
Swallowing Difficulty & Pain Tim Farrell, MD Tom Egan, MD.
88
Swallowing Difficulty & Pain Tim Farrell, MD Tom Egan, MD
-
Upload
james-hancock -
Category
Documents
-
view
215 -
download
0
Transcript of Swallowing Difficulty & Pain Tim Farrell, MD Tom Egan, MD.

Swallowing Difficulty & Pain
Tim Farrell, MD
Tom Egan, MD
Assumptions
• Students understand the anatomy,
physiology, and pathophysiology of
the swallowing mechanism and the
esophagogastric junction.

Objectives
Students will understand:
• Differential diagnosis for a patient with dysphagia. • Symptoms and treatment of GERD. • Pathophysiology and treatment of achalasia and diffuse
esophageal spasm. • Etiology and treatment of esophageal diverticula.• Common symptoms and management of hiatal hernias.• Management of adenocarcinoma of the E-G junction. • Presenting symptoms, etiology and treatment of
esophageal rupture.

Case 1
• An 80-year-old man presents with a trouble swallowing for a year. He regurgitates after meals, has heartburn, but no other pain and is in good health otherwise.
• He is thin, without neck mass. His chest is clear and his abdomen is soft and without masses.
Case 1
• What is the differential diagnosis?
AnatomicTumor, Stricture, Compression, Foreign
BodyFunctional
GERDMotility Disorder (achalasia, scleroderma)Neurologic (Parkinson’s, bulbar paralysis)
PsychologicalGlobus Hystericus

Case 1
• What test should be done, in what order, and why?
Anatomic Assessment Functional Assessment
Upper GI Series 24-hr pH
EGD Esophageal Manometry
Biopsy GES

GERD - Definition
Protracted exposure of the esophageal lining to stomach juice
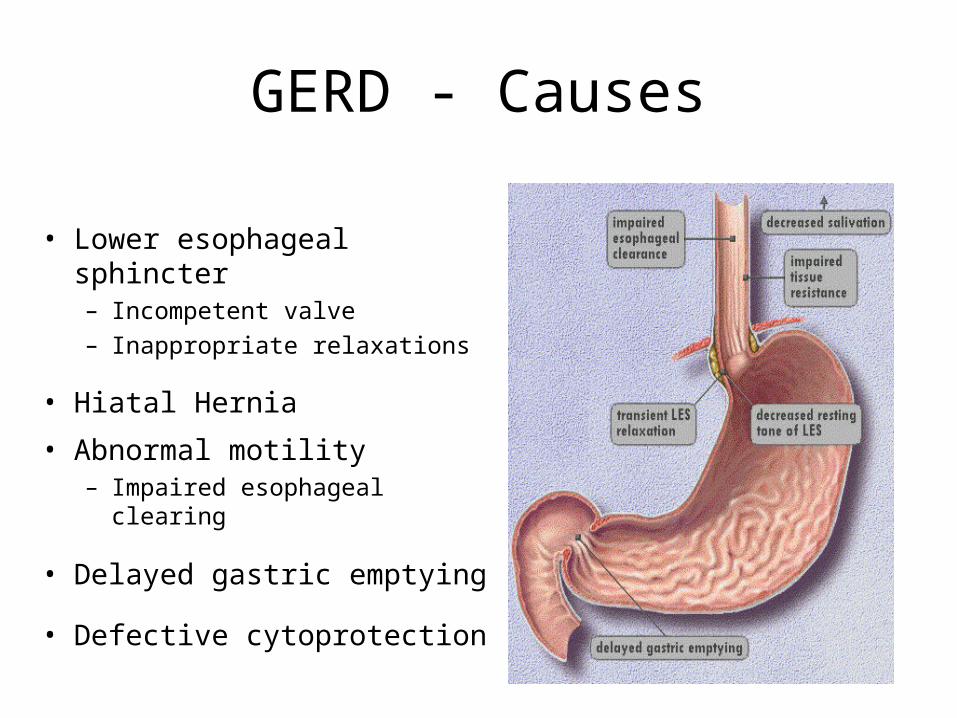
GERD - Causes
• Lower esophageal sphincter– Incompetent valve– Inappropriate relaxations
• Hiatal Hernia
• Abnormal motility– Impaired esophageal clearing
• Delayed gastric emptying
• Defective cytoprotection

GERD - Symptoms
Atypical Symptoms
Asthma
Cough
Hoarseness
Chest Pain
Typical Symptoms
Heartburn
Regurgitation
Trouble Swallowing

