
Surge Planning January 2017 Enclosure: F - Kingston Hospital · PDF fileSurge Planning Trust...
39
Surge Planning Trust Board Item: 10 Date: 25 th January 2017 Enclosure: F Purpose of the Report: To provide the Board with the Surge Plan for management of Emergency Adult and Paediatric Patients 2016/17. For: Information Assurance Discussion and input Decision/approval Sponsor (Executive Lead): Rachel Williams Chief Operating Officer Author: Rachel Williams Chief Operating Officer Author Contact Details: [email protected]. uk Risk Implications – Link to Assurance Framework or Corporate Risk Register: Strategic Objective 1 Legal / Regulatory / Reputation Implications: Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led Link to Relevant Corporate Objective: Strategic Objective 1 Document Previously Considered By: Recommendations: The Board is asked to note the Surge Plan.
Transcript of Surge Planning January 2017 Enclosure: F - Kingston Hospital · PDF fileSurge Planning Trust...
Surge Planning
Trust Board Item: 10
Date: 25th January 2017 Enclosure: F
Purpose of the Report:
To provide the Board with the Surge Plan for management of Emergency Adult and Paediatric Patients 2016/17.
For: Information Assurance Discussion and input Decision/approval
Sponsor (Executive Lead):
Rachel Williams Chief Operating Officer
Author:
Rachel Williams Chief Operating Officer
Author Contact Details:
Risk Implications – Link to Assurance Framework or Corporate Risk Register:
Strategic Objective 1
Legal / Regulatory / Reputation Implications:
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led
Link to Relevant Corporate Objective:
Strategic Objective 1
Document Previously Considered By:
Recommendations: The Board is asked to note the Surge Plan.
2
DRAFT
Kingston Hospital NHS Foundation Trust
Surge Plan for the management of
emergency adult and paediatric patients
2016 / 2017
Policy Authors Tracey Moore, Associate Director, Emergency Services
Version V 9
Ratifying Committee Executive Management Committee
Approved 18th January 2017
Review date EMC- January 2018
3
Contents
1. Introduction
3
2. Operational pressures escalation levels framework (OPEL)
3
3. Processes to monitor and manage demand
4
3.1 Emergency department (ED) 4
3.2 Bed meetings 4
3.3 Discharge processes 5
3.4 External discussions 5
3.5 Out of hours 5
4. Identifying a rising tide
7
5. Key actions in the management of a rising tide
8
6. Physical bed capacity
17
6.1 Medical wards 17
6.2 Orthopaedic Wards 17
6.3 Surgical Wards 17
6.4 Gynaecology 17
6.5 Bed escalation 18
7. Paediatrics
18
7.1 Operational pressures escalation levels framework (OPEL) 18
7.2 Process to monitor and manage demand 19
7.3 Identifying a rising tide 19
7.4 Key actions in the management of a rising tide 20
7.5 Physical bed capacity 21
7.6 Staff escalation 21
8. Escalation 21
9. Internal Incident 21
9.1 Internal Incident Standby 21
9.2 Declaration of an internal incident 22
9.3 Redirect and closure protocol 22
9.4 Internally declared incident management structure 23
10. Other factors which can impact on operational pressures 24
10.1 Staff escalation 24
10.2 Infection Control 24
10.3 Severe weather conditions 24
Appendicies
4
1. Infection Control Guidance for Bed Managers and On Call Managers 25
2. Severe Weather actions
27
3. Checklist for opening up beds 29
4. Escalation contacts and telephone numbers 31
5. Weekend template 37
6. Emergency Department Capacity Management, Redirect and Closure Protocol(ED Policy) v 8
38
5
1. Introduction
The aim of this plan is to provide an assurance and operational framework to support Kingston Hospital Foundation Trust (KHFT) in the management of operational pressures.
This plan will ensure that KHT:
Plans for peaks of activity providing both an operational structure for escalation and assurance framework for the Trust
Safeguards and maintains all essential services across the Trust;
Manages and safeguards staff
Works in partnership with other agencies
This plan is designed to support partiularly the management of increased activity particularly during the winter period by ensuring efficient and effective use of elective and emergency bed capacity.
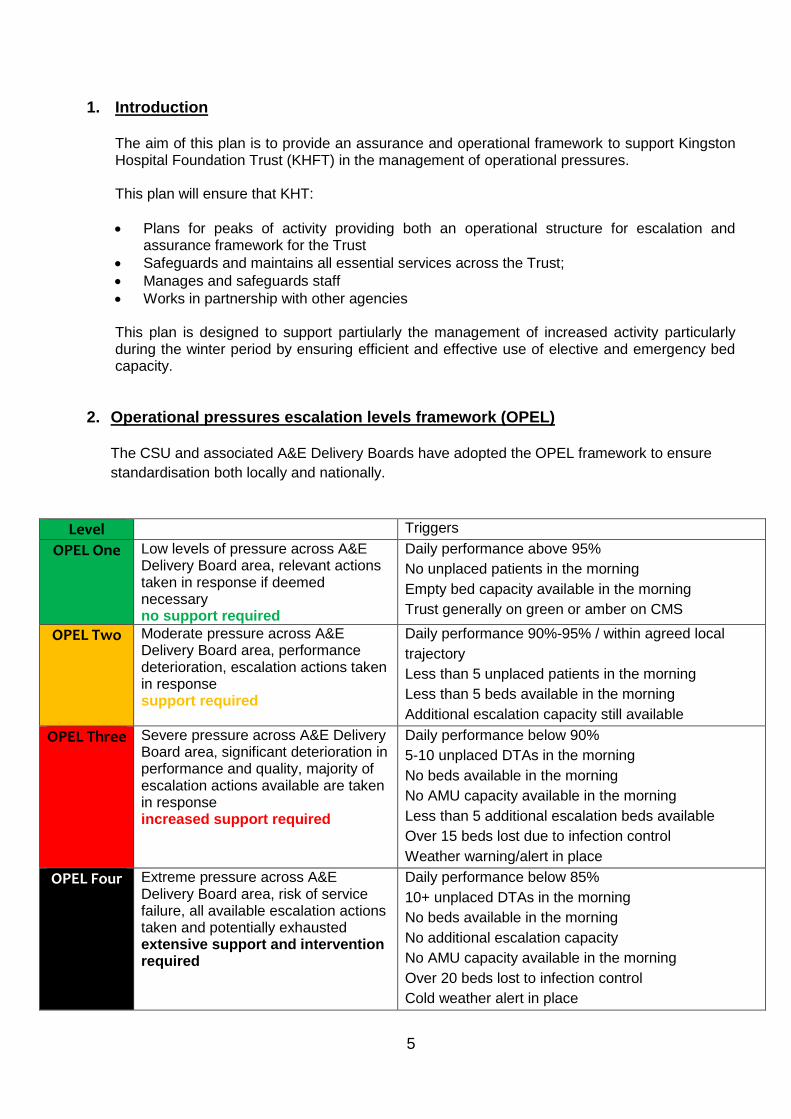
2. Operational pressures escalation levels framework (OPEL) The CSU and associated A&E Delivery Boards have adopted the OPEL framework to ensure
standardisation both locally and nationally.
Level Triggers
OPEL One Low levels of pressure across A&E Delivery Board area, relevant actions taken in response if deemed necessary no support required
Daily performance above 95%
No unplaced patients in the morning
Empty bed capacity available in the morning
Trust generally on green or amber on CMS
OPEL Two Moderate pressure across A&E Delivery Board area, performance deterioration, escalation actions taken in response support required
Daily performance 90%-95% / within agreed local
trajectory
Less than 5 unplaced patients in the morning
Less than 5 beds available in the morning
Additional escalation capacity still available
OPEL Three Severe pressure across A&E Delivery Board area, significant deterioration in performance and quality, majority of escalation actions available are taken in response increased support required
Daily performance below 90%
5-10 unplaced DTAs in the morning
No beds available in the morning
No AMU capacity available in the morning
Less than 5 additional escalation beds available
Over 15 beds lost due to infection control
Weather warning/alert in place
OPEL Four Extreme pressure across A&E Delivery Board area, risk of service failure, all available escalation actions taken and potentially exhausted extensive support and intervention required
Daily performance below 85%
10+ unplaced DTAs in the morning
No beds available in the morning
No additional escalation capacity
No AMU capacity available in the morning
Over 20 beds lost to infection control
Cold weather alert in place

6
3. Processes to monitor and manage demand 3.1 Emergency department (ED)
A briefing takes place each morning to review performance and operational issues from the previous day, to ensure that staffing – both medical and nursing – is robust, to consider any changes to process/flow and to problem resolve. The meeting is chaired by the COO or associate director for emergency services and is attended by the consultant and nurse in charge plus the service line manager and matron.
A member of the ED attends each bed meeting to provide an update on the status of the patients in ED and to escalate issues, as appropriate to the senior management team.
Board rounds take place every two hours, led by the consultant in charge of the shift to review all patients, reallocate resources and to identify any blockages to smooth flow.
