SYLLABUS - aagl.org 5_Syllabus.pdfCourse chairs, planning committee members, presenters, authors,...
19
Be a Surgical “Multiplier” in MIGS Inspire Brilliance Through Teamwork Scientific Program Chair Jubilee Brown, MD Honorary Chair Barbara S. Levy, MD President Marie Fidela R. Paraiso, MD SYLLABUS PLENARY 5 : Urogynecology
Transcript of SYLLABUS - aagl.org 5_Syllabus.pdfCourse chairs, planning committee members, presenters, authors,...

Be a Surgical “Multiplier” in MIGS Inspire Brilliance Through Teamwork
�
��
�
Scientific Program ChairJubilee Brown, MD
Honorary ChairBarbara S. Levy, MD
PresidentMarie Fidela R. Paraiso, MD
SYLLABUSPLENARY 5:
Urogynecology

Professional Education Information
Target Audience This educational activity is developed to meet the needs of surgical gynecologists in practice and in training, as well as other healthcare professionals in the field of gynecology.
Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
The AAGL designates this live activity for a maximum of 1.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Disclosure of Relevant Financial Relationships As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.
Anti-Harassment Statement AAGL encourages its members to interact with each other for the purposes of professional development and scholarly interchange so that all members may learn, network, and enjoy the company of colleagues in a professional atmosphere. Consequently, it is the policy of the AAGL to provide an environment free from all forms of discrimination, harassment, and retaliation to its members and guests at all regional educational meetings or courses, the annual global congress (i.e. annual meeting), and AAGL-hosted social events (AAGL sponsored activities). Every individual associated with the AAGL has a duty to maintain this environment free of harassment and intimidation.
AAGL encourages reporting all perceived incidents of harassment, discrimination, or retaliation. Any individual covered by this policy who believes that he or she has been subjected to such an inappropriate incident has two (2) options for reporting:
1. By toll free phone to AAGL’s confidential 3rd party hotline: (833) 995-AAGL (2245) during theAAGL Annual or Regional Meetings.
2. By email or phone to: The Executive Director, Linda Michels, at [email protected] or (714) 503-6200.
All persons who witness potential harassment, discrimination, or other harmful behavior during AAGL sponsored activities may report the incident and be proactive in helping to mitigate or avoid that harm and to alert appropriate authorities if someone is in imminent physical danger.
For more information or to view the policy please go to: https://www.aagl.org/wp-content/uploads/2018/02/AAGL-Anti-Harassment-Policy.pdf

Table of Contents Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 Total Laparoscopic Cerclage Sacrohysteropexy P.L. Rosenblatt .............................................................................................................................................. 3 Rectus Abdominis Pedicled Flap: An Innovative Robotic Approach R. Haverland .................................................................................................................................................. 4 Urethral Diverticulum Excision and Placement of Autologous Fascia Lata Sling D.A. Acosta .................................................................................................................................................... 5 Sacrohysteropexy with Anterior and Posterior Attachment A. Plair ........................................................................................................................................................... 6 Quality and Reliability of Publicly Accessible Information on Laser Treatments for Urinary Incontinence: What Is Available to Our Patients? C.J. Jolliffe ...................................................................................................................................................... 7 Non-puerperal Uterine Inversion Managed Robotically C. Jenny ......................................................................................................................................................... 8 A Prospective Randomized Control Trial Comparing Continuous Urinary Drainage to a Urinary Catheter Valve in Women Being Discharged with a Foley after Urogynecologic Surgery L. Dhariwal .................................................................................................................................................... 9 Occult Uterine Malignancy at the Time of Surgery for Pelvic Organ Prolapse: A Systematic Review E.R. Davenport ............................................................................................................................................ 12 Martius Labial Fat Pad Graft (Use in RVF Repair) D.A. Leach ................................................................................................................................................... 14 Robotic Assisted Excision of Obturator Mesh and Retropubic Urethropexy S. Boyd......................................................................................................................................................... 15 Cultural and Linguistics Competency ......................................................................................................... 16

