Surgery Stomach & Duodenum Tg
110
Surgery Stomach and duodenum Dr. T. Galdona PA-C
-
Upload
miami-dade -
Category
Health & Medicine
-
view
8.564 -
download
18
Transcript of Surgery Stomach & Duodenum Tg

SurgeryStomach and duodenum
Dr. T. Galdona PA-C

Stomach Anatomy and function
• It is a saccular organ.• Located (L) hypochondrium and epigastrium.• It has 2 regions:1) a proximal one, distal to GEJ called LES.• This region is marked by change from squamous to columnar
epithelium.• 2) Distal region is located at junction of distal
portion of stomach (antrum) with duodenum, at this point a define sphincter of smooth muscle, pylorus, is located.
• Pylorus prevents reflux of duodenal content to stomach and in association with antral pump controls the rate of stomach emptying.
• Stomach is divided in 3 portions: 1) fundus (proximal portion)• When food passes oropharynx into esophagus, vagal stimulation
relaxes the fundus preventing increase intraabdominal pressure and allowing food to pass and be stored. Here is located the pacemaker

StomachAnatomy and function
• Responsible for motor activity. Centered at greater curvature• 2) Corpus (Middle portion)• 3) Antrum (distal portion)• Wall of stomach has 4 layers:• Mucosa, submucosa, muscularis mucosa and serosa• Stomach has 3 layers of smooth muscle:• Outermost layer: longitudinal muscle• Middle layer: circular muscle (autonomic pacemaker)• Innermost layer: oblique muscle• Blood supply of stomach:• (R) & (L) gastric art. (lesser curvature)• (R) & (L) gastroeplipoic art. (greater curvature)

Stomach Anatomy and function
• Short gastric art. (Fundus).• Gastroduodenal art. (behind pylorus)• Innervation: Vagus nerve (Parasympathetic) very sensitive to
emotion)• Entering abdomen divides into 2 trunks:
• (L) trunk enters abdomen anteriorly to esophagus, gives off an anterior branch the hepatic that innervates the gallbladder, biliary tract, and liver.
• (R) trunk posterior to esophagus, gives off a posterior branch to the celiac plexus from which nerves pass to the midgut (pancreas, small intestine, and proximal colon).
• Both nerves innervate lesser curvature

Stomach anatomy

Stomach anatomy

StomachAnatomy and function
The vagus nerve stimulates the parietal cell mass to secrete hydrochloric acid; it also controls the motor activity of the stomach.
The pacemaking area of the stomach is found in the fundus on the greater curvature near the short gastric vessels.

Stomach Anatomy and physiology
• Fundus: • Parietal cells acid producing cells• Chief cells pepsinogen – producing cells• ECL (entero-chromaffin like) histamine producing cells
• Antrum: • G cell produce Gastrin• IF
• Throughout entire stomach:• Mucus secreting goblet cells cells

Stomach Physiology
• HCL Secretion:• Parietal cells are the ones that produce HCL acid.• H/K ATPasa pump exchanges H for K 1:1• ATP is the source of energy.• This pump is critical for active secretion of HCL acid.• Direct blockage of it inhibits its production (PPI’S)• Acid secretion occurs in 3 phases:• 1) cephalic phase:• Smell, sight, thought of food ----afferent neural pathway----CNS• Efferent pathway-----Hypothalamus------Stomach (via vagus)• Ach release by vagus ---stimulates parietal cells---binding to receptor M3• Receptor at cells----intracellular cascade----releases HCL

HCL secretion

StomachPhysiology
• Receptor at cells----intracellular cascade----releases HCL• Indirectly Ach ----stimulates antral cells----gastrin release protein
(GRP) ----gastrin release • Ach stimulates also ECL to release Histamine• 2)Gastric phase:• Starts when food enters stomach• Stretch receptors in stomach activates parasympathetic reflex• With release of Ach, alkalinization in antrum +AA• Stimulates G cells---release of gastrin. • Gastrin binds to CCK -----release of HCL, also promotes release of
HCL via ECL cells causing histamine release-----histamine binds to H2 receptors-----release of HCL
•

StomachPhysiology
• Intestinal phase:• When food arrives to small intestine• Associate with release of GI peptides and histamine
• 2 mechanisms for acid suppression:• 1) endocrine mediated (Review their mechanism giving in class go
to Lawrence) • A) Secretin• B) Somatostatin• C) CCK• D) GIP• 2) Gastric mucosal protection:

