
SYLLABUS - NASPGHAN
206
1 Washington Hilton Washington, DC October 8, 2015 SYLLABUS 1
Transcript of SYLLABUS - NASPGHAN
1
Washington Hilton Washington, DC October 8, 2015
SYLLABUS
1

NASPGHAN assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation.
The discussion, views, and recommendations as to medical procedures, choice of drugs and drug dosages herein are the sole responsibility of the authors. Because of rapid advances in the medical sciences, the Society cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure.
Some of the slides reproduced in this syllabus contain animation in the power point version. This cannot be seen
in the printed version.
Table of Contents
MODULE 1: NUTRITION OBESITY AND THE MICROBIOME 11
REDEFINING MALNUTRITION IN THE 21ST CENTURY 21
MANAGEMENT OF FOOD ALLERGIES AND FPIES 35
MODULE 2: ENDOSCOPY
UPDATES ON CAUSTIC INGESTIONS 46
UPDATES ON FOREIGN BODY INGESTIONS 56
THE PROBLEMATIC POLYP 64
MODULE 3: GI POTPOURRI CLOSTRIDIUM DIFFICILE: DIFFICULT BUT NOT IMPOSSIBLE 75
GLUTEN SENSITIVITY: SURELY A SENSITIVE, BUT PERHAPS NOT A GLUTEN, SUBJECT 86
MEDICAL MANAGEMENT OF REFRACTORY ABDOMINAL PAIN 97
NAUSEA: UPDATES THAT WON’T MAKE YOU SICK 114
MODULE 4: LIVER/PANCREAS NEW HORIZONS IN HEPATITIS C 128
RENAL COMPLICATIONS OF CHRONIC LIVER DISEASE 139
AN UPDATE ON WILSON’S DISEASE 147
BLAME THE GENES? FAMILIAL AND AUTOIMMUNE PANCREATITIS IN CHILDREN 157
MODULE 5: INTESTINAL INFLAMMATION
GETTING TO THE BOTTOM OF PERIANAL CROHN’S DISEASE 168
“IT’S ALL ABOUT THAT POUCH, 'BOUT THAT POUCH, NO COLON”: 179 EVALUATION AND MANAGEMENT OF COMPLICATIONS POST ILEAL POUCH ANAL ANASTOMOSIS
COMMUNICATING THE BENEFITS AND RISKS OF IBD THERAPY TO PATIENTS AND FAMILIES 192

FACULTY NASPGHAN POSTGRADUATE COURSE
Course Directors:
Melanie Greifer MD Assistant Professor of Pediatrics New York University School of Medicine Division of Pediatric Gastroenterology and Nutrition NYU Langone Medical Center New York, NY
Jennifer Strople MD, MS Assistant Professor of Pediatrics Northwestern University Feinberg School of Medicine Clinical Director, Inflammatory Bowel Disease Program Ann & Robert H. Lurie Children's Hospital of Chicago Chicago, IL
Faculty:
Carlo Di Lorenzo MD Chief, Division of Pediatric Gastroenterology, Hepatology and Nutrition Nationwide Children's Hospital Professor of Clinical Pediatrics The Ohio State University College of Medicine Columbus, OH
Praveen Goday MBBSProfessor Medical College of Wisconsin Division Pediatric GI, Hepatology & Nutrition Milwaukee, WI
Stefano Guandalini MDProfessor and Chief Section of Pediatric Gastroenterology University of Chicago Founder and Medical Director, Celiac Disease Center Chicago, IL
Simon Horslen MB, ChB, FRCPCH Director - Hepatobiliary Program Medical Director - Liver & Intestine Transplantation Seattle Children's Hospital Professor - Department of Pediatrics University of Washington School of Medicine Seattle, WA
Stacy A. Kahn MD Assistant Professor of Pediatrics and Medicine Pediatric Gastroenterology, Hepatology, & Nutrition Director, Transitional IBD Clinic The University of Chicago Medicine Chicago, IL
Robert E. Kramer MD, FASGECo-Medical Director DHI/ Director of Endoscopy Associate Professor of Pediatrics Digestive Health Institute Children’s Hospital Colorado/ University of Colorado Denver, CO
Daniel H. Leung MD Assistant Professor of Pediatrics Baylor College of Medicine Division of Gastroenterology, Hepatology, and Nutrition Texas Children's Liver Center Medical Director, Viral Hepatitis Clinic Houston, TX
Petar Mamula MD The Children's Hospital of Philadelphia Division of GI & Nutrition Philadelphia, PA
Mark McOmber MD Phoenix Children's Hospital Pediatric GI & Nutrition Phoenix, AZ
4

Adrian Miranda MD Associate Professor of Pediatrics Section of Pediatric Gastroenterology, Hepatology and Nutrition Children’s Hospital of Wisconsin Medical College of Wisconsin Milwaukee, WI
Jean P Molleston MD Indiana University/Riley Hospital for Children Indianapolis, IN
Véronique Morinville MD Director, Training Program Division of Pediatric Gastroenterology and Nutrition Montreal Children's Hospital Assistant Professor of Pediatrics McGill University Montreal, QC, Canada
Marialena Mouzaki MD, MSc Hospital for Sick Children University of Toronto Division of GI, Hepatology and Nutrition Toronto, ON
Maria Oliva-Hemker MD Stermer Family Professor of Pediatric Inflammatory Bowel Disease Director, Division of Pediatric Gastroenterology and Nutrition Johns Hopkins University School of Medicine Baltimore, MD
Joel R. Rosh MD Director, Pediatric Gastroenterology Vice Chairman, Clinical Development and Research Affairs Goryeb Children's Hospital/Atlantic Health, Morristown, NJ Hugh A. Sampson MD Kurt Hirschhorn Professor of Pediatrics Dean for Translational Biomedical Sciences Director, Conduits (Mount Sinai’s CTSA Program) Director, Jaffe Food Allergy Institute Department of Pediatrics Icahn School of Medicine at Mount Sinai New York, NY Corey A. Siegel MD, MS Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Director, IBD Center, Dartmouth-Hitchcock Medical Center Lebanon, NH
5

Continuing Medical Education
NASPGHAN CME Mission Statement The education mission of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition is to:
1) Advance understanding of normal development, physiology and pathophysiology of diseases of the gastrointestinal tract, liver and nutrition in children
2) Improve professional competence, quality of care, and patient outcomes by disseminating knowledge through scientific meetings, professional and public education.
Our activities, education, and interventions will strive to use Adult Learning Methods (ALM) designed to improve competence, practice performance, and patient outcomes in measurable ways. These educational activities will be targeted to board certified or board eligible pediatric gastroenterologists, physicians with an expertise in pediatric gastroenterology, hepatology and nutrition, subspecialty fellows in pediatric gastroenterology, and nurses specializing in pediatric gastroenterology, hepatology and nutrition.
Physicians
The North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
AMA PRA Statement
NASPGHAN designates this educational activity for a maximum of 8.25 AMA PRA Category 1 Credit(s)TM
Physicians should only claim credit commensurate with the extent of their participation in the activity.
6

Thursday, October 8, 2015
Postgraduate Course - “Updates for the Practitioner”
Course Directors: Melanie Greifer MD and Jennifer Strople MD 7:55AM – 8:00AM Welcome and Introduction
Melanie Greifer MD 8:00AM - 9:15AM MODULE 1: NUTRITION
Moderators: Melanie Greifer MD and Elizabeth Yu MD Obesity and the microbiome Marialena Mouzaki MD, The Hospital for Sick Children Learning objectives: 1. Understand the microbiota in obesity 2. Learn how dietary composition and caloric intake regulate the microbiota 3. Know the effect of the microbiota on the complications of obesity such as metabolic syndrome
Redefining malnutrition in the 21st century Praveen Goday, MBBS, Children’s Hospital of Wisconsin Learning objectives: 1. Discuss the new definitions for malnutrition 2. Identify patient populations with malnutrition that are likely to be seen by the pediatric
gastroenterologist 3. Discuss the management of different sub-populations with malnutrition
Management of food allergies and FPIES Hugh Sampson MD, Icahn School of Medicine at Mount Sinai Learning objectives: 1. Discuss factors that may account for the rise in food allergies 2. Recognize various forms of food allergies including FPIES and other gastrointestinal food allergic
disorders 3. Diagnose and manage various forms of food allergies
9:00AM – 9:15AM Rapid-Fire Q&A 9:15AM - 10:30AM MODULE 2: ENDOSCOPY Moderators: Melanie Greifer MD and Diana Riera MD
Updates on caustic ingestions Mark McOmber MD, Phoenix Children’s Hospital Learning objectives: 1. Know the timing and preparation of intervention 2. Learn the immediate post procedure management including reintroduction of feeds, NG tubes etc. 3. Understand the follow up and long term issues of ingestion including treatment of these issues
7

Updates on foreign body ingestions Robert Kramer MD, Children’s Hospital Colorado Learning objectives: 1. Know the timing and preparation of interventions dependent on ingestion 2. Review management of glass and sharps 3. Know the most current updates on magnets/batteries and detergent pod ingestions
The problematic polyp Petar Mamula MD, Children’s Hospital of Philadelphia Learning objectives: 1. Review prerequisites for successful polypectomy 2. Discuss techniques for difficult polyps 3. Review polypectomy complications
10:15AM – 10:30AM Rapid-Fire Q&A 10:30AM – 10:50AM BREAK 10:50AM – 12:25PM MODULE 3: GI POTPOURRI Moderators: Chris Liacouras MD and Jennifer Strople MD
Clostridium Difficile: Difficult but not impossible Stacy Kahn MD, University of Chicago Comer Children’s Hospital Learning objectives: 1. Learn appropriate identification and testing for C. Difficile 2. Know the updates on medical management 3. Understand fecal transplantation and the ethics involved in its use
Gluten sensitivity: surely a sensitive, but perhaps not a gluten, subject Stefano Guandalini MD, University of Chicago Comer Children’s Hospital Learning objectives: 1. Define non-celiac gluten sensitivity 2. Understand the current uncertainties around gluten sensitivity 3. Know how to approach patients with suspected non-celiac gluten sensitivity
Medical management of refractory abdominal pain Adrian Miranda MD, Children’s Hospital of Wisconsin Learning objectives: 1. Understand the mechanisms of refractory abdominal pain 2. Identifying the patient with refractory abdominal pain 3. Know the available and current treatment options
Nausea: Updates that won’t make you sick Carlo Di Lorenzo MD, Nationwide Children’s Hospital Learning objectives: 1. Understand the differential diagnosis of children presenting with nausea as the predominant
symptom 2. Become familiar with the medical interventions with the potential of improving functional nausea 3. Become familiar with the non-medical interventions with the potential of improving functional
nausea
12:10PM – 12:25PM Rapid-Fire Q&A 12:25PM – 1:50PM LEARNING LUNCHES
8

1. Blurred lines: Where gastroenterology and allergy intersect Moderator: Chris Liacouras Hugh Sampson and Tiffani Hays
2. The child swallowed what? Management of caustic and foreign body ingestions
Moderator: Deepali Tewari Robert Kramer and Mark McOmber
3. C. difficile meets its match: Approach to the complicated patient Moderator: Sunpreet Kaur Stacy Kahn and George Russell
4. Gluten sensitivity, more than a fad: A case based discussion Moderator: Kelly Thomsen Stefano Guandalini, Hilary Jericho and Pamela A. Cureton
5. Practical approach to treating the patient with persistent pain and nausea
Moderator: John Stutts Adrian Miranda and Katja Kovacic
6. Challenging liver disease cases Moderator: Ritu Walia Jean Molleston and Simon Horslen
7. Viral hepatitis: When do you treat? Moderator: Vicky Ng Daniel Leung and Jessica Wen
8. Perplexing cases in pancreatitis Moderator: Deborah Neigut Veronique Morinville and Soma Kumar
9. Management of pouch and perianal complications Moderator: Dinesh Pashankar Maria Oliva-Hemker and Joel Rosh
1:50PM – 3:25PM MODULE 4: LIVER/PANCREAS
Moderators: Melanie Greifer MD and Deborah Neigut MD New horizons in hepatitis C Daniel Leung MD, Texas Children’s Hospital Learning objectives: 1. Understand the epidemiology, burden of disease, and natural history of HCV 2. Appreciate the rapidity and timeline of HCV drug development 3. Become familiar with clinical indications to treat and soon to be available all-oral treatment regimens
Renal complications of chronic liver disease Jean Molleston MD, Riley Children’s Hospital Learning objectives: 1. Define prevalence of renal complications in chronic liver disease 2. Review mechanisms of ascites and the role of the kidneys and diuretic use 3. Understand the role of electrolyte monitoring and fluid balance in cirrhosis 4. Review definition of hepatorenal syndrome and treatment recommendations, including use of
terlipressin
9
cxAn update on Wilson’s Disease Simon Horslen MD, Seattle Children’s Hospital Learning objectives: 1. Review the clinical presentations in pediatric population and typical diagnostic evaluation 2. Understand genetics and patterns of inheritance to focus who should be screened 3. Understand treatment strategies and side effects of current and future therapies
Blame the genes? Familial and autoimmune pancreatitis in children Veronique Morinville MD, Montreal Children's Hospital Learning objectives: 1. Understand when to consider familial and autoimmune etiologies in a child presenting with
pancreatitis 2. Review the different genetic factors that may be involved in familial-type pancreatitis 3. Recognize factors implicated in autoimmune pancreatitis types 1 and 2 and what therapies may be
attempted
3:10PM – 3:25PM Rapid-Fire Q&A 3:25PM – 3:45PM BREAK 3:45PM – 5:00PM MODULE 5: INFLAMMATORY BOWEL DISEASE
Moderators: Judith Kelsen MD and Jennifer Strople MD Getting to the bottom of perianal Crohn’s disease Maria Oliva-Hemker MD, Johns Hopkins University Medical Center Learning objectives: 1. Review the classification systems for fistulizing disease 2. Understand the approach to initial diagnosis and assessment 3. Review surgical and medical therapy and role for each
“It’s all about that pouch, 'bout that pouch, no colon”: Evaluation and management of complications post ileal pouch anal anastomosis Joel Rosh MD, Goryeb Children’s Hospital Learning objectives: 1. Review the data for evaluation, treatment and prevention of pouchitis 2. Understand other complications of IPAA 3. Review cancer screening /surveillance recommendations
Communicating the benefits and risks of IBD therapy to patients and families Corey Siegel MD, Dartmouth-Hitchcock Medical Center Learning objectives: 1. Review the risks of immunomodulators and biologics 2. Discuss decision making between anti-TNF monotherapy or combination therapy 3. Learn about tools that can be used to better communicate the benefits and risks of IBD therapy
4:45PM – 5:00PM Rapid-Fire Q&A
10
Obesity and intestinal microbiomeMarialena Mouzaki, MD MSc
Hospital for Sick Children
University of Toronto
Disclosures
Nothing to disclose
Learning Objectives
Understand the microbiota in obesity
Learn how dietary composition and caloric intake regulate the microbiota
Know the effects of the microbiota on the complications of obesity, such as metabolic syndrome
11

Microbiota in obesity
Backhed et al. Proc Natl Acad Sci USA 2004; Turnbaugh et al. Nature 2006
Conventionally raised
ob/ob mice
Germ-free Weight gain
Germ-free obesity
Microbiota in obesityTWINS
Germ-free
Ridaura et al. Science 2013; Vrieze et al Gastroenterol 2012;Wendelsdorf NIH Research Matters 2013
Germ-free Obese
Lean
How can the microbiota contribute to obesity?
Obesity
Appetite
Energy extraction
Energy expenditure
Gene expression
Prebiotics & Probioticsincreased GLP-1, PYY
CHO fermentationSCFA arcuate nucleus
Example:Bacteria produce H2 which is then used by Archea Acetate + H2 CH4+ CO2
Bile acids SCFA
LL: FIAFDNL: SREBP, ChREBPFAO: AMPK
12

Intestinal microbiota composition in obesity
Study n - population Results
Ley et al. 2006 17 • Firmicutes/Bacteroidetes
Turnbaugh et al. 2009 14 (vs. 140) • bacterial diversity• Bacteroidetes
Verdam et al. 2013 28 • bacterial diversity• Firmicutes/Bacteroidetes
Duncan et al. 2008 37 • No difference in Bacteroidetes or Firmicutes
Jumpertz et al. 2011 21 • No difference in Bacteroidetes or Firmicutes
Schwiertz et al. 2010 101 • Firmicutes/Bacteroidetes
Karlsson et al. 2012 40 • No difference in Bacteroidetes or Firmicutes
Intestinal microbiota composition in obesity
Bottom line and considerations: Results vary; decreased bacterial diversity is consistentDifferences in methodology IM quantification Storage, timing of sample collection, etc.
Bahl et al. FEMS Microbiol Lett 2012; Thaiss et al. Cell 2014
Intestinal microbiota composition in obesity
Low bacterial richness Obesity
Pre-DM2, DM2
Dyslipidemia
Inflammation
High bacterial richness Synthesis of organic
acids
Synthesis of SCFA
Methane production
Carisili et al. Curr Opin Clin Nutr Metab Care 2014
13

Effect of diet on intestinal microbiota
10 adults, ages 21-33, BMI range 19-32
Placed on either diet x 5 days Observed x4 days pre and 6 days post
David et al. Nature 2014
Plant-based diet Animal-based dietSimilar intakes
No weight change Weight loss by day 3
Bilophila wadsworthia, Alistipes putredinis, Bacteroides
Prevotella genus*
Effect of diet on bacterial metabolism & gene expressionFecal SCFA correlate with diet
Diet alters microbial gene expression
David et al. Nature 2014
• Acetate, butyrate • Gluconeogenesis, glycolysis
• Isovalerate, isobutyrate• B6 metabolism, aromatic
hydrocarbon degradation
Effect of diet on fecal bile acids Increased fecal deoxycholic acid with animal diet
Product of bacterial metabolism Can inhibit growth of certain Firmicutes and Bacteroidetes In animals, linked to HCC
Increased expression of sulfite reductase with animal diet H2S can cause intestinal inflammation Link to B. wadsworthia and bile acids
David et al. Nature 2014;Devkota et al. Nature 2012
14
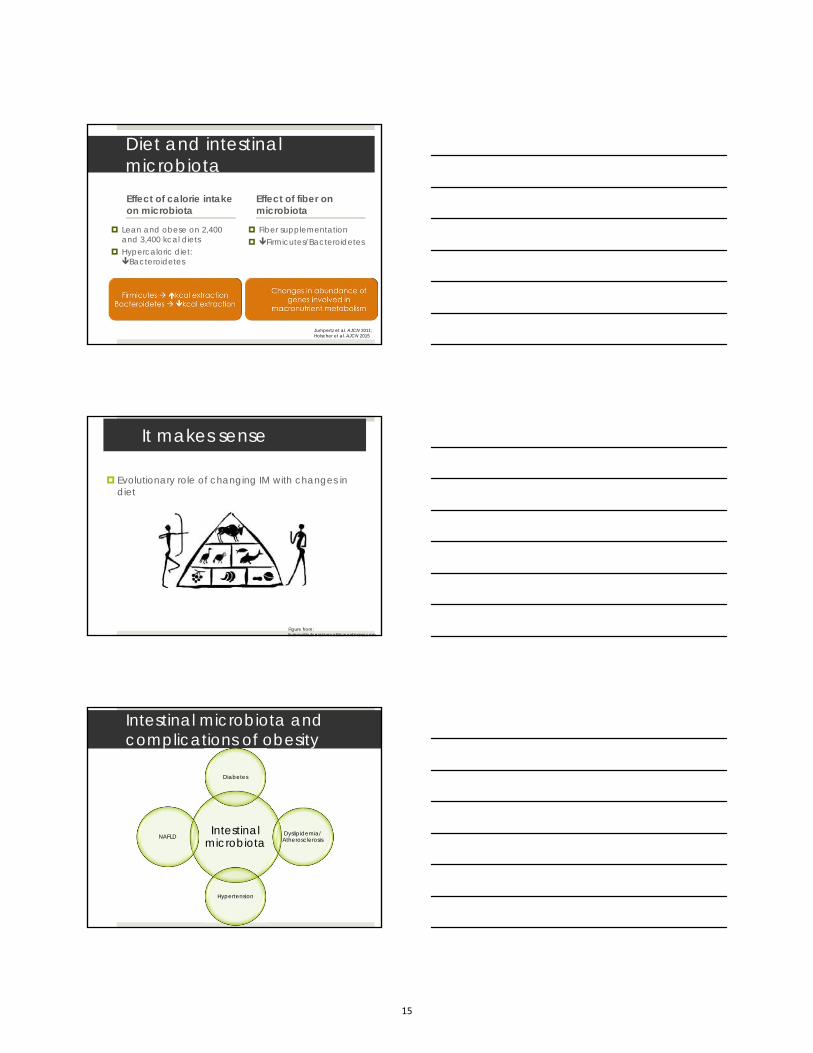
Diet and intestinal microbiotaEffect of calorie intake on microbiota
Lean and obese on 2,400 and 3,400 kcal diets
Hypercaloric diet: Bacteroidetes
Effect of fiber on microbiota
Fiber supplementation Firmicutes/Bacteroidetes
Jumpertz et al. AJCN 2011; Holscher et al. AJCN 2015
It makes sense
Evolutionary role of changing IM with changes in diet
Figure from:livingwithulcerativecolitis.wordpress.com
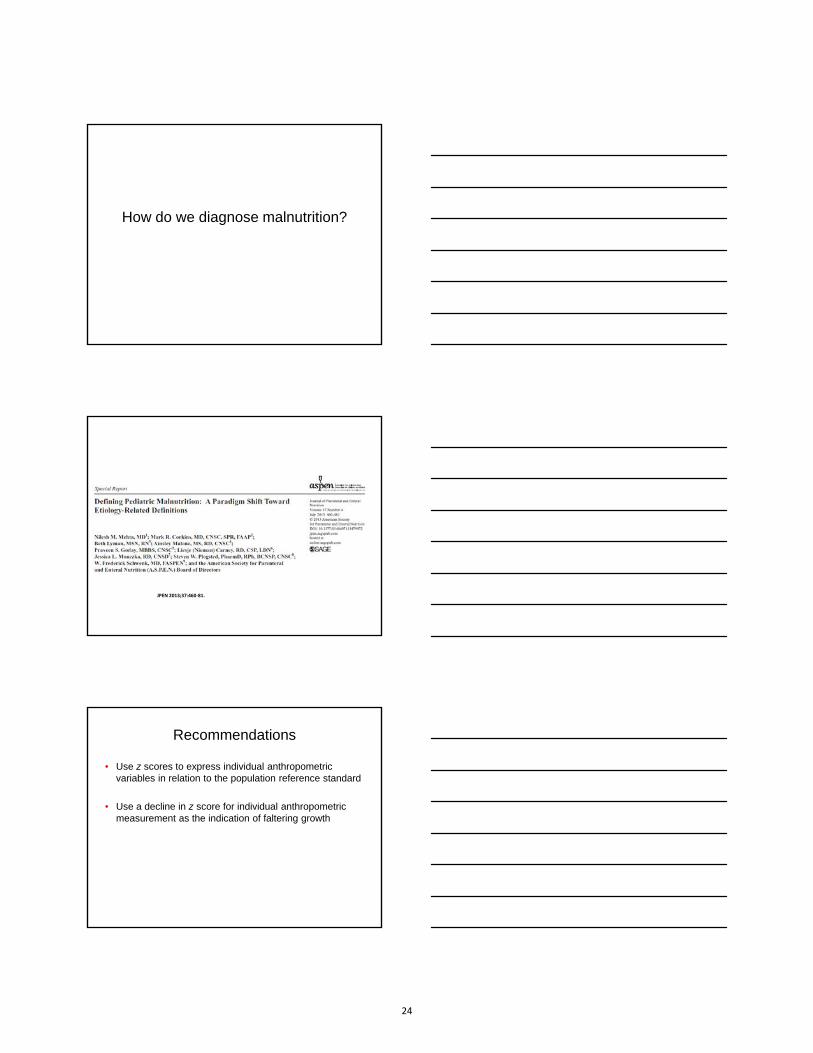
Intestinal microbiota and complications of obesity
Intestinal microbiota
Diabetes
Dyslipidemia/ Atherosclerosis
Hypertension
NAFLD
15

Intestinal microbiota & diabetes
Caricilli et al. Nutrients 2013; Amar et al. EMBO Mol Med 2011; Zhao et al. Am J Physiol Endocrinol Metab 2011; Tamrakar et al. Endocrinol 2010; Carvalho et al. Diabetologia 2012
High fat diet bacterial translocation and endotoxemia, prior to the development of diabetes
NOD-1 activation inflammation insulin resistance
NOD-2 activation insulin resistance in muscle
Antibiotics following high fat diet lead to improved insulin sensitivity
Intestinal microbiota and insulin sensitivity: human studies
• Systemic insulin resistance
• Improved insulin sensitivity
• Habitual intake correlates withfasting glucose levels
• Consumption leads to insulin resistance
Mehta et al. Diabetes 2010; Vrieze et al. Gastroenterol 2014; Suez et al. Nature 2014
Intestinal microbiota and insulin sensitivity: human studies
• Systemic insulin resistance
• Improved insulin sensitivity
• Habitual intake correlates withfasting glucose levels
• Consumption leads to insulin resistance
Mehta et al. Diabetes 2010; Vrieze et al. Gastroenterol 2014; Suez et al. Nature 2014
16

Intestinal microbiota and insulin sensitivity: human studies
• Systemic insulin resistance
• Improved insulin sensitivity
• Consumption leads to insulin resistance
• Fecal transplantation: humans to germ-free mice insulin resistance
Mehta et al. Diabetes 2010; Vrieze et al. Gastroenterol 2014; Suez et al. Nature 2014
Intestinal microbiota and hypertension
Common determinants of outcome
Environ-ment
DietGenes
Low-grade inflammation associated with hypertension
Probiotics improved BPMinocycline improved BP
Singh et al. Immunol Res 2014;Khalesi et al. Hypertension 2014; Shi et al. Hypertension 2010
Dysbiosis is linked to hypertension
Spontaneously HTN rat*
Rat with HTN 2ndary to
chronic AT-IIinfusion*
Human volunteers(adults)*
Diversity & richness
Firmicutes/Bacteroidetes -
Acetate & butyrate-producing bacteria
No change -
Yang et al. Hypertension 201
* Compared to controls
17

SCFA participate in blood pressure regulation
Kidney
Vessels of smallresistance
Colon
Olf78 reninBP
Gpr41 vasodilation
BP
Pluznick et al. Proc Natl Acad Sci USA 2013
Intestinal microbiota and dyslipidemia
Bile acids: bile salt hydroxylase activity improved lipid profiles, possibly due to FXR activation
Other molecules Mooradian et al. Nat Clin Pract Endocrinol Metab 2009; Org et al.Atherosclerosis 2015
& FIAF inhibition
Fatty acid oxidation, de novo lipogenesis
Intestinal microbiota and atherosclerosis
Org et al.Atherosclerosis 20
18

Intestinal microbiota and NAFLD
Mouzaki, Bandsma. Curr Drug Targets 20
Take home messages
Dysbiosis and altered microbial metabolism contribute to the development of obesity
Dietary modifications lead to rapid and predictable changes in the intestinal microbiota composition
Products of microbial metabolism interfere with host gene expression and contribute to the development of metabolic syndrome
Future directions
Understand further the interplay between environment, diet and intestinal microbiota
Identify microbial patterns that predict future risk of obesity, to allow disease prevention
Use the critical impact of the intestinal microbiota (SCFA and bile acids) on nutrient metabolism to develop treatments for obesity and its complications
19

Thank you
20
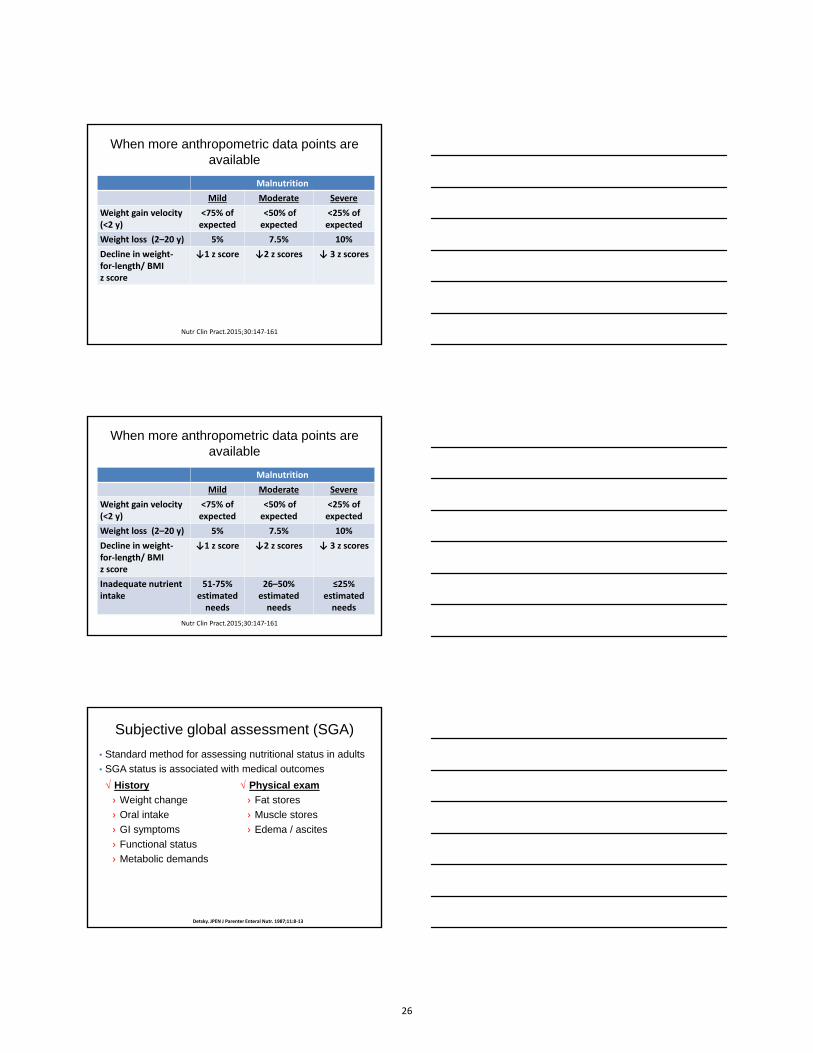
Redefining Malnutrition in the 21st
Century
Praveen S. Goday, MDProfessor
Pediatric Gastroenterology and NutritionMedical College of WisconsinDirector of Clinical Nutrition
Children’s Hospital of WisconsinMilwaukee, WI
Disclosures slide
Dr. Praveen Goday serves an expert reviewer for Best Doctors, Inc. and a consultant for Fresenius Kabi.
Any real or apparent conflicts of interest related to the content of this presentation have been resolved.
Learning objectives
• Discuss the new definitions for malnutrition
• Identify patient populations with malnutrition that arelikely to be seen by the pediatric gastroenterologist
• Discuss the management of different sub-populationswith malnutrition
21

• Are children in US hospitals malnourished?
• Do we care that they are malnourished?
• How do we diagnose malnutrition?
• Where are pediatric gastroenterologists going to seemalnutrition?
• What can we do about malnutrition?
Are children in US hospitals malnourished?
14.0%
8.0%7.1%
21.0%
11.0%
6.1%
0%
5%
10%
15%
20%
25%
UK1990
UK1995
USA1997
France2001
France2005
Germany2008
Clin Nutr 2008; 27:72–76; Arch Pediatr 2005; 12:1226–1231.Arch Pediatr 2001; 8:1203–1208; Arch Pediatr Adolesc Med 1995; 149:1118–1122.Clin Nutr 1997; 16:13–18; J Hum Nutr Diet 1990; 3:93–100.
Malnutrition in hospitalized US children
22

0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1Malnutrition
1.3% severe malnutrition
5.8% moderate malnutrition
25% obesity
17.4% mild malnutrition
Arch Pediatr Adolesc Med 1995; 149:1118–1122
Do we care that they are malnourished?
Subjective global nutrition assessment (SGNA)
Secker. Am J Clin Nutr. 2007 Apr;85(4):1083‐9.
Preoperative nutritional status in 175 children
undergoing surgery
- well nourished
- moderately malnourished
- severely malnourished
- ↑ rates of infection
- Longer post-op length of stay (8.2
vs 5.3 d) (P = 0.002)
Divided into
Malnourished children
23
How do we diagnose malnutrition?
JPEN 2013;37:460‐81.
Recommendations
• Use z scores to express individual anthropometricvariables in relation to the population reference standard
• Use a decline in z score for individual anthropometricmeasurement as the indication of faltering growth
24

