Surgical Anatomy of the Stomach

of 75
-
Upload
mohamoud-mohamed -
Category
Documents
-
view
251 -
download
0
Transcript of Surgical Anatomy of the Stomach
-
8/11/2019 Surgical Anatomy of the Stomach
1/75
SURGICAL ANATOMY OF THE STOMACH
Dr.M.Ardaale
-
8/11/2019 Surgical Anatomy of the Stomach
2/75
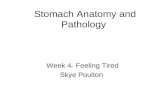
ANATOMY:
The stomach J-shaped. The stomach has
two surfaces (the anterior & posterior),
two curvatures (the greater & lesser), two
orifices (the cardia & pylorus).
It has fundus, body and pyloric antrum.
-
8/11/2019 Surgical Anatomy of the Stomach
3/75
STOMACH
The lesser curvature :forms the right border &extends from the cardiac orifice to thepylorus.It is suspended from the liver by the
lesser omentum.The greater curvature :forms the left border,
the greater omentum extends from the lowerpart to the transverse colon& the gastro-splenic omentum extend from the upperpart to the spleen .
-
8/11/2019 Surgical Anatomy of the Stomach
4/75
CONT..
The mucus membrane forms many folds called
rugaethat are longitudinal in direction.
It has 3 muscular layers: longitudinal ,
circular & oblique.
The stomach function is :storage of food ,mix
the food with gastric secretions to form
chyme, & the delivery of the chyme to the
small intestine.
Capacity: 1.5 L food; max capacity 4L (1
gallon)
-
8/11/2019 Surgical Anatomy of the Stomach
5/75
-
8/11/2019 Surgical Anatomy of the Stomach
6/75
-
8/11/2019 Surgical Anatomy of the Stomach
7/75
-
8/11/2019 Surgical Anatomy of the Stomach
8/75
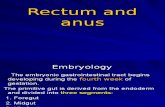
BLOOD SUPPLY:
. The left gastric artery
. Right gastric artery
. Right gastro epiploic artery
. Left gastro epiploic artery
. Short gastric arteries
The corresponding veins drain into portalsystem. The lymphatic drainage of thestomach corresponding its blood supply.
-
8/11/2019 Surgical Anatomy of the Stomach
9/75
-
8/11/2019 Surgical Anatomy of the Stomach
10/75
-
8/11/2019 Surgical Anatomy of the Stomach
11/75
-
8/11/2019 Surgical Anatomy of the Stomach
12/75
-
8/11/2019 Surgical Anatomy of the Stomach
13/75
-
8/11/2019 Surgical Anatomy of the Stomach
14/75
-
8/11/2019 Surgical Anatomy of the Stomach
15/75
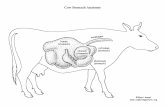
DUODENUM
The 2ndpart: is 8 cm long runs vertically downward infront of the right kidney & on right side of L1,2vertebrae. Its medial border receives the bile duct &the main pancreatic ducts in major duodenal papilla &receive the accessory panc. Duct higher up in the
minor duod. Papilla.The 3rdpart: is 8 cm long ,runs horizontally to the left, in
front of the vertebral column& the lower margin of thehead of panc.
The 4thpart: is 5 cm long, runs upward & to the left tothe duodeno-jejunal flexure.
The mucus memb. Is formed in circular folds calledPlicae circularis
-
8/11/2019 Surgical Anatomy of the Stomach
16/75
-
8/11/2019 Surgical Anatomy of the Stomach
17/75
-
8/11/2019 Surgical Anatomy of the Stomach
18/75
BLOOD SUPPLY OF DUODENUM
Blood supply:
superior
mesentericartery;
Veins drain intohepatic portal
vein
-
8/11/2019 Surgical Anatomy of the Stomach
19/75
HISTOLOGY OF STOMACH
Parietal cells:
These are in the body (acid-secreting portion) of
the stomach and line the gastric crypts, more
abundant distally. These are responsible for the production of
hydrogen ions to form hydrochloric acid, which
has a pH of around 1.