Tracking of the patients in ED is undertaken by the ED coordinator who reports directly to the nurse in charge on the shift and is available between 10am and 10pm every day. The ED board on CRS is used for this purpose
The service line manager for ED/nurse in charge of the shift maintains close liaison with the LAS. This ensures that both parties are aware of any expected increases in ambulance activity and can act accordingly. A board is available within ED which alerts the staff of incoming blue light ambulances.
CMS is utilized to record the situation at all ED’s throughout London. ED and the Advanced Site Practitioners (ASP’s) input the information 2 hourly throughout the day and 4 hourly at night to provide an overall view of demand across London. This information is viewed by LAS and the SW London CSU.
3.2 Bed meetings
The bed meetings, which take place three times per day, are used to confirm demand for services and to anticipate and plan for any potential increase in demand.
The bed meetings are chaired by a senior manager and are routinely attended by matrons for each clinical area and service line managers (as required). A transport representative also attends during particularly busy periods to understand and respond to the demand for transport.
At weekends, one bed meeting is held at 12noon. Additional meetings are called by exception by the Advanced Site Practitioner. The bed meeting is attended by social workers, community nurses and hospital and community occupational therapists (OTs)
Information reviewed at the bed meeting includes the following:
o ED attendances per hour o Number of LAS vehicles on the way – the information is available in ED o Drops in temperature as notified to the Trust by the Met office o Beds closed due to infection o Performance against the four hour standard dropping below 95% on two o Consecutive days. o Patients in ED waiting for an identified bed

7
o Patients in ED waiting for a speciality review o Waiting time to be seen by ED o Review ITU bed occupancy o Review patients awaiting repatriation
Bed meetings also identify potential reductions in staffing levels so that early escalation for bank and agency staff can be undertaken and that non-acute based clinical staff can be identified for acute based work e.g. nurse specialists, clinic nurses etc.
3.3 Discharge processes
A definition of DTOC has been agreed by the Trust and external organisations and
discharge coordinators are working to categorise all DTOC under these agreed headings. This is turn will identify early those patients who will benefit from in-reach from community colleagues.
An escalation process has been agreed
A daily ‘delays ‘meeting is chaired by a senior manager and requires each ward sister to identify delays – whether they be internal or external for patients who are clinically optimized. This information is shared with the external partners so that discharges can be facilitated.
An electronic patient tracking list (PTL) has been developed to support internal and external staff to manage the delays and to track progress.
Discharge coordinators work closely with the ward multidisciplinary teams to facilitate discharges and attend the daily RAG boards.
A weekly meeting to review all patients who have been in hospital for more than 7 days, whether they be clinically optimized or not is led by the senior discharge coordinator and includes internal and external colleagues.
3.4 External discussions
A conference call is held daily, led by the CCG. Input is provided by the hospital, CSU, community providers and Richmond and Kingston CCG. This provides an opportunity to report any pressures, to escalate issues requiring resolution and to agree actions.
3.5 Out of hours Each division/service line is responsible for providing the ASP with the following information
List of bank doctors and contact numbers
Weekend template to determine the on call staff working at the weekend and weekend discharges– Appendix 5
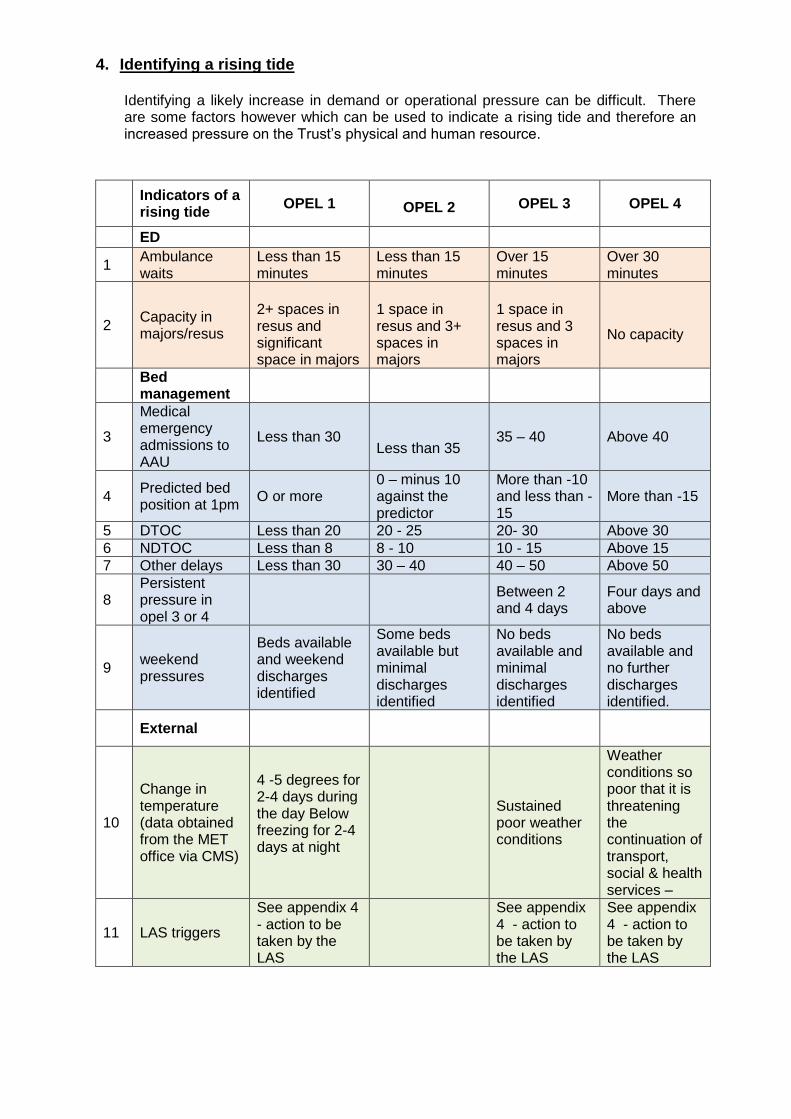
4. Identifying a rising tide
Identifying a likely increase in demand or operational pressure can be difficult. There are some factors however which can be used to indicate a rising tide and therefore an increased pressure on the Trust’s physical and human resource.
Indicators of a rising tide
OPEL 1
OPEL 2 OPEL 3 OPEL 4
ED
1 Ambulance waits
Less than 15 minutes
Less than 15 minutes
Over 15 minutes
Over 30 minutes
2 Capacity in majors/resus
2+ spaces in resus and significant space in majors
1 space in resus and 3+ spaces in majors
1 space in resus and 3 spaces in majors
No capacity
Bed management
3
Medical emergency admissions to AAU
Less than 30
Less than 35
35 – 40 Above 40
4 Predicted bed position at 1pm
O or more 0 – minus 10 against the predictor
More than -10 and less than -15
More than -15
5 DTOC Less than 20 20 - 25 20- 30 Above 30 6 NDTOC Less than 8 8 - 10 10 - 15 Above 15 7 Other delays Less than 30 30 – 40 40 – 50 Above 50
8 Persistent pressure in opel 3 or 4
Between 2 and 4 days
Four days and above
9 weekend pressures
Beds available and weekend discharges identified
Some beds available but minimal discharges identified
No beds available and minimal discharges identified
No beds available and no further discharges identified.
External
10
Change in temperature (data obtained from the MET office via CMS)
4 -5 degrees for 2-4 days during the day Below freezing for 2-4 days at night
Sustained poor weather conditions
Weather conditions so poor that it is threatening the continuation of transport, social & health services –
11 LAS triggers
See appendix 4 - action to be taken by the LAS
See appendix 4 - action to be taken by the LAS
See appendix 4 - action to be taken by the LAS
9
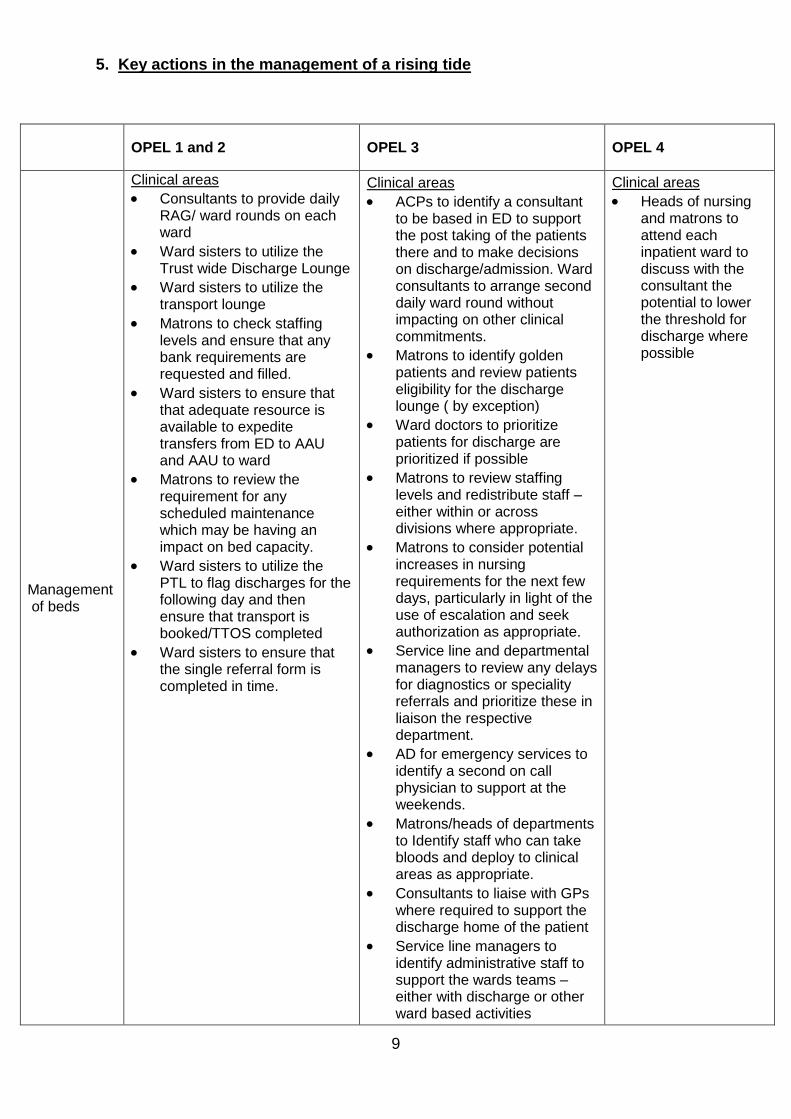
5. Key actions in the management of a rising tide
OPEL 1 and 2 OPEL 3 OPEL 4
Management of beds
Clinical areas
Consultants to provide daily RAG/ ward rounds on each ward
Ward sisters to utilize the Trust wide Discharge Lounge
Ward sisters to utilize the transport lounge
Matrons to check staffing levels and ensure that any bank requirements are requested and filled.
