
Symposium 1 Feeding in Pancreatitis -Ruth Newton …...acute pancreatitis: results of a randomized...
95
Symposium 1 “F di i P titi ” “Feeding in Pancreatitis”
Transcript of Symposium 1 Feeding in Pancreatitis -Ruth Newton …...acute pancreatitis: results of a randomized...

Symposium 1
“F di i P titi ”“Feeding in Pancreatitis”

BAPEN Annual Conference
Feeding in Acute PancreatitisFeeding in Acute Pancreatitis

Clinical presentationClinical presentation
A 45 year old man with a history of binge drinking of alcohol is admitted with acute upper abdominal pain. There are no signs of chronic hepatocellular disease but he has upper abdominal tenderness and has an elevated serum amylase concentration of 1250 (normal <100).
His Imrie score is 4 and a CT scan confirms pancreatic inflammation. There is no evidence of gall-stones on CT or on ultrasound scanning.

Clinical presentationClinical presentation
He is transferred to HDU for further care.By day 2 there has been some nausea andBy day 2, there has been some nausea and
a little vomiting, for which metoclopramide is prescribedis prescribed.
Artificial nutritional support is considered.

Question 1Question 1
Would you provide artificial nutrition at this stage?g
1) Y R d1) Yes Red 2) No Yellow) o e o

MUSTMUST
MUST score at this stage is 2 ( BMI 26; no prior weight loss; acute illness and no p g ;expectation of oral intake for >5 days).

Question 2Question 2
How would you provide artificial nutrition?
1) Naso-gastric feeding Red2) Naso-jejunal feeding Yellow3) Intravenous feeding Green3) Intravenous feeding Green

DiscussionDiscussion
What is the best route for providing artificialnutrition in acute pancreatitis?nutrition in acute pancreatitis?
Mr Ross CarterMr Ross Carter

What is the best route forWhat is the best route for providing artificial nutrition in acute pancreatitis?
BAPEN Annual Conference Harrogate Lister
Imrie
27th November, 2007
Pringle McEwen

Open debate?
Session programme
What is the best route for providing artificial nutrition in acutepancreatitis?
What evidence guides the prescription of naso-jejunalfeeds?
The effect of different routes of nutrient administration on human pancreatic exocrine function?human pancreatic exocrine function?

Changes in AP managementChanges in AP managementproblem traditional current
Prediction of severity Imrie/Ranson/CTSI Organ support
Nutrition TPN ?ERCP <48hrs in severes none (exc.cholangitis)( g )
Drug modulation Optimism none
Early Tx for sterile necrosis Open surgery noneEarly Tx for sterile necrosis Open surgery none
Prevention of infection Prophylactic Ab’s noneSurveillance for infection CT guided FNA none
1y surgery for sepsis Open surgery Perc necrosectomy
2y Tx for sepsis More open surgery Re-do necrosectomyy p p g y y
Treatment of OPN Open cyst gastro Lap cyst gastrostomy
Treatment of late pseudocyst Open cyst gastro EUS cyst gastrostomyTreatment of late pseudocyst Open cyst gastro EUS cyst gastrostomy

Nutritional issues in acute pancreatitis
Who needs fed? l th th t d it!…..only those that need it!
Wh t bidit i i t d ith h d lit ?What morbidity is associated with each modality?
Can feeding / the feed composition affect the clinical course of pancreatitis?

Spectrum of disease in acute pancreatitis
Mild acute Severe acuteMild acutepancreatitis
Severe acute pancreatitis
NO organ failure MOFNo necrosisRapid resolutionSecondary prevention
Extensive necrosisProlonged catebolic illnessTreatment of complicationsy p p

Spectrum of disease in acute pancreatitis
Mild acute Severe acuteMild acutepancreatitis
Severe acute pancreatitis
NO organ failure MOF80+%
No necrosisRapid resolutionSecondary prevention
Extensive necrosisProlonged catebolic illnessTreatment of complicationsy p p

“Rule of engagement”
Do no further harm:
- through neglect
- through establishing the delivery system
? through exacerbation of the disease process

Wh t i t d d t f tWhat is standard management of acute pancreatitis?
“Aggressive conservative therapy”
“drip and suck(?)” – concept of gut restoxygen(PsO2) and urinary catheterCVP Organ supportpethidine analgesiapethidine analgesiaInterval cholecystectomy Nutritional support as required
- how did it become standard

Hi t i l t f tHistorical management of acute pancreatitis
1878 Friedrich first described the association of alcohol with abdominal pain, vomiting and pancreatic inflammationp
1887 Socin was the first to describe an operation for acute pancreatitisp
1894 Werner Korte advised a conservative approach limiting surgery for “ suppuration in the ylesser sac (Arch Klin Chir 1894;48,720 )
1902 Kempe performed the first debridement
Diagnosis was generally at laparotomy / post mortem Mortality following surgery was 40-60%)Nutrition by diet as tolerated

Hi t i l t f tHistorical management of acute pancreatitis
1921 L i d i d h i l l NG b1921 Levin designed the single lumen NG tubefor feeding (JAMA 1921; 76(15), 1007)
1933 Wangensteen and Paine used the Levin tube for intestinal decompression (obstruction)JAMA 1933;101(20), 1532-1539.
1938 development of rapid amylase estimation(Somogyi M J Biol Chem 1938;125,399-414)
1940 promotion of initial conservative management including routine decompression of ileus using the “Wangensteen tube” (Morton JJ, Ann Surg. 1940 May;111(5):851-63)
GNutrition by diet or NG

Hi t i l t f tHistorical management of acute pancreatitis
1960 J h H d h h i i i l ill1960 John Howard – nurse through initial illnesssurgery for infectious complications(JAMA. 1960 Nov 26;174:1687-9 )
Overall mortaiity down to ~10%
1968 TPN a realistic option for nutritional support(Dudrick SJ Surgery 1968 64(1) 134-142)
1970 Feeding by a combination of diet, enteral (NG)gastrostomy / jejunostomy of TPN as required(Stephens RV – Use of concentrated, balanced, ( p , ,liquid elemental diet for nutritional management of catabolic states Ann Surg 1969, 170(4), 642-668)
Nutrition by diet or NG or occ. TPN