GERD - Complications
• Peptic Stricture
• Esophagitis / Ulcers
• Barrett's Esophagus

Indications for further Dx-Rx
• Persistent or frequent symptoms
• Dysphagia
• Frequent vomiting
• Early satiety
• Weight loss
• Significant respiratory complaints
• Age < 45

GERD - Diagnosis
• Barium Swallow
• Upper Endoscopy
• Esophageal Manometry
• 24-Hour Ambulatory
Esophageal pH
• Gastric Emptying Study

GERD - DiagnosisBarium Swallow

GERD - DiagnosisUpper Endoscopy

GERD - DiagnosisManometry

GERD - Treatment
• Environmental• Medical - OTC
– Antacids– H2-Blockers
• Medical -Prescription– Proton-Pump
Inhibitors
• Endoscopic• Surgical
– Fundoplication

Dietary Modifications
• Avoid large meals
• Limit foods which decrease LES pressure– Fatty foods, chocolate, mints, and alcohol
• Avoid irritating foods and beverages– Citrus, tomatoes, pepper, etc.
• Limit caffeine and carbonated beverages – Increases acid production– Increased gastric distension
• Candy or gum to increase saliva– Alkaline saliva neutralizes acid– Increases motility and clearance

Lifestyle Modifications
• Weight Loss
• Avoid smoking– Decreases LES pressure
• Avoid lying down for 2-3 hours after meals– Limits supine reflux
• Sleep with elevated head of bed– Improves esophageal clearance

Medications Worsening Reflux
– Calcium channel blockers – Anticholinergics – Theophylline– Progesterone
– β2-antagonists, α-antagonists
– Nitrates– Meperidine– Diazepam

GERD - Medical Treatment
Medications may be used to:
• Neutralize acid
• Increase LES tone
• Improve gastric emptying

OTC H2 Blockers
• Lower-dose formulations
• Acute treatment or prophylaxis
• Slower onset than antacids
• Longer duration of acid inhibition

Proton Pump Inhibitors

Endoscopic Treatment Modalities Thermal (Stretta®)
Thermal energy Mechanical / Neural
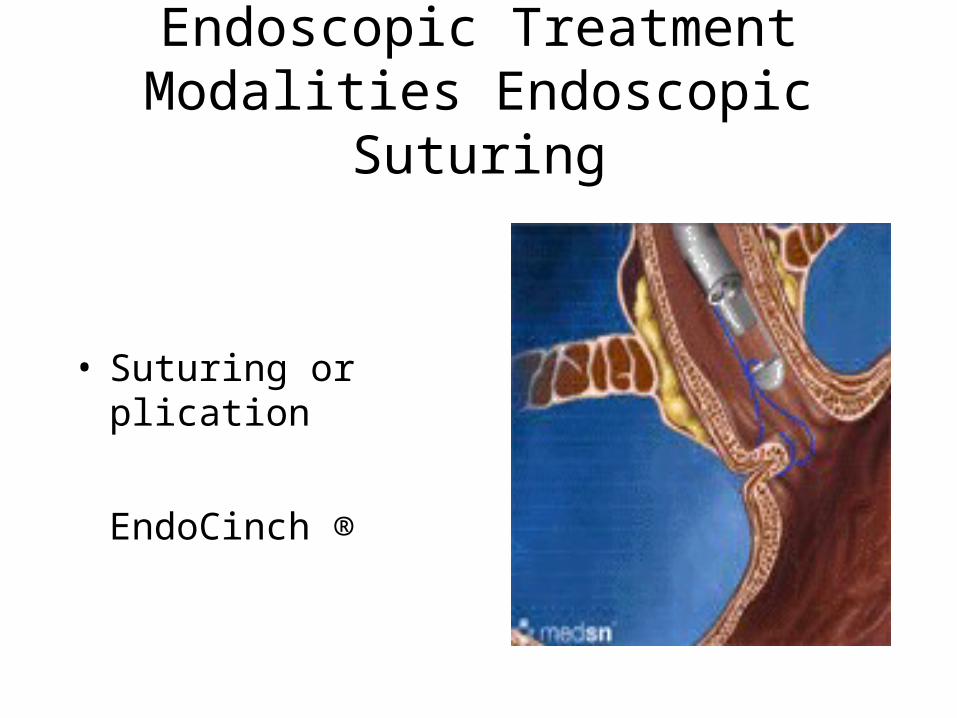
Endoscopic Treatment Modalities Endoscopic Suturing
• Suturing or plication
EndoCinch ®