Plenary 5: Urogynecology
Moderator: Carolyn C. Piszczek, Eun-Hee Yoo
Course Description This session presents a range of minimally invasive surgical techniques and provides long term data confirming the current management of different pelvic floor disorders.
Course Objectives Learning Objectives: At the conclusion of this session, the clinician will be able to: 1) Assess different minimally invasive surgical techniques to safely treat several pelvic floor conditions; 2) discuss diverse clinical approached to a wide range of urogynecological challenges.
11:00 Total Laparoscopic Cerclage Sacrohysteropexy Discussant: M.N. Wasson
P.L. Rosenblatt
11:10 Rectus Abdominis Pedicled Flap: An Innovative Robotic Approach Discussant: K. Keil
R. Haverland
11:20 Urethral Diverticulum Excision and Placement of Autologous Fascia Lata Sling Discussant: E.R. Sokol
D.A. Acosta
11:30 Sacrohysteropexy with Anterior and Posterior Attachment Discussant: M.V. Vargas
A. Plair
11:40 Quality and Reliability of Publicly Accessible Information on Laser Treatments for Urinary Incontinence: What Is Available to Our Patients? Discussant: S. Khalil
C.J. Jolliffe
11:50 Non-puerperal Uterine Inversion Managed Robotically Discussant: A.J. Park
C. Jenny
12:00 A Prospective Randomized Control Trial Comparing Continuous Urinary Drainage to a Urinary Catheter Valve in Women Being Discharged with a Foley after Urogynecologic Surgery Discussant: D. Bastawros
L. Dhariwal
12:10 Occult Uterine Malignancy at the Time of Surgery for Pelvic Organ Prolapse: A Systematic Review Discussant: T.B. McKinney
E.R. Davenport
12:20 Martius Labial Fat Pad Graft (Use in RVF Repair) Discussant: G.W. Cundiff
D.A. Leach
12:30 Robotic Assisted Excision of Obturator Mesh and Retropubic Urethropexy Discussant: S.J. Radtke
S. Boyd
Page 1

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop (listed in alphabetical order by last name). Art Arellano, Professional Education Director, AAGL* Linda D. Bradley, Medical Director, AAGL* Erin T. Carey Consultant: MedIQ Mark W. Dassel Contracted Research: Myovant Sciences Erica Dun* Adi Katz* Linda Michels, Executive Director, AAGL* Erinn M. Myers Speakers Bureau: Laborie Medical Technologies, Teleflex Medical Other: Unrestricted educational grant to support NC FPMRS Fellow Cadaver Lab: Boston Scientific Corp. Inc. Amy Park* Grace Phan, Professional Education Specialist, AAGL* Harold Y. Wu* Linda C. Yang Other: Ownership Interest: KLAAS LLC
SCIENTIFIC PROGRAM COMMITTEE Linda D. Bradley, Medical Director, AAGL* Jubilee Brown* Nichole Mahnert* Shanti Indira Mohling* Fariba Mohtashami Consultant: Hologic Marie Fidela R. Paraiso* Shailesh P. Puntambekar* Matthew T. Siedhoff Consultant: Applied Medical, Caldera Medical, CooperSurgical, Olympus Amanda C. Yunker Consultant: Olympus Linda Michels, Executive Director, AAGL*
FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Danilo A. Acosta* Dina Bastawros* Sarah Boyd* Geoffrey Cundiff* Erica R. Davenport* Laura Dhariwal* Rachael Haverland* Courtney Jenny* Courtney J. Jolliffe* Kristinell Keil* Susan Khalil* Douglas A. Leach* Timothy B. McKinney Consultant: Laborie Inc., Reddress Amy Park* Carolyn C. Piszczek* Andre Plair* Steven J. Radtke* Peter L. Rosenblatt Consultant: Boston Scientific Corp. Inc., Coloplast, CooperSurgical, Hologic, Medtronic, Tepha Contracted Research: Boston Scientific Corp. Inc. Stock Ownership: Pelvalon Other: Medical-legal defense: Bard Urological Division, Boston Scientific Corp. Inc., Ethicon Women's Health & Urology Eric R. Sokol Stock Ownership: Pelvalon Other: Grant funding to Stanford University: Acell, Coloplast, Cook MyoSite Other: Travel reimbursement: Contura Maria V. Vargas* Megan N. Wasson* Eun-Hee Yoo*
Content Reviewer has nothing to disclose.
Asterisk (*) denotes no financial relationships to disclose.
Page 2