StomachPhysiology
• 2) Gastric mucosal protection:• Goblet’s cells (mucopolysaccharide, HCO3 mechanism)
• Vit B12 Absorption:• B12 must bind IF in terminal ileum• IF produced by parietal cells• Pancreatic enzymes isolate it in proximal small bowel (only way to
bind B12).• Deficiency of B12---megaloblastic anemia----irreversible sensory
neuropathy, and dementia.• Schilling test

StomachBenign gastric Diseases
• PUD:• Stated in its simplest form, peptic ulcers of the upper gastrointestinal
tract occur when the mechanisms for defense are inadequate to deal with the physiologic, but hostile, intraluminal milieu. When such an event occurs, auto digestion of the mucosa occurs.
• In the definition are grouped benign gastric ulcers and duodenal ulcers.
• To help in the learning of these processes the clinical manifestation have been giving separate in order to make a differentiation between them. In real life, sometimes is not that clear cut between them.

StomachPUD
• Gastric ulcer:• Gastric ulcer pain usually occurs in the epigastrium and may radiate
through to the back.• It is produced by the ingestion of food.• Anorexia and weight loss is common in patients with gastric ulcers.• Classified in 4 groups according anatomical location:• Type I: lesser curvature• Type II: arise same place as duodenal ulcers/ combination of both• Type III: pre-pyloric region• Type IV: high in lesser curvature• Type I are the most common ones (lesser curvature) and type IV
less common ones both are associated with low acidity.

StomachPUD
• Type II and III associated with acid hypersecretion, to the point that they behave pretty much like duodenal ulcers in this case Tx follows duodenal ulcer Ds.
• Review H.pyloris and NSAID’S mechanism giving in class.• The diagnosis can be made by upper GI series and/or by
endoscopy.• Endoscopy and multiple biopsies taken establish the presence or
absence of carcinoma and it confirms the Dx. In this pathology endoscopy is crucial due to importance of r/o cancer in pts with gastric ulcers.

Stomach PUD
• Medical TX for uncomplicated Gastric ulcers:• 1) Stop NSAID’S,alcohol, tobacco,steroids, ASA.• 2) Tx of H.pyloris• 3) Additional options: sucralfate and misoprostol.• 4) endoscopy is mandatory 6 weeks after Dx: 2 outcomes• 1) ulcer healed substantially, • 2) ulcer does not heal continue Tx and endoscopy after 4-6 weeks• If ulcer did not heal -----surgery

Stomach PUD
• Surgical TX:• Surgery is indicated for bleeding, perforation, gastric outlet
obstruction, intractability, and suspicion of malignancy.• The ulcer must be excised. • The recurrence rate following surgical treatment for gastric ulcer is
extremely low.• Distal gastrectomy (approximately 50%) with excision of the ulcer is
the appropriate therapy (I, II, III).• Restoration of continuity is done by using one of these 3 options:• Bilroth I, Bilroth II and Roux en Y gastroenterostomy. (learn the
procedures).

Surgical TreatmentTruncal Vagotomy -- Antrectomy &
Billroth I Anastomosis

Surgical TreatmentTruncal Vagotomy -- Antrectomy &
Billroth II Anastomosis

Surgical TreatmentTruncal Vagotomy -- Antrectomy &
Roux-en-Y Anastomosis

StomachADC of stomach
• 95% of stomach Cancer are ADC.• It has declined over the past 50 years.• It is low incidence in USA and Europe and incidence is high in Asia
(Japan, China, Chile, Russia, Finland).• Risk factors: H.pyloris, achlorhydria, pernicious anemia, chronic
gastritis, caustic injury, adenomatous polyps.• Classification: • 2 types.• A) ulcerative, polypoid, scirrhous, superficial spreading subtypes
(based on endoscopic appearance. • B) intestinal (elderly, spreads hamatogenously), diffuse (younger ,
assotiated with blood group type A).• Linitis plastica is used to describe complete infiltration of stomach
with carcinoma, looks like leather bottle. Poor prognosis.

StomachADC of stomach
• S/S:Depends on stage
• Early stage asymptomatic, vague symptoms• More advance disease:• Vague epigastric pain• Weight loss• Dysphagia• Hematemesis• Melena • N/V• New onset of iron deficiency anemia• Guaic (+) stools.

