
Survival after conservative (palliative) management of pleural malignant mesothelioma
4
Journal of Surgical Oncology 2001;78:171–174 Survival After Conservative (Palliative) Management of Pleural Malignant Mesothelioma NEIL MERRITT, MD, CHRISTOPHER J. BLEWETT, MD, JOHN D. MILLER, MD, W. FREDERICK BENNETT, MD, J. EDWARD M. YOUNG, MD, AND JOHN D. URSCHEL, MD* Department of Surgery, McMaster University, Hamilton, Ontario, Canada Background and Objectives: Malignant mesothelioma is a lethal disease. Aggressive multimodality treatment protocols are reportedly associated with improved survival, but the apparent survival benefits may simply reflect patient selection and the variable natural history of this malignancy. Before embarking on our own protocol of experimental treatment for mesothelioma, we sought to identify important prognostic factors and document the survival of patients treated conservatively (with palliative intent only) in our region. Methods: We performed a retrospective review of all patients with a diagnosis of malignant mesothelioma seen at our center between 1987 and 1999. Since curative intent treatment had not been given, we assumed that measured survival would largely reflect the natural history of the malignancy. Results: There were 101 patients (80 males and 21 females). Mean age was 65 9.2 years. Symptoms of disease were present for a median time of 5 months before the diagnosis was established. The most common presenting symptoms were dyspnea (46 patients), chest pain (30 patients), and weight loss (22 patients). Sixty-eight patients (68%) had a history of asbestos exposure. Mesothelioma subtypes included epithelial (43 patients), sarcomatous (26 patients), mixed (19 patients), desmoplastic (4 patients), and unspecified (9 patients). All 101 patients were treated with palliative intent. Talc pleurodesis was performed in 70 patients. At the time of analysis, 90 patients had died and 11 remained alive. Median survival was 213 (95% CI 137–289) days. Survival for the three major histological subtypes was significantly different (log rank, P 0.0016). Histological subtype (epithelial favorable) was the only significant indepen- dent prognostic factor (Cox proportional hazard regression, P 0.0009). Conclusions: Patients with epithelial mesothelioma survive longer than those with other histological subtypes. Conservatively managed patients with pleural malignant mesothelioma have a median survival of approxi- mately 7 months. These data from conservatively treated patients can serve as baseline information for future studies of experimental treatments. J. Surg. Oncol. 2001;78:171–174. ß 2001 Wiley-Liss, Inc. KEY WORDS: mesothelioma; pleural neoplasms; prognosis; survival analysis; natural history INTRODUCTION Malignant mesothelioma of the pleura is a lethal malignancy for which, there is no standard treatment [1,2]. Innovative treatment strategies continue to be *Correspondence to: John D. Urschel, MD, Department of Surgery, St. Joseph’s Hospital, 50 Charlton Ave East, Hamilton, Ontario, Canada L8N 4A6. FAX: 905-521-6190. E-mail: [email protected] Accepted 30 July 2001 ß 2001 Wiley-Liss, Inc.
-
Upload
neil-merritt -
Category
Documents
-
view
213 -
download
1
Transcript of Survival after conservative (palliative) management of pleural malignant mesothelioma

Journal of Surgical Oncology 2001;78:171±174
Survival After Conservative (Palliative) Management ofPleural Malignant Mesothelioma
NEIL MERRITT, MD, CHRISTOPHER J. BLEWETT, MD, JOHN D. MILLER, MD, W. FREDERICK BENNETT, MD,J. EDWARD M. YOUNG, MD, AND JOHN D. URSCHEL, MD*
Department of Surgery, McMaster University, Hamilton, Ontario, Canada
Background and Objectives: Malignant mesothelioma is a lethal disease.Aggressive multimodality treatment protocols are reportedly associatedwith improved survival, but the apparent survival bene®ts may simplyre¯ect patient selection and the variable natural history of this malignancy.Before embarking on our own protocol of experimental treatment formesothelioma, we sought to identify important prognostic factors anddocument the survival of patients treated conservatively (with palliativeintent only) in our region.Methods: We performed a retrospective review of all patients with adiagnosis of malignant mesothelioma seen at our center between 1987 and1999. Since curative intent treatment had not been given, we assumed thatmeasured survival would largely re¯ect the natural history of themalignancy.Results: There were 101 patients (80 males and 21 females). Mean agewas 65� 9.2 years. Symptoms of disease were present for a median time of5 months before the diagnosis was established. The most commonpresenting symptoms were dyspnea (46 patients), chest pain (30 patients),and weight loss (22 patients). Sixty-eight patients (68%) had a historyof asbestos exposure. Mesothelioma subtypes included epithelial(43 patients), sarcomatous (26 patients), mixed (19 patients), desmoplastic(4 patients), and unspeci®ed (9 patients). All 101 patients were treatedwith palliative intent. Talc pleurodesis was performed in 70 patients. At thetime of analysis, 90 patients had died and 11 remained alive. Mediansurvival was 213 (95% CI 137±289) days. Survival for the three majorhistological subtypes was signi®cantly different (log rank, P� 0.0016).Histological subtype (epithelial favorable) was the only signi®cant indepen-dent prognostic factor (Cox proportional hazard regression, P� 0.0009).Conclusions: Patients with epithelial mesothelioma survive longer thanthose with other histological subtypes. Conservatively managed patientswith pleural malignant mesothelioma have a median survival of approxi-mately 7 months. These data from conservatively treated patients can serveas baseline information for future studies of experimental treatments.J. Surg. Oncol. 2001;78:171±174. ß 2001 Wiley-Liss, Inc.