Endoscopic Treatment ModalitiesBiocompatible Material
Enteryx ®

GERD - Surgical Treatment

GERD - Surgical Treatment

Nissen FundoplicationTechnique

Nissen FundoplicationTechnique

Nissen FundoplicationTechnique

Nissen FundoplicationTechnique

Nissen FundoplicationTechnique

Nissen FundoplicationTechnique

Nissen FundoplicationTechnique

GERD - Surgical TreatmentResults
• Procedure - 2 Hours
• Hospital - 1-2 Days
• Full Activity - 2 weeks
• Full Diet - 3 weeks
• Need to Open <1%
• Need for Blood <1%
• Off Medications - 95%
• Off Steroids - 50%
• Need 2nd Procedure - 5%
Effects of Fundoplication
Fundoplication
– augments LES resting pressure
– lessens frequency of transient LES relaxations
– reestablishes anatomy of the LES and crura
– may improve esophageal clearance
– may improve gastric emptying

Case 2
• A 61-year-old man presents with progressive difficulty swallowing. He has history of indigestion and heartburn. Until 12 months ago, food would come up into his throat when he was supine, with a sour taste and sometimes a cough. About 12 months ago, these symptoms improved but he developed progressive dysphagia.
• He smokes 1 PPD and drinks two beers at dinner.
• Exam is unremarkable except for barrel chest.

Case 2
• What is the differential diagnosis?
AnatomicTumor, Stricture, Compression, Foreign Body
FunctionalGERD, Motility Disorder (achalasia, scleroderma)Neurologic (Parkinson’s, bulbar paralysis)
PsychologicalGlobus Hystericus

Case 2
• How would you evaluate this patient?
Anatomic Assessment Functional Assessment
Upper GI Series 24-hr pH
EGD Esophageal Manometry
Biopsy GES

Case 2
• What are the treatment options for benign esophageal stricture?
• Medications• Endoscopic Dilation• Surgery

Case 2
• What are the treatment options for carcinoma of the esophagus?
– Esophagogastectomy• Ivor-Lewis• Transhiatal

Barrett’s EsophagusEpidemiology
• Affects 10% of patients with severe GER
• 40-fold increased risk of cancer
• Patients require endoscopic surveillance
• Esophagectomy for severe dysplasia/cancer