StomachADC of stomach
• Virchow’s node (supraclavicular node)• Blumer’s shelf ( a palpable rectal ridge)• Sister Mary Joseph’s node (palpable umbilical node)• Krukenberg’s tumor (metastasis to ovaries)• Metastasis are more common to lung, liver, ovaries.• Dx:• Upper endoscopy• Bx (multiple ones) • Endoscopy U/S ----depth of TU invasion ---for staging.• Xrays (chest)• CT abd and pelvis• Upper GI series are not as used as before, b/c they can miss some
cancers specially superficial spreading subtypes.

StomachADC of stomach
• B/C this type of cancer can metastasized to peritoneum and omentum and is not pick up by CT, laparoscopy has become a part of work up, also used for staging.
• Sixty percent of gastric carcinomas originate in the distal half of the stomach and the majority of these will occur in the pyloric gland area.
• Tx:• Gastrectomy with localized Ds.• With distal Ds radical subtotal gastrectomy + roux en y
gsatrojejunostomy.• Pancreatectomy and splenectomy may be needed.• Lymphadenectomy is controversial. • Adjuvant therapy (chemotherapy) is also controversial.

StomachADC of stomach
• Best curve rates are shown in Japan and in this scenario, 5 year survival is less than 50%, in other countries is 10%, best scenario with higher % of 5 year survival is incidental carcinoma found during stomach surgery for supposed benign disease, 75%
• Metastatic Ds can’t be cured.therapy in this case Palliative

StomachGastric lymphoma
• Gastric lymphomas are 2/3 of all GI’s lymphomas.• Prevalent in older pts and in non Hogking’s variant.• S/S:• Similar to those of gastric ADC.• Upper abdominal pain.• Unexplained weight loss.• fatigue and bleeding• Dx:• Endoscopy• Bx• If is a lymphoma it should be stage as any lymphoma:• Chest xray, Abd CT scan, Bone Marrow Bx.

StomachGI stromal TU (GIST)
• They are leiomyomas and leiomyosarcomas.• Submucosal growths• Arising from a variety of cells• MC place is stomach• Can be :• Benign and malignant• More than 6 cm + necrosis =malignancy• S/S:
similar to other gastric tumors• Some don’t give symptoms• Non specific abdominal pain• Bleeding and obstruction• Abdominal mass

StomachGI stromal TU (GIST)
• Dx: • endoscopy• Bx• Abdominal CT scan ---- gives tumor size, invasion and metast, liver
most common site for metast.• Tx: • local excision• Survival depends on presence of malignancy• Prognosis for benign is excellent• GIST --- malignant ones are very aggressive Tx here is chemo.

Stomach Postgastrectomy Syndromes
• Due to denervation of stomach the pyloric mechanism becomes incompetent and the control of stomach emptying is abolish. If we add the re-anastomotic of duodenum, posgastrectomy syndromes are the consequence.
• Early Dumping syndrome• Late dumping syndrome• Post-vagotomy Diarrhea• Afferent loop obstruction• Blind loop syndrome• Alkaline Reflux gastritis• Recurrent ulcer Ds• Gastric atony• Metabolic disturbances

StomachEarly Dumping Syndrome
• Symptoms occurs 15 minutes after meal.• S/S:• Anxiety, extreme weakness, tachycardia, diaphoresis, palpitations,
and desire to lie down. Also borborygmi are heard and diarrhea is common. Symptoms disappear gradually.
• Pathophysiology: • it is an uncontrolled emptying of hypertonic fluid into small intestine.• Fluid moves rapidly from intravascular space into intraluminal space
producing acute intravascular volume depletion.• As simple sugars are absorbed and dilution of hypertonic solution
occurs the symptoms decreased.• Substances like serotonin, neurotensin, histamine, glucagon,
vasoactive intestinal peptide, kinins.

StomachEarly dumping syndrome
• MCC are Billroth I and II.• Tx:• Somatostatin analogue, may be of benefit, and Beta blockers.• Avoid hypertonic liquid meals.• Altering the volume of meals.• Ingest some fat to slow gastric emptying• Liquids should be ingested before meals or 30’ after meals.• Billroth I and II are MCC.• Roux en Y is sometimes indicated b/c delays emptying.

Dumping syndrome

StomachLate dumping syndrome
• Symptoms begin 3 hours after meals.• S/S:• Sudden anxiety, diaphoresis, tachycardia, palpitations, weakness,
fatigue, and desire to lie down.• It is not associated with borborygm or diarrhea.• Pathophysiology: • Rapid changes in serum glucose and insulin levels.• Large glucose-bolus containing chyme presented to small intestine
has a lot of glucose in it, glucose is absorbed faster than when the intact pylorus controls emptying of stomach. This causes high levels of serum glucose shortly after meal and causes a big released of insulin. Insulin response exceeds what is necessary to clear glucose from blood and hypoglycemia symptoms happens. Symptoms are due to rapid fluctuations in serum glucose levels.

