Susceptibility of Mycobacterium leprae to Dapsone as a Determinant
11
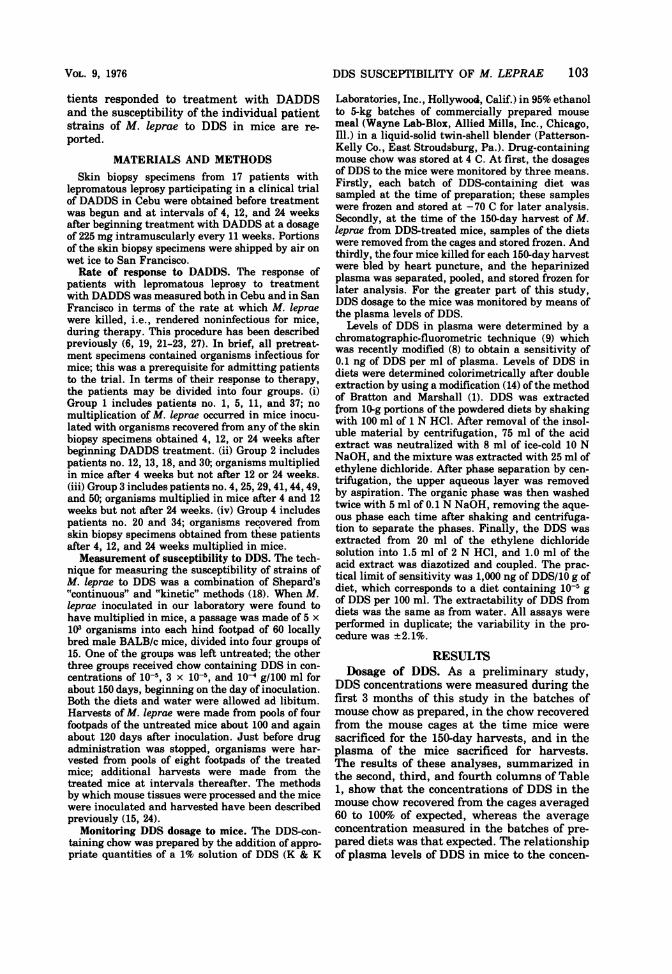
ANTmIucRoB3L AGENTS AND CHIMOTHRsAy, Jan. 1976, p. 102-112 ComowHr 0 1976 American Society for Microbiology Vol. 9, No. 1 Printed in U.SA. Susceptibility of Mycobacterium leprae to Dapsone as a Determinant of Patient Response to Acedapsone LOUIS LEVY* AND JOHN H. PETERS Leprosy Research Unit, Public Health Service Hospital, San Francisco, California 94118,* and Life Sciences Division, Stanford Research Institute, Menlo Park, California 94025 Received for publication 25 July 1975 In the course of a clinical trial of acedapsone therapy in 17 patients with lepromatous leprosy, the rate of response to therapy was measured by inocula- tion of mice with Mycobacterium leprae recovered from biopsy specimens of skin lesions obtained before treatment and at intervals of 4, 12, and 24 weeks after institution of treatment. The susceptibility of each isolate of M. leprae to dapsone (4,4'-diazninodiphenylsulfone [DDS]) was measured by passaging organisms that had multiplied in mice to new groups of untreated mice and to mice treated with DDS incorporated in the mouse chow in concentrations of 10-5, 3 x 10-5, and 10-4 gIlOO ml. The rate of response to acedapsone therapy and the sus- ceptibility of patient strains of M. leprae to DDS varied widely among patients. All isolates were inhibited from multiplication by treatment of mice with 10-4 g of DDS per 100 ml; all -but two isolates were susceptible to 3 x 10-5 g of DDS per 100 ml; and 17 of 36 isolates, representing nine patient strains, were susceptible to 10-5 g of DDS per 100 ml. Plasma levels of DDS measured in the mice adminis- tered these diets show that the minimal inhibitory concentration of DDS for M. leprae isolated from untreated patients is about 3 ng/ml. No relationship could be demonstrated between DDS susceptibility of pretreatment isolates i M. leprae and the rate at which patients responded to acedapsone therapy. Neither acedapsone treatment of patients nor DDS treatment of mice appeared to select genotypically more resistant M. leprae. Acedapsone (4,4'-diacetamidodiphenylsul- fone [DADDS]) is a relatively insoluble deriva- tive of dapsone (4,4'-diaminodiphenylsulfone [DDS]) which produces a prolonged low plasma level of DDS after intramuscular administra- tion (3). First developed for use in malaria chemoprophylaxis (27), DADDS was found to be effective against Mycobacterium leprae in footpad infection in mice (16) and in patients with lepromatous leprosy (21, 25), to whom the drug was administered .intramuscularly at a dosage of 225 mg every 11 weeks. This dosage of DADDS yielded a maximal plasma DDS con- centration of 50 to 80 ng/ml 1 to 5 weeks after the dose; plasma DDS levels fell to a minimum of 30 to 60 ng/ml 11 weeks after the dose (10, 13). Even these low levels of DDS would be ex- pected to produce a chemotherapeutic result, because they are substantially higher than the minimal inhibitory concentration of DDS for M. leprae. This has been established at less than 10 ng/ml of plasma in studies with mice (2, 10) and rats (11) infected with M. leprae. However, the DDS levels obtained after DADDS adminis- tration are much lower than the maximal levels of 2,000 ng/ml of plasma found in pa- tients receiving oral doses of 100 mg of DDS (11). A trial of DADDS therapy in 10 patients with previously untreated lepromatous leprosy showed that, in terms of the rate of killing of M. leprae, three patients responded as rapidly and seven patients responded more slowly than did patients receiving 50 mg of DDS daily (21). The' staging of a trial of DADDS therapy in Cebu, the Philippines, among patients with previously untreated lepromatous leprosy pro- vided the opportunity for a prospective study of possible determinants of the rate of response of patients during treatment with DADDS. (In a collaborative effort of the U.S. Leprosy Panel and the Leonard Wood Memorial, the efficacy of DADDS [225 mg intramuscularly every 77 days] has been compared with that of DADDS [225 mg] plus oral rifampin [1,500 mg] every 77 days and with that of oral rifampin [600 mg] daily.) In this paper, the results of a study of the relationship between the rate at which pa- 102
Transcript of Susceptibility of Mycobacterium leprae to Dapsone as a Determinant

ANTmIucRoB3L AGENTS AND CHIMOTHRsAy, Jan. 1976, p. 102-112ComowHr 0 1976 American Society for Microbiology
Vol. 9, No. 1Printed in U.SA.
Susceptibility of Mycobacterium leprae to Dapsone as aDeterminant of Patient Response to Acedapsone
LOUIS LEVY* AND JOHN H. PETERS
Leprosy Research Unit, Public Health Service Hospital, San Francisco, California 94118,* andLife Sciences Division, Stanford Research Institute, Menlo Park, California 94025
Received for publication 25 July 1975
In the course of a clinical trial of acedapsone therapy in 17 patients withlepromatous leprosy, the rate of response to therapy was measured by inocula-tion of mice with Mycobacterium leprae recovered from biopsy specimens of skinlesions obtained before treatment and at intervals of 4, 12, and 24 weeks afterinstitution oftreatment. The susceptibility ofeach isolate ofM. leprae to dapsone(4,4'-diazninodiphenylsulfone [DDS]) was measured by passaging organismsthat had multiplied in mice to new groups of untreated mice and to mice treatedwith DDS incorporated in the mouse chow in concentrations of 10-5, 3 x 10-5,and 10-4 gIlOO ml. The rate of response to acedapsone therapy and the sus-ceptibility of patient strains ofM. leprae to DDS varied widely among patients.All isolates were inhibited from multiplication by treatment of mice with 10-4 gof DDS per 100 ml; all-but two isolates were susceptible to 3 x 10-5 g of DDS per100 ml; and 17 of 36 isolates, representing nine patient strains, were susceptibleto 10-5 g ofDDS per 100 ml. Plasma levels ofDDS measured in the mice adminis-tered these diets show that the minimal inhibitory concentration of DDS forM. leprae isolated from untreated patients is about 3 ng/ml. No relationshipcould be demonstrated between DDS susceptibility of pretreatment isolates iM. leprae and the rate at which patients responded to acedapsone therapy.Neither acedapsone treatment of patients nor DDS treatment of mice appearedto select genotypically more resistant M. leprae.