Barrett’s EsophagusEndoscopic Appearance
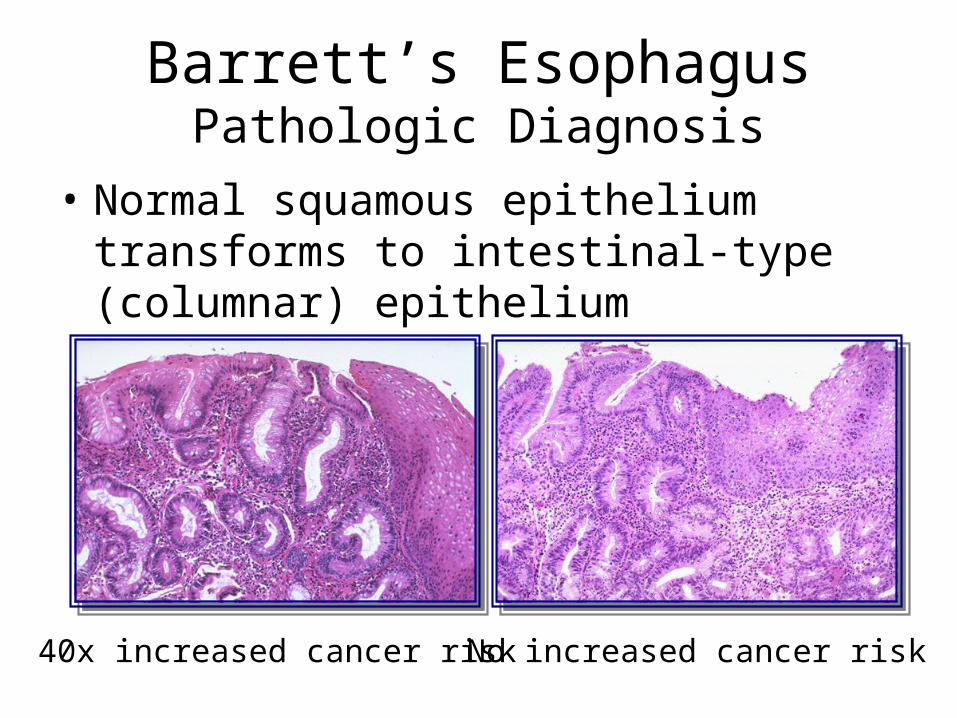
Barrett’s EsophagusPathologic Diagnosis
• Normal squamous epithelium transforms to intestinal-type (columnar) epithelium
40x increased cancer risk No increased cancer risk
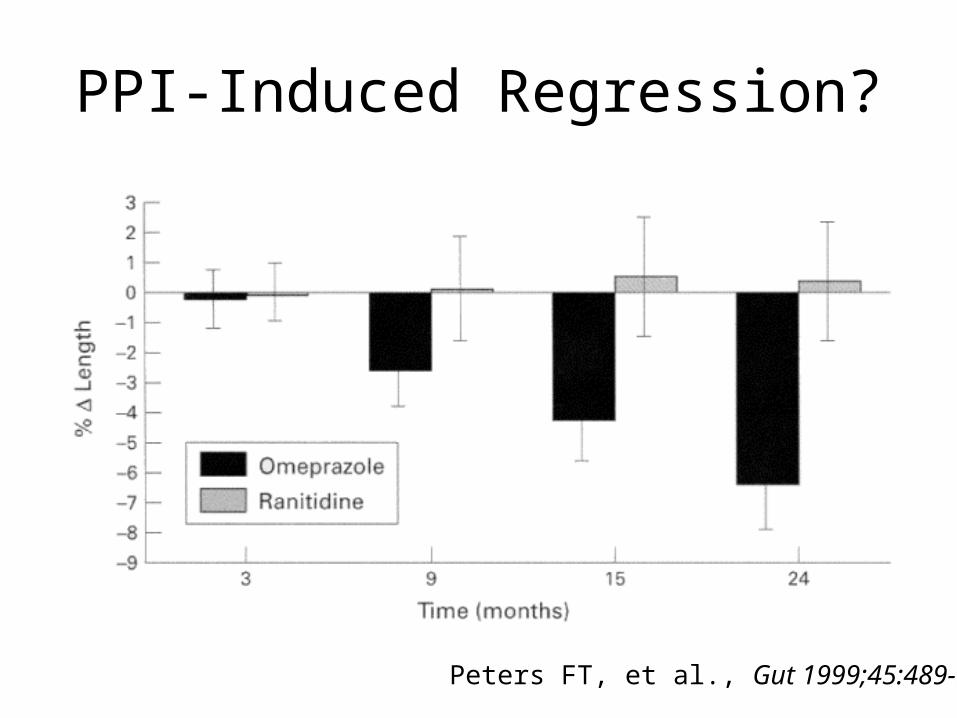
PPI-Induced Regression?
Peters FT, et al., Gut 1999;45:489-94.
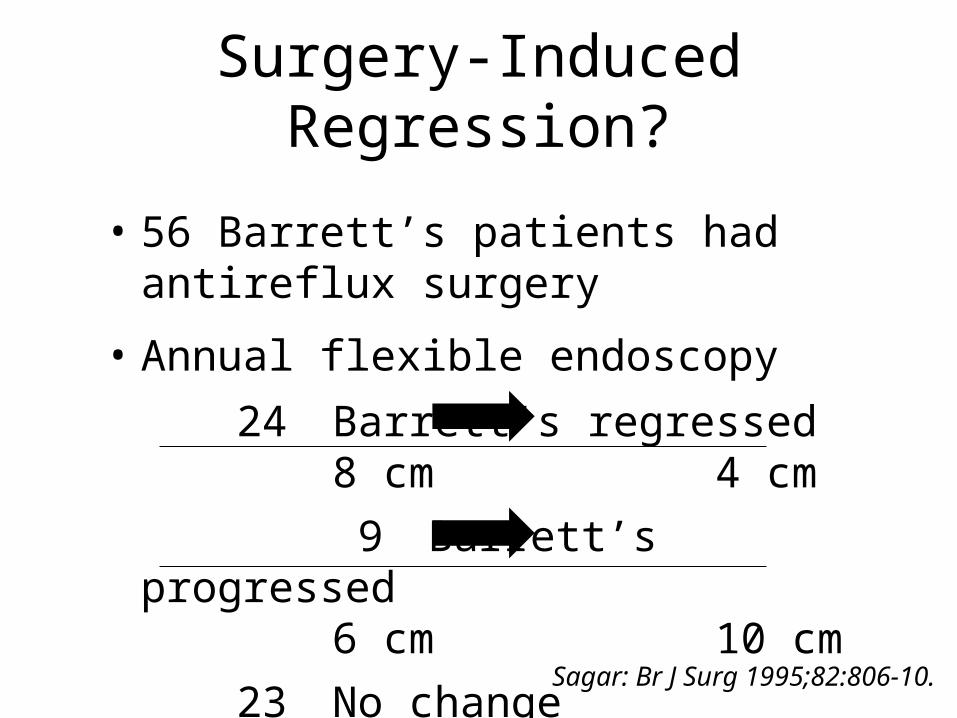
Sagar: Br J Surg 1995;82:806-10.
• 56 Barrett’s patients had antireflux surgery
• Annual flexible endoscopy
24 Barrett’s regressed 8 cm 4 cm
9 Barrett’s progressed 6 cm 10 cm
23 No change
Surgery-Induced Regression?
Barrett’s EsophagusDevelopment of Cancer Based on Grade
• No dysplasia 3%
• Low-grade dysplasia 18%
• High-grade dysplasia 28%
Morales and Sampliner, Arch Int Med 1999;159:1411-16.
Barrett’s EsophagusFollowing Patients Without Dysplasia
• Studies of cost-effectiveness are mixed
• Few cancers found during surveillance are
node-positive, versus >50% otherwise
• Optimal surveillance interval debated, but
data suggest q2-3 years

