progression of avascular necrosis of femoral head and choice of ...

Systemic Avascular Necrosis Following Steroid Administration for Acute Graft Versus Host Disease in a Post-Bone Marrow Transplant Adolescent – A Case Review
Nathan Howlett, M.Sc., OMS III; Khalil Rahman; Matthew Plante, M.D University of New England College of Osteopathic Medicine, Biddeford, ME
University of Connecticut, Storrs, CT Brown-Alpert Medical School, Providence, RI
With increased survival rates for pediatric leukemia, recognition of the adverse effects of leukemia treatment is becoming ever more important. One of the most debilitating side effects is avascular necrosis (AVN), also known as osteonecrosis.
Incidence rates for AVN following treatment for Acute Lymphoblastic Leukemia (ALL) are between 5 and 10%1 with recent prospective studies showing an incidence of around 6% for those treated with dexamethasone.2 For those afflicted with osteonecrosis, 60% have persistent symptoms over a 3-year period from diagnosis and of those, 20% have symptoms that affect their activities of daily living.2
There are many different treatment options for AVN, however very few are effective. In this case review, we will present a pediatric patient’s course of treatment and outcomes during a four-year period dealing with AVN.
Biphenotypic Acute Leukemia: Biphenotypic acute leukemias (BAL) are rare and represent about 5% of all leukemias.3 There is very little research studying the direct relationship between BAL and AVN, however there is solid evidence documenting the relationship between acute leukemias, specifically pediatric ALL, steroid therapy, and bone marrow transplantation with AVN.
Chondrocyte Physiology: Part of the difficulty in treating patients with avascular necrosis is the disadvantages that cartilage has to heal itself. Chondrocyte’s avascular nature and inability to replace lost hyaline cartilage all complicate healing and regeneration of healthy articular cartilage.7 Once collapse of the articular contour occurs, the process is irreversible and indicates a poor outcome and prognosis for that joint.4
Pathophysiology of Avascular Necrosis: Mechanisms of compromised bone vascularization include intraluminal obstruction of blood vessels by fat emboli, extraluminal obliteration from elevated marrow pressure and focal clotting due to procoagulant abnormalities.4
Risk Factors for Avascular Necrosis: • Age >10 and <20 1,5 • Female Gender 1,5 • High BMI 1,5 • Genetics 1,5
Steroid Use and Avascular Necrosis: • Cumulative Dosing5 (2880mg dosing had 4.2 fold higher probability than 800mg) • Daily dosing5,6 (4.6% increased risk of AVN for every 10mg/d increase in dose) • Oral steroid use versus parenteral steroid use6
Prevention of Avascular Necrosis: • Reduction of cumulative and daily dosing • Use of novel therapies such as MIP-2 rather than steroids for GVHD • Concurrent use of statin’s and/or low molecular weight heparin
Future Treatment Modalities: • Growth Factors: BMP-2, VEGF, G-CSF, HGF • Biophysical Therapy: Extra corporeal shockwave therapy, pulsed electromagnetic field therapy, hyperbaric oxygen therapy
1 Ducassou S., Perel, Y. Curing Acute Lymphoblastic Leukemia and Avoiding Osteonecrosis, Can’t We Have It All?. Pediatric Blood Cancer 2013; 60: 713-714. 2 Te Winkel M. Prospective study on incidence, risk factors, and long-term outcome of osteonecrosis in pediatric acute lymphoblastic leukemia. Journal of clinical oncology. 2011-11-01;29:4143-50. 3 Matutes E, et al. Definition of Acute Biphenotypic Leukemia. Haematologica 1997; 82:64-66. 4 Lafforgue P. Pathophysiology and natural history of avascular necrosis of bone. Joint Bone Spine. 2006;73: 500-507. 5 Powell C, et al. Steroid induced osteonecrosis: An analysis of steroid dosing risk. Autoimmunity Reviews 2010; 9: 721-743. 6 Weldon D. The effects of corticosteroids on bone: osteonecrosis (avascular necrosis of the bone). Annals of allergy, asthma and immunology. 2009-08-01; 103: 91-97. 7 Alford JW, Cole BJ. Cartilage Restoration, Part 1. The American journal of sports medicine. 2005; 33,2; 295-306. 8 Alford JW, Cole BJ. Cartilage Restoration, Part2. The American Journal of Sports Medicine. 2005; 33,3; 443-459. 9 Cho K, et al. Macrophage inflammatory protein-2 (MIP-2)/CXCR2 blockade attenuates acute graft-versus-host disease while preserving graft-versus-leukemia activity. Biochemical and biophysical research communications. 2012; 426: 558-564. 1 0 Rajpura A, et al. Medical Management of osteonecrosis of the hip: a review. Hip Int. 2011;21(04): 385-392. 1 1 Rackwitz L, et al. Stem cell and growth factor based regenerative therapies for avascular necrosis of the femoral head. Stem Cell Research and Therapy. 2012; 3:7; 1-9. 1 2 Girard P, et al. Symptomatic osteonecrosis in childhood leukemia survivors: prevalence, risk factors and impact on quality of life in adulthood. Haematologica. 2013; 98: xxx doi: 10.3324/haematol.2012.081265
In assessing AVN, the clinician needs to recognize the early signs and symptoms of joint pain in a patient with AVN risk factors and begin a non-weight bearing regimen immediately. Both medical and surgical treatments need to be utilized and a stepwise approach to management should be followed in order to leave options for future treatment. The ultimate treatment goal is to prevent irreversible subchondral collapse. Despite the many treatment modalities available, there is currently no cure for AVN. At this time, the best medicine physicians can provide for their patients with risk factors for AVN is to practice prevention and detect disease early in its course.
A healthy 13 year old male presented to his family physician’s office with diffuse lymphadenopathy, fatigue, and malaise of 2 days onset. A CBC was obtained and showed a WBC count of 131,000 with 52% blasts, highly suspicious for an acute leukemia. The patient was immediately referred to Connecticut Children’s Medical Center for a leukemia work up and underwent a bone marrow aspiration and biopsy.
A diagnosis of biphenotypic leukemia was made and standard chemotherapy induction with cytarabine, etoposide and daunorubicin was started. During this time, his older brother was found to be perfect HLA match. Once a complete remission was achieved, after a second induction regimen, the patient underwent a bone marrow transplant (BMT) at Boston Children’s Hospital.
During the third week post-transplant, the patient developed skin rash consistent with acute graft versus host disease (GVHD) and was started on high dose steroids.
Background
Leukemia, Bone Marrow Transplant and GVHD:
Imaging and Operative Pictures Discussion:
Conclusions
References
Osteonecrosis Course:
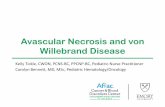
Several weeks following steroid treatment for acute GVHD, the patient began to experience bilateral knee pain. MRI showed multifocal areas of abnormal signal within the femoral head and condyle. The steroids were tapered immediately.
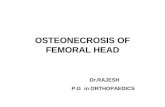
Six months later, repeat MRI revealed extensive AVN involving multiple joints. Non-weight bearing was implemented and the patient began both medical and surgical treatment.
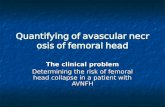
Treatment involved the following: Oral bisphophonates, IV bisphosphonates, hyperbaric oxygen, microfracture, core decompression, bone marrow stem cell infusion, iliac crest bone grafting and an osteochondral allograft of the right knee.