StomachLate Dumping syndrome
• Tx:• Conservative• Small snacks 2 hours after meals• If symptoms can not be controlled then the previous procedure has
to be converted to Billroth I or Roux en Y gastrojejunostomy.

StomachPostvagotomy Diarrhea
• After truncal vagotomy some pts develop changes in bowel habits.• Most cases symptoms disappear but small number (1%) of cases
present severe diarrhea. • Diarrhea is explosive, no related to meals, and without warning.• Etiology: hypoacidity of stomach and vagal denervation affects motility, and
decreased concentration of bile salts, all these factors have been considered as possible causes, but still no clear.
Tx: Restricted fluid intake increased food low in fluids If not a good response to medical Tx surgery is indicated.

StomachAfferent loop Obstruction
• Symptoms show immediately after a meal• Occurs only with Billroth II reconstruction• It happens at the afferent limb adjacent to the anastomosis.• S/S:
cramping pain defined as crushing• Within 45’ pt feels abdominal rush with increased of pain, follow by• N and vomit of a dark brown bitter tasting material with consistency
of motor oil.• Symptoms resolve with vomiting, profound weight loss to prevent
pain

Afferent loop obstruction

StomachAfferent Loop Obstruction
• Pathophysiology:• Distension of the afferent limb, when the pancreatic and biliary
secretions are trapped.• Spontaneous, forcefull, decompression of obstructed limb.
• Tx:• Conversion of Billroth II to roux en y Gastrojejunostomy • or to Billroth I.

StomachBlind Loop Syndrome
• MC after Billroth II than roux en y gastrojejunostomy. Also seen after irradiation or morbid obesity
• Associated to bacteria overgrowth in the limb of the intestine excluded from the flow of chyme. This limb has bacteria that proliferate and interfere with folate and Vit B12 metabolism, also bacterial overgrowth cause deconjugation of bile salts ---steatorrhea
• B12 deficiency leads to megaloblastic anemia• S/S:• Diarrhea• Weight loss• Weakness• anemia

StomachBlind Loop Syndrome
• Tx:• ANTBX (Tetracyclins)• Re-growth of bacteria can happen.• Conversion to Billroth I may be required for some pts.

StomachRecurrent Ulcer Disease
• MCC incomplete vagotomy, posterior vagal trunk or a branch of this trunk (criminal nerve of Grassi) is left intact.
• Truncal vagotomy + antrectomy lowest rate 2%• Proximal gastric vagotomy highest rate of 12%• Dx:• Endoscopy + Congo red (to demostrate areas of pH drop in gastric
mucosa after a secretagogue is administered, pentagastrin )• Tx:• PPI’S Long term• Reoperative vagotomy• Note:• Recurrent ulceration and verified complete vagotomy look for
endocrine etiology like family Hx of MEN-1. Also look for hyperparathyroidism and Gastrinoma as possible causes.

StomachGastric Atony
• Atony of stomach may result from gastric reconstruction and denervation (vagotomy) and ablation of pylorus.
• Motility of stomach is altered.• Rapid emptying of liquids can result in early or late dumping, yet
delayed of emptying solids due to gastric atony occurs.• MCC is roux en Y gastrojejunostomy• Only 50% of pts have symptoms.• Tx:• time will improve symptoms.• Promotility agents like metoclopramide, • erythromycin.

StomachAcute Gastritis
• It causes inflammation of stomach and it is associated to erosions and hemorrhage.
• S/S: • N/V, hematemesis, melena, RBPR, or hematochezia.• Risk factors:• H.pyloris, NSAID’S, ASA, bile reflux, alcohol ingestion, irradiation,
local trauma.• Tx:• Stop noxious agents, Tx of H. pyloris, H2 or PPI’S, adequate
nutrition.