Ward sisters to ensure that that adequate resource is available to expedite transfers from ED to AAU and AAU to ward
Matrons to review the requirement for any scheduled maintenance which may be having an impact on bed capacity.
Ward sisters to utilize the PTL to flag discharges for the following day and then ensure that transport is booked/TTOS completed
Ward sisters to ensure that the single referral form is completed in time.
Clinical areas
ACPs to identify a consultant to be based in ED to support the post taking of the patients there and to make decisions on discharge/admission. Ward consultants to arrange second daily ward round without impacting on other clinical commitments.
Matrons to identify golden patients and review patients eligibility for the discharge lounge ( by exception)
Ward doctors to prioritize patients for discharge are prioritized if possible
Matrons to review staffing levels and redistribute staff – either within or across divisions where appropriate.
Matrons to consider potential increases in nursing requirements for the next few days, particularly in light of the use of escalation and seek authorization as appropriate.
Service line and departmental managers to review any delays for diagnostics or speciality referrals and prioritize these in liaison the respective department.
AD for emergency services to identify a second on call physician to support at the weekends.
Matrons/heads of departments to Identify staff who can take bloods and deploy to clinical areas as appropriate.
Consultants to liaise with GPs where required to support the discharge home of the patient
Service line managers to identify administrative staff to support the wards teams –either with discharge or other ward based activities
Clinical areas
Heads of nursing and matrons to attend each inpatient ward to discuss with the consultant the potential to lower the threshold for discharge where possible

10
Bed management
ASPs to run 3 daily bed meetings
Senior manager to run daily delay meeting and ensure that information arising from this is shared with partners via email.
Senior discharge coordinator to run weekly LOS meeting with partners in attendances
Senior manager to represent KHFT at the daily conference call
Leader of the bed meeting to review the metrics in the above table to see if anything is triggering stage 2 or 3 and assess whether these can be managed within the individual department or have implications across the Trust.
Repatriations and referrals from ITU to be managed promptly.
All to delays as normal through the agreed escalation process
ASP and ED coordinator to update CMS
AD and CDs to ensure that all wards have adequate consultant and junior doctors’ support, reallocating where appropriate.
CD for AAU to liaise with the surgical team to agree any support of outlying medical patients on surgical wards by the surgical and urology FY1s.
Bed management
Leader of the bed meeting to request via service line representatives at the bed meeting that the status of the Trust be communicated to all consultants.
Service lines/divisions to ensure that they have a system in place to communicate to the consultants and to activate this at the request of the leader of the bed meeting.
Leader of the bed meeting to agree the opening of escalation beds ( see appendix 3)
Leader of the bed meeting to agree the use of beds for different specialities.
AD for emergency services to contact senior colleagues in partner organisations in accordance with the delays escalation process.
ASP to contact local hospitals & CCGs personally to achieve repatriations, check their status & establish support
Leader of the bed meeting to review the requirement for any scheduled maintenance which may be having an impact on bed capacity.
Service line managers to review elective programme and consider capacity available in the private patient unit/DSU
Service line managers to request that a member of the surgical/orthopaedic medical
Bed management
Leader of the bed meeting to contact the executive director (COO in hours/on call director out of hours) to join the bed meeting for senior direction.
On call consultants for ED, medicine and surgery to join the bed meeting to support decision making.
Executive director to consider cancellation of all elective admissions except „Clinically critical „ (who must receive care within 24 hours) or complex agreed. Inform theatres not to call new cases until approved by COO.
CDs, service line managers and matron to cancel staff study leave
Executive director to ensure that next stage of escalation is activated for DTOC and informal delays. This includes the calling of a conference call with all partner executives.
Executive director
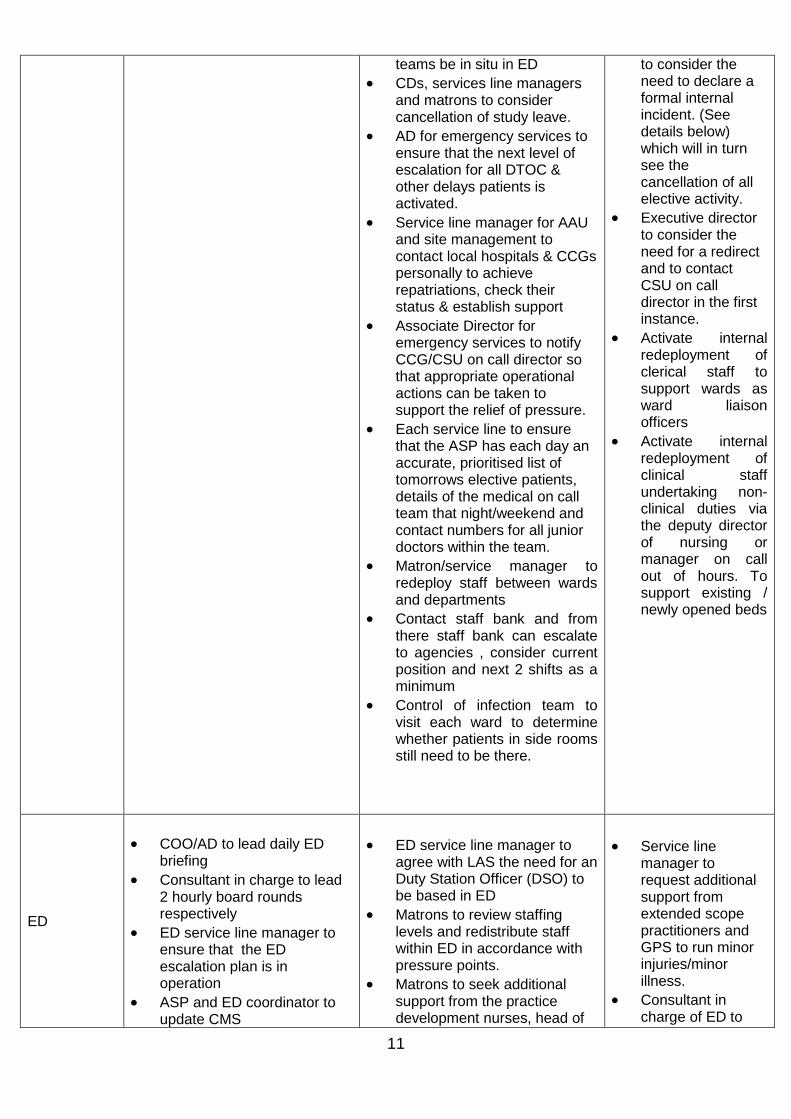
11
teams be in situ in ED
CDs, services line managers and matrons to consider cancellation of study leave.
AD for emergency services to ensure that the next level of escalation for all DTOC & other delays patients is activated.
Service line manager for AAU and site management to contact local hospitals & CCGs personally to achieve repatriations, check their status & establish support
Associate Director for emergency services to notify CCG/CSU on call director so that appropriate operational actions can be taken to support the relief of pressure.
Each service line to ensure that the ASP has each day an accurate, prioritised list of tomorrows elective patients, details of the medical on call team that night/weekend and contact numbers for all junior doctors within the team.
Matron/service manager to redeploy staff between wards and departments
Contact staff bank and from there staff bank can escalate to agencies , consider current position and next 2 shifts as a minimum
Control of infection team to visit each ward to determine whether patients in side rooms still need to be there.
to consider the need to declare a formal internal incident. (See details below) which will in turn see the cancellation of all elective activity.