When only one anthropometric data point is available
Malnutrition
Mild Moderate Severe
Weight-for-height or BMI for age z score
-1 to 1.9 - 2 to -2.9 ≤ - 3
Length/height-for-age z score
- - ≤ - 3
Mid–upper arm circumference z score
-1 to 1.9 - 2 to -2.9 ≤ - 3
Nutr Clin Pract.2015;30:147‐161
When more anthropometric data points are available
Malnutrition
Mild Moderate Severe
Weight gain velocity (<2 y)
<75% of expected
<50% of expected
<25% of expected
Nutr Clin Pract.2015;30:147‐161
When more anthropometric data points are available
Malnutrition
Mild Moderate Severe
Weight gain velocity (<2 y)
<75% of expected
<50% of expected
<25% of expected
Weight loss (2–20 y) 5% 7.5% 10%
Nutr Clin Pract.2015;30:147‐161
25
When more anthropometric data points are available
Malnutrition
Mild Moderate Severe
Weight gain velocity (<2 y)
<75% of expected
<50% of expected
<25% of expected
Weight loss (2–20 y) 5% 7.5% 10%
Decline in weight‐for‐length/ BMI z score
↓1 z score ↓2 z scores ↓ 3 z scores
Nutr Clin Pract.2015;30:147‐161
When more anthropometric data points are available
Malnutrition
Mild Moderate Severe
Weight gain velocity (<2 y)
<75% of expected
<50% of expected
<25% of expected
Weight loss (2–20 y) 5% 7.5% 10%
Decline in weight‐for‐length/ BMI z score
↓1 z score ↓2 z scores ↓ 3 z scores
Inadequate nutrient intake
51‐75% estimatedneeds
26–50% estimatedneeds
≤25% estimated needs
Nutr Clin Pract.2015;30:147‐161
Subjective global assessment (SGA)
√ History
› Weight change
› Oral intake
› GI symptoms
› Functional status
› Metabolic demands
√ Physical exam
› Fat stores
› Muscle stores
› Edema / ascites
Detsky. JPEN J Parenter Enteral Nutr. 1987;11:8‐13
• Standard method for assessing nutritional status in adults
• SGA status is associated with medical outcomes
26

Subjective global nutrition assessment (SGNA)
• History› Appropriateness of height
for age› Appropriateness of weight
for height› Changes in body weight› Oral intake› GI symptoms› Functional status› Metabolic demands
• Physical exam
› Fat stores
› Muscle stores
› Edema / ascites
• Should become the standard method for assessingnutritional status in children
Am J Clin Nutr. 2007 Apr;85(4):1083‐9.
How to Perform Subjective Global Nutritional Assessment in Children.Secker DJ and Jeejeebhoy KN. Journal of the Academy of Nutrition and Dietetics 2012. 112: 424–431.
GI symptoms
• Severe if symptoms have been present for2 weeks or longer
• Symptoms for 3 days or fewer, can bedisregarded
27

Functional status
• Has a lack of nutrition affected the child’sphysical function and altered her dailyactivities?
√Compare to the child pre-illness
Metabolic demands
Moderate metabolic stress• Routine surgery• Laparoscopic surgery• Exploratory surgery• Fracture• Infection
√ Bronchiolitis√ Gastroenteritis)
• Decubitus ulcer
Metabolic demands
Severe metabolic stress
• Major organ surgery
√ stomach, liver, pancreas, lung
• Major bowel resection
• Multiorgan failure
• Severe pancreatitis
• Severe sepsis
• Severe inflammation
• Chronic illness with acute deterioration
• Current treatment for malignancy
28

Albumin and prealbumin
• These proteins are negative acute phase reactants
√ They are, in most instances, not indicative ofmalnutrition
Where are pediatric gastroenterologists going to see malnutrition?
Causes of malnutrition
Non-illness related Starvation- Anorexia nervosa
Acute (<3 months)
- Trauma, burns
OR
+/-
Illness related
Chronic (> 3 months)
- CF, short gut syndrome
Nutrient loss
Hypermetabolism
Altered utilization of nutrients
Malabsorption
Inflammation
29

Malnutrition in Pediatric Gastroenterology
0
5
10
15
20
25
Normal Moderate Malnutrition Severe Malnutrition
43% 43%
7%
Of the malnourished • 50% were admitted
with a nutrition‐related diagnosis
• Only 40% received nutrition intervention
Malnutrition in the hospitalized Peds GI patient
Consult service
• Cardiac patients
• Renal patients
• Oncology/BMT
• PICU
• Neurology patients
• Cystic fibrosis
GI service
• Chronic liver disease
• Short bowel syndrome
• Crohn disease
Any patient that has been in the hospital for more than 4-5 days
What can we do about malnutrition?
30

Identify it!
Treatment of malnutrition
Non-illness related Starvation- Anorexia nervosa
Acute (<3 months)
- Trauma, burns
OR
+/-
Illness related
Chronic (> 3 months)
- CF, short gut syndrome
Nutrient loss
Hypermetabolism
Altered utilization of nutrients
Malabsorption
Inflammation
Feed!
Reverse nutrient loss & malabsorption
Treat inflammation
In the outpatient setting…
• High-calorie beverages
• Cyproheptadine
• Enteral nutrition
• Parenteral nutrition
31
In the inpatient setting…
• Enteral nutrition
• Parenteral nutrition
Billing and coding for malnutrition
Coding and Billing
Reimbursement = Primary Diagnosis + Comorbidity
• CPT Codes:
√ 263.1 = Mild malnutrition
√ 263 = Moderate malnutrition
√ 262 = Severe malnutrition
32

$3,950 $4,161
$5,304
$6,142
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
Asthma Tonsillitis
Malnutrition
Malnutrition
+38%
+47%
Billable hospital charges
Conclusions
• Malnutrition has a high prevalence and affects outcomes
• Seek out, identify and treat malnutrition
• You will be justified in billing the comorbidity ofmalnutrition if you identify and treat it!
33

34

Management of Food Allergy & FPIES
NASPGHAN 2015October 8, 2015
Hugh A Sampson, MD
Dean for Translational Biomedical Sciences
Professor of Pediatrics
Department of Pediatrics/Allergy & Immunology
Director, Jaffe Food Allergy Institute
Faculty Disclosures• FINANCIAL INTERESTS
I have disclosed below information about all organizations and commercial interests, other than my
employer, which may create or be perceived as a conflict of interest.
Name of Organization Nature of Relationship
Allertein Therapeutics, LLC Consultant, Minority StockholderRegeneron Therapeutics Consultant
Food Allergy Research & Education Medical Advisory BoardDanone Research Scientific Advisory Board
• RESEARCH INTERESTSI have disclosed below information about all organizations which support research projects for which I serve as an investigator.
Name of Organization Nature of Relationship
National Institutes of Health Grantee
Food Allergy Research & Education Grantee
ThermoFisher Scientific Grantee
• Patents – EMP-123 (recombinant protein vaccine) & FAHF-2 (herbal product)
Learning Objectives
Discuss factors that may account for therise in food allergies
Recognize various forms of food allergiesincluding FPIES and other gastrointestinalfood allergic disorders
Diagnose and manage various forms offood allergies including FPIES
35
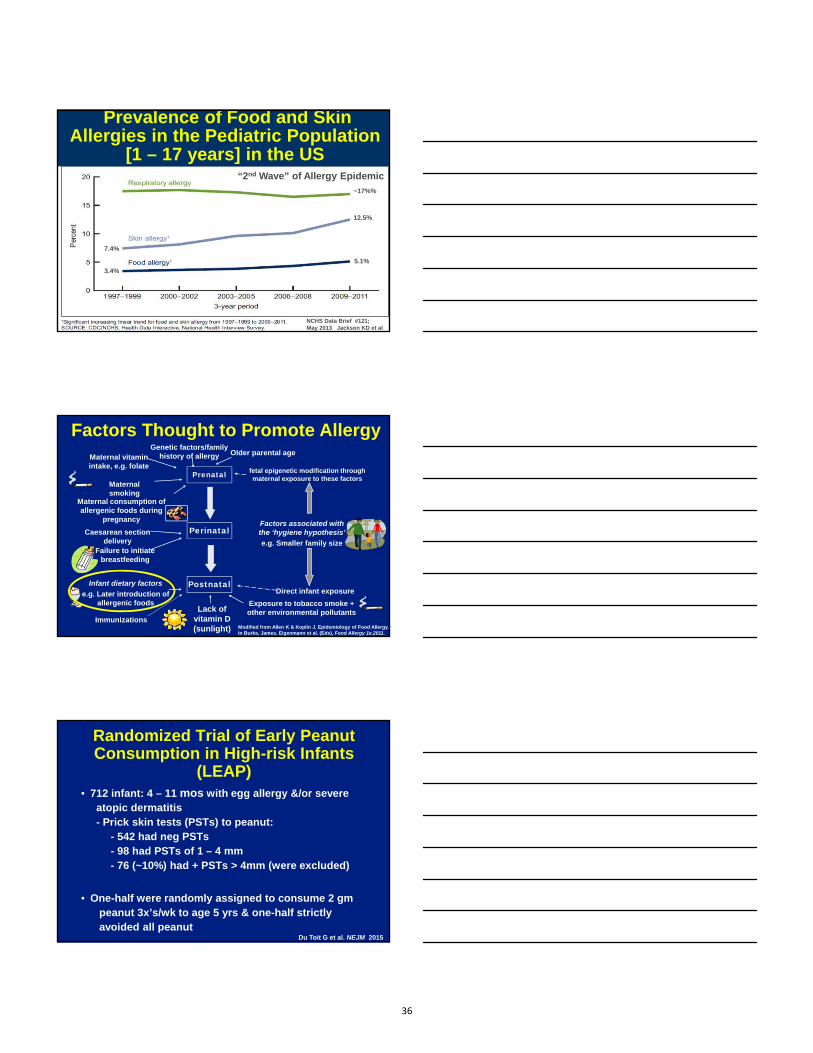
NCHS Data Brief #121; May 2013 Jackson KD et al
“2nd Wave” of Allergy Epidemic
5.1%
3.4%
7.4%
12.5%
~17%%
Prevalence of Food and Skin Allergies in the Pediatric Population
[1 – 17 years] in the US
Prenatal
Genetic factors/family history of allergy
Maternal smoking
Maternal consumption of allergenic foods during
pregnancy
Older parental age
Modified from Allen K & Koplin J. Epidemiology of Food Allergy. In Burks, James, Eigenmann et al. (Eds), Food Allergy 1e.2011.
fetal epigenetic modification through maternal exposure to these factors
Direct infant exposure
Factors associated with the ‘hygiene hypothesis’
e.g. Smaller family size
Maternal vitamin intake, e.g. folate
Perinatal
Failure to initiate breastfeeding
Caesarean section delivery
Factors Thought to Promote Allergy
Exposure to tobacco smoke + other environmental pollutants
Postnatal
Lack of vitamin D (sunlight)
Infant dietary factors
e.g. Later introduction of allergenic foods
Immunizations
Randomized Trial of Early Peanut Consumption in High-risk Infants
(LEAP)• 712 infant: 4 – 11 mos with egg allergy &/or severe
atopic dermatitis- Prick skin tests (PSTs) to peanut:
- 542 had neg PSTs - 98 had PSTs of 1 – 4 mm - 76 (~10%) had + PSTs > 4mm (were excluded)
• One-half were randomly assigned to consume 2 gmpeanut 3x’s/wk to age 5 yrs & one-half strictly avoided all peanut
Du Toit G et al. NEJM 2015
36

• One PST negative infant & 6 PST pos infantsreacted to peanut on initial challenge & did not consume peanut
- 4/7 still reacted at 5 yrs of age
• Adherence: median consumption at 2 yrs:- 0 gm in avoidance group - 7.7 gm in consumption group
• Safety: no difference in severe adverse events
Randomized Trial of Early Peanut Consumption in High-risk Infants
(LEAP)
Du Toit G et al. NEJM 2015
LEAP Trial Outcome
Du Toit G et al. NEJM 2015
85% relative reduction !
70% relative reduction !
<3 yrs Overall Milk 2.5 0.3%Egg 1.5% 0.2%Peanut 1.4% 0.8%Fish 0.1% 0.4%Shellfish 0.1% 2.0%Sicherer SH & Sampson HA. Annu Rev Med. 2009; 60:261-278.
1
2 3 4 5 6 7 8 9 10 20+
3
5
7
9
11
13
1
% P
reva
len
ce
Prevalence of Food Allergy by Age in the United States
Years of Age
Affects ~12 million Americans
37

Cutaneous Allergies
IgE-Mediated Non-IgE-Mediated
Urticaria Atopic DermatitisAngioedema Dermatitis Herpetiformis
ContactDermatitis
4 month old breastfed infant withan eczematousrash - cleared with exclusion ofegg from mother’sdiet
With permission
Atopic Dermatitis& Food Allergy
Mother ingestedeggs 4 hours beforebreast-feeding -
~30 minutes later, the baby is irritable and has developed facial rash
With permission
Atopic Dermatitis& Food Allergy
38

Erythematousrash on extensor surfaces
With permission
Atopic Dermatitis& Food Allergy
Gastrointestinal Allergies
IgE-Mediated Non-IgE-Mediated
Oral Allergy EoE EnterocolitisAcute GI AEG Enteropathy
Hypersensitivity - Celiac Disease
Proctocolitis
Eosinophilic Esophagitis (EoE)
• Onset - infancy to adulthood
• Symptoms- Young children: reflux esophagitis, vomiting, food
refusal, abdominal pain, irritability sleep disturbance & FTT
- Adolescents: chest pain, dysphagia, globus &impaction
• Foods implicated - milk, wheat, soy, egg, beef, corn- often involves multiple foods
• Diagnosis - failure to respond to PPIs- endoscopy and biopsy of esophagus
39

EoE: Endoscopic Diagnosis
Normal
Furrows
Rings
Plaques Plaques & Furrows
Pre-Diet Esophageal Biopsy
Kelly et al. Gastroenterology 1995
Post-Diet Esophageal Biopsy
Kelly et al. Gastroenterology 1995
40
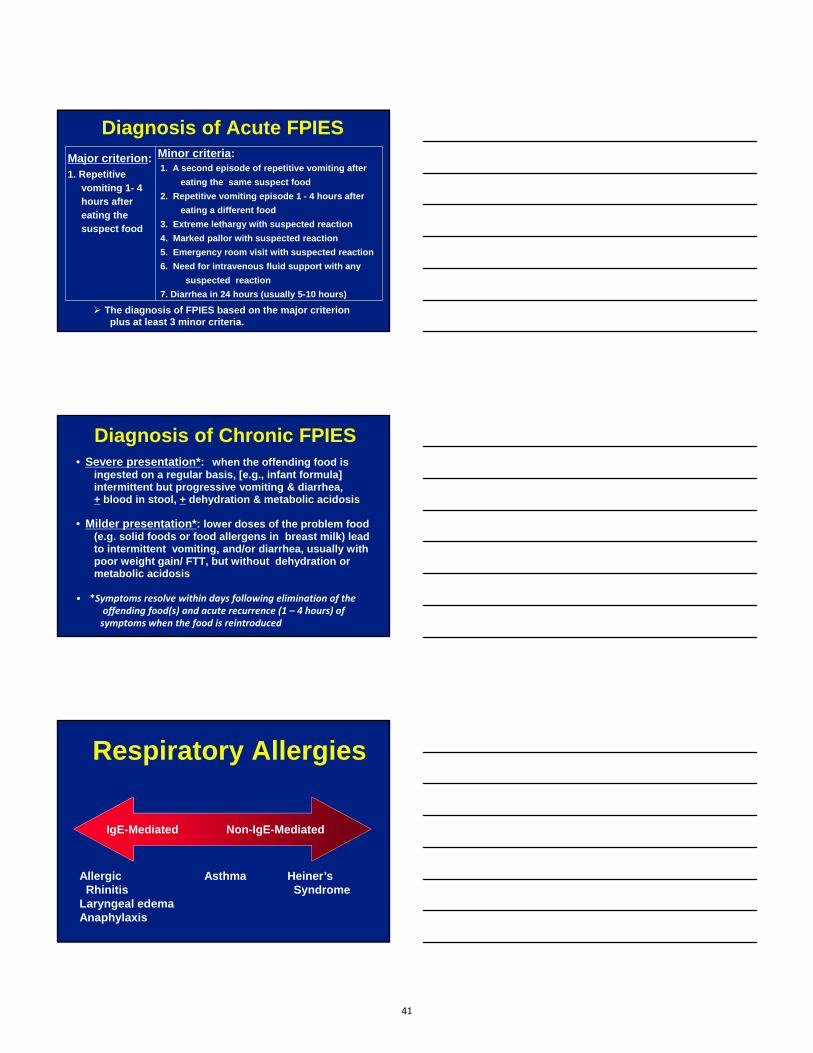
Diagnosis of Acute FPIES
Major criterion:1. Repetitive
vomiting 1- 4hours aftereating thesuspect food
Minor criteria:1. A second episode of repetitive vomiting after
eating the same suspect food
2. Repetitive vomiting episode 1 - 4 hours after
eating a different food
3. Extreme lethargy with suspected reaction
4. Marked pallor with suspected reaction
5. Emergency room visit with suspected reaction
6. Need for intravenous fluid support with any
suspected reaction
7. Diarrhea in 24 hours (usually 5-10 hours)
The diagnosis of FPIES based on the major criterionplus at least 3 minor criteria.
Diagnosis of Chronic FPIES • Severe presentation*: when the offending food is
ingested on a regular basis, [e.g., infant formula] intermittent but progressive vomiting & diarrhea, + blood in stool, + dehydration & metabolic acidosis
• Milder presentation*: lower doses of the problem food(e.g. solid foods or food allergens in breast milk) lead to intermittent vomiting, and/or diarrhea, usually with poor weight gain/ FTT, but without dehydration or metabolic acidosis
• *Symptoms resolve within days following elimination of the offending food(s) and acute recurrence (1 – 4 hours) of symptoms when the food is reintroduced
Respiratory Allergies
IgE-Mediated Non-IgE-Mediated
Allergic Asthma Heiner’sRhinitis Syndrome
Laryngeal edemaAnaphylaxis
41
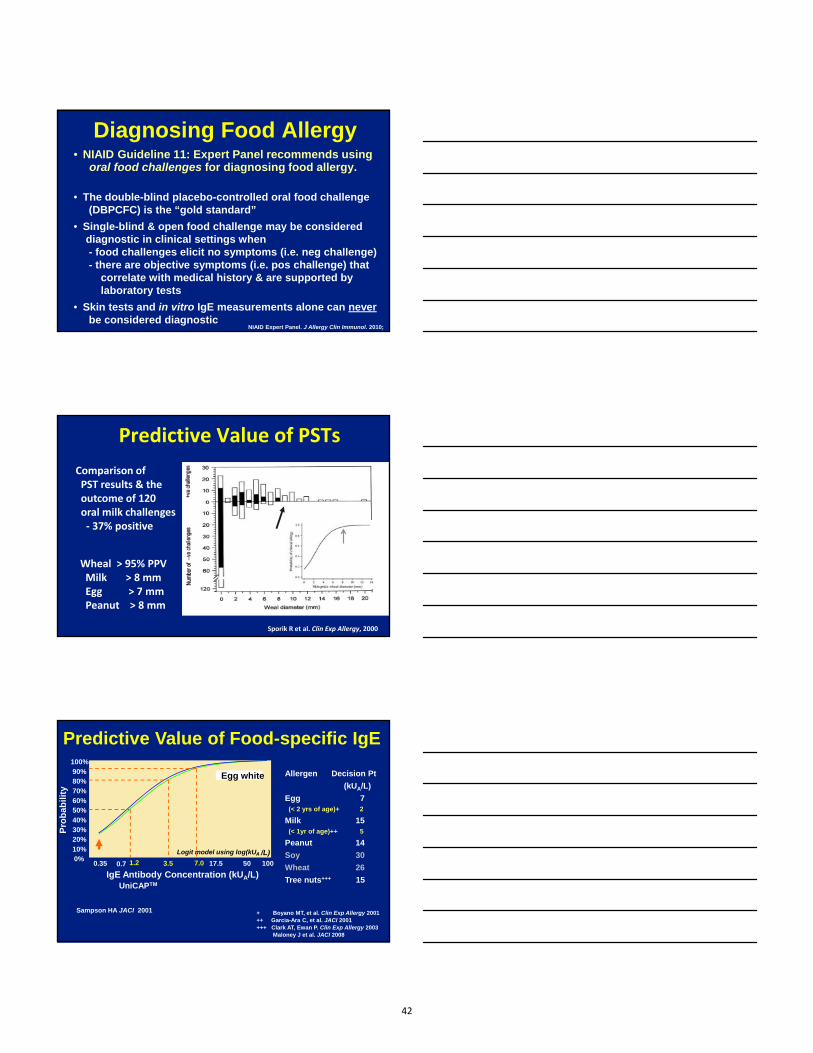
Diagnosing Food Allergy• NIAID Guideline 11: Expert Panel recommends using
oral food challenges for diagnosing food allergy.
• The double-blind placebo-controlled oral food challenge(DBPCFC) is the “gold standard”
• Single-blind & open food challenge may be considereddiagnostic in clinical settings when - food challenges elicit no symptoms (i.e. neg challenge) - there are objective symptoms (i.e. pos challenge) that
correlate with medical history & are supported bylaboratory tests
• Skin tests and in vitro IgE measurements alone can neverbe considered diagnostic
NIAID Expert Panel. J Allergy Clin Immunol. 2010;
Predictive Value of PSTs
Comparison ofPST results & theoutcome of 120 oral milk challenges‐ 37% positive
Sporik R et al. Clin Exp Allergy, 2000
Wheal > 95% PPVMilk > 8 mmEgg > 7 mmPeanut > 8 mm
Predictive Value of Food-specific IgE100%
80%90%
70%60%50%
40%30%20%
10%0%
0.35 0.7 17.5 50 100
IgE Antibody Concentration (kUA/L)UniCAPTM
Pro
bab
ilit
y
Egg white
Logit model using log(kUA /L)
7.03.51.2
Sampson HA JACI 2001
Allergen Decision Pt
(kUA/L)
Egg 7(< 2 yrs of age)+ 2
Milk 15(< 1yr of age)++ 5
Peanut 14
Soy 30
Wheat 26
Tree nuts+++ 15
+ Boyano MT, et al. Clin Exp Allergy 2001++ Garcia-Ara C, et al. JACI 2001+++ Clark AT, Ewan P. Clin Exp Allergy 2003
Maloney J et al. JACI 2008
42

FPIES Oral Food Challenge
Major Criterion Minor CriteriaVomiting in the 1-4 hour periodafter ingestion of the suspect food and the absence of classic IgE-mediated allergic skin or respiratory symptoms
1. Lethargy 2. Pallor3. Diarrhea in 5-10 hours after
food ingestion 4. Hypotension5. Hypothermia6. Increased PMN’s > 1500
above the baseline count
Challenge: 0.06 – 0.6 gm/kg (up to 3 gm) in 3 doses over 30 mins
Treatment: IV saline bolus (20ml/kg); ondansetron (0.1-0.15 mg/kg IV or IM)
Natural Course of Food Allergy
Birth 2 4 6 8 Years
• Following standard of care: strict food allergen avoidance
Pe
rce
nt
wit
h c
linic
al
foo
d
alle
rgy
100
80
60
40
20
0
Effect of Baking (heat-denaturation) on Sequential & Conformational
Epitopes of Food Proteins
1
2
LLI
M
KM I
Heat &Processing
M II
M
K
LK
L
K
~80% of young children with milk (egg) allergy “outgrow” theirfood allergy; react primarily to conformational epitopes
43

Development of Tolerance
N = 60
N = 57
Milk: Treated vs. Controls
16 x’s more likely to develop fulltolerance at 5 yrs compared tocontrol; p < 0.0001
Kim et al. JACI 2011; 128:125-131
~15 x’s morelikely to tolerateegg at 6 years
Egg: Treated vs. Controls
Leonard S et al. JACI 2012; 130:473-80
Managing Food Allergy & Food-induced Anaphylaxis
• Appropriate diagnosis of specific food allergy
• Education- strict avoidance of food allergen- learn to read food labels & recognize high risk situations- early signs of an allergic / anaphylactic reaction
• Provide emergency treatment plans in writing- FARE website: www.foodallergy.org
• Provide self-Injectable epinephrine& liquid antihistamine
• Instructions to go to amedical facility
Managing FPIES• Strict elimination of the culprit food(s)
- milk, soy, rice, oat, other grains, fish & shellfish
• Plans for dietary advancement- infants should be challenged every 1 – 2 years
• Treatment of symptoms at presentation or re-exposure- IV fluids (10-20ml/kg); IV or IM ondansetron; - International Association for Food Protein Enterocolitis
website, http://fpies.org/docs/Emergency_Plan.pdf
• Plan for supervised OFCs to address FPIES resolution- in milk-FPIES diagnosed by 6 mos, 50% outgrown by 1
year and 90% by 3 years of age- 50% of children with “solid food” FPIES react to more
than one food; reactivity may persist longer
44

Immunotherapeutic Strategies in Human Trials
• Allergen-specific Immunotherapy- Heat-denatured protein- Oral immunotherapy (OIT) + omalizumab- Sublingual immunotherapy (SLIT)- Epicutaneous immunotherapy (EPIT)- Engineered recombinant protein- Nanoparticles with CpG
• Allergen non-specific immunotherapy
- Chinese Herbal medications- Anti-IgE immunotherapy
Conclusions• Food allergy has increased dramatically over the
past 15 years and now affects ~4% of the US population
• Although the oral food challenge remains the “goldstandard” for diagnosis, laboratory tests are becoming more sensitive and specific
• Several therapeutic strategies are underinvestigation, but OIT provides the most protection
• Omalizumab dramatically reduces adverse reactionsto OIT and markedly alters its safety profile
• Several new therapeutic approaches in the“pipeline” that could induce more lasting effect
45

Dangerous Mimicry: Addressing Caustic Ingestions
in Children
Mark E. McOmber, M.D.Director of Endoscopy and Therapeutic Endoscopy
Phoenix Children’s HospitalPhoenix, AZ
Financial Disclosure
I have no financial relationship with any commercial entity to disclose
Objectives
• Review the epidemiology and pathophysiologyof caustic ingestions
• Know the key features of the clinicalassessment
• Review the treatment options and long termmanagement
46

Epidemiology
• Nearly 200,000 ingestions reported per year• Most are accidental and the amounts small• Most are young children from 1‐3 yrs old• In adolescents the ingestions tend to be
intentional, as a suicide attempt, and thequantities are larger
• There are limited reports of ingestion injury asa result of child abuse
Accidental Ingestions
• Alkaline agents more common than acidic• Household cleaning products
– Toilet bowl and oven cleaners
• Cosmetic products– Hair relaxers
• Dishwasher/Laundry agents• Pool products
* Batteries/magnets are unique and were covered separately
Mimicry‐ When Marketing and Safety are at Polar Opposites
• Agents are often mistaken for more palatableitems by young children– Colorful– Misleading container or wrapper may suggest a
safer substance– Overly Accessible
47

Colorful
A delicious candy?‐ offered by a smooth talking person with a fancy accent
Or poison?
Misleading Wrappers and Containers
Accessibility

Mechanism of Injury
• Alkaline agents (esp. pH >11.5),– injury through LIQUEFACTION necrosis– Deep penetration dependent on concentration and
duration of exposure
• Acidic agents (esp. pH <2),– injury through COAGULATION necrosis– more superficial because of the esophageal mucosa
and the coagulum/eschar– Antral spasm can pool the acid in the stomach,
resulting in outlet obstruction from injury and fibrosis
Mechanism of Injury
• Delayed damage beyond the necrosis over thefirst week– From inflammatory process– From vascular thrombosis
• By the third week fibrogenesis and stricturesbecome more likely
Clinical Manifestations
• Dysphagia is the MOST COMMON symptom– Related to dysmotility from inflammation, and
later from fibrosis/stricture• Drooling (even in the absence of oral burn)• Pain• Vomiting• Perforation• Airway injury with stridor, hoarse voice,
respiratory distress
49

Evaluation
• History– Timing of exposure– Type and amount of exposure
• pH can be measured or use of Material Safety Data Sheets or Poison Control Center (in U.S. 800.222.1222)
• Exam– Mental status, vitals, respiratory and oral exams
Evaluation
• Imaging– CXR if respiratory symptoms
• Retained foreign body, perforation, or pneumonia– Esophagram unreliable for early injury unless
perforation is suspected by other imaging• If done, use only water‐soluble contrast
– CT or MRI when perforation is suspected or concern of vascular involvement
Initial Management
• Supportive with IVF and limit further injury• Induction of vomiting is CONTRAINDICATED
– Leads to further esophageal injury and risk ofaspiration
• Neutralizing agents, dilution, and charcoal areNOT recommended– Additional damage from heat injury– Increase risk of vomiting– Obscure findings on endoscopic evaluation
50

Initial Management
• Asymptomatic (no oral burn, dysphagia, emesis, etc.)
– Endoscopy unnecessary unless . . .• pH of substance is more caustic (>11.5 or <2) or the
causticity is unknown
• Symptomatic– Admit for supportive care– Prepare for endoscopy– Hold oral nutrition until initial evaluation is
complete
Initial Management
• Endoscopy– Ideally within 24 hours of ingestion– Very early endoscopy (less than 6 hours after
ingestion) may not show full extent of the injury– After 4 days, the risk of perforation increases
• Contraindications– Hemodynamic instability– Evidence of perforation– Respiratory distress– Severe oropharyngeal injury with edema and necrosis
Endoscopy
• Staging– Grade 0 is normal mucosa– Grade 1 is superficial with edema or
hyperemia– Grade 2a: friable, hemorrhage, erosions,
blisters, shallow ulcerations, white membrane• 2b‐ above plus circumferential OR focal but
deep – Grade 3a: grade 2 PLUS focal necrosis that is
brown‐black or grey discoloration• 3b‐ extensive whereas 3a is only focal
2b
3a
51

Outcome by Stage
• 1 or 2a‐ most have a good prognosis and donot develop stricture or outlet obstruction– Risk of stricture with 2a is 4.7%
• 2b and 3‐ 32% to 75% develop strictures in 2band 3 grade burns, respectively
• 3b‐ mortality reported up to 65%; majorityrequire esophagectomy/replacementsurgeries
Management
• Grade 1 or 2a‐ short observationand PO challenge
• Grade 2b and 3– Consider NG placement under
endoscopic guidance• Maintain lumen• Route for future feeding
VS.
• Concern for infection, GER• Concern for long stricture
2a
3a
2b
Management of Grade 2b and 3
• Steroids?– Prevent strictures in animal models– Mixed results in human studies
• *3 days of high dose methylprednisolone (1g/1.73m2) reduced the stricture occurrence without noted side effects in 83 children with grade 2b burns
• Other studies suggest increased incidence ofinfection without a decrease in stricture incidence
*Usta et al. Pediatrics 2014
52

Management of Grade 2b and 3• Antibiotics?
– Lack of evidence to support or guide use andpatient selection
– Suggested in cases where infection is suspected or at an increased risk
• Perforation• Grade 3 esophageal injury• On corticosteroid therapy
– 3rd generation cephalosporins, ampicillin/sulbactam, piperacillin/tazobactam, etc.
Management of Grade 2b and 3
• Acid Blocker (PPI or H2RA)?– Decrease acid and pepsin exposure to the injury– No controlled trials for efficacy– No study to determine duration or dose
Endoscopy
• Endoscopic Ultrasound (EUS)– Miniprobe EUS
• Safe but not all centers are trained in EUS • No difference in predicting early complications• May detect if muscle layer is intact which may
predict less stricture formation or the response to dilation
• More studies needed
Kamijo et al. Am J Gastroenterol 2004
53

Strictures
• Most common serious long‐term complicationof caustic ingestions
• 32‐75% chance of developing strictures ingrade 2b and 3 injury
• Develop as early as 3wks with 80% ofstrictures by 8 weeks post injury
Strictures
• Diagnostic imaging to evaluate forstricture is usually performed about2‐3 weeks after the injury.
• Dilation typically recommendedstarting 4‐6 weeks after injury– *Recent studies have shown less
stricture when done sooner (5‐15 days) but these retrospective studies were small with milder injuries (2a,2b)
*Boskovic et al. Eur J Gastroenterol Hepatol 2014;Temiz et al. World J Gastroenterol 2012
Endoscopic Dilation
54

Dilation
• Historically, Savary and Tuckerdilators‐ longitudinal shearing forces
• Currently, endoscopic balloondilation‐ applies radial pressure
• Serial dilations are often requiredand typically are done every 1‐3weeks until oral feeds are tolerated– Prospective studies are needed to
evaluate frequency
Long‐term Management
• Risk of esophageal adenocarcinoma orsquamous cell carcinoma is 1000x theoccurrence rate of the general population.
• Recommended to begin surveillance 15‐20years after the injury and repeat every 1‐3years thereafter.
Summary
• Accidental caustic ingestions are a majorhealth risk for young children
• Clinical symptoms can be misleading soendoscopy is the primary means of evaluation
• Stricture is the main complication• Evidence based treatment protocols are still
lacking and prospective studies are needed• Increased risk of esophageal cancer even years
after injury
55

