Surgical Procedure Joining the Lateral Rectus and Superior Rectus ...
6
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX 1 Surgical Procedure Joining the Lateral Rectus and Superior Rectus Muscles With or Without Medial Rectus Recession for the Treatment of Strabismus Associated With High Myopia Serpil Akar, MD; Birsen Gokyigit, MD; Erkin Aribal, MD; Abdulvahit Demir, MD; Yasin Sakir Göker, MD; Ahmet Demirok From the Department of Pediatric Ophthalmology and Strabismus (SA, BG), Prof. Dr. N. Resat Belger Beyoglu Education and Research Eye Hospital (ADemir, YSG, ADemirok), Istanbul, Turkey; and the Department of Radiology, Marmara University Hospital School of Medicine, Istanbul, Turkey (EA). Submitted: March 6, 2013; Accepted: October 10, 2013; Posted online: November 26, 2013 The authors have no financial or proprietary interest in the materials presented herein. Correspondence: Serpil Akar, MD, Acibadem cad, Yurtsever sok. Alsancak sitesi, E Blk, Da:19 Acibadem/Kadikoy/ Istanbul, Turkey. E-mail: akarserpil@ yahoo.com doi: 10.3928/01913913-20131119-01 ABSTRACT Purpose: To evaluate the outcomes of a surgical pro- cedure involving the muscle union of the superior rec- tus (SR) and lateral rectus (LR) muscles with or without medial rectus (MR) recession for the treatment of stra- bismus associated with high myopia and the anatomic changes from before and after surgery. Methods: Thirty-five eyes of 20 patients who had un- dergone a muscle union of the SR and LR muscles with or without MR recession for treatment of acquired stra- bismus associated with an inferior displacement of the LR and nasal displacement of the SR in magnetic reso- nance imaging of the orbit due to axial high myopia were observed prospectively. Main outcome measures were the angles of the dislocation of the globe, angles of horizontal or vertical deviations, abductions, and su- praductions. The angles of the dislocation of the globe were analyzed using magnetic resonance imaging (1.5 Tesla Magnet; Siemens Symphonia, Munich, Germany). Results: The axial lengths ranged from 26 to 36 mm (mean: 30.6 ± 2.8 mm). The angle of dislocation of the globe changed from 178º ± 10º to 101º ± 6º, the angle of esotropia changed from 58.6 ± 2.5 to 6.8 ± 1.4 prism diopters (PD); and the angle of hypotropia changed from 12.5 ± 1.3 to 3.3 ± 1.1 PD postoperatively. Ab- duction and supraduction improved significantly after surgery. At the 4-year follow-up, the postoperative out- comes were stable. Conclusions: In the treatment of strabismus caused by high myopia, the surgical procedure involving the muscle union of the SR and LR muscles with or without MR recession was effective on both the restoration of the dislocated globe into the muscle cone and the im- provement of ocular motility. [J Pediatr Ophthalmol Strabismus 20XX;XX(X):XX- XX.] INTRODUCTION Adult patients with unilateral or bilateral high axial myopia may acquire a typical restrictive mo- tility disorder associated with obvious esodeviation and hypodeviation named strabismus fixus conver- gens. 1-4 The exact mechanism is not well under- stood, but several studies have noted a superotem- poral herniation of the elongated eyeball beyond the muscle cone in the orbit. 2,3 Surgical management of myopic strabismus fixus is complex. 4 Conventional maneuvers are resection- recession procedures that mainly affect muscle forc- es. 5,6 Modified procedures include transposition tech- niques that alter the muscle paths. 4,7-10 Yokoyama et
Transcript of Surgical Procedure Joining the Lateral Rectus and Superior Rectus ...
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX 1
Surgical Procedure Joining the Lateral Rectus and Superior Rectus Muscles With or Without Medial Rectus Recession for the Treatment of Strabismus Associated With High Myopia
Serpil Akar, MD; Birsen Gokyigit, MD; Erkin Aribal, MD; Abdulvahit Demir, MD; Yasin Sakir Göker, MD; Ahmet Demirok
From the Department of Pediatric Ophthalmology and Strabismus (SA, BG), Prof. Dr. N. Resat Belger Beyoglu Education and Research Eye Hospital (ADemir, YSG, ADemirok), Istanbul, Turkey; and the Department of Radiology, Marmara University Hospital School of Medicine, Istanbul, Turkey (EA).
