger-
man shepherd was
presented to a referral center for
evaluation of lethargy, constipa-
tion, tenesmus, dysuria, and in-
appetence. Te dog had ingested
rib bone and cartilage within
fve days of presentation. It also
had reportedly had a subjective-
ly distended abdomen since a
cesarean section and ovariohys-
terectomy were performed two
years prior to presentation.
INITIAL FINDINGSAt presentation, the
patient was bright,
alert, and responsive
and had an elevated
body temperature of
102.8 F (39.3 C). Te
dog’s heart rate was
168 beats/min, its
mucous membranes
were tacky, and it
was estimated that
the dog was 5% to 7%
dehydrated. Te dog’s
abdomen was tense
and distended. No
other signifcant fnd-
ings were identifed.
A serum chemis-
try profle revealed
hyperglobulinemia,
hyperphosphatemia, hypo-
natremia, hyperkalemia, and
decreased lipase activity. A
complete blood count revealed
neutrophilia, monocytosis, and
leukocytosis (see Table 1 at
dvm360.com/gossypiboma
for specifc values).
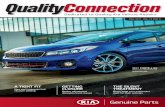
Two-view abdominal radiog-
raphy demonstrated decreased
serosal detail (Figures 1 & 2). An
approximately 18-x-17-x-14-cm
soft tissue opacity was visual-
ized in the right cranioventral
abdomen, displacing the stom-
ach in a craniodorsal direction
and the intestines caudally.
An approximately 8-x-1-cm
folded, linear, mineral-opaque
foreign structure was in close
association with and possibly
within the abnormal-appearing
opacity.
Relevant fndings from an
abdominal ultrasonographic
examination included a large
volume of focculent ascites and
an approximately 12-cm-wide
cystic structure that contained
additional focculent fuid and
Gossypiboma-induced abdominal fbrosarcoma in a German shepherd
>>>1 & 2. Right lateral and ventrodorsal abdom-inal radiographs reveal-ing a round soft tissue opacity (edges marked by black arrows) and a linear mineral-opaque object in the cranial abdomen (white arrow).
2
1
ES519854_vetm1114_346.pgs 10.27.2014 20:20 ADV blackyellowmagentacyan

CALL 800.255.6864, ext. 6 CLICK TheCVC.com EMAIL [email protected] FOLLOW
© 2015 Advanstar Veterinary CVCAT024
A member of the dvm360 family of veterinary resources
dvm360 dvm360.com veterinary medicine veterinary economics firstline
ourapproach
to the delivery of
veterinarycontinuing education
is so simple it’s...
tunity to earn CE credits.
ses, and workshops centered
est Coast, or Midwest location to suit
vention atmosphere
alking distance of your
egistration options to meet your available time and interests.
vention.
e free
or special savings.
ES514616_VETE1114_INSERT1_FP.pgs 10.09.2014 00:00 ADV blackyellowmagentacyanPerforation

MAXIMUM CE IN MINIMUM TIME
¡ A schedule built to maximize your opportunity to earn CE credits.
More than 500 hours of courses over 4 days.
¡ Exceptional programming, led by the industry’s most
accomplished educators and experts.
¡ Seminars, Clinical Techniques Courses, and workshops centered
on speaker interaction.
¡ RACE-approved programming; New York State-approved
CE provider.
SIMPLE TO P LAN AND TO NAVIGATE
¡ Select an East Coast, West Coast, or Midwest location to suit
your available time and budget, each with a convention atmosphere
conducive to your learning experience.
¡ Enjoy dining and entertainment within easy walking distance of your
hotel and convention venues.
¡ Build a program that best meets your needs.
REGISTRATION AND TRAVEL COSTS THAT MAKE SENSE.
¡ Registration options to meet your available time and interests.
¡ Breakfast, lunch, and snacks provided onsite at the convention.
¡ Hotel prices negotiated to save money and add extras like free
internet and discounts on food and parking.
Take a break
from the
traditional.
Try CVC’s
unconventional,
attendee-centric
approach to
veterinary
continuing education
conventions.
CALL 800.255.6864, ext. 6 CLICK TheCVC.com EMAIL [email protected] FOLLOW
Which CVC will you choose?
Don’t wait! Visit thecvc.com for details. Register now and use Priority Code CVCAT024 for special savings.
ES514615_VETE1114_INSERT2_FP.pgs 10.09.2014 00:00 ADV blackyellowmagentacyanPerforation

MAXIMUM CE IN MINIMUM TIME
¡ A schedule built to maximize your opportunity to earn CE credits.
More than 500 hours of courses over 4 days.
¡ Exceptional programming, led by the industry’s most
accomplished educators and experts.
¡ Seminars, Clinical Techniques Courses, and workshops centered
on speaker interaction.
¡ RACE-approved programming; New York State-approved
CE provider.
SIMPLE TO P LAN AND TO NAVIGATE
¡ Select an East Coast, West Coast, or Midwest location to suit
your available time and budget, each with a convention atmosphere
conducive to your learning experience.
¡ Enjoy dining and entertainment within easy walking distance of your
hotel and convention venues.
¡ Build a program that best meets your needs.
REGISTRATION AND TRAVEL COSTS THAT MAKE SENSE.
¡ Registration options to meet your available time and interests.
¡ Breakfast, lunch, and snacks provided onsite at the convention.
¡ Hotel prices negotiated to save money and add extras like free
internet and discounts on food and parking.
Take a break
from the
traditional.
Try CVC’s
unconventional,
attendee-centric
approach to
veterinary
continuing education
conventions.
CALL 800.255.6864, ext. 6 CLICK TheCVC.com EMAIL [email protected] FOLLOW
Which CVC will you choose?
Don’t wait! Visit thecvc.com for details. Register now and use Priority Code CVCAT024 for special savings.
ES514615_VETE1114_INSERT2_FP.pgs 10.09.2014 00:00 ADV blackyellowmagentacyanPerforation

CALL 800.255.6864, ext. 6 CLICK TheCVC.com EMAIL [email protected] FOLLOW
© 2015 Advanstar Veterinary CVCAT024
A member of the dvm360 family of veterinary resources
dvm360 dvm360.com veterinary medicine veterinary economics firstline
ourapproach
to the delivery of
veterinarycontinuing education
is so simple it’s...
tunity to earn CE credits.
ses, and workshops centered
est Coast, or Midwest location to suit
vention atmosphere
alking distance of your
egistration options to meet your available time and interests.
vention.
e free
or special savings.
ES514616_VETE1114_INSERT1_FP.pgs 10.09.2014 00:00 ADV blackyellowmagentacyanPerforation