Total Laparoscopic Cerclage Sacrohysteropexy
Presenter: Peter L. Rosenblatt, MD Mount Auburn Hospital
Cambridge, MA
Video Objective: There has been a growing interest among both patients and surgeons in preserving the uterus during the treatment of pelvic organ prolapse. In this video we are demonstrating a novel surgical approach towards the treatment of pelvic organ prolapse. This surgical procedure simplifies the laparoscopic sacrohysteropexy procedure by significantly reducing endoscopic suturing and knot tying, without the need for a combined laparoscopic and vaginal surgical approach.
Setting: A 69 -year-old G2P2 Caucasian female suffering from stage II pelvic organ prolapse. Her POP-Q was notable for anterior and apical prolapse to the level of the hymen. The laparoscopic cerclage sacrohysteropexy was initiated following a bilateral salpingo-oophorectomy and completed entirely from the laparoscopic approach.
Interventions: Laparoscopic cerclage sacrohysteropexy.
Conclusion: This case demonstrates that a laparoscopic cerclage sacrohysteropexy is an efficient, simple, and time saving surgical option for women with pelvic organ prolapse.
Page 3

Rectus Abdominis Pedicled Flap: An Innovative Robotic Approach
Presenter: Rachael Haverland, MD Mayo Clinic Arizona
Phoenix, AZ
Video Objective: To provide education on the utility of rectus muscle flap during pelvic floor reconstruction and describe in detail a minimally invasive technique to avoid laparotomy.
Setting: Patients requiring pelvic floor reconstruction at an academic medical center
Interventions: The rectus abdominis muscle flap can be used as a workhorse flap for pelvic reconstruction, providing a large volume of well vascularized soft tissue that can be used in treatment of complex pelvic floor reconstruction, including genital fistulas, post-radiation pelvic exenteration and abdominoperineal resection defects. Intraperitoneal harvest of the rectus muscle using a robotic approach allows avoidance of laparotomy and subsequent disruption of the anterior rectus sheath, thus preserving the integrity of the abdominal wall. This educational video demonstrates robotic docking as well as surgical techniques in detail to show the feasibility for robotic-assisted rectus flap harvest and pelvic floor reconstruction.
Conclusion: Robotic-assisted rectus abdominis flap harvest for pelvic floor reconstruction is a reliable means of defect closure. This novel approach is surgically feasible for the reconstructive surgeon and maintenance of minimally invasive technique allows for significant advantages over the traditional laparotomy approach.
Page 4

Urethral Diverticulum Excision and Placement of Autologous Fascia Lata Sling
Presenter: Danilo A. Acosta, MD Minimally Invasive Gynecology Surgery Department, Maimonides Medical Center
Brooklyn, NY
Video Objective: To show the repair of an uncommon urogynecological pathology, and to illustrate a case where an autologous fascial graft is placed for management of stress urinary incontinence.
Setting: The patient is a 59-year-old with abdominal pain, urinary incontinence, incomplete bladder emptying, and hematuria. She has a complex past medical and surgical history. Pre-operative urodynamic testing showed genuine stress urinary incontinence, and office cystoscopy was unremarkable. Imaging demonstrated a urethral diverticulum containing multiple stones. The patient proceeded to the operating room for excision of the diverticulum and placement of an autologous sling.
Interventions: Fascia lata from patient’s right thigh was harvested and prepared with polypropylene sutures at each end. Cystourethroscopy identified the diverticulum opening in the posterior mid urethra. The anterior vaginal mucosa was incised and the pubocervical fascia was dissected. The bulge of the urethral diverticulum was identified. Entry into the diverticulum was encountered during the dissection, and multiple stones were removed. The entire diverticular sac was dissected from the posterior urethra and pubocervical fascia. The urethral wall was reapproximated. The periurethral fibromuscularis was closed in a vest-over-pants fashion in order to avoid overlapping suture line with the urethral closure. An abdominal incision was made above the pubic symphysis. Needle trocars were passed vaginally through retropubic space. The polypropylene stitches on the fascial lata graft were threaded through the needles and pulled onto the abdomen, placing the sling in place. The sutures were then sewn through the rectus fascia and tied in the midline. Final cystourethroscopy confirmed patent ureteral orifices, normal bladder mucosa, and intact urethral repair. A Foley catheter was replaced and maintained for 4 weeks. A voiding cystogram showed intact bladder and urethra.
Conclusion: This case depicts a scenario where autologous sling is preferable over synthetic mesh due to decreased risk of erosion when a urethral diverticulum is repaired.
Page 5

