
“Symptoms and syndromes based on the data of auscultation of a heart" prof. S.M. Andreychyn.
51
“Symptoms and syndromes based on the data of auscultation of a heart" prof. S.M. Andreychyn
-
Upload
jody-hodges -
Category
Documents
-
view
215 -
download
2
Transcript of “Symptoms and syndromes based on the data of auscultation of a heart" prof. S.M. Andreychyn.

“Symptoms and syndromes based on the data of
auscultation of a heart"
prof. S.M. Andreychyn

Auscultation of a heart
• Method of examination based on listening to sounds which are created during activity of a heart
• Auscultation may be:
• Direct (immediate).
• Indirect (mediate).

Auscultation introduced into medical practice french clinician Rene
Laennekom

The first device for The first device for auscultation was a auscultation was a
stetoscopestetoscope

First binaural First binaural stethoscopestethoscope

First First phonendoscopephonendoscope

A modern A modern stethophonendoscopstethophonendoscop
ee

Auscultative phenomena which are called Auscultative phenomena which are called heart sounds are created due to vibrations heart sounds are created due to vibrations of anatomical structures of a heart during of anatomical structures of a heart during
its activityits activity

Heart valves

The mechanism of formation of heart tones

Formation of heart tone-atrial component of the heart; b-valve components of I tone; c-components
of muscle tone, vascular components I tone; e-formation second tone; / III tone-formation

Heart valves projection on the thorax

Sequence of Sequence of auscultationauscultation
• The mitral valve - at the heart The mitral valve - at the heart apex;apex;
• the aortic valve - in the second the aortic valve - in the second intercostal space to the right of intercostal space to the right of the sternum), the sternum),
• the pulmonary valve - in the the pulmonary valve - in the second intercostal space, to the second intercostal space, to the left of the sternum,left of the sternum,
• tricuspid valve - at the base of tricuspid valve - at the base of the xyphoid process, the xyphoid process,
• the aortic valve again at the the aortic valve again at the Botkin-Erb point. Botkin-Erb point.

Rules for auscultation of the heart.Rules for auscultation of the heart.
• Sounds associated with the mitral valve Sounds associated with the mitral valve pathology are well heard when the pathology are well heard when the patient lies on his left side, since the patient lies on his left side, since the heart apex is at its nearest position to the heart apex is at its nearest position to the chest wall.chest wall.
• Aortic valve defects are best heard when Aortic valve defects are best heard when the patient is in the upright posture or the patient is in the upright posture or when he lies on his right side. when he lies on his right side.
• The heart sounds are better heard if the The heart sounds are better heard if the patient is asked to inhale deeply and patient is asked to inhale deeply and then exhale deeply and keep breath for then exhale deeply and keep breath for short periods of time so that the short periods of time so that the respiratory sounds should not interfere respiratory sounds should not interfere with auscultation of the heart. with auscultation of the heart.

Standards for cardiac auscultation
Each of the four heart valves can best be heard at specific anatomic locations on the chest wall. While there may be some variation from patient to patient, listen to the heart beat at each of these areas:
• Aortic (2nd right interspace)
• Pulmonic (2nd left interspace)
• Tricuspid (Lower left sternal border)
• Mitral (Apex)

Points of auscultation of a Points of auscultation of a heartheart

Sequence ofSequence of auscultationauscultation

Basic Rules on Cardiac Auscultation
• 1 - The First Heart Sound is simultaneous to the carotid pulse.Its identification is the first obligate step on cardiac auscultation.
• 2 - The Second Heart Sound must be analyzed,with the membrane of the stethoscope, at the pulmonary area,where its two components are best identified. Observe its respiratory variations and splitting.
• 3 - The Third Heart Sound is usually best heard at cardiac apex, in the partial left lateral decubitus position, with the bell of the stethoscope.
• 4 - The Fourth Heart Sound is best heard with the bell of the stethoscope, at cardiac apex (left origin) or tricuspid area (right origin).
• 5 - In Systole we can hear early systolic ejection sounds (aortic or pulmonary stenosis), nonejection mid- to late- systolic clicks (prolapse, extracardiac), and also holosystolic (mitral or tricuspid regurgitations or interventricular communication), protomesosystolic ejection (innocent or aortic or pulmonary stenosis) and mesotelesystolic (prolapse) murmurs.