Executive director to consider the need for a redirect and to contact CSU on call director in the first instance.
Activate internal redeployment of clerical staff to support wards as ward liaison officers
Activate internal redeployment of clinical staff undertaking non-clinical duties via the deputy director of nursing or manager on call out of hours. To support existing / newly opened beds
ED
COO/AD to lead daily ED briefing
Consultant in charge to lead 2 hourly board rounds respectively
ED service line manager to ensure that the ED escalation plan is in operation
ASP and ED coordinator to update CMS
ED service line manager to agree with LAS the need for an Duty Station Officer (DSO) to be based in ED
Matrons to review staffing levels and redistribute staff within ED in accordance with pressure points.
Matrons to seek additional support from the practice development nurses, head of
Service line manager to request additional support from extended scope practitioners and GPS to run minor injuries/minor illness.
Consultant in charge of ED to

12
Matrons to check staffing levels and ensure that any bank /agency requirements are requested and filled.
Medical staffing coordinators to check medical staff shifts and ensure that these are filled/escalated as appropriate
Nurse in Charge and Senior Doctor of each clinical area to manage respective teams to ensure the delivery of safe, effective, care.
ED consultant in charge to maintain close liaison with ACP on call to maintain effective flow for medical patients.
Nurse in charge to ensure that patients are moved within a maximum of 15 minutes of bed becoming available.
Nurse in charge to monitor waits in streaming and allocate resources accordingly.
Nurse in charge to attend bed meetings.
Nurse in charge to ensure any accepted medical patients meeting the fast track criteria are moved to the AAU.
Nurse in charge to ensure that effective communication with patients is maintained: advise them of the waiting time and offer alternative pathways as appropriate (GP Out of Hours; walk-in centre)
Service line manager to liaise closely with the LAS.
midwifery, matrons, directorate of nursing. .
ED consultant in charge to contact consultants on call in each specialty to request attendance in ED and early identification of patients for fast tracking.
ED consultant in charge to request support from the anesthetists and outreach team in the management of resus.
Service line manager/matron to identify porters and nurses to support transfers and to contact other matrons for assistance as required.
ED consultant in charge to request support from any clinicians on site and on non-clinical duties to support clinical area as required by Consultant in charge
ISS to ensure that adequate number of beds/trolleys are available in the ED.
Matrons to check that adequate supplies are available within ED.
Matrons to contact the outreach team and seek support where possible in resus
Matrons to liaise with pharmacy and ISS regarding the provision of medication and food/drink to any patients in ED awaiting admission.
direct as many staff as possible to the management of resus and majors.
Service line manager/matron/ consultant in charge to redesignate space within ED to ensure that patients are safe and appropriately managed.
Consultant in charge and Executive director to consider the booking of alternative community appointments for appropriate patients waiting in ED.
Clinical support services
Departmental heads to ensure that internal standards are being met
Therapies to participate in RAG board meetings and ensure that all assessments are completed in time/escalated as appropriate.
Therapies to attend the weekend bed meeting and
Departmental heads to nominate a representative to attend the bed meeting and take action as appropriate.
Pharmacy to track and report TTO orders at bed meetings
The cardiology team to adjust the elective/non-elective split of activity in the Cath Lab, to accommodate additional in-patient work, whilst
Radiology, physiotherapy, opd theatres to act on instruction from COO to instigate the internal incident plan and cancel outpatient activity and redirect staff to inpatient areas.
Radiology to

13
work collaboratively with therapists in-reaching into the Trust.
All departments to provide 7 day services in accordance with ‘business as usual’.
maintaining elective waiting times.
The service line manager for cardiology to review the need for additional weekend physiology sessions.
The radiology team to adjust the elective/non-elective split of activity to accommodate additional inpatient work if required
The radiology service line manager to review the need for additional sessions at weekends and in the evening if required.
Departmental heads to review workload and prioritise discharges wherever possible
Departmental heads to identify any additional staff available to support the need for increased resource.
Mortuary staff to organize the Nutwell storage unit to be installed in the PM room – as appropriate
ensure requesting doctors are phoned with all inpatient results.
All to cancel meetings and place all clinical staff in clinical areas –with a focus on AAU and ED as appropriate.
External partners
Community health ( see HRCH for detailed information below)
YHC and HRCH to provide in reach services.
Community rehab units to ensure that referrals are reviewed early in the day and that decisions are communicated immediately to the respective ward.
Social care
Social care to ensure that packages of care are set up as soon as possible from the issuing of notification.
Social care to provide details of potential nursing homes for families to visit and to provide families with a deadline for completion of the visits.
Community health ( see HRCH for detailed information below)
YHC to provide information Social care Richmond and Wandsworth and Kingston
Social Care to review additional support that can be offered to expedite discharges
Additional on-site support for assessments will be available as soon as practical upon notification
Joint working with community
Community health ( see HRCH for detailed information below)
YHC to provide information
Social care Richmond and Wandsworth and Kingston
flexing of placement criteria for short term placements to alleviate pressure on acute beds within available capacity
14
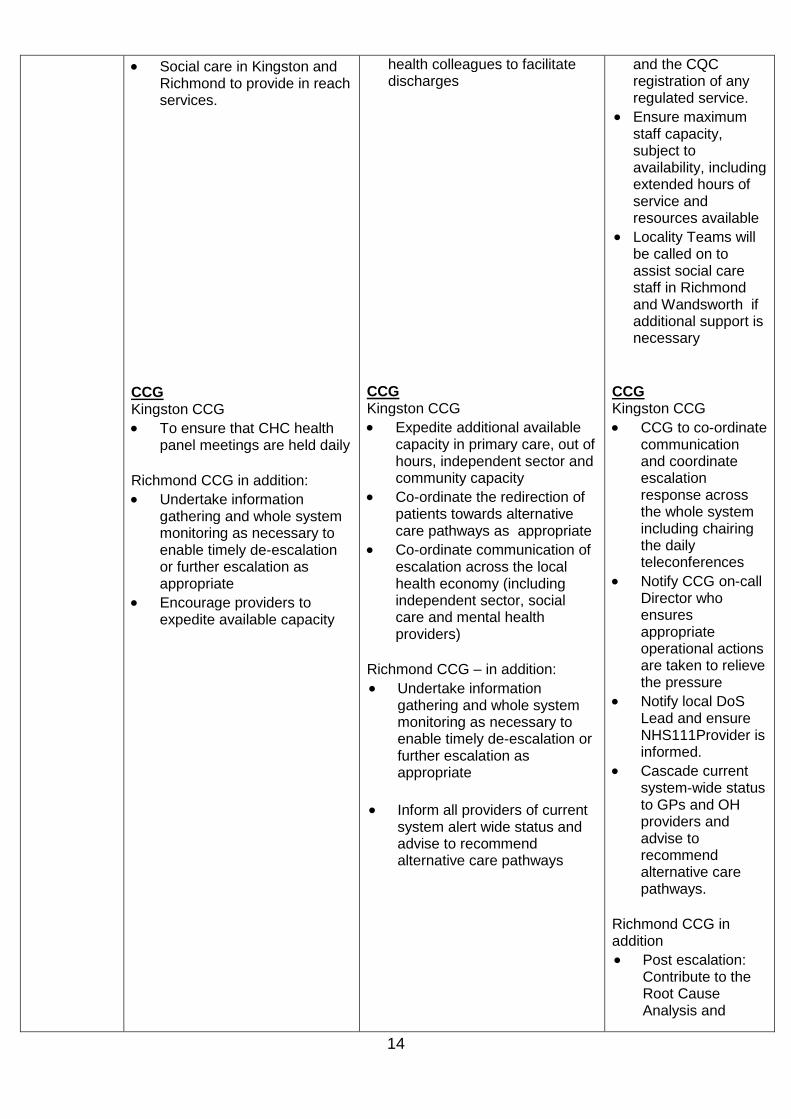
Social care in Kingston and Richmond to provide in reach services.
CCG Kingston CCG
To ensure that CHC health panel meetings are held daily
Richmond CCG in addition:
Undertake information gathering and whole system monitoring as necessary to enable timely de-escalation or further escalation as appropriate
Encourage providers to expedite available capacity
health colleagues to facilitate discharges
CCG Kingston CCG
Expedite additional available capacity in primary care, out of hours, independent sector and community capacity
Co-ordinate the redirection of patients towards alternative care pathways as appropriate
Co-ordinate communication of escalation across the local health economy (including independent sector, social care and mental health providers)
Richmond CCG – in addition:
Undertake information gathering and whole system monitoring as necessary to enable timely de-escalation or further escalation as appropriate
Inform all providers of current system alert wide status and advise to recommend alternative care pathways
and the CQC registration of any regulated service.
Ensure maximum staff capacity, subject to availability, including extended hours of service and resources available
Locality Teams will be called on to assist social care staff in Richmond and Wandsworth if additional support is necessary
CCG Kingston CCG
CCG to co-ordinate communication and coordinate escalation response across the whole system including chairing the daily teleconferences
Notify CCG on-call Director who ensures appropriate operational actions are taken to relieve the pressure
Notify local DoS Lead and ensure NHS111Provider is informed.