Historical management of acute pancreatitis
1970’s concern enteral feeding may exacerbate APKonturek SJ Am J Physiol 1972;222 16-20Konturek SJ Am J Physiol 1972;222,16 20Ragins H Am J Surg 1973, 126, 606-614Cassim MM Ann Surg 1974, 180,228-231Vidon N Gut 1978;19,194-8Mitchell CJ Scand J Gastro 1983;18,5-8Evander A Digestion 1982;24,159-167
1973 E li TPN f di t t d th b tt1973 Earlier TPN feeding started the betterFeller JH Am J Surg 1973;127,196-201Blackburn GL Am J Surg 1976;131(1),114-124
1977 Concern enteric feeding may increase septic complicationsR J S 1977 82(1) 99 106Ranson J Surgery 1977;82(1), 99-106
Feeding by (early TPN)

Hi t i l t f tHistorical management of acute pancreatitis
1980‘s Decade of Dogma
Gastric decompressionGastric decompressionGut restEarly TPNEarly TPN
Debridement for sepsisopen laparostomy /packingBradley EL Ann Surg 1987;206(4),542-550
closed lavageclosed lavageBeger HG Br J Surg 1988;75(3),207-212

“striking back”
Nasogastric suctionNavarro S Ros E Aused R et alNavarro S, Ros E,Aused R, et al Comparison of fasting, nasogastric suction and cimetidine in the treatment of acute pancreatitisDigestion 1984;30 224 230Digestion 1984;30,224-230
The use of nasogastric suction was associated with a delay the resumption of bowel activity, prolong the duration of pain, analgesic requirements and hospital stayrequirements and hospital stay

“striking back”
Nasogastric suctionNavarro S, Ros E,Aused R, et al , , ,Comparison of fasting, nasogastric suction and cimetidine in the treatment of acute pancreatitisDigestion 1984;30,224-230
The use of nasogastric suction was associated with a delay the resumption of bowel activity,
l th d ti f i l iprolong the duration of pain, analgesic requirements and hospital stay
NO role for the routine prolonged use of NG suction / decompression

Berlin wall 1989
Climate of change
Early parenteral support is beneficialEarly parenteral support is beneficialSax HC,Warner BW,Talamini MA et al Early total parenteral nutrition in acute pancreatitis: lack of beneficial effectsAm J Surg 1987;153,117-124
TPN associated with a significantly higher rate of catheter-related sepsis no difference in the number of days to oral intake total hospital stay or number of complicationsto oral intake, total hospital stay, or number of complications

Berlin wall 1989
Climate of change
Early parenteral support is beneficialEarly parenteral support is beneficialSax HC,Warner BW,Talamini MA et al Early total parenteral nutrition in acute pancreatitis: lack of beneficial effectsAm J Surg 1987;153,117-124
TPN associated with a significantly higher rate of catheter-related sepsis no difference in the number of days to oral intake total hospital stay or number of complicationsto oral intake, total hospital stay, or number of complications
Early (<7days) TPN is worse than no feedingno feeding

Is gut rest essential?McClave SA,et alComparison of the safety of early enteral vs parenteral nutrition in mild acute pancreatitis. pJPEN 1997;21(1):14-20.Nakad A, et alIs early enteral nutrition in acute pancreatitis dangerous? About 20 patients fed by an endoscopically placed nasogastrojejunal tube. Pancreas 1998;17(2):187-93.
Kalfarentzos F, et alEnteral nutrition is superior to parenteral nutrition in severe acute pancreatitis: Results of a randomized prospective trial.B J S 1997 84(12) 1665 9Br J Surg 1997;84(12):1665-9.Abou-Assi S, et alHypocaloric jejunal feeding is better than total parenteral nutrition in acute pancreatitis: results of a randomized comparative studyacute pancreatitis: results of a randomized comparative study.Am J Gastroenterol 2002;97(9):2255-62.

Is gut rest essential?McClave SA,et alComparison of the safety of early enteral vs parenteral nutrition in mild acute pancreatitis. pJPEN 1997;21(1):14-20.Nakad A, et alIs early enteral nutrition in acute pancreatitis dangerous? About 20 patients fed by an endoscopically placed nasogastrojejunal tube. Pancreas 1998;17(2):187-93.
Kalfarentzos F, et alEnteral nutrition is superior to parenteral nutrition in severe acute pancreatitis: Results of a randomized prospective trial.B J S 1997 84(12) 1665 9Br J Surg 1997;84(12):1665-9.Abou-Assi S, et alHypocaloric jejunal feeding is better than total parenteral nutrition in acute pancreatitis: results of a randomized comparative studyacute pancreatitis: results of a randomized comparative study.Am J Gastroenterol 2002;97(9):2255-62.
E l t l f d i t l t d d idEarly enteral feed is tolerated and avoids the TPN associated morbidity

? Other benefits of enteral nutrition
Mucosal barrier defence mechanism Ammori B et al J Gastrointest Surg 1999;3,252-262Kotani J et al Arch Surg1999;134,287-292
Improvements in metabolic controlpPetrov MS et al, Clin Nutr 2007;26,514-523
ImmunomodulationWindsor ACJ et al. Gut 1998; 42: 431-5Gupta R et al Pancreatology 2003,3,406-413
Enhanced feedingBengmark S Curr opin Clin Nutr Metab Care 2005;8,557-561

Feeding must be distal to the Ligament g gof Treitz
Eatock FC et al.Nasogastric feeding in severe acute pancreatitis may be practical and safe. Int J Pancreatol 2000; 28: 25-31
E t k FC t lEatock FC et al.A randomized study of early nasogastric versus nasojejunal feeding in severe APAm J Gastroenterol 2005; 100: 432-9.
Eckerwall GE et al Early nasogastric feeding in predicted severe AP - a randomised controlled studyAnn Surg 2006;244,959-967
Kumar A et alEarly enteral nutrition in severe acute pancreatitis – a prospective randomisedControlled trial comparing nasojejunal and nasogastric routesControlled trial comparing nasojejunal and nasogastric routesJ Clin Gastroenterol 2006;40,431-434