Barrett’s EsophagusPatients With Low-Grade Dysplasia
• Repeat endoscopy to avoid sampling error
• Surveillance q6 mo. x 1 year then q12 mo.
• May regress allowing increased interval

Barrett’s EsophagusPatients With High-Grade Dysplasia
• Must confirm the diagnosis
• Treatment is controversial
• Some advocate aggressive biopsy protocol
• Some advocate esophagectomy

Barrett’s EsophagusPatients With High-Grade Dysplasia
Case for Aggressive Surveillance (q3-6 mos.):
• Regression may occur (25%)
• Most patients will not progress to cancer
• Cancers remain surgically curable
• Esophagectomy carries morbidity (up to
40%) and mortality (3-6%)

Barrett’s EsophagusPatients With High-Grade Dysplasia
Case for Esophagectomy:
• 40% may already have cancer
• Surveillance delays definitive treatment
• Risk of esophagectomy low in high-
volume centers

Barrett’s EsophagusSpecific Treatment
Ablative Techniques
• laser
• electrocautery
• photodynamic therapy (PDT)
Resective Techniques
• Endoscopic mucosal resection (EMR)

Barrett’s Esophagus Take-Home Points
• Barrett’s esophagus is not a
contraindication to antireflux operation
• Medical or surgical therapy does not
eliminate need for Barrett’s surveillance
• Management of high-grade dysplasia is
evolving away from esophagectomy
Case 3
• A 53-year-old patient presents with a history of difficulty swallowing for years. More recently she is having increasing trouble swallowing, and has been regurgitating undigested food. Exam is unrevealing, but on chest film there is an air fluid level seen behind the heart in the mid chest.

Case 3
• Describe a differential diagnosis and diagnostic evaluation.

Case 3
• Discuss the management options for a patient with achalasia.

AchalasiaIncidence
• 0.5 new cases / 100,000 population / year
• Dysphagia, regurgitation, cough,
wheezing, aspiration, pulmonary infections
• 50% initially misdiagnosed

AchalasiaPathophysiology
• Involves degeneration of Auerbach’s
plexus and elevated LES resting pressure
• Poor LES relaxation results in esophageal
dilation with progressive loss of peristalsis

AchalasiaDiagnosis
• Ba swallow: – esophageal dilation / narrowing at GE junction
• EGD: – patulous esophagus, retained food, thickening
• Esophageal manometry: – LES resting pressure– LES relaxation on swallowing– primary peristalsis

Achalasia Treatment Options
• Non-Surgical options: – Nitrates and Ca++-channel blockers
– Endoscopic injection of Botox
– Pneumatic balloon dilatation
• Surgical options: – Heller myotomy (laparoscopic, thoracoscopic)