Submitted: March 6, 2013; Accepted: October 10, 2013; Posted online: November 26, 2013The authors have no financial or proprietary interest in the materials presented herein.Correspondence: Serpil Akar, MD, Acibadem cad, Yurtsever sok. Alsancak sitesi, E Blk, Da:19 Acibadem/Kadikoy/ Istanbul, Turkey. E-mail: akarserpil@
yahoo.comdoi: 10.3928/01913913-20131119-01
ABSTRACT
Purpose: To evaluate the outcomes of a surgical pro-cedure involving the muscle union of the superior rec-tus (SR) and lateral rectus (LR) muscles with or without medial rectus (MR) recession for the treatment of stra-bismus associated with high myopia and the anatomic changes from before and after surgery.
Methods: Thirty-five eyes of 20 patients who had un-dergone a muscle union of the SR and LR muscles with or without MR recession for treatment of acquired stra-bismus associated with an inferior displacement of the LR and nasal displacement of the SR in magnetic reso-nance imaging of the orbit due to axial high myopia were observed prospectively. Main outcome measures were the angles of the dislocation of the globe, angles of horizontal or vertical deviations, abductions, and su-praductions. The angles of the dislocation of the globe were analyzed using magnetic resonance imaging (1.5 Tesla Magnet; Siemens Symphonia, Munich, Germany).
Results: The axial lengths ranged from 26 to 36 mm (mean: 30.6 ± 2.8 mm). The angle of dislocation of the globe changed from 178º ± 10º to 101º ± 6º, the angle of esotropia changed from 58.6 ± 2.5 to 6.8 ± 1.4 prism diopters (PD); and the angle of hypotropia changed from 12.5 ± 1.3 to 3.3 ± 1.1 PD postoperatively. Ab-duction and supraduction improved significantly after surgery. At the 4-year follow-up, the postoperative out-comes were stable.
Conclusions: In the treatment of strabismus caused by high myopia, the surgical procedure involving the muscle union of the SR and LR muscles with or without MR recession was effective on both the restoration of the dislocated globe into the muscle cone and the im-provement of ocular motility.
[J Pediatr Ophthalmol Strabismus 20XX;XX(X):XX-XX.]
INTRODUCTIONAdult patients with unilateral or bilateral high
axial myopia may acquire a typical restrictive mo-tility disorder associated with obvious esodeviation and hypodeviation named strabismus fixus conver-gens.1-4 The exact mechanism is not well under-stood, but several studies have noted a superotem-
poral herniation of the elongated eyeball beyond the muscle cone in the orbit.2,3
Surgical management of myopic strabismus fixus is complex.4 Conventional maneuvers are resection-recession procedures that mainly affect muscle forc-es.5,6 Modified procedures include transposition tech-niques that alter the muscle paths.4,7-10 Yokoyama et

2 Copyright © SLACK Incorporated
al.8 and Yamaguchi et al.11 described a surgical proce-dure involving the muscle union of the superior rec-tus (SR) and lateral rectus (LR) muscles to restore the dislocated globe back to the muscle cone.
The purpose of this study was to evaluate the outcomes of a surgical procedure involving the mus-cle union of the SR and LR muscles with or with-out medial rectus (MR) recession for the treatment of strabismus associated with high myopia and the anatomic changes from before and after surgery.
PATIENTS AND METHODSThis was a single-center, prospective, consecu-
tive cohort study. Approval from the Ethics Com-mittee and the Institutional Review Board at the Prof. Dr. N. Resat Belger Beyoglu Education and Research Eye Hospital, Istanbul, Turkey, was ob-tained. Informed consent was obtained from each participant. The study and data collection con-formed to all local laws and was compliant with the tenets of the Declaration of Helsinki.