Feeding must be distal to the Ligament g gof Treitz
Eatock FC et al.Nasogastric feeding in severe acute pancreatitis may be practical and safe. Int J Pancreatol 2000; 28: 25-31
E t k FC t lEatock FC et al.A randomized study of early nasogastric versus nasojejunal feeding in severe APAm J Gastroenterol 2005; 100: 432-9.
Eckerwall GE et al Early nasogastric feeding in predicted severe AP - a randomised controlled studyAnn Surg 2006;244,959-967
Kumar A et alEarly enteral nutrition in severe acute pancreatitis – a prospective randomisedControlled trial comparing nasojejunal and nasogastric routes
Proximal feeding is possible without apparent exacerbation of disease
Controlled trial comparing nasojejunal and nasogastric routesJ Clin Gastroenterol 2006;40,431-434
apparent exacerbation of disease

Potential problems with enteral feeding
Theoretical prolongation of disease
Tolerance ( ? Peptide / fibre feeds / aspiration)
Ri k f t b i ti ( d i / di l i l)Risks of tube insertion ( endoscopic / radiological)
Adequate absorption of delivered feed?q p
Pain on refeeding? (25%)Petrov MSPetrov MSOral refeeding after onset of acute pancreatitis – a review of the literature ( Levy, Pandey and Chebli studies)Am J Gastroenterol 2007;102,2079-2084

Theoretical advantages Theoretical advantages Measurable clinically relevant Measurable clinically relevant relating to feed deliveryrelating to feed delivery morbidity of nutritional delivery morbidity of nutritional delivery

Theoretical advantages Theoretical advantages Measurable clinically relevant Measurable clinically relevant relating to feed deliveryrelating to feed delivery morbidity of delivery systemmorbidity of delivery system
Pragmatic approach to maintenance Pragmatic approach to maintenance of nutritional integrityof nutritional integrity
Oral dietOral diet NGNG NJNJ TPNTPNOral diet Oral diet NGNG NJNJ TPNTPN


Clinical presentationClinical presentation
A dual-lumen naso-jejunal tube is passed to enable naso-gastric aspiration and naso-g pjejunal feeding.

Question 3Question 3
What type of feed would you use via a naso-jejunal tube?j j
1) P l i R d1) Polymeric Red2) Peptide-based Yellow) ept de based e o3) Elemental Green

DiscussionDiscussion
What evidence guides the prescription of naso-jejunal feeds?j j
Miss Olivia Boydss O a oyd

What evidence guides the i ti f j j lprescription of naso-jejunal
feeds?feeds?
Olivia BoydManchester Royal Infirmaryy y

What we will coverWhat we will cover• Background• Background
• Literature search
• Results from the trials
• Nutritional assessment
C t li i l ti• Current clinical practice
• Future developments• Future developments

BackgroundBackground• Conventional treatment resting the pancreas• Conventional treatment - resting the pancreas
• Pancreatic rest enables pain relief
• Associated with increased catabolic state
• Leads to increased energy expenditure
D d t iti l t t• Decreased nutritional status
• Nutritional support prevents malnutritionpp p
• Debate: when using the enteral route, what feed should we use?we use?

Literature searchLiterature searchAim to look for RCT on enteral feeding in pancreatitis• Aim to look for RCT on enteral feeding in pancreatitis comparing feeds
• Databases searched included medline1950-onwards, EMBASE from 1974, CINAHL from 1982, Allied & Complementary medicine from 1985Complementary medicine from 1985
• Pancreatitis, enteral nutrition, nutritional support, words d i MESHtruncated using MESH terms
• Limited to English & human studies• Limited to English & human studies
• 340 hits, 48 related, 3 met criteria340 hits, 48 related, 3 met criteria

The studiesThe studies Author Sample Route Feeds Regimen Outcome p g
measures 1 Lasztity et
al, 2004 14 treatment (T)14 control (C)
NJ T = n-3 PUFAC = polymeric
Started with half strength feed increased
Time receiving NJ feed LOSfeed, increased
over 3 days LOSComplications
2 Tiengou et l 2006
15 treatment (T)15 t l (C)
NJ T = semi l t l
35kcal/kg over 18h
Weight loss & LOSal, 2006 15 control (C) elemental
C = polymeric18hrsIncreaed by 500ml/d until goal achieved
LOS
g
3 Pearce et al, 2006
15 treatment (T)16 control (C)
NJ T = immune enhancing C = polymeric
As per dietetic protocol Fed for a
CRP by 40mg/L
C po y e c ed o aminimum of 3 days

Polymeric Vs. n-3 PUFA’sLasztity et al, 2004
• Moderate - severe pancreatitis
• Enteral nutrition - commenced within 24hrsEnteral nutrition commenced within 24hrs
• Total of 3.3g n-3 PUFA plus additional Vit E given/day
• Feed tolerance was similar between the 2 groups
• LOS & duration of jejunal feed was reduced in the n-3• LOS & duration of jejunal feed was reduced in the n-3
PUFA group (p<0.05)
• Tendency for fewer complications in the n-3 PUFA group

Polymeric Vs. Peptide(Tiengou et al, 2006)
M d t t titi i i NJ• Moderate - severe acute pancreatitis requiring NJ feeding
• Patients were NBM for 7-8 days prior to NJ feeding
• 50% of patients in each group received PN for approximately 8 days
• Tolerance of the feed was similar between both groups
• Semi-elemental feed resulted in less weight loss (p=0 01) and shorter length of stay (P=0 006)(p=0.01) and shorter length of stay (P=0.006)– ITT LOS: remained significant (p< 0.03)

Polymeric Vs. Immune(Pearce et al, 2006)
P ti t di t d t d l t titi• Patients predicted to develop severe acute pancreatitis
• Enteral nutrition commenced within 72hrs of onset of• Enteral nutrition commenced within 72hrs of onset of symptoms
• CRP reduced in 2/15 treatment vs. 6/16 control– By day 3 CRP significantly less in control vs. treatment (p=0.028)
• Tolerance of feeds was similar – Vomiting – 7 treatment / 1 control (p=0.029)

Nutritional assessmentNutritional assessmentI iti l i MUST• Initial screening MUST – Body mass index– Percentage weight loss in previous 3-6 months– Percentage weight loss in previous 3-6 months
• History of oral intakeHistory of oral intake
• Weight historyWeight history
• Subjective global assessmentSubjective global assessment – Estimated dry weight– Physical assessmenty