KEY WORDS: mesothelioma; pleural neoplasms; prognosis; survival analysis;natural history
INTRODUCTION
Malignant mesothelioma of the pleura is a lethalmalignancy for which, there is no standard treatment[1,2]. Innovative treatment strategies continue to be
*Correspondence to: John D. Urschel, MD, Department of Surgery,St. Joseph's Hospital, 50 Charlton Ave East, Hamilton, Ontario, CanadaL8N 4A6. FAX: 905-521-6190. E-mail: [email protected]
Accepted 30 July 2001
ß 2001 Wiley-Liss, Inc.

developed and tested. Some investigators have usedaggressive multimodality treatment approaches andreported encouraging phase II survival data [3±5].However, it is possible that patient selection couldbe responsible for the survival bene®ts attributed toaggressive treatment [6,7]. Before embarking on ourown protocol of aggressive experimental treatment formalignant mesothelioma, we sought to identify importantprognostic factors, and document the natural history ofpatients treated conservatively, with palliative intent only,in our region. Such data could then serve as a baselinefor future comparisons.
MATERIALS AND METHODS
The Hamilton Regional Cancer Centre and St. Joseph'sHospital in Hamilton, Ontario, Canada, are regionalreferral centers for cancer care (medical and radiationoncology) and thoracic surgical oncology, respectively.Our centers serve a population of 1.8 million people.A retrospective review was carried out to identify allpatients with a diagnosis of malignant mesothelioma ofthe pleura seen at our centers between 1987 and 1999.During this time period, patients with mesothelioma weretreated conservatively, with palliative intent only. Chartswere reviewed from the cancer centre, hospital, andsurgeons' of®ces. In addition, living patients werecontacted by telephone. Data was collected on age,sex, asbestos exposure, symptoms, diagnostic methods,histology, stage, palliative treatments, and survival.Since, curative intent treatment had not been given, weassumed that the observed survival would largely re¯ectthe natural history of the malignancy.
Statistical analysis was done, using SPSS 9.0 software(SPSS, Chicago, IL). General data are presented asmean�SD. Survival (Kaplan±Meier) data are presentedas median survival in days with 95% con®dence intervals(CI) provided. Comparisons of survival were done usingthe log-rank test to evaluate equality of Kaplan±Meiersurvival distributions. Cox proportional hazards regres-sion model was used to identify independent predictors ofsurvival. A P< 0.05 was taken to indicate signi®cance.
RESULTS
One hundred and one patients were diagnosed withmalignant mesothelioma of the pleura at our centersbetween 1987 and 1999. There were 80 males and21 females. Age at diagnosis ranged from 43±84 years,with a mean of 65� 9.2 years. Symptoms of disease werepresent for a median time of 5 months, before thediagnosis was established. The most common present-ing symptoms were dyspnea (46 patients), chest pain(30 patients), and weight loss (22 patients). Sixty-eightpatients (68%) had a history of asbestos exposure.
All patients were diagnosed by surgical biopsies(thoracoscopy or open pleural biopsy). The diagnosis ofmalignant mesothelioma was established, using lightmicroscopy and immunohistochemistry. Malignantmesothelioma subtype histology was speci®ed in 92 of101 patients. Forty-three patients had epithelial, 26 hadsarcomatous, 19 had mixed, and 4 had desmoplasticmesotheliomas. The attending clinicians did not rigor-ously stage the patients at time of diagnosis, and wecould not accurately stage the patients with con®dence inretrospect. Therefore, data on stage of disease are notpresented.