Scheme of weakeningScheme of weakening (а) (а) and intensificationand intensification (б) (б) of both heart soundsof both heart sounds

Differential symptoms of heart tones
• I heart sound:I heart sound: -the valve component, i.e. vibrations of the cusps of the atrioventricula -the valve component, i.e. vibrations of the cusps of the atrioventricula
valves during the isometric contraction phasevalves during the isometric contraction phase -the muscular one due to the myocardial isometric contraction-the muscular one due to the myocardial isometric contraction -the vascular one. This is due to vibrations of the nearest portions of the -the vascular one. This is due to vibrations of the nearest portions of the
aorta and the pulmonary trunk caused by their distention with the blood aorta and the pulmonary trunk caused by their distention with the blood during the ejection phaseduring the ejection phase
-atrial one is generated by vibrations caused by atrial contractions-atrial one is generated by vibrations caused by atrial contractions
• II heart sound:II heart sound: The second sound is generated by vibrations arising at the early diastole The second sound is generated by vibrations arising at the early diastole
when the semilunar cusps of the aortic valve and the pulmonary trunk are when the semilunar cusps of the aortic valve and the pulmonary trunk are shut (the valve component) and by vibration of the walls at the point of shut (the valve component) and by vibration of the walls at the point of origination of these vessels (the vascular component).origination of these vessels (the vascular component).

Differentiation of Differentiation of І І andand ІІ ІІ heart sounds in heart sounds in tachycardia is performed by assessment of carotic tachycardia is performed by assessment of carotic artery pulsationartery pulsation

Special rules auscultation of the heart
• This instructional techniques designed to create optimal conditions for auscuiltation and detailed analysis of each of the 4 heart valves.

• Auscultated in 1-point (the tip of the heart) during breath-hold exhale when standing, lying on his back on the left side.
Mitral valve

Aortic valve
Auscultated in the 2nd and 5th spots in breath-hold at expiration, in standing, lying on his back, on the right side, sitting with torso forward.

Pulmonary artery valves
Listen in 3-point and stood at breath-hold at expiration in the supine position and on the left side.

• Auscultated in 4-th point in standing, lying on spynii on the right side with breath-hold at expiration.
Tricuspid valve

Analysis of heart sounds
• 1. Listening tones. General characteristics of tones: the sound is normal, loud, relaxed, do not listen.
• 2. Characteristics of the first tone: standard, enhanced, weakened, bifurcate.
• 3. Characteristics of the second tone: standard, enhanced, weakened, hoof, no. Give separately for aortic valve (A) and pulmonary valve (LA).
• 4. Accent II Tone: A tone on the second louder than the second tone on tone II or LA to LA louder than the second tone on A.

Characteristics of the first tone
• 1. Norm - And louder tone of the second tone at the top and xiphoid process.
• 2. Amplification and tone observed in mitral stenosis, thyrotoxicosis. Tone slapping, resulting from insufficient blood the left ventricle.
• 3. Relaxation - due to deposition of the valve and the weakening of the muscle components (MN, TN, AN) infarction.
• No - instead I hear the tone systolic murmur. Sometimes in heart failure, atrial fibrillation.
• 4. Bifurcation and tone: atrioventricular valves are closed simultaneously.

Weakening of the first tone

Characteristics of the second tone
• 1. Normal - second tone from the heart for louder and tone.
• 2. weakening - due to a decrease in the mobility of the valve leaflets of incomplete closing in diastole. Sometimes when defects (AN, PN).
• 3. No - instead the second tone be heard noise. The resulting total estate valves valves.
• 4. Strengthening second tone of the aorta (second point) - due to increased blood pressure in a large circulation or sklarozom aortic wall.
• 5. Strengthening second tone on the pulmonary artery (3rd point) - due to hypertension in the pulmonary circulation.
• 6. Splitting of the second tone - a violation of intraventricular conduction or pidvyshennya pressure in the pulmonary artery.