Assessing requirementsAssessing requirements
• 30% will be malnourished presenting with acute pancreatitis (Meler et al., 2002)
• Basal metabolic rate increases due to:Basal metabolic rate increases due to:– Inflammatory stress– PainPain – 80% of patients are catabolic (Shaw et al., 1986)

Calculating requirementsCalculating requirementsSt d d ti t l l t BMR• Standard equation to calculate BMR e.g. Schofield
• Stress factors vary:Stress factors vary: – 3% chronic pancreatitis
10% acute pancreatitis– 10% acute pancreatitis – 20% sepsis & abscess
(PENG Clinical Handbook, 2004)( )

Current clinical practiceCurrent clinical practiceM t t i l h d tid b d f d• Most trials have used peptide-based feeds
Demonstrated to be safe• Demonstrated to be safe
Pragmatic view due to lack of robust clinical• Pragmatic view due to lack of robust clinical trials
• It is common to start with a polymeric feed
• If this is not tolerated change to a peptide formula (ESPEN Guidelines 2006)formula (ESPEN Guidelines 2006)

Future developmentsFuture developments
• Role of probiotics
• Novel substrates use
• n-3 fatty acids• n-3 fatty acids
• Specific micronutrient supplementation

Clinical presentationClinical presentation
One of the factors in treating acute pancreatitis is the concept of resting the p p gpancreas to reduce its exocrine secretion and limit autodigestionand limit autodigestion.

Question 4Question 4
Which of the following methods of feeding stimulate pancreatic exocrine secretion?p
1) N t i R d1) Naso-gastric Red2) Naso-jejunal Yellow) aso jeju a e o3) Intravenous Green4) None of these Blue

DiscussionDiscussion
What is the evidence that pancreatic secretion is influenced by different types of y ypartificial nutrition?
Is the concept of pancreatic rest important inIs the concept of pancreatic rest important in treating acute pancreatitis?
Professor Peter LayerProfessor Peter Layer

The effect of different routesThe effect of different routesThe effect of different routesThe effect of different routesThe effect of different routes The effect of different routes of nutrient administration onof nutrient administration onThe effect of different routes The effect of different routes of nutrient administration onof nutrient administration onof nutrient administration on of nutrient administration on human pancreatic exocrinehuman pancreatic exocrine
of nutrient administration on of nutrient administration on human pancreatic exocrinehuman pancreatic exocrinehuman pancreatic exocrine human pancreatic exocrine
functionfunctionhuman pancreatic exocrine human pancreatic exocrine
functionfunctionPeter LayerPeter Layer

Interdigestive And Postprandial Interdigestive And Postprandial g pg pPancreatic Secretion*Pancreatic Secretion*
MealMeal MealMeal
FedFastingFastingCephalic PhaseGastric PhaseIntestinal PhaseIntestinal Phase
*Coordinated with gastric and bile output, and GI motility

Oral NutrientsOral NutrientsOral NutrientsOral Nutrients
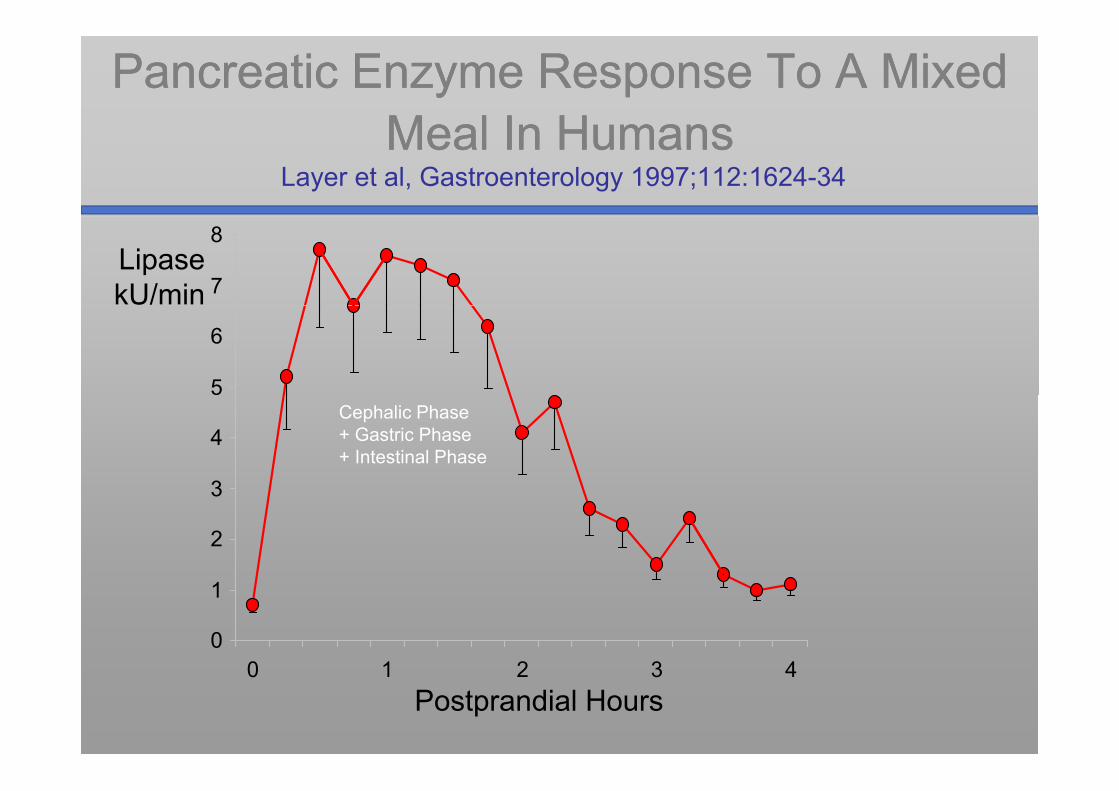
Pancreatic Enzyme Response To A Mixed Pancreatic Enzyme Response To A Mixed Meal In HumansMeal In HumansMeal In HumansMeal In Humans
Layer et al, Gastroenterology 1997;112:1624-34
7
8LipasekU/min
5
6
3
4Cephalic Phase + Gastric Phase+ Intestinal Phase
2
3
0
1
0 1 2 3 40 1 2 3 4Postprandial Hours