Gossypiboma-induced tumor peer-reviewed
dvm360.com | Veterinary medicine | November 2014 | 347
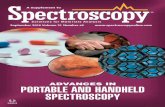
material with a hyperechoic
appearance (Figure 3). A sample
of the ascites was collected via
abdominocentesis for evaluation
in-house by the veterinarian.
Tis fuid had a serosanguineous
appearance with a total protein
concentration of 3 g/dl, specifc
gravity of 1.025, a packed cell
volume of 5%, and a glucose
concentration of 132 mg/dl.
Microscopic evaluation revealed
red blood cells and nondegener-
ate neutrophils. No intracellular
or extracellular bacteria were
seen. Aerobic culture of the
abdominal fuid was negative for
growth after 72 hours.
Although not performed in
this case, further evaluation of
the ascites by a pathologist can
yield critical diagnostic infor-
mation. Specifcally, a difer-
ential cell count is required to
classify the efusion into a tran-
sudate or exudate. Additionally,
a more through microscopic
evaluation or sedimentation
examination may have resulted
in information regarding the
focculent material noted dur-
ing the ultrasound.
DIFFERENTIAL DIAGNOSESTe main diferential diag-
nosis at this time was cystic
encapsulation of foreign
material located outside of the
gastrointestinal tract. Potential
causes included gossypiboma,
penetrating injury, or migration
of ingested foreign material.
EXPLORATORY LAPAROTOMYAn abdominal ex-
ploratory surgery was
performed. Numerous
fbrous adhesions were
found throughout the
entire abdomen. Te
cystic structure had
a frm capsule that
adhered to the stomach, spleen,
intestines, and peritoneum. Te
small intestines were adhered
together and were sequestered
to the caudal abdomen. Te
intestinal serosa was bright red,
and fbrous adhesions covered
all serosal surfaces. No intesti-
nal motility was noted.
Te small intestinal adhe-
sions were dissected by using a
combination of bipolar electro-
cautery and digital manipula-
tion. Te abnormal tissue was
removed en masse and saved
for histologic examination. A
Jackson-Pratt drain was placed
in the abdomen and secured
with 3-0 Prolene (Ethicon)
suture in a Chinese fnger-trap
pattern. Te abdomen was
lavaged and drained before clo-
sure. Anesthesia and recovery
were uneventful.
POSTOPERATIVE CAREA 75-μg fentanyl patch (2 μg/
kg cutaneously) was placed for
continuous analgesia. Postop-
erative care included admin-
istering a balanced hypotonic
crystalloid fuid (150 ml/hr
intravenously), hydromorphone
(0.1 mg/kg intravenously q.i.d.
as needed for pain), cefazolin
(22.7 mg/kg intravenously
t.i.d.), and tramadol (4 mg/kg
orally b.i.d.).
Te Jackson-Pratt drain was
maintained for an additional
two days and was emptied every
two to four hours during that
time. Te fuid volume collected
ranged from 640 to 750 ml (17
to 20 ml/kg) per 24-hour period.
Te drain was removed three
days after surgery. Te pa-
tient’s vital signs were normal
at that time, and the dog was
discharged to its owners later
that day.
SECOND PRESENTATIONTirteen days after the surgery,
the patient was presented to the
referral center for evaluation of
weakness, persistent vomiting,
and anorexia. Te admitting
physician assessed the patient
to be hypovolemic. Te dog
exhibited pain upon palpation
of the abdomen.
Hospitalization and diag-
nostic testing to determine
the cause of the vomiting and
>>>3. An ultrasono-gram revealing a large fluid-filled cyst and hyperechoic shadow. The edges of the cyst are marked by red ar-rows, and the shadowing representing the foreign material is marked by a white arrow.
3See larger versions
of all the images
in this article at
dvm360.com
/gossypiboma.
ES519855_vetm1114_347.pgs 10.27.2014 20:19 ADV blackyellowmagentacyan

Gossypiboma-induced tumor peer-reviewed
348 | November 2014 | Veterinary medicine | dvm360.com
supportive care to control the
clinical signs were recommend-
ed and declined. Te owners
said that they had previously
discussed euthanasia because
of the dog’s deterioration and
would request that service from
the referring veterinarian. How-
ever, the patient died at home
the day after its last evaluation
at our referral center.
HISTOLOGIC
EXAMINATION
Te abdominal cyst was fxed in
10% neutral bufered formalin
and submitted to the University
of Arizona Veterinary Diagnos-
tic Laboratory for examination.
Gross examination revealed a
fbrous-connective-tissue-
encapsulated cystic mass con-
taining a largely intact cotton
gauze foreign body and green
metal radiographic marker strip
surrounded by fbrinohemor-
rhagic exudate, consistent with a
gossypiboma (Figures 4A & 4B).1
Sections of the cyst capsule
and its contents were prepared
and processed routinely and
stained with hematoxylin and
eosin for histologic examination.
Histologically, the cyst capsule
was composed principally of
organizing fbrous connective
tissue containing multifocal lym-
phocytic aggregates and areas
of mineralization. Numerous
longitudinal and cross-sectional
profles of clear refractile fbrillar
foreign material were embed-
ded in the inner aspect of the
capsule and present in the lu-
men. Individual fbers contained
a hollow core and had collective
morphologic features consistent
with cotton fbers. Cotton fbers
were surrounded by amorphous
eosinophilic matrix and cellular
debris within the lumen (Figure
5) and by numerous macro-
phages within the inner aspect
of the capsule.
Multifocally, within the
capsule, there was an infltra-
tive population of moderately
pleomorphic polygonal-to-
spindle-shaped neoplastic cells
arranged in bundles, transition-
ing from areas of fbroplasia
(Figures 6A & 6B). Neoplastic
cells contained large ovoid-
to-spindle-shaped nuclei with
prominent nucleoli and were
invested within eosinophilic
stroma with indistinct cytoplas-
mic borders. Tere was an aver-
age of fve mitotic fgures per
10 400X-magnifcation felds.
Multiple extracapsular venules
contained emboli composed of
neoplastic cells similar to those
in the wall but having greater
pleomorphism and higher mi-
totic activity (Figures 6C & 6D).
Immunohistochemistry
revealed that neoplastic cells in
both the capsule and venules
were strongly positive for vimen-
tin expression and negative for
smooth muscle actin expression,
consistent with a fbrosarcoma.
DISCUSSION
Te term gossypiboma is de-
rived from the Latin gossypium,
meaning cotton, and the sufx
-oma, meaning growth. It is a
general term used to refer to
surgical equipment or textiles
accidentally left in a body cavity
>>>5. A photomicro-graph of the foreign body matter in the cystic lumen. Note the multiple longitudinal and cross-sectional profiles of clear refractile fibers (arrow) surrounded by amorphous eosinophilic matrix and cellular de-bris. The hollow core of individual fibers and oth-er morphologic features is consistent with cotton (hematoxylin-eosin stain; bar = 50 μm).
>>>4A. The opened cystic mass after partial fixation in formalin. Note the irregular fibrous connective tissue capsule, cystic cavity, and fibrinohemorrhagic exudate with embedded cotton gauze foreign matter along the inner aspect of the capsule. >>>4B. The contents of the cystic mass after partial fixation in formalin. Note the largely intact cotton gauze foreign body and green metal marker strip (arrow), consistent with a retained laparotomy towel.
4
5
ES519856_vetm1114_348.pgs 10.27.2014 20:19 ADV blackyellowmagentacyan

Gossypiboma-induced tumor peer-reviewed
dvm360.com | Veterinary medicine | November 2014 | 349
after surgery. Reports of granu-
lomas and malignant tumors
induced from surgically derived
foreign material are infrequent-
ly reported in the veterinary
and human medical literature.
Reported cases To our knowledge, this case
report is only the second report
involving the development of
an intra-abdominal fbrosar-
coma associated with a sponge
gossypiboma in a dog.2 Case
reports regarding malignant
tumors in the human medical
feld include the development
of angiosarcoma3,4 and nu-
merous other sarcoma types.4
Veterinary reports include the
development of an extraskeletal
osteosarcoma in a dog5 and
fbrosarcoma development in a
cat6 and in a mouse model.7
An accurate frequency of oc-
currence of gossypiboma is im-
possible to determine given the
lack of standardized reporting
mandates and asymptomatic
nature of most veterinary cases.
Induction of a malignant tumor
by a gossypiboma is likely to
represent only a small percent-
age of this population.
In veterinary reports, foreign
bodies have been inadvertently
left behind during cranial cruci-
ate ligament repair,5 ovariohys-
terectomy (elective or pyome-
tra),2,6,8-11 laparotomy (retained
testicle or intestinal biopsy),11
and wound repair11 but frequent-
ly did not induce a malignancy.
Although several case reports
involved fabric-derived foreign
material inadvertently left at the
time of surgery, other foreign
bodies frequently reported are
metal and are the result of trau-
matic events (bullet, shrapnel,
wire) or medical implants.4
Models to determine the
carcinogenic properties of sur-
gically implanted sterile foreign
material have been developed
in animals.7,12 Te surface of
the implanted foreign material
is soon covered with plasma
proteins and surrounded by
neutrophils, lymphocytes, and
monocytes. Te monocytes
diferentiate into macrophages
and form multinucleated giant
cells, making up most of the
cells surrounding the foreign
material.12 Eventually a fbrous
connective tissue capsule forms
around the foreign material to
create a microenvironment for
the proliferation of abnormal
mesenchymal stem cells,
making this microenviron-
ment possibly the most
important determinant
of transformation into a
neoplastic process.3,4 Te
generation of free radicals3
and mutation of normal
cells appear to play a role in
the perpetuation of chronic
infammation and the even-
tual development of tumors
and is described in detail
elsewhere.12-14
Clinical signs of gossypibomaPatients may not become
symptomatic for weeks
to years, and discovery is
often incidental.6,8,11,15,16 In
symptomatic cases, reported
clinical signs have included
vomiting and diarrhea11;
depression, weight loss,
and anorexia10; infection,
abdominal cramping, and
>>>6A. A photomicrograph of a fibrosarcoma arising in the cyst capsule and invading venules. Note the infiltra-tive population of neoplastic cells arranged in bundles, transitioning from areas of fibroplasia within the cyst capsule. Arrows indicate the interface between fibroplasia and neoplasia (hematoxylin-eosin stain; bar = 200 μm). >>>6B. A photomicrograph of higher magnification of the neoplastic tissue noted in Fig-ure 6A. Note the polygonal-to-spindle-shaped neoplastic cells containing large ovoid-to-spindle-shaped nuclei with prominent nucleoli and indistinct cytoplasmic borders invested within eosinophilic stroma. Also note the mitotic figure (arrow) (hematoxylin-eosin stain; bar = 50 μm). >>>6C. A photomicrograph of a representative tumor embolus in an extracapsular venule (hematoxylin-eosin stain; bar = 200 μm).>>>6D. A photomicrograph of higher magnification of the tumor embolus depicted in Figure 6C. Note the high mi-totic rate and pleomorphism. Also note the mitotic figures (arrows) (hematoxylin-eosin stain; bar = 50 μm).
6
ES519857_vetm1114_349.pgs 10.27.2014 20:19 ADV blackyellowmagentacyan