Weakening of the second tone

General characteristics of heart tones
• 1. Tons of normal volume.
• Cardiac captured without tension at the first hearing apposition stethoscope listening to a point.
• 2. Strengthening both heart tones.
• Observed at:
• - Weight loss in asthenics;
• - With fever (high temperature);
• - When tereotoksykozi;
• - In mitral stenosis;
• - Anemia;
• - Exertion.

• 3. Weakening of both heart tones.
• For auscultation of heart tones needed to focus and auditory stress.
• Observed at:
• - Obesity III-IV century.
• - The athletes.
• - In exudative pericarditis;
• - With myocarditis and other diseases of the myocardium;
• - In the aortic heart defects;
• - With emphysema;
• - Vascular insufficiency.

• 5. Additional colors: the third tone, fourth tone TVMK (II-OS), halopnyy tons (GT).
• 6. Heart Rhythm Tone: binomial (normal), threefold: the rhythm of quail (IT + + TVMK IIT), gallop (IT + IIT + GT).
• 7. Heart rhythm: right, extrasystoles, atrial fibrillation, bradycardia, sinuauricular block, paroxysmal tachycardia.
• 8. Intracardiac murmurs: systolic and diastolic. Characteristics of each noise: volume, tone, character, location. implementation, functional, organic.
• 9. Extracardiac murmur: pericardial friction, kardiopulmonalni, pleuropericardial, vascular.

•Occurs in protodiastoli during the rapid filling of the ventricles with blood from hitting a large volume of blood flowing in the ventricle, its wall.
•Quiet often intermittent sound, listen over 0.12 s after the second tone.
•Observed in children, adolescents, sporstmeniv at MN Academy
ІII tone

• Occurs before systole during atrial contraction in the active phase of ventricular filling with blood. Vibrations are caused by ventricular infarction due to loss of tone.
• Dull, quick sound, listen to systole, like splitting and tone.
• Observed in diseases infarction, heart failure.
ІV tone

