Systemic Lupus Erythematosus
40
Systemic Lupus Erythematosus (SLE)
-
Upload
ishmael-callahan -
Category
Documents
-
view
30 -
download
1
description
Systemic Lupus Erythematosus. (SLE). OUTLINE. Definition Epidemiology Pathophysiology Clinical features Classification and diagnosis Treatment Prognosis Lupus related syndromes APS??. Definition. - PowerPoint PPT Presentation
Transcript of Systemic Lupus Erythematosus

Systemic Lupus Erythematosus
(SLE)

Definition Epidemiology Pathophysiology Clinical features Classification and diagnosis Treatment Prognosis Lupus related syndromes APS??
OUTLINE

Inflammatory autoimmune disorder affecting multiple organ systems characterized by the production of autoantibodies
Typically the course of the disease is a series of remissions and exacerbations.
Virtually any organ of the body may be involved, but most often harms the heart, joints, skin, lungs, blood vessels, liver, kidneys, and nervous system.
Definition

Prevalence influenced by age, gender, race, and geographical area◦ Prevalence=30-50/100000◦ Peak incidence 15-45 years◦ Female predominance-F:M=9:1
Can occur in childhood or later in life
Epidemiology

Immunologic anomalies
Genetic predisposition
Enviromental factors
Hormonal factors
Etiology

Genetic predisposition:HLA DR and DQ and non HLA
Enviromental factors: Ultraviolet light (especially UVB) Smoking Viral infections: Ebstein Baar virus Silica and mercury exposure Drugs Extreme stress Hormonal factors (female predominance):
estrogen

Pathophysiology

Sustained presence of autoantigens: increased apoptosis , impaired clearance of apoptosis
Hyperactivity in B and T lymphocyte. Increased expression of surface molecules
participating in cell activation in both B- and T-cell.
Overproduction of IL-6 and IL-10 Defective regulatory mechanism.
Abnormal immune system

Autoantibodies to DNA, RNA, and a host of other cell nucleus antigens.
Circulating immune complexes are frequently observed and these may deposit in the kidney, skin, brain, lung, and other tissues. It causes inflammation and tissue damage by a number of mechanism, notably fixation and activation of the complement system.

Skin cell
T cell T cell
B cell
APC
APC
Defective IC clearance
UV light
External AgSelf Ag
Ab
IC
Target
Gen
etic
su
scep
tibility



Fever Fatigue Weight loss Malaise = generally feeling ill Anorexia
General simptoms:

Cutaneous manifestations: LE-specific lesions can be classified into acute, subacute, and chronic. LE-non specific lesions:alopecia, urticarial lesions, vasculitic lesions,
sclerodactyly, livedo reticularis, Raynaud phenomenon. Musculoskeletal: arthritis, myositis, osteonecrosis. Cardiopulmonary involvement: pleurisy, pericarditis, Libman-Sacks
endocarditis, pulmonary hypertension, interstitial pneumonitis, coronary artery disease.
Renal manifestations: lupus nephritis (nephrotic syndrome in progresion to renal insufficiency and failure-renal biopsy VI classes of lupus nephritis. Histologic classification by renal biopsy is useful to plan therapy ), lupus cystitis.
Neuropsychiatric manifestations: psychosis, seizures, encephalopathy, coma, stoke, meningitis, peripheral neuropathy.
Gastrointestinal involvement: esophageal dysmotility, hepatomegaly, splenomegaly, mesenteric vasculitis.
Ocular features: secondary Sjogren syndrome, slcleritis, retinitis, uveitis.
Clinical features:

ANA - 95-100%-sensitive but not specific for SLE Anti -ds DNA-specific(60%)-specific for SLE, but positive to other
non lupus conditions 4 RNA associated antibodies
◦ Anti-Sm (Smith)-high dagnostic specifity for SLE◦ Anti Ro/SSA-antibody◦ Anti La/SSB-antibody◦ Anti-RNP
Antiphospholipid antibody◦ Biologic false + RPR◦ Lupus anticoagulant (antibodies to coagulation factors; risk factor for
venous and arterial thrombosis and miscarriage. Prolonged aPTT)◦ Anti-cardiolipin
Depressed serum complement Anti hystones antibodies
Immunological findings

American College of Rheumatology 4/11 criteria=diagnosis SLE“SOAP BRAIN MD” Serositis – heart, lung, peritoneum Oral ulcers – painless esp palate Arthritis – non-erosive Photosensitivity
Classification and diagnosis

Blood disorders - ↓RBC (Coombs +), PLT, WCC, Lymphocytes
Renal involvement ANA titer Immunologic phenomena – anti-dsDNA Ab, anti-
Sm Ab, antiphospholipid Ab, false WR + Neurological disorders Malar rash Discoid rash

1.Malar rash=fixed erithema,flat or raised over the malar eminences, tending to spare the nasolabial folds (“butterfly rash”)