Acedapsone (4,4'-diacetamidodiphenylsul-fone [DADDS]) is a relatively insoluble deriva-tive of dapsone (4,4'-diaminodiphenylsulfone[DDS]) which produces a prolonged low plasmalevel of DDS after intramuscular administra-tion (3). First developed for use in malariachemoprophylaxis (27), DADDS was found tobe effective against Mycobacterium leprae infootpad infection in mice (16) and in patientswith lepromatous leprosy (21, 25), to whom thedrug was administered .intramuscularly at adosage of 225 mg every 11 weeks. This dosageofDADDS yielded a maximal plasma DDS con-centration of 50 to 80 ng/ml 1 to 5 weeks afterthe dose; plasma DDS levels fell to a minimumof30 to 60 ng/ml 11 weeks after the dose (10, 13).Even these low levels of DDS would be ex-pected to produce a chemotherapeutic result,because they are substantially higher than theminimal inhibitory concentration ofDDS for M.leprae. This has been established at less than10 ng/ml of plasma in studies with mice (2, 10)and rats (11) infected with M. leprae. However,the DDS levels obtained after DADDS adminis-
tration are much lower than the maximallevels of 2,000 ng/ml of plasma found in pa-tients receiving oral doses of 100 mg of DDS(11).A trial ofDADDS therapy in 10 patients with
previously untreated lepromatous leprosyshowed that, in terms of the rate of killing ofM. leprae, three patients responded as rapidlyand seven patients responded more slowly thandid patients receiving 50 mg of DDS daily (21).The' staging of a trial of DADDS therapy inCebu, the Philippines, among patients withpreviously untreated lepromatous leprosy pro-vided the opportunity for a prospective study ofpossible determinants of the rate of response ofpatients during treatment with DADDS. (In acollaborative effort of the U.S. Leprosy Paneland the Leonard Wood Memorial, the efficacyof DADDS [225 mg intramuscularly every 77days] has been compared with that of DADDS[225 mg] plus oral rifampin [1,500 mg] every 77days and with that of oral rifampin [600 mg]daily.) In this paper, the results of a study ofthe relationship between the rate at which pa-
102
DDS SUSCEPTIBILITY OF M. LEPRAE 103
tients responded to treatment with DADDSand the susceptibility of the individual patientstrains of M. leprae to DDS in mice are re-ported.
MATERIALS AND METHODSSkin biopsy specimens from 17 patients with
lepromatous leprosy participating in a clinical trialof DADDS in Cebu were obtained before treatmentwas begun and at intervals of 4, 12, and 24 weeksafter beginning treatment with DADDS at a dosageof 225 mg intramuscularly every 11 weeks. Portionsof the skin biopsy specimens were shipped by air onwet ice to San Francisco.
Rate of response to DADDS. The response ofpatients with lepromatous leprosy to treatmentwith DADDS was measured both in Cebu and in SanFrancisco in terms of the rate at which M. lepraewere killed, i.e., rendered noninfectious for mice,during therapy. This procedure has been describedpreviously (6, 19, 21-23, 27). In brief, all pretreat-ment specimens contained organisms infectious formice; this was a prerequisite for admitting patientsto the trial. In terms of their response to therapy,the patients may be divided into four groups. (i)Group 1 includes patients no. 1, 5, 11, and 37; nomultiplication of M. leprae occurred in mice inocu-lated with organisms recovered from any of the skinbiopsy specimens obtained 4, 12, or 24 weeks afterbeginning DADDS treatment. (ii) Group 2 includespatients no. 12, 13, 18, and 30; organisms multipliedin mice after 4 weeks but not after 12 or 24 weeks.(iii) Group 3 includes patients no. 4, 25, 29, 41, 44, 49,and 50; organisms multiplied in mice after 4 and 12weeks but not after 24 weeks. (iv) Group 4 includespatients no. 20 and 34; organisms recovered fromskin biopsy specimens obtained from these patientsafter 4, 12, and 24 weeks multiplied in mice.
Measurement of susceptibility to DDS. The tech-nique for measuring the susceptibility of strains ofM. Ieprae to DDS was a combination of Shepard's"continuous" and "kinetic" methods (18). When M.leprae inoculated in our laboratory were found tohave multiplied in mice, a passage was made of 5 x103 organisms into each hind footpad of 60 locallybred male BALB/c mice, divided into four groups of15. One of the groups was left untreated; the otherthree groups received chow containing DDS in con-centrations of 10-5, 3 x 10-5, and 10-4 g/100 ml forabout 150 days, beginning on the day of inoculation.Both the diets and water were allowed ad libitum.Harvests of M. leprae were made from pools of fourfootpads of the untreated mice about 100 and againabout 120 days after inoculation. Just before drugadministration was stopped, organisms were har-vested from pools of eight footpads of the treatedmice; additional harvests were made from thetreated mice at intervals thereafter. The methodsby which mouse tissues were processed and the micewere inoculated and harvested have been describedpreviously (15, 24).
Monitoring DDS dosage to mice. The DDS-con-taining chow was prepared by the addition of appro-priate quantities of a 1% solution of DDS (K & K
Laboratories, Inc., Hollywood, Calif.) in 95% ethanolto 5-kg batches of commercially prepared mousemeal (Wayne Lab-Blox, Allied Mills, Inc., Chicago,Ill.) in a liquid-solid twin-shell blender (Patterson-Kelly Co., East Stroudsburg, Pa.). Drug-containingmouse chow was stored at 4 C. At first, the dosagesof DDS to the mice were monitored by three means.Firstly, each batch of DDS-containing diet wassampled at the time of preparation; these sampleswere frozen and stored at -70 C for later analysis.Secondly, at the time of the 150-day harvest of M.leprae from DDS-treated mice, samples of the dietswere removed from the cages and stored frozen. Andthirdly, the four mice killed for each 150-day harvestwere bled by heart puncture, and the heparinizedplasma was separated, pooled, and stored frozen forlater analysis. For the greater part of this study,DDS dosage to the mice was monitored by means ofthe plasma levels of DDS.
Levels of DDS in plasma were determined by achromatographic-fluorometric technique (9) whichwas recently modified (8) to obtain a sensitivity of0.1 ng of DDS per ml of plasma. Levels of DDS indiets were determined colorimetrically after doubleextraction by using a modification (14) of the methodof Bratton and Marshall (1). DDS was extractedfrom 10-g portions of the powdered diets by shakingwith 100 ml of 1 N HCI. After removal of the insol-uble material by centrifugation, 75 ml of the acidextract was neutralized with 8 ml of ice-cold 10 NNaOH, and the mixture was extracted with 25 ml ofethylene dichloride. After phase separation by cen-trifugation, the upper aqueous layer was removedby aspiration. The organic phase was then washedtwice with 5 ml of 0.1 N NaOH, removing the aque-ous phase each time after shaking and centrifuga-tion to separate the phases. Finally, the DDS wasextracted from 20 ml of the ethylene dichloridesolution into 1.5 ml of 2 N HCI, and 1.0 ml of theacid extract was diazotized and coupled. The prac-tical limit of sensitivity was 1,000 ng of DDS/10 g ofdiet, which corresponds to a diet containing 10-5 gof DDS per 100 ml. The extractability of DDS fromdiets was the same as from water. All assays wereperformed in duplicate; the variability in the pro-cedure was ±2.1%.