Gossypiboma-induced tumor peer-reviewed
350 | November 2014 | Veterinary medicine | dvm360.com
small bowel obstruction16; and
hematuria and pain.8 Physical
examination fndings have in-
cluded swelling, a palpable ab-
dominal or subcutaneous mass,
and draining sinus tracts.5,9,11,15
ImagingA gossypiboma can be discov-
ered and confrmed by using
a combination of imaging
modalities including radiogra-
phy,5,11 ultrasonography,10,11,17
fstulography,9 computed
tomography,17 and magnetic
resonance imaging.18
Radiographic fndings can be
unremarkable if a gauze foreign
body does not contain radi-
opaque material similar to what
was seen in this case.9 Te most
frequent radiographic fnding
in a case series of eight dogs
with retained surgical sponges
was a localized gas lucency that
appeared either speckled or in
a whirl-like confguration.11 In
another case study, the gauze
foreign body was diagnosed
when radiopaque mono-
flaments within the surgical
sponge were observed during
survey radiography of the af-
fected limb.12
If survey radiographs are
nondiagnostic, then an ultraso-
nographic examination of the
afected area or abdomen can
be performed. Reports of the
ultrasonographic appearance
of a foreign body have varied
and include an ill-defned mass
with acoustic shadowing,9 a hy-
perechoic mass,15 a mass with
a hypoechoic outer layer and
a hyperechoic inner layer with
acoustic shadowing seen deep
to the mass (for an encapsu-
lated mass),10 and a hypoechoic
mass with an irregular hyper-
echoic center.11 Te fndings
in this report included echo-
genicities that were consistent
with encapsulated, hyperechoic
abnormal material and fuid.
Masses may be associated with
granulomas, abscesses, calcif-
cation, or gas pockets, and the
acoustic shadowing for each
will difer.10
Treatment and preventionSurgery is the treatment of
choice to remove any foreign
material and any abnormal tis-
sue with which it is associated.
Adhesions found throughout
the abdomen complicated the
complete removal of all ab-
normal tissue in this case. Te
severity of the adhesions found
in this case is not uncommon
and has been reported in other
cases involving the bladder and
small intestines8 and the jeju-
num, colon, arteries, kidneys,
and ureter.18
Te aggressive nature of the
foreign body-associated tumor
described in this case report
underscores the importance of
appropriate surgical technique,
including accurate preopera-
tive and postoperative sponge
counts. Risk factors associ-
ated with a gossypiboma in
people include an unplanned
procedure, distractions in
the operating gallery, poor
communication between the
technical staf and surgeons,
staf changes, patient obesity,
and surgeries performed on an
emergency basis.16 Although
veterinary studies to evaluate
specifc risk factors are lacking,
these events should be consid-
ered risk factors in veterinary
patients as well.
Standardized processes for
communication and for ac-
counting for all instruments,
laparotomy towels, and gauze
and an established protocol
to further investigate missing
materials are simple strategies
that can prevent this surgical
complication. Furthermore,
the use of radiopaque markers
embedded within laparotomy
towels and gauze can facilitate
the rapid discovery of a re-
tained surgical foreign body by
using survey radiography.
A. Catherine Peace, DVM
BluePearl Specialty and Emergency
Medicine for Pets
11950 W. 110th St.
Overland Park, KS 66210
Michael W. Riggs, DVM, PhD,
DACVP
Veterinary Diagnostic Laboratory
School of Animal and Comparative
Biomedical Sciences
University of Arizona
Tucson, AZ 85705
View the references
for this article at
dvm360.com
/gossypiboma.
ES519866_vetm1114_350.pgs 10.27.2014 20:20 ADV blackyellowmagentacyan

social media
Managing your social media in
1 hour per week
A special monthly package
designed to help boost client
compliance and make it
easy for your team to educate
pet owners about regular
pet wellness care.
November 2014 | dvm360.com/toolkit
Your social media tools:
PLU
S
p2
Team handoutA social media policy for your
practice
>> PLUS 4 social media
mistakes you DON’T
want to makep04
Facts & fi guresWhat your peers think about
social media—and how they
actually use itp05
Videos>> Dr. Ernie Ward on how team
members help make your
clinic’s social media successful
>> Drs. Andy Roark and Dave
Nicol with the top 10 ways to
blow it on social media
>> Dr. Andy Roark on the
importance of being funny to
increase engagementp06
Marketing tool>> Prewritten posts and
tweets on annual exams
>> The comprehensive
post & tweet topicsp07
Take Action>> Easy video ideas
for YouTube
>> Handout: Help clients
show love for your clinic p08
Get social!
Social media is here to stay—and in order to see and be seen,
you have to participate! For expert ideas on how to get started,
fi nesse your current strategy, or avoid common mistakes, head
over to dvm360.com/socialtoolkit.
ES517516_dvmtoolKit1114_001.pgs 10.21.2014 19:02 ADV blackyellowmagentacyan

2 | November 2014 | dvm360.com/toolkit
social media
Your clients are using Facebook, Twitter and LinkedIn. If you want them to see you, use these 6 steps to manage your presence. (And stop wasting your time!)
There is no doubt that
people today are looking
online for their veteri-
nary care providers. Tat being
said, there is also a valid need
to expend marketing resources
wisely. With that in mind, here
is a six-step plan for maintain-
ing a useful social media pres-
ence by devoting just one hour
per week. Let’s get started.
1 Set reasonable expectationsJust like with a work-
out routine, you can’t expect
to put in minimal time and get
herculean results. However,
focusing your eforts in an ef-
cient, meaningful way can give
you results in the long term.
You shouldn’t expect to get
thousands of fans, but rather to
communicate with—and stay
in the minds of—people who
may actually bring their pets to
you for care. You’re going for
quality in your connections,
not quantity.
2 Remember your brandYes, the photo of the
cat smoking a pipe you saw on
the Internet may have been hi-
larious, but is that the picture
you want associated with your
clinic? Every post or tweet you
put out should ft the brand
image you want to build in
people’s minds. If in doubt,
err on the side of caution and
come across as caring and
professional.
3 Pick a platformIt’s better to have a sin-
gle, well-run presence
than a half-dozen neglected
and disorganized eforts that
all make you look bad.
For most practices, I recom-
mend a Facebook business
page. Te other social media
sites are great, but Facebook
is easy to learn. It’s also the
largest network by far, and
the number of posts you need
to stay visible is manageable.
Facebook’s recommendation
system also helps put your
page in front of people who
live in your geographic area,
and that’s a big plus.
4 Find your contentNo one wants to
see you pitching your sales
and services 24/7. Tey want
follow your practice because
you share information that’s
interesting, educational, help-
ful, funny and engaging. You
should give them what they
want (with a moderate dose of
information about your prac-
tice, of course).
One easy way to do this is
to let other people create the
content and deliver it to you so
that you can share the best of
it with your own clients. Email
newsletters are a wonderful
way to get articles, blog posts
and videos delivered right to
your inbox. Some of the best
media outlets you can sub-
By Andy Roark, dvm
1 hour a weekManage your social media in
Dr. Andy Roark is the
founder/managing
director of veterinary
consulting frm Tall
Oaks Enterprises,
LLC. Check him out
on Facebook or
@DrAndyRoark
on Twitter.
ES517567_dvmtoolKit1114_002.pgs 10.21.2014 20:37 ADV blackyellowmagentacyan