Butterfly rash

2.Discoid rush=erythematous raised patches with adherent keratotic scaling and follicular plugging;atrophic scarring may ocur in older lesions
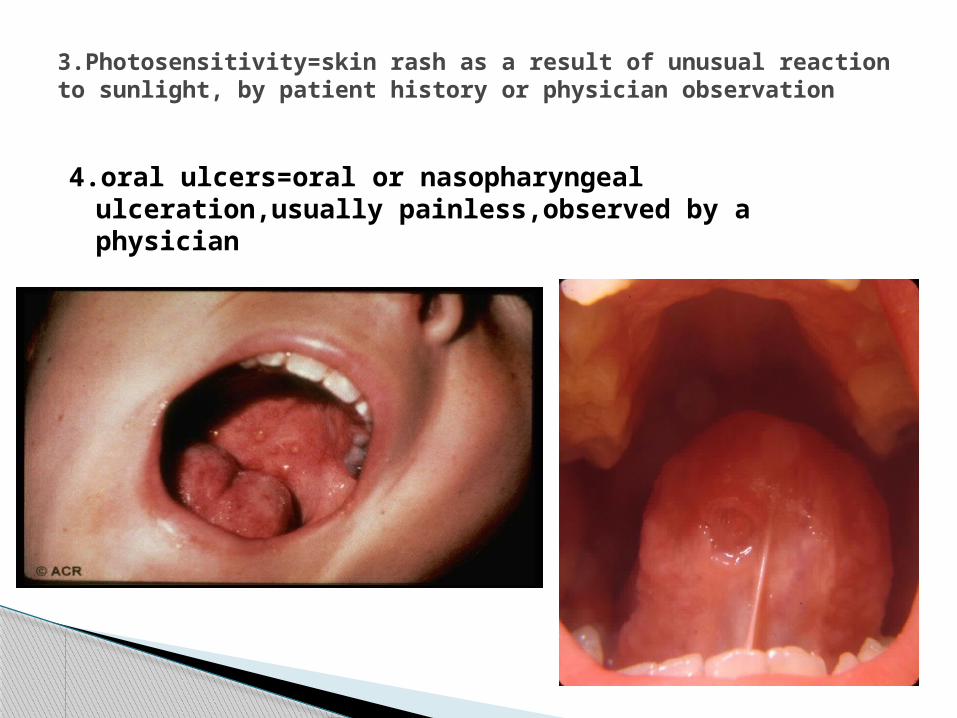
4.oral ulcers=oral or nasopharyngeal ulceration,usually painless,observed by a physician
3.Photosensitivity=skin rash as a result of unusual reaction to sunlight, by patient history or physician observation

Jaccoud’s Arthopathy: Nonerosive, Reduceble Deformities
5.arthritis=nonerosive arthritis involving two or more peripheral joints, characterized bt tenderness, swelling or effusion (RX: no erosions, periarticular osteopenia + soft tissue swelling)

7.renal disorder-proteinuria>0.5 g/day or >3+ dipstick proteinuria or cellular casts
8.neurologic disorder=seizures or psychosis in the absente of offending drugs or known metabolic derangements
9.hematologic disorder:-hemolytic uremia or-leukopenia <4000/mm3 on two or more occasions
or-lymphopenia<1500/mm3 on two or more
occasions or-thrombocytopenia<100,000/mm3 in the absence
of offending drugs
6.serositis-pleuritis=convincing history of pleuritic pain or rub heard by physician or evidence of pleural effusion or -pericarditis documented by EKG or rub or evidence of pericardial effusion

10.immunologic disorders:• Antibody to native DNA• Antibody to Sm• Positive test for antiphospholipid antibodies
including -abnormal Ig G or IgM anticardiolipin -lupus anticoagulant -fals-positive serologic test for syphilis (WR)11.Positive antinuclear antibodies (ANA) in the
absence of drugs known to be associated with drug-induced lupus

Must have 4 of 11 for Classification◦ Sensitivity 96%◦ Specificity 96%
Like RA, diagnosis is ultimately clinical Not all “Lupus” is SLE
◦ Discoid Lupus◦ Overlap syndrome◦ Drug induced lupus◦ Subacute Cutaneous Lupus
Clinical diagnosis?!?