1
Updates on Foreign Body Ingestions
Robert E. Kramer, MD, FASGE
Director of Endoscopy
Associate Professor of Pediatrics
Children’s Hospital Colorado
Financial Disclosure
No relevant financial relationships to disclose
Objectives
•Outline the timing and preparation of interventions dependent on type of ingestion
•Discuss changes in the management of button battery and magnet ingestions
•Review the management of glass and other sharp ingestions
•Summarize current state of knowledge regarding ingestion of detergent pods and superabsorbent materials
3
56

2
Crystalline Opportunity
•“What we are drawn to in this imperfect science, what we in fact covet in our way, is the alterable moment‐the fragile but crystalline opportunity for one's know‐how, ability, or just gut instinct to change the course of another's life for the better.”
― Atul Gawande, Complications: A Surgeon's Notes on an Imperfect Science
4
Timing of Endoscopic Intervention
5
Type Location Symptoms Timing
ButtonBattery
Esophagus YesorNo Emergent
Gastric/SB Yes Emergent
No Urgent(ifage<5andBB≥20mm)
Elective(ifnotmovingonserialX‐ray)
Magnets Esophagus Yes Emergent(ifnotmanagingsecretions,otherwiseurgent)
No Urgent
Gastric/SB Yes Emergent
No Urgent
Sharp Esophagus Yes Emergent(ifnotmanagingsecretions,otherwiseurgent)
No Urgent
Gastric/SB Yes Emergent(ifsignsofperforationthenwithsurgery)
No Urgent
FoodImpaction
Esophagus Yes Emergent(ifnotmanagingsecretions,otherwiseurgent)
No Urgent
Coin Esophagus Yes Emergent(ifnotmanagingsecretions,otherwiseurgent)
No Urgent
Gastric/SB Yes Urgent
No Elective
LongObject Esophagus YesorNo Urgent
Gastric/SB YesorNo Urgent
AbsorptiveObject
Esophagus Yes Emergent(ifnotmanagingsecretions,otherwiseurgent)
No Urgent
Gastric/SB YesorNo Urgent
Emergent (< 30 Min)
Emergent (< 2 hours)
Urgent (<8 Hours)
Elective (<24 Hours)
Preparation
• Optimal venue• Endoscopy unit, OR, IR, IC, Hybrid OR
• Additional personnel • Pediatric surgery, ENT, Cardiac surgery,
Interventional Cardiology• Fully stocked "Foreign Body" Tool Box• Ex‐vivo practice run to select best device• Additional tools
• Foreign body hood• Overtube• Blakemore tube• Banding device
6
57
3
Tools of the Trade
7
Raptor Forceps Multi-Prong Forceps Coin Grasper Rubber-Tipped Forceps
Polyp Snare Roth Net Wire Basket Endoscopy Caps
Foreign Body Hood Overtube
The Usual Suspects
8
10
30
20
1
60
50
40
mm
Button Batteries
• Home Movie Demonstration
9
58

4
Button Batteries (BB)‐ New Aspects
• Gastric/SB : Consider endoscopy in high risk group (Age ≦5, BB diameter ≧ 20 mm)
• Purpose: assess for esophageal injury, removal of battery is secondary
• To date only a single patient survived from aortoesophageal fistula (AEF)
• Further need to refine multidisciplinary care• Consider immediate transfer to Interventional Cardiology/
Hybrid OR for high risk cases• Vigilant for sentinel bleed, warning sign of catastrophic
hemorrhage• Ongoing injury, risk of AEF up to 3 weeks after removal• Maintain high index of suspicion for BB ingestion
• Any child < 5 with even slight hematemesis (consider X‐ray?)10
Magnet Ingestions
• Controversial aspect: Beyond ligament of Treitz, asymptomatic• Spectrum: observation surgical removal• Take ownership, especially long distance patients
• Balloon enteroscopy a good option• Highlights need for rapid endoscopic removal from
proximal GI tract• Advise against metal buckles, etc• Though technically off the market, still millions in
circulation
11
Neodymium Magnets
12
59
5
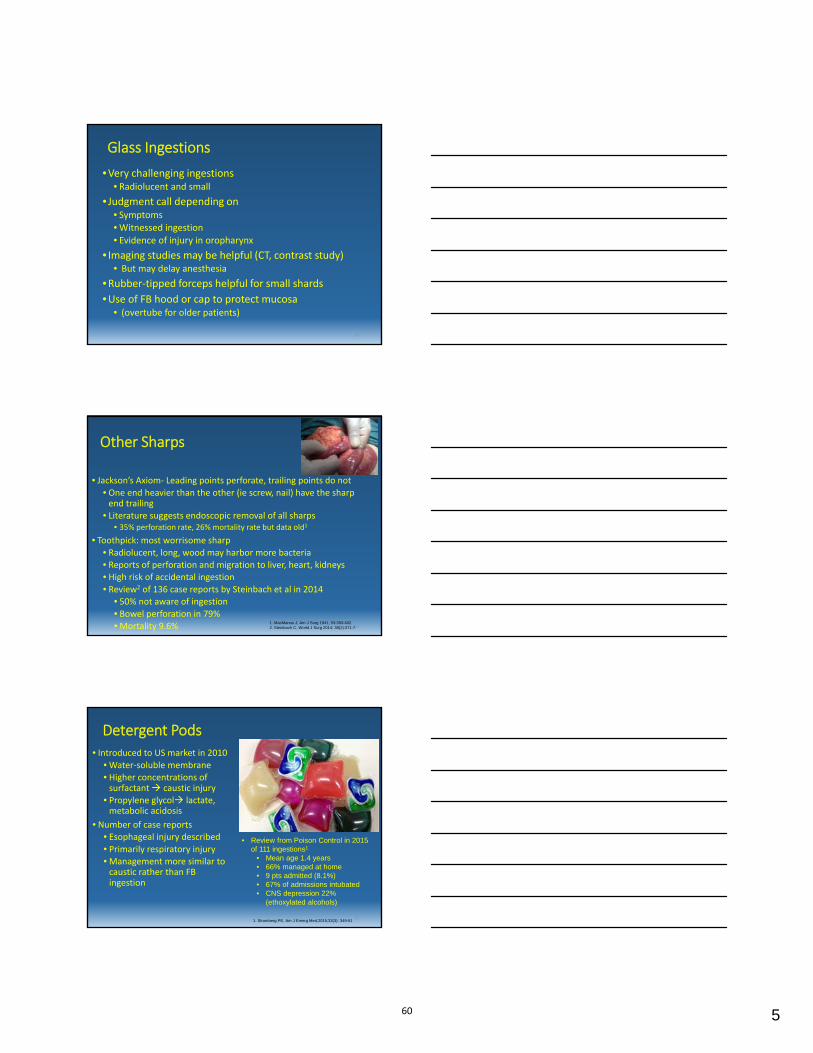
Glass Ingestions
• Very challenging ingestions • Radiolucent and small
• Judgment call depending on• Symptoms• Witnessed ingestion• Evidence of injury in oropharynx
• Imaging studies may be helpful (CT, contrast study)• But may delay anesthesia
• Rubber‐tipped forceps helpful for small shards• Use of FB hood or cap to protect mucosa
• (overtube for older patients)
13
Other Sharps
• Jackson’s Axiom‐ Leading points perforate, trailing points do not• One end heavier than the other (ie screw, nail) have the sharp
end trailing• Literature suggests endoscopic removal of all sharps
• 35% perforation rate, 26% mortality rate but data old1
• Toothpick: most worrisome sharp• Radiolucent, long, wood may harbor more bacteria• Reports of perforation and migration to liver, heart, kidneys• High risk of accidental ingestion• Review2 of 136 case reports by Steinbach et al in 2014
• 50% not aware of ingestion• Bowel perforation in 79%• Mortality 9.6% 14
1. MacManus J, Am J Surg 1941; 53:393-402.2. Steinbach C, World J Surg 2014; 38(2):371-7.
Detergent Pods
• Introduced to US market in 2010• Water‐soluble membrane• Higher concentrations of
surfactant caustic injury• Propylene glycol lactate,
metabolic acidosis• Number of case reports
• Esophageal injury described• Primarily respiratory injury• Management more similar to
caustic rather than FBingestion
15
• Review from Poison Control in 2015 of 111 ingestions1
• Mean age 1.4 years• 66% managed at home• 9 pts admitted (8.1%)• 67% of admissions intubated• CNS depression 22%
(ethoxylated alcohols)
1. Stromberg PE, Am J Emerg Med,2015;33(3): 349-51
60

6
Superabsorbent Objects
• Polymers that can absorb up to 100x their weight in water• Found in a number of household objects
• Diapers, feminine hygiene products• Used in many toys, under the name Water Balz, H2O Orbs
• Radiolucent• May reach 30‐60x original volume• May be easily swallowed and cause obstruction as they expand• Large round shape, likely best removed with a net
• Four reports in the literature with one documented death1
• Led to a recall by CPSC in 2012• Reports of canine ingestion of feminine hygiene products in
veterinary literature, but none in humans
161. Zamora IJ, Pediatrics 2012; 130(4):e1011-4.
Water Balz
17
Coin Ingestions• Most common FBI in children
• >250,000 ingestions, 20 deaths in 10 year period1
• Distal esophageal coins may clear in up to 60%2
• Coins > 23.5 mm (American, Canadian quarters) more likely tobecome impacted in children < 5 yo
• Majority of ingestions are pennies• Post 1982 zinc 5% 97.5%• Causes corrosive injury in acid environment
• Production of hydrogen gas and zinc chloride production (O’Hara S)• Newer pennies may appear less dense in center on X‐ray• Coin grasper may not be as effective as rat‐tooth or alligator jaw
forceps• Get lateral film to differentiate from BB
18
1. Chen X, Int J Pediatr Otorhinolaryngol 2006;70:325-9.2. Tander B, J Laroendosc Adv Surg Tech A 2009;19:241-3.
61

7
Summary
•Management of FBI’s in children depends on the object, location, timing, age and symptoms
•BBI and multiple magnet ingestion remain the most dangerous FBI in children and may require aggressive management even in asymptomatic patients
•A multidisciplinary approach is often necessary in complicated FBI’s and requires good communication between GI, surgery, CV surgery, ED, Radiology, ENT
•Detergent pods and superabsorbent objects pose an emerging threat for ingestion in children
19
APPENDIX 1‐ BUTTON BATTERY
20
Witnessed or suspectedBB Ingestion
Esophageal
Otherwise Stable:
Immediate Endoscopic
Removal
Active Bleeding or Clinically Unstable:
Endoscopic removal in OR with Surgery/CV surgery
present
If evidence of any esophageal injury:
Admission, NPO, IV anbx
Consider CT Angiography to exclude aortic injury. Consider MRI of chest to determine proximity of
injury to aorta
No significant injury to surrounding tissue or
proximity to aorta
Esophagram to exclude leak before
advancing diet as tolerated
Demonstation of injury close to aorta
Continue NPO and Anbx and serial MRI q 5‐7 days until injury seen to recede from
aorta
If presence of hematemesis or UGI bleeding within 21 days of removal, assume aortoenteric fistula and emergently prepare for thoracotomy
with CV surgery
Gastric or Beyond
<5 years of age AND
BB >20 mm
Consider assessment of any esophageal injury
and endoscopic removal if possible, within 24‐48
hours
If esophageal injury present: Admit, NPO, IV anbx and consider CT Angiography, MRI
of chest
≥5 years of ageAND/OR
BB < 20mm
May consider outpatient
observation only
Repeat X‐ray in 48 hours for BB ≥20 mm,
repeat at 10‐14 days for BB < 20 mm if failure to
pass in stool
Endoscopic removal if
develops GI symptoms or not passed stomach by time of X‐ray
at time described above
Adapted from Kramer RE, et al. JPGN, 2015, PMID 25611037
APPENDIX 2‐MAGNET INGESTION
21
I i i l P i
Determinesingleversusmultiplemagnetingestion
InitialPresentation‐ObtainHistory
‐KnownMagnetingestion‐UnexplainedGIsymptomswithrareearthmagnetsinenvironment
‐ObtainanabdominalX‐ray.Ifmagnetsarepresentonflatplateobtainlateralx‐ray‐Determinesingleversusmultiplemagnetingestion
SingleMagnet MultipleMagnet(orsinglemagnet&metallicobject)
Withinthestomachoresophagus
‐Option1:ConsultPediatricGIifavailable‐Considerremovalifpatientatincreasedriskforfurtheringestion‐Option2:Followserialx‐raysasoutpatientandeducateparents*
Beyondthestomach‐ConsultpediatricGIifavailable.‐Considerremovalifpossible.‐Followwithserialx‐raysasoutpatient‐Educateparents*‐Confirmpassagewithserialx‐ray‐IfdelayedprogressionmayusePEG3350orotherlaxativetoaidpassage
Allwithinthestomachoresophagus
‐IfpediatricGIavailablenotifyforremovalespeciallyiflessthan12hours
‐Ifnotavailable,transfertoreferralcenter
‐Ifgreaterthan12hoursuntiltimeofprocedure,thenconsultpediatricsurgerypriortoendoscopicremoval
Successfulremoval
‐Dischargehomewithfollow‐up&education
Unsuccessfulremoval
‐Refertosurgeryforremoval
Beyondthestomach
‐ConsultpediatricGIandpediatricsurgeonifavailable
‐Ifnotavailablesendtoreferralcenter
‐Managementdependsonwhethersymptomaticorasymptomatic
Symptomatic
‐Refertopediatricsurgeryforremoval
Asymptomatic
‐Ifnoobstructionorperforationonx‐raymayremovebyenteroscopyorcolonoscopyifavailableorfollowwithserialx‐ray
‐Maydoserialx‐rayinEDtocheckforprogressionevery4‐6hours
SuccessfulEndoscopicRemoval‐Dischargeafterfeedingtolerance,withappropriatefollow‐upandeducation
Noprogressionon
serialx‐rays
‐Admitforfurthermonitoringandserialx‐raysorsurgicalremoval
‐MayusePEG3350orotherlaxativetoaidinpassageandtohelpprepareforcolonoscopy
‐Continueserialx‐rayevery8‐12hours.Ifnosymptomsthenproceedwithsurgicalremovalorendoscopicremovalwithsurgicalback‐up
Progressionofmagnetsonserialx‐rays
‐Educateparentsonprecautions*anddischargewithclosefollow‐up
‐Confirmpassagewithserialx‐rays
‐Ifatanytimemagnetsdonotprogressorpatientbecomessymptomatic,admittohospitalforremovalofmagnets
*ParentalEducation:‐Removeanymagneticobjectsnearby‐Avoidclotheswithmetallicbuttonsorbeltswithbuckles‐Ensurenoothermetalobjectsormagnetsareinthechildenvironmentforaccidentalingestion
Adapted from Kramer RE, et al. JPGN, 2015, PMID 25611037
62

8
APPENDIX 3‐ SHARP INGESTION
22
Known or suspected ingestion of sharp object
Radio‐opaque
Esophageal: Urgent endoscopic
removal
Gastric
Consider endoscopic removal unless short object with heavier
blunt end
Small bowel (distal to ligament of Treitz)
Symptomatic
Enteroscopy or surgical removal
Asymptomatic
Follow clinically with serial X‐ray
Enteroscopy or surgical removal considered if develops symptoms or
> 3 days without passage
Radiolucent
Symptomatic self‐reported or
witnessed ingestion:Urgent endoscopic
evaluation and removal
Asymptomatic: Consider CT, ultrasound, MRI or esophagram for further
assessment
Evidence of FB: Endoscopic
removalNo evidence of FB:
Clinical observation, close follow‐up,
reassess if develops symptoms
Adapted from Kramer RE, et al. JPGN, 2015, PMID 25611037
APPENDIX 4‐ FOOD IMPACTION
23
Suspected EFI
Consider FB series with water‐soluble contrast to identify
obstruction
Not tolerating secretions:Urgent endoscopic
removal
Obtain Proximal and distal esophageal biopsies and assess for stricture
GI Follow‐up
Stricture without eosinophilic
inflammation
Consider repeat endoscopy with possible
dilation
Eosinophilic inflammation with
stricture
Consider repeat endsocopy after 4‐8 weeks of PPI therapy and/or EoE therapy
Eosinophillic inflammation without
stricture
Consider repeat endsocopy after 4‐8 weeks of PPI therapy
No eosinophilic inflammation and no
stricture
Follow clinical status and consider PPI if
nonspecific inflammation present
Tolerating secretions:Endoscopic removal
within 24 hours
Adapted from Kramer RE, et al. JPGN, 2015, PMID 25611037
APPENDIX 5‐ COIN INGESTION
24
Coin ingestion:PA and lateral films,
ensure no button battery
Esophageal
Symptomatic (drooling, dysphagia, respiratory
compromise):Urgent endoscopic
removal
Asymptomatic:Endoscopic removal
within 24 hoursConsider glucagon if
distal esophageal coin or if endoscopy not readily
available
Gastric
No endoscopy needed: Consider straining stools,
laxatives, repeat x‐ray at 2 weeks
Endoscopic removal if not passed within 2‐4 weeks
Repeat X‐ray immediately prior to removal to ensure
coin still present
Small bowel
Clinical observation: Enteroscopy/surgical
removal if symptomatic
Adapted from Kramer RE, et al. JPGN, 2015, PMID 25611037
63
THE PROBLEMATIC POLYP
Petar Mamula, MDThe Children’s Hospital of Philadelphia
• I have no financial relationships to disclose
OBJECTIVES
1. Review prerequisites for successfulpolypectomy
2. Discuss techniques for difficult polyps
3. Review polypectomy complications
64

Polypectomy video clip
DEFINITION
• Greek polύpous‐ animal withmouth surrounded by tentacleslike hydra
• Difficult or problematic polyp‐ any polyp thatposes difficulties in removing and can be furtherdefined by its size, location, shape, or number
DEFINITION• SIZE: 2‐3 cm large and >3 cm giant polyp• LOCATION:
– involving 2 colon folds– >1/3 of luminal circumference– cecum/right colon, appendiceal orifice, IC
valve, upper GI tract• SHAPE: Pedunculated‐ stalk and head
Sessile‐ height > ½ base diameterFlat‐ height < ½ base diameter
• NUMBER: >10 polyps
65

DEFINITION
Gupta et al. Gut. A129. 2011.
SMSA ClassificationLevel 1 (4‐5)Level 2 (6‐9)Level 3 (10‐12)Level 4 (>12)
NASPGHAN Training Guidelines‐ 10 procedures
PREREQUISITES
• PATIENT: anti‐coagulation/NSAIDS,preparation, laboratories
• EQUIPMENT: generator, accessories, irrigationpump, CO2 insufflation
• STAFF: experienced technician, collaborativeanesthesiologist
• ENDOSCOPIST: knowledge, experience
ENDOSCOPIST
Liu et al. JPGN. 2007.
66

EQUIPMENT‐ GENERATOR
• Ohm’s law: V = I x R• Power (Watts): P = V x I• Joule’s law: Q = I2 x R x t• Current types: coagulation (slower increase in
tissue temperature) and cut (cell burst)• Current density: (current/area)2
• Waveform (duty cycle)
EQUIPMENT‐ GENERATOR
Modern units with microprocessor keep voltage constant while power fluctuates depending on change in impedance
EQUIPMENT‐ ACCESSORIES
Monkemuller et al. Clinic Gastroenterol Hepatol. 2009.
67

POLYPECTOMY TECHNIQUE
• Colonoscope position: 5‐6 o’clock• Place the snare proximal to distal and parallel
to the colon wall• May require retroflexion, abdominal pressure,
or patient repositioning• Once snare in place lift the polyp and “jiggle”
during resection to avoid contact with the wall
POLYPECTOMY TECHNIQUE
POLYPECTOMY TECHNIQUE
• Pedunculated– Large stalk (>1 cm) may contain large vessel‐ consider
epinephrine injection or clip/loop placement– Large polyp may benefit from epinephrine head
injection in order to shrink it (up to 80% in size)– Giant polyp could be resected piecemeal
Tholoor et al. Ann Gastroenterol. 2013.
68
POLYPECTOMY TECHNIQUE
• Video stalk clip placement
POLYPECTOMY TECHNIQUE
• Sessile/flat polyps– Up to 7 mm: cold snare– 1‐3 mm: cold biopsy forceps– <5 mm: hot biopsy‐ potential for thermal injury and
destroys the tissue (lift and burn)– >15 mm: endoscopic mucosal resection (EMR) with
submucosal injection which prevents injury to deeper layer and entrapment of muscularis propria
• Injectate‐ variety of solutions, commonly normal saline with methylene blue, amount may vary from few to >30 mL
POLYPECTOMY TECHNIQUE
• Sessile/flat polyps– Inject proximal to distal at a 30‐45° angle around or
into the polyp, start injecting before needle in– >20 mm in size: piecemeal resection– May consider cautery demarcation prior to injection– Important to have a feel for the amount of tissue
ensnared (mark the snare handle)– As the sheath is jiggled the polyp should move
independently from the colon wall
69
POLYPECTOMY TECHNIQUE
• Sessile/flat polyps– Aspirate and lift in order to tent the mucosa from
the submucosa prior to resection– Smooth snare closure– Worrisome signs‐ ulcer, induration, friability, and
no lift– Consider APC to treat remaining polyp tissue/edges– Tattoo the site
Polypectomy video clip
ADJUNCT POLYPECTOMY TECHNIQUES
• Cap‐assisted polypectomy• Two colonoscopes or combination of two
instruments• Double‐channel colonoscope• Side‐viewing duodenoscope• Laparoscopy‐assisted• Wide‐angle colonoscopy• Chromoendoscopy/NBI• Autofluorescence/Confocal laser microscopy• Endoscopic submucosal dissection
70

POLYP RETRIEVAL
• Up to 16% specimens lost• Net or snare• Polyp trap for small polyps
(≤5 mm)• Use the gravity effect to find
specimens
• Polyp retrieval video (cold snare/suction)
COMPLICATIONS
PERFORATION (0.1‐0.3%)• Risk higher with flat or sessile polyps, large
polyps, cecum, and longer electrocautery time• Post‐EMR inspection for “target sign”
Swan et al. GIE. 2011.
71

COMPLICATIONS
PERFORATION• Clip closure for lesions <15 mm• Stent placement• Over TheScope Clip
• If perforation not recognized and patientdischarged, likely to need surgery
Haito‐Chavez et al. GIE. 2014.
COMPLICATIONS
BLEEDING (0.3‐6%)• Early more likely to occur with the cutting
current and late (up to 2 weeks) with the coagulation current
• Treatment– Tamponade– Clips– Cautery, but risk of transmural burn– Prophylactic clip or loop
• Polyp bleeding video
72

COMPLICATIONS
POST‐POLYPECTOMY SYNDROME (2%)• Fever• Leukocytosis• Abdominal pain• Absence of free air on imaging
• Thermal energy extending into muscularis propriaand serosa
• Treatment consists of bowel rest, IV fluids and abx
SUMMARY
• Be prepared• Know your equipment and staff• Know your limitations• 1‐3 mm polyps can be removed with a cold
forceps, 5‐7 mm with a cold snare
SUMMARY
• >15 mm sessile/flat lesions requiresubmucosal injection
• >20 mm piecemeal resection• Consider pre‐treating large pedunculated
polyps• Instruct patient/family about possible
complications
73

REFERENCES1. Electrosurgery in Gastrointestinal Endoscopy: Principles to
Practice, Morris et al. Am J Gastroenterol. 2009.2. Electrosurgical generators. Technology Status Evaluation
Report. Tokar et al. GIE. 2013.3. Polypectomy Devices. Technology Status Evaluation
Report. Carpenter et al. GIE. 2007.4. Advanced Colon Polypectomy. Monkemuller et al. Clinic
Gastroenterol Hepatol. 2009.5. Colon Polypectomy. Kedia and Waye. J Clin Gastroenterol.
2013.6. Advanced Polypectomy. Waye, J. Gastrointest Endoscopy
Clin N Am. 2005.7. Colonoscopic Polypectomy. Tolliver and Rex. Gastroenterol
Clin N Am. 2008.
Thank you
74

C. difficile: Clostridium “Difficult” But Not Impossible
Stacy A. Kahn, MDAssistant Professor of Pediatrics and Medicine
Section of Pediatric Gastroenterology, Hepatology, & Nutrition
Director, Transitional IBD ClinicThe University of Chicago Medicine
Disclosures and Disclaimers
• Consultant: AbbVie• Fecal microbiota transplantation (FMT) is not
an approved therapy.• The FDA considers FMT a biologic and a
drug.• The use of FMT for indications other than
recurrent Clostridium difficile infection (CDI)or for research purposes requires FDA approval and an Investigational New Drug(IND) application.
Learning Objectives
• Learn appropriate identification and testingfor C. difficile
• Understand the current medical managementfor C. difficile
• Understand the role of fecal microbiotatransplantation (FMT) in C. difficile
75

• Leading cause of hospital-associated GI illness
• Increasing cause of community-associated GIillness
• Costs $3.2 billion annually1
• Rates of CDI have been increasing since 2000
• 2011: CDI was responsible for2
• ~ 500,000 infections
• 29,000 deaths
CDI: A Significant Healthcare Burden
1. Surawicz et.al. American J Gastroenterology 2013. 2. Lessa et. al. NEJM. 2015.
Incidence of Nosocomial CDI
Leffler DA, Lamont JT. N Engl J Med 2015;372:1539-1548
Rates of Pediatric CDI
• Overall Incidence: 24.2/100,000 (2011)1
– Community-Associated: 17.9/100,000
– Health-Care Associated: 6.3/100,000
• Estimated # of cases: 16,900 (2011)1
– Community-Associated: 12,500
– Health-Care Associated: 4,400
• Significant increase of CDI in pediatric IBD2
– 28.6/1,000 (1993-2012) vs. 46.9/1.000 (2009-12)
1. Lessa FC et al NEJM 2015. 2. Hourigan SK et al. Dig Dis Sci. 2014.
76

Severe Pediatric CDI• Far less common than in adults (2% vs 8-20%)
• More often hospital-associated (74%)
• Underlying conditions: malignancy, HSCT, geneticsyndrome, IBD, transplant, CF
• Symptoms: Fever (47%), abd pain (35%), bloodystool (17%), ileus (2%)
• Diarrhea: mild (22%), moderate (44%), severe(27%)
• 5/299 (2%) required ICU admission
• 1/299 (0.3%) death in HSCT pt w/CDI + GN sepsis
Schwartz KL et al. BMC Pediatrics. 2014.
Why is C. Diff so Difficult?
• Gram positive spore forming anaerobic bacteria
– Vegetative and dormant states
• “Bacillus difficile” because it was hard to grow &isolate
• Spores are HIGHLY resistant
– Heat, acid, disinfectants, antibiotics
• C. diff survives:
– Vegetative cells survive on surfaces for 24 hr
– Spores survive for months to years!Rupnik M. et al. Nature Reviews Microbiology 2009. www.bioquellus.com/technology/microbiology/clostridium-difficile/
• North American pulse-field type 1• Associated with epidemics (hospital-acquired)• Hypervirulent
– Exhibits quinolone resistance– Produces binary toxin which increases
production of toxins A + B– Increased use of quinolones may have
contributed to selection of this strain• Highly pathogenic
– Mortality 3x higher than other strains
Emergence of Virulent and Resistant Strains: NAP1/BI/027
1. Kelly et. al. NEJM. 2008. 2. Surawicz et. al. Nature Reviews: Gastroenterology & Hepatology. 2011. 3. Rupnik M et al. Nature Reviews Microbiology. 2009. 4. Leffler and Lamont. NEJM 2015.
77
• Disease caused by enterotoxin A and cytotoxin B– Interfere with protein synthesis– Causes cell membrane disruption and death1
• Host immune response may determine whodevelops symptoms2
– ~5% of healthy individuals are colonized withC. difficile2
– Development of IgG Abs against toxin A maycontribute to asymptomatic state3
– High IgG Abs decrease risk for RCDI by afactor of 444
CDI Mechanisms and Host Response
1. Khanna et. al. Inflamm Bowel Dis. 2013. 2. Warny et. al. Infect. Immun. 1994. 3. Surawicz et. al. Nature Reviews: Gastroenterology & Hepatology. 2011 4. Kelly et. al. NEJM. 2008.
• Clinical symptoms of CDI and IBD are the same.• Since 2000: significant increase of CDI in IBD• 1997‐2011: Hospitalization rates 5‐fold increase in
children/young adults with IBD and CDI– Compared with < doubling of the hospitalization
rates for IBD without CDI2
• Recurrent CDI in up to 1/3 of children and adults• Many IBD therapies increase risk of CDI and worsen its
clinical course
CDI in IBD: A Growing Problem
1. Russell et. al. Gastroenterology. 2014. 2. Sandberg et. al. Inflamm Bowel Dis. 2014.
“Traditional” Risk Factors:
• Antibiotic use (number and duration)
• Advanced Age (> 65 yo)
• Recent/prolonged hospitalization
• Immunosuppression
• Comorbidities
• Proton-pump inhibitors
• NG tubes
Risk Factors for CDI in the General Population
Vardakas et. al. International Journal of Infectious Dis. 2012.
78

• Antibiotic use less important
– Abx use preceding CDI is less common
• 40% of IBD patients vs. 69% in non-IBDpatients1
• 39% of IBD patients with CDI: no recentAbx use2
• Advanced age and comorbidities
– Average age of CDI in IBD cohortssignificantly lower3
Risk Factors are Not the Same in Patients with IBD
1. Bossuyt et. al. J Crohns Colitis. 2009. 2. Issa et. al. Clin Gastroenterol Hepatol 2007.3. Jen et. al. Ailment Pharmacol Ther. 2011.
Risk Factors: A Balancing Act In IBD
• Immunosuppression– Risk of therapy in CDI still unclear
• Maintenance immunosuppressive therapyassociated with 2x risk of CDI1
• No association between use immunosuppressivetherapy and heightened CDI risk in UC patients2
– Corticosteroids may heighten risk of infection
• Steroid initiation tripled the risk of CDI3
• IBD is an independent risk factor for CDI– 3x increased risk as compared to non-IBD patients4
1. Issa et. al. Clin Gastroenterol Hepatol. 2007.2. Kariv et. al. J Crohns Colitis. 2011.
3. Schneeweiss et. al. Ailment Pharmacol Ther. 2009. 4. Rodemann et. al. Clin Gastroenterol Hepatol. 2007.
• Only patients with diarrhea (> 3 liquidstools/day) should be tested for CDI!
• All hospitalized patients with IBD with a diseaseflare
• Ambulatory patients who develop diarrhea(even with no known risk factors)
• Patients s/p colectomy and IPAA that aresymptomatic
Who should we test?
Surawicz et. al. The Am Journal of Gastroenterol. 2013.
79