The study population consisted of patients who underwent surgery to unite the muscle bellies of the LR and SR muscles with or without MR recession for treatment of acquired progressive esotropia-hypot-ropia associated with high myopia. All procedures were performed at Prof. Dr. N. Resat Belger Beyoglu Education and Research Eye Hospital between July 2005 and January 2009. Patients fulfilling the fol-lowing criteria were included in the study: axial high myopia (axial length longer than 27 mm), acquired strabismus (esotropia-hypotropia) associated with an inferior displacement of the LR muscle, and nasal displacement of the SR muscle in magnetic resonance imaging (MRI) of the orbit. Patients with neurological or developmental disorders and those who had undergone previous strabismus surgery were excluded from the study. Originally, this study was designed with a 4-year follow-up after surgery. No patients meeting the inclusion criteria were ex-cluded from the study during the study period.
Before surgical intervention, all patients re-ceived complete ophthalmic and orthoptic exami-nations. The angle of ocular deviation was measured by the alternate prism cover test at 6 and 0.33 m with the patient’s optimum myopic correction. For patients in whom neither eye could abduct past the midline, the Krimsky test was used with prisms placed in front of both eyes. The limitation of ocular movements was divided into four grades
(-1 = minimal limitation, -4 = no movement toward and/or beyond the primary position).4,9,10 A- and B-scan echography (Ocuscan; Alcon Laboratories, Inc., Fort Worth, TX) were performed in all patients to determine the axial length of the globes.
The orbits of all patients were imaged using MRI (1.5 Tesla Magnet, Siemens Symphonia, Mu-nich, Germany). High-resolution coronal and axial T2-weighted spin echo images were obtained with the following settings: repetition time = 550 ms and echo time = 15 ms, field of view = 21 3 21 cm, pixel matrix = 256 3 512, three acquisitions, slice thick-ness 3 mm, and distance factor 0.25. All patients were instructed to remain still in the infraducted eye position. We tried to avoid the influence of gaze position on the anatomic relationships between the globe and extraocular muscles. Therefore, we con-trolled the gaze at the same position in all patients. As suggested by Yokoyama et al.8 and Yamaguchi et al.,11 we used infraduction to analyze the results of MRI for every patient under the same conditions.
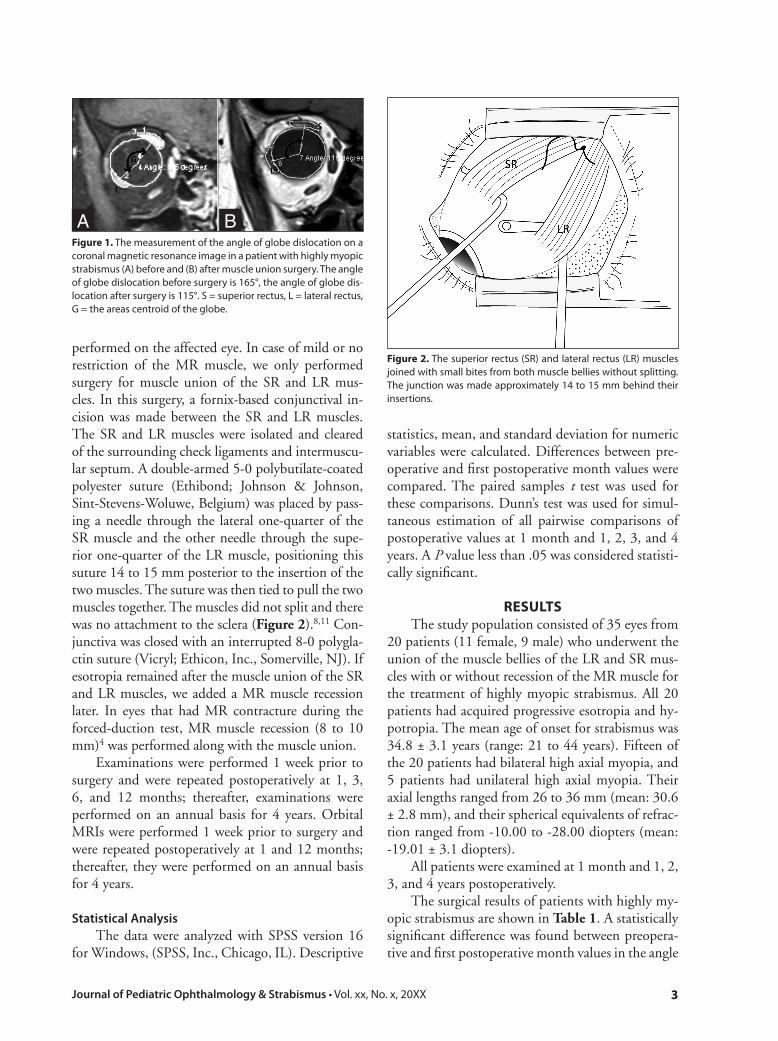
For the orbital measurement, we used a coronal slice image 9-mm anterior to the globe-optic nerve junction in each orbit to avoid any influence of globe shape, such as staphyloma. On this slice image, we first traced the outlines of the cross-sectional orbits and the SR and LR muscles and then the area centroid of each object was determined using the XY center tool of the Syngo via postprocessing software (Siemens A.G., Munich, Germany). Lines were drawn between the orbital centroid and each extraocular muscle (LR and SR) centroid. As recommended by Yokoyama et al.8 and Yamaguchi et al.11 the angle of dislocation of the globe was defined as the angle formed by a line connecting the area centroid of the SR muscle and the globe and another line connecting the area cen-troid of the LR muscle and the globe (including the superior temporal quadrant of the orbit) (Figure 1).