RESULTSDosage of DDS. As a preliminary study,
DDS concentrations were measured during thefirst 3 months of this study in the batches ofmouse chow as prepared, in the chow recoveredfrom the mouse cages at the time mice weresacrificed for the 150-day harvests, and in theplasma of the mice sacrificed for harvests.The results of these analyses, summarized inthe second, third, and fourth columns of Table1, show that the concentrations of DDS in themouse chow recovered from the cages averaged60 to 100%o of expected, whereas the averageconcentration measured in the batches of pre-pared diets was that expected. The relationshipof plasma levels of DDS in mice to the concen-
VOL. 9, 1976
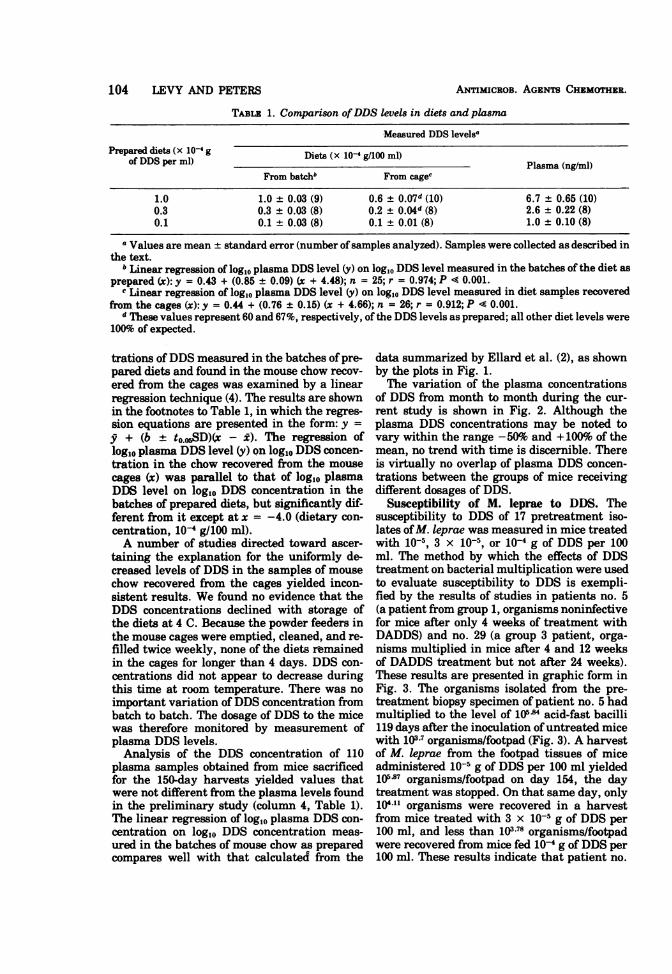
TABLE 1. Comparison ofDDS levels in diets and plasma
Measured DDS levelsaPrepared diets (x 10-4 g Diets (x 1O-4 g/100 mI)
of DDS per ml) _______Plasma (nglml)
From batch" From cagec
1.0 1.0 ± 0.03 (9) 0.6 ± 0.07d (10) 6.7 ± 0.65 (10)0.3 0.3 + 0.03 (8) 0.2 ± 0.04d (8) 2.6 ± 0.22 (8)0.1 0.1 ± 0.03 (8) 0.1 ± 0.01 (8) 1.0 ± 0.10 (8)
a Values are mean ± standard error (number ofsamples analyzed). Samples were collected as described inthe text.
"Linear regression of log1O plasma DDS level (y) on log1O DDS level measured in the batches of the diet asprepared (x): y = 0.43 + (0.85 ± 0.09) (x + 4.48); n = 25; r = 0.974; P 4 0.001.
c Linear regression of log1O plasma DDS level (y) on log10 DDS level measured in diet samples recoveredfrom the cages (x): y = 0.44 + (0.76 ± 0.15) (x + 4.66); n = 26; r = 0.912; P 4 0.001.
d These values represent 60 and 67%, respectively, of the DDS levels as prepared; all other diet levels were100% of expected.
trations ofDDS measured in the batches of pre-pared diets and found in the mouse chow recov-ered from the cages was examined by a linearregression technique (4). The results are shownin the footnotes to Table 1, in which the regres-sion equations are presented in the form: y =y + (b + to.05SD)(x - i). The regression oflog1o plasma DDS level (y) on log1O DDS concen-tration in the chow recovered from the mousecages (x) was parallel to that of log1o plasmaDDS level on log1O DDS concentration in thebatches of prepared diets, but significantly dif-ferent from it except at x = -4.0 (dietary con-centration, 10-4 g/100 ml).A number of studies directed toward ascer-
taining the explanation for the uniformly de-creased levels of DDS in the samples of mousechow recovered from the cages yielded incon-sistent results. We found no evidence that theDDS concentrations declined with storage ofthe diets at 4 C. Because the powder feeders inthe mouse cages were emptied, cleaned, and re-filled twice weekly, none of the diets rmainedin the cages for longer than 4 days. DDS con-centrations did not appear to decrease duringthis time at room temperature. There was noimportant variation ofDDS concentration frombatch to batch. The dosage of DDS to the micewas therefore monitored by measurement ofplasma DDS levels.Analysis of the DDS concentration of 110
plasma samples obtained from mice sacrificedfor the 150-day harvests yielded values thatwere not different from the plasma levels foundin the preliminary study (column 4, Table 1).The linear regression of log10 plasma DDS con-centration on log10 DDS concentration meas-ured in the batches of mouse chow as preparedcompares well with that calculated from the
data summarized by Ellard et al. (2), as shownby the plots in Fig. 1.The variation of the plasma concentrations
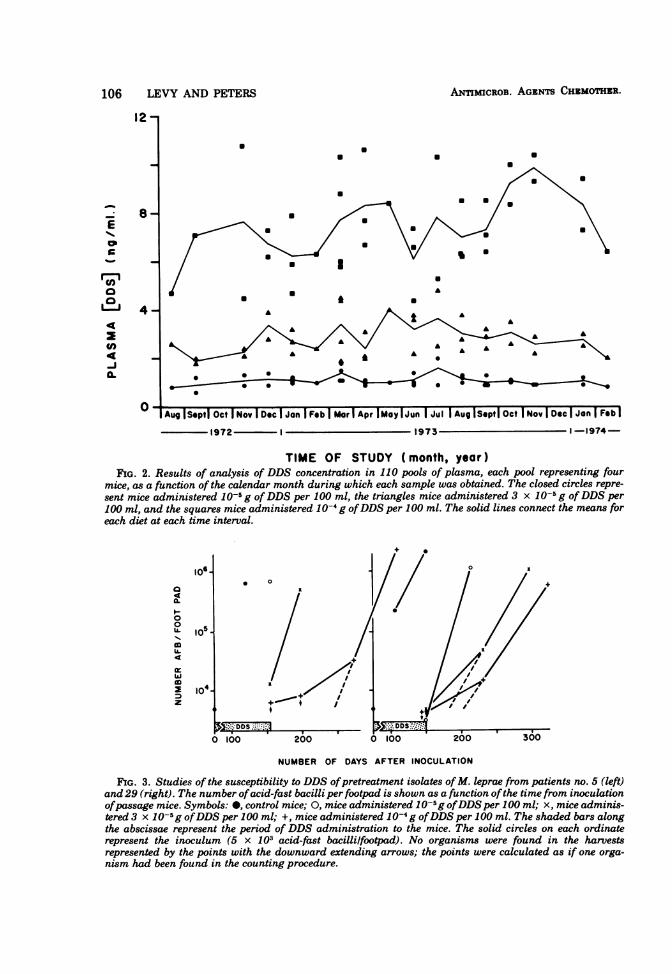
of DDS from month to month during the cur-rent study is shown in Fig. 2. Although theplasma DDS concentrations may be noted tovary within the range -50% and + 100%o of themean, no trend with time is discernible. Thereis virtually no overlap of plasma DDS concen-trations between the groups of mice receivingdifferent dosages of DDS.