The hydrogen ions are actively pumped by the
proton pump, a hydrogenpotassium APTase
(Sachs) which exchanges intraluminal potassium
for hydrogen ions.
-
8/11/2019 Surgical Anatomy of the Stomach
20/75
-
8/11/2019 Surgical Anatomy of the Stomach
21/75
-
8/11/2019 Surgical Anatomy of the Stomach
22/75
-
8/11/2019 Surgical Anatomy of the Stomach
23/75
CONT..
a key factor in gastric acid secretion.
In addition, there are large numbers of
somatostatin-producing D cells throughout
the stomach, and
somatostatinhas a negative regulatory role.
-
8/11/2019 Surgical Anatomy of the Stomach
24/75
DUODENUM
The duodenum is lined by a mucus-
secreting columnar epithelium.
In addition, Brunners glands lie beneath
the mucosa and are similar to the
pyloric glands in the pyloric part of the
stomach.
Endocrine cells in duodenum produce
cholecystokinin and secretin
-
8/11/2019 Surgical Anatomy of the Stomach
25/75
PHYSIOLOGY OF THE STOMACH AND
DUODENUM
The stomach mechanically breaks upingested food and, together with
the actions of acid and pepsin, forms
chymethat passes into the duodenum. In contrast to the acidic environment of the
stomach, that of the duodenum is alkaline,as a result of the secretion of bicarbonate
ionsfrom both the pancreasand theduodenum.
-
8/11/2019 Surgical Anatomy of the Stomach
26/75
CONT..
This neutralisesthe acid chyme and adjusts
the osmolarityto approximately that of
plasma.
Endocrine cells in the duodenum produce
cholecystokininthat stimulates
the pancreas to produce trypsinand the gall
bladder to contract.
-
8/11/2019 Surgical Anatomy of the Stomach
27/75
CONT..
Secretinis also produced by the endocrine
cells of the duodenum.
This hormone inhibits gastric acid
secretion and promotes production of
bicarbonate by the pancreas.
-
8/11/2019 Surgical Anatomy of the Stomach
28/75
GASTRIC ACID SECRETION
The secretion of gastric acid and pepsin
tends to run in parallel,
although the understanding of the
mechanisms of gastric acid secretion is
considerably greater than that of pepsin.
Numerous factors are involved
to some degree in the production of the
gastric acid.
-
8/11/2019 Surgical Anatomy of the Stomach
29/75
CONT..
These include neurotransmitters,
neuropeptidesand peptide hormones, and
several other factors.
As mentioned above, hydrogen ions are
produced by the parietal cell by the
proton pump.
-
8/11/2019 Surgical Anatomy of the Stomach
30/75
GASTRIC MUCUS AND THE GASTRIC MUCOSAL
BARRIER
The gastric mucous layer is essential to theintegrity of the gastric mucosa.
It is a viscid layer of mucopolysaccharides
produced by the mucus-producing cells ofthe stomach and the pyloric glands.
Gastric mucus is an importantphysiological barrier to protect the gastricmucosa from mechanical damage, andalso the effectsof acid and pepsin.
-
8/11/2019 Surgical Anatomy of the Stomach
31/75
CONT..
Its consider-able bufferingcapacity is
enhanced by the presence of bicarbonate
ions within the mucous.
Many factors can lead to the break down ofthis gastric mucous barrier.
These include bile, nonsteroidal anti-
inflammatory drugs (NSAIDs), alcohol,trauma and shock.
-
8/11/2019 Surgical Anatomy of the Stomach
32/75
CONT..
The stomach is the most sensitive to
ischaemia following a hypovolaemic insult
and also the slowest to recover.
This may explain the high incidence of
stress ulceration in the stomach.
-
8/11/2019 Surgical Anatomy of the Stomach
33/75
PEPTIDES AND NEUROPEPTIDES IN THE
STOMACH AND DUODENUM
Many peptides recognized as hormones
may also be produced by neurons, hence the
term neuropeptides.
The term messenger can be used to
describe all such products.