The forced-duction test under general anesthe-sia for verifying restriction preoperatively was ap-plied for all cases. Forced-duction testing was grad-ed on a 3-point scale as mild, moderate, or severe.12 The forced-duction test was performed again post-operatively.
Surgical TechniqueThe surgical approach was conducted according
to the previous description by Yokoyama et al.8 All surgeries were performed under general anesthesia. As an initial procedure, the forced-duction test was
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX 3
performed on the affected eye. In case of mild or no restriction of the MR muscle, we only performed surgery for muscle union of the SR and LR mus-cles. In this surgery, a fornix-based conjunctival in-cision was made between the SR and LR muscles. The SR and LR muscles were isolated and cleared of the surrounding check ligaments and intermuscu-lar septum. A double-armed 5-0 polybutilate-coated polyester suture (Ethibond; Johnson & Johnson, Sint-Stevens-Woluwe, Belgium) was placed by pass-ing a needle through the lateral one-quarter of the SR muscle and the other needle through the supe-rior one-quarter of the LR muscle, positioning this suture 14 to 15 mm posterior to the insertion of the two muscles. The suture was then tied to pull the two muscles together. The muscles did not split and there was no attachment to the sclera (Figure 2).8,11 Con-junctiva was closed with an interrupted 8-0 polygla-ctin suture (Vicryl; Ethicon, Inc., Somerville, NJ). If esotropia remained after the muscle union of the SR and LR muscles, we added a MR muscle recession later. In eyes that had MR contracture during the forced-duction test, MR muscle recession (8 to 10 mm)4 was performed along with the muscle union.
Examinations were performed 1 week prior to surgery and were repeated postoperatively at 1, 3, 6, and 12 months; thereafter, examinations were performed on an annual basis for 4 years. Orbital MRIs were performed 1 week prior to surgery and were repeated postoperatively at 1 and 12 months; thereafter, they were performed on an annual basis for 4 years.
Statistical AnalysisThe data were analyzed with SPSS version 16
for Windows, (SPSS, Inc., Chicago, IL). Descriptive
statistics, mean, and standard deviation for numeric variables were calculated. Differences between pre-operative and first postoperative month values were compared. The paired samples t test was used for these comparisons. Dunn’s test was used for simul-taneous estimation of all pairwise comparisons of postoperative values at 1 month and 1, 2, 3, and 4 years. A P value less than .05 was considered statisti-cally significant.
RESULTSThe study population consisted of 35 eyes from
20 patients (11 female, 9 male) who underwent the union of the muscle bellies of the LR and SR mus-cles with or without recession of the MR muscle for the treatment of highly myopic strabismus. All 20 patients had acquired progressive esotropia and hy-potropia. The mean age of onset for strabismus was 34.8 ± 3.1 years (range: 21 to 44 years). Fifteen of the 20 patients had bilateral high axial myopia, and 5 patients had unilateral high axial myopia. Their axial lengths ranged from 26 to 36 mm (mean: 30.6 ± 2.8 mm), and their spherical equivalents of refrac-tion ranged from -10.00 to -28.00 diopters (mean: -19.01 ± 3.1 diopters).