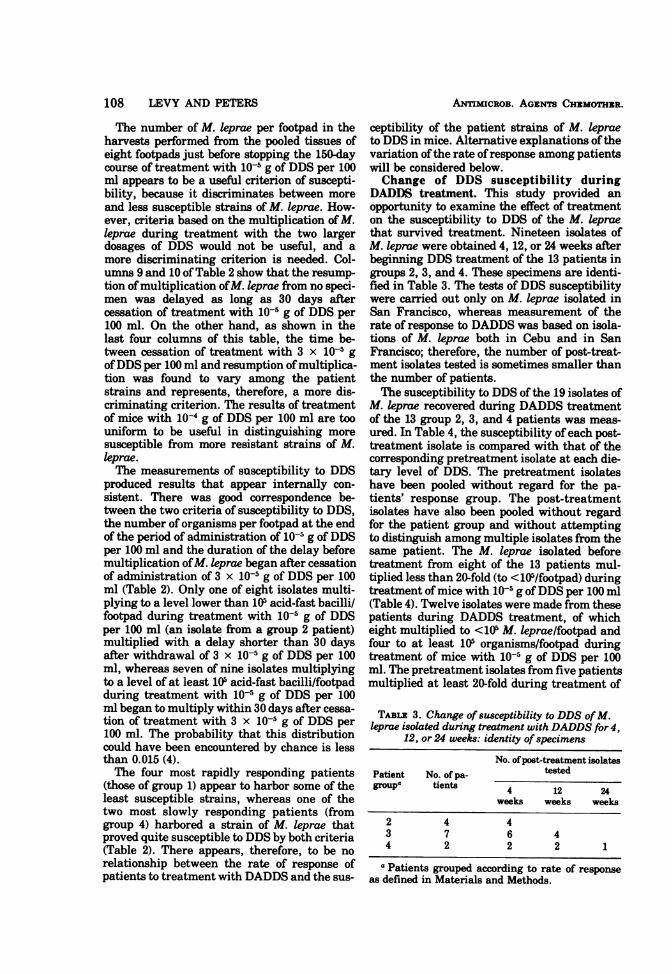
Susceptibility of M. Ieprae to DDS. Thesusceptibility to DDS of 17 pretreatment iso-lates ofM. leprae was measured in mice treatedwith 10-5, 3 x 10-5, or 10-4 g of DDS per 100ml. The method by which the effects of DDStreatment on bacterial multiplication were usedto evaluate susceptibility to DDS is exempli-fied by the results of studies in patients no. 5(a patient from group 1, organisms noninfectivefor mice after only 4 weeks of treatment withDADDS) and no. 29 (a group 3 patient, orga-nisms multiplied in mice after 4 and 12 weeksof DADDS treatment but not after 24 weeks).These results are presented in graphic form inFig. 3. The organisms isolated from the pre-treatment biopsy specimen of patient no. 5 hadmultiplied to the level of 105-" acid-fast bacilli119 days after the inoculation of untreated micewith 103-7 organisms/footpad (Fig. 3). A harvestof M. leprae from the footpad tissues of miceadministered 10-5 g of DDS per 100 ml yielded10587 organisms/footpad on day 154, the daytreatment was stopped. On that same day, only104lO organisms were recovered in a harvestfrom mice treated with 3 x 10-5 g of DDS per100 ml, and less than 103.71 organisms/footpadwere recovered from mice fed 10-4 g of DDS per100 ml. These results indicate that patient no.
104 LEVY AND PETERS ANTiMICROB. AGENTS CHZMOTHZR.

DDS SUSCEPTIBILITY OF M. LEPRAE 105
2.0- HiL
aa0
20
-I .
- 5.0 -4.0 -3.0 -2.0 -1.0
LOGIO DIETARY [DDS] (g %)
FIG. 1. Regression of the logi0 plasma concentration of DDS on the log1o concentration of DDS in themouse chow. The broken line connecting the open circles represents the line that fits the data that resultedfrom this study; the linear regression of log,Oplasma DDS level (y) on log10 DDS level ofprepared diets (x):y = 0.46 + (0.82 + 0.05)(x + 4.50); n = 110; r = 0.953; P < 0.0001. The solid line connecting theclosed circles represents the least-squares line best fitting the data ofEllard et al. (2): y = 3.01 + (1.05 ± 0.09)(x + 2.06); n = 24; r = 0.982; P < 0.01. Although the slope of the line calculated from our 110 specimens isdifferent from that calculated from Ellard's data (P < 0.05), the values for y at x = -4.0 and x = -5.0 (cor-responding to dietary DDS concentrations of1O-4 and 10-5g/Il00 ml) calculated from the two regression linesare not different at the 95% level of confidence.
5's organisms were susceptible to 10-4 and 3 x10-5 g of DDS but not to 10-s g of DDS per 100ml.The M. leprae isolated from the pretreatment
specimen of patient no. 29 proved more suscep-tible to DDS. These had multiplied to the levelof 106/footpad in untreated mice by day 150, theday drug administration was stopped, whereasno multiplication was found in the mice fed anyof the DDS-containing diets.The susceptibility of an organism to the
action of an antimicrobial drug is traditionallymeasured in terms of the ability of the drug toinhibit multiplication ofthe organism. The datapresented in Fig. 3 suggest a second criterion ofsusceptibility. When multiplication ofM. lepraehas been inhibited during administration of adrug, multiplication of the organisms mayresume immediately after the cessation of drugtreatment, or only after some delay longer thancan be accounted for by the presence of effectiveconcentrations of the drug in the mouse, or notat all. Once treatment has been withdrawn,multiplication ofM. leprae will resume immedi-ately if the effect of the drug is primarily bac-teriostatic, whereas no multiplication mayoccur if the drug has exerted a bactericidaleffect. A delay between cessation of treatment
and resumption of multiplication may resultfrom killing of a portion of the inoculum, withonly the surviving fraction giving rise to latermultiplication. Alternatively, delayed multipli-cation may represent prolonged bacteriostasis,with later multiplication arising from the entirebacterial population (5). Shepard has shown (17)that the duration of the delay is proportionalto the dosage of DDS, suggesting that the delaybetween cessation of DDS treatment of miceand resumption of multiplication of M. lepraemay represent a useful criterion of susceptibil-ity of the organism to the drug.
In Fig. 3, multiplication of M. leprae may benoted to have resumed without delay in thecase oftwo growth curves, that of patient no. 5'sorganisms in mice treated with 3 x 10-5 g ofDDS per 100 ml and that of patient no. 29'sorganisms in mice treated with 10-5 g of DDSper 100 ml, whereas multiplication resumedonly after some delay in both groups of micetreated with 10-4 g of DDS per 100 ml and inmice infected with organisms from patient no.29 and treated with 3 x 10-5 g of DDS per 100ml. The time of resumption of multiplication isestimated by extrapolating the growth curve tothe level of 5 x 103 acid-fast bacilli/footpad, thesize of the inoculum; the duration of the delay
VOL. 9, 1976
ANTIMICROB. AGENTS CHZMOTHIR.