Pancreatic Enzyme Response To A Mixed Meal Pancreatic Enzyme Response To A Mixed Meal In HumansIn HumansIn HumansIn Humans
Layer et al, Gastroenterology 1997;112:1624-34*Beglinger et al, J Clin Invest 1985;75:1471-76
7
8LipasekU/min 100
% Maximum*
5
680
3
4 60Cephalic Phase + Gastric Phase+ Intestinal Phase
2
3
20
40
0
1
0 1 2 3 40
20
0 1 2 3 4Postprandial Hours

Pancreatic Secretion In Response To A Pancreatic Secretion In Response To A Carbohydrate Meal In HumansCarbohydrate Meal In HumansCarbohydrate Meal In HumansCarbohydrate Meal In Humans
Layer P et al, Gastroenterology 1986;91:41-48
600
700Trypsin
U/min 100% Total Response
500 80
100
Intestinal Phase
300
40060
200
20
40
0
100
0 1 2 3 4
Cephalic + Gastric Phase
0
20
0 1 2 3 4Postprandial Hours

Role ofRole ofo e oDuodenal
o e oDuodenalDuodenal N t i tDuodenal N t i tNutrientsNutrients

Human Pancreatic Enzyme Output During Human Pancreatic Enzyme Output During I t d d lI t d d l E ti l A i A idE ti l A i A idIntraduodenalIntraduodenal Essential Amino AcidsEssential Amino Acids
Go VLW et al, Gastroenterology 1970;68:321-328
Duodenal EAA Perfusion
100
„Wash Out“100
kU/20min
Stimulated Secretion50
Li
0
LipaseTrypsin
0 1 2 3 4 5 6 10 min Periods

Human Trypsin Response to Graded Human Trypsin Response to Graded D d l A i A id P f iD d l A i A id P f iDuodenal Amino Acid PerfusionDuodenal Amino Acid Perfusion
Keller J et al, Pancreas 1996;13:442
150
100in
Human Subjectsn = 23Mean ± SE
100
n, U
/m
p = 0.00350
Tryp
sin
0 56 112 225 4500
Essential Amino Acids, µmol/min i.d.

Pancreatic Response to Oral vs Pancreatic Response to Oral vs Duodenal NutrientsDuodenal NutrientsDuodenal NutrientsDuodenal Nutrients
O‘Keefe SJ et al, Am J Physiol 2003;284:G27-36
250Amylase
200
y aseOutput,U/kg.h
150
100
0
50
0Placebo Oral Duodenal Duod
Elemental

Duodenal Triglyceride Perfusion Duodenal Triglyceride Perfusion ±± Lipase Inhibitor Orlistat (THL)Lipase Inhibitor Orlistat (THL)±± Lipase Inhibitor Orlistat (THL)Lipase Inhibitor Orlistat (THL)
Hildebrand P et al, Gastroenterology 1998;114:123-129
TrypsinResponse
LipaseActivity
CCK Release
Free Fatty AcidGeneration
8
p
120
140 NaCl THL
140
160
h
60
6
80
100
U/h 100
120
pmol
/L.h
40A
4*
∆kU
/h
40
60∆kU
60
80
AU
C, p
20
% F
FA
2
20
40
* 20
40 *20
*00
*p<0.01
00