dvm360.com/toolkit | November 2014 | 3
social media
scribe to are from the AVMA,
(gratuitous plug alert!) dvm360.
com and ASPCA Poison
Control. When you need great
content for your social media
outlet, voila!
5 Use a schedulerNow that you have
clear goals, your brand
on your mind, and a host of
helpful, funny, interesting, edu-
cational and engaging content
that you’re ready to share, it’s
time to take action.
First, schedule one hour per
week as social media time.
Ten create a plan for what
content you want to put out
over the next seven days. Use a
web-based program to sched-
ule your posts automatically at
designated times.
My favorite scheduler is
Hootsuite (hootsuite.com). Us-
ers can write their posts, attach
fles or links, and then set the
date and time for the informa-
tion to appear on Facebook,
Twitter and other outlets. It’s
free to use, and once you decide
how often you want to put out
information, you can set your
entire week in a single sitting.
Te greatest activity on Face-
book is on weekdays at 3 p.m.,
followed by 11 a.m. and 8 p.m.
Wednesday at 3 p.m. is consis-
tently the busiest time in the
week, while Sunday is the slow-
est day. Keep these patterns in
mind when deciding how best
to schedule your posts.
6 Monitor what’s happeningOnce your social media
initiative is up and rolling,
you can’t take your hands
totally of the wheel. You
must be responsive when
clients communicate
through your social media
channel. Have notifca-
tions about client com-
ments sent to your clinic
via a regularly checked
email address. And decide
up front who will address
these comments.
When clients reach out in
this way, don’t panic. You don’t
have to respond immediately,
like you would if they showed
up in person. Twenty-four
hours (48 on a weekend) is a
good response time and won’t
leave clients feeling ignored.
Like global warming and
Justin Bieber, social media is an
unstoppable force. It’s undeni-
ably changing and improving
the way we communicate with
pet owners. Even if you have
the
most
cutting-
edge medical
practice, you run
the risk of seeming
outdated without a presence in
social media. So carve out an
hour a week to log in and have
fun with it. Ten get back to the
work of being a vet.
Ready-made content makes your “social” life a breeze
cut down your time spent by using the prewritten
posts and tweets from dvm360. You’ll find client-
facing posts and tweets on topics including pain
management, behavior and nutrition—just to name
a few! copy and paste the content right into your
Hootsuite account, scheduling it out at your leisure.
check it out at dvm360.com/postnow or go to page 7
of this toolkit for examples.
geTTY ImAges/eseNkArTAL
ES517566_dvmtoolKit1114_003.pgs 10.21.2014 20:37 ADV blackyellowmagentacyan

4 | November 2014 | dvm360.com/toolkit
SOCIAL MEDIA
BoundariesComputer, email, and Internet usage:
Veterinary Specialty Care’s e-mail and Internet must
be used in an ethical and professional manner. E-mail
and Internet access may not be used for transmitting,
retrieving, or storing communications of a defama-
tory, discriminatory, or harassing nature or materials
that are obscene or X-rated. Messages with deroga-
tory or inflammatory remarks about an individual’s
race, age, disability, religion, national origin, physical
attributes, or sexual preference shall not be transmit-
ted. Abusive, offensive, or profane language in trans-
missions as well as harassment of any kind is strictly
prohibited.
Electronic communications sent on our computers
are considered hospital property and are not guaran-
teed to be private or confidential. Veterinary Specialty
Care reserves the right to examine and monitor files,
emails, and Internet usage. Do not download files
from the Internet and do not open files if you do not
know the sender.
Employees must not transmit copyrighted materi-
als on the practice’s network. Staff must respect all
copyrights and may not copy, retrieve, modify, or
forward copyrighted materials. If you wish to share
something of interest on the Internet with others,
do not copy it to a network drive. Instead, supply the
URL (uniform resource locator, or “address”) for the
recipient to look at.Veterinary Specialty Care has a strict social media
policy. Unless specifically authorized by the hospital
administrator, you are not permitted to blog or use
other forms of social media or technology on the In-
ternet during working hours. Tis applies to personal
electronic and mobile devices, as well. Tese actions
can include, but are not limited to:• Video or wiki postingsª Personal or professional blog postings
• Chat room conversations• Facebook updates
• MySpace updates• Twitter updates• YouTube searches and videosVeterinary Specialty Care recognizes and encourages
your rights to self-expression and the use of social
media on your own time. Please be aware of, and
follow these professional guidelines for independent
self-expression:• Bloggers are personally responsible for their
commentary.• Employees cannot use the Internet to harass,
threaten, discriminate against, or disparage other
employees or anyone associated with the Veterinary
Specialty Care. Negative statements about Veteri-
nary Specialty Care, its products and services, its
team members, its clients, or any other related entity
may lead to disciplinary action up to and including
termination of employment. In addition, appropriate
legal action may be taken if warranted.
• Employees who identify themselves as employees of
any of Veterinary Specialty Care must state that the
views expressed are their own and not those of Vet-
erinary Specialty Care or of any person or organiza-
tion affiliated with Veterinary Specialty Care
• Employees cannot post the name, trademark, logo,
or any other privileged information associated with
Veterinary Specialty Care or any business connect-
ed to Veterinary Specialty Care. Tis includes post-
ing advertisements and selling hospital products.
• Employees cannot post photographs or videos of
clients, vendors, other team members, suppliers
or people engaged in business or events without
express written consent and authorization from the
hospital administrator.• Employees cannot link to internal or external web-
sites without obtaining written permission.
• Veterinary Specialty Care reserves the right to use
content management tools to monitor, review, and
block content on hospital blogs and websites that
violate Veterinary Specialty Care Internet and Social
Media rules and guidelines.
Internet usage and Social media policy for Veterinary Specialty Care
To download this policy and
more, just head over to
dvm360.com/socialtoolkit.
Set the team on the right social-media track at your practice with
this customizable policy.
As everybody dives
into the world of
online networking
and social media, you need to
be sure your team members
know their boundaries when
it comes to talking about
work on the web. Try cus-
tomizing this sample policy
for your practice.
4 social media mistakes you DON’T want to make
1Humble pie
When owners of Amy’s Baking
Company went on Gordon Ramsay’s
“Kitchen Nightmares” show, it got hot
in the kitchen. In addition to the fi ery
on-air exchanges between Ramsay
and the restaurateurs, the show
aired footage that made the owners
seem downright nutty. They took
to social media sites to explain—or
rather hysterically rant—their side
of the story. The couple’s postings
went viral and caused an enormous
backlash, forcing the restaurant to
close for several days.
2 Post politics
There are many stories about
employees accidently posting their
personal views. That’s what hap-
pened when a Kitchen Aid employee
discussed his negative opinion of
President Obama. This accident cost
the tweeter his job and proved to
be a mess for Kitchen Aid that took
weeks to clean up.
3 McMayhem
In 2012 McDonalds asked
customers to post their stories
about McDonalds using the hashtag
#mcdstories. And customers came
through. In just two hours, there
were more tales of unhealthy food
and bad service than calories in a
Big Mac. This tweet proved to be the
real fat in the fryer.
4 TMI FTW!
Imagine one manager’s surprise
when her veterinarian turned in her
notice ... on Facebook! It was against
company policy and TMI for this
DVM’s online followers. The resulting
swirl of online traffi c had prospective
employers gasping OMG.
KNOWING THE
For your own
customizable
version of this
tool, go to
dvm360.com/socialtoolkit.
ES517528_dvmtoolKit1114_004.pgs 10.21.2014 19:04 ADV blackyellowmagentacyan