All 101 patients were treated with palliative intent.No aggressive surgical interventions, with curative intent,were performed. Talc pleurodesis, by chest tube slurry oroperative poudrage, was performed in 70 patients. Thirtypatients received radiotherapy in attempt to controlsymptoms such as chest pain. Only 2 of these patientsreceived over 20 Gy. Nine patients received chemother-apy, usually as a radiosensitizer.
At the time of analysis, 90 patients had died and11 remained alive. Median survival was 213 (95% CI137±289) days (Fig. 1). Palliative treatments, such aspleurodesis, radiotherapy, and chemotherapy, had nosigni®cant impact on survival (P� 0.59). Median survi-val, according to histology was 239 (95% CI 58±420)days in epithelial, 83 (95% CI 39±127) days insarcomatous, and 264 (95% CI 191±337) days in mixedmesothelioma (log rank, P� 0.0016). Although, themixed mesothelioma histology group had a slightlylonger median survival than the other groups, patientswith epithelial histology had the highest one-year andlong-term survival (Fig. 2). Comparisons of survival forthe desmoplastic and unspeci®ed histology subgroups
Fig. 1. Kaplan±Meier survival curve for malignant mesothelioma.
172 Merritt et al.
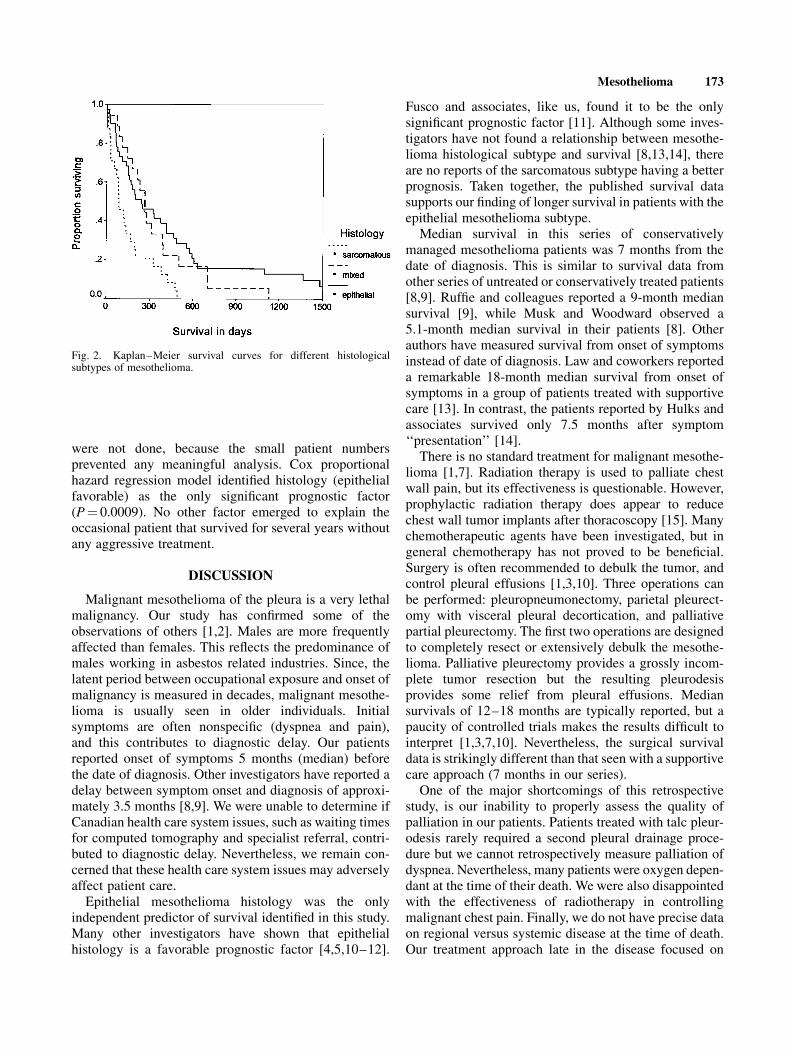
were not done, because the small patient numbersprevented any meaningful analysis. Cox proportionalhazard regression model identi®ed histology (epithelialfavorable) as the only signi®cant prognostic factor(P� 0.0009). No other factor emerged to explain theoccasional patient that survived for several years withoutany aggressive treatment.