Sacrohysteropexy with Anterior and Posterior Attachment
Presenter: Andre Plair, MD Female Pelvic Medicine and Reconstructive Surgery, Wake Forest Baptist Health
Winston Salem, NC
Video Objective: This video discusses patient selection, different surgical approaches, and outcomes data for sacrohysteropexy. We present a case presentation employing one of the approaches to sacrohysteropexy.
Setting: This video presents a case of a 40 year old female with Stage II uterovaginal prolapse who seeks a durable surgical repair. She does not desire future fertility and has risk factors for native tissue repair failure.
Interventions: The patient underwent a robotic-assisted laparoscopic sacrohysteropexy, bilateral salpingectomy, and posterior colporrhaphy.
Conclusion: Sacrohysteropexy is an effective and appropriate surgery for patients with uterovaginal prolapse and risk factors for native tissue failure who do not want a hysterectomy. Sacrohysteropexy can be performed with a posterior vaginal attachment only or with posterior and anterior vaginal attachments. The posterior only attachment is best for patients who may desire future fertility as it does not involve surgery into the broad ligament or anterior cul-de-sac. There are two approaches to sacrohysteropexy that also include an anterior attachment to provide anterior vaginal support. Both approaches bring anterolateral mesh arms through windows created in the broad ligament. One technique sutures these arms in addition to the posterior mesh’s sacral arm to the sacral promontory. The other technique sutures the lateral arms to the posterior cervix leaving only the posterior mesh sacral arm to be attached at the sacral promontory. Overall sacrohysteropexy has been shown to have a symptomatic success rate of 90-95% and an anatomical success rate of 70%. Sacrohysteropexy has been shown to have reduced operative time, blood loss, hospital stay length, and to have greater vaginal length preservation than its hysterectomy with sacrocolpopexy alternative.
Page 6

Quality and Reliability of Publicly Accessible Information on Laser Treatments for Urinary Incontinence: What Is Available to Our Patients?
Presenter: Courtney J. Jolliffe, MD
Division of Urogynecology, Department of Obstetrics and Gynecology, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, ON, Canada
Study Objective: This study aims to determine the quality and reliability of the top 20 internet search results for laser vaginal treatment of urinary incontinence in women. Design: Website review Setting: n/a Patients or Participants: n/a Interventions: The phrases “laser treatment of urinary incontinence” and “vaginal laser therapy for urinary incontinence” were searched in the most popular search engine (Google) and the top 20 search results (as of August 2018) were analysed by 2 medical students, 2 clinical fellows and 3 urogynecologists. The quality, credibility and transparency of information was determined using the HONcode, JAMA Benchmarks and DISCERN tool. Readability was determined using the Flesch-Kincaid grade level and automated readability index. Measurements and Main Results: The 20 sites evaluated had an average HON reliability score of 35.0% (± 14.2%) and an average DISCERN scores of 40.4 (± 7.7)/80 or 51%, indicating a lack of credibility and transparency. None of the sites analyzed fulfilled all 4 JAMA Benchmark criteria (Authorship, Attribution, Disclosure, Currency). The average grade level was determined to be 13.9 (± 2.8) and 14.1(± 3.1) by the Flesch-Kincaid grade level and automated readability index respectively. This is consistent with a high school to college graduate level. Conclusion: This study indicates that there is a lack of reliable, high quality information available to patients on the topic of laser treatment for urinary incontinence. The information is presented such that it might be difficult for patients to understand as the grade level indicates a high level of difficulty meant for skilled readers. The available information is not geared towards informing patients about the therapies, but rather focuses on the recruitment of patients to practices, often leaving out important information in the process. Patients should be made aware of the short-comings of current available resources and use caution when reading potentially low-quality information on this topic online.
Page 7