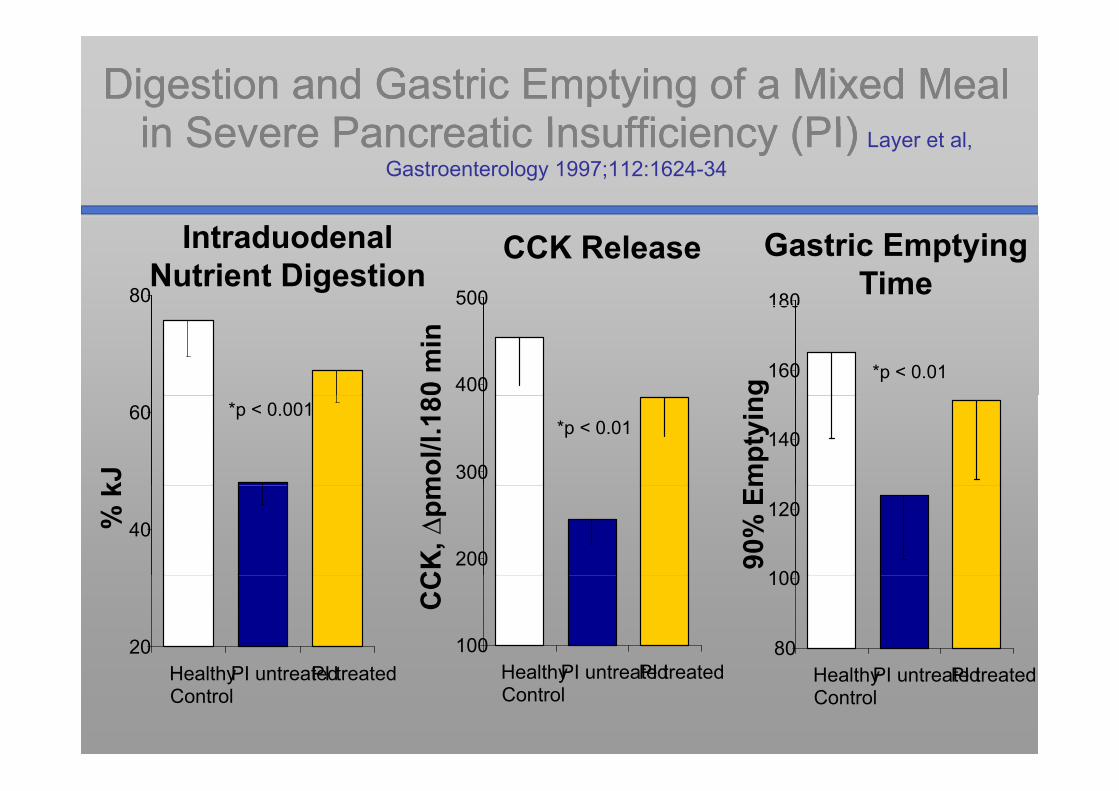
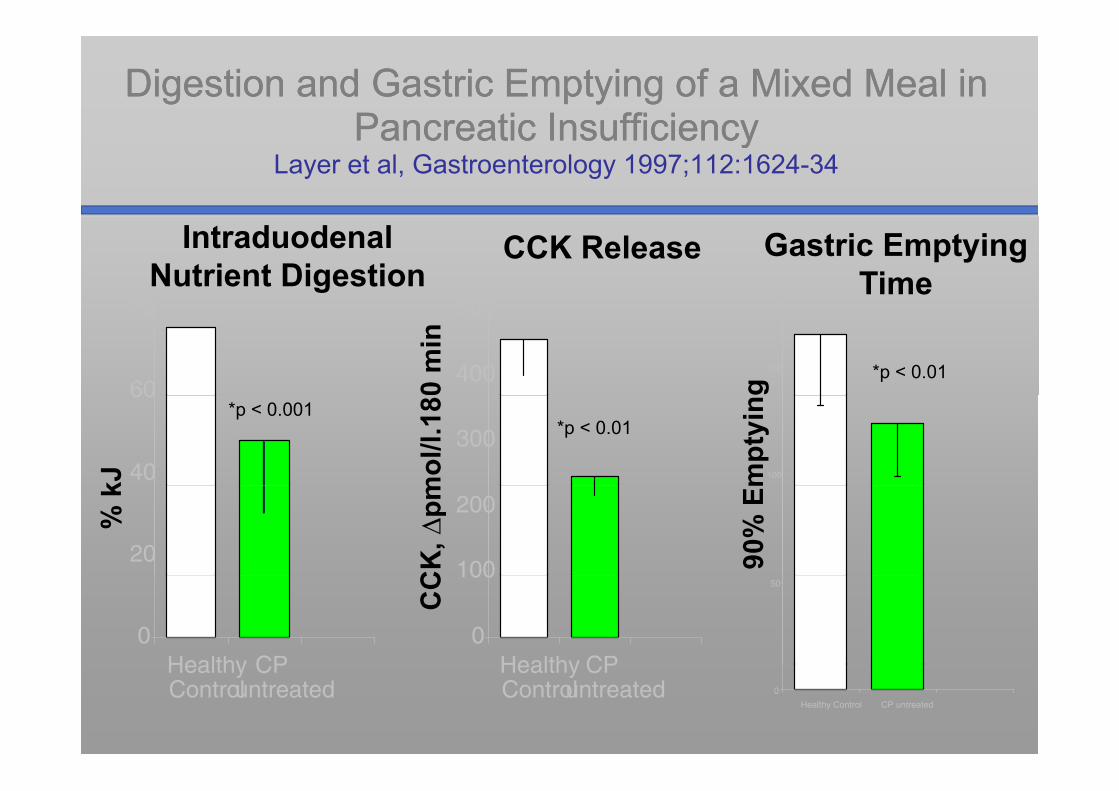
Digestion and Gastric Emptying of a Mixed Meal Digestion and Gastric Emptying of a Mixed Meal in Severe Pancreatic Insufficiency (PI)in Severe Pancreatic Insufficiency (PI)in Severe Pancreatic Insufficiency (PI)in Severe Pancreatic Insufficiency (PI)
Layer et al, Gastroenterology 1997;112:1624-34
80
IntraduodenalNutrient Digestion
500
CCK Release180
Gastric EmptyingTime
400
500
0 m
in
160
180
*p < 0.01g
60 *p < 0.001
kJ 300
*p < 0.01m
ol/l.
18140
mpt
yin
40% k
200
CK
, ∆pm
100
120
90%
Em
20 100H lth PI t t d
CC
80
100
HealthyControl
PI untreated HealthyControl
PI untreated HealthyControl
PI untreated
Digestion and Gastric Emptying of a Mixed Meal Digestion and Gastric Emptying of a Mixed Meal in Severe Pancreatic Insufficiency (PI)in Severe Pancreatic Insufficiency (PI)in Severe Pancreatic Insufficiency (PI)in Severe Pancreatic Insufficiency (PI) Layer et al,
Gastroenterology 1997;112:1624-34
80
IntraduodenalNutrient Digestion
500
CCK Release180
Gastric EmptyingTime
4000 m
in
160
180
*p < 0.01g
60 *p < 0.001
kJ 300
*p < 0.01m
ol/l.
18140
mpt
yin
40% k
200
CK
, ∆pm
100
120
90%
Em
20 100H lth PI t t dPI t t d
CC
80
100
HealthyControl
PI untreatedPI treated HealthyControl
PI untreatedPI treated HealthyControl
PI untreatedPI treated

Regulation of Postprandial Pancreatic Regulation of Postprandial Pancreatic g pg pSecretion: Role of Duodenal NutrientsSecretion: Role of Duodenal Nutrients
Duodenum: sufficient to elicit the full pancreatic stimulatory response to oral nutrientstimulatory response to oral nutrient administration
cephalic gastric contributions adjuvant– cephalic, gastric contributions adjuvant– Marginal stimulatory contribution of jejunum
Mill LJ t l Di Di S i 1979 24 150 54Miller LJ et al, Dig Dis Sci 1979;24:150-54
Stimulation stronger in response to complex vs elemental nutrients
Stimulatory response to lipid requiresStimulatory response to lipid requires predigestion (i.e., presence of FFA)

Regulation of Pancreatic Functional States:Regulation of Pancreatic Functional States:Regulation of Pancreatic Functional States:Regulation of Pancreatic Functional States:Induction of Fed ResponsesInduction of Fed Responses
CephalicGastric
DuodenalMediation
Interdigestive Fed*
State State
*Vagal cholinergic*Peptide hormones*Peptide hormones

Stimulation of Pancreatic Enzyme Secretion Stimulation of Pancreatic Enzyme Secretion yyBy Duodenal NutrientsBy Duodenal Nutrients
CNSDuodenalLumen
AfferentNeurons Efferent
Neurons
Neural ReflexesCNS
Neurons
PancreaticAcinus
NutrientsOsmolarity DistensionDistensionetc
GI RegulatoryPeptides:
± ReleasingPeptides ? CCKCCK
Peptides:Hormones, Neuromodulators