There are three conventional modes of
action which overlap.
-
8/11/2019 Surgical Anatomy of the Stomach
34/75
-
8/11/2019 Surgical Anatomy of the Stomach
35/75
CONT..
The autocrinemode of action should be
mentioned for completeness.
Here messengers are released from cell to
act on receptors on the same cells surfacemembrane.
Many growth factors such as epidermal
growth factor and transforming growthfactors alpha and beta work in this way.
-
8/11/2019 Surgical Anatomy of the Stomach
36/75
INVESTIGATION OF THE STOMACH AND
DUODENUM
Flexible endoscopy
Amongst all of the methods used toinvestigate and image the stomach
and duodenum, flexible endoscopy is nowthe gold standard.
The original gastroscopes were fibre-optic
(Hirschowitz), but now most use a solid-state camera mounted at the
instruments tip.
-
8/11/2019 Surgical Anatomy of the Stomach
37/75
-
8/11/2019 Surgical Anatomy of the Stomach
38/75
-
8/11/2019 Surgical Anatomy of the Stomach
39/75
ULTRASONOGRAPHY
Standard ultrasound imaging can be used toinvestigate the stomach, particularly inpatients with neoplasia.
Thickening of the gastric wall can be seen in malignancy, some assessment
made of local invasion, and liver andperitoneal diseaseis often detected.
However, used, conventionally, it is lesssensitive than other modalities.
-
8/11/2019 Surgical Anatomy of the Stomach
40/75
CONT..
By contrast, endoluminal ultrasound and
laparoscopic ultrasound are probably the
most sensitive techniques available in the
preoperative staging of gastric
cancer. In endoluminal ultrasound the
transduceris usually attached to
the distal tip of the instrument.
-
8/11/2019 Surgical Anatomy of the Stomach
41/75
CONT..
Five layers of the gastric wall may beidentified on endoluminal ultrasound andthe depth of invasion of a tumour can be
assessed with exquisite accuracy (90 percent accuracy for the T
component of the staging). Enlarged lymphnodes can also be identified
and the techniques accuracy in thissituation is about 80 pet cent.
-
8/11/2019 Surgical Anatomy of the Stomach
42/75
-
8/11/2019 Surgical Anatomy of the Stomach
43/75
OTHER INVESTIGATIONS
Laparoscopy: (gastric cancer, peritoneal
Disease such as patients ascitesor bulkyintraperitoneal disease)
Gastric emptying studies:(gastricdysmtility disorders, follow gastric surgery)
Tests of gastric acid secretion and of pH
monitoring(gastric acid secretion commonlyfound in patients with duodenal ulcerdisease)
24-hour intragastric pH monitoring
-
8/11/2019 Surgical Anatomy of the Stomach
44/75
MEASUREMENT OF PLASMA GASTRIN
The measurement of plasma gastrin by
radioimmunoassay is of use in the diagnosis
of gastrinoma (ZollingerEllison syn-
drome). In most assays the normal fasting gastrin
level is about 50 ng/litre, but in gastrinomas
very high levels, some-times manythousands of ng/litre, can be found.
-
8/11/2019 Surgical Anatomy of the Stomach
45/75
CONT..
the other common cause of
hypergastrinaemia is hypochlorhydria
associated with gastric atrophy and very
high gastrin levels are found in perniciousanemia.
-
8/11/2019 Surgical Anatomy of the Stomach
46/75
-
8/11/2019 Surgical Anatomy of the Stomach
47/75
CONT..
In some cases there seems to be a familial
association.
In such families the mother has suffered
from the condition in 50 per cent of cases,
and 10 per cent of male siblingsand 2 per
cent of female siblings are affected.
-
8/11/2019 Surgical Anatomy of the Stomach
48/75
PATHOLOGY
The classical feature is that the musculature
of the pylorusand adjacent antrum is
grossly hypertrophied,
the hypertrophy being maximum in the
pylorus itself.
The mucosa is compressed such that only
a probe can be inserted.