dvm360.com/toolkit | November 2014 | 5
SOCIAL MEDIA
SOURCE: DVM360’S “WHAT VETERINARIANS THINK” STUDY, 2014.
77% 81%of survey respondents
own a smartphone.
Of those 77%,
of social media users use one or more
of these platforms: Facebook, Twitter,
Pinterest, Google+, LinkedIn, YouTube,
Instagram.
For millenials, this jumps to 96.7%
63%use their smartphone
for social media.
This is what they use those platforms to do:
42%
Top answer
from men: To
educate and
connect with
veterinary clients.
49%
Top answer from women:
To connect with
veterinary peers.
40% use social media
several times a day
6% use social media
once a week
60% use Facebook both
personally and professionally
38% use YouTube both personally
and professionally
Let’s say your practice Facebook
page receives 200 Likes this
month. If the average Facebook
user has 234 friends, that’s
46,800 potential exposures for
your business—for free.
Your clients, on social
Each month, 800 million unique users visit
YouTube and 72 hours of video are uploaded
every minute. In 2011, YouTube had more than 1
trillion views, or around 140 views for every per-
son on Earth. More than half of videos on YouTube
have been rated or include comments from the
community. For every click on dislike, YouTube
videos get 10 likes.
200 LIKES
1 TRILLIONVIEWS
by the numbersWhat veterinarians thinkdvm360 conducted
a survey of nearly
3,000 veterinarians and
team members, asking
them to evaluate their
information sources.
Why do theybother?
ES517554_dvmtoolKit1114_005.pgs 10.21.2014 19:33 ADV blackyellowmagentacyan

6 | November 2014 | dvm360.com/toolkit
SOCIAL MEDIA
Scan the QR
codes below
with your
smartphone to
watch these
videos now.
No phone handy? No problem.
The videos are ready to watch at
dvm360.com/socialtoolkit.
Watch and learn: Social media made easyWherein cute cat photos can actually save lives.
If our experts agree on one thing, it’s that social media is one of the most powerful business tools
you have at your disposal. It can be a very ef cient way to connect with clients. Best of all? It’s
FREE. So take these tips to heart and watch your business boom.
Involve the teamDr. Ernie Ward explains how team members are
crucial to the success of the clinic’s social media
presence, because team members are the source of
much of the content. Expanding team members’ roles
as content creators will add authenticity and precision
to your social media strategy.
Focus on the funnyIt’s easy to be goofy on Facebook and Twitter, but
not for business, right? Actually, Dr. Andy Roark
says humor fosters the elusive, magical word that
everybody’s after: engagement. By increasing your
funny and otherwise likeable posts and tweets, you
ultimately do a better job of spreading your message.
Don’t blow it Drs. Dave Nicol and Andy Roark are experts at
applying social media in the world of veterinary
medicine. It just so happens that the two are also
experts at playing bumbling novices. Here they
demonstrate the top 10 ways to blow it on social
media. Do you see any similarities to the way your
clinic handles online interaction?
ES517574_dvmtoolKit1114_006.pgs 10.21.2014 20:47 ADV blackyellowmagentacyan

dvm360.com/toolkit | November 2014 | 7
SOCIAL MEDIA
dvm360’s social media marketingUse your social media network to stress the importance of these preventive care topics to your client base.
The dvm360.com team wrote Facebook posts and tweets for your
team to use to raise awareness of key health care issues with your
clients and to help you encourage clients to visit and get the care
their pets need. Get started today by visiting dvm360.com/postnow
and copying the prewritten posts and tweets on these topics:
Scan the QR code
to send this tweet
right now!
If we haven’t seen your pets all year,
then painful conditions could be going
undetected and untreated. Set up an
appointment today so we can be sure
everything is A-OK.
Myth #245: Indoor cats don’t need
preventive care. Schedule Roxy’s annual
exam and we’ll set the record straight.
#pet #pethealth #petcare
When was the last time we saw your
#pet? The more we see your cat or dog,
the sooner we can detect problems.
#petcare
When you don’t bring your pets in for
regular exams, we can’t spot conditions
like heartworm disease or kidney failure.
Set up a time so we can examine your
cat or dog.
Annual exams
>> Adopting a pet
>> Canine aggression
>> Important vaccinations
>> Feline dental care
>> Itchy ears
>> Cat stats, facts & folklore
>> Pain prevention
>> Ways to pay
>> Fleas
>> Year-round fl ea and tick
protection
>> Older pets’ failing senses
>> Inappropriate elimination
>> Life stages
>> Holiday pet hazards
>> Fear free veterinary visits
>> Puppy & kitten care
>> Dermatology
>> Fun pet facts
... and many, many
more!
Check out these posts and tweets about annual exams
GETTY IMAGES/ISTOCKPHOTO
ES517562_dvmtoolKit1114_007.pgs 10.21.2014 19:52 ADV blackyellowmagentacyan

One more tip
Most of our new clients now fi nd
us on the web and potential clients
search reviews and compare the
“star” ratings of each hospital. Writ-
ing those reviews isn’t always easy,
and there are many steps involved.
To encourage reviews we make
it as easy as possible by giving a
brochure to clients that gives them
step-by-step instructions on how to
write a review for our clinic.
—Robert Henrickson, DVM
Manhasset Animal Hospital
Manhasset, N.Y.
FROM YOUR VETERINARIAN
REVIEW US! I
f you love our service, let others know! We’d appreciate your online feedback. To make it easy, we’ve put together this handout that details the steps needed to leave a review on the most popular online review sites. Thank you!
1 Visit yelp.com and find our business using the search bar at the very top of the page. Narrow results by using our exact business name and city.
2 Click on our business page, and click the “Write a review” button.
This button is located underneath the business’ address, telephone number and website.
3 Select a rating for your overall experience of our clinic. Use the
scale they give you (the ratings range between 1 star and 5 stars). The submissions will not let the review be posted without a rating.
How to post a Google review:
1 To write a Google
review you will need a free Google account.
2 To post a review,
Google the name of our clinic.
3 On the right side of the page
you will see reviews that have already been written.
4 Click the “Write
a review” button under clinic’s name.
5 Log in to your Google
account and type your review into the field provided.
6 Just click the
“publish” button and you’re finished!
How to post a Yelp! review:
4 Understand the star ratings. To help you out, as you hover over the rating box, there will be several words that will help you explain your rating. Click the star-rating you believe should best match the conditions of your upcoming review.
5 Write your review, based on the rating you gave it. Below the review, you’ll find a place to write a text-based review-box.
6 Decide if you would like to share this review with (not only your Yelp friends, but also on Facebook). Below this, you’ll find a box to share this with all of your friends on Facebook. In another tab, open and log in to Facebook, then return to this review in this other tab (make sure you save your email for future use). Once again on this checkbox, click the box to place a checkmark in the box.
8 | November 2014 | dvm360.com/toolkit
EASY VIDEO IDEAS for YouTube
Help clients show love for your clinic
SOCIAL MEDIA
Give a hospital tourHave your most charismatic employee give a brief
walking tour of your hospital, from the front desk
through the exam rooms and into the treatment area.
Shoot your video while the hospital is open for business
so viewers can see your team in action. T en, post it
on your practice website and on your Facebook feed.
Ask your Facebook friends to share the video so their
friends can see what your hospital looks like.
Showcase your equipmentNarrate steps while taking dental x-rays and then have
a doctor describe the f ndings. Show what ear mites
look like under the microscope. Make a video of a
technician performing preanesthetic testing. And teach
with instructional videos for clients—show clients how
to brush pets’ teeth, clean ears, give pills and trim nails.
Promote what’s newWelcome a new doctor or staf member with a brief
video interview about his or her areas of medical
interest, expertise and family pets, then post it on the
“About our practice” page on your website, and tweet
a link to that page. If you start of ering a new drug, ex-
plain what it does for pets. If your practice does board-
ing and grooming, show of your suites and describe
the pampering pets will get. Invite people to drop in
for a personal tour. Even if the service isn’t brand new,
showing it on video makes it feel fresh.
This instructional handout for clients explains
how to post a review on the two of the most
popular platforms, Google and Yelp. To download
your copy, visit dvm360.com/socialtoolkit.
TAKE ACTION:
ES517538_dvmtoolKit1114_008.pgs 10.21.2014 19:16 ADV blackyellowmagentacyan