DISCUSSION
Malignant mesothelioma of the pleura is a very lethalmalignancy. Our study has con®rmed some of theobservations of others [1,2]. Males are more frequentlyaffected than females. This re¯ects the predominance ofmales working in asbestos related industries. Since, thelatent period between occupational exposure and onset ofmalignancy is measured in decades, malignant mesothe-lioma is usually seen in older individuals. Initialsymptoms are often nonspeci®c (dyspnea and pain),and this contributes to diagnostic delay. Our patientsreported onset of symptoms 5 months (median) beforethe date of diagnosis. Other investigators have reported adelay between symptom onset and diagnosis of approxi-mately 3.5 months [8,9]. We were unable to determine ifCanadian health care system issues, such as waiting timesfor computed tomography and specialist referral, contri-buted to diagnostic delay. Nevertheless, we remain con-cerned that these health care system issues may adverselyaffect patient care.
Epithelial mesothelioma histology was the onlyindependent predictor of survival identi®ed in this study.Many other investigators have shown that epithelialhistology is a favorable prognostic factor [4,5,10±12].
Fusco and associates, like us, found it to be the onlysigni®cant prognostic factor [11]. Although some inves-tigators have not found a relationship between mesothe-lioma histological subtype and survival [8,13,14], thereare no reports of the sarcomatous subtype having a betterprognosis. Taken together, the published survival datasupports our ®nding of longer survival in patients with theepithelial mesothelioma subtype.
Median survival in this series of conservativelymanaged mesothelioma patients was 7 months from thedate of diagnosis. This is similar to survival data fromother series of untreated or conservatively treated patients[8,9]. Ruf®e and colleagues reported a 9-month mediansurvival [9], while Musk and Woodward observed a5.1-month median survival in their patients [8]. Otherauthors have measured survival from onset of symptomsinstead of date of diagnosis. Law and coworkers reporteda remarkable 18-month median survival from onset ofsymptoms in a group of patients treated with supportivecare [13]. In contrast, the patients reported by Hulks andassociates survived only 7.5 months after symptom`̀ presentation'' [14].
There is no standard treatment for malignant mesothe-lioma [1,7]. Radiation therapy is used to palliate chestwall pain, but its effectiveness is questionable. However,prophylactic radiation therapy does appear to reducechest wall tumor implants after thoracoscopy [15]. Manychemotherapeutic agents have been investigated, but ingeneral chemotherapy has not proved to be bene®cial.Surgery is often recommended to debulk the tumor, andcontrol pleural effusions [1,3,10]. Three operations canbe performed: pleuropneumonectomy, parietal pleurect-omy with visceral pleural decortication, and palliativepartial pleurectomy. The ®rst two operations are designedto completely resect or extensively debulk the mesothe-lioma. Palliative pleurectomy provides a grossly incom-plete tumor resection but the resulting pleurodesisprovides some relief from pleural effusions. Mediansurvivals of 12±18 months are typically reported, but apaucity of controlled trials makes the results dif®cult tointerpret [1,3,7,10]. Nevertheless, the surgical survivaldata is strikingly different than that seen with a supportivecare approach (7 months in our series).
One of the major shortcomings of this retrospectivestudy, is our inability to properly assess the quality ofpalliation in our patients. Patients treated with talc pleur-odesis rarely required a second pleural drainage proce-dure but we cannot retrospectively measure palliation ofdyspnea. Nevertheless, many patients were oxygen depen-dant at the time of their death. We were also disappointedwith the effectiveness of radiotherapy in controllingmalignant chest pain. Finally, we do not have precise dataon regional versus systemic disease at the time of death.Our treatment approach late in the disease focused on
Fig. 2. Kaplan±Meier survival curves for different histologicalsubtypes of mesothelioma.
Mesothelioma 173

symptom control, as opposed to active investigation andtreatment of malignancy.
Given the dismal results of mesothelioma treatmentmany innovative treatment strategies have been devel-oped [7]. Some treatment protocols combine surgerywith one or more additional treatment modalities. Thesenovel treatment approaches include pleuropneumonect-omy followed by chemoradiotherapy [4], pleurectomyor pleuropneumonectomy combined with intracavitaryphotodynamic therapy [5,6], and surgery combinedwith gene therapy [16]. Reported median survivals withthese treatments vary with stage. Sugarbaker and colle-agues reported an overall median survival (all stages) of19 months after pleuropneumonectomy followed bychemoradiotherapy [4]. Surgery combined with intraca-vitary photodynamic therapy was associated with a 14±15 month median survival (all stages) at two institutions(Roswell Park Cancer Institute, Buffalo, NY, andNational Institutes of Health, Bethesda, MD) investigat-ing this treatment [5,6].
