Surgical approaches to the heart - Assets - Cambridge...
10
Surgical approaches to the heart 1 1 © Cambridge University Press www.cambridge.org Cambridge University Press 1841100285 - Surgical Anatomy of the Heart Benson R. Wilcox, Andrew C. Cook and Robert H. Anderson Excerpt More information
Transcript of Surgical approaches to the heart - Assets - Cambridge...

Surgical approaches to the heart
11
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

Surgical anatomy of the heart2
When the heart is described in this and insubsequent chapters, we account for theorgan in its anatomical position1.Whenever possible, however, the heart willbe illustrated as it would be viewed by thesurgeon during an operative procedure,irrespective of whether the pictures aretaken in the operating room, or arephotographs of autopsied hearts. Wherean illustration is in a non-surgicalorientation, this is clearly stated.
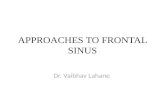
In the normal individual, the heart liesin the mediastinum with two-thirds of itsbulk to the left of the midline (Fig. 1.1).The surgeon, therefore, can approach theheart and great vessels either laterallythrough the thoracic cavity, or directlythrough the mediastinum anteriorly. Tomake such approaches safely, knowledge isrequired of the salient anatomical featuresof the chest wall, and of the vessels andthe nerves that course through the
mediastinum. The approach used mostfrequently is a complete median sternotomy,although increasingly the trend is to usemore limited incisions. The incision in thesoft tissues is made in the midline betweenthe suprasternal notch and the xiphoidprocess. Inferiorly, the white line, or lineaalba, is incised between the two rectussheaths, taking care to avoid entry to theperitoneal cavity, or damage to an enlargedliver, if present. Reflection of the origin of
Sup. Inf.
Left
Right
Obtuse marginApex
Long axisof heart
Acute margin
Base ofventricular mass
2/3
Long axisof body
1/3
Fig. 1.1 This cartoon shows the usual position of the heart within the thorax, illustrating the vital landmarks and areasseen with the patient supine on the operating table, as viewed from the perspective of the surgeon.
Left lobeof thymus
Right lobeof thymus
Superior caval vein Phrenic nerve
Pericardial sac
Sup. Inf.
Left
Right
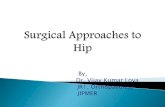
Fig. 1.2 This operative view, taken througha median sternotomy in an infant, shows theextent of the thymus gland.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

the rectus muscles in this area reveals thexiphoid process, which is then incised toprovide inferior access to the anteriormediastinum. Superiorly, a vertical incisionis made between the sternal insertions ofthe sternocleidomastoid muscles. Thisexposes the relatively bloodless midlineraphe between the right and left
sternohyoid and sternothyroid muscles.An incision through this raphe then givesaccess to the superior aspect of the anteriormediastinum. The anterior mediastinumimmediately behind the sternum is devoidof vital structures, so that the superior andinferior incisions into the mediastinum cansafely be joined by blunt dissection in the
retrosternal space. When the sternum hasbeen split, retraction will reveal thepericardial sac, lying between the pleuralcavities. Superiorly, the thymus gland wrapsitself over the anterior and lateral aspectsof the pericardium in the area of exit of thegreat arteries, the gland being a particularlyprominent structure in the infant (Fig. 1.2).
Surgical approaches to the heart 3
Sup. Inf.
Left
Right Brachiocephalic vein
Thymic veins
Aorta inpericardium
Right lobe ofthymus
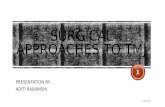
Fig. 1.3 This operative view, again taken through a mediansternotomy, shows the delicate veins that drain from the thymus gland to the left brachiocephalic veins.
Left internal thoracic artery
Right vagus and recurrent laryngeal nerveRight pericardiophrenic
artery and vein
Right phrenic nerve
Left vagus and recurrent laryngeal nerve
Left phrenic nerve
Left pericardiophrenicartery and vein
Fig. 1.4 As shown in this cartoon of amedian sternotomy, the pericardium can beopened so that the phrenic and vagus nervesstay well clear of the operating field.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