Nucleic acid amplification tests (NAATs)• PCR for toxin genes• Superior to A + B EIA testing• Risk of false positive even after Tx/asymptomatic pt
Toxins A + B Enzyme Immunoassay (EIA)• Lower sensitivity and specificity• Risk of false positive even after Tx/asymptomatic pt
Glutamate dehydrogenase (GDH) screening• Used in testing algorithms• Unable to distinguish toxigenic and nontoxigenic
strains
CDI Test Options
Surawicz et. al. The Am Journal of Gastroenterol. 2013.
Which Test to Choose?
TEST SENSITIVITY SPECIFICITY
NAAT PCR 100% 99.2%
A + B EIA 75 - 95% 83-98%
GDH screening 75 - >90% low
Surawicz et. al. The Am Journal of Gastroenterol. 2013.
The Perfect CDI Drug
High level of drug in colon
Little systemic absorption
Minimal disruption to commensalmicrobiota
Good safety profile
Affordable
Approved for pediatric use
http://www.examiner.com/article/new‐weight‐loss‐pills‐no‐cure‐for‐obesity‐crisis
80
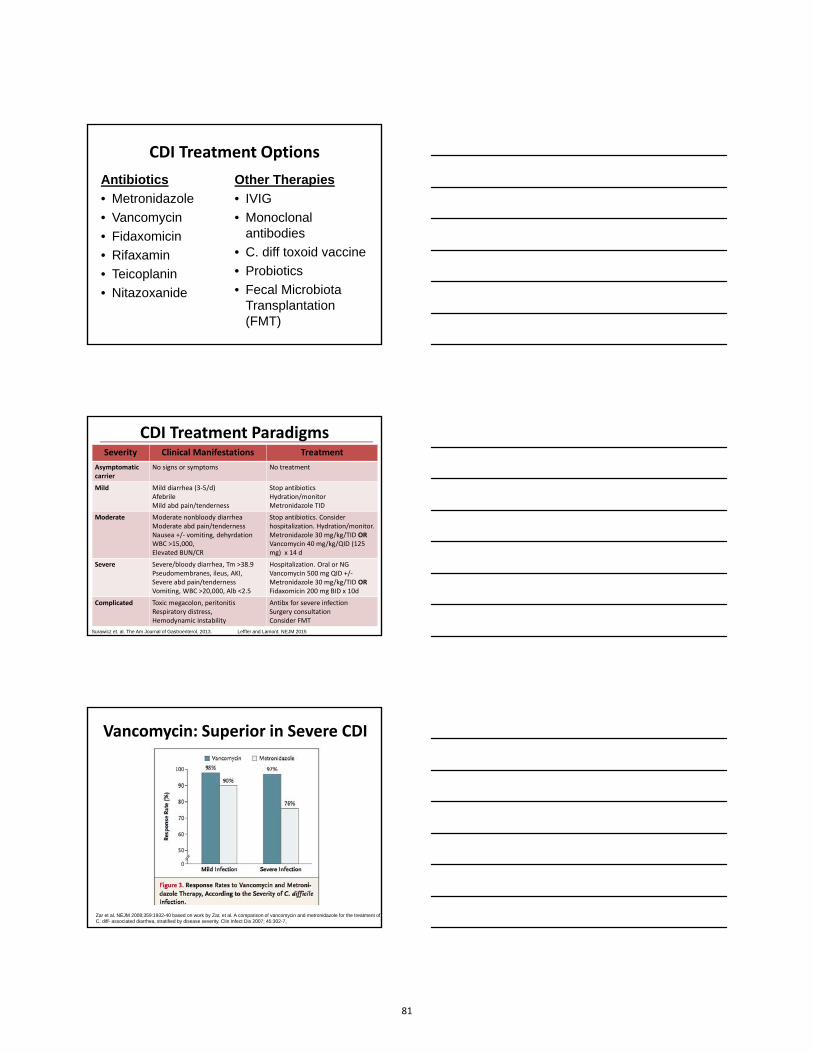
CDI Treatment Options
Antibiotics
• Metronidazole
• Vancomycin
• Fidaxomicin
• Rifaxamin
• Teicoplanin
• Nitazoxanide
Other Therapies
• IVIG
• Monoclonalantibodies
• C. diff toxoid vaccine
• Probiotics
• Fecal MicrobiotaTransplantation(FMT)
Severity Clinical Manifestations Treatment
Asymptomatic carrier
No signs or symptoms No treatment
Mild Mild diarrhea (3‐5/d)AfebrileMild abd pain/tenderness
Stop antibioticsHydration/monitorMetronidazole TID
Moderate Moderate nonbloody diarrheaModerate abd pain/tendernessNausea +/‐ vomiting, dehyrdationWBC >15,000,Elevated BUN/CR
Stop antibiotics. Consider hospitalization. Hydration/monitor.Metronidazole 30 mg/kg/TID OR Vancomycin 40 mg/kg/QID (125 mg) x 14 d
Severe Severe/bloody diarrhea, Tm >38.9Pseudomembranes, ileus, AKI,Severe abd pain/tendernessVomiting, WBC >20,000, Alb <2.5
Hospitalization. Oral or NGVancomycin 500 mg QID +/‐Metronidazole 30 mg/kg/TID ORFidaxomicin 200 mg BID x 10d
Complicated Toxic megacolon, peritonitisRespiratory distress, Hemodynamic instability
Antibx for severe infectionSurgery consultationConsider FMT
CDI Treatment Paradigms
Surawicz et. al. The Am Journal of Gastroenterol. 2013. Leffler and Lamont. NEJM 2015
Zar et al. NEJM 2008;359:1932-40 based on work by Zar, et al. A comparison of vancomycin and metronidazole for the treatment of C. diff- associated diarrhea, stratified by disease severity. Clin Infect Dis 2007; 45:302-7,
Vancomycin: Superior in Severe CDI
81

Fidaxomicin Decreases RCDI
Louis T. et al.. NEJM. 2011.
• Antimicrobial agent(s) should be discontinued
• On-going immunosuppression medicationscan be maintained
• Escalation of therapy in IBD should beavoided during the acute phase
Modifying Therapy in CDI
Surawicz et. al. The Am Journal of Gastroenterol. 2013.
• After initial Tx of CDI, chance of RCDI within 8weeks is 10 – 20 %
• After 1st recurrence, rates of recurrenceincrease to 40 – 65 %
• Recurrence can be due to the same or differentstrain
• RCDI may be due to impaired immuneresponse or alteration of the gut microbiota
Recurrent CDI, A Recurring Problem
Surawicz et. al. The Am Journal of Gastroenterol. 2013.
82

Jiang et al. Am J Gastroenterol. 2006,.
Treatment Failure IncreasesRisk of Recurrence
How is Pediatric RCDI Different?
• C. diff is constitutive flora until after 6 monthsof age, 10 % carriage rate at 1 year
• 10-fold rise in incidence from 1991-2009• Refractory C. diff is rare. Recurrence risk is
about 22-30% as in adults.• Community acquired CDI: more common than
in adults• 23-43% lack antimicrobial exposure history• Up to 38% of previously healthy children with
RCDI have NAP1/B1/027 serotype
Benson L, et al. Infect Control Hosp Epidemiol. 2007;28(11):1233–1235.Khanna S BL, et al. Clin Infect Dis. 2013;56(10):1401‐1406. Janqi S, et al. JPGN. 2010; 51:2‐7.
• 1st recurrence: treat with same regimen
• 2nd recurrence: pulsed or tapered vancomycinor fidaxomicin 200 mg BID x 10 days
• No consensus on optimal pulsed/taperingregimen
**Severe CDI: vancomycin +/- metronidazole and surgery consult
CDI Again?! No Easy Answers
Surawicz et. al. The Am Journal of Gastroenterol. 2013. Leffler and Lamont. NEJM 2015.
83

• If there is a 3rd recurrence, fecal microbiotatransplant (FMT) should be considered1
More than 3 Recurrences: Consider FMT
1. Surawicz et. al. Am Journal of Gastroenterol. 2013.2. Kelly et. al. NEJM. 2008.
• Due to reduced efficacy of otherantimicrobial therapies, FMT holdspromise as effective Tx for RCDI2
• Since 2000, failure rates ofmetronidazole for uncomplicated CDIhave increased from 2.5% to > 18%2
FMT for Recurrent CDI• 1958:
– 4 patients with pseudomembranous colitis1
– Resolution of symptoms in 48 hrs
• 2010:
– First pediatric FMT for recurrent CDI, NAP1/B1/0272
• 2012:
– First colonoscopic FMT for a child with recurrent CDI3
• 2013:
– Randomized controlled trial of FMT (terminated early)4
– FMT is superior to vancomycin +/- bowel lavage
• Present:
– FMT is ~89% effective and safe5
1. Eiseman et al. Surgery 1958 2. Russel G et al. Pediatric 20103. Kahn S et al. Am J Gastro 2012 4. van Nood et al. NEJM 20135. Kassam Z et a. Am J Gastro 2013 http://emedicine.medscape.com/article/186458-overview
Regulatory, Safety, and Ethical Issues in FMT
Clinical• Safety• Risk• Screening of recipients • Stigma the “yuck” factor• Selection of donors• Screening of donors• Privacy• Access• Regulation• Cost and insurance coverage• Stool banks
Research• Safety• Risk• IRB approval• Informing subjects and
donors of results• Invasiveness of sampling• Data sharing• Privacy• Biobanking• Regulation
84

• Surgical consultation should be obtained onall patients with complicated CDI
• Consider surgery:
– hypotension requiring vasopressor therapy
– clinical signs of sepsis and organ dysfunction
– mental status changes; WBC count ≥ 50
– lactate ≥ 5
– complicated CDI with failure to improve onmedical therapy after 5 days
Surgical Consultation
Surawicz et. Al. Am Journal of Gastroenterol. 2013.
Take Home Points
• CDI is on the rise…
both in the hospital and in the community.
• IBD patients are at increased risk for RCDI.
• Recurrent CDI demands tailored treatment.
• Always use antibiotics judiciously!
• Always wash your hands!
– Hand sanitizer isn’t effective against CDI.
Consensus Guidance on Donor ScreeningDonor Selection
• A family member, close contact, or a well screened universal donor.• Donor questionnaire should be similar to AABB donor Questionnaire
Donor Exclusion Criteria
• Antibiotic treatment 3 months preceding donation.• History of GI intrinsic illnesses• Autoimmune, atopic disease, or ongoing immune modulating therapy• Chronic pain syndromes, neurologic, or neurodevelopmental disorders • Metabolic syndrome, obesity (BMI of >30), or moderate‐to‐severe malnutrition• History of malignant illnesses, ongoing oncologic therapySerum Testing (to be performed within 2‐4 weeks of donation)
• Hepatitis A,B, C, syphilis testing, HIV (within 2 weeks)Stool Testing (to be performed within 4 weeks of donation)
• C. Difficile toxin B (PCR), Culture, O+P (if travel history suggests)
85

Gluten sensitivity: Surely a sensitive but perhaps not a gluten subject
Stefano Guandalini, MDProfessor of Pediatrics
October 8, 2015
Disclosure slide
• Consultant for AbbVie• Consultant for ThermoFisher
86

Objectives
• Identify the three clinical disorders currentlythought to be associated with wheat intake
• Realize the lack of evidence for gluten asresponsible of the so‐called «Non‐celiacgluten sensitivity»
• Be able to approach critically and effectively apatient suspect of having «Non‐celiac glutensensitivity»
Wheat - related disorders
Wheat Allergy~0.1%
Celiac Disease1%
Gluten Sensitivity?0.5-1.0?%
No gene associatedIgE‐mediated
Infants and Bakers
HLA‐DQ2, DQ8Autoimmune disease
Any age
No gene associatedLikely Immune‐
mediatedMostly adults
Serum specific IgE
CD autoantibodiesCD autoantibodiesBiopsy
Nodiagnostic marker
87

Gluten (or Wheat) related disorders
Wheat Allergy~0.1%
Celiac Disease1%
Non-celiacGluten Sensitivity
?%
No gene associatedIgE-mediated
Infants and Bakers
HLA-DQ2, DQ8Autoimmune disease
Any age
No gene associatedImmune-mediated?
Mostly adults
Respiratory, skinsymptoms
GI and extra-GIsymptoms
GI and extra-GIsymptoms
Wheat - related disorders
Gluten (or Wheat) related disorders
Wheat Allergy~0.1%
Celiac Disease1%
Non-celiacGluten Sensitivity
?%
No gene associatedIgE-mediated
Infants and Bakers
HLA-DQ2, DQ8Autoimmune disease
Any age
No gene associatedImmune-mediated?
Mostly adults
Serum specific IgE
CD autoantibodiesCD autoantibodiesBiopsy
Nodiagnostic marker
Wheat - related disorders
Gluten (or Wheat) related disorders
Wheat Allergy~0.1%
Celiac Disease1%
Non-celiacGluten Sensitivity
?%
No gene associatedLargely IgE-mediated Children and Bakers
HLA-DQ2, DQ8Autoimmune disease
Any age
No gene associatedImmune-mediated?
Mostly adults
Serum specific IgE
CD autoantibodiesCD autoantibodiesBiopsy
Nodiagnostic marker
Wheat - related disorders
88

An Italian survey on 486 patients:Who suspected it?
Volta U et al., BMC Medicine 2014
Volta U et al., BMC Medicine 2014
An Italian survey on 486 patients:Gastrointestinal symptoms
An Italian survey on 486 patients:Extra‐intestinal symptoms
Volta U et al., BMC Medicine 2014
89

An Italian survey on 486 patients:Anti‐Gliadin Antibodies
Volta U et al., BMC Medicine 2014
A study from Australia Inclusion criteriaAge older than 16 Symptoms of IBS according to Rome III criteria
that improved on a GFD Symptoms well controlled on GFDCeliac disease excluded
Biesekierski JR et al., Gastroenterology 2013
90

Design – RDBPCT (Crossover)
ScreeningScreening Run in / Low FODMAP dietRun in / Low FODMAP diet
High gluten(16g)
High gluten(16g)
WashoutWashout
Low Gluten(2g)
Low Gluten(2g)
WashoutWashout
Placebo(0g)
Placebo(0g)
WashoutWashout
1 Week 2 Weeks 1 Week > 2 Weeks
Gluten free diet
Low FODMAP diet
Shepherd SJ, Am J Gast 2013Gibson PR, Aliment Pharmacol Ther. 2005
FermentableOligosaccharidesDisaccharidesMonosaccharidesAndPolyols
Biesekierski JR et al Gastroenterology 2013
No effect of gluten
Effect of FODMAP withdrawalEffect of FODMAP withdrawal
91

Number of studies so far published on NCGS that utilized pure gluten (not wheat) to challenge:
(Zero)
“Of note, no study on NCGS has specifically used as the re-challenging agent gluten or gliadin” – Molina-Infante J et al., Aliment Pharmacol Ther April 2015
The only study testing the effect of gluten (4.4 g/d) in NCGS
Di Sabatino A. et al., Clin Gastroenterol Hepatol, Epub only
Di Sabatino A. et al., Clin Gastroenterol Hepatol, Epub only
The only study testing the effect of gluten (4.4 g/d) in NCGS
92
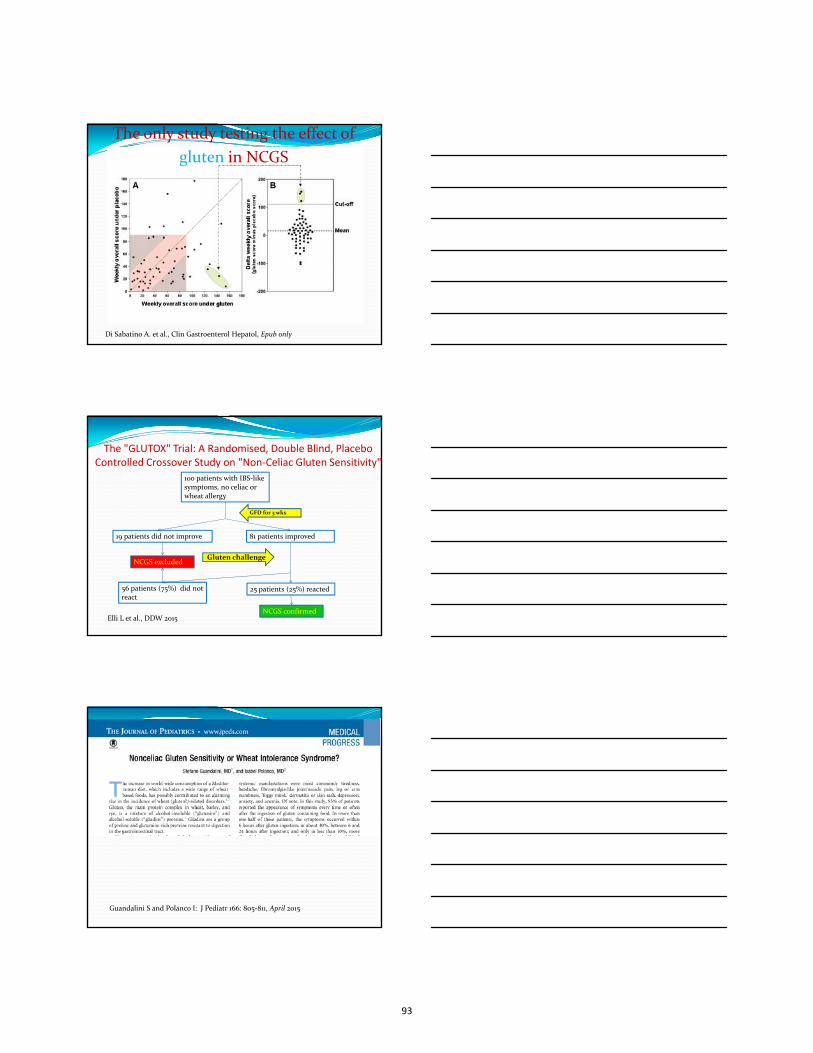
The only study testing the effect of
gluten in NCGS
Di Sabatino A. et al., Clin Gastroenterol Hepatol, Epub only
The "GLUTOX" Trial: A Randomised, Double Blind, PlaceboControlled Crossover Study on "Non‐Celiac Gluten Sensitivity"
Elli L et al., DDW 2015
100 patients with IBS‐like symptoms, no celiac or wheat allergy
81 patients improved 19 patients did not improve
NCGS excluded
56 patients (75%) did not react
25 patients (25%) reacted
GFD for 3 wks
Gluten challenge
NCGS confirmed
Guandalini S and Polanco I: J Pediatr 166: 805‐811, April 2015
93
Guandalini S and Polanco I: J Pediatr 166: 805‐811, 2015
The umbrella of WIS:6 groups of patients!
Gluten sensitive
?
ATISensitive
?
FODMAP
sensitive
Early‐stage celiac
Non IgE‐wheat allergic
Placebo/Nocebo
Not 1 mention of children in the whole paper!
But wait! What about children?
94
• Open‐label (unblinded!)• Challenge with undefined «gluten‐containing
food» (gluten 5g/d)• Challenge for 48 hrs with F/U with diary for 2
weeks• Age range: 1.6‐15.0 years (!)
The only paper in children!
WIS – A Practical ApproachWIS – A Practical Approach
Pt on GFDPt on GFDUnwilling to abandon the GFDWilling to undergo gluten challenge
HLA‐DQ2, DQ8
Positive Negative
No Celiac:Enjoy your GFD!
Enjoy your GFD: But remember you could be celiac
Gluten for ≥6 weeks
Positive
TTG and Biopsy
Celiac
Negative
Symptoms recurred?
Yes No
WIS WIS ruled out
No Celiac
What you have hopefully learned
• Wheat can adversely affect humans by threedifferent entities:– Wheat allergy (0.1‐0.2%)– Celiac disease (1%)– Wheat Intolerance Syndrome (0.6%??)
• WIS is an umbrella term, encompassing:– Placebo/Nocebo– Early Celiac Disease– FODMAP sensitivity.... Etc.
• How to approach a patient suspect of WIS
95

Cureceliacdisease.org
96

Treatment of the Refractory Abdominal Pain Patient
Adrian Miranda, M.D.Associate Professor of Pediatrics
Division of Pediatric Gastroenterology
Medical College of Wisconsin
Children’s Hospital of Wisconsin
-I am a consultant to QOL Medical-No other financial relationships with any commercial entity to disclose
Objectives:
Understand the mechanisms ofabdominal pain
Identifying the patient with refractoryabdominal pain
Know the available and currenttreatment options
97

A brief word about abdominal pain (AP) prevalence
Demographics AP prevalenceMale 43% 29%
Female 57% 36%
Average age (range), years 11.8 (8-15)
Average age of boys 11.7
Average age of girls 11.9
African-American 33% 30%
Latino 22% 32%
Caucasian 21% 33%
Other 16% 35%
Asian 8% 42%
Saps M et al., J Pediatr. 2009
*278 subjects with weekly questionnaires for 1 year
Geographic distribution of functional abdominal pain in children (pooled-prevalence)
Korterink JJ, et al., Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-Analysis. PLoS ONE. 2015.
Proposed Underlying Mechanisms for Chronic Functional Abdominal Pain
Altered HPA-axis
BacterialOvergrowth
Altered ReceptorExpression(5HT, NMDA,TRPV1)
Autonomic Dysfunction
Neuronal Sensitization
Descending Pain Modulation
Carbohydrate Intolerance
MotilityDisorder
98

Stressors Psychological stress
Inflammatory
Sleep
spinewave.co.nz
Where?1. Intestinal microbiome2. Mucosal changes3. Enteric nervous system4. Primary afferents5. Genome6. CNS
Possible associations with psychosocial stress and post-infectious gastrointestinal symptoms
Drossman DA. Gut 1999
Effect of acute psychological stress on small intestinal permeability in humans
Vanuytsel et al, Gut 2014
99

Important fact in post-infections/inflammatory pain?
Not all patients that have stress orgastrointestinal infections develop IBS
Not all animals develop visceralhyperalgesia following “stress”
Post-inflammatory- Animal Model
Zhou et al., Journal of Pain, 2007
-24% of rats maintained hyperalgesia at 4 months
Author Okhuysenet al.
Stermeret al.
Trivedi et al.
Pitzurraet al. Nair et al. Lalani et al.
Year 2004 2006 2011 2011 2014 2014Destinations Mexico Worldwide Egypt or
Turkey Worldwide Mexico Worldwide
Study design Prospective Prospective Retrospecti
ve Prospective Prospective Prospective
Follow-up (months) 6 6 up to 7 6 6 6 6
Number of participants (complete follow-up)
97 405 120 2476 817 515
Male/female (complete study population)
47/50 216/189 89/32 1218/1258 227/590 254/261
IBS occurrence (exposed)
10.0% (6/60)
13.6% (16/118)
17.2% (16/93)
3.1% (26/852)
5.7% (20/348)
2.4% (3/126)
IBS occurrence (non-exposed)
0% (0/37) 2.4% (7/287)
3.7% (1/27)
0.7% (12/1624)
2.6% (12/469)
1.8% (7/389)
Post Infectious IBS
100

Diarrhoea-predominant irritable bowel syndrome: an organic disorder with structural abnormalities in the jejunal epithelial barrierCristina Martínez, Beatriz Lobo, Marc Pigrau, Laura Ramos, Ana Maria González-Castro, Carmen Alonso, Mar Guilarte, Meritxell Guilá, Ines de Torres, Fernando Azpiroz, Javier Santos, María Vicario
Gut. 2013
Pain
Sleep
Autonomic Resoponse
Role of Amygdala A critical component of the anxiety neuro-circuitry
Associated with fear learning
Memory consolidation
vmPFC
Hippocampus
Amygdala
Hypothalamus
PAG
Ressler, et al 2010Cullen, et al 2011Pezawas et al, 2005
Suppresses negative affect by inhibiting amygdala output
Descending pain modulation
101

Amygdala Functional Connectivities
Healthy Control IBS Patient
Subliminal
Liminal
Subliminal
Liminal
VmPFC
VmPFC
Sood et. al., NASPGHAN 2014
Why is There No Algorithm for Treatment?
No data to support decision tree
Phenotype is not well understood
Mechanism of disease and medicationsnot well understood
Very few clinical trials in children
How far Have We Really Come?
1959
8 randomized, controlled trials (4 positive)
55 years
421 children studied
102

Why we can’t believe all clinical trials?
Patient A:15 y/o with 22 month history of chronic abdominal pain
-pain daily, 9/10
-nausea and lightheaded daily, struggles to get out of bed with fatigue
-has missed 28 days of school this year
Patient B:10 y/o with 3 month history of chronic abdominal pain-pain 4 days per week 3/10 on scale-pain only at night-no nausea or fatigue-has not missed school or activities
Targeting therapy is not always easy
Kovacic, et al. J Peds 2014
Responding to Placebo Does Not Make You “Crazy”
©2005 by Society for Neuroscience
Perform distractingtasks activate periaqueductal grey(PAG), Anterior Cingulate Cortex, andorbitofrontal cortex
Placebo activatesendogenous opioidsand induces mildrespiratory depressionand decreasesadrenergic activity
Benedetti F et al., J.Neurosci. 2005Pollo et al., Pain 2003
103

Psychological Therapy Parent Attention Versus Distraction: impact on
symptom complaints by children with and withoutchronic functional abdominal pain.
Walker LS et al., 2006
Cognitive-behavioral therapy for children withfunctional abdominal pain and their parentsdecreases pain and other symptoms.
Levy RL et al., 2010
A randomized controlled trial of a cognitive-behavioral family intervention for pediatricrecurrent abdominal pain.
Robins PM et al., 2005
Hypnotherapy for children with functional abdominal pain or irritable bowel syndrome: a randomized controlled trialVlieger AM, Menko-Frankenhuis C, Wolfkamp SC, Tromp E, Benninga MA
After therapy At 6 mo follow-up At 1 y follow-up
SMT group (n = 25)
HT group (n = 27)
SMT group (n = 24)
HT group (n = 27)
SMT group (n = 24)
HT group (n = 27)
No effect 56% 15% 66% 7% 46% 4%
Improved 32% 26% 17% 22% 29% 11%
Clinical remission 12% 59% 17% 71% 25% 85%
Gastroenterology, 2007
Biofeedback
Changes maladaptive thoughts and pain perception
Patient able to visualize changes in RR, HR and temperature
104

Project to hypothalamus,amygdala, pre-frontalcortex, periaqueductalgrey (PAG) and locuscoeruleus (LC)
Regulate emotional,autonomic andbehavioral responses
C.H. Knowles, Q. Aziz. PAIN. 2009
Gut Vagal Afferents Differentially Modulate Innate Anxiety and Learned FearKlarer M, Arnold M, Günther L, Winter C, Langhans W, Meyer U. J Neurosci. 2014
Efferent activity ismeasured non-invasively via heartrate variability (HRV)
Afferents maymodulate adrenalmedullary factors: epi,norepi, dopamine,endogenous opioids,substance P
Vagal Nerve Afferents Modulate Autonomic Control
Khasar et al. Eur J Neruosci. 2003
Vagal nerve stimulation
Neuro-stimulator (NSS) device veryencouraging results in chronic pain trials
Stimulation of auricular
branch of vagus nerve
Could restore autonomic
function and pain pathways
105

Pharmacological Treatment Options
Pain (with disability)
-TCAs (amitriptyline)
-SSRIs (citalopram)
-Gabapentin
-Antispasmodics (hyoscyamine , dicyclomine)
-Cyproheptadine
-Rifaximin
Constipation
-Linaclotide
-Lubiprostone
Mild Pain (no disability)
-Peppermint oil
-Iberogast
-Melatonin
-Probiotics?
-Acid suppression?
Rehabilitation Program
Education and ReassuranceAntispasmodic- situational pain Loperamide- situational diarrhea
Cyproheptadine (follow weight closely)
MelatoninPeppermint oil
Proton pump inhibitorIberogast
Rifaximin (suspected SIBO)
AmitriptylineAdjust school schedule
( sleep, exercise, fluids)
GabapentinSSRI
Bottom–up Approach for Mild Abdominal Pain
Don’t Forget to Ask the Important Question that will Dictate Therapy?
How many days of school or activities have you missed?
106

Rehabilitation Program
Top-down Approach for Disabled Pain Patient
Education and Reassurance
Rifaximin (bloating, excess gas)
Amitriptyline
Adjust school schedule( sleep, exercise, fluids)
GabapentinSSRI
Cyproheptadine (nausea, pain)
Melatonin (sleep)Proton pump inhibitor (dyspepsia)
Iberogast (nausea, pain, dyspepsia)
Fludrocortisone (orthostatic intolerance)
CoQ10 (fatigue)
Amitriptyline
Bahar RJ et al., J Pediatr. 2008
Study in Children-RCT in adolescents 8 weeks of 10, 20 or 30mg based on weight (n=33)
-Improvement in QOL and pain over placebo
-Negative placebo effect for pain
Mechanism
-Inhibits Na channels, endogenous opioids, NMDA antagonist, anxiolytic.
Dose:0.1-2mg/kg/d at bedtime
Side EffectsConstipation, dry mouth, dizziness, somnolence
IBS, FAP and FD patients were randomizedto 4 weeks of placebo or amitriptyline
Dose: (10 mg/d, <35 kg, 20 mg/d, >35 kg) Pain was assessed daily with self-report
diaries No better than placebo in improving
abdominal pain Reduced anxiety scores (P < 0.0001)
compared to placebo
Saps et al., Gastroenterology. 2009
107

Citalopram Citalopram 12-week open label, flexible dose-trial in
children with RAP Initial dose 10mg and increase to 40 mg if no
response by week 4
Campo JV et al., 2004
Methodological limitation: -not placebo controlled or blinded-small group size (n=25)
CitalopramStudy in Children-RCT of 20mg/day vs. placebo for 4 weeks in children with FAP based on Rome III
Roohafza et al., Neurogastroenterol Motil. 2014
GabapentinNo Data in Children-Increased rectal compliance in adult IBS-D
-Attenuated rectal mechanosensitivity
MechanismBinds alpha 2 delta receptors of Ca channels in CNS (spinal cord, PAG etc.)
Dose:8-35mg/kg/d divided 3x/daily (max 3600mg/d)
Side Effectsdizziness, somnolence, fatigue, ataxia
Lee KJ, Kim JH, Cho SW. Aliment Pharmacol Ther. 2005
108

-10-day course of 550 mg of rifaximin vs. placebo TID
- No difference in symptoms, including pain
-Adult studies show a therapeutic gain over placebo about 9-12%
MechanismAlteration in the quantity, location, or quality of the hosts' intestinal microbiota
Dose:8-35mg/kg/d divided 3x/daily (max 3600mg/d)
Side Effectsdizziness, somnolence, fatigue, ataxia
Double-blind, Placebo-controlled Antibiotic Treatment Study of Small Intestinal Bacterial Overgrowth in Children with Chronic Abdominal PainCollins BS, Lin HC. J Pediatr Gastroenterol Nutr. 2011
Pain assessed at 1 and 2 weeks (n=29)
Improvement (87%) vs. placebo (43%)
Primary outcome measure was the self-reported changeof frequency and duration of abdominal pain
Did not use validated questionnaires
MechanismAntagonist of serotonin, histamine and muscarinic receptors
Improved gastric accommodation through 5HT receptors?
Dose:0.25-0.5mg/kg/d divided 2-3x/daily
Side EffectsWeight gain, somnolence, irritability
Cyproheptadine for the Treatment of Functional Abdominal Pain in Childhood: a double-blinded randomized placebo-controlled trialSadeghian M, Farahmand F, Fallahi GH, Abbasi A. Minerva Pediatr. 2008
Study: Retrospective, open label study of 80 children with dyspepsia
Cohort: GER, post fundoplication, diabetes, mitochondrial dysfunction, post Ladd’s procedure
Safety and Efficacy of Cyproheptadine for Treating Dyspeptic Symptoms in ChildrenRodriguez L, Diaz J, Nurko S. J Pediatr. 2013
109

Complementary and Supplementary Therapy
Approximately 12% of non-clinicalpopulation seeks complementary therapiesfor their children with pain
It is NOT always the answer, but plays animportant role as adjuvant therapy
Placebo in mild pain?
Barnes et al. , 2008
Melatonin
Melatonin Improves Bowel Symptoms in Female Patients with Irritable Bowel Syndrome: a double-blind placebo-controlled studyLu WZ, Gwee KA, Moochhalla S, Ho KY.
Therapeutic effect of melatonin in patients with functional dyspepsia.Klupińska G, Poplawski T, Drzewoski J, Harasiuk A, Reiter RJ, Blasiak J, Chojnacki J
Influence of melatonin on symptoms of irritable bowel syndrome in postmenopausal women.Chojnacki C, Walecka-Kapica E, Lokieć K, Pawłowicz M, Winczyk K, Chojnacki J, Klupińska G.
(STW 5) Iberogast 9 plant extracts: Chamomile flowers, bitter candytuft,
angelica root, caraway fruits, milk thistle, lemon balm leaves, greater celandine, licorice root, and peppermint leaves
Mechanism
Likely anti-hyperalgesic properties, improve proximal gastric accommodation, and may have pro-secretory and anti-spasmodic properties
Dose
10 drops (1 ml) before each meal
Cost: 100ml for $32
Side effects
Abdominal cramps, diarrhea, nausea, dizziness
110
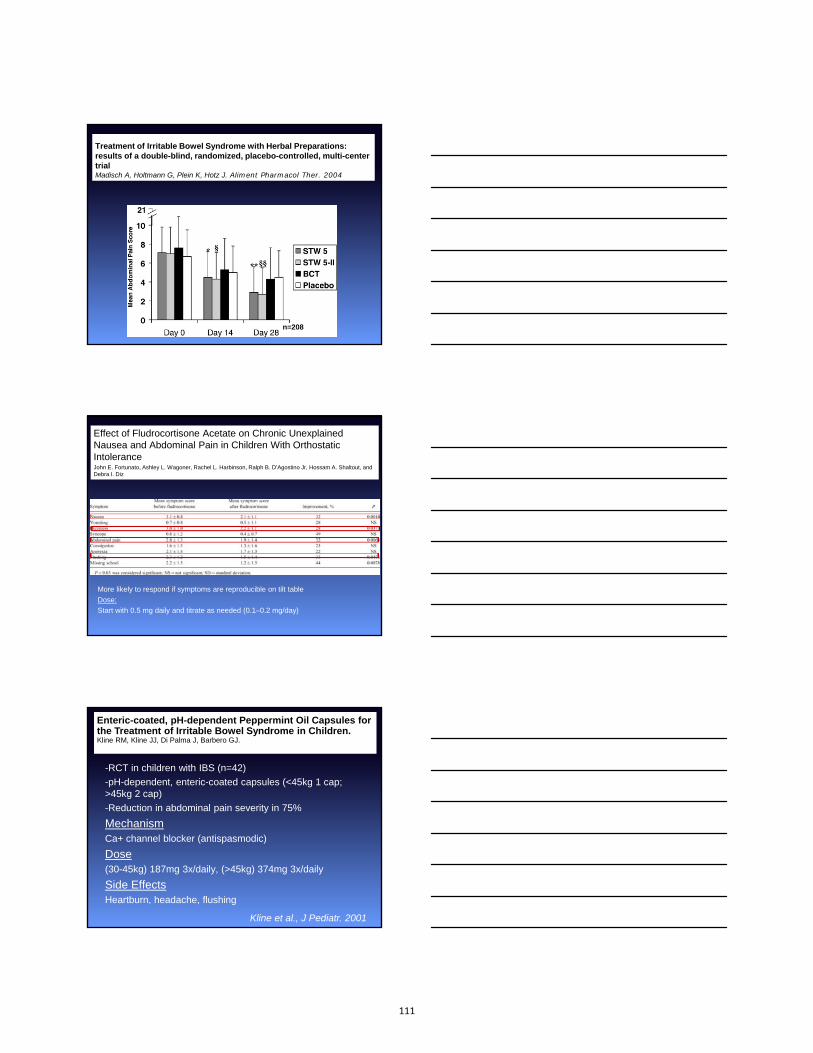
Treatment of Irritable Bowel Syndrome with Herbal Preparations: results of a double-blind, randomized, placebo-controlled, multi-center trialMadisch A, Holtmann G, Plein K, Hotz J. Aliment Pharmacol Ther. 2004
n=208
Effect of Fludrocortisone Acetate on Chronic Unexplained Nausea and Abdominal Pain in Children With Orthostatic IntoleranceJohn E. Fortunato, Ashley L. Wagoner, Rachel L. Harbinson, Ralph B. D’Agostino Jr, Hossam A. Shaltout, and Debra I. Diz
More likely to respond if symptoms are reproducible on tilt table
Dose:
Start with 0.5 mg daily and titrate as needed (0.1–0.2 mg/day)
Peppermint oil
-RCT in children with IBS (n=42)
-pH-dependent, enteric-coated capsules (<45kg 1 cap; >45kg 2 cap)
-Reduction in abdominal pain severity in 75%
MechanismCa+ channel blocker (antispasmodic)
Dose(30-45kg) 187mg 3x/daily, (>45kg) 374mg 3x/daily
Side EffectsHeartburn, headache, flushing
Kline et al., J Pediatr. 2001
Enteric-coated, pH-dependent Peppermint Oil Capsules forthe Treatment of Irritable Bowel Syndrome in Children.Kline RM, Kline JJ, Di Palma J, Barbero GJ.
111