StomachAcute Gastritis
• Gastritis has 2 basic types:– Acute (erosive/ hemorrhagic)
• toxic injury from drugs like NSAIDS, ASA, & Alcohol• MC sx is UGI bleed “coffee-ground” emesis
– Non-erosive, Non-specific/Chronic• 1. Infectious gastritis (80% caused by H. pylori)• 2. Autoimmune gastritis
– Pernicious anemia (a chronic illness caused by impaired absorption of vitamin B-12 because of a lack of intrinsic factor (IF) in gastric secretions).
– Increased risk of adenocarcinoma

StomachStress gastritis
• Another cause of acute gastritis.• Mostly seen in pts under Stress. Mucosal erosions at proximal
stomach that progress rapidly to the rest of the stomach
Burn pts develop stress ulcers called Curling’s ulcers• Pts with CNS injuries, severe trauma and organ failure can develop
ulcers called Cushing’s ulcers.• Ulcers develop as soon as 24 hours from onset of stress.• MCC is hemorrhage (RBPR, or in NG tube, or decreased in Hct or
hemodynamic instability).• Dx: • endoscopy

StomachStress gastritis
• Tx: • Nasogastric tube aspiration.• Antacid instillation through tube (repeated)• Early prophylaxis with H2, PPI’s, sucralfate, misoprostol, antiacids• Persistent hemorrhage ----surgery (vagotomy + pyloroplasty)

Gastric regulation

Erosive gastritis

Stress ulcer

Erosive gastritis

Hemorrhagic gastritis

PUD

Stomach Hypertrophic Gastritis (Menetrier’s Ds)
• It is a process characterize by massive hypertrophy of gastric rugae.
• Hyperplasia of mucus secreting cells in corpus and fundus of stomach.
• Possible autoimmune, b/c of TNF B over expression.
• S/S:
• Epigastric pain, N/V, occult hemorrhage, weight loss, diarrhea, progression of Ds----protein losing gastropathy----hypoproteinemia----peripheral edema
• Dx:
• Upper endoscopy, BX
• Tx:
• Non-surgical/ acid suppression/ nutritional status monitored/ anticholinergic medication (help control protein loss). Close watch b/c is a risk factor for ADC of stomach

StomachMallory- Weiss syndrome
• Upper GI hemorrhage due to tearing of GEJ.• Repeated strenuous retching or vomiting may be
responsible for the tears in the mucosa• Significant hemorrhage can occur• results from prolonged and forceful vomiting, coughing or
convulsions. • Typically the mucous membrane at the junction of the
esophagus and the stomach develops lacerations which bleed, evident by bright red blood in vomitus, or bloody stools.
• It may occur as a result of excessive alcohol ingestion. • This is an acute condition which usually resolves within
10 days without special treatment.

StomachMallory- Weiss syndrome
• Etiology:• Strong Valsalva maneuvers, causes stress on mucosa• Retching from acute alcohol intoxication• Heavy lifting• Child birth• Vomiting • Blunt abd. Trauma• Seizures.

Mallory-Weiss Tear

Mallory –Weiss Tear

StomachMallory-Weiss syndrome
• S/S:• Hematemesis• Melena• Hematochezia• Symptoms of hemodynamic instability (back of bleeding)• Lab:• Coagulation values and serial Hct.• Dx:• Presence of blood in NG tube when gastric lavage, then should
prompt endoscopy.

StomachMallory-Weiss syndrome
• Tx:• Conservative• Due to hypovolemia (bleeding) fluid resuscitation• Acid suppression• H2, PPI’s• Surgery is last resort

StomachGastric polyps
• Rare in stomach, but since more pts have undergone endoscopy the Dx of this pathology has become more common.
• 2 types:• Hyperplastic, more common, benign• Adenomatous, more risk of malignant degeneration• Size:• Less than 0.5 risk of malignancy is very low• Greater than 1.5 great risk of malignancy• Peutz-Jeghers syndrome is an autosomal dominant, characterized
by benign polyps in small intestine and melanous spots on lips and buccal mucosa. 50% may develop cancer.
• Tx is conservative, infrequently malignancy.

StomachBezoar
• Large masses of indigestible fiber within stomach.• Phytobezoar ---it is a bezoar made up of vegetable fiber• Trichobezoar ---it is made up of hair• MC seen in children and mentally challenged inmates in mental
institutions• S/S:• As a gastric outlet syndrome symptoms• Dx: endoscopy.

Fabric Bezoar

Stomach Bezoar

Duodenum
• It receives chyme from stomach.• Drainage of bile from liver and pancreatic secretions.• Intestinal Phase (3rd phase )of acid stimulation happen
when products of digestion arrive at the small intestine. It produces some hormones, enterooxyntin which stimulates acid production, Secretin (by Duodenal S cells) inhibits acid production, Gastrin, and motility of stomach. CCK and GIP (gastro inhibitory peptide) also released by duodenal cells supress gastric acid production
• 4 regions:• Duodenal bulb (1st part)

Duodenum
• Descending duodenum (2nd part, intestinal pacemaker site, Ampulla Of Vater (hepato-pancreatic ampulla and smooth muscle sphyncter or sphyncter of Oddi)enters duodenum in this portion and through this sphyncter bile and pancreatic secretions are released in the GIT)
• Transverse duodenum (3rd part)• Ascending duodenum (4th part)• Duodenum becomes jejunun at ligament of Treitz• Duodenum is mostly retroperitoneal.