All patients were examined at 1 month and 1, 2, 3, and 4 years postoperatively.
The surgical results of patients with highly my-opic strabismus are shown in Table 1. A statistically significant difference was found between preopera-tive and first postoperative month values in the angle
Figure 1. The measurement of the angle of globe dislocation on a coronal magnetic resonance image in a patient with highly myopic strabismus (A) before and (B) after muscle union surgery. The angle of globe dislocation before surgery is 165°, the angle of globe dis-location after surgery is 115°. S = superior rectus, L = lateral rectus, G = the areas centroid of the globe.
A B
Figure 2. The superior rectus (SR) and lateral rectus (LR) muscles joined with small bites from both muscle bellies without splitting. The junction was made approximately 14 to 15 mm behind their insertions.
4 Copyright © SLACK Incorporated
of globe dislocation (P = .001). Figure 1 shows the measurement of the angle of globe dislocation in a patient with highly myopic strabismus. There were statistically significant differences between preop-erative and first postoperative month values in the angles of horizontal and vertical deviations (P = .001 and .049, respectively). A statistically significant dif-ference was found between preoperative and first postoperative month values in abduction and supra-duction (P = .001 and .038, respectively).
No significant differences were found between 1 month and 1, 2, 3, and 4 years postoperatively, which reflects the stability of improvements in the angle of globe dislocation, the angles of horizontal and vertical deviation abduction, and supraduction after surgery (P > .05 for each comparison).
The forced-duction test revealed positive results (severe or moderate restriction) in the abduction of 24 eyes of 13 patients before surgery. The MR reces-sion was performed at the same time as the muscle union in these 24 eyes. After surgery, a forced-duc-tion test in these eyes demonstrated negative results in abduction. Nine eyes were cured only by uniting the SR and LR muscles. We recessed the MR muscle 5 to 9 months later in 2 eyes of 2 patients because they remained esotropic despite the union of the SR and LR muscles. Two patients had -1 adduction after larger MR recession operation.
No intraoperative or postoperative complica-tions occurred in any treated eye.
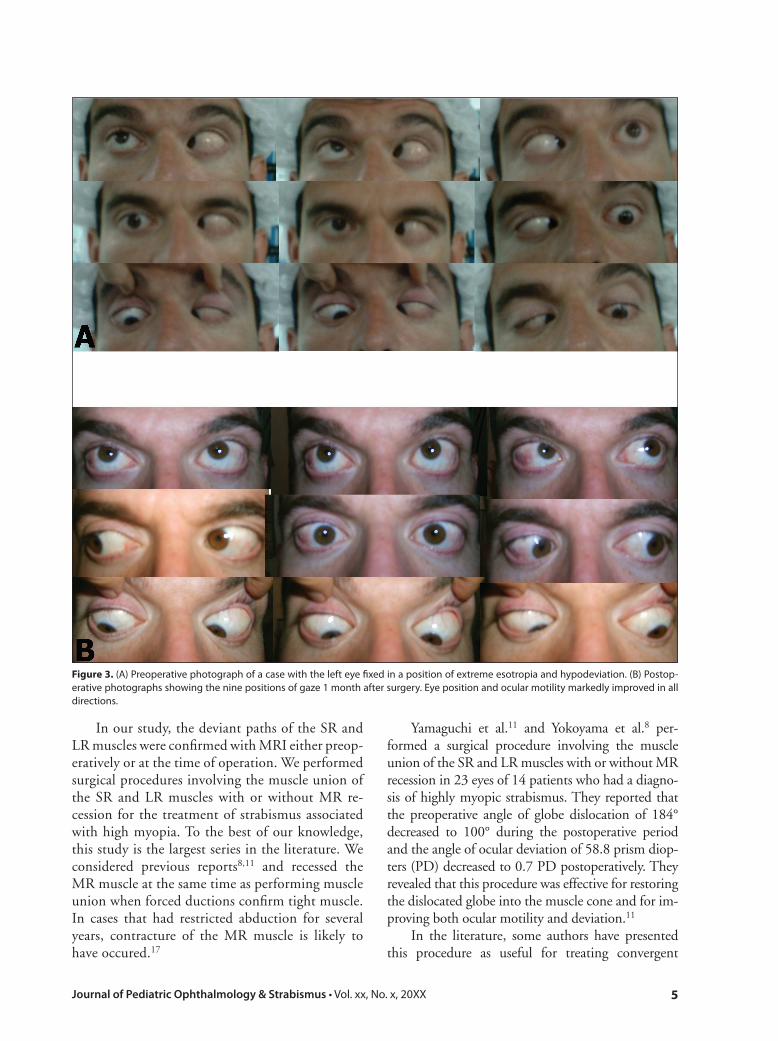
Figure 3 shows preoperative and postoperative photographs of one case.