Heller MyotomyTechnique

Heller MyotomyTechnique
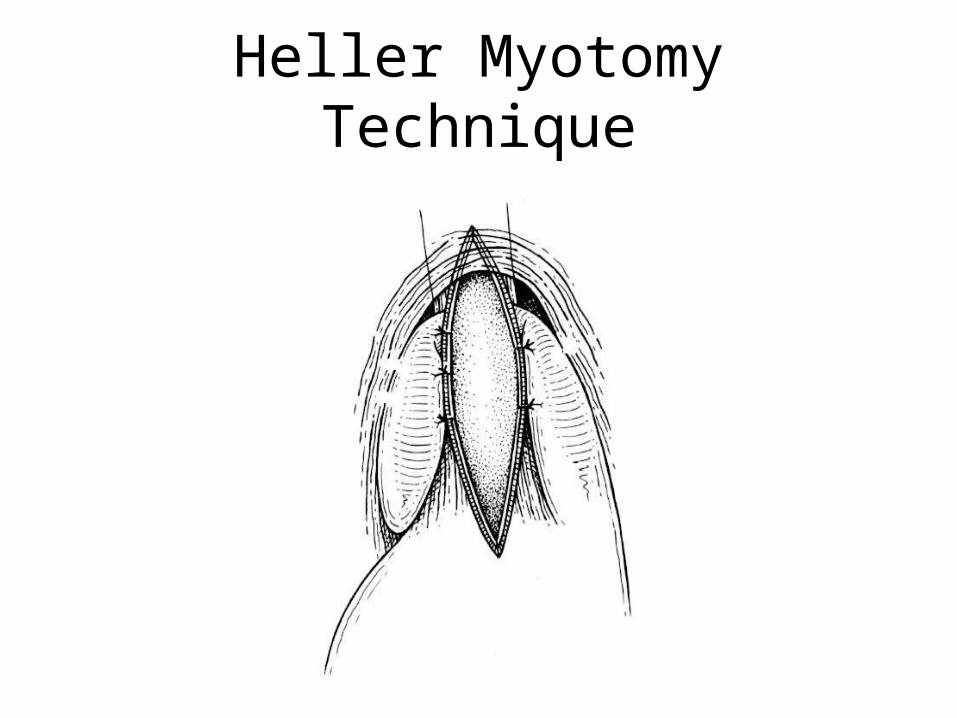
Heller MyotomyTechnique
Heller MyotomyOutcomes
• 40 laparoscopic Heller myotomies
• No conversions, mean op time - 180 min
• Median hospital stay - 2 days
• One intraop mucosal injuriey repaired
• Dysphagia alleviated in > 95%
Case 3
• Discuss the management of a patient with paraesophageal hernia.
EpidemiologyHiatal Hernias
• Herniation of the stomach through the
esophageal hiatus
• Para-esophageal type - 5%
– Occurs in elderly patients (~ 65 years)
– Frequent co-morbid conditions

• Classification depends on location of GEJ
– Type I- “sliding” hiatal hernia
– Type II- true paraesophageal hernia
– Type III- “mixed” hernia- sliding hernia and
true paraesophageal hernia
– Type IV- intra-abdominal organ involvement
ClassificationHiatal Hernias

Sliding Hiatal Hernia
• Type I
• GE junction “slides”
into the mediastinum
• Most HH
• May be associated with
symptomatic GERD
• Surgery not indicated

True Paraesophageal Hernia
• Type II
• GEJ in the abdominal cavity, fundus in the mediastinum
• 5% of all HH
• Risk of incarceration and strangulation

Mixed Paraesophageal Hernia
• Type III
• GE junction and gastric fundus are located in mediastinum
• 5% of all HH
• Risk of incarceration and strangulation