Cause or Effect ?
IBSSleep
Anxiety
Stress
Dysautonomia
Genetics Adverse early life
Microbiome Epigenetics
Adolescent sleep across the last 20 years
Keyes et al., Pediatrics. 2015
Sleep disturbances in clinic patients with functional bowel disorders Fass R, Fullerton S, Tung S, Mayer EA.
Am J Gastroenterol. 2000J Neurogastroenterol Motil. 2014J Korean Med Sci. 2013Am J Gastroenterol. 2010
Psychosocial stress in nurses with shift work schedule is associated with functional gastrointestinal disordersKoh SJ, Kim M, Oh da Y, Kim BG, Lee KL, Kim JW.
Impact of shiftwork on irritable bowel syndrome and functional dyspepsiaKim HI, Jung SA, Choi JY, Kim SE, Jung HK, Shim KN, Yoo K
The impact of rotating shift work on the prevalence of irritable bowel syndrome in nursesNojkov B, Rubenstein JH, Chey WD, Hoogerwerf WA.
112
Role of Exercise in Pain ControlRat model: Exercise increased β-endorphin and met-
enkephalin in rostral ventral medulla (RVM) and periaqueductal grey (PAG)
Ameliorated thermal and tactile hypersensitivity
Prospective, randomized, controlled, open-labelstudy of 12 weeks (n=102)
20–60 min of moderate-to-vigorous intensivephysical activity 3 to 5 days per week
IBS scores, physical functioning, emotion, sleep,energy, and social role were significantly improved
Stagg, NJ et al. Anesthesiology 2011
Johannesson et al., Am J Gastroenterol 2011
Adult IBS
Conclusions Careful evaluation should include
assessment of decreased functioning in orderto target therapy
Combination therapy is necessary in thesevere, disabled patients
Psychological therapy is key in almost ALLpatients
We must take advantage of the placeboeffect in the less severe patients andencourage healthy lifestyles (sleep andexercise)
113

NAUSEA: UPDATES THAT WON’T MAKE YOU SICK
Carlo Di Lorenzo, M.D.
Twitter: @carlodilorenzo1
I have no financial relationships relevant to this presentation to
disclose
ImportanceImportance
Common reason for referral
Co-exists with other FGIDs
Highly distressing
Sparse literature
No objective measurement tools
No diagnostic algorithms
Ineffective treatments
Common reason for referral
Co-exists with other FGIDs
Highly distressing
Sparse literature
No objective measurement tools
No diagnostic algorithms
Ineffective treatments
114

CaseCase
15 year old adolescent girl
4 mo hx of waking up everymorning with nausea
Improves throughout the day
Worse on school days when shehas to wake up earlier
Rarely vomits, no weight loss
CaseCase
ROS positive for migraines anddizziness
Normal growth and development
Normal PE
Neg HCG, “routine” labs, UA, toxscreen, abdominal US
Have you seen this before?
115

J Pediatr Gastroenterol Nutr 2013;57:311-5
Disability was related to higher nausea:Full school days missed and unable to do home activities
significantly correlated with nausea frequency
Disability was related to higher nausea:Full school days missed and unable to do home activities
significantly correlated with nausea frequency
Percentages
Nausea in pediatric FGID
Associated symptoms
Kovacic K, et al, JPGN 2013;57:311-5.
Is functional nausea a pediatric functional GI disorder?
It will be in Rome IV!
116

Early morning nausea
Morning nausea in adolescents isalmost always a manifestation of ananxiety disorder
Cortisol levels peak in the earlymorning hours (usually around 8AM)
Cortisol is also released as aresponse to stress and is a mediatorof anxiety
Share this FACT with the parents andpatient
If you look for what is causing the nausea….
You may find this
117
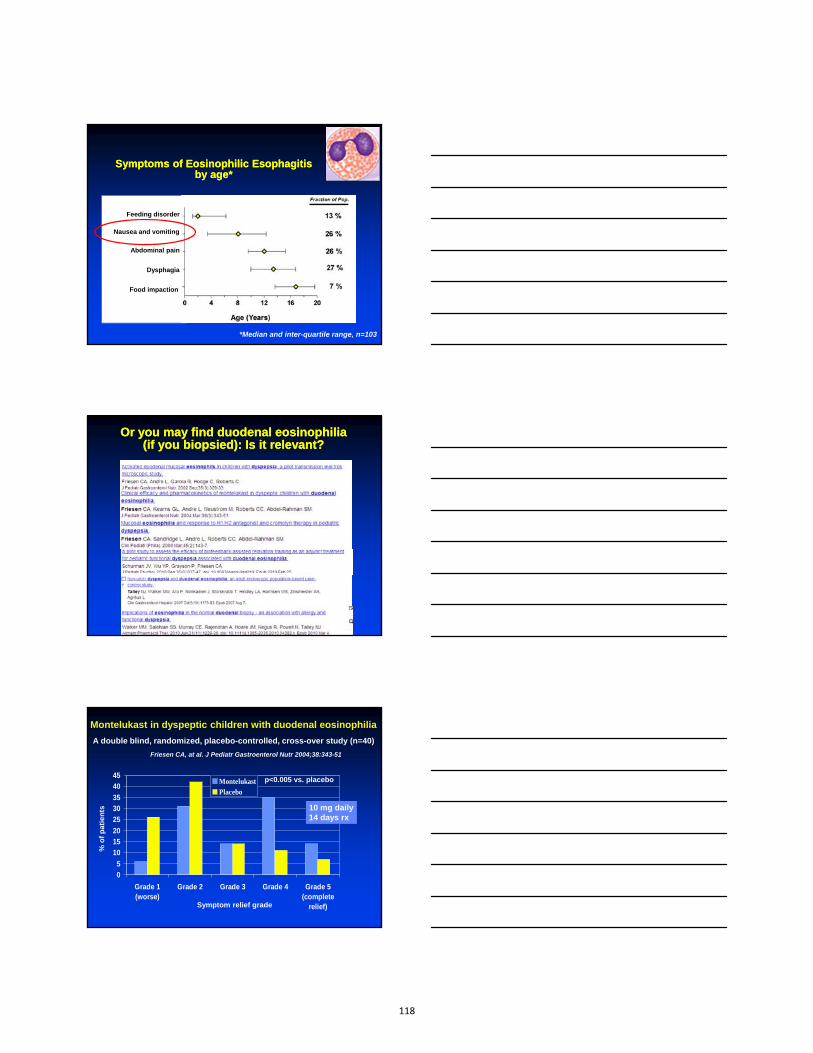
Symptoms of Eosinophilic Esophagitis by age*
Symptoms of Eosinophilic Esophagitis by age*
*Median and inter-quartile range, n=103
Feeding disorder
Nausea and vomiting
Abdominal pain
Dysphagia
Food impaction
Or you may find duodenal eosinophilia (if you biopsied): Is it relevant?
Or you may find duodenal eosinophilia (if you biopsied): Is it relevant?
Friesen CA, at al. J Pediatr Gastroenterol Nutr 2004;38:343-51
0
5
10
15
20
25
30
35
40
45
Grade 1(worse)
Grade 2 Grade 3 Grade 4 Grade 5(complete
relief)
MontelukastPlacebo
% o
f p
atie
nts
Symptom relief grade
p<0.005 vs. placebo
Montelukast in dyspeptic children with duodenal eosinophilia
A double blind, randomized, placebo-controlled, cross-over study (n=40)
10 mg daily14 days rx
118

More tests?
Nuclear Medicine
Pediatric normal values?Pediatric normal values?
Depends upon the meal Use adult data for a solid meal (2
large eggs, 2 slides of bread, jam,water, 345 KCal):Abnormal >10% left in the stomachafter 4 hours, >60% after 2 hours
No pediatric data available, butlook for extremes
Depends upon the meal Use adult data for a solid meal (2
large eggs, 2 slides of bread, jam,water, 345 KCal):Abnormal >10% left in the stomachafter 4 hours, >60% after 2 hours
No pediatric data available, butlook for extremes
Abell TL et al. J Nucl Med Technol. 2008;36:44-54
119

(JPGN 2013;56: 439–442)
• 71 patients (32 boys, average age 10.8 yr)• 62% children had abnormal GES; 23% who
had normal values at 2 h had abnormal GESat 4 h (p<0.0001)
• Survey: Only 5 of the top 20 pediatric GIcenters in the US conducted 4-h GES
• Conclusions: Extending GES to 4 h resultedin a considerable increase in diagnosis ofgastroparesis
SmartPill pH.p Capsule
• 26mm x 13mm
• 5+ day battery life
• Senses and records pH, pressure
and temperature data from
within the GI tract
• Wirelessly transmits data to the SmartPill Data Receiver
pH SENSOR
PRESSURE SENSOR
BATTERIES
TRANSMITTER
MICROPROCESSOR
120
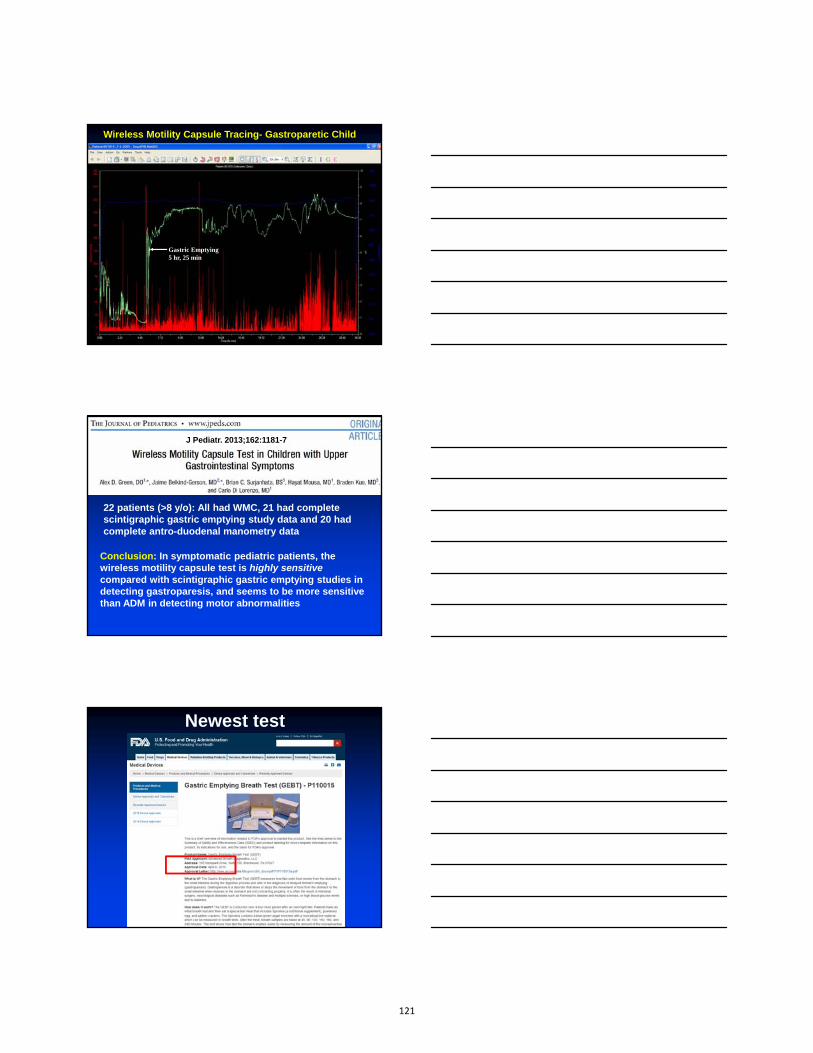
Gastric Emptying 5 hr, 25 min
Wireless Motility Capsule Tracing- Gastroparetic Child
Conclusion: In symptomatic pediatric patients, the wireless motility capsule test is highly sensitive compared with scintigraphic gastric emptying studies in detecting gastroparesis, and seems to be more sensitive than ADM in detecting motor abnormalities
22 patients (>8 y/o): All had WMC, 21 had complete scintigraphic gastric emptying study data and 20 had complete antro-duodenal manometry data
J Pediatr. 2013;162:1181-7
Newest test
121

Treatment
Try everything!
Old but good…
Cyproheptadine
First generation anti-histamine with additional anticholinergic, antiserotonergic, and local
anesthetic properties
122

J Pediatr 2013 (in press)
80 children (mean age 10 y)
17 pts with chronic idiopathic nausea, with orthostatic intolerance by abnormal tilt table tests (88%) or gastric dysrhythmias (71%)
Fludrocortisone: 0.1-0.2 mg/day for 4 weeks
IberogastIberogast
Iberogast is comprised of the following 9 ingredients: Iberis amara, Angelica, Chamomile, Caraway Fruit, St. Mary’s Thistle, Balm Leaves, Peppermint Leaves, Celandine, and Liquorice Root.
123

Gastrointestinal Symptom score during 8 wk of treatment with STW 5 (Iberogast) or placebo
von Arnim U, et al. Am J Gastroenterol. 2007;102:1268-75
Iberogast in Functional Dyspepsia
Iberogast in Functional Dyspepsia
Hypnotherapy for nausea?Hypnotherapy for nausea?
In five of these studies the participants were children. Studies report positive results including statistically significant reductions in anticipatory and CINV. Meta-analysis revealed a large effect size of hypnotic treatment when compared with treatment as usual, and the effect was at least as large as that of cognitive–behavioural therapy
Acupuncture for nausea?Acupuncture for nausea?
124

Authors’ conclusions: P6 acupoint stimulation prevented PONV. There was no reliable evidence for differences in risks of postoperative nausea
or vomiting after P6 acupoint stimulation compared to antiemetic drugs
The ReliefBandThe ReliefBand
Botulinum Toxin: 100-200 Units divided in 4 quadrants
125

Gastrointest Endosc. 2012 Feb;75:302-9
Gastric Electrical Stimulation (GES):The nausea Holy Grail in pediatrics?
126
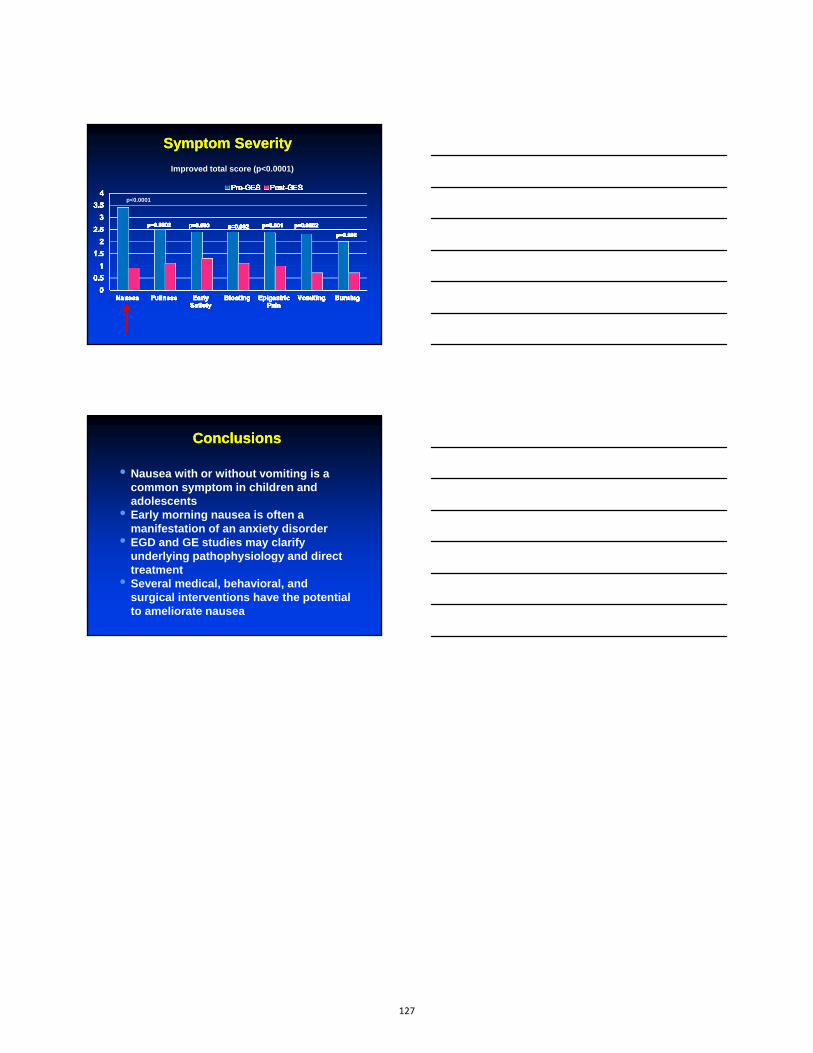
Symptom Severity Symptom Severity
Improved total score (p<0.0001)
p<0.0001
ConclusionsConclusions
• Nausea with or without vomiting is acommon symptom in children andadolescents
• Early morning nausea is often amanifestation of an anxiety disorder
• EGD and GE studies may clarifyunderlying pathophysiology and directtreatment
• Several medical, behavioral, andsurgical interventions have the potentialto ameliorate nausea
127
1
Pediatrics
New Horizons in Hepatitis CNASPGHAN Postgraduate Course
Washington, DC
Daniel H. Leung, MDBaylor College of MedicineTexas Children’s Liver Center
•Research support as Principal Investigator for clinical trials sponsored by Gilead, Merck, BMS, Roche, and Vertex.
•Served on medical advisory board for Gilead.
•Brand names will be referenced for the purposes of identification and learning of future studies.
Disclosures
•Understand the epidemiology, burden of disease, and natural history of HCV
•Become familiar with indications to treat and upcoming all-oral treatment regimens
•Appreciate the rapidity and approach of HCV drug development
Objectives
128

2
•Hepatitis C (HCV) is an RNA virus that affects ~200 million worldwide. 3 million in US. #1 cause of HCC in US
•Vertical transmission (5-7%) is the most common route in infants and children with approximately 7,500 new cases/year in the US.
•There are an estimated 23,000-46,000 children with chronic HCV (CHC) infection in the US and 6,600 in Canada.
Hepatitis C: Burden of disease
Alter MJ et al. Ann Intern Med 2006.Jhaveri R. et al. J Pediatr 2006.El Saadany S. et al. Can J Gastroenterol 2000.
Histology of chronic pediatric HCV
Goodman ZD, Makhlouf HR, Liu L, et al. Pathology of chronic hepatitis C in children: liver biopsy findings in the Peds‐C Trial. Hepatology 2008; 47: 836–43
Maternal transmission
5‐7%
Maternal transmission
5‐7%
Most clinically well
Most clinically well
15% with mild symptoms
15% with mild symptoms
1‐2% develop cirrhosis
1‐2% develop cirrhosis
HCC5 reports
HCC5 reports
Spontaneous resolution <2 yrs
25‐40%
Spontaneous resolution <2 yrs
25‐40%
Persistent CHC 48‐69%
Persistent CHC 48‐69%
Children/Adolescents
Develop CHC but clear at <7 yrs
6‐12%
Develop CHC but clear at <7 yrs
6‐12%
Natural History
129

3
Mean Ishak (0‐6) 1.6 ± 1.3‐Children < 15 yr 1.5 ± 1.3
‐Children > 15 yr 2.3 ± 1.2
Multi-Center European Study 1980-1998“Mild but Progressive”
+HCV RNAN=224
87% asymptomatic
48% ALT< 2x ULN
6% viral clearance and ALT normalization
79% Genotype 1
17% Genotype 2/3
Liver bxn=92
Jara et al. Clinical Infect Dis. 2003
200 followed for mean of 6.2 ± 4.7 yrs
Cirrhosis 1 (1%)
Overweight children in US with HCV at risk for increased fibrosis
•Peds-C Trial (U.S.)
•N=121
• 4.2 % bridging fibrosis
• 1.7 % cirrhosis
• 44% steatosis (minimal
in 34%, mild in 10%)
• Steatosis correlated with serum ALT and BMI z-scores
Goodman ZD, Makhlouf HR, Liu L, et al. Hepatology 2008.
IshakScore
BMI‐Z<1.64 (n=92)
BMI‐Z>1.64(n=29)
0 16% 7%1 46% 45%2 36% 31%3 2% 11%
4 ‐ ‐
5 ‐ 3%
6 ‐ 3%
Obesity and impact on Treatment in US children
Delgado‐Borrego et al. JPGN 2010
Obesity MAY
• Decreases IFN bioavailability
• Alter cytokine function
• Increase insulin resistance
1 unit in BMI z‐score = ‐12% response rate
130

4
•Recent observations in adults with CHC indicate that hepatocellular carcinoma may develop in the absence of cirrhosis
•Children with early stage, treatment-naive HCV demonstrated cognitive impairment with memory most affected
Why worry?
Lok AS et al. Gastroenterology 2009. Madhoun MF et al. Am J Med Sci 2010. Faddan et al. Journal of Viral Hepatitis 2014.
•-Recommended age:>18 months due to maternal antibody (NASPGHAN 1B; AIII)
•-HCV antibody: specificity and sensitivity of the third generation EIAs are >98% and >97% respectively
•-HCV RNA quantitative PCR reserved for confirmation (NASPGHAN 2B; BIII)-maternal anxiety
Screening/Monitoring Infants <3 yrs
Mack, CL et al. J Pediatr Gastroenterol Nutr. 2012.
•Annual evaluation in children with HCV not on antiviral therapy
‐Ongoing education and physical exams
‐Laboratory investigations (NASPGHAN 2A; BII):
•Serum aminotransferases
•Bilirubin (total/direct or conjugated)
•Albumin
•HCV RNA quant
•CBC
•PT/INR
Monitoring in Children
Mack, CL et al. J Pediatr Gastroenterol Nutr. 2012 .
131

5
•In children with significant liver disease (hepatic fibrosis or cirrhosis):
Abdominal ultrasonographyAND
Serum alpha-fetoprotein
should be considered ANNUALLY to screen for HCC (NASPGHAN 2B; BII*).
Monitoring in Children
Mack, CL et al. J Pediatr Gastroenterol Nutr. 2012.
Role of HCV genotyping
•Predictor of RESPONSE and OPTIMAL DURATION
•Genotype 1:<40%*
•Genotype 2 or 3: >80% chance of cure
•This has changed with advent of new therapies
Wirth, World Journal of Pediatric Gastroenterology, 2012
*
Liver biopsy may be considered if the result will influence medical decision-making.
‐To investigate clinical hepatic decompensation
‐To assess severity of liver disease for antiviral candidacy
‐May forego pre-treatment liver biopsy in children with HCV genotypes 2 or 3 who have a high (>80%) probability of achieving a virologic cure (NASPGHAN 2B; BII recommendation).
Role of liver biopsy
Mack, CL et al. J Pediatr Gastroenterol Nutr. 2012.
132

6
Pegylated Interferon + Ribavirin
‐Two U.S. licensed pegylated interferons
•Peginterferon alfa-2b (Peg-Intron®)
•Peginterferon alfa-2a (Pegasys®)
•Ribavirin: (Rebetol®, Ribasphere®)
How effective is current therapy?
Wirth, World Journal of Pediatric Gastroenterology, 2012
•5 largest pediatric prospective clinical trials
•Overall SVR is 60%
•51% in G1
•93% in G2/3
To treat or not to treat?
Treat Wait
High response rate (Genotypes 2 or 3)
Chance for spontaneous clearance
Improved tolerability in children Psychiatric disorder
Lower viral load Morbid obesityParental oversight Low response rate
(Genotype 1)
Family history of HCC or cirrhosis
Puberty
Reduce social burden More advanced therapies ahead
133

7
‐Children with genotype 1/4 can be treated with peginterferon alfa-2a + ribavirin for 48 weeks
‐Children with genotypes 2 and 3 can be treated with peginterferon alfa-2 + ribavirin for 24 weeks
‐Insufficient/no data to support benefit vs risk in increasing duration and dose of treatment
Duration of Treatment
Hadziyannis SJ et al. Ann Intern Med 2004.Zeuzem S, et al. J Hepatol 2006.Dalgard O et al., Gut, 2007.
Treatment Endpoints
Each outcome has prognostic significance. RVR is the strongest predictor of SVR (gold standard for cure)
U.S. Department of Veterans Affairs ‐ 810 Vermont Avenue, NW ‐ Washington, DC 20420
HCV Life Cycle: Understanding the Future
Dan
134

8
•HCV encodes one single polyprotein that is cleaved into 10 structural and non-structural proteins by viral enzymes
•Direct Acting Antivirals (DAA) are designed to inhibit viral proteins involved in the HCV life cycle. The complexity of the viral machinery allows for numerous potential targets.
Future Therapeutics: A new era
Personalized HCV Therapy
Nature Publishing Group, 2005
•Discovery of first two DAA against the NS3/4A serine protease for use in genotype 1 HCV
• Ketoamide inhibitors, boceprevir and telaprevirwere approved in 2011
HCV Structure: Understanding the Future
135

9
Sofosbuvir
Nucleos(t)ide Polymerase inhibitors
Ledipasvir
Protease inhibitors
Translation/Processing
Dasabuvir
Welsch, C. Et al. Gut 2012;61(Suppl 1):i36ei46. doi:10.1136/gutjnl‐2012‐302144
Non‐Nucleoside Polymerase inhibitors
What’s the big deal?
•HCV superseded HIV cause of death in US since 2007
•89 investigational medications studied between 1998-2014 to treat HCV
•Growing pipeline of potent direct antivirals for HCV currently totals 75 in the US alone!
Pharmaceutical Research and Manufacturers of America. 2015 biopharmaceutical research industry profile. Washington, DC: PhRMA; April 2015
SOFOSBUVIR (NS5B): THE NEW “BACKBONE” OF HCV THERAPY ?
• Approved in December 2013
• 1st in combo with PEG-IFN +ribavirin, >85% SVR in 12 wks
• 2nd with ribavirin, the first interferon-sparing treatment regimen for G2 (12 wks) or G3 (24 wks) with >95%
Lancet Infect Disease 2013 May;13(5):401‐8
136

10
Telaprevir (Incivek®) and Boceprevir (Victrelis®), May 2011
Sofosbuvir (Sovaldi®), Dec 2013
Ledipasvir (Harvoni®), Oct 2014
Simeprevir (Olysio®), Nov 2014
Ombitasvir, paritaprevir, ritonavir +dasabuvir (Viekira pak®), Dec 2014
Timeline of recently FDA approved HCV drugs
Scientific mix & match
• + Ledipasvir (NS5A) >90% for G1 in 12 weeks,October 2014
• + Simeprevir (NS3/4A) : 93% in 12 wks G1, 97%in 24 weeks, November 2014
• + Daclatasvir (NS5A) 98% for G1 in 12 weeks (NoFDA)
•Viekira Pak (ombitasvir (NS5A), paritaprevir (NS3-4A) and ritonavir tablets co-packaged with dasabuvir tablets (NS5B)
•95% for G1 and G4 in 12 weeks
•Grazoprevir (NS3/4A)/Elbasvir (NS5A) for G1/4 and those with endstage renal disease on dialysis
•Daclatasvir (NS5A) + Asunaprevir (NS3) (FDA app withdrawn)
Non-Sofosbuvir combinations
137

11
•G3, not G1 is now the most difficult to treat with new DAA’s with higher relapse rates after 12 weeks of treatment.
•G3 patients are more responsive to pegylatedinterferon, but require 24 weeks of Sofosbuvir instead of 12 (G1)
•This same trend has been demonstrated with other DAA combinations
A genotypic paradigm shift
•Treat the child with >75% chance of responding to PEG-IFN (G2 and G3). Really?
•For mild inflammation and fibrosis, wait for all-oral DAA drugs or consider trials
•Offer children with aggressive inflammation and fibrosis on liver biopsy entry into pediatric DAA trials
Empiric approach to pediatric HCV
•HCV progression is mild in children but not without risk
•Fibrosis and poor response associated with obesity
•Peg IFN+RBV is the current standard of care. Genotype will predict response and duration of treatment differently.
• Future: Single pill, 12 weeks, no SE’s, >90% cure
Summary
138

Renal Complications of Chronic Liver Disease
NASPGHAN Post-Graduate Course 2015
Jean Pappas Molleston, M.D.
Professor of Clinical Pediatrics
Indiana University School of Medicine
Disclosures
• I have research funding from Lumena, Vertex,Gillead, Abbvie
• I have research funding from the CFFoundation
• I have received funding from Vindico for amedical education presentation
Objectives:
• Define renal complications in chronic liverdisease
• Review mechanisms of ascites, role of thekidney, and diuretic use
• Understand fluid balance in cirrhosis
• Review definition of Hepatorenal Syndrome(HRS) and treatment recommendations
139

Physiology of Portal Hypertension
• Peripheral and splanchnic vasodilation withincreased cardiac output
• Increased resistance to portal vein inflow dueto cirrhosis
• Increased portal vein pressure• Consequences: *renal dysfunction
*ascitesvariceal bleedinghypersplenism
Fagundes AJKD 2012
Kidney in Portal HTN/Cirrhosis
• Systemic arterial vasodilation
• Decreased effective arterial blood volume
• Renal vasoconstriction
• Possible role of inflammatory response
• Possible role of angiogenic factors
• Renal sodium and water retention
140

Ascites: Physiology
• Vasodilation and effective hypovolemia resultin stimulation of the renin-angiotensin,aldosterone system; salt and water are retained
• Portal hypertension increaseshydrostatic pressure insplanchnic circulation,exceeding capacityof lymphatics
• Low albumin decreasescolloid oncotic pressure,allowing fluidto leak into interstitium
Giefer JPGN 2011
Management of Ascites in Cirrhosis
• Mild sodium restriction• Diuretics
– Spironolactone: inhibits aldosterone (acts distally) 2-3mg/kg/d
– Furosemide: loop diuretic 1-2mg/kg/d
• Albumin infusion 1g/kgof 25% albumin
• Paracentesis +/- albumin• TIPS
Giefer JPGN 2011
Hyponatremia in Cirrhosis
Cirrhosis/portal hypertension
Splanchnic/systemic vasodilation
Decreased effective arterial blood volume
Activation of neurohumoral systems
Renal tubule/water retention
Dilutional hyponatremiaAdapted from MohantyGastroenterol Hepatol 2015
141

Consequences of Hyponatremiain Cirrhosis
• Higher mortality
• More encephalopathy
• Associated with ascites, HRS
• Associated with impaired QOL
Mohanty Gastroenterol Hepatol 2015
Hyponatremia in Cirrhosis: Treatment
Cirrhosis/portal hypertension
Splanchnic/systemic vasodilation
Activation of neurohumoral systems:
Renal tubule/water retention
Dilutional hyponatremia Adapted from MohantyGastroenterol Hepatol 2015
Water restriction?Vaptans?
Albumin infusionsHold diuretics
Transplant
Decreased effective arterial blood volume
Causes of Renal Dysfunction in Cirrhosis
• Intra-renal 29% (glomerulonephritis, interstitialnephritis)
• Pre-renal 70%– 66% respond to volume expansion– 34% do not respond to volume HRS
• Precipitating factors:– Infection, esp. spontaneous bacterial peritonitis– GI bleeding– Excessive diuresis– Diarrhea (lactulose)– Drugs (including antibiotics, NSAIDS)
Charlton Liver Transplant 2009
142