Cascade current system-wide status to GPs and OH providers and advise to recommend alternative care pathways.
Richmond CCG in addition
Post escalation: Contribute to the Root Cause Analysis and
15
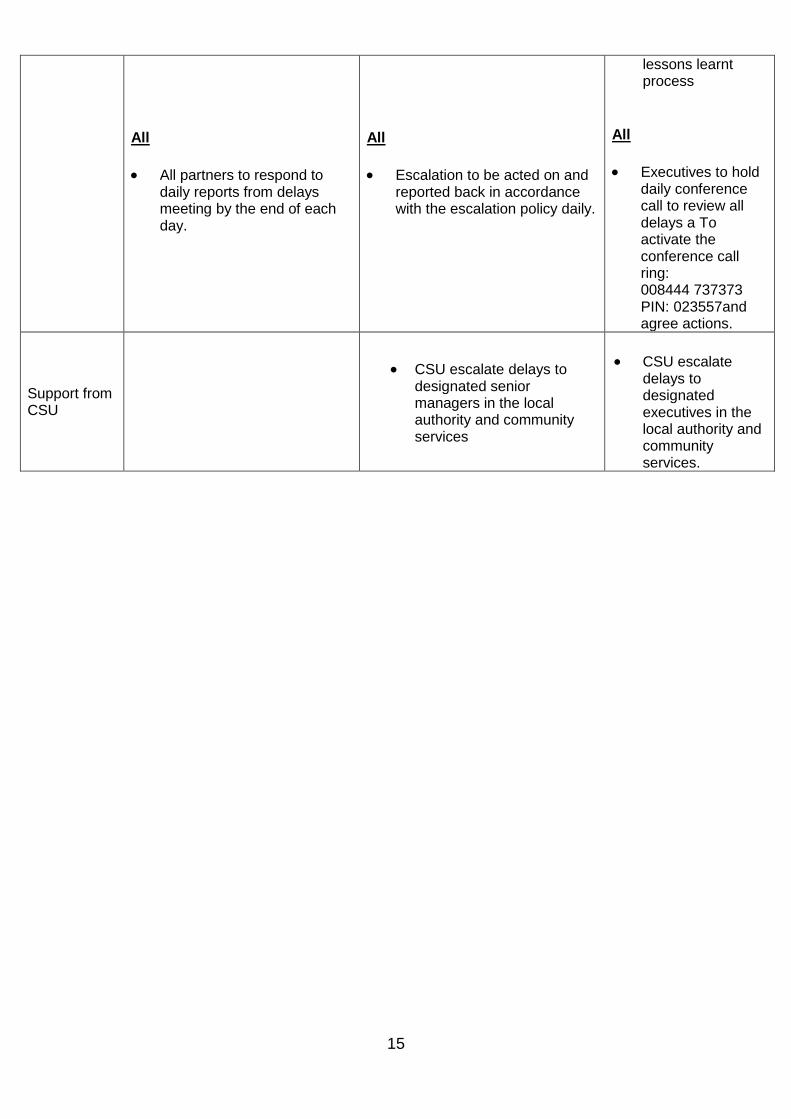
All
All partners to respond to daily reports from delays meeting by the end of each day.
All
Escalation to be acted on and reported back in accordance with the escalation policy daily.
lessons learnt process
All
Executives to hold daily conference call to review all delays a To activate the conference call ring: 008444 737373 PIN: 023557and agree actions.
Support from CSU
CSU escalate delays to designated senior managers in the local authority and community services
CSU escalate delays to designated executives in the local authority and community services.
16
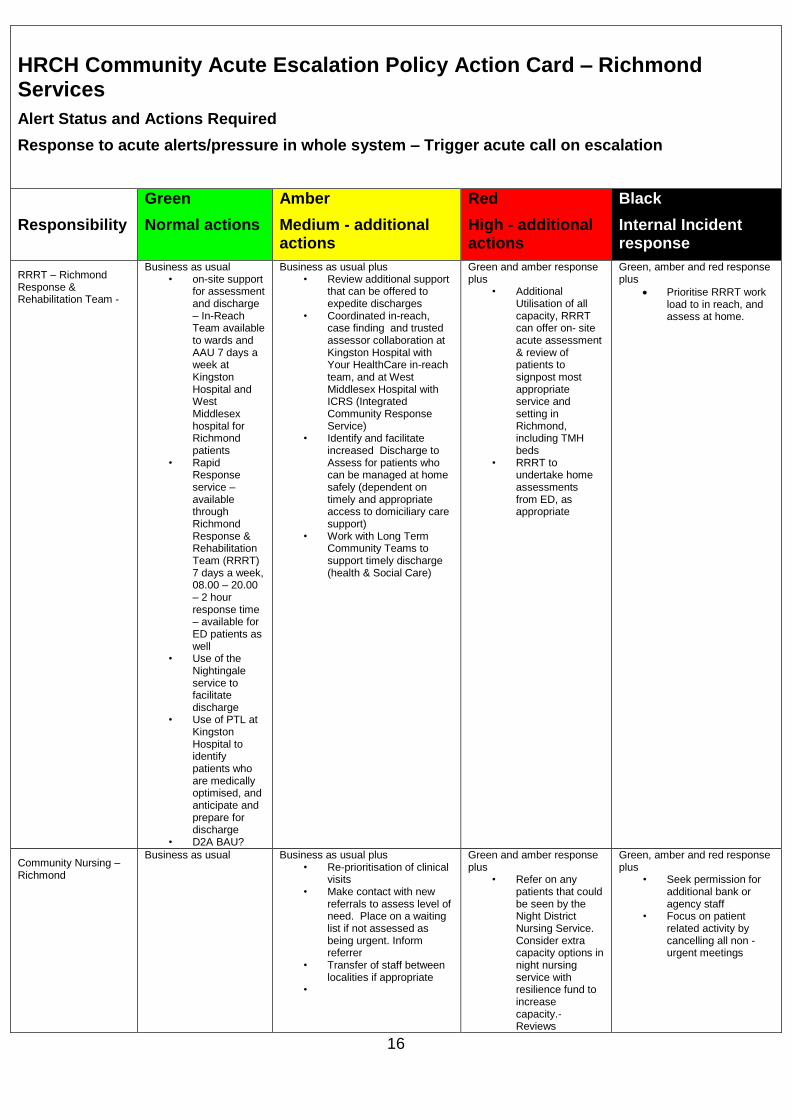
HRCH Community Acute Escalation Policy Action Card – Richmond Services
Alert Status and Actions Required
Response to acute alerts/pressure in whole system – Trigger acute call on escalation
Responsibility
Green
Normal actions
Amber
Medium - additional actions
Red
High - additional actions
Black
Internal Incident response
RRRT – Richmond Response & Rehabilitation Team -
Business as usual • on-site support
for assessment and discharge – In-Reach Team available to wards and AAU 7 days a week at Kingston Hospital and West Middlesex hospital for Richmond patients
• Rapid Response service – available through Richmond Response & Rehabilitation Team (RRRT) 7 days a week, 08.00 – 20.00 – 2 hour response time – available for ED patients as well
• Use of the Nightingale service to facilitate discharge
• Use of PTL at Kingston Hospital to identify patients who are medically optimised, and anticipate and prepare for discharge
• D2A BAU?
Business as usual plus • Review additional support
that can be offered to expedite discharges
• Coordinated in-reach, case finding and trusted assessor collaboration at Kingston Hospital with Your HealthCare in-reach team, and at West Middlesex Hospital with ICRS (Integrated Community Response Service)
• Identify and facilitate increased Discharge to Assess for patients who can be managed at home safely (dependent on timely and appropriate access to domiciliary care support)
• Work with Long Term Community Teams to support timely discharge (health & Social Care)
Green and amber response plus
• Additional Utilisation of all capacity, RRRT can offer on- site acute assessment & review of patients to signpost most appropriate service and setting in Richmond, including TMH beds
• RRRT to undertake home assessments from ED, as appropriate
Green, amber and red response plus
Prioritise RRRT work load to in reach, and assess at home.
Community Nursing – Richmond
Business as usual Business as usual plus • Re-prioritisation of clinical
visits • Make contact with new
referrals to assess level of need. Place on a waiting list if not assessed as being urgent. Inform referrer
• Transfer of staff between localities if appropriate
•
Green and amber response plus
• Refer on any patients that could be seen by the Night District Nursing Service. Consider extra capacity options in night nursing service with resilience fund to increase capacity.- Reviews
Green, amber and red response plus
• Seek permission for additional bank or agency staff
• Focus on patient related activity by cancelling all non -urgent meetings

17
community matron availability, reallocate as required
Community Matrons - Richmond
Business as usual Business as usual plus
Review community matron
availability, reallocate as
required.
Green and amber response plus
Cancel non-urgent
assessment/revie
ws and optimise
support from CM
to enhance
DN/RRRT
capacity.