DISCUSSIONMany surgical methods to stabilize the globe
in high myopia have been described, including te-notomy, large recession of the MR muscle, recession of the nasal conjunctiva, recession-resection proce-dures and/or the traction suture, disinsertion, and myectomy of MR muscles with LR resection.5,6,13-16 A large amount of the recession of the MR muscle is effective in some cases, but relapse can occur.4,14,17
Krzizok et al. reported that a common reces-sion and resection procedure may even aggravate the deviation.13 Recently, several researchers have paid special attention to the shift in the extraoc-ular muscle paths in myopic strabismus fixus, re-porting that these shifts were caused by a posterior prolapse of an elongated eyeball beyond the muscle cone in the orbit.2,3,8,14,18-20 Rutar and Demer sug-gested that LR-SR muscle band degeneration leads to downward shift of the LR muscle.21 Noting the displacement of the SR and LR muscles in myo-pic strabismus fixus, some authors have reported the superior fixation of the LR muscle belly,13 hemitransposition of the SR and LR muscle,20 and loop myopexi between the SR and LR muscle.22,23 Yokoyama et al. introduced a surgical procedure uniting the muscle bellies of the SR and LR muscles for patients with highly myopic strabismus fixus.8 Some authors reported that patients in whom con-tracture of the MR muscles was not found were cured only by this procedure and the recession of the MR muscle was not essential for treating highly myopic strabismus.8,11
TABLE 1
Surgical Results in Patients With Highly Myopic Strabismus
Variable PreopPostop
1 MonthPostop 1 Year
Postop 2 Years
Postop 3 Years
Postop 4 Years
No. of eyes/patients 35/20 35/20 35/20 35/20 35/20 35/20
Angle of dislocation of the globe (°)(mean ± SD [min to max])
178 ± 10 (160 to 200)
101 ± 6 (90 to 115)
103 ± 5 (90 to 120)
102 ±9 (90 to 120)
101 ± 4 (90 to 120)
103 ± 7 (90 to 120)
Angle of esotropia (PD) (mean ± SD [min to max])
58.6 ± 2.5 (50 to 90)
6.8 ± 1.4 (0 to 10)
6.7 ± 1 (0 to 10)
6.9 ± 1 (0 to 15)
6.7 ± 1.2 (0 to 15)
6.8 ±0.7 (0 to 15)
Angle of hypotropia (PD) (mean ± SD [min to max])
12.5 ± 1.3 (8 to 20)
3.3 ± 1.1 (0 to 4)
3.5 ± 0.2 (0 to 5)
3.4 ± 0.1 (0 to 5)
3.2 ± 0.4 (0 to 5)
3.3 ± 0.05 (0 to 5)
Abduction (mean ± SD [min to max])
-2.9 ± 1.6 (-2 to 4)
-0.7 ± 0.8 (0 to 2)
-0.7 ± 0.1 (0 to 2)
-0.8 ± 0.2 (0 to 2)
-0.9 ± 0.4 (0 to 2)
-0.7 ± 0.5 (0 to 2)
Supraduction (mean ± SD [min to max])
-2.4 ± 0.9 (-1 to 3)
-0.6 ± 0.1 (0 to 2)
-0.6 ± 0.1 (0 to 2)
-0.7 ± 0.2 (0 to 2)
-0.5 ± 0.05 (0 to 2)
-0.7 ± 0.2 (0 to 2)
Preop = preoperative; postop = postoperative; SD = standard deviation; min = minimum; max = maximum; PD = prism diopter
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX 5
In our study, the deviant paths of the SR and LR muscles were confirmed with MRI either preop-eratively or at the time of operation. We performed surgical procedures involving the muscle union of the SR and LR muscles with or without MR re-cession for the treatment of strabismus associated with high myopia. To the best of our knowledge, this study is the largest series in the literature. We considered previous reports8,11 and recessed the MR muscle at the same time as performing muscle union when forced ductions confirm tight muscle. In cases that had restricted abduction for several years, contracture of the MR muscle is likely to have occured.17