Heart melodiesHeart melodies
• Intensification of S3 or S4 sounds gives a three-sound or even four- three-Intensification of S3 or S4 sounds gives a three-sound or even four- three-sound rhythm, known as sound rhythm, known as the the gallop rhythmgallop rhythm (because it resembles the (because it resembles the galloping of a horse). The rrhythm indicates heavy lesions of cardiac galloping of a horse). The rrhythm indicates heavy lesions of cardiac muscle (inflammatory, degenerative, toxic), it is called as " cry of a heart muscle (inflammatory, degenerative, toxic), it is called as " cry of a heart for help".for help".
• The gallop rrhythm is conditionally divides into protodiastolic (intensified The gallop rrhythm is conditionally divides into protodiastolic (intensified III sound arises up though III sound arises up though 0,12-0,2 0,12-0,2 sec. after second sound), sec. after second sound), mesodiastolic(at tachicardia descend coalescence of III and IV sounds and mesodiastolic(at tachicardia descend coalescence of III and IV sounds and it is accepted at auscultation as a single sound) and presystolic it is accepted at auscultation as a single sound) and presystolic ((is is conditioned by pathological IV cardiac sound).conditioned by pathological IV cardiac sound).• Triple rrhythm Triple rrhythm ((Rhithmus coeturnici)Rhithmus coeturnici)
• The rhythm consists of intensified I sound, II heart sound (weakened) and opening The rhythm consists of intensified I sound, II heart sound (weakened) and opening snap soundsnap sound
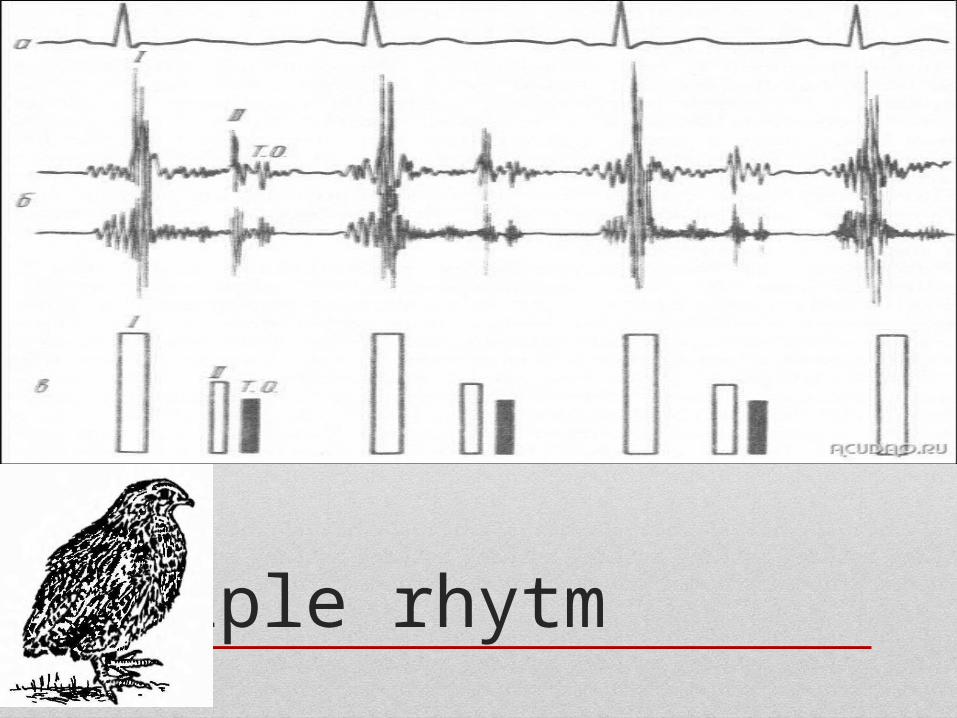
Triple rhytm

The mitral valve opening soundThe mitral valve opening sound
• The The mitral valve opening soundmitral valve opening sound (opening snup) is heard at the (opening snup) is heard at the heart apex of patients with mitral stenosis 0.07-0.13 s heart apex of patients with mitral stenosis 0.07-0.13 s following the second sound, during diastole.following the second sound, during diastole.
• Extra-pericardial-sound Extra-pericardial-sound can occur in pericardial adhesion. It can occur in pericardial adhesion. It originates during diastole, 0.08-0.14 s after the second sound, originates during diastole, 0.08-0.14 s after the second sound, and is generated by the vibrating pericardium during the rapid and is generated by the vibrating pericardium during the rapid dilatation of the ventricles at the beginning of diastole.dilatation of the ventricles at the beginning of diastole.

Gallops rhytm
• A gallop rhythm refers to a (usually abnormal) rhythm of the heart on auscultation.[1] It includes three or four sounds,[2] thus resembling the sounds of a gallop.
• The normal heart rhythm contains two audible heart sounds called S1 and S2 that give the well-known "lub-dub" rhythm; they are caused by the closing of valves in the heart.
• A gallop rhythm contains another sound, called S3 or S4, dependent upon where in the cycle this added sound comes.
• It can also contain both of these sounds forming a quadruple gallop, and in situations of very fast heart rate can produce a summation gallop where S3 and S4 occur so close as to be indistinguishable.

Cardiac murmursCardiac murmurs
• Intracardial murmurs:Intracardial murmurs:
• Organic and functional (relative),Organic and functional (relative),
• Systolic and diastolic,Systolic and diastolic,
• Ejection and regurgitation murmurs,Ejection and regurgitation murmurs,
• They are also different in character, intensity, duration.They are also different in character, intensity, duration.
• Extracardial (pericarial friction murmur and pleuropericardial murmur)Extracardial (pericarial friction murmur and pleuropericardial murmur)

Systolic murmurs
•A. Organic
• - Damage to the valves, chordae, papillary muscles, MN, TN;
• - Narrowing of the aortic orifice (AU) and pulmonary embolism (PS);
• - Perf IBE.
•B. functional
•- Ventricular cavity dilation with the appearance of relative MN, TN;
•- Acceleration of blood flow relative AC, PS;
•- Expansion of the aorta and pulmonary artery.