Anger can spill into veterinarians’
relationships with nonprofi t shelters
and rescues, so we’re trying to heal
the divide with information and
advice here and in the pages of our
sister magazines this month ...
Can this relationship be saved?
A close look at the contentious
relationship between private
practice and nonprofi t groups—
plus where there’s more
collaboration than competition.
The war is over. Find out how
one practice wins clients with a
closer relationship with a local
rescue group.
Come together. Get updates on
the veterinary technician shelter
medicine specialty as well as
tips on how shelter and practice
team members work together
to protect pets in need.
dvm360.com | Veterinary Medicine | November 2014 | 351
SHELTER MEDICINE:
A view from both sidesGet the inside story of one veterinarian’s transition to shelter medicine and, along the way, let’s debunk common myths that some private practitioners hold about shelter practice—and vice versa.
Editor’s note: We cor-
responded with Frank
Bossong, DVM, an
active leader in shelter
medicine in the South-
ern California area,
to get a view of what
practice is like from
both sides of this issue.
Dr. Bossong started his
career in general practice and then became the
staff veterinarian at the San Gabriel Valley Hu-
mane Society in San Gabriel, California. In 2009,
Dr. Bossong became an assistant professor at the
College of Veterinary Medicine at Western Uni-
versity of Health Sciences in Pomona, California,
where he has assisted the college in expanding
and improving its curriculum in shelter medicine.
Q: You started out in private prac-
tice at an AAHA-certifi ed practice.
What prompted your switch to
working in a shelter?
A: I had thought about working in
a shelter setting when I f rst gradu-
ated from the University of Georgia
College of Veterinary Medicine, but
I felt that it would be best as a new
graduate to work at a clinic that prac-
ticed “best medicine” so that I could
develop a solid surgery and medicine
background. After four years out in a
multidoctor practice, I felt conf dent
enough to go out on my own. Al-
though I loved my clients, I felt that
the majority of my time was spent with
the owners in comparison to the time I
was actually spending with their pets; I
felt like I wanted to focus more on the
animals. I also had a client who started
to bring shelter animals for me to see
at the clinic. She was trying to help the
local shelter out. My bosses allowed
me to provide these shelter dogs and
cats with veterinary care and even
discounted the services they received.
A year or so later, I was beginning
to see more shelter patients (unfor-
tunately, the discounts ended). I also
became more aware of the multiple
ILLUSTRATION BY GABRIEL UTASI
ES519879_vetm1114_351.pgs 10.27.2014 20:39 ADV blackyellowmagentacyan

Leadership challenge
352 | November 2014 | Veterinary Medicine | dvm360.com
problems these animals were
facing at the shelter. Te shelter
had no registered veterinary
technicians and no veterinarian.
Te facility also had a very bad
reputation for housing sick and
undesirable animals and had a
high euthanasia rate.
On the fourth anniversary of
my starting date at the clinic, I
began to do some soul search-
ing and felt like I wanted to
dedicate most of my time to
the animals that seemed to be
in desperate need of care. I also
had received a complaint from a
Shelter medicine educational resources> Most major veterinary con-
ferences offer lectures
in shelter medicine. (Join
Cynthia Karsten, DVM, from
the UC Davis Koret Shelter
Medicine Program during
the CVC in Washington, D.C.,
April 23-28, 2015.)
> The UC Davis Koret Shelter Medicine Program
(sheltermedicine.com) has extensive online
resources such as a shelter medicine lecture series,
information sheets, and a reference library.
> The University of Florida has an online course that
provides CE credit and work toward a graduate cer-
tificate in shelter medicine at sheltermedicine
.vetmed.ufl.edu/certificate-programs/online.
> The Association of Shelter Veterinarian’s website,
sheltervet.org, provides information on how to
apply for certification in shelter medicine and
additional resources and guidelines for medical
and surgical care of shelter animals. At sheltervet
.org/smoc you’ll find details regarding shelter
medicine’s official recognition as the newest
veterinary specialty.
client who was concerned about
one of the shelter animals being
in the same lobby as her pet.
Tis was the catalyst for one of
those “clear-life moments” and
I decided I would approach the
director of the shelter to see if
they would hire me as their staf
veterinarian. Tis was 2005, and
in 2001, when I graduated from
veterinary school, I had never
taken a shelter medicine course
and I did not even really see it
as a separate discipline. I simply
wanted to use my veterinary
skills at a facility that needed
some assistance.
Q: What were the reactions
of your colleagues when you
made this decision?
A: My bosses and colleagues
were initially shocked when I
turned down the ofer to renew
my contract for another year. I
had a large clientele and I had
associates that I really loved
working with and respected.
One of my associates was also
a very good mentor. Te sal-
ary was competitive and the
facility was upscale. At frst my
bosses were worried I was leav-
ing to open my own practice.
When I told them where I
was going they initially looked
relieved and then seemed a
little surprised. My colleagues
gave me the impression that I
was making a mistake and that
the facility that I was going to
would refect badly upon me as
a veterinarian. Tey also were
shocked at the signifcant pay
cut I was going to be receiving.
More surprising was the
reaction of my clients. Some
were angry that I was leav-
ing. Some clients requested to
follow me to receive services at
the shelter. Others thought that
I must have been fred or did
something wrong to be going
to a “dirty shelter” and leaving a
well-regarded AAHA-certifed
practice. I did have one client
say that she was “not surprised”
and was very supportive of me
“helping more animals.” She was
the only one.
Q: What did you find
when you started working
at the shelter?
A: Let’s just start by saying that
you can’t make the really shock-
ing stuf up. Where do I begin?
Te place was a real mess. Te
poor reputation was not totally
unfounded. Te place had been
mismanaged for years by highly
unqualifed individuals. A do-
nor to the facility had been the
one to push for my hire.
During the frst several weeks
I was totally overwhelmed. My
frst shock was that none of the
controlled drugs at the prem-
ises were properly locked away.
Tere was an open drawer near
the euthanasia room—a room
that looked like it was out of a
Stephen King novel. When I
opened the drawer, several par-
tially used bottles of euthanasia
solution rolled to the front of
the drawer and about 20 pages
of “logged-out drugs” fell to the
ES519875_vetm1114_352.pgs 10.27.2014 20:39 ADV blackyellowmagentacyan