12 -
Ecpb
aa-I
a.(A
8-
4-
0
aa
a.
aa
a
a
a
a I* I
a
a
a Aa
A
Aug ISepti Oct I Nov I Dec I Jon FFeb ] Mar Apr IMay I Jun I Jul I Aug ISeptI Oct I Nov I Dec I Jan I Feb I
1972 1 1973 1-1974-
TIME OF STUDY (month, year)FIG. 2. Results of analysis of DDS concentration in 110 pools of plasma, each pool representing four
mice, as a function of the calendar month during which each sample was obtained. The closed circles repre-sent mice administered 10-5 g ofDDS per 100 ml, the triangles mice administered 3 x 10-5 g ofDDS per100 ml, and the squares mice administered 10-4 g ofDDS per 100 ml. The solid lines connect the means foreach diet at each time interval.
i06.
a4
IL0lL.
4
z
s10
104
.
0 100
NUMBER OF DAYS AFTER INOCULATION
FIG. 3. Studies of the susceptibility to DDS ofpretreatment isolates ofM. leprae from patients no. 5 (left)and 29 (right). The number ofacid-fast bacilli per footpad is shown as a function ofthe time from inoculationofpassage mice. Symbols: *, control mice; 0, mice administered 10-5g ofDDS per 100 ml; x, mice adminis-tered 3 x 10-g ofDDS per 100 ml; +, mice administered 10-4 g ofDDS per 100 ml. The shaded bars alongthe abscissae represent the period of DDS administration to the mice. The solid circles on each ordinaterepresent the inoculum (5 x 103 acid-fast bacillilfootpad). No organisms were found in the harvestsrepresented by the points with the downward extending arrows; the points were calculated as if one orga-nism had been found in the counting procedure.
106 LEVY AND PETERS
Ak,
0 0 0 00 1.11----------- e 41
*------ 0 90

DDS SUSCEPTIBILITY OF M. LEPRAE 107
is then the number of days between cessation ofDDS administration and resumption of multi-plication of M. leprae.
Multiplication of patient no. 5's organismsmay be noted to have begun without apparentdelay when treatment with 3 x 10-5 g of DDSper 100 ml was stopped. On the other hand,multiplication after cessation oftreatment with10-4 g of DDS per 100 ml began only after a
delay of 91 days. Harvests of M. leprae iso-lated from the pretreatment biopsy specimen ofpatient no. 29 showed that multiplication beganwithout delay once treatment with 10-5 g ofDDS per 100 ml was stopped, whereas therewas a delay of 37 days after treatment with3 x 10-$ g of DDS per 100 ml was stopped beforemultiplication of M. leprae began; and multi-plication was delayed for 52 days after stoppingtreatment with 10-4 g of DDS per 100 ml. Theseresults suggest that the susceptibility of an iso-late ofM. leprae to DDS might be characterizedboth by the level to which the organisms hadmultiplied during treatment with a given dos-age of DDS and by the duration of delay be-tween cessation oftreatment and resumption ofmultiplication.The results of the studies of DDS susceptibil-
ity and the relationship between the rate atwhich patients responded to DADDS and thesusceptibility of patient strains of M. leprae toDDS are summarized in Table 2, in which thesusceptibility to DDS of the strains ofM. lepraeis compared for the four groups of patients.
Patient groups are ranked according to the rateof response; group 1 patients are those respond-ing most rapidly and group 4 patients are thoseresponding most slowly to DADDS treatment.The results of the studies in patients no. 5 and29 are included in this table.The data of Table 2 suggest a broad range of
susceptibility to DDS among isolates of M.leprae from patients with previously untreatedlepromatous leprosy. Eight of 17 patient strainsof M. leprae (column 3) were inhibited frommultiplication to the level of 105 organisms/footpad by treatment of mice with 10-5 g ofDDS per 100 ml; these strains may be consid-ered susceptible to this dosage. On the otherhand, M. leprae of two patient strains multi-plied at least 20-fold (i.e., to 105 organisms/foot-pad) but less than 100-fold (i.e., <5 x 105 orga-nisms/footpad) during treatment of mice with10-5 g of DDS per 100 ml (column 4); thesestrains may be considered partially susceptible.Finally, the organisms of seven strains (alsocolumn 4) underwent at least 100-fold multipli-cation from the standard inoculum of 5 x 103 or-
g'anisms/footpad during administration of theDDS in the smallest dosage. The organisms ofonly two patient strains demonstrated greaterthan 20-fold but less than 100-fold mulitiplica-tion during treatment with 3 x 10-5 g of DDSper 100 ml, indicating partial susceptibility tothis dosage of DDS. As already noted, the orga-nisms of all patient strains were susceptible toDDS administered in a dosage of 10-4 g/100 ml.
TABLE 2. Rate of response to DADDS therapy and susceptibility ofpretreatment isolates to DDS
No. of isolates multiplying with following characteristics
M. Ieprae per footpad after 150 days oftreatment Delay between withdrawal of DDS and resump-Patient No. of with DDS tion of multiplication (days)groupa patients 3 x 10-5 g/100 3 x 10; g/100
10-5g100MI Ml 10-4 g/l00 Ml 10-5 gIllOO Mlb MlX104g/100 MI/0
<105 .105 <10' .105 <105 l105 .30 <30 {30 <30 .30 <30
1 4 2c 2 2 2 1 1 22d ~~2 2 2 2 2
2 4 3 3 3 3 2 1 3
1 3d 3 3 3 3 2 a4 2 11 1 2 2 2 [2 2
a Patients grouped according to rate of response as defined in Materials and Methods.bAmount of DDS.c One of these two strains actually multiplied to 7.34 x 105 M. leprae/footpad.d These strains actually multiplied at least to 5 x 105 organisms/footpad.
VOL. 9, 1976
ANTmicROB. AGENTS CHEMOTHER.