-
8/11/2019 Surgical Anatomy of the Stomach
49/75
CLINICAL FEATURES
First-born male child that is most
commonly affected.
This condition is seen at 4 weeks after birth
ranging from the third week to, on rare
occasions, the seventh.
A premature infant will also develop the
condition at about 4 weeks after birth.
-
8/11/2019 Surgical Anatomy of the Stomach
50/75
CLINICAL PRESENTATIONS
Vomiting is the presenting symptom that
after 23 days becomes forcible and
projectile.
The child vomits milk and no bile ispresent. Immediately after vomiting the baby
is
usually hungry.
Weight loss is a striking feature and rapidly
the infant becomes emaciated and de-
hydrated.
-
8/11/2019 Surgical Anatomy of the Stomach
51/75
DIAGNOSIS
Feeding tube (NG tube)
This may produce characteristic peristaltic
wavesthat can be seen to pass across the
upper abdomen.
At the same time, using a warm hand, the
abdomen is palpated to detect the lump
-
8/11/2019 Surgical Anatomy of the Stomach
52/75
PYLORIC STENOSIS CONT.
Signs:
1.Vis ib le per istal t ic waves pass ing from lef t to
right across the upper abdomen (golf ball
waves).
2.A palpable tumor in the
epigastr ium or r ight
hypochondr ium (most important).
-
8/11/2019 Surgical Anatomy of the Stomach
53/75
IMAGING
Ultrasonographyis the investigation ofchoice as it can, with-out difficulty, detect the
classical features in the pyloric canal.
Differential diagnosis:
GERD
UTI
Intestinal obstruction
-
8/11/2019 Surgical Anatomy of the Stomach
54/75
TREATMENT
Correct dehydration level (with low sodium,chloride and potassium, and a metabolic
alkalosis).
The child should be rehydrated withdextrosesaline and potassium (2.5 per
cent dextrose plus 0.45 per cent sodium
chloride plus 1 g of potassium chloride per500 ml of
fluid).
-
8/11/2019 Surgical Anatomy of the Stomach
55/75
-
8/11/2019 Surgical Anatomy of the Stomach
56/75
DEFINITIVE MANAGEMENT(SURGERY)
Ramstedtsoperation:
it is important that the stomach is emptied
and washed out with saline, and that
hypothermia is avoided.
Procedure:transverse incision placed
in the upper abdomen over the right rectus
sheath, which is opened in the same line.
-
8/11/2019 Surgical Anatomy of the Stomach
57/75
Treatment :
Treatment is theoperation of
pyloromyotom
(Ramstedts
operation).
-
8/11/2019 Surgical Anatomy of the Stomach
58/75
CONT..
The rectus muscle is then split along theline of its fibresand the posterior rectus
sheath opened in the line of the skin incision.
The hypertrophied pylorus is delivered androtated so that its superior surface comes
into view .
Thus, the least vascular portion can beselected for incision.(Pyloratomy).
-
8/11/2019 Surgical Anatomy of the Stomach
59/75
DUODENAL ATRESIA
This occurs at the point of fusion betweenthe foregut and midgut, and therefore lies in
the neighborhood of the ampulla of Vater.
There is a diaphragm, which is usuallycomplete, across the duodenum at this point
and the condition is frequently accompanied
by other defects.
-
8/11/2019 Surgical Anatomy of the Stomach
60/75
CONT..
The diagnosis is now made antenatally inmost cases through the use of
ultrasound.
This shows the characteristic appearanceof a
dilated stomach and first part of the
duodenum (double bubble). The child vomits from birth and the vomitus
is bile stained.
-
8/11/2019 Surgical Anatomy of the Stomach
61/75
-
8/11/2019 Surgical Anatomy of the Stomach
62/75
DIFFERENTIAL DIAGNOSIS
High intestinal obstruction
Pyloric stenosis
Treatment:(surgery)
operation of the
duodenoduodenostomyin which the
dilated proximal duodenum isanastomosedto the atrophic distal
duodenum.