ES521253_VETM1114_353_FP.pgs 10.29.2014 00:06 ADV blackyellowmagentacyan

A healthy relationshipSee how
Cavanaugh Pet
Hospital in Blue
Springs, Missouri,
has found its
relationship with
local shelter and
rescue groups
rewarding for
all involved by
scanning the QR
code below or by
visiting dvm360.
com/cavanaugh.
Leadership challenge
354 | November 2014 | Veterinary Medicine | dvm360.com
foor. By the end of my frst day,
I had called and made an ap-
pointment with someone from
the local DEA ofce to stop
by and advise me. Tey were
very helpful and supportive in
getting things in order before I
registered my license there.
On my frst surgery day,
I was using an anesthesia
machine from the 1950s.
Tere was no pulse oximeter,
and I was assigned one kennel
worker to assist me. Tere
were canister rolls of cat gut
and stainless steel for suture
material. Ironically, the surgical
packs were OK and are still
in use today; I was told they
had been donated. Tere was
no pharmacy to speak of and
equipment was limited (e.g. no
microscope, no otoscope).
Tere were no designated
isolation areas for sick animals.
Tere was a room called “infr-
mary” and one called “isolation,”
but there was so much junk and
such unclean (many wooden)
cages that they were essentially
unusable. In one of the back
rooms, I was presented with 20
to 30 boxes of sharps in open
Styrofoam containers. I was
told that Stericycle had stopped
coming a year or so prior (the
account had not been renewed
or kept current). One of the
staf had covered everything
with Christmas decorations!
I had to be careful in ad-
dressing these issues with the
administrators at the time. I
was successful in working out
an arrangement with a medical
waste company to address this
situation. I, also, at a later date,
invited OSHA to the facility
after convincing the “powers
that be” that they were not
the enemy but rather there to
protect us all by ensuring a safe
work environment.
In addition to the shortcom-
ings of the physical plant, I
think the biggest shock was
how untrained and unmoti-
vated most of the staf was.
Te well-attended area was the
smoking area. Animals were
not being properly screened on
intake. Tere was no standard
operating procedure (SOP) for
performing a health examina-
tion or determining an animal’s
sex (I did witness two dogs mat-
ing at a later date). Shots were
sometimes given, sometimes
not. I scanned animals that had
been impounded for weeks and
found microchips and started
calling their owners.
Without any formal shelter
training, my frst impulse (com-
mon sense) was to deliver some
basics to the staf. I started
with training the staf to follow
through on what I called the
three Ss: determine Sex, Scan
for a microchip, and give ap-
propriate Shots upon intake. A
more formal protocol on han-
dling intake evolved from there
as did additional training. Te
animal control ofcers were
sent to Sacramento for certifed
euthanasia training.
I realize in retrospect that
many other area shelters were
not in such a bad state of afairs
as this one. Somehow these
transgressions were overlooked
by many individuals in the
area for quite some time. I was
surprised that no intervention
had occurred sooner, although
most of these issues were not in
public view.
Q: How is everything
at the shelter today?
A: I am pleased to say that the
facility has and is continuing
to make real progress. When
I left as the staf veterinarian
about six years ago, there was a
change in the board of direc-
tors, and a complete change in
the management immediately
followed. I joined the board at
this time and remain a com-
mitted board member. During
my three years there as the
staf veterinarian, I managed to
MORE RESOURCES> dvm360’s complete Leadership Challenge
coverage: dvm360.com/workingwithshelters
> Humane Society of the United States:
> Maddie’s Institute: maddiesinstitute.org
> ASPCA—free webinars recorded and posted
along with slides and materials at
aspcapro.org/training
> State Humane Association of California—
webinars, euthanasia training, and more:
californiastatehumane.org/training.htm
> Pet Smart Charities: learning@
petsmartcharities.org
> VIN, Veterinary Information Network—
consultation, courses, webinars: vin.com
ES519877_vetm1114_354.pgs 10.27.2014 20:39 ADV blackyellowmagentacyan

See Dr. Bossong’s
thoughts on his
shelter’s relation-
ship with his
community today
and more in an
extended version
of this Q&A at
dvm360.com
/shelterQA.
Leadership challenge
hire the facility’s frst registered
veterinary technician (there are
now three). Te surgical suite
was updated, and the facility
provides low-cost spay and
neuter for the public and covers
the majority of the surgical pro-
cedures needed by the shelter
animals they serve. We opened
a low-cost vaccine clinic as well.
Within the last year, the
facility fnally transitioned
from paper records to a shelter
software system. Te mission
statement and bylaws have been
updated and restated, and we
have expanded our board. We
have a website up and running.
Tere are many written SOPs
for managing infectious disease,
cleaning and disinfection, vac-
cination, medical treatments,
etc. Proper euthanasia proto-
cols have been established and,
that being said, the shelter is
at the point where no “healthy
adoptable” animals are put to
sleep. Te shelter now has an
active volunteer program and
they work with local registered
veterinary technician programs
and the shelter club at the local
veterinary school. Much of the
staf has received continuing
education to improve their skills
in serving the animals under
their care. I’m really excited that
the facility has survived and is
being managed by ethical, car-
ing employees and volunteers.
Q: How is practicing shelter
medicine different from
general practice?
A: I think the main diference
is that sometimes you have
to make a decision about an
animal that is in the best inter-
est of the group or herd rather
than the individuals themselves.
I could give so many examples
here. Tis can vary from facility
to facility in terms of the care
that a given shelter can aford to
ES519878_vetm1114_355.pgs 10.27.2014 20:39 ADV blackyellowmagentacyan

Leadership challenge
356 | November 2014 | Veterinary Medicine | dvm360.com
Shelters are taking away business from private practice.Most clients who come to a shelter for surgeries or
vaccinations would not go to a general practice be-
cause of their fi nancial limitations. By providing these
services, shelters decrease the numbers of litters
entering their facility—thus decreasing the euthana-
sia rate—and the vaccinations help to protect the
community from disease outbreak (public health).
Medical protocols that occur at shelters are usually “second rate.”If you think of the sheer volume of surgeries done
at the shelter by a licensed veterinarian, you might
accept the notion that a shelter veterinarian might
become even more profi cient at these procedures.
Additionally, as more veterinarians train to become
shelter veterinarians, those training them make the
point that “best medicine” should be practiced in all
facilities—both private practice and shelters alike.
Shelter veterinarians are at shelters because they could not handle private practice or were not particularly good veterinarians.Many shelter veterinarians started out in private
practice or still participate part time in private
practice. Some might say that working at a shelter
is a calling, if you will, or vocation. I am now seeing
young graduates who are associates in a private
practice taking part-time positions at shelters be-
cause they want to make a difference.
Shelter and herd health protocols don’t apply to private practice.How often have we seen a kennel cough outbreak
at a private practice that does “medically supervised
boarding”? Any time we have groups of animals
congregated in a limited space, we can be faced
with herd health issues. I personally have learned so
much more about proper cleaning and disinfection
protocols because of my continuing education in
shelter medicine. I think back to my private practice
days and now realize I could have done a better
job in this regard and that much of this information
would also benefi t the animals entering a private
practice facility.
Shelter medicine only involves spays, neuters, and vaccinations.It involves so much more—population management,
shelter facility design and operation, sanitation,
preventive healthcare, diagnosis and management
of infectious disease, animal behavior and welfare,
issues and policies regarding euthanasia, public
relations, adoption strategies, fundraising, abuse in-
vestigation, veterinary forensics, public health—and
the list goes on.
A shelter veterinarian has to euthanize a lot of animals.From my own experiences and from the dozen or so
shelters I work with in my area, shelter veterinarians
are busy with so many other tasks that the technical
staff and animal control offi cers perform the
majority of euthanasia. Certainly there
are times, as in general practice,
where the veterinarian is
performing these procedures.
Personally I euthanized more
animals out in private practice
than I have as a shelter veterinar-
ian. This being said, I realize I have
been fortunate to work with many
shelters that have lower than national
average euthanasia rates.
TOP MYTHS ...
… private veterinary practitioners have about shelters
ES519880_vetm1114_356.pgs 10.27.2014 20:39 ADV blackyellowmagentacyan

Leadership challenge
dvm360.com | Veterinary Medicine | November 2014 | 357
… shelter workers have about private veterinary practitioners
Most of the time better medicine and surgery occurs out in private practice.Just because the building is a shelter
does not mean that the veterinarian prac-
ticing there needs to change how they
approach a surgical or medical workup. A
well-funded facility can refer cases as well
when appropriate.
Private practitioners are only in it for the money.In order for a shelter or a private practice
to remain in business, services need to
generate fees so that expenses can be
covered. Even shelters charge the cities
they serve fees for animal control services.
Low-cost vaccine and surgery services
have fee schedules as supplies need to
be purchased and medical staff paid. The
whole veterinary community—private and
nonprofi t—must show fi nancial sustainabil-
ity to remain in business.
Private practitioners resent the local shelters as they are fi nancial competition.Many private practices, especially those
providing emergency coverage, often have
partnerships with local shelters. Some
private practitioners provide overfl ow cov-
erage for shelters when necessary. Some
specialists donate their skills or lower the
cost of services for special cases.
give. T e shelter uses the Asilomar
Accords for assessing the animals
that come into their care. An
“unhealthy, untreatable” animal
for this shelter, for example, is
a parvo-positive dog showing
clinical signs. For other facilities
this may be “treatable rehabilitat-
able.” However, this shelter does
not have the funding, medi-
cal oversight, or physical plant
(adequate isolation) necessary to
treat that other facilities might. In
this scenario, the shelter humanely
euthanizes to protect further
spread of infection to the rest of
the young animals in their care.
Out in practice, depending on the
resources of an owner, one usually
treats the individual—the clinician
in practice is generally not think-
ing of herd safety per se.
Ironically, in both private
practice and in a shelter setting
f nances play a role. Additionally,
a general practitioner could see
the rest of your clients (patients in
your care) as a herd so the isolation
and disinfection protocols should
be the same. Actually I think some
small-animal hospitals may have a
lot to learn from proper isolation
and disinfection protocols followed
at our more cutting-edge shelters.
Another big dif erence is that
in general practice, most people
consider their pets as part of the
family. Owners desire to keep
their pets healthy and attempt to
maximize their longevity. In the
shelter setting, a shelter veterinar-
ian is always considering how to
best manage the patients to get
them out of the shelter and into a
home as soon as possible while at
the same time protecting public
health and safety. We are dealing
with an “unwanted” population of
individuals rather than a “cher-
ished” group of dogs and cats. T e
shelter veterinarian’s goal is to
place as many of these shelter ani-
mals into the “cherished group” as
ef ciently as possible.
Q: What can veterinarians do
to connect with shelters in
their area, and why should
they make the effort?
A: Call, volunteer, become a
member of the board of directors.
Find out how your local shelter
impacts the health of the animals
in your community. One example
would be providing information
or insight regarding the early de-
tection of community outbreaks.
As a clinic owner, you could add
your clinic name to the shelter’s
list of veterinarians in the area for
new pet owners to choose from.
Your clinic could be a resource
for referrals such as radiology or
ultrasound (as many shelters lack
this equipment), emergency care,
or surgical overf ow.
I think it is critical for private
practitioners to establish a rela-
tionship with their local animal
control and/or humane society
so that they have a trusted re-
source if they are ever faced with
suspected animal abuse or public
health threats such as rabies or
even animal hoarding.
It is also important to remem-
ber that many of our shelter ani-
mals are your future patients!
ES519876_vetm1114_357.pgs 10.27.2014 20:39 ADV blackyellowmagentacyan