The number of M. leprae per footpad in theharvests performed from the pooled tissues ofeight footpads just before stopping the 150-daycourse of treatment with 10-5 g of DDS per 100ml appears to be a useful criterion of suscepti-bility, because it discriminates between moreand less susceptible strains of M. leprae. How-ever, criteria based on the multiplication of M.leprae during treatment with the two largerdosages of DDS would not be useful, and amore discriminating criterion is needed. Col-umns 9 and 10 of Table 2 show that the resump-tion ofmultiplication ofM. leprae from no speci-men was delayed as long as 30 days aftercessation of treatment with 10-5 g of DDS per100 ml. On the other hand, as shown in thelast four columns of this table, the time be-tween cessation of treatment with 3 x 10-5 g
ofDDS per 100 ml and resumption ofmultiplica-tion was found to vary among the patientstrains and represents, therefore, a more dis-criminating criterion. The results of treatmentof mice with 10-4 g of DDS per 100 ml are toouniform to be useful in distinguishing moresusceptible from more resistant strains of M.leprae.The measurements of susceptibility to DDS
produced results that appear internally con-sistent. There was good correspondence be-tween the two criteria of susceptibility to DDS,the number of organisms per footpad at the endof the period of administration of 10-5 g ofDDSper 100 ml and the duration of the delay beforemultiplication ofM. leprae began after cessationof administration of 3 x 10-5 g of DDS per 100ml (Table 2). Only one of eight isolates multi-plying to a level lower than 105 acid-fast bacilli/footpad during treatment with 10-5 g of DDSper 100 ml (an isolate from a group 2 patient)multiplied with a delay shorter than 30 daysafter withdrawal of 3 x 10-5 g of DDS per 100ml, whereas seven of nine isolates multiplyingto a level of at least 105 acid-fast bacilli/footpadduring treatment with 10-5 g of DDS per 100ml began to multiply within 30 days after cessa-tion of treatment with 3 x 10-5 g of DDS per100 ml. The probability that this distributioncould have been encountered by chance is lessthan 0.015 (4).The four most rapidly responding patients
(those of group 1) appear to harbor some of theleast susceptible strains, whereas one of thetwo most slowly responding patients (fromgroup 4) harbored a strain of M. leprae thatproved quite susceptible to DDS by both criteria(Table 2). There appears, therefore, to be norelationship between the rate of response ofpatients to treatment with DADDS and the sus-
ceptibility of the patient strains of M. lepraeto DDS in mice. Alternative explanations ofthevariation ofthe rate ofresponse among patientswill be considered below.Change of DDS susceptibility during
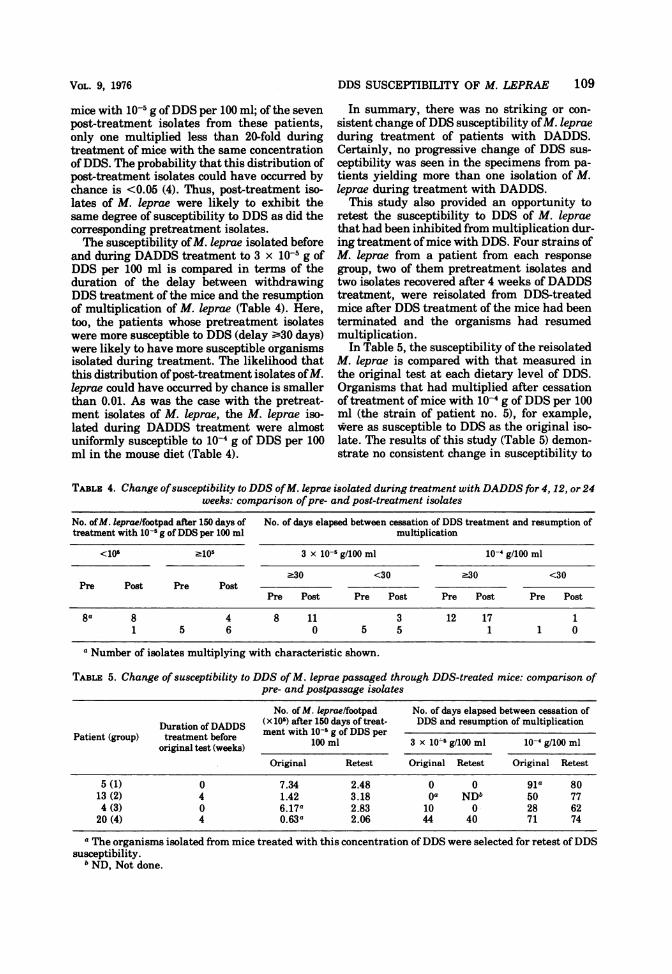
DADDS treatment. This study provided anopportunity to examine the effect of treatmenton the susceptibility to DDS of the M. lepraethat survived treatment. Nineteen isolates ofM. leprae were obtained 4, 12, or 24 weeks afterbeginning DDS treatment of the 13 patients ingroups 2, 3, and 4. These specimens are identi-fied in Table 3. The tests of DDS susceptibilitywere carried out only on M. leprae isolated inSan Francisco, whereas measurement of therate of response to DADDS was based on isola-tions of M. leprae both in Cebu and in SanFrancisco; therefore, the number of post-treat-ment isolates tested is sometimes smaller thanthe number of patients.The susceptibility to DDS of the 19 isolates of
M. leprae recovered during DADDS treatmentof the 13 group 2, 3, and 4 patients was meas-ured. In Table 4, the susceptibility of each post-treatment isolate is compared with that of thecorresponding pretreatment isolate at each die-tary level of DDS. The pretreatment isolateshave been pooled without regard for the pa-tients' response group. The post-treatmentisolates have also been pooled without regardfor the patient group and without attemptingto distinguish among multiple isolates from thesame patient. The M. leprae isolated beforetreatment from eight of the 13 patients mul-tiplied less than 20-fold (to <105/footpad) duringtreatment ofmice with 10-5 g ofDDS per 100 ml(Table 4). Twelve isolates were made from thesepatients during DADDS treatment, of whicheight multiplied to <105 M. keprae/footpad andfour to at least 105 organisms/footpad duringtreatment of mice with 10-5 g of DDS per 100ml. The pretreatment isolates from five patientsmultiplied at least 20-fold during treatment of
TABLE 3. Change of susceptibility to DDS ofM.leprae isolated during treatment with DADDS for4,
12, or 24 weeks: identity of specimens
No. ofpost-treatment isolatesPatient No. of pa- testedgroupa tients 4 12 24
weeks weeks weeks
2 4 43 7 6 44 2 2 2 1
a Patients grouped according to rate of responseas defined in Materials and Methods.
108 LEVY AND PETERS
VOL. 9, 1976
mice with 10-5 g ofDDS per 100 ml; of the sevenpost-treatment isolates from these patients,only one multiplied less than 20-fold duringtreatment of mice with the same concentrationof DDS. The probability that this distribution ofpost-treatment isolates could have occurred bychance is <0.05 (4). Thus, post-treatment iso-lates of M. keprae were likely to exhibit thesame degree of susceptibility to DDS as did thecorresponding pretreatment isolates.The susceptibility ofM. leprae isolated before
and during DADDS treatment to 3 x 10-5 g ofDDS per 100 ml is compared in terms of theduration of the delay between withdrawingDDS treatment of the mice and the resumptionof multiplication of M. keprae (Table 4). Here,too, the patients whose pretreatment isolateswere more susceptible to DDS (delay ;s30 days)were likely to have more susceptible organismsisolated during treatment. The likelihood thatthis distribution ofpost-treatment isolates ofM.leprae could have occurred by chance is smallerthan 0.01. As was the case with the pretreat-ment isolates of M. leprae, the M. leprae iso-lated during DADDS treatment were almostuniformly susceptible to 10-4 g of DDS per 100ml in the mouse diet (Table 4).
DDS SUSCEPTIBILITY OF M. LEPRAE 109
In summary, there was no striking or con-
sistent change of DDS susceptibility ofM. leprae
during treatment of patients with DADDS.Certainly, no progressive change of DDS sus-ceptibility was seen in the specimens from pa-tients yielding more than one isolation of M.leprae during treatment with DADDS.
This study also provided an opportunity toretest the susceptibility to DDS of M. leprae
that had been inhibited from multiplication dur-ing treatment ofmice with DDS. Four strains ofM. leprae from a patient from each responsegroup, two of them pretreatment isolates andtwo isolates recovered after 4 weeks of DADDStreatment, were reisolated from DDS-treatedmice after DDS treatment of the mice had beenterminated and the organisms had resumedmultiplication.
In Table 5, the susceptibility of the reisolatedM. leprae is compared with that measured inthe original test at each dietary level of DDS.Organisms that had multiplied after cessationof treatment of mice with 10-4 g of DDS per 100ml (the strain of patient no. 5), for example,were as susceptible to DDS as the original iso-late. The results of this study (Table 5) demon-strate no consistent change in susceptibility to
TABLE 4. Change ofsusceptibility to DDS ofM. keprae isolated during treatment with DADDS for 4, 12, or 24weeks: comparison ofpre- and post-treatment isolates
No. ofM. leprae/footpad after 150 days of No. of days elapsed between cessation of DDS treatment and resumption oftreatment with 10-5 g ofDDS per 100 ml multiplication
<10' -105 3 x 10-5 g/100 ml 10-4 g/100 ml
.30 <30 .30 <30Pre Post Pre Post
Pre Post Pre Post Pre Post Pre Post
8a 8 4 8 11 3 12 17 11 5 6 0 5 5 1 1 0
a Number of isolates multiplying with characteristic shown.