Redeployment
and use
community
matrons for
assessment and
reviews within DN
teams
Green, amber and red response plus
• Reprioritise patient related activities to those with life supporting care needs and those that would need hospital admission if the service was withdrawn
• Seek permission for additional bank or agency staff
• Focus on patient related activity by cancelling all non -urgent meetings
• Community matrons join inreach at the hospital , with known patients
Specialist Nursing - Richmond
Business as usual Business as usual
Green and amber response plus
• Increase capacity with resilience fund for bank/agency hours to cope with IV therapy demand.
Green, amber and red response plus
• Review specialist team’s availability, reallocate as appropriate to support capacity in DN/CM/RRRT/ICRS teams.
Teddington Memorial Hospital In Patient Unit - Richmond
Business as usual • Daily liaison
with RRRT in reach and rapid response to facilitate timely access to step up and step down beds at TMH
• Clear Estimated Date of Discharge (EDD) set on admission, and actions towards discharge monitored & reviewed at weekly MDTs and daily board rounds
• Regular escalation of delays to relevant internal and external stakeholders to expedite planned discharge
Business as usual plus • Review potential bringing
forward of TMH discharges to expedite transfers from acutes as appropriate and within admission criteria
• Keep social care managers informed
Green and amber response plus
• Daily liaison with social care, RRRT reablement & Continuing Healthcare to prioritise resources to expedite transfers
Green, amber and red response plus
• Reciprocal arrangement to consider admission to Teddington Memorial Hospital or Tolworth Hospital for appropriate patients requiring rehabilitation registered with Richmond & Kingston CCGs between HRCH and Your HealthCare when one or the other has limited capacity
18
6. Physical bed capacity
6.1 Medical wards
The medical unit comprises 7 wards with a total of 204 funded beds plus the acute assessment unit which has 50 beds. During period of increased activity, no additional physical space is available for escalation. Medical patients can however be accommodated in available beds on Isabella, subject to appropriate nurse staffing. Medicine can also access additional beds on AAU if surgery accommodates its emergency demand through Astor and Alex Ward.
16 beds are available on Claremont Ward and can be used if appropriately staffed.
6.2 Orthopaedic Wards
Orthopaedics has 38 funded beds for its elective and emergency activity. During the periods of increased activity the service can flex into a further 18 beds on Claremont Ward for elective activity thereby releasing bed capacity for the emergency activity. Staffing levels have been modelled in anticipation of this increase.
6.3 Surgical Wards
The surgical ward has 40 funded beds, but has access to a further 10 beds on level 4 of the surgical centre to cope with increased emergency activity and to maintain elective activity throughout busy periods
Surgical emergency admissions are admitted to the AAU from where they are transferred to a surgical inpatient ward if an inpatient stay of over 72 hours is required. These beds can be used flexibly with the department of medicine and can be flexed up and down as required. Again the use of these beds is dependent on appropriate staffing levels.
6.4 Gynaecology
Isabella, the gynaecology ward has 15 funded beds and has access to a further 7 beds as required, if appropriately staffed. Gynaecology can also use the assisted conception unit (ACU) for recovery of elective patients, subject to activity in the ACU.
19
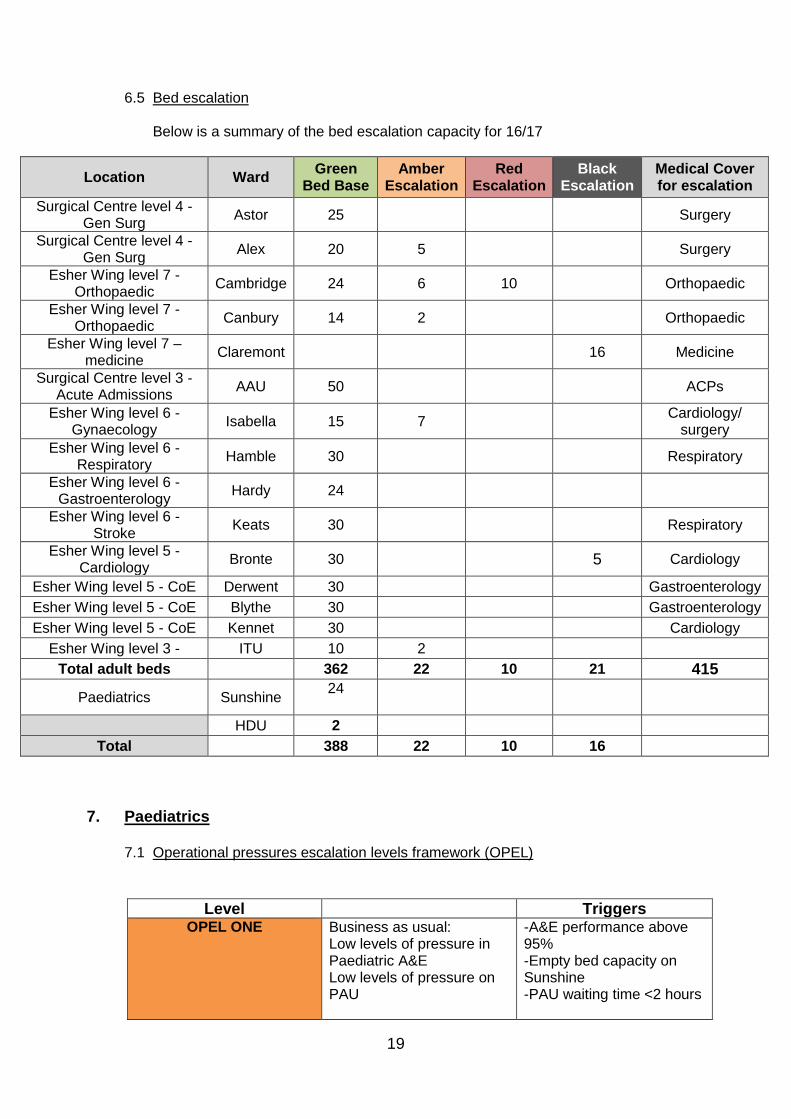
6.5 Bed escalation
Below is a summary of the bed escalation capacity for 16/17
Location Ward Green
Bed Base Amber
Escalation Red
Escalation Black
Escalation Medical Cover for escalation
Surgical Centre level 4 - Gen Surg
Astor 25
Surgery
Surgical Centre level 4 - Gen Surg
Alex 20 5
Surgery
Esher Wing level 7 - Orthopaedic
Cambridge 24 6 10
Orthopaedic
Esher Wing level 7 - Orthopaedic
Canbury 14 2
Orthopaedic
Esher Wing level 7 – medicine
Claremont 16 Medicine
Surgical Centre level 3 - Acute Admissions
AAU 50
ACPs
Esher Wing level 6 - Gynaecology
Isabella 15 7
Cardiology/ surgery
Esher Wing level 6 - Respiratory
Hamble 30
Respiratory
Esher Wing level 6 - Gastroenterology
Hardy 24
Esher Wing level 6 - Stroke
Keats 30
Respiratory
Esher Wing level 5 - Cardiology
Bronte 30
5 Cardiology
Esher Wing level 5 - CoE Derwent 30
Gastroenterology
Esher Wing level 5 - CoE Blythe 30
Gastroenterology
Esher Wing level 5 - CoE Kennet 30
Cardiology
Esher Wing level 3 - ITU 10 2
Total adult beds 362 22 10 21 415
Paediatrics Sunshine 24
HDU 2
Total
388 22 10 16
7. Paediatrics
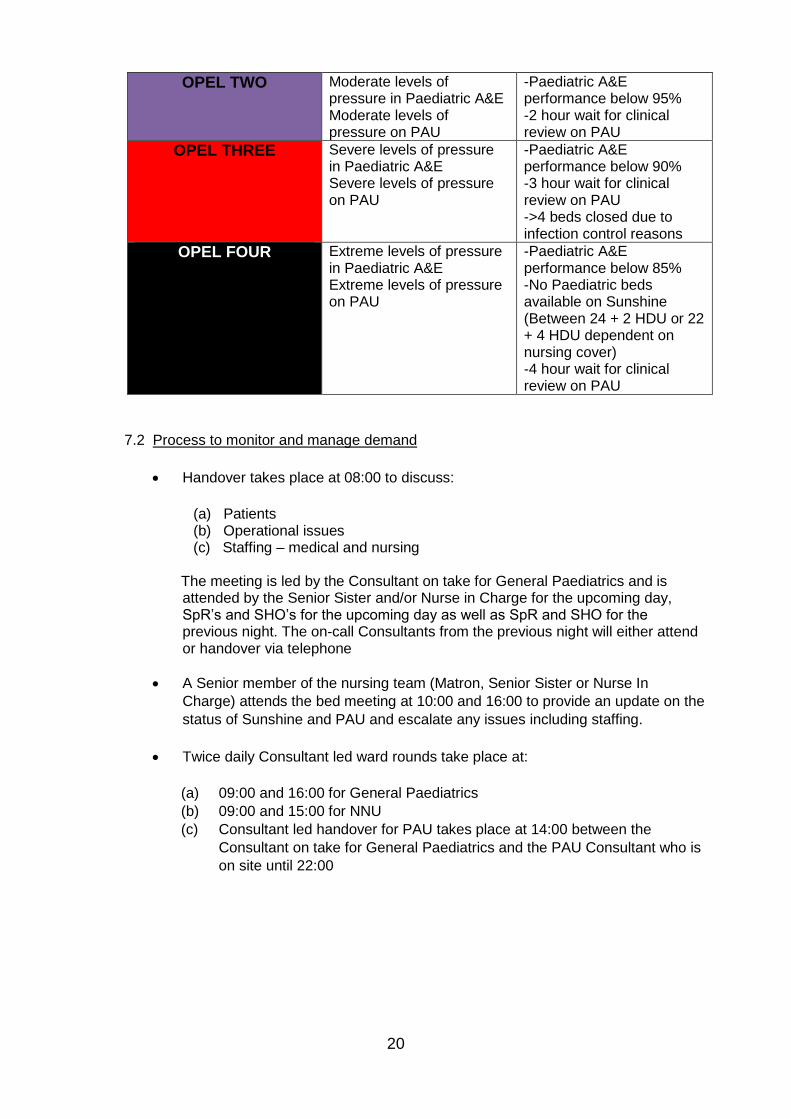
7.1 Operational pressures escalation levels framework (OPEL)
Level Triggers OPEL ONE Business as usual:
Low levels of pressure in Paediatric A&E Low levels of pressure on PAU
-A&E performance above 95% -Empty bed capacity on Sunshine -PAU waiting time <2 hours
20
OPEL TWO Moderate levels of pressure in Paediatric A&E Moderate levels of pressure on PAU
-Paediatric A&E performance below 95% -2 hour wait for clinical review on PAU
OPEL THREE Severe levels of pressure in Paediatric A&E Severe levels of pressure on PAU