Non-puerperal Uterine Inversion Managed Robotically
Presenter: Courtney Jenny, MD Department of Obstetrics and Gynecology, University of Tennessee Medical Center
Knoxville, TN
Video Objective: To demonstrate a method for surgical correction of chronic non-puerperal uterine inversion. Setting: Patient with chronic non-puerperal uterine inversion of unknown duration, symptomatic for 3 months. She was referred to Urogynecology at a tertiary referral center for presumed pelvic organ prolapse. Interventions: Surgical video demonstration of robotic assisted total laparoscopic hysterectomy and bilateral salpingo-oophorectomy in the setting of complete uterine inversion. Conclusion: We found that the chronic nature of this patient's uterine inversion precluded reduction with traditional methods. We demonstrate additional surgical techniques that may be used to ensure safe dissection of pelvic anatomy.
Page 8

A PROSPECTIVE RANDOMIZED CONTROLLED TRIAL COMPARING CONTINUOUS URINARY DRAINAGE TO A
URINARY CATHETER VALVE IN WOMEN BEING DISCHARGED WITH A FOLEY AFTER UROGYNECOLOGIC SURGERY
Laura Dhariwal, MD, FPMRS Fellow
Disclosure
I have no financial relationships to disclose.
Objectives
● Compare UTI rates associated with a continuous urinary drainage bag to a urinary catheter valve after urogynecologic surgery
● Compare patient satisfaction with continuous drainage bag versus cathetervalve
● Compare number of days to spontaneous void
Background
● Urinary tract infection rates range from 11-40% after urogynecologic surgery● Risk is further increased by incomplete bladder emptying and transurethral
catheterization ● 25% of women have transient urinary dysfunction after urogynecologic
surgery● Indwelling catheters due to postoperative voiding dysfunction significantly
reduces patient satisfaction
Methods
● Non-inferiority prospective randomized controlled trial ○ June 2016-June 2019
● Inclusion criteria:
○ Women being discharged home with an indwelling urinary catheter after prolapse or anti-incontinence surgery
● Exclusion criteria:
○ Intra-operative complication requiring continuous bladder drainage
○ Dementia/altered cognitive function
Outcome Measures
● Primary outcome: number of UTIs within 30 days after surgery
○ UTIs defined as:
■ Catheterized culture sample with > 1,000 colonies bacteria/mL or
■ Empiric treatment for UTI per CDC guidelines up to 4 weeks post-operative
○ Cultures obtained via catheterized specimen at:
■ First outpatient visit after failed voiding trial (post-operative days 2-7)
■ First post-operative visit (post-operative weeks 2-4)
● Secondary outcomes: patient satisfaction and number of days to spontaneous void
○ Subjects completed a 5-question Foley satisfaction questionnaire
Page 9