Paraesophageal HerniaVolvulus
Mesoaxial Volvulus Organoaxial Volvulus
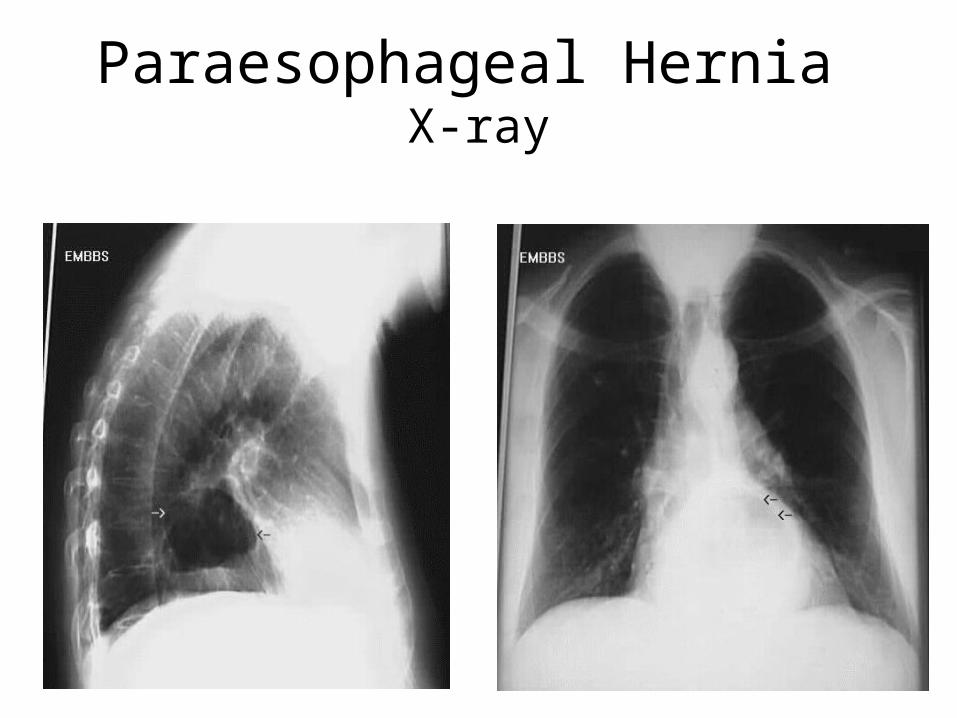
Paraesophageal Hernia X-ray
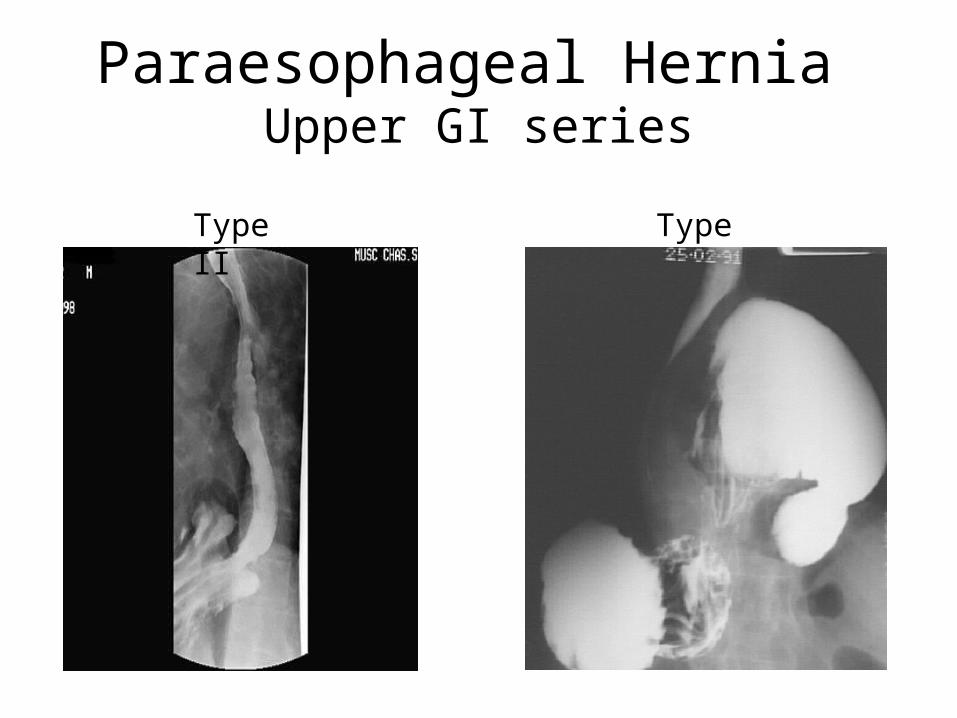
Paraesophageal Hernia Upper GI series
Type II Type III

Paraesophageal Hernia EGD

Paraesophageal Hernia Treatment Options
• Observation
• Medical Therapy
• Surgery

Paraesophageal Hernia Observation
• Assumes a low rate of gastric strangulation• Allen et al.
– 23 of 147 patients followed for 12-268 mos (median 78 mos).
– Only 4 pts had progressive symptoms and 2 had elective repair
– Estimate prevalence of one gastric strangulation per 245 pts
J Thorac Cardiovasc Surg 1993;105:253