-Paediatric A&E performance below 90% -3 hour wait for clinical review on PAU ->4 beds closed due to infection control reasons
OPEL FOUR Extreme levels of pressure in Paediatric A&E Extreme levels of pressure on PAU
-Paediatric A&E performance below 85% -No Paediatric beds available on Sunshine (Between 24 + 2 HDU or 22 + 4 HDU dependent on nursing cover) -4 hour wait for clinical review on PAU
7.2 Process to monitor and manage demand
Handover takes place at 08:00 to discuss:
(a) Patients (b) Operational issues (c) Staffing – medical and nursing
The meeting is led by the Consultant on take for General Paediatrics and is attended by the Senior Sister and/or Nurse in Charge for the upcoming day, SpR’s and SHO’s for the upcoming day as well as SpR and SHO for the previous night. The on-call Consultants from the previous night will either attend or handover via telephone
A Senior member of the nursing team (Matron, Senior Sister or Nurse In
Charge) attends the bed meeting at 10:00 and 16:00 to provide an update on the
status of Sunshine and PAU and escalate any issues including staffing.
Twice daily Consultant led ward rounds take place at:
(a) 09:00 and 16:00 for General Paediatrics
(b) 09:00 and 15:00 for NNU
(c) Consultant led handover for PAU takes place at 14:00 between the
Consultant on take for General Paediatrics and the PAU Consultant who is
on site until 22:00
21
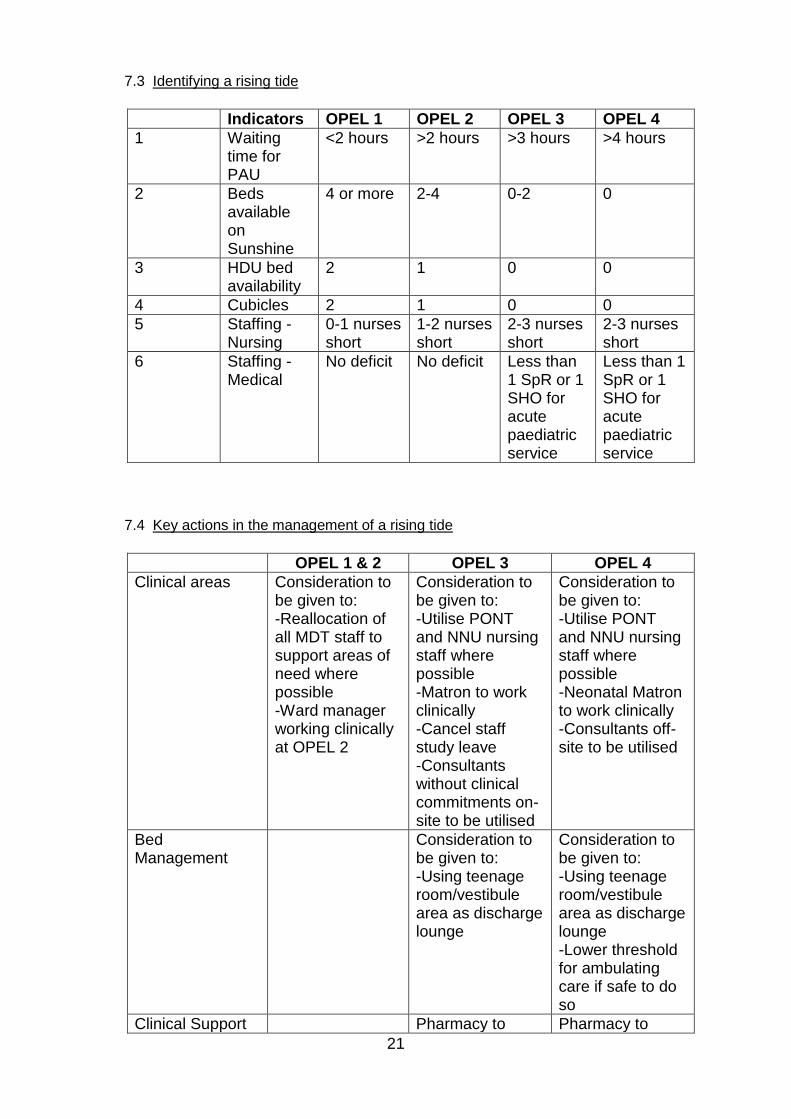
7.3 Identifying a rising tide
Indicators OPEL 1 OPEL 2 OPEL 3 OPEL 4
1 Waiting time for PAU
<2 hours >2 hours >3 hours >4 hours
2 Beds available on Sunshine
4 or more 2-4 0-2 0
3 HDU bed availability
2 1 0 0
4 Cubicles 2 1 0 0
5 Staffing - Nursing
0-1 nurses short
1-2 nurses short
2-3 nurses short
2-3 nurses short
6 Staffing - Medical
No deficit No deficit Less than 1 SpR or 1 SHO for acute paediatric service
Less than 1 SpR or 1 SHO for acute paediatric service
7.4 Key actions in the management of a rising tide
OPEL 1 & 2 OPEL 3 OPEL 4
Clinical areas Consideration to be given to: -Reallocation of all MDT staff to support areas of need where possible -Ward manager working clinically at OPEL 2
Consideration to be given to: -Utilise PONT and NNU nursing staff where possible -Matron to work clinically -Cancel staff study leave -Consultants without clinical commitments on-site to be utilised
Consideration to be given to: -Utilise PONT and NNU nursing staff where possible -Neonatal Matron to work clinically -Consultants off-site to be utilised
Bed Management
Consideration to be given to: -Using teenage room/vestibule area as discharge lounge
Consideration to be given to: -Using teenage room/vestibule area as discharge lounge -Lower threshold for ambulating care if safe to do so
Clinical Support Pharmacy to Pharmacy to
22
Services prioritise/fast track TTOs
prioritise/fast track TTOs
Community See above re PONT and ambulatory care
See above re PONT and ambulatory care
7.5 Physical bed capacity
Sunshine ward compromises of 24 beds (8 cubicles) plus 2 HDU beds PAU compromises of 7 beds (3 cubicles) There is no additional/escalation capacity for Paediatric patients If no beds are available, the department would implement our treat and transfer policy
7.6 Staff escalation
As per above table: ‘4. Key actions in the management of a rising tide’
8. Escalation
It is critical that communication between partner organisations is effective at all Times, but particularly when pressures increase and organisations move between opel 1 and 2 to levels 3 and 4. Appendix 4 provides details of contacts at each level in hours and out of hours.
9. Internal incident
If the Trust is at OPEL 4, consideration will be given as to whether an internal
incident should be called.
9.1 Internal Incident Standby
The Chief Operating Officer (COO) is responsible for the declaration of the standby phase. In considering this, the COO will liaise with: The ED consultant in charge The Acute Care physician on call The medical director SWL CSU - 0844 822 2888 – pager is SWL1 Out of hours the on call director will liaise with
23
The ED consultant in charge The acute care physician on call The internal incident standby phase should be initiated if there is a likelihood (See Triggers) that we are moving from OPEL level 3 (Red) to level 4 (Black). The standby phase will allow us to pre-emptively strengthen and enhance our existing management arrangements (for example the required attendance of medical/surgical consultants at the bed management meetings). The Standby phase affords all decision makers an opportunity to gain situational awareness and implement additional command and control arrangements in a measured and proportionate manner. Decisions made during the standby phase should be recorded in a contemporaneous decision log, this should also include the rational for escalation and de-escalation of the Incident. Switchboard has a list of those members of staff who will be contacted to inform them that we are in ‘internal incident standby’ – in hours and out of hours. These are as follows:
ASP
Oncall manager
COO/On call director
Associate Directors
On call consultant physician
On call communications officer
AE sister in charge
Bleep holders for surgical, paeds, orthopaedics, medical, maternity, breast and gynaecology wards.