Duodenum
• Numerous type of cells:• Absorptive, goblet, granular, endocrine, intestinal and duodenal glands
called Brunner’s glands which protect mucosa.• Blood supply is given by gastroduodenal art. And SMA. Gastroduodenal art
passes posterior to duodenal bulb. Massive upper gastrointestinal hemorrhage may occur when the ulcer erodes into the gastroduodenal artery
• there is a valve at Jejunum and its junction with large intestine and a sphyncter called ileoceccal sphyncter and ileoceccal valve.
• Duodenal bicarbonate Secretion• These are several mechanism that protect duodenum mucosa:• 1) Brunner’s glands secrete mucus that protects mucosa.• 2) duodenal cells secrete NAHCO3, that neutralizes all H ions in duodenal
bulb, secreted by stimulation produce by irritation.• 3) Additional HCO3 comes from pancreas, in response to Secretin.

StomachBenign duodenal ulcer
• This forms part of PUD with gastric ulcers.• 500,000 new cases are Dx every year in USA.• Risk factors are NSAID’S, H. pyloris, tobacco.• Duodenal ulcers rarely arbor malignancy.• S/S:• Burning epigastric abdominal pain, it may radiate to the back (if
ulcer is located in posterior aspect of duodenal bulb.• Pain occurs 1 to 3 hours after food ingestion• Pain is accentuated by fasting, may awaken pt from sleep• Food intake can improve pain• Weight gain• Signs of occult blood loss (guaic + stool), pallor, orthostatic
hypotension

StomachBenign duodenal ulcer
• Dx:
• Upper GI series, now a days is infrequently used as a primary diagnostic tool for PUD, it tends to miss many acute lesions of duodenum.
• Gastric acid analysis is more use for cases that develop duodenal ulcers due to gastrinomas, and due to evolution also has fallen into disuse.
• Current Dx:
• With typical S/S Dx is mostly empirical and non invasive
• Test for H. pyloris:
• Qualitative and quantitave serologic antibodies, good in younger pts
• b/c is low incidence, in older individuals is less reliable of active disease since it can stay for years after infection has been successfully eradicated

StomachBenign duodenal ulcer
• Urease test (identify h. pyloris indirectly by urease activity, urease hydrolyzes urea into ammonia and carbon dioxide. Increased carbon dioxide can be detected in blood or breath. Only good for active disease and when there is erradicaton of bacteria.
• Another non-invasive test is fecal antigen test, that identifies H. pyloris by its antibodies.
• Endoscopy is for pts that failed Tx or worrisome symptoms like gastric ulceration.
• Bx (test for H.pyloris, mostly from antrum)• Tx:• Remove of ulcerogenic agents• Erradication of H.pyloris with antibiotics

StomachBenign duodenal ulcer
• Complications of benign duodenal ulcer:• 1) Perforation, hemorrhage, gastric outlet obstruction and
intractability• Perforated ulcer S/S:• It is a surgical emergency• Acute onset of severe epigastric pain• Tachycardia• Rigid abdomen from diffuse chemical peritonitis• Sometimes it can present as an acute appendicitis when the gastric
acid drains to the right paracolic gutter.• Dx: • abdominal x-ray can give pneumoperitoneum

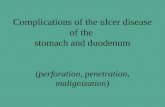
Perforated duodenal ulcer with visible vessel
ulcer
Visible vessel

Perforated duodenal ulcer

PUD

StomachBenign duodenal ulcer
• Tx:• Surgery • if the perforation is less than 6 hours • Plication (oversawn) + acid reducing procedure• If the perforation is more than 6 hours• Plication no acid reducing procedure

StomachBenign duodenal ulcer
• 2) hemorrhage ulcer S/S:• Hematemesis• Melena• Or RBPR• Signs of early or late shock due to bleeding• Hypotension• Tachycardia• Pallor• Mental status changes• Active bleeding

StomachBenign duodenal ulcer
• Dx: • H/P• Endoscopy is affirmatory• Tx: • NG tube + gastric lavage presence of blood suggest upper GI
bleeding • volume resuscitation with cristalloids or whole blood• serial Hct
Coagulation parameters• Blood type and crossmatch• By using endoscopy electrocauterization, heater probe, injection
therapy

StomachBenign duodenal ulcer
• Surgery for refractory bleeding• Acid reducing precedure.• 3) Gastric outlet obstruction S/S:• Usually from ulcer scarring• Stomach needs to be decompress with NG tube for few days. This
helps to decrease swelling and resolution of obstruction.• NPO• Nutrition and fluids IV.• Projectile vomiting of food shortly after eating (seen in babies with
pyloric stenosis).