Consequences of Renal Dysfunction in Cirrhosis
• Ascites
• Hyponatremia
• Hepatorenal syndrome– Type 1: acute renal failure
– Type 2: chronicrenal failure
Fagundes AJKD 2012
Hepatorenal Syndrome: Clinical Characteristics
• Diagnostic criteria:– Cirrhosis with ascites– Elevated creatinine (Cr)– No improvement of Cr after withdrawal of
diuretics for 2 days and albumin infusions toexpand plasma volume
– No shock, no nephrotoxic drugs– No parenchymal kidney disease (proteinuria,
hematuria, abnormal u/s)
Fagundes AJKD 2‐12, Wong Nat Rev: Gastro/Hep 2012
Treatment of Hepatorenal Syndrome
• Recognize/prevent/treat precipitating factors• Try 1g/kg albumin IV up to 100g in adults• Vasoconstrictor therapy:
– Terlipressin* plus albumin (34-43% resolution of HRS in RCT)
– Midodrine plus octreotide/albumin (30% effective, uncontrolled studies; compared to terlipressin/albumin 29% vs 70%)
– Norepinephrine plus albumin ? equivalent to terlipressin (RCT)
*terlipressin not available in US Reviewed in Wong Nat Rev Gast 2012; GluudCochrane 2012; Cavallin Hepatol 2015
143

Medical Management of
HRS with Vasoconstrictors
Wong Nat Rev Gastr/Hep 2012
Hepatorenal Syndrome and Renal Replacement Therapy (RRT)
• Decision for RRT depends on fluid balance,metabolic derangements (K+, acidosis), andlevel of renal dysfunction
• CVVHD is preferred to intermittenthemodialysis to minimize hemodynamicinstability
• There are issues like choice of anticoagulant(role of citrate?)
Long Term Outcomes of Children with HRS Receiving RRT then
Liver Transplant
Received RRT (8) Matched controls, no RRT (24)
P Value
Survival 5/8 (63%) 24/24 (100%) 0.01
GFR/years of follow‐up 97 (60‐122)/3.2yrs 114 (65‐236)/4.9yrs NS
Need for f/u antihypertensives 1/5 (20%) 2/22 (9%) NS
Adapted from Parsons Liver Transplant 2014
144

Hepatorenal Syndrome and TIPS• Adult studies in type I and II hepatorenal syndrome
HRS indicate improvement in renal function after TIPS placement
• Use of TIPS in decompensated cirrhosis isproblematic: can result in encephalopathy or even liver failure; bili>3-5 considered contraindication
Rossle Gut 2010
Effects of a Transjugular Intrahepatic Portosystemic Shunt (TIPS) on Urinary Sodium
Excretion and Creatinine concentration.
. Rossle Gut 2010
Hepatorenal Syndrome and Transplantation
• HRS resolves in 76% of adults in 13 days• 6% increase in chance of not resolving per pre-
transplant dialysis day• Guidelines recommend isolated liver transplant
if duration of RRT is less than 6-12 weeks• Combined liver kidney transplant if duration of
RRT is >8 wks– 3 year patient, kidney and liver survival all >65%– Not always better than isolated liver tx
Wong Liver Transplant 2015Davis Liver Transplant 2005Locke Transplantation 2008
145

Impact of the Etiology of Acute Kidney Injury on Outcomes Following Transplantation: Acute Tubular
Necrosis Versus Hepatorenal Syndrome Liver
Nadim Liver Transpl 2012
Summary
• Peripheral/splanchnic vasodilation, decreasedeffective blood volume and renalvasoconstriction lead to renal complications ofcirrhosis: ascites, hyponatremia, HRS
• Treatment of these complications revolves onunderstanding the kidney’s role in Na and H20balance in cirrhosis
• There are some encouraging data regardingvasoconstrictor + albumin therapy for HRS inadults; pediatric research is needed!
Take Home Messages
• Carefully monitor renal status in cirrhosis
• Avoid over-diuresis & nephrotoxic drugs andtreat infection early to avoid precipitating HRS
• Try providing colloid when HRS is suspected
• Consider adding vasoconstrictor therapy inHRS (need pediatric data)
• HRS often reverses after liver transplant
146

Wilson Disease – an update
Simon Horslen MB ChB FRCPCHDirector Hepatobiliary ProgramMedical Director Liver & Intestine TransplantationSeattle Children's Hospital
Professor Department of PediatricsUniversity of Washington School of Medicine
Disclosure
In the past 12 months, I have had no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or providers(s) of commercial services discussed in this CME activity
I do not intend to discuss an unapproved or investigative use of a commercial product or device in my presentation
Learning Objectives
1. Review the clinical presentations in pediatric populationand typical diagnostic evaluation.
2. Understand genetics and patterns of inheritance tofocus who should be screened.
3. Understand treatment strategies and side effects ofcurrent and future therapies
147

Content
• History
• Presentation of Wilson disease
• Physiology of copper
• Genetics of Wilson disease
• Diagnosis
• Prognosis
• Treatment & Monitoring
• Future directions
Samuel Alexander Kinnier Wilson
• Progressive degeneration of lenticular nuclei associated with hepatic cirrhosis was recognized as a distinct clinical entity in 1912
• John Nathaniel Cumings made the link with copper accumulation in both the liver and the brain in 1948
• Derek Denny-Brown first reported effective treatment with metal chelatorBritish anti-Lewisite in 1951
• Penicillamine, first effective oral agent,was introduced in 1956 by John Walshe.
• Gene locus chromosome 13q 1985
• Gene cloned – P-type ATPase 1993
History
Phenotypic Presentation of Wilson Disease
Hepatic presentationsH1: Acute hepatic Wilson diseaseH2: Chronic hepatic Wilson disease
Neurologic PresentationsN1: Associated with symptomatic liver disease N2: Not associated with symptomatic liver diseaseNX: presence or absence of liver disease not investigated
Other (O)
148

Classic Pediatric Presentation
• 7-16 year old child• Previously healthy• 2 weeks malaise and increasing jaundice• Coomb’s negative hemolytic anemia• Modest elevation of transaminases• Low alkaline phosphatase• Prolonged prothrombin time• Low ceruloplasmin level• High urinary copper excretion
Copper kinetics and metabolism
• Regular diet averages 5 mg/d
• Exchange ~ 2mg a day (net absorption ≈ net losses)
• Total body copper ~100 mg (Liver 20%, Blood 10% Other tissues70%)
• Liver rapidly clears newly absorbed copper
• Ceruloplasmin made by hepatocytes, each molecule contains 6 copper atoms incorporated during biosynthesis
• Failure to incorporate copper either because of dietary deficiency or Wilson disease leads to a reduced serum ceruloplasmin level
Copper kinetics
Hours after oral 65Cu dose
% e
nric
hmen
t
0
5
10
15
0 20 40 60 80
Stable isotope enrichment studies (65Cu) showing normal range and a patient with Wilson disease (blue line)
149

From: Disorders of Copper Transport: The Online Metabolic and Molecular Bases of Inherited Disease, 2014Date of download: 6/22/2015 Copyright © 2015 McGraw-Hill Education. All rights reserved
Copper metabolism in the hepatocyte
Ceruloplasmin
ER
Trans-Golgi Network
Bile canaliculus
Hepatic Sinusoid
To Plasma(secretion)
cytochromeoxidase
HAH1Wilson ATPase
Ccs
Cu/Zn superoxidedismutase
Cox17
IL-6TNF
Ctr1Cu-histidineCu-albumin
metallothionein
Molecular biology of Wilson disease
• ATP7B Chromosome 13q14.3
• 21 exons, 60 kb
• >500 mutations described
• H1069Q most common in Europeans 35-40%
• A778L up to 30% of Asian populations
• Genotype- phenotype correlation notstrong
• Genetic modifiers – MTHFR,COMMD1, ATOX1, XIAP
• Environmental modifiers - dietCopper-binding domain
ATP-binding domain
Diagnostic Tests
• KF rings
• Ceruloplasmin
• Serum copper
• Urinary copper
• Liver biopsy
• Molecular genetics
150

Kayser-Fleischer Rings
• Occur in 90-95% of WD patients with a neurological presentation
• But only 40-65% in hepatic presentations
• Slit-lamp examination often necessary
• Can occur in other forms of copper toxicosis and chronic cholestatic syndromes (pseudo-rings)
Ceruloplasmin
• Typically low (<20 mg/dL) in WD
• Levels may be normal in 20-50% at presentation
• Acute-phase reactant
• May be low in copper deficiency, chronic liver disease, nephroticsyndrome and protein-losing enteropathy
Serum Copper
• Circulating copper may be:• Low - because the
ceruloplasmin level is low
• High –liver necrosis releases ‘free’ copper
• Normal – a normal level does not exclude the diagnosis
• Free (non-ceruloplasmin bound) copper• Calculated parameter and subject to error
• Better for treatment monitoring than diagnosis
• > 25 g/dL in most untreated patients
Serum copper
151

Urinary copper excretion
• 24 hour collection
• Collected into acid-washed container to prevent coppercontamination
• Basal copper excretion >5 mol/24 h (320 g/24 h)suggestive of WD
• Műller et al 2007 used >1.6 mol/24 h (100 g/24 h)• 94% symptomatic patients• 69% asymptomatic siblings• 22% controls
• Penicillamine challenge - >25 mol/24 h (1600 g/24 h)
Liver Biopsy
• Histology may be supportive but features arenot pathognomonic
• Copper stains frequently negative• Hepatic copper content
• Normal < 50 g/g dry weight• WD > 250 g/g dry weight but may be lower than this
in up to 20% of WD patients• Maybe as high in chronic cholestasis• Avoid contamination, place biopsy directly into dry
plastic copper-free container. Do not use fixed tissue.
Molecular Genetics – ATP7B
• Haplotype and targeted mutation analysis
• Many laboratories now offer full gene sequenceanalysis and deletion/duplication analysis
• Carrier frequency ~1 in 90 based on caseidentification
• Population based studies using moleculartechniques suggest higher rates
• No mutation identified in up to 13% but others havehad 98% success in identifying gene defect
152

Leipzig Score 8th International conference on Wilson's disease and Menkes Disease. Leipzig/ Germany, April 16-18, 2001
Symptoms ScoreKF rings (slit lamp examination)
Present 2Absent 0
Neuropsychiatric symptoms suggestive of WD (or typical brain MRI)
Present 2Absent 0
Coombs negative hemolytic anemia (+ high serum copper)
Present 1Absent 0
Mutation analysisDisease causing mutations on both chromosomes 4Disease causing mutation on one chromosome 1No disease causing mutations detected 0
Laboratory Tests ScoreCeruloplasmin (mg/dL)
Normal 010-20 1< 10 2
Urinary copper (in absence of acute hepatitis)
Normal 01-2x ULN 1>2x ULN 2Normal but >5x ULN with penicillamine challenge 2
Liver Cu quantitationNormal -1<5x ULN 1>5x ULN 2
Rhodanine positive hepatocytes (only if hepatic Cu level not available)
Absent 0Present 1
Wilson Index for Predicting Mortality
Score Bilirubin
mol/L)
INR AST
(IU/L)
WCC
(x109 /L)
Albumin
(g/L)
0 0-100 0-1.2 0-100 0-6.7 >45
1 101-150 1.3-1.6 101-150 6.8-8.3 34-44
2 151-200 1.7-1.9 151-300 8.4-10.3 25-33
3 201-300 2.0-2.4 301-400 10.4-15.3 21-24
4 >300 >2.5 >401 >15.4 <20
Dhawan A et al Liver Transpl. 2005
A score 11 – PPV 92% & NPV 97%
Treatment
• Aim to start chelation therapy asap in symptomaticindividuals
• Treatment is life-long, including during pregnancy
• If one treatment modality is discontinued, an alternativemodality must be substituted
• Discontinuation of all treatment leads to hepatic andneurologic decompensation, which may be refractory tofurther medical intervention
153

Treatment
• D-Penicillamine (chelator)• Serious side effects can occur in up to 30% of individuals
• Severe thrombocytopenia, leukopenia, aplastic anemia,nephrotic syndrome, polyserositis, Goodpasture syndrome,severe skin reactions
• Trientine (chelator)• Rash, anorexia, abdominal pain, aplastic anemia, muscle
cramps
• Zinc (blocks copper absorption)• GI disturbance
• Dietary copper restriction
Monitoring
• Why monitor?• Inadequate therapy, or non-adherence
• Adverse drug effects (especially with D-penicillamine treatment)
• Excessive long-term treatment may result in copper deficiency
• Frequency of monitoring visits depends on time fromdiagnosis, changing medications and compliance
• Serum copper and ceruloplasmin, LFTs, INR, CBC,urinalysis, and physical examination
• 24-hour urinary excretion of copper at least annually
• Primarily indicated for children and adolescents withfulminant presentation
• Chronic liver insufficiency
• Neurological injury not generally responsive
• Outcomes based on UNOS data• Pediatric survival 90% and 89% at 1 and 5 years
• Adult survival 88% and 86%
• 1 year survival better if transplanted for chronic liver disease than for ALF
Liver transplantation for Wilson disease
Arnon R et al. Liver transplantation for children with Wilson disease: comparison of outcomes between children and adults. Clin Transplant. 2011 Jan-Feb;25(1):E52-60.
154

Asymptomatic siblings
• The goal is to identify affected siblings of a probandbefore they become symptomatic
• If mutations known, testing with molecular genetics isappropriate
• If mutations not known standard clinical testing can beconducted
• Treatment with zinc alone may suffice, but is requiredlife-long
Future directions: New research
• Phenotypic variation• Genetic
• Epigenetic
• Environmental
• New Drug Treatments• (Ammonium tetrathiomolybdate)
• Intrahepatic copper chelator
• Screening
Gateau & Delangle Ann N Y AcadSci. 2014
Future directions: Population screening
• Population frequency 1 in 30,000
• Presymptomatic diagnosis is reliable, treatment canprevent manifestations of disease
• Ceruloplasmin and serum copper not useful for infantscreening
• A novel proteomic screening approach is beinginvestigated using liquid chromatography–multiplereaction monitoring–mass spectrometry (LC-MRM-MS)looking at ATP7B protein levels
155
Conclusion
• Understanding copper metabolism helps explain findings in Wilson disease
• Scoring systems are available to aid diagnosis and prognosis
• Molecular genetic testing is most direct and reliable method of diagnosis
• Treat promptly and monitor copper status carefully in follow up
• Treatment is life-long• Neonatal screening has the potential to prevent morbidity
and death from Wilson disease
156

Blame the Genes?Familial and Autoimmune Pancreatitis in Children
Véronique Morinville MD, FRCP(C)Pediatric Gastroenterology and Nutrition
Montreal Children’s HospitalMcGill University Health Centre
Montreal, QC, Canada
2015 NASPGHAN POSTGRADUATE COURSEThursday October 8, 2015; Washington DC
I have no financial relationships with a
commercial entity to disclose
Objectives of Presentation
• Understand when to consider familial andautoimmune etiologies in a child presentingwith pancreatitis
• Review the different genetic factors that maybe involved in familial‐type pancreatitis
• Recognize factors implicated in autoimmunepancreatitis (AIP) types 1 and 2 and whattherapies may be attempted
157

OBJECTIVE 1
When to consider familial and autoimmune etiologies in pediatric pancreatitis?
AP = Acute PancreatitisARP = Acute Recurrent Pancreatitis
CP = Chronic Pancreatitis
ETIOLOGIES‐Single Episode AP Pediatric Series
Morinville 2008; Lautz 2011; Morinville 2012, others
AnatomicBiliary/ StonesTraumaticMedications / ToxinsMulti‐SystemicInfectionsMetabolicIatrogenicFamilial/ Hereditary “Idiopathic” (↓)
Diagnosis of AP:
At least 2 of 3 of:
• Pain compatiblewith pancreas origin
• Amylase and/or Lipase ≥ 3 x ULN
• Imaging
Etiologies ARP and CP
Etiologies Adults: TIGAR‐O classification
– Toxic/ Metabolic (EtOH,smoking)
– Idiopathic– Genetic (? %)– Autoimmune (2‐6%)– Recurrent and severe
acute pancreatitis‐associated CP
– Obstructive
Etiologies Pediatrics:
– TIGAR‐O
– Multiple risk factors within same child
example: cohort of 105 CP children: 80% with ≥ 1 genetic mutation; 30%obstructive, 20% toxic/ metabolic (Uc: INSPPIRE cohort; 2015 DDW)
Okazaki 2005; UpToDate; Schwarzenberg 2015, Uc DDW Abstracts 2015, Oracz 2014; B Etemad 2001
158
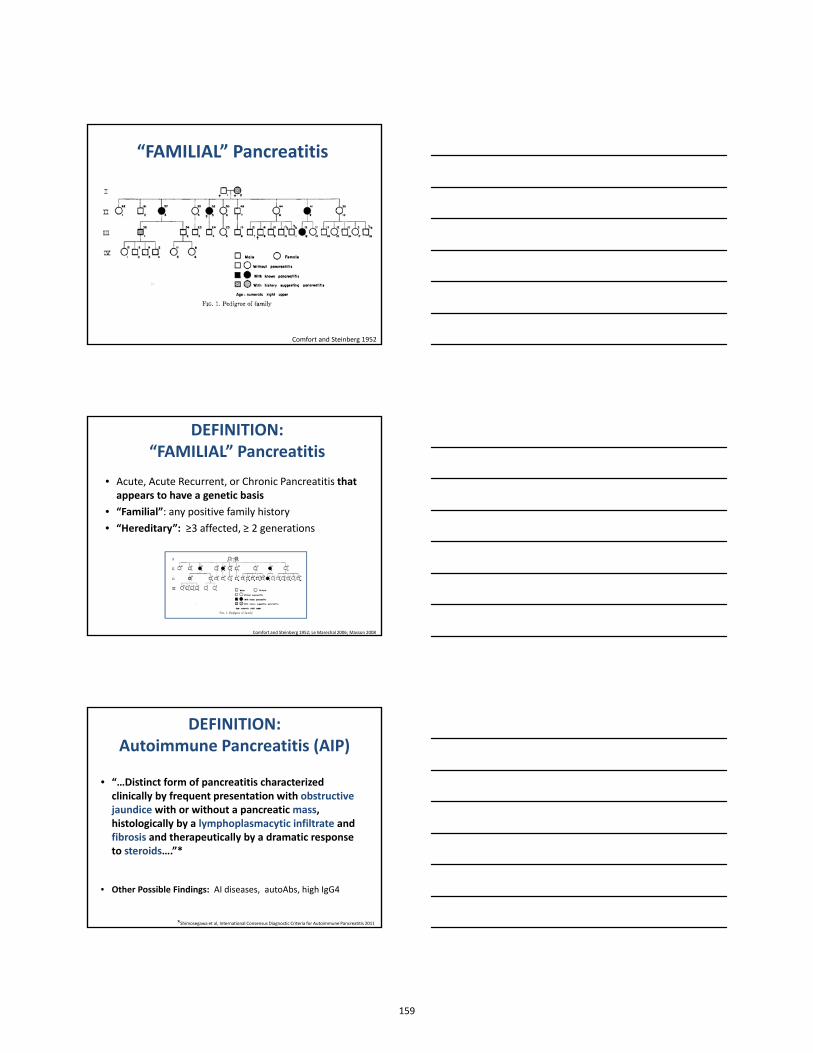
“FAMILIAL” Pancreatitis
Comfort and Steinberg 1952
DEFINITION: “FAMILIAL” Pancreatitis
• Acute, Acute Recurrent, or Chronic Pancreatitis that appears to have a genetic basis
• “Familial”: any positive family history • “Hereditary”: ≥3 affected, ≥ 2 generations
Comfort and Steinberg 1952; Le Marechal 2006; Masson 2008
DEFINITION: Autoimmune Pancreatitis (AIP)
• “…Distinct form of pancreatitis characterized clinically by frequent presentation with obstructive jaundice with or without a pancreatic mass, histologically by a lymphoplasmacytic infiltrate and fibrosis and therapeutically by a dramatic response to steroids….”*
• Other Possible Findings: AI diseases, autoAbs, high IgG4
*Shimosegawa et al, International Consensus Diagnostic Criteria for Autoimmune Pancreatitis 2011
159

WHEN to Consider “Familial” –Type Pancreatitis?
• Presentations: ARP +++, CP +++ (esp. calcific), even AP
• “Pancreas‐only” manifestations (certain genes)
• Family History + ; > 1 generation involved +++
• “Younger” age of onset (= all pediatrics)
• Pancreatitis with Absence of Obvious Trigger(**multiple risks)
WHEN to Consider AIP?
• Presentation: CP > AP, ARP (but all possible)
• HPI: ill‐defined > acute presentation
• Sx: Abdominal pain, jaundice, weight loss
• PMHx IBD, Auto‐immunity
• Imaging: diffuse or focal mass, narrowed PD,dilated CBD
• Relatively rare, but ‐ *Any Pancreatitis withAbsence of Obvious Trigger *
OBJECTIVE 2
Review of Genetic Factors In Familial‐Type Pancreatitis
Comfort and Steinberg 1952; AGA Pancreas Gastroslides
160

Familial‐type Pancreatitis: Genetics
The trypsin‐dependent pathological model of chronic pancreatitis (Dr. D. Whitcomb, All rights reserved; Special thanks for use)
Consider Genetics in ALL Children with ARP or CP
CPA1CELCLDN2
PRSS1: Cationic Trypsinogen“Hereditary Pancreatitis”
• AD; Incomplete Penetrance; often extensive pedigrees
• PRSS1 gain‐of‐function mutations: ↑ activation trypsinogen intracellularly ↑ activation zymogen cascade
• Other mechanisms described
• ARP; CP; Exocrine and Endocrine insufficiency; Cancer
(R122H; N29I; A16V; rare)
AGA GastroSlides Pancreas
SPINK1: Secretory Trypsin Inhibitor Serine Protease Inhibitor Kazal Type 1
Active site
SPINK1
Trypsin
• SPINK1 in secretory granules; Binds active site trypsin 1:1• Clinically:
• mostly Co‐factor: disease‐modifying > disease‐”causing”•Tropical calcific pancreatitis‐ India; homozygous N34S
“Mutations” / variants ie N34S, P55S
161
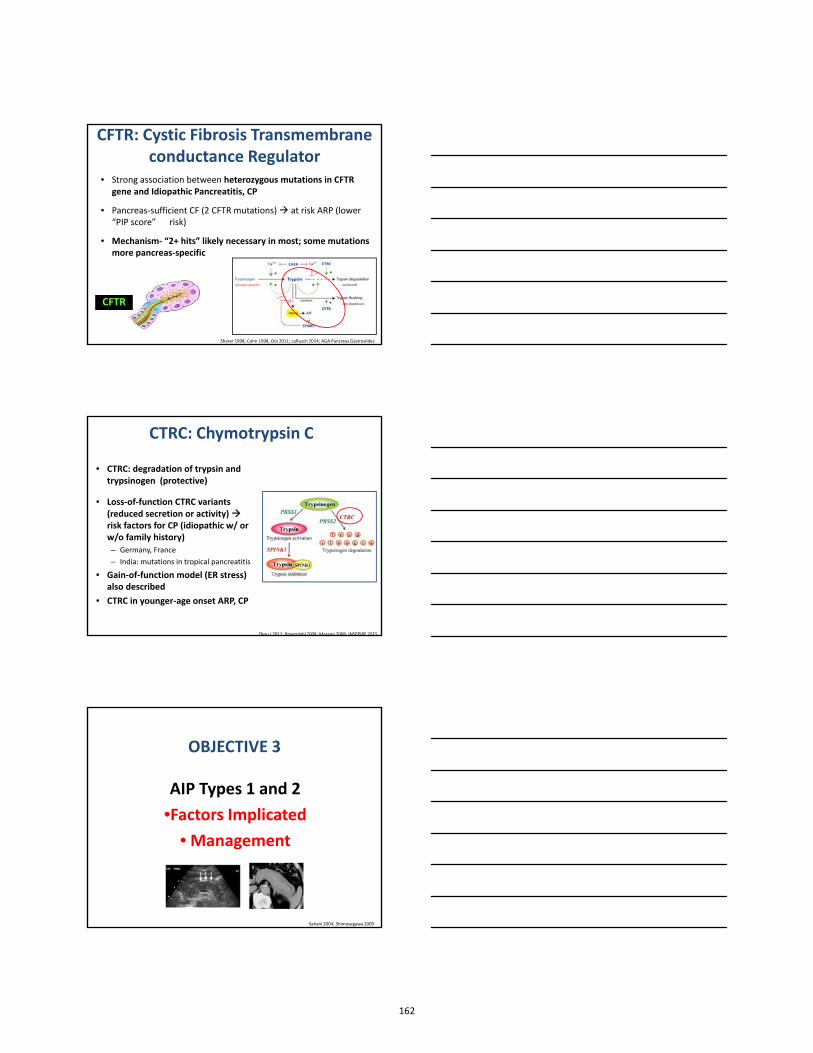
CFTR: Cystic Fibrosis Transmembraneconductance Regulator
• Strong association between heterozygous mutations in CFTR gene and Idiopathic Pancreatitis, CP
• Pancreas‐sufficient CF (2 CFTR mutations) at risk ARP (lower “PIP score” ↑ risk)
• Mechanism‐ “2+ hits” likely necessary in most; some mutationsmore pancreas‐specific
CFTRCFTR
Sharer 1998; Cohn 1998, Ooi 2011; LaRusch 2014; AGA Pancreas Gastroslides
CTRC: Chymotrypsin C
• CTRC: degradation of trypsin and trypsinogen (protective)
• Loss‐of‐function CTRC variants(reduced secretion or activity) risk factors for CP (idiopathic w/ orw/o family history)– Germany, France – India: mutations in tropical pancreatitis
• Gain‐of‐function model (ER stress) also described
• CTRC in younger‐age onset ARP, CP
Zhou J 2011; Rosendahl 2008; Masson 2008; INSPPIRE 2015
OBJECTIVE 3
AIP Types 1 and 2
•Factors Implicated
• Management
Sahani 2004; Shimosegawa 2009
162

AIP: History and Terminology
• “Chronic inflammatory sclerosis of the pancreas: an autoimmune pancreatic disease?” 1960s
• “Autoimmune Pancreatitis” 1990s
– Autoimmune propensity: other AI, autoAbs, steroid response– But no specific genes implicated
• Types 1 and 2 AIP described‐ 2000s; Sx, associations, histology
• Q. Several terms referring to AIP “spectrum”?
– Idiopathic sclerosing, primary inflammatory, lymphoplasmacytic
Sarles 1961; Chari 1994; Yoshida 1995
CHARACTERISTICS AIP
• Type 1– “pancreatic manifestation of
systemic fibroinflammatory disease” (bile ducts, salivary,kidney, LNs, retroperitoneal); “IgG4‐related”
– Pain, V, wt loss, jaundice– Elevated IgG4 (*cutoff dif.)– Peak age 60s, M> F, Asia– Mass pancreas head or
diffuse enlargement
*Can diagnose w/o histology
• Type 2– “pancreas‐specific”
(but: 1/3 IBD)
– Pain, V, wt loss, jaundice– No or low levels IgG4
– Peak age 40s, M=F, N.A.– Mass pancreas head or
diffuse enlargement
*Definitive Dx req biopsy
HISTOLOLOGY AIP: Core Biopsy, Resection
Type 1: Histology– LPSP: lymphoplasmacytic
sclerosing pancreatitis
– Periductal dense infiltrate plasma cells and lymphocytes; storiform fibrosis
– Obliterative phlebitis– No GELs
– Abundant IgG4+ plasma cells( > 10 cells/ hpf)
Type 2: Histology– IDCP: Idiopathic duct‐centric
pancreatitis
– periductal lymphoplasmacytic infiltrate; periductal, perilobular fibrosis, duct narrowing
– “GEL”: Granulocytic Epithelial Lesion‐ disruption small‐ med duct epithelium/ invasion neutrophilic granulocytes
– Low / no IgG4 cells ie < 10/hpf
Kusuda 2010Shimosegawa 2009
163

Diagnosis AIP: Adults
• 2000s: multiple societies/ countries publishing different diagnostic criteria
• 2007‐2011: HISORt and InternationalConsensus Diagnostic Criteria (ICDC)– Histology (core biopsy)– Imaging– Serology (IgG4 serum levels): > 2x ULN– Other organ involvement– +/‐ Response to steroid therapy (2w)– “Definitive” and “Probable” diagnoses
HISORt: Chari J Gastro 2007; ICDC: Shimosegawa et al Pancreas 2011
Criteria to Diagnose Type 1 AIP
Criterion Level 1 Evidence Level 2 Evidence
Histology LPSP (core biopsy/ resection)At least 3 criteria within
LPSP (core biopsy)2 criteria within
Imaging: Parenchyma
Imaging:Ductal
Diffuse enlargement/ delayed enhancement
> 1/3 length main PD or multiple strictures, no upstream dilation
segmental/ focal enlargement, delayed enhancement
Segmental narrowing PD, no upstream dilation (duct <5mm)
Serology IgG4 > 2x ULN IgG4: 1‐2x ULN
Other Organ Involvement
Histology extrapancreatic organsTypical Radiology (CBD, retroperit)
Histology extrapancreatic organsPhysical/ Radiologic evidence
Response totherapy
Diagnostic Steroid TrialImprovement 2w
Diagnostic Steroid TrialImprovement 2w
ADULT Criteria. Shimosegawa. International Consensus 2011
Criteria to Diagnose Type 2 AIP
Criterion Level 1 Evidence Level 2 Evidence
Histology:Core biopsy/ specimen
IDCP and:GEL w/ or w/o granulocytic acinarinflammation +
No/ scant IG4+ (0‐10 cells/ hpf)
Both: Granulocytic and lymphoplasmacytic acinarinfiltrate +
No/ scant IgG4 (0‐10 cells/ hpf)
Imaging: Parenchyma
Imaging:Ductal
Diffuse enlargement with delayed enhancement (typical)
Long (> 1/3 main PD) or multiple strictures, no upstream dilatation
Segmental/ focal enlargement with delayed enhancement
Segmental narrowing w/o upstream dilatation (duct <5mm)
Serology ‐ ‐
Other Organs ‐ IBD
Response totherapy
Diagnostic steroid trialImprovement 2w
Diagnostic steroid trialInvolvement 2w
ADULT Criteria. Shimosegawa. International Consensus 2011
164

AIP in Pediatrics: LiteratureCase Reports/ Small Series
• Presentations: Abdo pain (>> adults), V, weight loss, jaundice
• Imaging: globular enlarged, ill‐defined mass panc head; obstructionCBD; irreg/ multiple narrowings PD; DDx tumors but rarer
• Serology: Negative AI markers in most; IgG4 often N; rare > 2x ULN
• Other Organs: Few extrapancreatic manifestations‐ except IBD
• Histology: EUS‐guided trucut biopsy or laparoscopic bx via duo;laparotomy; AIP 2 > AIP 1 or NOS (histology not always obtained)
• Steroid response: not frequent empiric trial
* No Pediatric‐Specific Criteria for Diagnosis
* AIP type 2 > type 1 tendency suspected in recent years
Fukumori 2005; El‐Matary 2006; Blejter 2008; Refaat 2009; Gargouri 2009;Mannion 2011; Friedlander 2012; Fujii 2013; Oracz 2014; Zen 2014; Long 2015
Management AIP
• Surgical Resections (e.g. Whipple) – esp. older series, adults– Not 1st line in kids‐ if concern dx/neoplasm intra‐op biopsy
• Conservative Management: ↑ recent cases
• Biliary/ Pancreatic Stents to relieve obstruction (x few weeks)
• Corticosteroid therapy: Mainstay +/‐ Diagnostic (AIP 1 adult)– Prednisone 1 mg/kg/d x 2‐4 weeks; taper 2.5‐5 mg/w; +/‐ long term
• Immunomosuppression : if maintenance needed– MMF*, 6MP*, azathioprine, rituximab (*peds)
• Monitoring for recurrences/ complications‐ long‐term– Resolution? Atrophy? Other organs? Exocrine/ endocrine insufficiencies?
Fukumori 2005;El‐Matary 2006; Blejter 2008; Refaat 2009; Gargouri 2009; Mannion 2011; Friedlander 2012; Fujii 2013; Oracz 2014; Zen 2014; Long 2015
Management AIP:Long‐Term Outcomes Adults
• Retrospective: 23 institutions/ 10 countries/ 1064 patients• High response steroids: AIP 1‐ 99%, AIP 2‐ 92%• Biliary stents: for jaundice• Surgery: not primary Tx for AIP; done when unclear Dx• Relapses : AIP 1 ‐ 31%; AIP 2 ‐ 9%• Relapses: response to steroids +/‐ other (x 1‐3y)* No data in children
Hart 2013
Hart PA. Gut 2013
165