Yamaguchi et al.11 and Yokoyama et al.8 per-formed a surgical procedure involving the muscle union of the SR and LR muscles with or without MR recession in 23 eyes of 14 patients who had a diagno-sis of highly myopic strabismus. They reported that the preoperative angle of globe dislocation of 184° decreased to 100° during the postoperative period and the angle of ocular deviation of 58.8 prism diop-ters (PD) decreased to 0.7 PD postoperatively. They revealed that this procedure was effective for restoring the dislocated globe into the muscle cone and for im-proving both ocular motility and deviation.11
In the literature, some authors have presented this procedure as useful for treating convergent
Figure 3. (A) Preoperative photograph of a case with the left eye fixed in a position of extreme esotropia and hypodeviation. (B) Postop-erative photographs showing the nine positions of gaze 1 month after surgery. Eye position and ocular motility markedly improved in all directions.

6 Copyright © SLACK Incorporated
strabismus fixus.24 We achieved satisfactory out-comes from uniting the muscle bellies of the SR and LR muscles with or without MR recession in myo-pic strabismus cases. The preoperative mean angle of globe dislocation of 178º decreased to 101º on the postoperative period. The angle of horizontal de-viation was 58.6 PD and decreased to 6.8 PD post-operatively, and the angle of vertical deviation was 12.5 PD and decreased to 3.3 PD postoperatively. In all cases, abduction and supraductions were sig-nificantly improved after surgery. We observed that the physiological muscle plane may be reestablished by this surgery. Postoperatively, the angles of the dis-location of the globe, angles of horizontal or verti-cal deviations, abductions, and supraductions were stable for all patients throughout the follow-up pe-riod. This procedure has many advantages, including elimination of the risk of scleral perforation because no suture is placed in the globe. Additionally, the risk of anterior segment ischemia is eliminated or mini-mized because the anterior ciliary circulation would be less compromised, as the muscles are not cut.
We determined that the surgical procedure in-volving the muscle union of the SR and LR mus-cles with or without MR recession was sufficient to restore the dislocated globe back into the muscle cone and to achieve improvement of esotropia-hypotropia, abduction, and supraduction in pa-tients with highly myopic strabismus. We especially recommend an additional recession of MR muscle when forced ductions confirm tight muscle. We ob-served that the postoperative outcomes remained stable during the 4 years of follow-up.
REFERENCES 1. Kaynak S, Durak I, Ozaksoy D, Canda T. Restrictive myopic
myopaty: computed tomography, magnetic resonance imag-ing, echography, and histological findings. Br J Ophthalmol. 1994;78:414-415.
2. Krzizok TH, Schroeder BU. Measurement of recti eye muscle paths by magnetic resonance imaging in highly myopic and nor-mal subjects. Invest Ophthalmol Vis Sci. 1999;40:2554-2560.
3. Aoki Y, Nishida Y, Hayashi O, et al. Magnetic resonance imag-ing measurements of extraocular muscle path shift and posterior eyeball prolapse from the muscle cone in acquired esotropia with high myopia. Am J Ophthalmol. 2003;136:482-489.
4. Sturm V, Menke MN, Chaloupka K, Landau K. Surgical treat-ment of myopic strabismus fixus: a graded approach. Graefes Arch Clin Exp Ophthalmol. 2008;246:1323-1329.
5. Demer JL, von Noorden GK. High myopia as an unusual cause of restrictive motility disturbance. Surv Ophthalmol. 1989;33:281-284.