CCK Links Postprandial Motor and CCK Links Postprandial Motor and Secretory ResponsesSecretory Responses
Intraduodenal Nutrient Delivery Gastric
E t idetermines
Bile
Emptying
i hibit-
-
Nutrientincreases
increases
Bile Output
inhibits
++
++
Nutrient Digestion
increases
increasesPancreatic
Enzyme Outputti l t
++
++CCK
Releasestimulates
stimulates
ReleaseFed Motility
Patternstimulates

ParenteralParenteralParenteral Parenteral NutrientsNutrients
Parenteral Nutrients Do Not Stimulate Parenteral Nutrients Do Not Stimulate Exocrine Pancreatic SecretionExocrine Pancreatic Secretion
Animal experiments (dogs)Animal experiments (dogs) Traverso LW et al, 1981; Fried GM et al, 1982
H t diHuman studies Stabile BE 1984; Niederau C 1984; Variyam EP 1985

Pancreatic secretion in response to Pancreatic secretion in response to d d l IV f did d l IV f diduodenal vs IV feedingduodenal vs IV feeding
O‘Keefe SJ et al, Am J Physiol 2003;284:G27-36
250Amylase
200
y aseOutput,U/kg.h
150
100
50
0Placebo Duodenal Intravenous

Jejunal NutrientsJejunal NutrientsJejunal NutrientsJejunal Nutrients

Effects of Effects of JejunalJejunal Nutrients on Human Nutrients on Human Pancreatic Secretion Depend on Perfusion SitePancreatic Secretion Depend on Perfusion SitePancreatic Secretion Depend on Perfusion Site Pancreatic Secretion Depend on Perfusion Site
DiMagno EP et al, J Lab Clin Med 1973; Miller LR et al, Gastroenterology 1979Vu MK et al, Eur J Clin Invest 1999
100
% Maximum
5060 cm
0Basal Jejunal

Pancreatic enzyme response to jejunal Pancreatic enzyme response to jejunal d d l f did d l f divs duodenal feedingvs duodenal feeding
Kaushik N et al, Pancreas 2005;31:353-59
400Trypsin
300
ypsOutput,
U/h
200
100
0
Basal Intravenous Duodenal Mid-Jejunal

Ileal NutrientsIleal NutrientsIleal NutrientsIleal Nutrients

Ileal Pancreatic BrakeIleal Pancreatic BrakeIleal Pancreatic BrakeIleal Pancreatic BrakeLayer P et al, Am J Physiol 1990;G196-G201
N Cl CHO Li id
+ Ileal ExposureDuodenal Amino Acids
250
300NaCl CHO Lipid
AmylaseU/min
200
250
100
150N = 9
p<0.001
50
100 p
0-15 0 15 30 45 60 75 90 105 120 min

Effect of Ileal Nutrients on Effect of Ileal Nutrients on Plasma GlucagonPlasma Glucagon Like PeptideLike Peptide 11Plasma GlucagonPlasma Glucagon--Like PeptideLike Peptide--11
Layer P, Holst JJ et al, Dig Dis Sci 1995;40:1074-82
70Ileal NaCl / CHO / Lipid
Duodenal Amino Acids
60
70
40
50GLP-1
pmol/ml
20
30pmol/ml
N = 9p<0.001
10
20
0-15 0 15 30 45 60 75 90 105 120 min

Lipase Output In Response To A Mixed Lipase Output In Response To A Mixed Meal In HumansMeal In HumansMeal In HumansMeal In Humans
Keller J et al, Am J Physiol 1997;272:G632-G637
Meal5
“Switch-Off”:
4
min
Induced by ileal nutrients
2
3
e, k
U/m
1
2
Lipa
se
0
1
0 1 2 3 4Hours postprandially

Regulation of Gastrointestinal Fed and Regulation of Gastrointestinal Fed and ggFasting States: Contribution of IleumFasting States: Contribution of Ileum
CephalicGastric
DuodenalStimulation
Interdigestive FedState State
Ileal Inhibition(“Brake”)

SummarySummarySummarySummary

Regulation Of Human Pancreatic Regulation Of Human Pancreatic S ti B I t ti l N t i tS ti B I t ti l N t i tSecretion By Intestinal NutrientsSecretion By Intestinal Nutrients
Keller J & Layer P, Gut 2005; 54(S): 1-28
Oral vs Intraduodenal:no difference
O‘Keefe 2003
Oral/Gastric,Duodenal:
(Sub-)maximal100
∆ Output
O Keefe 2003(Sub )maximalstimulationBeglinger 1985
Layer 1997O‘Keefe 2003
50
Jejunum: 100 ∆ Output
O Keefe 20030
jModerate (proximal)or no (distal)stimulation
100 ∆ Output
Ileum:0
stimulationDiMagno 1973Miller 1979Vu 1999
50Ileum:
SubmaximalinhibitionL 1990
-50
Kaushik 2005 0Layer 1990Keller 1997
-100 ∆ Output
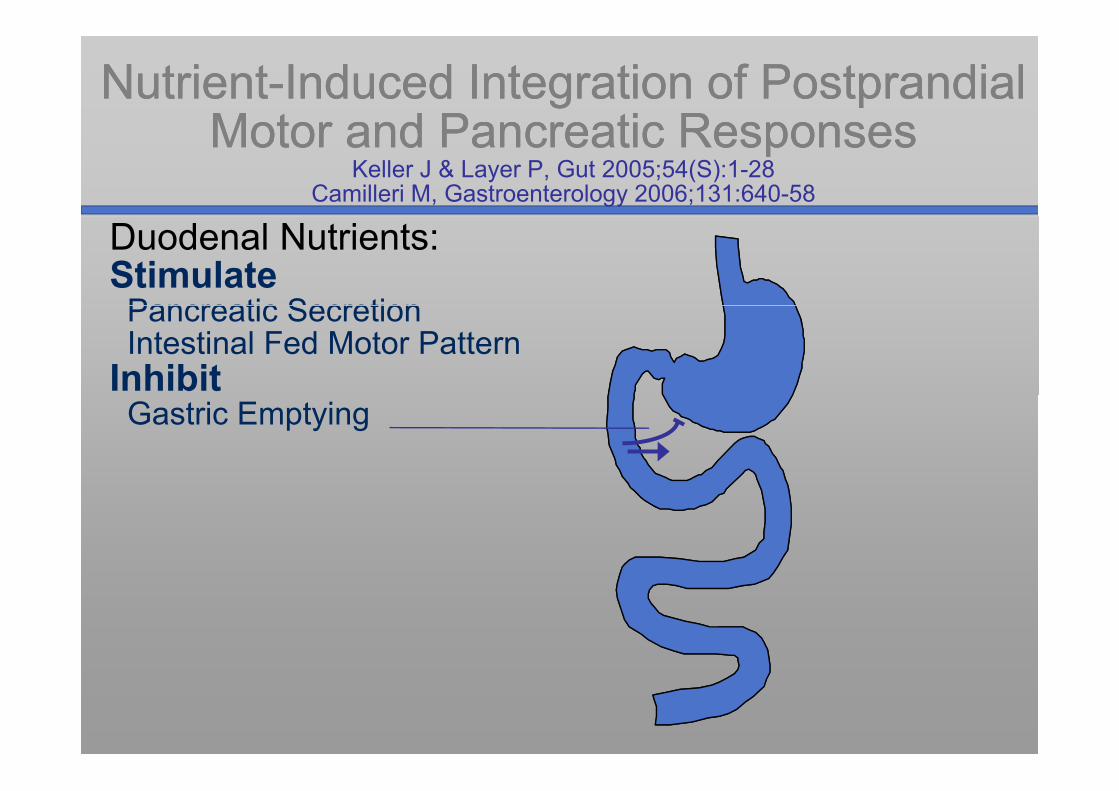
NutrientNutrient--Induced Integration of Postprandial Induced Integration of Postprandial Motor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic Responses
Keller J & Layer P, Gut 2005;54(S):1-28Camilleri M, Gastroenterology 2006;131:640-58
Duodenal Nutrients:StimulatePancreatic SecretionPancreatic SecretionIntestinal Fed Motor Pattern
InhibitGastric Emptying