TABLE 5. Change of susceptibility to DDS ofM. leprae passaged through DDS-treated mice: comparison ofpre- and postpassage isolates
No. of M. leprae/footpad No. of days elapsed between cessation ofDuration of DADDS (x 10s) after 150 days of treat- DDS and resumption of multiplication
Patient (group) treatment before ment withl1-5g of DDS peroriginal test (weeks) 100 ml 3 x 10-' g/100 ml 10- g/100 ml
Original Retest Original Retest Original Retest
5 (1) 0 7.34 2.48 0 0 gla 8013 (2) 4 1.42 3.18 Oa ND" 50 774 (3) 0 6.17a 2.83 10 0- 28 6220 (4) 4 0.63a 2.06 44 40 71 74
a The organisms isolated from mice treated with this concentration ofDDS were selected for retest ofDDSsusceptibility.
b ND, Not done.
ANTmMICROB. AGENTS CHEMOTHER.
DDS of M. leprae that have multiplied afterwithdrawal of DDS treatment. Certainly, thereis no evidence that DDS treatment of mice se-lected genotypically more resistant individ-uals in the inoculum of M. leprae.The previously unpublished data of some
other work carried out in this laboratory arerelevant to this presentation. Mice were inocu-lated with M. leprae of a strain that has beenused for all of the drug studies carried out inthis laboratory and found to be susceptible to3 x 10-5 g ofDDS per 100 ml but not to 10-5 g ofDDS per 100 ml. Treatment with 10-4 g of DDSper 100 ml was begun 75 days after inoculationand continued for the duration of the experi-ment. A harvest performed on day 509 showedthat some multiplication of M. leprae had oc-curred. A harvest and passage were performed77 days later. Multiplication of the organismswas inhibited by treatment of the passage micewith 1o-4 g of DDS per 100 ml.In a second experiment, mice were inocu-
lated with the same strain of M. leprae, and10-1 g of DDS per 100 ml was administered for90 days beginning 60 days after inoculation. Byday 322, the organisms were found to havemultiplied and were harvested and passagedtwice through untreated mice. Multiplication ofthe organisms in the third serial passage wasinhibited by treatment of the mice with 10-4 gof DDS per 100 ml. Thus, treatment of micewith DDS did not appear to select genotypicallymore resistant strains of M. leprae.
DISCUSSION
In an earlier study (20), it was shown thatM. leprae isolated from previously untreatedpatients with lepromatous leprosy were in-hibited from multiplying in mice by administra-tion to the mice of a diet containing 10-4 g ofDDS per 100 ml. Some isolates were found to beinhibited by DDS administered in a concentra-tion of 10-5 g/100 ml. The current study wascarried out to learn if differences of DDS sus-ceptibility among patient strains of M. leprae,all susceptible to 10-4 g of DDS per 100 ml,might explain differences of the rate at whichM. leprae are killed during DADDS therapy ofpatients with previously untreated lepromatousleprosy.The technique by which the susceptibility of
strains ofM. leprae to DDS was measured in thecurrent study was a combination of Shepard's"continuous" and "kinetic" methods (18). In thecontinuous method, mice are treated from theday of inoculation, whereas in the kineticmethod treatment is begun only after the be-ginning of logarithmic multiplication. The con-
tinuous method is, therefore, a more sensitivetest. Because it requires the cessation of ther-apy after multiplication of the organisms in un-treated mice has reached its maximum, thekinetic method permits a distinction betweenmerely bacteriostatic and bactericidal activity.The use of the combined technique in this studyprovided two criteria by which the susceptibilityto DDS of each strain could be evaluated. Be-ginning treatment on the day of inoculationamplified the effects of the smallest dosage ofDDS. Because virtually all of the isolates wereinhibited from multiplication by treatment ofmice with the two larger dosages, use of thecontinuous method alone would have providedvery little additional information. Withdrawalof treatment after about 150 days, on the otherhand, permitted the distinction of degrees ofsusceptibility to the larger dosages of DDS.Pretreatment isolates of M. leprae from the
17 patients in this study were all inhibited frommultiplication by the administration to mice of10-4 g of DDS per 100 ml. The susceptibility ofthe 17 patient strains of M. leprae to smallerconcentrations of DDS was found to vary over a10-fold range: eight strains were susceptible to10-5 g of DDS per 100 ml; two strains werepartially susceptible to 10-5 g of DDS per 100ml and fully susceptible to 3 x 10-5 g of DDSper 100 ml; five strains were resistant to 10-5 gof DDS per 100 ml and fully susceptible to 3 x10-5 g of DDS per 100 ml; and two strains wereresistant to 10-5 g of DDS per 100 ml and par-tially susceptible to 3 x 10-5 g of DDS per 100ml.A by-product ofthis study is the measurement
of the minimal inhibitory concentration ofDDSfor 17 strains of M. leprae from previously un-treated patients. The mean plasma concentra-tion ofDDS obtained by administering 3 x 10-5g ofDDS per 100 ml in the mouse chow may benoted in Table 1 to be slightly smaller than 3ng of DDS per ml. Because 15 of the 17 patientstrains of M. leprae were susceptible to thisplasma concentration ofDDS, the results of thisstudy confirm earlier estimates of the minimalinhibitory concentration of DDS for M. leprae(1 to 10 ng/ml in the mouse [2,10], and 1.5 to 4ng/ml in the rat [11]).The rate at which M. leprae were rendered
noninfective for mice during treatment of these17 patients with DADDS varied as much in thisstudy as in an earlier trial of DADDS treat-ment of patients with previously untreatedlepromatous leprosy (21). No correlation co4ldbe found, however, between the rate at whichM. leprae were killed during DADDS treatmentof patients and the susceptibility of the orga-nisms to DDS in mice. Because variation of the
110 LEVY AND PETERS
DDS SUSCEPTIBILITY OF M. LEPRAE 111
rate at which M. leprae were killed could not beexplained by variation of the susceptibility ofthe organisms to DDS, some alternative expla-nation for the individual variation of the rate ofresponse to DADDS must be sought. Peters etal. have studied the metabolism of DDS andDADDS in many of these same patients andhave found no evidence of a relationship be-tween the several parameters of drug metabo-lism studied and the rate of response toDADDS (12). An explanation is implicit in thedescription by Mitchison of studies in tuber-culosis (7). These studies suggested that M.tuberculosis in stationary phase were more
resistant to mild heat treatment (53 C for 60min) than were organisms tested during loga-rithmic multiplication, and that tuberculosispatients whose sputum contained organismsmore susceptible to heat treatment respondedmore rapidly to isoniazid than did patientswhose sputum contained heat-resistant orga-nisms. The technique by which the rate of re-
sponse to DADDS was measured required re-
peated biopsies from the same lesion. All ofthe lesions in a patient with lepromatousleprosy do not appear to evolve at the samerate, some having been established for some
time and others having only recently appearedat the time that the patient presents for treat-ment. It may well be that the rate of responsetruly measures the rate at which M. leprae are
killed in a given lesion rather than in the pa-
tient as a whole, and that the response will bemore rapid when new lesions (organisms in log-arithmic phase) are sampled and less rapidwhen old lesions (organisms in stationaryphase) are biopsied. Because the organisms ob-tained from one lesion are very likely geno-typically identical with those ofany other lesionof the same patient, one should not expect a
good correlation between the susceptibility ofthe strain of M. leprae to DDS and the rateat which the organisms in a given lesion are
killed during effective antimicrobial therapy.That the M. leprae of a particular patient
are genotypically identical is suggested by theresults ofthe studies ofDDS susceptibility aftersome period of DADDS therapy, or after pas-sage through DDS-treated mice. An obviousshortcoming of the study of changes of DDSsusceptibility during DADDS therapy is thatthe most complete information will becomeavailable from those patients who respondmost slowly, whereas no organisms can be iso-lated for measurement of DDS susceptibilityonce DADDS therapy of the most rapidly re-
sponding patients has begun. Nevertheless, a
comparison of the DDS susceptibility of isolatesobtained later during DADDS therapy with
that of the pretreatment isolates suggests thatDADDS therapy does not select genotypicallymore resistant individuals in the bacterialpopulation. The studies of the organisms recov-ered from DDS-treated mice yielded similarresults. These results say nothing about DDS-resistant M. leprae (i.e., organisms that mul-tiply in mice treated with 10-4 g of DDS per100 ml), which are undoubtedly present in theuntreated patient with lepromatous leprosy butin such small numbers that they are unlikely tobe encountered among the small numbers ofM.leprae recovered from skin biopsy specimensand inoculated into mice.