Products & Services SHOWCASE | dvm360.com/products
Se
arc
h f
or
the
co
mp
an
y n
am
e y
ou
se
e i
n e
ac
h o
f th
e a
ds i
n t
his
se
cti
on
fo
r FR
EE
IN
FO
RM
AT
ION
!
358 | November 2014 | Veterinary Medicine | dvm360.com
D E N T A L P R O D U C T S
Searchlebalab
ES521151_vetm1114_358_CL.pgs 10.28.2014 23:33 ADV blackyellowmagentacyan

dvm360.com | MARKETPLACE
dvm360.com | Veterinary Medicine | November 2014 | 359
ANESTHESIA EQUIPMENT
MEDICAL EQUIPMENT
dvm360.com
TAGS
Outdoor
Tradeshow/POP Displays
Direct Mail
Social Media
Print Advertising
Radio & Television
Marketing solutions ft for:
Logo Licensing • Reprints
Eprints • Plaques
Leverage branded content
from Veterinary Medicine to
create a more powerful and
sophisticated statement about
your product, service, or company
in your next marketing campaign.
Contact Wright’s Media to fnd
out more about how we can
customize your acknowledgements
and recognitions to enhance your
marketing strategies.
For more information,
call Wright’s Media at
877.652.5295
or visit our website at
www.wrightsmedia.com
Content
Licensing for
Every Marketing
Strategy
721 York St PO Box 72430Newport KY 41072-0430 USA
(859) 261-2035 Fax (800) 261-TAGS (8247)
Highest Quality, Faithful Service, Honest Values Since 1902
OnlineInteractiveOrderSystem
Follow us!
Get instant updates on
critical developments
in veterinary medicine,
business, and news by
following dvm360.
facebook.com/
dvm360
twitter.com/
dvm360
ES521150_vetm1114_359_CL.pgs 10.28.2014 23:33 ADV blackyellowmagentacyan

To view this
video, scan this
QR code or visit
dvm360.com
/SuperCarrier.
IDEA EXCHANGE tips from the trenches
360 | November 2014 | Veterinary Medicine | dvm360.com GETTY IMAGES/GREMLIN
Weekly photos illustrate
gradual changes in masses
Whenever I see a patient with a suspected benign
skin mass that will not be immediately biopsied, I
recommend that the owner take a weekly picture
of the mass with a ruler underneath it. Gradual change is often
unnoticed, but this weekly photo provides an objective way to
determine whether the mass is growing or shrinking. It is espe-
cially useful for those owners who want to try a benign-neglect
approach. Since most owners have a camera on their phones or
digital cameras, it is usually easy for them to comply.
Andrew G. Smith, DVM
East Ridge, Tennessee
Watch this easy way to demon-
strate for owners how to get
their cats into their carriers by
using the blind Superman technique.
Mike Karg, DVM
Frederick, Maryland
We need your ideas!
We’ll pay $50 for
regular submissions and
$75 for video
submissions that we
publish in print or online.
Email [email protected],
fax us at (913) 273-9876,
or write to Idea
Exchange
Editor at 8033
Flint, Lenexa, KS
66214.
Read the latest
Miller onlineThe secret to staying youngDr. Robert Miller shares
his inspiration for living life
to the fullest, regardless
of age. Find this and
previous columns by visiting
dvm360.com/Miller.
How to perform a
belt-loop gastropexy
dvm360.com/MedicineVideos
CAPC’s Tick of the Month:
Brown dog tick
dvm360.com/capc
Also online …
Faster than a speeding bullet,
the cat is in the carrier
ES519899_vetm1114_360.pgs 10.27.2014 20:42 ADV blackyellowmagentacyan

6
CALL 800.255.6864, ext. 6 CLICK TheCVC.com EMAIL [email protected] FOLLOW
THE CONTINUING EDUCATION YOU WANT
• Exceptional programming, led by the industry’s most
accomplished educators and experts
• A schedule built to maximize your opportunity to earn CE credits
WHERE YOU WANT IT
• Choose an East Coast, West Coast, or Midwestern location to
suit your available time and budget
• Each with a convention atmosphere conducive to your
learning experience
Try CVC’s unconventional, attendee-focused approach
to continuing education conventions.
CVC’s approach to the delivery of
continuing education
is so simple it’s
unconventional!
©Copyright Advanstar Veterinary, 2014 CVCSD14_AT017
ES521260_VETM1114_CV3_FP.pgs 10.29.2014 00:06 ADV blackyellowmagentacyan

© 2014 Virbac Corporation. All Rights Reserved. C.E.T., VEGGIEDENT, and
HEXTRA are registered trademarks of Virbac Corporation. 7/14 14805
C.E
.T.®
HO
ME DENTAL CA
RE
AL
C
OVER 25 YEARS
TAKE A SCIENTIFIC APPROACH
TO YOUR PATIENTS’ DENTAL HEALTH
C.E.T.® VEGGIEDENT® Tartar Control Chews for Dogs
Clinically proven to reduce plaque and calculus and freshen breath4
Great-tasting, free of animal protein and wheat gluten
Exclusive “Z” shape for effective mechanical cleansing
Supported by VOHC* Acceptance for Tartar Control
with the proven technology behind the
C.E.T.® Home Dental Care line of quality chews.
References: 1. Harvey CE, Emily P. Small Animal Dentistry. St. Louis: Mosby;
1993:122. 2. Pader M. Oral Hygiene Products and Practice. New York: Marcel
Dekker, Inc.; 1988. 3. Foulkes DM. Some toxicological observations on
chlorhexidine. J Periodontal Res Suppl. 1973;12:55–60. 4. Clarke DE, Kelman
M, Perkins N. Effectiveness of a vegetable dental chew on periodontal disease
parameters in toy breed dogs. J Vet Dent. 2011; 28(4): 230–235.
HELP REDUCE PLAQUE AND CONTROL TARTAR WITH . . .
C.E.T.® HEXTRA® Premium Chews for Dogs
The unique and proprietary binding-releasing system ensures maximal release
of chlorhexidine, the most effective antiplaque agent1, into a dog’s saliva that:
Readily binds to dental pellicle to exert localized antiseptic activity2
Has a wide margin of safety3
Has been widely accepted by veterinarians for years
Contact your Virbac representative, call 800-338-3659, or visit www.virbacvet.com.
* Veterinary Oral Health Council
ES521259_VETM1114_CV4_FP.pgs 10.29.2014 00:06 ADV blackyellowmagentacyan