Diastolic murmurs
• A. Organic
• - Damage to valves: aortic (AN), pulmonary (PN);
• - Narrowing of the valve openings: mitral (MS), tricuspid (TC).
• B. Functional
• - Expansion of the ascending aorta and pulmonary trunk with the appearance of relative AN and PN.

The quality of murmurs is hard to The quality of murmurs is hard to define. Terms such as harsh, define. Terms such as harsh,
blowing, musical, rumbling, high or blowing, musical, rumbling, high or low pitched arc used.low pitched arc used.
Properties of Properties of murmursmurmurs
• DurationDuration• The murmurs of mitral (and tricuspid) The murmurs of mitral (and tricuspid)
regurgitation start simultaneously with the first regurgitation start simultaneously with the first heart sound and continue throughout systole heart sound and continue throughout systole (pansystolic). The ejection systolic murmur of (pansystolic). The ejection systolic murmur of aortic or pulmonary stenosis begins aortic or pulmonary stenosis begins after after the the first heart sound, reaches maximal intensity in first heart sound, reaches maximal intensity in midsystole and stops before the second heart midsystole and stops before the second heart sound.sound.
• Character and pitchCharacter and pitch

• At an auscultation it is necessary At an auscultation it is necessary to determine: to determine:
• 1) 1) relation of murmur to the phase relation of murmur to the phase of cardiac cycle (systole or of cardiac cycle (systole or diastole);diastole);
• 2) 2) properties of murmur, its properties of murmur, its character, intensity, duration; character, intensity, duration;