ACKNOWLEDGMENTSWe are grateful to D. C. Ghoul, G. R. Gordon, J. E.
Lynch, J. F. Murray, Jr., L. P. Murray, S. M. O'Neill,and N. M. Ullmann for their capable assistance.
This research was supported by the U.S. Leprosy Panelof the U.S.-Japan Cooperative Medical Science Programadministered by the Geographic Medicine Branch, NationalInstitute of Allergy and Infectious Diseases, Bethesda, Md.(grants R22 AI 07801 and 08214, contract no. 1-Al 02283,and Interagency Agreement YO 1-Al 10004).
LITERATURE CITED
1. Bratton, A. C., and E. K. Marshall. 1939. A new cou-pling component for sulfanilamide determination. J.Biol. Chem. 128:537-550.
2. Ellard, G. A., P. T. Gammon, R. J. W. Rees, and M. F.R. Waters. 1971. Studies on the determination of theminimal inhibitory concentration of 4,4'-diamino-diphenyl-sulphone (dapsone, DDS) against Mycobac-terium leprae. Lepr. Rev. 42:101-117.
3. Glazko, A. J., W. A. Dill, R. G. Montalbo, and E. L.Holmes. 1968. A new analytical procedure fordapsone. Am. J. Trop. Med. Hyg. 17:465473.
4. Goldstein, A., 1964. Biostatistics. The Macmillan Co.,New York.
5. Levy, L. 1970. Death of Mycobacterium leprae in mice,and the additional effect of dapsone administration.Proc. Soc. Exp. Biol. Med. 135:745-749.
6. Levy, L., C. C. Shepard, and P. Fasal. 1972. Clof-azimine therapy of lepromatous leprosy caused bydapsone-resistant Mycobacterium leprae. Am. J.Trop. Med. Hyg. 21:315-321.
7. Mitchison, D. A. 1972. Current problems in thechemotherpay of tuberculosis: laboratory aspects.Trans. V.A.-Armed Forces Pulmonary Dis. Res.Cc-nf. 31:23-29.
8. Murray, J. F., Jr., G. R. Gordon, C. C. Gulledge, andJ. H. Peters. 1975. Chromatographic-fluorometricanalysis of antileprotic sulfones. J. Chromatogr.107:67-72.
9. Murray, J. F., Jr., G. R. Gordon, and J. H. Peters.1971. A chromatographic-fluorometric procedure forthe determination of nanogram quantities of anti-leprotic sulfones. J. Lab. Clin. Med. 78:464-471.
10. Ozawa, T., C. C. Shepard, and A. B. A. Karat. 1971.Application of spectrophotofluorometric procedures tosome problems in Mycobacterium leprae infections inmice and man treated with dapsone (DDS), diacetyl-DDS (DADDS), and di-formyl-DDS (DFD). Am. J.Trop. Med. Hyg. 20:274-281.
11. Peters, J. H., G. R. Gordon, J. F. Murray, Jr., A. H.Fieldsteel, and L. Levy. 1972. Minimal inhibitory con-centration of dapsone for M. leprae in rats. Int. J.Lepr. 40:467-469.
VOL. 9, 1976
ANTiMICROB. AGENTS CHEMOTHER.
12. Peters, J. H., G. R. Gordon, J. F. Murray, Jr., andL. Levy. 1974. Metabolic disposition versus thera-peutic response to acedapsone. Int. J. Lepr. 42: 375-.376.
13. Peters, J. H., G. R. Gordon, J. F. Murray, Jr., L.Levy, D. A. Russell, and C. C. Shepard. 1974.Acedapeone treatment of leprosy: metabolic disposi-tion versus therapeutic response. Int. J. Lepr. 42:503-504.
14. Peters, J. H., S. C. Lin, and L. Levy. 1969. A rapidqualitative spot test for the detection of dapeone inurine. Int. J. Lepr. 37:46-51.
15. Shepard, C. C. 1960. The experimental disease thatfollows the injection of human leprosy bacilli intofootpads of mice. J. Exp. Med. 112:445-454.
16. Shepard, C. C. 1967. Activity of repository sulfonesagainst Mycobacterium leprae in mice. Proc. Soc. Exp.Biol. Med. 124:430-433.
17. Shepard, C. C. 1969. Further experience with thekinetic method for the study of drugs against Myco-bacterium leprae in mice. Int. J. Lepr. 37:389-397.
18. Shepard, C. C. 1971. A survey of the drugs with activ-ity against M. keprae in mice. Int. J. Lepr. 39:.340-348.
19. Shepard, C. C., L. Levy, and P. Fasal. 1968. The deathof Mycobacterium leprae during treatment with4,4'-diaminodiphenylsulfone (DDS). Initial rate in pa-tients. Am. J. Trop. Med. Hyg. 17:769-775.
20. Shepard, C. C., L. Levy, and P. Fasal. 1969. The sensi-tivity to dapsone of Mycobacterium leprae from pa-
tients with and without previous treatment. Am. J.Trop. Med. Hyg. 18:258-263.
21. Shepard, C. C., L. Levy, and P. Fasal. 1972. The deathrate of Mycobacterium leprae during treatment oflepromatous leprosy with acedapsone (DADDS). Am.J. Trop. Med. Hyg. 21:440445.
22. Shepard, C. C., L. Levy, and P. Fasal. 1972. Rapidbactericidal effect of rifampin on Mycobacteriumleprae. Am. J. Trop. Med. Hyg. 21:446-449.
23. Shepard, C. C., L. Levy, and P. Fasal. 1974. Furtherexperience with the rapid bactericidal effect ofrifampin on M. leprae. Am. J. Trop. Med. Hyg. 23:1120-1130.
24. Shepard, C. C., and D. H. McRae. 1968. A method forcounting acid-fast bacteria. Int. J. Lepr. 36:78-82.
25. Shepard, C. C., J. G. Tolentino, and D. H. McRae.1968. The therapeutic effect of 4,4'-diacetyldiamino-diphenylsulfone (DADDS) in leprosy. Am. J. Trop.Med. Hyg. 17:192-201.
26. Thompson, P. E., B. Olsewwski, and J. A. Waitz. 1965.Laboratory studies on the repository antimalarial ac-tivity of 4,4'-diacetylaminodiphenylsulfone, aloneand mixed with cycloguanil pamoate (Cl-50l). Am. J.Trop. Med. Hyg. 14:343-353.
27. U.S. Leprosy Panel (U.S.-Japan Cooperative MedicalScience Program) and the Leonard Wood Memorial(Collaborative effort). 1975. Rifampin therapy oflepromatous leprosy. Am. J. Trop. Med. Hyg. 24:475-484.
112 LEVY AND PETERS