Results
100 women met criteria
2 spontaneously voided after
randomization
1 withdrew
97 included in final
analysis
51 women 46 women
Demographic Details
Continuous Drainage Bag (n=51)
Urinary Catheter Valve(n=46)
p-value
Age, mean (SD) 67.18 (11.56) 64 (11.9) 0.187
Caucasian Race, n (%) 42 (82.353%) 40 (86.957%) 0.585
BMI, mean (SD) 26.8 (4.8) 26.1 (4.6) 0.498
Menopausal, n (%) 43 (84%) 37 (80.4%) 0.616
Gravity, median (Q1,Q3) 3 (2-4) 2 (2-3) 0.223
Parity, median (Q1,Q3) 2 (2-3) 2 (2-3) 0.558
Operative DetailsContinuous Drainage Bag
n=51Urinary Catheter Valve
n=46p-value
Vaginal hysterectomy, n (%) 22 (43) 16 (35) 0.485
Laparoscopy hysterectomy, n (%) 11 (21) 7 (15) 0.482
Apical suspension – laparoscopic approach, n (%)
10 (20) 8 (17) 0.526
Apical suspension – vaginal approach, n (%)9 (18) 11 (23) 0.421
Obliterative procedure, n (%) 16 (31) 12 (26) 0.596
Anterior repair, n (%) 29 (57) 23 (50) 0.499
Posterior repair, n (%) 32 (63) 25 (54) 0.402
Sling, n (%) 33 (65) 36 (78) 0.141
EBL, mean (SD) 130.3 (12.1) 127.1 (14.4) 0.865
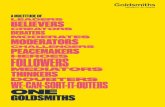
Primary Outcome
Continuous drainage bag
Urinary catheter valve p-value
n=51 n=46
UTI rate, n (%) 17/51 (33.33%) 15/46 (32.61%) >0.999
Secondary Outcomes
Continuous drainage
bag
Urinary catheter valve
p-value
Days to spontaneous void, mean (SD) 4.86 (2.14)4.37 (2.27)
0.276
Questionnaire score, median (min-max) 46, (0-19) 44, (0-12) <0.001
• Do you feel embarrassed to have the catheter in place? 1 (0-4) 0 (0-4) 0.008
• How much difficulty did you experience manipulating or using the catheter?
1 (0-4) 0 (0-2) 0.003
• Were you bothered while performing your daily activities (Cleaning, laundry, exercising, driving, riding in care, showering etc…) with the catheter in place?
2 (0-4) 0 (0-4) <0.001
• Was it difficult to walk around with the catheter in place? 1 (0-4) 0 (0-3) 0.001
• Was it painful or uncomfortable to have the catheter in place?
2 (0-4) 0.5 (0-3) <0.001
Conclusion
● Strengths
○ Randomized controlled trial
○ Large number of subjects
● Limitations
○ Secondary outcomes were not powered
○ Non-validated questionnaire
Page 10

Conclusion
● Rates of urinary tract infections and number days to spontaneous void were similar in both groups.
● The urinary catheter valve is a convenient alternative to a continuous urinary drainage bag with higher patient satisfaction.
Acknowledgments
● Charbel Salamon, MD, FPMRS Fellowship and Division Director
References
● Albo ME, et al. Burch colposuspension versus fascial sling to reduce urinary stress incontinence. N Engl J Med, 2007 356:2143–2155
● FitzGerald M, et al. Pelvic support, pelvic symptoms, and patient satisfaction after colpocleisis. Int Urogynecol J, 2008 19:1603–1609
● Mutone N, et al. Factors that influence voiding function after the tension-free vaginal tape procedure for stress urinary incontinence. Am J Obstet Gynecol. 2003 188:1477–1483
Page 11

Erica Davenport, MD Minimally Invasive Gynecologic Surgery Fellow
Las Vegas Minimally Invasive Surgery/University of Nevada Las Vegas School of Medicine
OOccult Uterine Malignancy at the time of Surgery for Pelvic Organ Prolapse:A Systematic Review
Disclosures
I have no financial relationships to disclose.
Objective
At the conclusion of this activity, the participant will be able to recognize the characteristics of occult uterine malignancy and to
understand its prevalence among the population of women undergoing surgery for pelvic organ prolapse.
Background
• Pelvic organ prolapse (POP) is a benign condition that commonlyoccurs in women once child bearing years are complete.
• It is estimated that the number of surgical cases to treat prolapse isprojected to grow from 166,000 in 2010 to 245,970 in 2050 1
• The risk of occult malignancy is unclear at the time of hysterectomy forPOP.
Objective
• The primary aim of this study was to conduct a systematic review andmeta-analysis to estimate the prevalence of occult malignancy of anysubtype, specifically at the time of hysterectomy, for POP.
• Our ultimate goal is to provide surgeons who perform hysterectomy forPOP with robust evidence-based data for preoperative counseling.
Methods
• The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed in this systematicreview.
• We did not restrict articles based on language.
• We narrowed articles down based on whether they included dataon occult malignancy at time of hysterectomy specifically for pelvicorgan prolapse.
Page 12