• 3) 3) localization of murmur, i.e. localization of murmur, i.e. place of the best auscultation; place of the best auscultation;
• 4) 4) condution of murmur condution of murmur (irradiation).(irradiation).
Causes of systolic murmursCauses of systolic murmurs
• Ejection systolic murmurEjection systolic murmur• Increased flow through normal valvesIncreased flow through normal valves• ••'Innocent systolic murmur':'Innocent systolic murmur':• feverfever• athletes (bradycardia -> large stroke volume)athletes (bradycardia -> large stroke volume)• pregnancy (cardiac output maximum at 15 weeks)pregnancy (cardiac output maximum at 15 weeks)• Atrial septal defect (pulmonary flow murmur)Atrial septal defect (pulmonary flow murmur)• Severe anaemiaSevere anaemia• Normal or reduced flow though stenotic valveNormal or reduced flow though stenotic valve• Aortic stenosisAortic stenosis• Pulmonary stenosisPulmonary stenosis• Other causes of flow murmursOther causes of flow murmurs• Hypertrophic obstructive cardiomyopathy (obstruction at subvalvular level)Hypertrophic obstructive cardiomyopathy (obstruction at subvalvular level)• Aortic regurgitation (aortic flow murmur)Aortic regurgitation (aortic flow murmur)
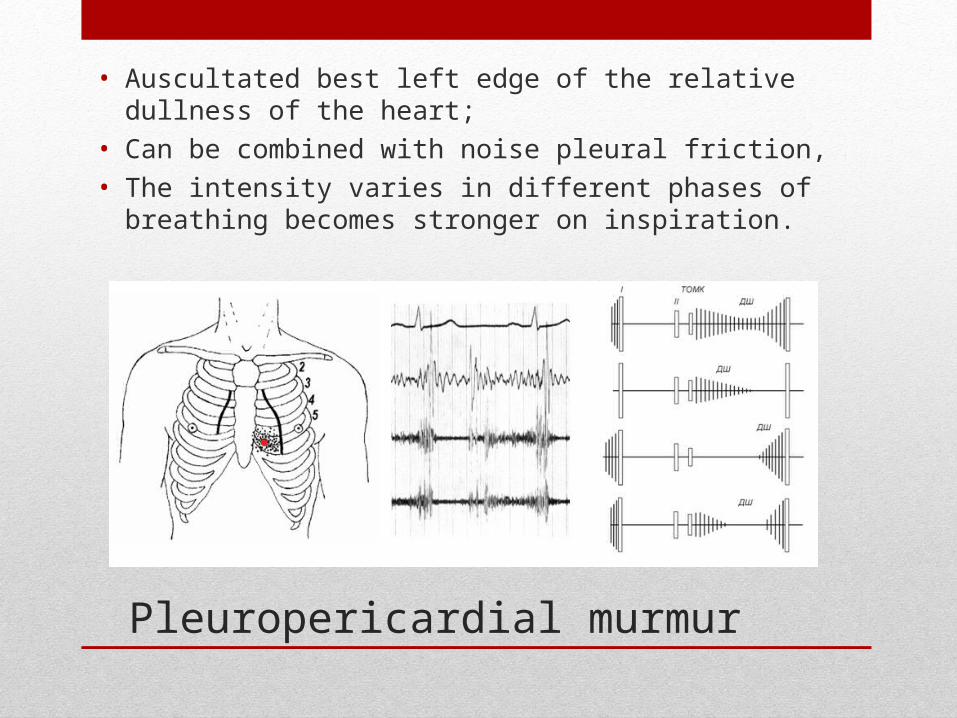
Pleuropericardial murmur
• Auscultated best left edge of the relative dullness of the heart;
• Can be combined with noise pleural friction,
• The intensity varies in different phases of breathing becomes stronger on inspiration.
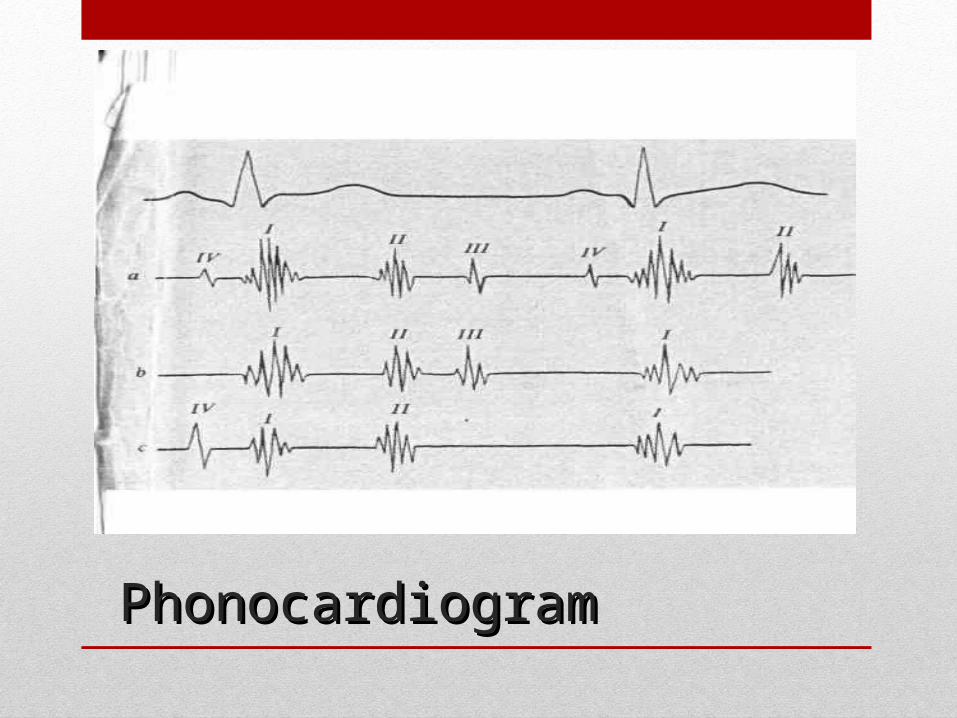
PhonocardiogramPhonocardiogram


Thanks you for your attention!


