-
8/11/2019 Surgical Anatomy of the Stomach
63/75
GASTRITIS
Type A gastritis:
This is an autoimmune condition in which
there are circulating antibodies to the parietal
cell.
This results in the atrophy of the parietal
cell mass, hence hypochlorhydria and
ultimately achlorhydria.
-
8/11/2019 Surgical Anatomy of the Stomach
64/75
CONT..
As intrinsic factor is also produced by theparietal cell there is malabsorption of vitaminB12,
which, if untreated, may result in perniciousanaemia.
In type A gastritis the antrum is not affectedand the hypochlorhydria leads to the
production of high levels of gastrin from theantral G cells.
This results in chronic hypergastrinaemia.
-
8/11/2019 Surgical Anatomy of the Stomach
65/75
-
8/11/2019 Surgical Anatomy of the Stomach
66/75
TYPE B GASTRITIS
Most commonly type B gastritis affects
the antrum, and it is these patients who are
prone to peptic ulcer disease.
Helicobacter-associated pangastritisis also
a very common manifestation of infection,
but gastritis affecting the corpus alone
does
not seem to be associated.
-
8/11/2019 Surgical Anatomy of the Stomach
67/75
CONT..
Patients with pangastritis seem to be mostprone to the development of gastric cancer.
Intestinal metaplasia is associated with
chronic pangastritis with atrophy.Although intestinal metaplasiaper se is
common, intestinal metaplasia associatedwith dysplasia has significant malignantpotential,
and if this condition is identified the patientshould be regularly screened
endoscopically.
-
8/11/2019 Surgical Anatomy of the Stomach
68/75
EROSIVE GASTRITIS
This is caused by agents which disturb thegastric mucosal barrier; NSAIDs andalcohol are common causes.
The nonsteroidal-induced gastric lesion isassociated with inhibition of the cyclo-oxygenase type 1
(Cox 1) receptor enzyme, hence reducing theproduction of cytoprotectiveprostaglandins in the stomach.
-
8/11/2019 Surgical Anatomy of the Stomach
69/75
STRESS GASTRITIS
This is a common sequel of serious illnessor injury and is characterized by a reduction
in the blood supply to superficial mucosa
of the stomach.
-
8/11/2019 Surgical Anatomy of the Stomach
70/75
MNTRIERS DISE SE
This is an unusual condition characterized bygross hyper-trophy of the gastric mucosal
folds, mucus production and
hypochlorhydria. The condition is premalignant and may
present with hypoproteinaemia and
anaemia. There is no treatment other than a
gastrectomy.
-
8/11/2019 Surgical Anatomy of the Stomach
71/75
CONT..
The disease seems to be caused by over_expressionof transforming growth factor
alpha (TGF-alpha).
Like epidermal growth factor (EGF), this
peptide also binds to the EGF receptor.
The histological features of Mntriers
-
8/11/2019 Surgical Anatomy of the Stomach
72/75
LYMPHOCYTIC GASTRITIS
This type of gastritis is seen rarely.
It is characterizedby the infiltration of
the gastric mucosa by T cells and is
probably associated with H. pylori infection.
-
8/11/2019 Surgical Anatomy of the Stomach
73/75
OTHER FORMS OF GASTRITIS
Eosinophilic gastritis appears to have an allergicbasis, and is treated with steroids andchromoglycate. Granulomatous gastritis isseen rarely in Crohnsdisease and also may be
associated with tuberculosis.Acquired immunodeficiency syndrome (AIDS)
gastritis is secondary to infection withcryptospirodiosis.
Phlegmonous gastritis is a rare bacterialinfectionof the stomach found in patients withsevere intercurrent illness.It is usually anagonal event.
-
8/11/2019 Surgical Anatomy of the Stomach
74/75
-
8/11/2019 Surgical Anatomy of the Stomach
75/75
ASSIGNMENTS
Duodenal ulceration
Gastric ulcers
Malignancy in gastric ulcers
Operations for duodenal/Gastric
ulceration
Small stomach syndrome
Haematemesis and melaena