Paraesophageal Hernia Medical Therapy
• One-third of patients have heartburn alone
– Acid inhibition
– Patient clearly informed of risk of gastric
strangulation and consequences• Excessive (10-50%) mortality for surgical repair of
gastric strangulation
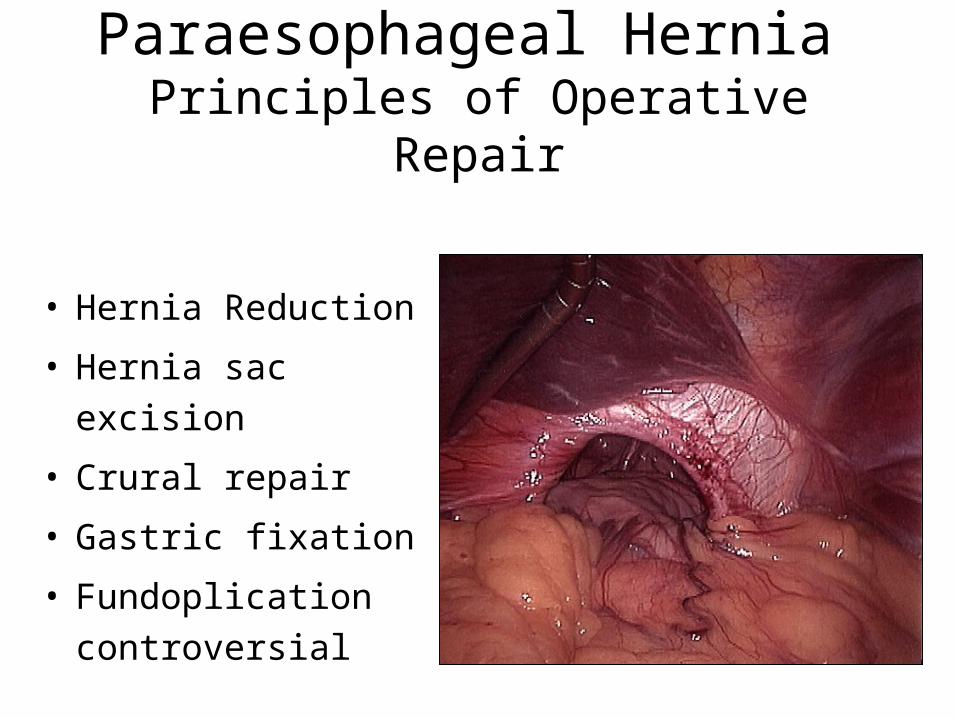
Paraesophageal Hernia Principles of Operative Repair
• Hernia Reduction
• Hernia sac excision
• Crural repair
• Gastric fixation
• Fundoplication
controversial

Paraesophageal Hernia Hernia Reduction
• Entire stomach and
at least 2 cm of
esophagus must be
intra-abdominal

Paraesophageal Hernia Sac Excision
• Entire sac must be
excised to decrease
risk of recurrence
• Remnants of sac
along inferior border
of left crus lead to
recurrence

Paraesophageal Hernia Crural Repair
• Primary repair alone
• Primary repair with
relaxing incision
• Mesh repair

Paraesophageal Hernia Fundoplication
• Recent series report high rate of GERD without fundoplication
• Wrap provides bulk to create “plug” at site of crural repair
Paraesophageal Hernia Surgical Outcomes
• Luketich et al.: 100 pts lap PH repair
– 12% intraop complications; technically demanding
– 3 conversions to open procedures
– 28% postop complication rate; 0% mortality
– 3% reoperation rate
– 91% satisfied, 2-day hospital stay
Ann Surg 2000;232:608

Paraesophageal Hernia Take-Home Points
• Uncommon, rarely present with strangulation
• Repair advised for non-GER symptoms
• Repair is technically demanding
• Laparoscopic vs. open remains controversial
• Prospective study to determine recurrence
Case 4
• A 47-year-old woman has chest pain after eating dinner at home 4 hours following upper GI endoscopy for dilatation of her achalasia.
• What is the presumed diagnosis?
Case 4
• What is the best means of making the diagnosis?
Case 4
• What is the appropriate management? Under what circumstances might you manage this non-operatively?
• What might be an appropriate management for a small perforation at the GE junction with minimal soiling?


