Future Directions: Autoimmune and Genetic Markers within Same Patients?
• Multiple risk factors within same children: 129 CPchildren tested for AIP (no tissue); genetics (CFTR, PRSS1, SPINK1)– Autoimmune Abs: 75/129. Of these: 32/75 genetic mutation;
16/75 anatomic AbN– IgG4 ↑: 24/68. Of these: 17/24 mutation; 5/24 anatomic– Suspicion AIP: 6 (5M): 11‐17y; 2 treated with steroids– Chronic autoimmune condition: 13 (UC 6, PSC 3, CD 1, others)
* High rate AutoAbs in pediatric CP. Significance?
* Interactions of Co‐factors? Further research indicated
Oracz G. Prz Gastroenterol 2014
TAKE HOME POINTS:Familial and Autoimmune Pancreatitis
in Children
1. Consider in all children – especially when without obvious etiology (metabolic, anatomic) or if recurrent/chronic (ARP, CP)
2. Virtually all “familial” patterns pancreatitis have a genetic predisposition (PRSS1, SPINK1, CTRC, CFTR‐ and others NYD)
• Multiple risks within one patient
• Many: genetic risk found / No known family history!
TAKE HOME POINTS: Familial and Autoimmune Pancreatitis
in Children
3. Autoimmune Pancreatitis: rarer , likely under‐diagnoseddue to need for tissue (for Type 2)
• Suspect Type 2 > Type 1 in children
4. Management AIP: #1 Corticosteroids; Observation;+/‐ Stents; +/‐ Immunomodulators; Surgery ↓ u lized;Long‐term Follow‐up necessary
5. Future Research: Risk Factor Interactions ?
166
Thank you
167

Getting to the Bottom of Perianal Crohn’s DiseaseGetting to the Bottom of
Perianal Crohn’s Disease
Maria Oliva-Hemker, M.D.Chief, Division of Pediatric Gastroenterology & Nutrition
Stermer Family Professor of Pediatric IBDJohns Hopkins University School of Medicine
Baltimore, MD
DisclosuresDisclosures
• Abbvie Immunology—grant funding• Abbvie Immunology—grant funding
Learning ObjectivesLearning Objectives
• Identify the lesions associated with perianalCrohn’s disease
• Review the pathophysiology andclassification systems for perianal fistulizingdisease
• Understand the approach to assessing andtreating the patient with perianal fistulizingdisease
• Identify the lesions associated with perianalCrohn’s disease
• Review the pathophysiology andclassification systems for perianal fistulizingdisease
• Understand the approach to assessing andtreating the patient with perianal fistulizingdisease
168

PerianalCrohn’s Disease
Fistula AbscessTags
Fissures
www.gicare.com
Prevalence of Pediatric Perianal Crohn’s Disease
Prevalence of Pediatric Perianal Crohn’s Disease
• Up to 38% of pediatric CD develop perianaldisease– 41/276 (15%) newly diagnosed children with
CD had perianal lesions within 30 days ofdiagnosis
– 28/276 (10%) had fistulas and/or abscesses
• 1 in 20 (5%) present with isolated fistulousdisease (and have no evidence ofintestinal involvement at presentation)
• Up to 38% of pediatric CD develop perianaldisease– 41/276 (15%) newly diagnosed children with
CD had perianal lesions within 30 days ofdiagnosis
– 28/276 (10%) had fistulas and/or abscesses
• 1 in 20 (5%) present with isolated fistulousdisease (and have no evidence ofintestinal involvement at presentation)
Keljo DJ et al, Inflamm Bowel Dis 2009
Skin Tags: Prevalence in Crohn’s Disease of Up to 70%Skin Tags: Prevalence in Crohn’s Disease of Up to 70%
• Type 1: “Elephant ear” tags– Flat or round, smooth– Soft/compressible– Flesh colored– Varying sizes– Painless
• Type 1: “Elephant ear” tags– Flat or round, smooth– Soft/compressible– Flesh colored– Varying sizes– Painless
• Type 2: arise from healed fissures, ulcers or hemorhoids– Edematous, usually hard– Red, blue or cyanotic– Larger than Type1– Irregular surface– Painful
• Type 2: arise from healed fissures, ulcers or hemorhoids– Edematous, usually hard– Red, blue or cyanotic– Larger than Type1– Irregular surface– Painful
Bonheur JL et al, Inflamm Bowel Dis 2008
169

Anal FissuresAnal Fissures
• Prevalence of up to 20%
• Broad based and deep
• Usually painless
• May be associated with large skin tags
• May be multiple and placed at variouslocations around the anal canal
• Spontaneously heal >80% of patients
• Prevalence of up to 20%
• Broad based and deep
• Usually painless
• May be associated with large skin tags
• May be multiple and placed at variouslocations around the anal canal
• Spontaneously heal >80% of patients
Schwartz DA et al Inflamm Bowel Dis 2015Parks AG et al, Br J Surg 1976
Schwartz DA et al Inflamm Bowel Dis 2014Bell SJ et al Aliment Pharmacol Ther 2003
Simple Fistulas Complex Fistulas
170

Assessment of Perianal FistulasAssessment of Perianal Fistulas
• Flexible sigmoidoscopy or colonoscopy– to evaluate for rectosigmoid involvement
(predicts more aggressive course)
• Exam under anesthesia (EUA)– gold standard (for experienced surgeon)
• Pelvic MRI is considered gold standardimaging technique– Endoanal ultrasound (EUS) may be useful
alternative to MRI (adults)
• Flexible sigmoidoscopy or colonoscopy– to evaluate for rectosigmoid involvement
(predicts more aggressive course)
• Exam under anesthesia (EUA)– gold standard (for experienced surgeon)
• Pelvic MRI is considered gold standardimaging technique– Endoanal ultrasound (EUS) may be useful
alternative to MRI (adults)
Treatment Goals for Fistulizing DiseaseTreatment Goals for Fistulizing Disease
• Short Term– Drainage of abscesses/control sepsis– Relief of symptoms
• Long Term– Resolution of drainage– Fistula closure– Improve quality of life– Avoid proctocolectomy and permanent ostomy
• Short Term– Drainage of abscesses/control sepsis– Relief of symptoms
• Long Term– Resolution of drainage– Fistula closure– Improve quality of life– Avoid proctocolectomy and permanent ostomy
Critical Evaluation of Data from Therapeutic Trials
Critical Evaluation of Data from Therapeutic Trials
Medication Evidence Efficacy
Antibiotics B+ Good
Corticosteroids D Poor
6-Mercaptopurine/Azathioprine
C+ Good
Methotrexate C+ Good/Fair
Cyclosporine C+ Fair
Tacrolimus C+ Good
Infliximab A+ Excellent
Adalimumab A Excellent
Certolizumab Pegol A Excellent
Vedolizumab A Good
Schwartz DA et al, Inflamm Bowel Dis 2015
171
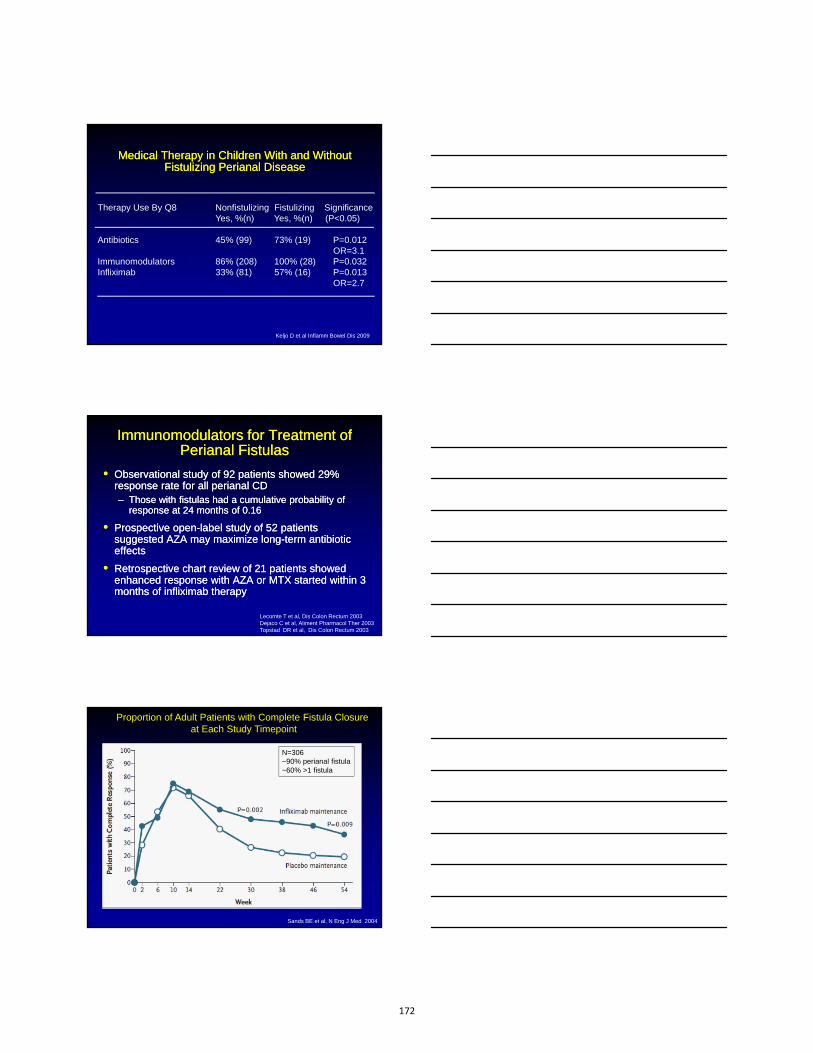
Therapy Use By Q8 Nonfistulizing Fistulizing SignificanceYes, %(n) Yes, %(n) (P<0.05)
Antibiotics 45% (99) 73% (19) P=0.012OR=3.1
Immunomodulators 86% (208) 100% (28) P=0.032Infliximab 33% (81) 57% (16) P=0.013
OR=2.7
Medical Therapy in Children With and Without Fistulizing Perianal Disease
Medical Therapy in Children With and Without Fistulizing Perianal Disease
Keljo D et al Inflamm Bowel Dis 2009
Immunomodulators for Treatment of Perianal Fistulas
Immunomodulators for Treatment of Perianal Fistulas
• Observational study of 92 patients showed 29%response rate for all perianal CD– Those with fistulas had a cumulative probability of
response at 24 months of 0.16
• Prospective open-label study of 52 patientssuggested AZA may maximize long-term antibiotic effects
• Retrospective chart review of 21 patients showedenhanced response with AZA or MTX started within 3 months of infliximab therapy
• Observational study of 92 patients showed 29%response rate for all perianal CD– Those with fistulas had a cumulative probability of
response at 24 months of 0.16
• Prospective open-label study of 52 patientssuggested AZA may maximize long-term antibiotic effects
• Retrospective chart review of 21 patients showedenhanced response with AZA or MTX started within 3 months of infliximab therapy
Lecomte T et al, Dis Colon Rectum 2003Dejaco C et al, Aliment Pharmacol Ther 2003Topstad DR et al, Dis Colon Rectum 2003
Sands BE et al, N Eng J Med 2004
Proportion of Adult Patients with Complete Fistula Closureat Each Study Timepoint
N=306~90% perianal fistula~60% >1 fistula
172

Maintenance of Complete Fistula Closure in Crohn’s Disease with Anti-TNFα Agents
Maintenance of Complete Fistula Closure in Crohn’s Disease with Anti-TNFα Agents
Infliximab at 1 yrN=306
Adalimumab at 1 yrN=117
Certolizumab at 6 mosN=58
17%
36%
Sands BE et al, N Eng J Med 2004Colombel JF et al Gut 2009Schreiber S et al, Alimen Pharmacol Ther 2011
Improved Fistula Healing with Adalimumab and Ciprofloxacin Improved Fistula Healing with Adalimumab and Ciprofloxacin
Dewint P et al, Gut 2014
Patients received Ada 160 mg wk 0, 80 mg wk 2 and then 40 mg qo wk. Then Randomized to Cipro 500 mg bid or placebo
Dupont-Lucas C et al, Aliment Pharmacol Ther 2014
Time to First Loss of Response to Infliximab in 89 Children with Perianal Fistulas
0 2 4 6 8 10
89 84 80 68 62 48
1.0
0.8
0.6
Duration of follow-up (months)
Pa
tient
s w
ith s
usta
ined
per
iana
l res
pons
e (%
)
0.4
0.2
0.0
173

Medical Management of Pediatric Perianal Fistulas
Medical Management of Pediatric Perianal Fistulas
• No large clinical trials or long-term follow-upexists in children
• Various small studies have suggestedhealing rates superior to adults (>70%)following infliximab therapy
• Loss of response and recurrences ascommon as among adults
• No large clinical trials or long-term follow-upexists in children
• Various small studies have suggestedhealing rates superior to adults (>70%)following infliximab therapy
• Loss of response and recurrences ascommon as among adults
Crandall W et al, J Pediatr Gastroenterol Nutr 2009Di Bie CI et al, Inflamm Bowel Dis 2012Hyams J et al, Gastronenterology 2007
Surgical Management of Fistulizing Perianal Disease
Fichera A & Zoccali M, Inflamm Bowel Dis 2015
EUA
I&D, Drains, Setons
Fistulotomy, Glue, Plug,Setons, Advancement Flap
Proctectomy,Total Proctocolectomy
Sepsis control
Definitive surgical treatment
Resolution
Resolution
Failure
Failure
Management of Perianal Abscesses
Schwartz DA et al, Ann Intern Med 2001Fichera A & Zoccali M, Inflamm Bowel Dis 2015
Simple incision& drainage
Placement of mushroomcatheter
Noncutting seton
174

Fistulotomy for Simple FistulasFistulotomy for Simple Fistulas
• Initial healing rates in adults– 80%-100% in 13 studies– 60-79% in 5 studies– ≤59% in 3 studies
• Recurrence rates 0-20% in 7 of 10 studies
• Initial healing rates in adults– 80%-100% in 13 studies– 60-79% in 5 studies– ≤59% in 3 studies
• Recurrence rates 0-20% in 7 of 10 studiesSandborn WJ et al Gastroenterology 2003DA Schwartz et al Ann Intern med 2001
ProbeExternalopening
Fistula
Open fistulatract
Anus
Setons Prevent Premature Fistula ClosureSetons Prevent Premature Fistula Closure
Schwartz DA et al Inflamm Bowel Dis 2014
Per
cent
age
of P
atie
nts
Response (p=0.14) Recurrence (p=0.001)
83%
100%
44%
79%
Response and Recurrence Rates Among Adults with Perianal Fistulas Treated with Infliximab +/- Setons
Response and Recurrence Rates Among Adults with Perianal Fistulas Treated with Infliximab +/- Setons
Regueiro M & Mardini H, Inflamm Bowel Dis 2003
175

Anal Fistula Plug
Bioabsorbable xenograftmade of lyophilized porcineintestinal submucosa
Infection resistant
No foreign body reaction
Within months becomespopulated with host celltissue
24-87% success rates instudies 6-12 months follow-up
Cook®Biodesign® Anal Fistula Plug
Rizzo JA et al Surg Clin N Am 2009
Fibrin GlueFibrin Glue
• Mixture of fibrinogen andthrombin & calcium
• Insoluble clot formed
• Believed to stimulatewound healing andinduce angiogenesis
• Discrepant findings havebeen reported in meta-analysis
• Mixture of fibrinogen andthrombin & calcium
• Insoluble clot formed
• Believed to stimulatewound healing andinduce angiogenesis
• Discrepant findings havebeen reported in meta-analysis
Citocchi R et al, Ann Ital Chir 2010Rizzo JA et al Surg Clin N Am 2009
Colorectalsurgeonsydney.com.au
Endorectal Advancement Flap
Ruffolo C et al Colorectal Dis 2010Fichera A & Zoccali M, Inflamm Bowel Dis 2015
• Success rates 40%->90% reported• Incontinence is a concern• Option for rectovaginal fistula
176

Yassin NA et al, Aliment Pharmacol Ther 2014
Combined Surgical and Medical Therapy Increases Perianal Fistula Healing
Combined Surgical and Medical Therapy Increases Perianal Fistula Healing
• Systematic review of 24 articles; 1139 patients– 40% received single treatment (Anti-TNF ±
immunomodulator or surgical intervention)– 60% combo therapy
• Outcomes– Single therapy 191/448 (43%) in complete remission
• 34% had no response– Combo 180/349 (52%) in complete remission
• 23% had no response
• Systematic review of 24 articles; 1139 patients– 40% received single treatment (Anti-TNF ±
immunomodulator or surgical intervention)– 60% combo therapy
• Outcomes– Single therapy 191/448 (43%) in complete remission
• 34% had no response– Combo 180/349 (52%) in complete remission
• 23% had no response
Outcome of Patients with Perianal Crohn’s Disease Undergoing Temporary Fecal Diversion
Outcome of Patients with Perianal Crohn’s Disease Undergoing Temporary Fecal Diversion
Fecal Diversionn=138
Successful Stoma Closuren=36
Persistent Stoman=102
Repeat DiversionN=6
Stoma Closuren=30
Indefinite Stoman=45
Permanent Stoman=63
Gu J et al, Colorectal Dis 2014
n=30
n=4
n=60
n=41
n=2
(22%) (33%) (45%)
Simple fistula without rectal inflammation
• Antibiotics and AZA/6MP
• Consider Anti-TNF
Proposed Treatment Algorithm for Simple Perianal FistulasProposed Treatment Algorithm for Simple Perianal Fistulas
Simple fistula with rectal inflammation
Antibiotics, AZA/6-MP& Anti-TNF
(consider monitoring healing with repeat imaging study)
1. Consider seton2. Fistulotomy3. Consider fibrin glue,
fistula plug or endorectaladvancement flap
4. If 1-3 fails, treat as complex fistula
Continue maintenance AZA/6-MP or Anti-TNF if
started
Treat as complex
fistula
Continue maintenance AZA/6-MP &
Anti-TNF
TreatmentFailure
TreatmentSuccess
TreatmentSuccess
TreatmentFailure
Schwartz DA et al, Inflamm Bowel Dis 2015; de Zoeten EF et al, J Pediatr Gastro Nutr 2013
History and physical exam (digital exam for stricture) Colonoscopy (assess for proctitis; dilation if needed) Exam under anesthesia (EUA) Imaging (EUS or MRI) to delineate perianal disease
177

History and physical exam (digital exam for stricture) Colonoscopy (assess for proctitis, dilation if needed) Exam under anesthesia (EUA) Imaging (EUS or MRI) to delineate perianal disease
Proposed Treatment Algorithm for Complex Perianal FistulasProposed Treatment Algorithm for Complex Perianal Fistulas
TreatmentSuccess
TreatmentFailure
Schwartz DA et al, Inflamm Bowel Dis 2015; de Zoeten EF et al, J Pediatr Gastro Nutr 2013
ComplexFistula
• Seton placement• Antibiotics, Anti
TNF, AZA/6-MP (consider monitoring
healing with repeat imaging study)
1. Remove seton2. Continue
maintenance AZA/6-MP & Anti-TNF
1. Consider tacrolimusin selected patientsOR
2. Proctocolectomy
Take Home Points for Perianal FistulizingCrohn’s Disease
Take Home Points for Perianal FistulizingCrohn’s Disease
• Use MRI and EUA for suspected disease todefine the anatomy
• Drain abscesses
• Use setons as required to control sepsis
• Treat proctitis/intestinal inflammation
• More definite surgical closure should beconsidered only after intestinal inflammationunder control
• Team approach: gastroenterologists, surgeonsand radiologists
• Use MRI and EUA for suspected disease todefine the anatomy
• Drain abscesses
• Use setons as required to control sepsis
• Treat proctitis/intestinal inflammation
• More definite surgical closure should beconsidered only after intestinal inflammationunder control
• Team approach: gastroenterologists, surgeonsand radiologists
178

“IT’S ALL ABOUT THAT POUCH…”EVALUATION & MANAGEMENT OF
COMPLICATIONS POST ILEAL POUCH ANAL ANASTOMOSIS
Joel R. Rosh, MDDirector, Pediatric Gastroenterology
Goryeb Children’s Hospital/Atlantic HealthProfessor of Pediatrics
Icahn School of Medicine, Mount Sinai School of Medicine
A “Tale” of Two Pouches:The Agony and the Ecstasy
Joel R. Rosh, MDDirector, Pediatric Gastroenterology
Goryeb Children’s Hospital/Atlantic HealthProfessor of Pediatrics
Icahn School of Medicine, Mount Sinai School of Medicine
Disclosures
• Grant Support:– Abbvie, Janssen
• Consultant:– Abbvie, Janssen, Receptos
179

Objectives
• Review the data for evaluation, treatment andprevention of pouchitis
• Understand other complications of IPAA• Review cancer screening /surveillance
recommendations
The Allure
“Patients will be better off after operation…Their colitis will be cured…feeling of good health and a satisfactory quality of life will return”
Kelly KA. Advanced Therapy of IBD, 2001
The Allure
“Patients will be better off after operation…Their colitis will be cured…feeling of good health and a satisfactory quality of life will return”
Kelly KA. Advanced Therapy of IBD, 2001
So true when it all goes right…
180
Colectomy Risks
• Bleeding• Post‐op obstruction• Wound infection• Intra‐abdominal infection• Wound hernia• Thromboembolic events• Urinary retention
EIM After Surgery
Usually Resolve
• Peripheral arthritis• Uveitis• Thromboembolic
risk
May Not Resolve
• Skin– Erythema nodosum– Pyoderma
gangrenosum
• PSC• AIH• Central arthritis
(spondylitis)
Surgical Options After Colectomy
• Brooke Ileostomy– Noise, odor, leak, local skin breakdown
• Kock Pouch (continent ileostomy)– Pouchitis, need for revision of reservoir
• Ileal anal anastomosis– A more culturally acceptable Kock pouch– Mechanical issues, pouchitis, ischemia
181

} ~1 1/2 inches
Slide courtesy of Dr. Michael Harris
Creating the Pouch
Slide courtesy of Dr. Michael Harris
Creating the Pouch
“J” “S” “K”
Tip of “J”
Afferent limb (neo-TI)
Efferent limb
Outlet/cuff/anal transitionalzone
Inlet
Efferent limb
Types of Ileal Pouch
Nipple valve
Slide courtesy of Dr. Bo Shen
182

Slide courtesy of Dr. Michael Harris
Mucosectomy vs. 2 Staple IPAA
Disorders of the Ileal Pouch
FunctionalSurgical/Mechanical
Inflammatory/Infectious
• Anastomotic leak• Pelvic sepsis• Sinus• Fistula• Strictures.• Infecundity• Sexual dysfunction• Portal vein thrombi• Prolapse• Twist/volvulus
Pouchitis Cuffitis Crohn’s SBBO Inflammatory
polyps
Neoplastic
Pouch/ATZ Neoplasia
Lymphoma Squamous
cell cancer
Systemic/Metabolic
Anemia Bone loss Vit D/B12
def. Renal stone Celiac dis. High PTH
Modified from Shen B, et al. AJG 2005;100;93-101
Irritable pouch Poor
compliance Pseudo-
obstruct megapouch “Pouchalgia
fugax”
Disorders of the Ileal Pouch
FunctionalSurgical/Mechanical
Inflammatory/Infectious
• Anastomotic leak• Pelvic sepsis• Sinus• Fistula• Strictures• Infecundity• Sexual dysfunction• Portal vein thrombi• Prolapse• Twist/volvulus
Pouchitis Cuffitis Crohn’s SBBO Inflammatory
polyps
Neoplastic
Pouch/ATZ Neoplasia
Lymphoma Squamous
cell cancer
Systemic/Metabolic
Anemia Bone loss Vit D/B12
def. Renal stone Celiac dis. High PTH
Irritable pouch Poor
compliance Pseudo-
obstruct megapouch “Pouchalgia
fugax”
Modified from Shen B, et al. AJG 2005;100;93-101
183

Disorders of the Ileal Pouch
FunctionalSurgical/Mechanical
Inflammatory/Infectious
• Anastomotic leak• Pelvic sepsis• Sinus• Fistula• Strictures• Infecundity• Sexual dysfunction• Portal vein thrombi• Prolapse• Twist/volvulus
Pouchitis Cuffitis Crohn SBBO Inflammatory
polyps
Neoplastic
Pouch/ATZ Neoplasia
Lymphoma Squamous
cell cancer
Systemic/Metabolic
Anemia Bone loss Vit D/B12
def. Renal stone Celiac dis. High PTH
Irritable pouch Poor
compliance Pseudo-
obstruct megapouch “Pouchalgia
fugax”
Modified from Shen B, et al. AJG 2005;100;93-101
Disorders of the Ileal Pouch
FunctionalSurgical/Mechanical
Inflammatory/Infectious
• Anastomotic leak• Pelvic sepsis• Sinus• Fistula• Strictures• Infecundity• Sexual dysfunction• Portal vein thrombi• Prolapse• Twist/volvulus
Pouchitis Cuffitis Crohn SBBO Inflammatory
polyps
Irritable pouch Poor
compliance Pseudo-
obstruct megapouch “Pouchalgia
fugax”
Neoplastic
Pouch/ATZ Neoplasia
Lymphoma Squamous
cell cancer
Systemic/Metabolic
Anemia Bone loss Vit D/B12
def. Renal stone Celiac dis. High PTH
Modified from Shen B, et al. AJG 2005;100;93-101
Disorders of the Ileal Pouch
FunctionalSurgical/Mechanical
Inflammatory/Infectious
• Anastomotic leak• Pelvic sepsis• Sinus• Fistula• Strictures• Infecundity• Sexual dysfunction• Portal vein thrombi• Prolapse• Twist/volvulus
Neoplastic
Neoplasia Lymphoma Squamous
cell cancer
Systemic/Metabolic
Pouchitis Cuffitis Crohn SBBO Inflammatory
polyps
Irritable pouch Poor
compliance Pseudo-
obstruct megapouch “Pouchalgia
fugax”
Anemia Bone loss Vit D/B12
def. Renal stone High PTH
Modified from Shen B, et al. AJG 2005;100;93-101
184

Pouch Evaluation
• Stool cultures including C. Difficile
• Pouchoscopy with biopsy– Rule out mucosal disease (inflamm vs malig.)
• Imaging– If suspect mechanical issue
– Cross-sectional
– “pouchagram” (emptying, leak)
Pouchoscopy—Owl Eye View
Endoscopic Patterns in Pouchitis
Classic Pouchitis
Immune-MediatedPouchitis
Ischemic Pouchitis
Slide courtesy of Dr. Bo Shen
185

Pouchitis Therapy
• Antibiotics/Probiotics– Metronidazole
– Cipro
– Rifaximin
– VSL #3 (?prophylaxis)
– ???Fecal Microbial Transplant (FMT)
• Anti-Inflammatory– Topical
– Systemic
Ischemic Pouchitis: Think Tension
Shen B, et al, Inflamm Bowel Dis 2010;16:836–46
Crohn’s Disease of the Pouch
Inflammatory Fibrostenotic Fistulizing
Slide courtesy of Dr. Bo Shen
186
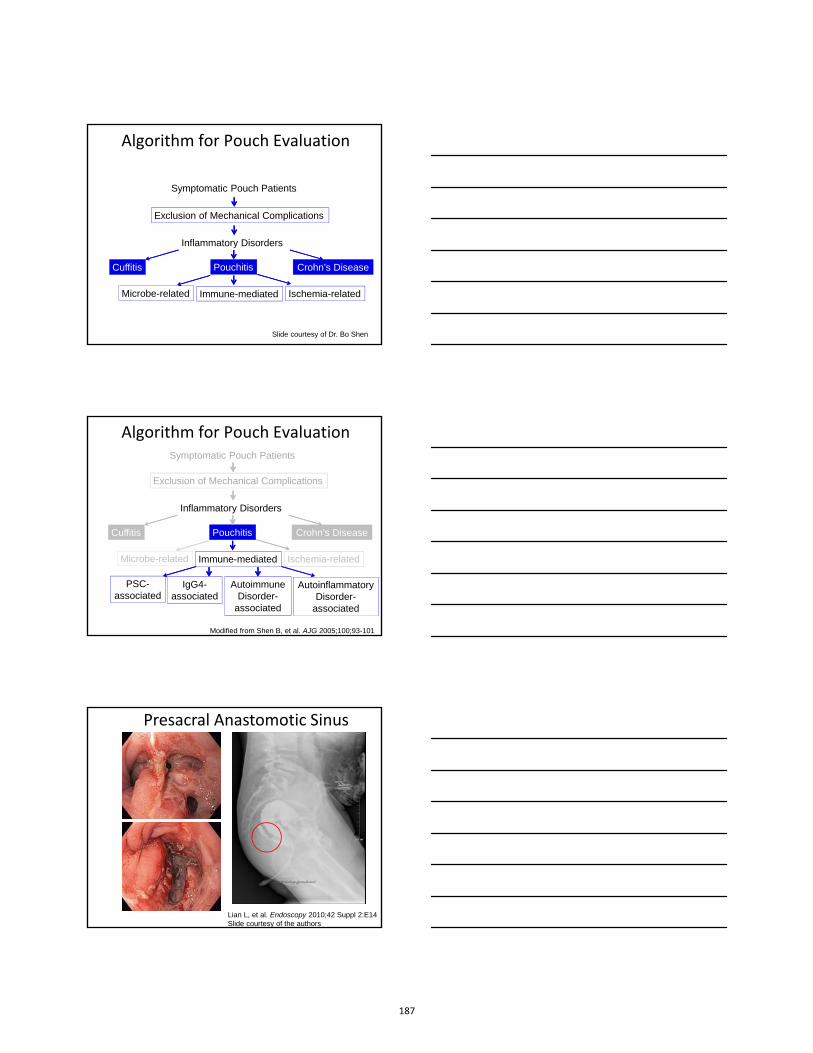
Algorithm for Pouch Evaluation
Symptomatic Pouch Patients
Exclusion of Mechanical Complications
Inflammatory Disorders
Cuffitis Pouchitis Crohn’s Disease
Microbe-related Immune-mediated Ischemia-related
Slide courtesy of Dr. Bo Shen
Symptomatic Pouch Patients
Exclusion of Mechanical Complications
Inflammatory Disorders
Cuffitis Pouchitis Crohn’s Disease
Microbe-related Immune-mediated Ischemia-related
PSC-associated
IgG4-associated
Autoimmune Disorder-
associated
AutoinflammatoryDisorder-
associated
Algorithm for Pouch Evaluation
Modified from Shen B, et al. AJG 2005;100;93-101
Presacral Anastomotic Sinus
Lian L, et al. Endoscopy 2010;42 Suppl 2:E14Slide courtesy of the authors
187

IPAA: Pediatric Outcomes
• 202 children over 30 years at Mayo
• 87% returned questionnaires
• Median follow up 181.5 months (7.8-378.5)
Polites SF. J Pediatr Surg 2015 epub
IPAA: Pediatric Outcomes
• UC pouch survival 92%
• 16% diagnosed with CD (61% pouch survival)
• 12% chronic pouchitis
• 7% pouch failure
• QOL excellent in majority
Polites SF. J Pediatr Surg 2015 epub
IPAA: Cancer Risk• 42 reports of pouch adenocarcinoma• Possibly due to “Islets” after mucosectomy
• Potential contributing factors:– ?pouchitis
– ?Primary Sclerosing Cholangitis (PSC)
• Previous neoplasia is main risk factor
Cancer 2011;117:3081–3092Colorectal Dis 2012;14:92–97Gastroenterology 2014;146:119–128
188
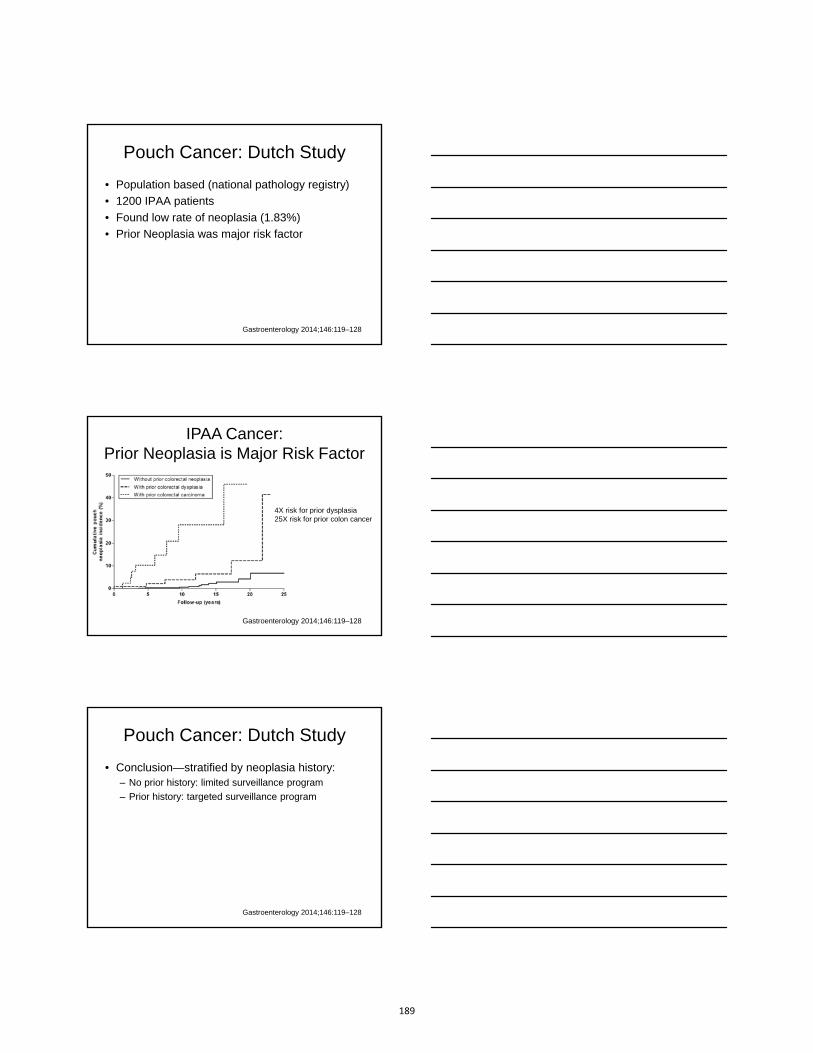
Pouch Cancer: Dutch Study
• Population based (national pathology registry)
• 1200 IPAA patients
• Found low rate of neoplasia (1.83%)
• Prior Neoplasia was major risk factor
Gastroenterology 2014;146:119–128
IPAA Cancer: Prior Neoplasia is Major Risk Factor
Gastroenterology 2014;146:119–128
4X risk for prior dysplasia25X risk for prior colon cancer
Pouch Cancer: Dutch Study
• Conclusion—stratified by neoplasia history:– No prior history: limited surveillance program
– Prior history: targeted surveillance program
Gastroenterology 2014;146:119–128
189