NutrientNutrient--Induced Integration of Postprandial Induced Integration of Postprandial Motor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic Responses
Keller J & Layer P, Gut 2005;54(S):1-28Camilleri M, Gastroenterology 2006;131:640-58
Duodenal Nutrients:StimulatePancreatic SecretionPancreatic SecretionIntestinal Fed Motor Pattern
Inhibit
Induce, Regulate & IntegrateP t di l R
Gastric Emptying
Postprandial Response

NutrientNutrient--Induced Integration of Postprandial Induced Integration of Postprandial Motor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic Responses
Keller J & Layer P, Gut 2005;54(S):1-28Camilleri M, Gastroenterology 2006;131:640-58
Gastric Emptying
Duodenal Nutrients:StimulatePancreatic Secretion
Gastric &
EmptyingPancreatic SecretionIntestinal Fed Motor Pattern
Inhibit Gastric &PancreaticSecretionInduce, Regulate & Integrate
P t di l R
Gastric Emptying
Small Ileal Nutrients (“Brake”):
Postprandial Response
Intestinal Transit
Ileal Nutrients ( Brake ):Inhibit Fed Motility and Secretion

NutrientNutrient--Induced Integration of Postprandial Induced Integration of Postprandial Motor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic ResponsesMotor and Pancreatic Responses
Keller J & Layer P, Gut 2005;54(S):1-28Camilleri M, Gastroenterology 2006;131:640-58
Gastric Emptying
Duodenal Nutrients:StimulatePancreatic Secretion
Gastric &
EmptyingPancreatic SecretionIntestinal Fed Motor Pattern
Inhibit Gastric &PancreaticSecretionInduce, Regulate & Integrate
P t di l R
Gastric Emptying
Small Ileal Nutrients (“Brake”):
Postprandial Response
Intestinal Transit
Switch Off Fed Response
Ileal Nutrients ( Brake ):Inhibit Fed Motility and Secretion
pInduce Subsequent Interdigestive Pattern
Digestion and Gastric Emptying of a Mixed Meal in Digestion and Gastric Emptying of a Mixed Meal in Pancreatic InsufficiencyPancreatic InsufficiencyPancreatic InsufficiencyPancreatic Insufficiency
Layer et al, Gastroenterology 1997;112:1624-34
80
IntraduodenalNutrient Digestion
500
CCK Release Gastric EmptyingTime
60
80
400
500
0 m
in
150 *p < 0.01g
40
60*p < 0.001
kJ
300 *p < 0.01m
ol/l.
18100m
ptyi
n
20
% k
100
200
CK
, ∆pm
90%
Em
0Healthy CP
0
100
Healthy CP
CC 50
HealthyControl
CPuntreated
HealthyControl
CPuntreated 0
Healthy Control CP untreated

Digestion and Gastric Emptying of a Mixed Meal in Digestion and Gastric Emptying of a Mixed Meal in Pancreatic InsufficiencyPancreatic InsufficiencyPancreatic InsufficiencyPancreatic Insufficiency
Layer et al, Gastroenterology 1997;112:1624-34
80
IntraduodenalNutrient Digestion
500
CCK Release Gastric EmptyingTime
60
80
400
500
0 m
in
150 *p < 0.01g
40
*p < 0.001
kJ
300*p < 0.01
mol
/l.18
100
mpt
yin
20
% k
100
200
CK
, ∆pm
5090%
Em
0
Healthy CP CP treated
0
100
Healthy CP CP
CC
0
Healthy CP CPHealthy
Control
CP
untreated
CP treated Healthy
Control
CP
untreated
CP
treatedHealthy
Control
CP
untreated
CP
treated

CCK Links Postprandial GI Motor and Secretory CCK Links Postprandial GI Motor and Secretory ResponsesResponses
Intraduodenal Nutrient Delivery GNutrient Delivery Gastric
Emptying determines
-Bile
Output inhibits-
Lipid Digestion
increasesincreases
p
Pancreatic ++
++
Digestionincreases Enzyme Output
stimulates
++
CCKRelease
stimulates



Clinical presentationClinical presentation
The patient makes a gradual recovery and resumes ad libitum food intake but is advised to avoid alcohol

DiscussionDiscussion



