SLE disease activity index (SLEDAI)
Clinical feature score
seizure , psychosis , organ brain syndrome 8 visual disturbance, cranial nerve disorder 8 lupus headache, cerebrovascular accidents, 8 vasculitis 8 arthritis 4 myositis 4 urinary casts, hematuria, proteinure, pyuria 4 rash, alopecia, mucosal ulcers, 2 pleurisy, pericarditis 2 low complement, increased DNA binding 2 fever 1 thrombocytopenia, leucopenia 1
Monitoring the lupus pacients

Drug-induced lupus Other connective tissue diseases: RA,
dermatomyositis, overlap syndrome Fibromyalgia Some Viral infections: parvovirus,
HIV,hepatitis B or C Malignancy
Differential diagnosis

1. SLE complications: Renal failure occurs in lupus nephritis Strokes can occur from active central nervous system lupus 2. Glucocorticoid complications: Cataracts Osteoporotic fractures Osteonecrosis Diabetes mellitus Infections Cushingoid habitus Weight gain Acne franck depression
3.Opportunistic infections: until proved otherwise,consider infection in a pacient with SLE who is febrile
4. Malignancy.
Complications

Treatment plans are based on patient age, sex, health, symptoms, and lifestyle
Goals of treatment are to: -prevent flares -treat flares when they occur -minimize organ damage and complications
1.Lifestyle changes avoiding direct sunlight, covering up with sun-protective clothing, and
using strong UVA/UVB sunblock lotion can also be effective in preventing photosensitivity problems.
weight loss is also recommended in overweight and obese patients to alleviate some of the effects of the disease, especially where joint involvement is significant
avoiding infections,extreme stress or fatigue Avoiding drugs lupus-like effect (procainamide,
hydralazine,methyldopaisoniazid).
Treatment SLE

NSAIDs Antimalarials Glucocorticoids immunosuppressive agents : -azathioprine 1-2 mg/kg/day
-mycophenolate mofetil 500-1500mg/day
-methotrexate: 20 mg/week Cyclosporine Intravenous immunoglobulin therapy Rituximab ?!? Belimumab
2.Drug theraphy

NSAIDs have been used with success for the management of SLE manifestations such as fatigue, constitutional symptoms, musculoskeletal complaints, and serositis.
In contrast to antimalarial drugs there is no evidence that NSAIDs
reduce the risk of flare nor is there a rationale for administering them
chronically in the absence of symptoms Adverse effects of NSAIDs: renal insufficiency resulting from decreased glomerular filtration, impairment of blood
flow, and, occasionally, interstitial nephritis; hepatitis; fluid retention; hypertension and development of gastric and duodenal
NSAIDs

The antimalarial drugs (hydroxychloroquine, chloroquine, and quinacrine) are the mainstay of management for mild to moderately severe lupus and are also indicated as adjunctive therapy of severe lupus and to prevent flares.
The major complication: ocular toxicity!! These drugs appear to have several favorable effects on
thrombotic and cardiovascular risk.
Plaquenil 200-400 mg/day
Antimalarials

Corticosteroids are the mainstay of initial treatment of active lupus requiring prompt treatment.
Corticosteroids rapidly suppress the majority of inflammatory disease manifestations if given in sufficient quantity
Improvement is generally more rapid than the response to immunosuppressive or antimalarial drugs.
Corticosteroids

Mild cases (mild skin or joint involvement): NSAID, local treatment, hydroxy-chloroquin
Cases of intermediate severity (serositis, cytopenia, marked skin or joint involvement): corticosteroid (12-64 mg methylprednisolon), azathioprin, methotrexat
Severe, life-threatening organ involvements (carditis, nephritis, systemic vasculitis, cerebral manifestations): high-dose intravenous corticosteroid + iv. cyclophosphamide + in some cases: plasmapheresis or iv. immunoglobulin, or, instead of cyclophosphamide: mycophenolate mofetil
Some cases of nephritis (especially membranous), myositis, thrombocytopenia: cyclosporine
Immunosupresive drogs


Unpredictable course 10 year survival rates exceed 85% Most SLE patients die from infection,
probably related to therapy which suppresses immune system
Prognostic

APS is an autoimmune multisystemic disorder of recurrent thrombosis and/or pregnancy losses that is associated with the presence of antiphospholipid (aPL) antibodies.
50% of pacients with SLE have APS. Clinical findings: Cutaneous: livedo reticularis, superficial thrombophlebitis, leg
ulcers Cardiopulmonary: pulmonary emboli and pulmonary infarcts,
miocardial infarctation, Libman Scks endocarditis. Gastrointestinal:hepatic or splenic infarcts, Budd-Chiari syndrome Neurologic: Transient ischemic attacks or strokes Endocrinologic: adrenal insufficiency Reproductive:pregnancy losses, preeclampsia,HELLP syndrome. Optic neuropathy
Antiphospholipid Antibody Syndrome (APS)

Vascular thrombosis-arterial,venous or small vessel ORPregnancy morbidity One or more fetal deaths One or more premature births due to severe preeclampsia or
placental insufficiency Three or more first trimester losses PLUS one of laboratory criteria:
1. False-positive test for syphilis?!???2. Lupus anticoagulant
3. Anticardiolipin4. Anti beta2 glycoprotein 1
APS is present if at least one of the clinical criteria and one of the laboratory criteria are met.
APS Classification criteria

◦ Anticoagulation with warfarin (teratogenic)◦ subcutaneous heparin and aspirin is usual
approach in pregnancy
Treatment APS

Thank you