Results
The search terms used were“occult malignancy” or
“occult uterine pathology”, paired with “morcellation” or “hysterectomy”.
Cut off date= March 25 2019
Pooled estimate= 0.22%
Discussion
• This is the first attempt, that we are aware of, to synthesize data on occult uterine malignancies among women specifically undergoing hysterectomy for pelvic organ prolapse.
• IIn this meta-analysis we found that the pooled prevalence of occult uterine malignancy at the time of hysterectomy for POP was 0.22%.
• The prevalence in the overall group of studies showed little heterogeneity and suggests that the overall pooled prevalence is an appropriate estimate.
Conclusion/Future Considerations
• In light of this data: Is it cost effective or beneficial to obtain an endometrial biopsy or preoperative workup for women with pelvic organ prolapse prior to surgical intervention?
• Additional research should focus on creating an algorithm or risk stratification for women undergoing a hysterectomy for pelvic organ prolapse.
• This will assist surgeons with determining which patients deserve preoperative evaluation for uterine cancer.
• Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstet Gynecol2009;114:1278-83.
• Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979-1997. Am J Obstet Gynecol 2003;188:108-15.
• Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 1997;89:501-6.
• Desai VB, Wright JD, Gross CP, et al. Prevalence, characteristics, and risk factors of occult uterine cancer in presumed benign hysterectomy. Am J Obstet Gynecol 2019;221:39 e1- e14.
References
LLead author: Erica Davenport, M.D. (MIGS Fellow, LVMIS/UNLV)
Faculty mentor: David Howard, M.D., Ph.D. (Director of Research, FMIGS
program, LVMIS/UNLV)
Lucas James B.S (UNLV School of Medicine)
Jasmine Hankey (OB-STATS Inc, Provided editorial assistance)
Elite Research Network (Conducted the meta-analysis)
UNLV Graduate and Professional Student Association (For funding and
travel for Lucas James)
Acknowledgments
Page 13

Martius Labial Fat Pad Graft (Use in RVF Repair)
Presenter: Douglas A. Leach, MD Division of Urogynecology, Mayo Clinic, Rochester, MN
Video Objective: To demonstrate the utility of the Martius Labial Fat Pad Graft in pelvic fistula repair.
Setting: We present a minimally invasive surgical approach for a patient with recurrent rectovaginal fistula.
Interventions: An incision is made over the labium majus exposing the yellow fibrofatty graft. This graft is first retracted medially where a natural tissue plane facilitates dissection from the adjacent labium majus. It is then retracted laterally where a plane between it and the bulbocavernosus muscle is developed. To avoid devascularization of adjacent skin, a thin fatty layer is left attached at its undersurface.
The division of the flap is begun in this case, at its anterior pedicle. It is important to develop a flap that easily covers the defect with a good degree of overlap.
Once the flap has been sufficiently mobilized, a shellcross is used to create the subepithelial defect to enable passage of the flap through the levator plate. This defect is widened enough to prevent compression on the pedicled blood supply.
After appropriate positioning, the flap is sewn into place by attaching it to the adjacent, underlying rectovaginal fascia with interrupted 2-0 Vicryl suture. It is important to note that no tensioning of the flap is required to approximate it to the adjacent tissue. The posterior vaginal wall is next closed over the graft in two layers followed by closure of the labial defect.
Conclusion: The Martius flap has multiple minimally invasive advantages in fistula repair to include low morbidity, lack of a cosmetic defect and the need for only a single surgical field. Its’ abundant blood supply promotes rapid neovascularization of the transplanted graft and lends itself well to a variety of surgical modifications that can be utilized in the repair of even the most difficult of fistulas.
Page 14

Robotic Assisted Excision of Obturator Mesh and Retropubic Urethropexy
Presenter: Sarah Boyd, MD Obstetrics and Gynecology, University of Tennessee, College of Medicine
Chattanooga, TN
Video Objective: To showcase a new approach to treatment of chronic pelvic pain after transobturator mesh placement
Setting: A community based academic institution
Interventions: A robotic approach to an excision of transobturator mesh causing chronic pelvic pain and a robotic retropubic urethropexy for stress urinary incontinence
Conclusion: Robotic technology can be used in combination to a vaginal approach to explore the obturator space and removed improperly placed mesh in appropriate candidates. While performing this procedure, it is also possible to perform a robotic urethropexy in patients with persistent stress urinary incontinence symptoms
Page 15

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
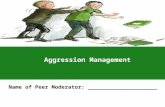
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
Page 16