StomachBenign duodenal ulcer
• Most cases will need operative intervention b/c cicatricial scarring around ulcer, with removal of obstruction or its bypass, antrectomy or gastroenterotomy to drain stomach.
• Acid reducing procedure also necessary.• Endoscopy is necessary to evaluate extension of scarring and take
Bx’s if necessary and screen of H.pyloris• 4) intractable ulcer S/S:• pt has persistent symptoms after adequate Tx. Unresponsive to
conventional medical Tx
this presentations are not very common now a days• It should alert about rare causes of ulceration like Zollinger-Ellison
syndrome

StomachBenign duodenal ulcer
• Surgery is mostly to decrease acid secretion• Vagal interruption by truncal vagotomy with subsequent denervation
of parietal cells, but also causes denervation of antral pump, pyloric sphincter, and abdominal viscera. Also gastric motility is disrrupted.
• Consequences are gastric antral dilation with difficulty draining stomach, and gastrin release. To avoid this is indicated pyloroplasty (pyloroplasty + truncal vagotomy this is associated with lower recurrences).
• Antrectomy is also done instead of pyloroplasty, if previous technique is not possible (antrectomy + truncal vagotomy).
• Other procedures are selective vagotomy,• proximal gastric vagotomy (crows foot near antrum are spare)

Duodenal vs Gastric ulcer
• Duodenal– Increased acid
production
– H. pylori
– relieved by food & awakens patient
– NOT Malignant
• Gastric– Normal or decreased acid
production– Decreased mucosal
resistance
– H. pylori– NSAIDS
– worsened by food
– Malignancy is associated

Surgical TreatmentTruncal Vagotomy -- Heineke-Mikulicz
Pyloroplasty

Selective Vagotomy & Heineke-Mikulicz Pyloroplasty

Proximal Gastric Vagotomy

Massive Gastric Hemorrhage

Perforated Prepyloric Ulcer

Perforated Prepyloric Ulcer

Duodenal Ulcer

Duodenal Ulcer
Penetrating into pancreas

StomachDuodenal polyps
• It is usually of an inherited familial disorder, familail adenomatous polyposis.
• Pts with this autosomal disorder have multiple adenomatous polyps in colon and gastroduodenal region.
• Because possible malignant degeneration of these polyps close monitoring is required.
• Early prophylactic removal of colon• Routine endoscopic evaluation

Duodenal polyp

Stomach and duodenal polyps

Duodenal polyp

Duodenal polyposis

Duodenal polyps

Stomach polyps

StomachZollinger- Ellison Syndrome
• It is caused by a gasrin producing neoplasm (gastrinoma)• Hypergastrinemia --- stimulate parietal cells --- HCL acid is
constantly secreted. • 2/3 of these Tumors are located between cystic duct with common
bile duct, the junction of 2nd and 3rd portion of duodenum and neck of pancreas.
• Gastrinomas can be part of an inherited familial disorder.• There is strong association with MEN 1 (pytuitary adenoma,
hyperparathyroidism, and pancreatic isles cell tumor ( of which gastrinoma is the most common).
• 60 % of gastrinomas are malignant.• 50% of pts with malignant variant die within 5 years of Dx.• Due to slow growth long term survival up to 15 years has been seen.

StomachZollinger- Ellison Syndrome
• S/S: ulcer like symptoms with chronic or severe diarrhea multiple duodenal ulcers in atypical places (jejunun or ileum) Family or personal Hx of refractory PUD or endocrine disease
(MEN-1) Dx: hypergastrinemia (fasting serum gastrin levels over 1000 pg/ml is a
comfirmatory testing + hypersecretion of acid tumor localization Clinical staging CT scan, MRI and U/S screening for MEN-1

StomachZollinger- Ellison Syndrome
• Dx:• H/P ( unusual presentation, family Hx of MEN-1)• Dx rests on establishing hypergastrinemia c hypersecretion of acid.• Fasting serum gastrin levels, Gastrin levels over 1000pg/ml is
considered diagnosis.• Discontinuation of PPI’s 1 week prior. PPI’s increase gastrin levels.• When Dx. is in doubt, test of choice is Secretin stimulation test.
Hight specificity and sensitivity. Elevation of baseline Gastrin level are Dx (IV infusion of Secretin and fasting serum gastrin level taken at 5,10.15, 30, 45, 60 minutes). Values are equal or greater than 200 pg/ml.