It has two lateral lobes, joined more or lessin the midline. Sometimes this junctionmust be divided, or partially excised, toprovide adequate exposure. The arterialsupply to the thymus is from the internalthoracic, or mammary, and inferiorthyroid arteries. If divided, these arteriestend to retreat into the surrounding softtissues, and can produce troublesomebleeding. The veins are fragile, oftenemptying into the left brachiocephalic, or innominate, vein via a common
trunk (Fig. 1.3). Undue traction on the gland can lead to damage to this major vessel.
When the pericardial sac is exposedwithin the mediastinum, the surgeonshould have no problems in gaining accessto the heart. The vagus and phrenic nervestraverse the length of the pericardium, butare well lateral (Fig. 1.4). The phrenicnerve on each side passes anteriorly, andthe vagus nerve posteriorly, to the hilumof the lung.
The course of the phrenic nerve is seenmost readily through a lateral thoracotomy(Fig. 1.5). It is when the heart isapproached through a median sternotomy,therefore, with the nerve not immediatelyevident, that it is most liable to injury.Although it can sometimes be seen throughthe reflected pericardium (Fig. 1.6), itsproximity to the caval veins (Figs. 1.7, 1.8)is not always easily appreciated when thesevessels are dissected from the anteriorapproach. Near the thoracic inlet, it passes
Surgical anatomy of the heart4
Left pericardiophrenic vein
Left pericardiophrenic artery
Left phrenic nerve
Ant.
Post.
Inf. Sup.
Fig. 1.5 This operative view, taken through a left lateral thoracotomy, showsthe course of the left phrenic nerve over the pericardium.
Sup. Inf.
Left
Right
Right phrenic nerveSuperior cavalvein
Right atrialappendage
Fig. 1.6 This operative view, taken througha median sternotomy, shows the rightphrenic nerve as seen through the reflectedpericardium.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

Surgical approaches to the heart 5
Cut edge ofpericardium
Right phrenicnerve
Right pulmonary veins
Sup. Inf.
Left
RightSuperior
caval vein
Fig. 1.7 This operative view, taken through a median sternotomy having pulledback the edge of the pericardial sac, showsthe right phrenic nerve in relation to theright pulmonary veins.
Ant.
Post.
Inf. Sup.
Left phrenicnerve
Persistentleft superiorcaval vein
Arch ofaorta
Superiorintercostal
veinFig. 1.8 This operative view, taken through a left thoracotomy,shows the relationship of the left phrenic nerve to a persistentleft superior caval vein. Note also the course of the superiorintercostal vein.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

close to the internal thoracic artery (Fig. 1.9), exposing it to injury eitherdirectly during takedown of that vessel, orby avulsing the pericardiophrenic arterywith excessive traction on the chest wall.The internal thoracic arteries themselvesare most vulnerable to injury duringclosure of the sternum. The phrenic nervemay be injured when removing thepericardium to use as a cardiac patch, orwhen performing a pericardiectomy.
Injudicious use of cooling agents withinthe pericardial cavity may also lead tophrenic paralysis or paresis.
A standard lateral thoracotomyprovides access to the heart and greatvessels via the pleural space. Left-sidedincisions provide ready access to the great arteries, left pulmonary veins, andthe chambers of the left side of the heart.Most frequently, the incision is made in the fourth intercostal space. The
posterior extent is through the triangular,relatively bloodless, space between theedges of the latissimus dorsi, trapezius,and teres major muscles (Fig. 1.10). The floor of this triangle is the sixth intercostal space. Division of thelatissimus dorsi, and a portion oftrapezius posteriorly, together withserratus anteriorly, frees the scapula so that the fourth intercostal space can be identified. Its precise identity
Surgical anatomy of the heart6
Right internalthoracic artery
Right phrenic nerve
Superiorcaval vein
Azygos vein
Ant.
Post.
Sup. Inf. Fig. 1.9 This operative view, taken through a right thoracotomy, shows the relationship of the right phrenicnerve to the right internal thoracic artery and the superiorcaval vein.
Serratus anteriorTeres major
Rhomboid
Latissimus dorsi Bloodless triangle(seventh rib)
Trapezius Fig. 1.10 This cartoon shows the location of thebloodless area overlying the posterior extent ofthe sixth intercostal space.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