6. Bagolini B, Tamburrelli C, Dickmann A, Colosimo C. Conver-gent strabismus fixus in high myopic patients. Doc Ophthalmol. 1991;74:309-320.
7. Miller JM, Demer JL, Rosenbaum AL. Effect of transposition surgery on rectus muscle paths by magnetic resonance imaging. Ophthalmology. 1993;100:475-487.
8. Yokoyama T, Ataka S, Tabuchi H, Shiraki K, Miki T. Treatment of progressive esotropia caused by high myopia: a new surgical pro-cedure based on its pathogenesis. In: Proceedings from the 27th Meeting of the ESA; June 6-9, 2001; Florence, Italy.
9. Larsen PC, Gole GA. Partial Jensen’s procedure for the treatment of myopic strabismus fixus. J AAPOS. 2004;8:393-395.
10. Wong I, Leo SW, Khoo BK. Loop myopexy for treatment of myo-pic strabismus fixus. J AAPOS. 2005;9:589-591.
11. Yamaguchi M, Yokoyama T, Shiraki K. Surgical procedure for correcting globe dislocation in highly myopic strabismus. Am J Ophthalmol. 2010;149:341-346.
12. Santiago AP, Rosenbaum AL. Test of muscle function. In: Rosen-baum AL, Santiago AP, eds. Clinical Strabismus Management: Principles and Surgical Techniques, 1st ed. Philadelphia: W.B. Saunders Company; 1999:37-51.
13. Krzizok TH, Kaufmann H, Traupe H. New approach in strabis-mus surgery in high myopia. Br J Ophthalmol. 1997;81:625-630.
14. Hayashi T, Iwashige H, Maruo T. Clinical features and surgery for acquired progressive esotropia associated with high myopia. Acta Ophthalmol Scand. 1999;77:66-71.
15. Mohan K, Sharma A, Gupta R, Gupta A. Treatment of strabismus fixus convergence. J Pediatr Ophthalmol Strabismus. 1999;36:94-97.
16. Bagheri A, Adhami F, Repka MX. Bilateral recession-resection surgery for convergent strabismus fixus associated with high myo-pia. Strabismus. 2001;9:225-230.
17. Aydin P, Kansu T, Sanac AS. High myopia causing bilateral ab-duction defficiency. J Clin Neuroophthalmol. 1992;12:163-165.
18. Herzau V, Ioannakis K. Pathogenesis of eso- and hypotropia in high myopia [article in German]. Klin Monbl Augenheilkd. 1996;208:33-36.
19. Yokoyama T, Tabuchi H, Ataka S, Shiraki K, Miki T, Mochizuki K. The mechanism of development in progressive esotropia with high myopia. In: Proceedings from the 26th Meeting of the ESA; September 14-16, 2000; Barcelona, Spain.
20. Yamada M, Taniguchi S, Muroi T, Satofuka S, Nishina S. Rectus eye muscle paths after surgical correction of convergent strabis-mus fixus. Am J Ophthalmol. 2002;134:630-632.
21. Rutar T, Demer JL. “Heavy eye” syndrome in the absence of high myopia: a connective tissue degeneration in elderly strabismic pa-tients. J AAPOS. 2009;13:36-44.
22. Basmak H, Sahin A, Yildirim N. Surgical treatment of strabis-mus fixus associated with high myopia. Ophthalmic Surg Lasers Imaging. 2008;39:397-398.
23. Durnain JM, Maddula S, Marsh IB. Treatment of “heavy eye syn-drome” using simple loop myopexy. J AAPOS. 2010;14:39-41.
24. Rowe FJ, Noonan CP. Surgical treatment for progressive esotropia in the setting of high-axial myopia. J AAPOS. 2006;10:596-597.






![The Kugel repair for groin hernias1.ppt [Read-Only] orifice: “window of groin” Henry Fruchaud Boundaries: laterally Iliopsoas Medially lateral rectus Superiorly (IOM/TOM) Inferiorly](https://static.fdocuments.us/doc/165x107/5b09ffc57f8b9aba628b7b46/the-kugel-repair-for-groin-read-only-orifice-window-of-groin-henry-fruchaud.jpg)