CONCLUSIONS
Our study of conservatively managed patients withpleural malignant mesothelioma showed a mediansurvival of approximately 7 months, with epithelial histo-logy, being the only signi®cant prognostic factor. Thissurvival is clearly inferior to that reported after surgicalresection, or surgical resection in the context of multi-modality treatment. Although, aggressive treatmentappears to result in a modest prolongation of survivalthis apparent survival bene®t could be explained bypatient selection. A randomized trial would be needed tode®nitively show that active treatment was superior tosupportive care, but it seems unlikely that such a trialcould be mounted. Therefore, contemporary supportivecare data such as ours may still be useful; the data servesas baseline information for future studies of experimentaltreatments. This data may be especially valuable in thefuture, if we successfully change our regional manage-ment strategy, and introduce an aggressive treatmentprotocol for malignant mesothelioma.
REFERENCES
1. Rusch VW: Clinical features and current treatment of diffusemalignant pleural mesothelioma. Lung Cancer 1995;12 (Suppl 2):S127±S146.
2. Moskal TL, Urschel JD, Anderson TM, et al.: Malignantpleural mesothelioma: a problematic review. Surg Oncol 1998;7:5±12.
3. Rusch VW, Piantadosi S, Holmes EC: The role of extrapleuralpneumonectomy in malignant pleural mesothelioma. A LungCancer Study Group trial. J Thorac Cardiovasc Surg 1991;102:1±9.
4. Sugarbaker DJ, Flores RM, Jaklitsch MT, et al.: Resectionmargins, extrapleural nodal status, and cell type determinepostoperative long-term survival in trimodality therapy ofmalignant pleural mesothelioma: results in 183 patients. J ThoracCardiovasc Surg 1999;117:54±65.
5. Moskal TL, Dougherty TJ, Urschel JD, et al.: Operation andphotodynamic therapy for pleural mesothelioma: 6-year follow-up. Ann Thorac Surg 1998;66:1128±1133.
6. Pass HI, Temeck BK, Kranda K, et al.: Phase III randomized trialof surgery with or without intraoperative photodynamic therapyand postoperative immunochemotherapy for malignant pleuralmesothelioma. Ann Surg Oncol 1997;4:628±633.
7. Boylan AM: Mesothelioma: new concepts in diagnosis andmanagement. Curr Opin Pulm Med 2000;6:157±163.
8. Musk AW, Woodward SD: Conventional treatment and its effecton survival of malignant pleural mesothelioma in WesternAustralia. Aust N Z J Med 1982;12:229±232.
9. Ruf®e P, Feld R, Minkin S, et al.: Diffuse malignant mesotheliomaof the pleura in Ontario and Quebec: a retrospective study of 332patients. J Clin Oncol 1989;7:1157±1168.
10. Rusch VW, Venkatraman ES: Important prognostic factors inpatients with malignant pleural mesothelioma, managed surgi-cally. Ann Thorac Surg 1999;68:1799±1804.
11. Fusco V, Ardizzoni A, Merlo F, et al.: Malignant pleuralmesothelioma. Multivariate analysis of prognostic factors on113 patients. Anticancer Res 1993;13:683±689.
12. Curran D, Sahmoud T, Therasse P, et al.: Prognostic factors inpatients with pleural mesothelioma: the European Organizationfor Research and Treatment of Cancer experience. J Clin Oncol1998;16:145±152.
13. Law MR, Gregor A, Hodson ME, et al.: Malignant mesotheliomaof the pleura: a study of 52 treated and 64 untreated patients.Thorax 1984;39:255±259.
14. Hulks G, Thomas JS, Waclawski E: Malignant pleural meso-thelioma in western Glasgow 1980±1986. Thorax 1989;44:496±500.
15. Boutin C, Rey F, Viallat JR: Prevention of malignant seeding afterinvasive diagnostic procedures in patients with pleural mesothe-lioma. A randomized trial of local radiotherapy. Chest 1995;108:754±758.
16. Sterman DH, Kaiser LR, Albelda SM: Gene therapy for malignantpleural mesothelioma. Hematol Oncol Clin North Am 1998;12:553±568.
174 Merritt et al.


