should be confirmed by counting down from above. The intercostal muscles are then divided equidistantbetween the fourth and fifth ribs. Theincision is carried forward beyond themidclavicular line in a submammaryposition, being careful to avoid damage to the nipple and the tissue of the breast.The intercostal neurovascular bundle iswell protected beneath the lower margin of the fourth rib. Having divided themusculature as far as the pleura, thepleural space is entered, and the lungpermitted to collapse away from the chest wall. Posterior retraction of the lung reveals the middlemediastinum, in which the left lateral lobe of the thymus, with its associatednerves and vessels, is seen overlying
the pericardial sac and the aortic arch.Intrapericardial access is usually gained anterior to the phrenic nerve. On occasion, the thymus gland mayrequire elevation when the incision isextended superiorly. The sameprecautions should then be taken asdiscussed above. The lung is retractedanteriorly to approach the aortic isthmusand descending thoracic aorta, and theparietal pleura is divided on itsmediastinal aspect. This is usually done posterior to the vagus nerve. In this area, the vagus nerve gives off its left recurrent laryngeal branch, whichthen passes round the inferior border ofthe arterial ligament, or duct (Fig. 1.11). It then ascends towards the larynx on the medial aspect of the posterior wall of
the aorta. Excessive traction of the vagus nerve as it courses into the thorax along the left subclavian artery can cause injury to the recurrent laryngeal nerve just as readily as can direct trauma to the nerve in the environsof the ligament. The superior intercostalvein is seen crossing the aorta andinsinuating itself between the phrenic and vagus nerves (Fig. 1.12). This structure, however, is rarely ofsurgical significance. The thoracic duct (Fig. 1.13) ascends through this area, draining into the junction of the left subclavian and internal jugularveins. Accessory lymph channels draining into the duct can be troublesome when dissecting the origin of the left subclavian artery.
Surgical approaches to the heart 7
Lung
Patentarterial
duct
Aorta
Left recurrentlaryngeal
nerve
Left vagusnerve
Ant.
Post.
Inf. Sup.
Fig. 1.11 This operative view, taken through a left lateralthoracotomy in an adult, shows the left recurrent laryngealnerve passing round the arterial duct.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

Surgical anatomy of the heart8
Thoracic duct
Left subclavian arteryAortic isthmus
Ant.
Post.
Inf. Sup.Fig. 1.13 In this operative view, taken through a left thoracotomy, the thoracic duct is seen coursing below the left subclavian artery to its termination in the brachiocephalic vein.
Left phrenicnerve
Left superiorintercostal vein
Leftvagusnerve
Left subclavianartery
Aorta
Ant.
Post.
Inf. Sup.
Fig. 1.12 This operative view, again taken through aleft lateral thoracotomy, shows the left superior intercostal vein.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

A right thoracotomy in either thefourth or fifth interspace is made throughan incision similar to that for a left one.The fifth interspace is used whenapproaching the heart, while the fourthpermits access to the right-sided greatvessels. Access to the pericardium isgained by incising anterior to the phrenic nerve, this approach oftennecessitating retraction of the right lobe of the thymus. To reach the rightpulmonary artery and its adjacentmediastinal structures, it is sometimesuseful to divide the azygos vein near itsjunction with the superior caval vein.Extension of this incision superiorly
exposes the origin of the right subclavianbranch of the brachiocephalic trunk.Laterally, this artery is crossed by theright vagus nerve, the right recurrentlaryngeal nerve taking origin from thevagus and curling round theposteroinferior wall of the artery beforeascending into the neck (Fig. 1.14). Alsoencircling the subclavian origin on thisright side is the subclavian sympatheticloop, the so-called ansa subclavia, a branch of the sympathetic trunk that runs up into the neck. Damage to thisstructure can produce Horner’s syndrome.
An anterior right or left thoracotomy is occasionally used in treating
congenital malformations. Once the chest is opened, the same basic anatomical rules apply as described above. Thus far, our account haspresumed the presence of normalanatomy. In many instances, thedisposition of the thoracic structures willbe altered by a congenital malformation.These alterations will be described in theappropriate sections.
Reference
1. Cook AC, Anderson RH. Attitudinallycorrect nomenclature. Heart 2002; 87: 503–506
Surgical approaches to the heart 9
Trachea
Right commoncarotid artery
Right subclavian artery
Brachiocephalic artery
Brachiocephalic vein
Sup. Inf.
Left
Right
Right recurrentlaryngeal nerve
Fig. 1.14 This operative view, takenthrough a median sternotomy, shows thecourse of the right recurrent laryngeal nerverelative to the right subclavian artery.
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information

Anatomy of the cardiac chambers
22
© Cambridge University Press www.cambridge.org
Cambridge University Press1841100285 - Surgical Anatomy of the HeartBenson R. Wilcox, Andrew C. Cook and Robert H. AndersonExcerptMore information