StomachZollinger- Ellison Syndrome
• Acid hypersecretion is also measure, values are 2.5 or less are considered (+).
• Next step is localization of TU and staging using Ct scan, MRI and U/S.
• Somatostatin receptor scintigraphy and endoscopic U/S are most used.
• These Tumors are very small and difficult to locate.• Liver is 1st place for MTs.• Beside all these measures Ca is should be obtain b/c if elevated get
levels of PTH if elevated can also suggest hyperparathyroidism which is hightly suggestive of MEN-1

StomachZollinger- Ellison Syndrome
• Newly Dx. Zollinger-Ellison syndrome screen for MEN-1.
• Tx:• MC Tx was total gastrectomy with esophageal anastomosis, but
associated with high mortality and associated metabolic complications like pernicious anemia, malnutrition and weight loss.
• New approach is: PPI’s (high doses) to control HCL, to prevent ulceration.
• H2 are 2nd line agents.

StomachZollinger- Ellison Syndrome
• Surgical exploration only in pts with sporadic gastrinoma w/out mets, and in these cases proximal gastric vagotomy is done to decreased acid production. If tumor is found cure is possible.
• Tx for gastrinomas + MEN-1 is controversial. If hyperparathyroidism is present, parathyroidectomy is indicated b/c it may attenuate gastrin released.
• Cure in this setting c MEN-1 is rare and some experts recommend no surgical exploration if no mets. Other surgeons recommend the opposite, it is controversial and depends on the experience of the surgeon.
• If there are already mets options are: debulking, chemotherapy, hepatic embolization, hormonal tx c Somatostatin analogues (octreotide) which in turn suppresses levels of gastrin and slow tumor growth
• also PPI’S need to be added in this setting.

ZES Jejunal Ulcer

ADC of Duodenum
• Duodenum MC site for ADC.• 2/3 are located in 2nd part of duodenum around peri-ampullar region.• It is no commom and it presents late in its course.• S/S: • Nonespecific abdominal pain, weight loss, gastric outlet obstruction,
melena, hematochezia (due to ulceration of lesion)• H/P unremarkable.• Dx is made by Upper endoscopy and Bx.• CT for local invasion or mets spread.

ADC of Duodenum
• Surgery: • excision when is possible resection of disease
pancreaticoduodenectomy if tumor is in 1st or 2nd portion• if tumor is in 3rd or 4th portion small bowel resection c
duodenojejunostomy• if tumor is unresectable or mets are presented then• gastroenterostomy is indicated• Post surgery radiation can be helpful.• (+) nodes poor prognosis, 5 y survival less than 15%

Duodenal Lymphoma
• Very rare in duodenum MC in ileum.• S/S: • same as those of ADC of duodenum • Nonespecific abdominal pain, weight loss, gastric outlet obstruction,
melena, hematochezia (ulceration of lesion), fatigue.• Complications: perforation, bleeding, and obstruction.• H/P unremarkable• Dx:• Endoscopy• CT for Ds extent.• Follow same guidelines for any lymphoma.• Adjuvant chemo post operatory• Disseminated Ds only chemo + local radiation.

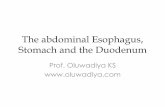
Figures 1 A and B: CT scan (with contrast) of the abdomen and pelvis revealing 7cm, ill-defined mass in the pancreatic head region with involvement of the adjacent duodenum,
peri-pancreatic adenopathy and mild biliary duct dilatation

Duodenal lymphoma

TNM classification
• Tumor Staging: – is determined by TNM classification
• T= primary tumor:
T1=mucosa; T2=invasion of subcutaneous area; T3=adventitia; T4=adjacent tissue
• N= Nodes:
N0=no nodes N1=regional nodes• M= metastatic
M0= no metastasis M1=distant spread

TNM classification
• Based on TNM classification we stage as follows:– Stage I= T1,N0,M0– Stage II= T2,N1,M0– Stage III= T3,N1,M0– Stage IV= any T or N, M1