Pouch Surveillance: Society Guidelines
• ACG, AGA, ASGE—none
• British Society of GI:– Yearly if high risk: Neoplasia, PSC, atrophy, inflammation
– Every five years in all others
Summary
• Pouch surgery improves quality of life
• Mechanical and inflammatory complications• Technical expertise of surgeon• Importance of team approach
Summary
Pouchitis: multiple potential etiologies—Bacteria-related (C. difficile is emerging)—If antibiotic refractory consider:
• Immune-mediated (including De novo Crohn’s)
• Ischemia-related
190

Summary
Cancer of the pouch rarely occurs• Prior neoplasia is biggest risk factor• PSC, chronic pouchitis also contribute• Surveillance guidelines are not yet optimized
• ?3-5 years unless high risk
191

Communicating the Benefits and Risks of IBD Therapy to Patients and Families
Corey A. Siegel, MD, MS
Geisel School of Medicine at Dartmouth
Dartmouth-Hitchcock Medical Center
NASPGHAN2015 Postgraduate Course
Disclosures
Consultant/Advisory BoardAbbvie, Given Imaging, Janssen, Salix, Lilly, Pfizer, Prometheus, Takeda, UCB
Speaker for CME activities Abbvie, Janssen, Takeda, UCB
Grant supportCCFA, AHRQ (1R01HS021747-01)
Abbvie, Janssen, UCB, Salix
Intellectual propertyDartmouth-Hitchcock Medical Center and Cedars-Sinai Medical Center have a patent pending
for a “System and Method of Communicating Predicted Medical Outcomes”, filed 3/34/10. Dr.
Corey Siegel and Dr. Lori Siegel are inventors.
Different aspects decision making
Medical Decision Making
Severity of illness
Benefits and Risks of
Treatment
Patient and Family Preferences
192

Hierarchy of Needs for the IBD Patient
Leaving the house, going to school or workAbility to eat and maintain weight
Staying AlivePatient focus
Physician focus
Just feel normalAvoid hospitals and surgery
Diarrhea, Bleeding, Pain, Fatigue, Incontinence
Endoscopic Remission
Clinical Remission
Histologic Remission
Learning Objectives
» To review the risks of immunomodulators and biologics
» To discuss decision making between anti-TNF monotherapy or combination therapy
» To learn about tools that can be used to better communicate the benefits and risks of IBD therapy
193

Crohn’s disease causes damage
Typical Course of a Crohn’s Patient
Damage occurs in UC as well
1. Proximal extension of disease
2. Stricturing
3. Pseudopolyposis
4. Dysmotility
5. Anorectal dysfunction
6. Impaired permeability
Torres, et al. Inflamm Bowel Dis 2012;18:1356.
194
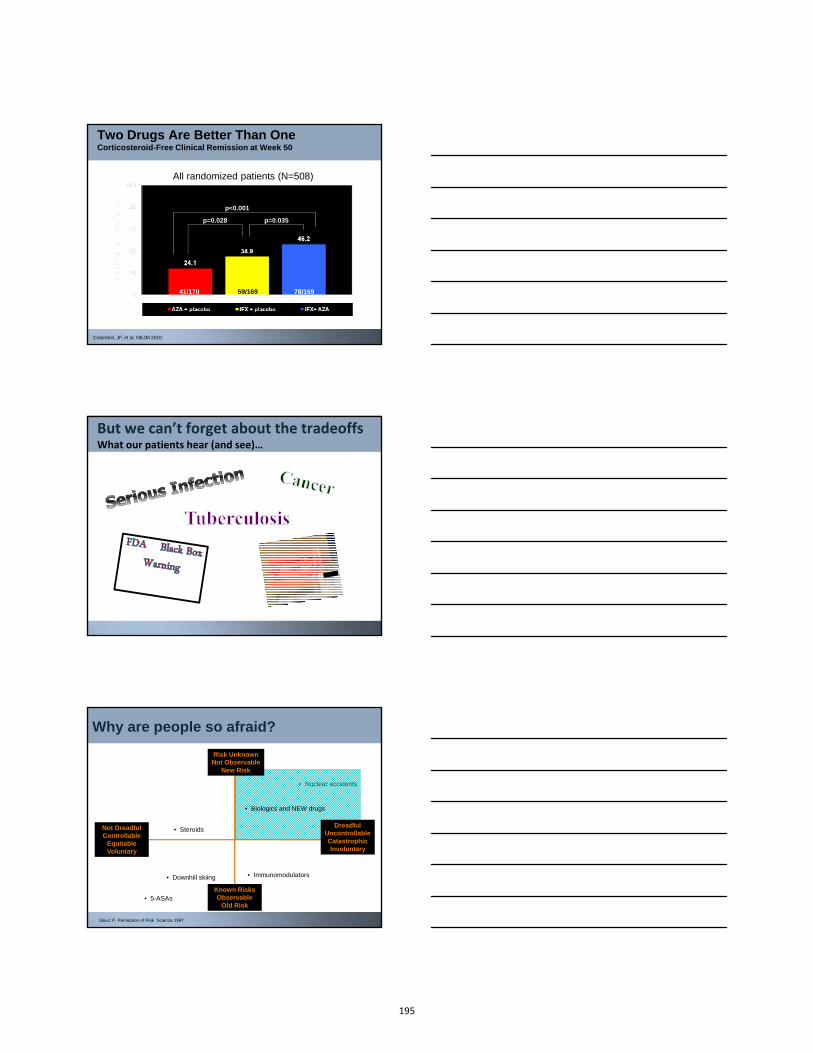
Two Drugs Are Better Than OneCorticosteroid-Free Clinical Remission at Week 50
All randomized patients (N=508)
p<0.001
p=0.028 p=0.035
41/170 59/169 78/169
Colombel, JF, et al. NEJM 2010
But we can’t forget about the tradeoffsWhat our patients hear (and see)…
Why are people so afraid?
Dread Risk
Unknown Risk
• Nuclear accidents
• 5-ASAs
• SteroidsNot DreadfulControllable
EquitableVoluntary
Known RisksObservable
Old Risk
DreadfulUncontrollableCatastrophicInvoluntary
Risk Unknown Not Observable
New Risk
Slovic P. Perception of Risk. Science 1987.
• Biologics and NEW drugs
• Immunomodulators• Downhill skiing
195

What are the most important side-effects of 6MP/Azathioprine?
Siegel CA, et al. APT 2005 (weighted average); Siegel CA, et al. CGH 2009Beaugerie et al, Lancet 2009;7:374.
EventFrequency Estimate
Stop therapy due to adverse event 11%
Allergic reactions 2%
Nausea 2%
Hepatitis 2%
Pancreatitis 3%
Serious infections 5%
Non-Hodgkin’s lymphoma0.04%-0.09% (4-
9/10,000)
Solid tumors and thiopurines in IBD(non-GI and non-skin cancers)
Study Types of cancer Number of patients
Statistically significant
Armstrong 2010 lung, breast 1955 NO
Fraser 2002breast, bronchial,
renal6262 NO
Connell 1994gastric, lung,
breast, cervical755 NO
No clear association between thiopurines and solid tumors in IBD
Methotrexate and Lymphoma
»Not a lot out there in IBD› PubMed search for “(Crohn’s OR ulcerative colitis) AND
methotrexate AND lymphoma” – 1 case report
› Farrell study: 2 of 4 cases of NHL were treated with MTX (2 out of 31 patients treated with MTX!)
»More info available for RA› Sweden: 348 lymphomas in RA patients, 37 were EBV+,
29/37 exposure to MTX
› Australia: SIR 5.1 (95% CI 2.2-10)
› United States: OR 1.4 (0.7-2.9)
Farrell, et al. Gut 2000. Baecklund, et al. Curr Opin Rheumatol 2004. Burchbinder, et al. Arthritis Rheum 2008.Wolfe, et al. Arhthritis Rheum 2007.
196

Adverse Events Associated with anti-TNF Treatment
Siegel CA. The inflammatory bowel disease yearbook, volume 6.; Infliximab package insert; Vermeire Gastro 2003; Cush, Ann Rheum Dis 2005; Lenercept study group, Neurology 1999; ATTACH trial 2003
Event Estimated Frequency
Stop therapy due to adverse event 10%
Infusion or injection site reactions 3%-20%
Drug related lupus-like reaction 1%
Serious infections 3%
Tuberculosis 0.05% (5/10,000)
Non-Hodgkin’s lymphoma (combo) 0.06% (6/10,000)
Multiple sclerosis, heart failure, serious liver injury
Case reports only
Same Mono or Combo
Risk of Dying from Sepsis on Infliximab: Systematic Review
Reference Study Design# Deaths from sepsis thought
attributable to infliximab# of
Patients
Ljung et al. Gut 2004Population
Based Cohort 1 191
Seiderer et al. Digestion 2004
Single-Center Cohort 0 92
Colombel et al. Gastroenterology 2004
Single-Center Cohort 5 500
Sands et al. NEJM 2004 Randomized Controlled Trial 2 282
Hanauer et al. Lancet 2002
Randomized Controlled Trial 1 573
Rutgeerts et al. Gastroenterology 1999
Randomized Controlled Trial 0 73
Siegel et al. Clin Gastroenterol Hepatol. 2006;4:1017-1024.
Risk of death from sepsis = 4/1000 pt-yrs
BUT it is a subgroup of patients at this high risk
»Older› Average age = 63 (systematic review); 67 (Mayo)
»Multiple co-morbidities
»Concomitant steroids and/or narcotics
»Long-standing disease
Siegel, CGH 2006; Colombel, Gastro 2004; Lichtenstein CGH 2006; Toruner, Gastro 2008
Young “healthy” patients are not in the clear, but probably at much less risk
197

» 8905 patients representing 20,602 pt-years of exposure
» 13 Non-Hodgkin’s lymphomas
» Mean age 52, 62% male
» 10/13 exposed to IM* (really a study of combo Rx)
Risk of NH Lymphoma with anti-TNF + IM treatment for Crohn’s Disease: A Meta-Analysis
NHL rate per 10,000
SIR 95% CI
SEER all ages 1.9 - -
IM alone 3.6 - -
Anti-TNF + IM vs SEER 6.1 3.23 1.5-6.9
Anti-TNF+ IM vs IM alone 6.1 1.7 0.5-7.1
Siegel et al, CGH 2009;7:874. *not reported in 2
6.1 per 10,000 pt-years
Risk without medicationRisk of lymphoma with immune suppression
Risk of Developing non-Hodgkin’s LymphomaPatient receiving Immunomodulator +/- anti-TNF Therapy for 1 year
Siegel CA, Inflamm Bowel Dis 2010;16:2168.
What do we know about the risk of solid tumors and anti-TNF?
Type of Cancer Odds Ratio
All cancers 1.0 (0.8-1.2)
All solid tumors 1.0 (0.8-1.2)
Colon 0.8 (0.3-1.7)
Lung 1.1 (0.7-1.8)
Breast 0.9 (0.5-1.3)
Pancreas 0.5 (0.1-2.6)
Melanoma 2.3 (0.9-5.4)
Non-melanoma 1.5 (1.2-1.8)
» Rheumatoid arthritis
» 13,000 patients, ½ on biologics
Wolfe, Arthritis and Rheumatism 2007;56:2886.Mason, Inflamm Bowel Dis 2013;19:1306.
Type of study Associated risk
Population based651 patients
SIR 0.7 (0.2-1.7)
Single center734 patients
OR 0.97 (0.56-1.65)
» Inflammatory bowel disease
» Fairly limited data
198
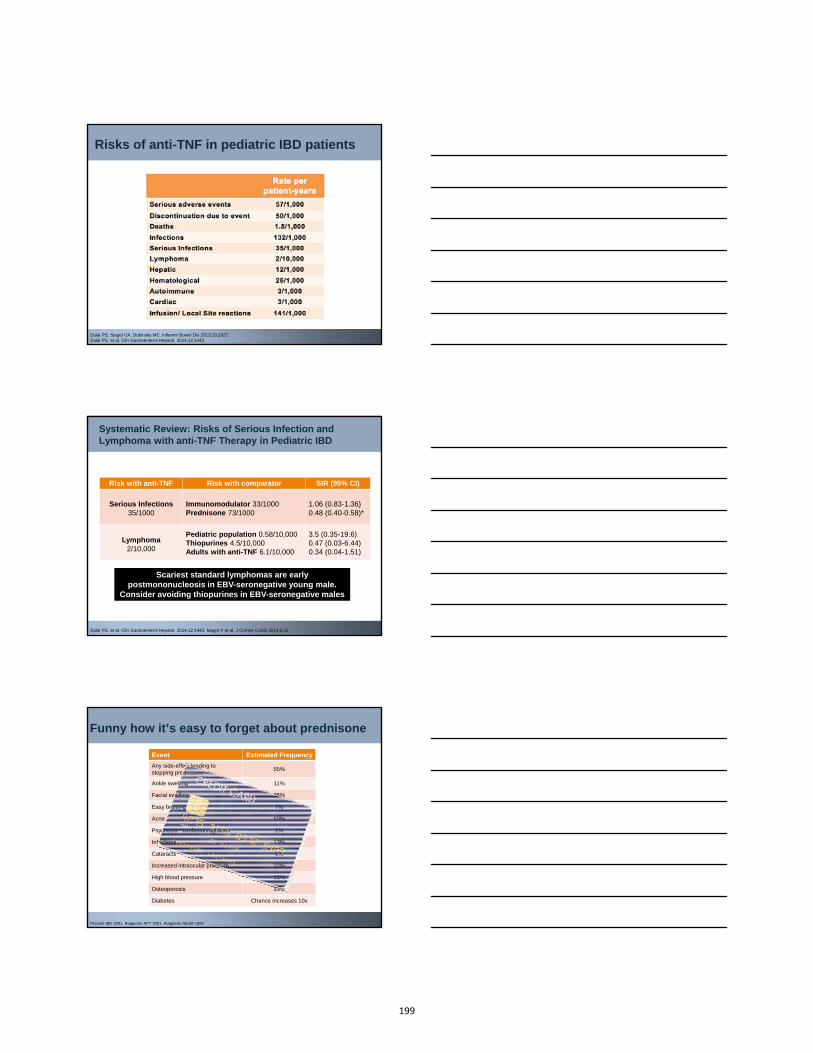
Risks of anti-TNF in pediatric IBD patients
Dulai PS, Siegel CA, Dubinsky MC. Inflamm Bowel Dis 2013:19:2927. Dulai PS, et al. Clin Gastroenterol Hepatol. 2014;12:1443.
Systematic Review: Risks of Serious Infection and Lymphoma with anti-TNF Therapy in Pediatric IBD
Risk with anti-TNF Risk with comparator SIR (95% CI)
Serious Infections35/1000
Immunomodulator 33/1000Prednisone 73/1000
1.06 (0.83-1.36)0.48 (0.40-0.58)*
Lymphoma2/10,000
Pediatric population 0.58/10,000Thiopurines 4.5/10,000Adults with anti-TNF 6.1/10,000
3.5 (0.35-19.6)0.47 (0.03-6.44)0.34 (0.04-1.51)
Dulai PS, et al. Clin Gastroenterol Hepatol. 2014;12:1443. Magro F et al. J Crohns Colitis 2014;8:31.
Scariest standard lymphomas are early postmononucleosis in EBV-seronegative young male.
Consider avoiding thiopurines in EBV-seronegative males
Funny how it’s easy to forget about prednisone
Event Estimated Frequency
Any side-effect leading to stopping prednisone
55%
Ankle swelling 11%
Facial swelling 35%
Easy bruising 7%
Acne 50%
Psychosis - confusion/agitation 1%
Infections 13%
Cataracts 9%
Increased intraocular pressure 22%
High blood pressure 13%
Osteoporosis 33%
Diabetes Chance increases 10x
Present IBD 2001, Rutgeerts APT 2001, Rutgeerts NEJM 1994
199
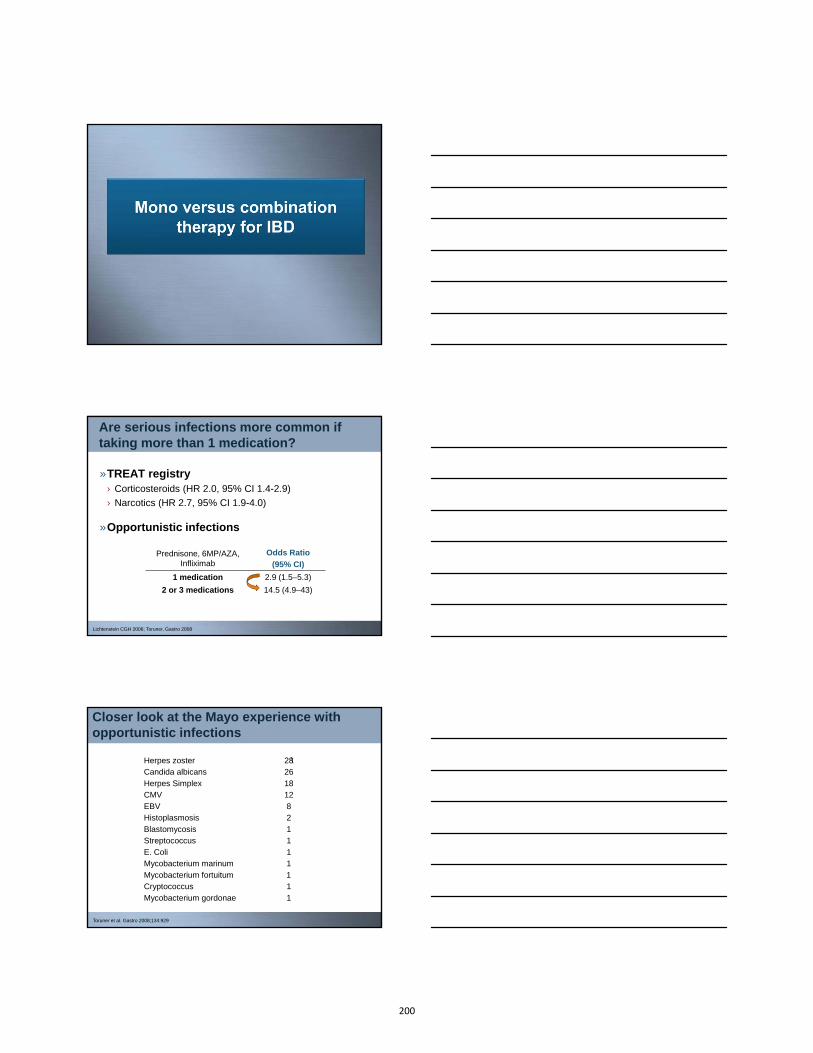
Are serious infections more common if taking more than 1 medication?
»TREAT registry› Corticosteroids (HR 2.0, 95% CI 1.4-2.9)
› Narcotics (HR 2.7, 95% CI 1.9-4.0)
»Opportunistic infections
Lichtenstein CGH 2006; Toruner, Gastro 2008
Prednisone, 6MP/AZA, Infliximab
Odds Ratio
(95% CI)
1 medication 2.9 (1.5–5.3)
2 or 3 medications 14.5 (4.9–43)
Closer look at the Mayo experience with opportunistic infections
Herpes zoster \Candida albicans
Herpes SimplexCMV
EBVHistoplasmosis
BlastomycosisStreptococcus
E. ColiMycobacterium marinum
Mycobacterium fortuitumCryptococcus
Mycobacterium gordonae
2826
1812
82
11
11
11
1
Toruner et al. Gastro 2008;134:929
200

Number of meds Cases Controls OR 0 38 129 1.0 (ref)
1 38 59 2.9 (1.5-5.3)2 or 3 24 12 14.5 (4.9-43)
Specific combinations
Corticosteroids alone 16 27 2.2 (1.0-4.9)6MP/AZA alone 20 31 3.4 (1.5-7.5)
IFX alone 3 2 11.1 (0.8-148) AZA/6MP + steroids 16 6 17.5 (4.5-68)
AZA/6MP + IFX 1 5 1.6 (0.1-19) AZA/6MP + IFX + steroids 5 0 1.1 (1.0-1.2)
Closer look at the Mayo experience with opportunistic infections
Toruner et al. Gastro 2008;134:929
COMMIT and SONIC Safety Results
AZA+ placebo(n=161)
IFX+ placebo(n=163)
IFX+ AZA
(n=179)
Total
(n=503)
Pts with 1 AE, n (%) 138 (85.7%) 139 (85.3%) 156 (87.2%) 433 (86.1%)
Pts with 1 SAE, n (%) 39 (24.2%) 26 (16.0%) 25 (14.0%) 90 (17.9%)
Serious infections 8 (5.0%) 4 (2.5%) 6 (3.4%) 18 (3.6%)
COMMIT
SONIC
Feagan et al. Digestive Disease Week, San Diego, CA 2008. Sandborn, WJ et al. ACG 2008
MTX (n=63
Placebo(n=63)
Blood and lymphatic system disorders 6.3% 11.1%
GI disorders 71.4% 76.2%
Infections 58.7% 61.9%
Connective tissue disorders 44.4% 38.1%
Respiratory disorders 20.6% 23.4%
012345678
0-2 >2 to 4 >4 to 6 >6 to 8 >8 to10
>10
Nu
mb
er o
f ca
ses
Years exposure prior to HSTCL
Anti-TNF + Thiopurine
0
1
2
3
4
5
6
0-2 >2 to 4 >4 to 6 >6 to 8 >8 to10
>10
Nu
mb
er
of
case
s
Years exposure prior to HSTCL
Thiopurine only
N=19 N=11
Kotlyar et al. Clin Gastroenterol Hepatol. 2011;9:36. Magro F et al. J Crohns Colitis 2014;8:31.
Risk of HSTCL is related to duration of thiopurine use
Estimated risk in “at risk” group with combo ≈ 1-3/10,000
Consider this: Even in young males Induce with our “best” therapy (thiopurine + anti-TNF) and stop thiopurine after 6-12
months when in deep remission
201

It’s not so easy!
Siegel, et al. DDW 2011.
Numbers are hard!
»Numeracy (quantitative literacy)
› ½ of patients were unable to convert:» 1% to 10 in 1000
› 80% of patients were unable to convert:» 1 in 1000 to 0.1%
› Patient have difficulty determining which is the higher risk: » 1 in 27 versus 1 in 37
Schwartz LM et al. Ann Intern Med. 1997;127(11):966-72.
Sheridan SL, Pignone M. Eff Clin Pract. 2002;5:35.
202
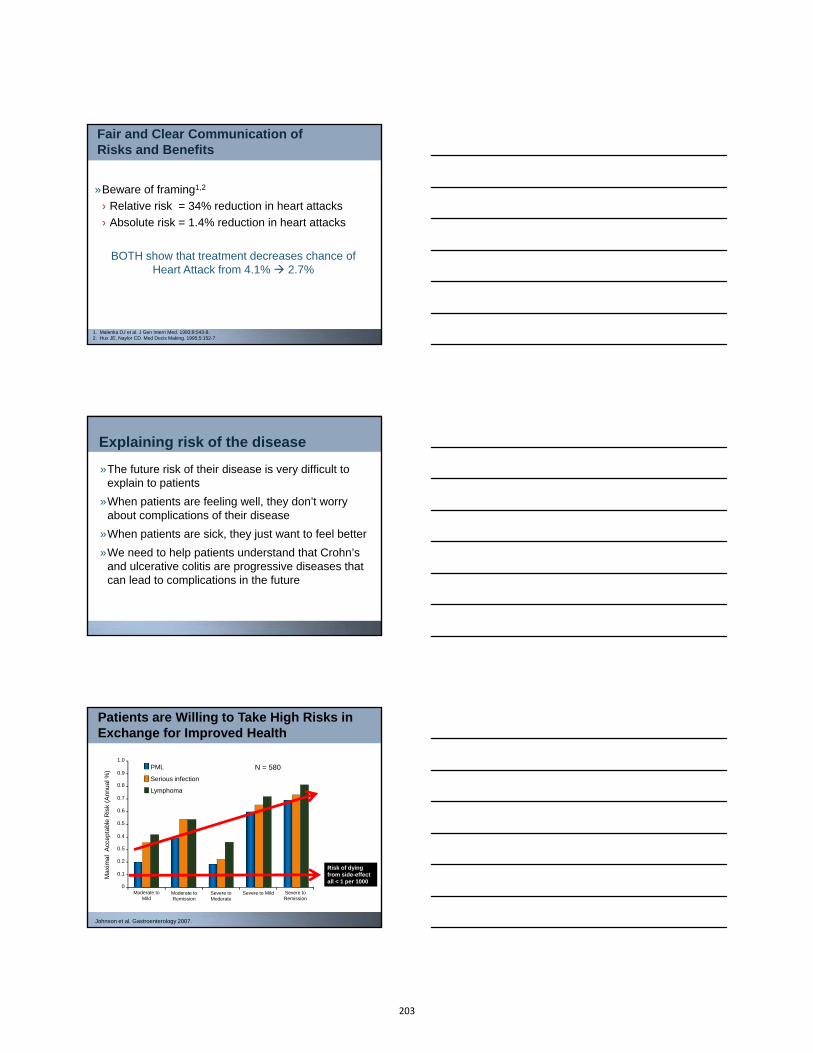
Fair and Clear Communication of Risks and Benefits
»Beware of framing1,2
› Relative risk = 34% reduction in heart attacks
› Absolute risk = 1.4% reduction in heart attacks
1. Malenka DJ et al. J Gen Intern Med. 1993;8:543-8.2. Hux JE, Naylor CD. Med Decis Making. 1995;5:152-7.
BOTH show that treatment decreases chance of Heart Attack from 4.1% 2.7%
Explaining risk of the disease
»The future risk of their disease is very difficult to explain to patients
»When patients are feeling well, they don’t worry about complications of their disease
»When patients are sick, they just want to feel better
»We need to help patients understand that Crohn’s and ulcerative colitis are progressive diseases that can lead to complications in the future
Ma
xim
al
Acc
ep
tab
le R
isk
(An
nu
al %
)
0
0.1
0.2
0.9
1.0
0.5
0.6
0.7
0.8
Moderate to Mild
Moderate to Remission
Severe to Mild Severe to Remission
Severe to Moderate
0.4
0.5
Patients are Willing to Take High Risks in Exchange for Improved Health
Johnson et al. Gastroenterology 2007.
Serious infection
Lymphoma
PML N = 580
Risk of dying from side-effect all < 1 per 1000
203

Parents are willing to take even higher risks of lymphoma…but only if their kids are sick!
0
0.2
0.4
0.6
0.8
1
1.2
Severe to Remission Moderate to Mild
Maximal Acceptable
Risk of Lymphoma
(%)
Adult patients
Parents
Johnson et al. Risk Analysis 2009
Crohn’s Disease Decision Aid Sample Clips
Benefits Risks Early Therapy
204

Ulcerative Colitis Decision Aid Video Sample Clips
Surgical Options for UC
Medical Therapy for UC
Option Gridshttp://www.optiongrid.co.uk/
Crohn’s Disease Treatments (Pediatrics)Use this grid to help you and your clinician decide on the best treatment for your disease
Frequently Asked Questions
ImmunomodulatorAzathioprine (Imuran, Azasan);
6-mercaptopurine (6MP, Purinethol), Methotrexate
Anti-TNFInfliximab (Remicade); Adalimumab (Humira);
Certolizumab pegol (Cimzia)
Combination Therapy
What type of medication is this?
An immunomodulator is a medicine that is taken to regulate or quiet down
the immune system which then decreases inflammation.
An anti-tumor necrosis factor (TNF) drug blocks one specific chemical (TNF) in the body. Blocking TNF
regulates or quiets down the immune system which then decreases
inflammation.
Using an immunomodulator and an anti-TNF drug together.
How is this treatment administered?
Daily, as a pill (azathioprine or 6MP), or weekly as a pill or shot
(methotrexate). It may take weeks to months to be fully effective, so your
doctor may prescribe a steroid, such as prednisone, to start.
Infliximab is given intravenously (injected into the vein) three times in the
first 6 weeks, then every 6-8 weeks. Adalimumab is given subcutaneously (injected under the skin) every other
week, and Certolizumab is given subcutaneously monthly. These
medications act faster than immunomodulators, so you likely won’t
need steroids.
Daily pills (or weekly shots if methotrexate) PLUS injections either
intravenous (into the vein) or subcutaneous (under the skin).
After 6 months of treatment, how many
people get relief of their symptoms and don’t need steroids (e.g.,
prednisone)?
There are no research studies in children directly comparing immunomodulators to anti-TNF drugs to combination therapy. But, we do have good estimates based on research in children and adults for each of these options.
Approximately 40 people out of 100 (40%).
Approximately 55 people out of 100 (55%).
Approximately 60 people out of 100 (60%).
What are some common, but short-lasting, side
effects?
Approximately 3 people out of 100 (3%) develop pancreatitis, where the
pancreas becomes inflamed and painful. Other short-term side-effects may include nausea, fever, fatigue,
lowering of the white blood cell count, or increase in liver tests.
Allergic reactions like a rash or shortness of breath from an infusion, or pain or swelling at the injection site can
occur.
With combination therapy, possible to get side effects from both
immunomodulators and anti-TNF drugs.
205

Crohn’s Disease Treatments (Pediatrics)Use this grid to help you and your clinician decide on the best treatment for your disease
Frequently Asked Questions
ImmunomodulatorAzathioprine (Imuran, Azasan);
6-mercaptopurine (6MP, Purinethol), Methotrexate
Anti-TNFInfliximab (Remicade); Adalimumab (Humira);
Certolizumab pegol (Cimzia)
Combination Therapy
How common are serious infections?
Approximately 3%-6% (between 3-6 people of out 100) experience serious infections for each treatment option.
How many people stop taking the medication because of side effects?
Approximately 10 out of 100 (10%).Approximately 6-7 people out of 100
(6%-7%).
If side-effects occur, it might be possible to stop one of the medications
and continue the other.
What is the risk of getting lymphoma
(lymph node cancer)?
Approximately 4 people out of 10,000(0.04%) for azathioprine and 6MP. It is not clear if methotrexate has any risk of lymphoma, but not enough
research has been done to prove this.
It is not clear that anti-TNF therapy on its own increases the risk of lymphoma at all, but not enough research has been
done to prove this.
There does not seem to be a meaningful increase in the risk of lymphoma if
adding an anti-TNF to an immunomodulator. The risk is
approximately 4 people of out 10,000 (0.04%)
What is the risk of getting lymphoma if not
taking these medications?
The risk of developing lymphoma in the general pediatric population is 0.0058% This is equal to approximately 0.58 per 10,000 or 5-6 people out of 100,000
What else should I know about the risks of these
treatments?
A rarer form of cancer is hepatosplenic T-cell lymphoma. We don’t know exactly how often it occurs, but it is very rare (less often than the type of lymphoma described above). It is seen mostly in young males. It is usually not treatable. This
lymphoma has occurred in people taking 6-MP or azathioprine by itself or as combination therapy with an anti-TNF drug. There have not been cases reported in Crohn’s disease with either methotrexate or anti-TNF therapy on its own.
For women, it is important to note that methotrexate cannot be taken when trying to become pregnant.
Summary
»Immunomodulators and biologics have real, measurable risks
»But the absolute risk is still very small
»Clearly communicating these data is hard!
»Shared decision making tools can make this easier
206


