Emergency Planning manager
ISS manager
Education centre/security for access to the command rooms
Director of estates and facilities
9.2 Declaration of an internal incident.
The Chief Operating Officer (COO) in hours or the on call director out of hours is responsible for the declaration of an internal incident. On declaration the Chief Operating Officer (COO) in hours or the on call director out of hours will assume the role of Gold Commander and will notify switchboard to confirm to the above, that ‘ an internal incident has been declared’ plus a description of the nature of the incident. The business continuity plan, rapid discharge policy and major incident policy will be used to manage the internal incident ( via the intranet) until such a time as an internal incident policy is agreed.
9.3 Redirect and closure protocol
Guidance issued by NHS England (London) and effective from 9th December 2016 states that Trusts must seek to manage pressure locally without resorting to a redirection or closure.
Redirection of ambulance traffic is no longer possible, across London, with the following limited exceptions:

24
Under extra-ordinary circumstances, LAS have the option of instigating a blue light redirect if they are aware of very high numbers of blue light conveyances
having been directed to one site over a short duration. These would be advised to NHS England via pager message as now. Trusts may not contact LAS to request this.
Closure or redirect for serious infrastructure failure - fire, flood etc (Section 5)
For an agreed period during departmental works (Section 6).
NHS England London, in conjunction with NHSI, reserves the right to consider the implementation of a diversion or closure in certain scenarios, where it considers this is appropriate for the preservation of service integrity and resilience.
See appendix 6 for further details. Although a request for a redirect is not permissible for capacity shortfalls, it is recommended that the LAS switchboard is contacted via Kingston switchboard. When put through, ask for the incident delivery manager for south London and discuss the capacity pressures. Site presence from the LAS may be requested.
9.4 Internally declared incident management structure
On declaration of an internal incident the management and coordination
processes that are currently in place will move to a formal incident management structure.
In hours – 9 am – 5pm Out of Hours 5pm – 9am
Gold – Executive
level Chief Operating Officer On Call Director
Silver – Management
Level
Associate Directors
Head of Nursing Deputy directors of nursing Head of Communications
ASP On Call Manager
On Call Medical Consultant On Call Communications
Bronze – Operational
Level
Service line managers Matrons
All ward managers Discharge Coordinators
Nurses in Charge On Call Staff
NHS England (London) and the CSU will need to be informed in the event of an Internal Incident being declared.
The following roles and responsibilities will apply in the event of an Internal Incident being declared:
Executive Team / COO (in hours) or On Call Director (out
of hours)
Provide gold command and communications outside and inside organisations. Ensure support for general staff wellbeing.
On Call Manager Act a silver command and lead the management of the situation
Medical Consultant On Call Be part of the Incident Management Team to manage the medical response
Site Team Be part of the Incident Management Team to manage patient

25
flow
Departmental Heads Ensure all ward activity is prioritised and activate local escalation steps/plans. Provide where possible ward liaison staff.
Matrons, ward managers and discharge coordinators:
Flex staffing to support activity and focus on patients who might be suitable for discharge and escalate accordingly.
Clinical Directors Instigate additional ward rounds and actively pull patients from AAU. Allocate registrars to work directly in ED to process specialty referrals speedily
Community Teams
Attend the hospital site and under the direction of discharge coordinators actively review and transfer patients out (without prejudice) or if working offsite, ensure regular liaison with discharge coordinators to facilitate this.
10. Other factors which can impact on operational pressures
10.1 Staff Escalation
If bed numbers need to be increased and therefore additional staff are required, the Head of Nursing or ASP (out of hours) should:
Redeploy staff between wards and departments
Contact staff bank and from there staff bank can escalate to agencies ,
consider current position and next 2 shifts as a minimum
Activate internal redeployment of clinical staff undertaking non-clinical
duties via the deputy director of nursing or manager on call out of hours.
To support existing / newly opened beds
Activate internal redeployment of clerical staff to support wards as ward
liaison officers
10.2 Infection Control
Infection control guidance is shown in Appendix 1 The guidance advises on the arrangements in place for infectious conditions and how cohorting can be used. For further general guidance refer to the Trust Infection Control Policies and Procedures that are published via the Intranet, which include:
Pandemic Influenza plan
Pandemic flu guidelines
Diarrhoea Procedure / Diarrhoea Algorithm / Diarrhoea Checklist
Chicken pox and Shingles Guidelines
Major Outbreak Plan
Isolation Procedures
Cleaning Procedures
Hand Hygiene Policy
10.3 Severe weather conditions
See appendix 2.
26
Appendix 1 - Infection Control Guidance for Bed Managers and On Call Managers For full Infection Control guidance please refer to the infection control pages on Datix. In particular:
Outbreak Management Policy
Isolation Procedures – source isolation
The three cleans Policies are also available on each infectious condition outlined below. Contacting the Infection prevention & Control Team (IPCT): The microbiologists provide 24-hour cover to the Trust via switchboard. During normal working hours call:
Consultant Microbiologist: 3540 Infection Control Clinical Nurse Specialists: 2310/ 3369 or bleep 667/ 668
Conditions requiring priority for isolation (The IPCT will advise on priority for isolation when necessary)
Flu
TB
Diarrhoea and / or vomiting
Chicken Pox / Shingles
Meningitis – bacterial
MRSA o Priority for side room in orthopaedics and surgery at all times. o In medicine a side room is necessary if open wound, exfoliating skin or
coughing.
Highly resistant organisms such as ‘ESBL’ coliforms, Acinetobacter or VRE
TB
If TB is suspected the patient must go to a side room, with the door closed. If the patient is either young, has a history of HIV, drug abuse or is of Afro-Caribbean or African origin then they should go into a Negative pressure isolation room. This is until we can exclude multi drug resistant strains. Isolation must be maintained until the patient has had 2 weeks of treatment.
Diarrhoea and Vomiting (i.e. Norovirus)
Any patient presenting with diarrhoea and /or vomiting, which is likely to be an infectious cause, should be nursed in a single room. The diarrhoea algorithm (available on Datix) can be used as a tool to enable diagnosis of likely infectious cause of diarrhoea. Isolation must continue until the patient is 48 hours free of symptoms. If a patient with symptoms is moved out of a bay into a side room, the bay must remain closed for 48 hours until it is evident that no other patients are symptomatic. If there is more than one patient with symptoms of diarrhoea and / or vomiting in a bay, it is possible to cohort the patients together in the bay. Again, isolation must continue until the patients are 48 hours free of symptoms. Symptomatic patients must not be moved from one ward to another. The IPCT will advise on the movement of patients within the ward areas. Before re-opening any bays or single rooms to new admissions an ‘Isolation clean’ (see The Three Cleans, available on Datix) must be carried out, which includes cleaning with Chlor-clean and the changing of curtains.
Clostridium difficile Diarrhoea

27
Patients with / suspected to have Clostridium difficile diarrhoea (an antibiotic associated diarrhoea which is easily spread among patients) must be isolated in a single room, with the door closed, within 4 hours of diagnosis / suspicion. Once asymptomatic for 48 hours (patient must ideally have passed at least one normal stool), they may come out of isolation. The room must have an ‘Isolation clean’ before anyone else can be admitted.
Chicken Pox / Shingles
Chicken pox is infectious from 2 days before the rash starts until 5 days after (once the spots have dried / crusted over). Most UK born adults will be immune however cancer patients and others who are immunosuppressed will be vulnerable. Patients with chicken pox / shingles must not be admitted to an Oncology ward e.g. Derwent. Shingles is a reactivation of the chicken pox that the person had as a youngster. It is not possible to catch shingles from shingles, however it is possible to catch chicken pox from shingles if you have not had chicken pox. Shingles is usually less infectious than chicken pox, however a single room is still recommended.
Meningitis
Bacterial meningitis patients require a side room for the first 48 hours of treatment. Patients with meningitis will suffer from bad headaches and photophobia, so every effort should be made to leave them in a side room until recovered. Viral meningitis can only be treated symptomatically and these patients would ideally have a side room for their own comfort.
MRSA
MRSA in Surgery and Orthopaedics If patients are found to have MRSA whilst on orthopaedic or surgical wards they must be moved to a side room. The bay they were in should not be used for any further admissions. All the patients in that bay must have an MRSA screen taken, and the bay should remain closed until they have all been confirmed negative (contact bay). In circumstances where the bed cannot be allowed to remain unoccupied then only patients who are not going for surgery, with no open wounds and no invasive devices can be admitted. The bed area must have an ‘Isolation clean’. If there is a bay with more than one patient with confirmed MRSA, the bay must remained closed with no further admissions (active bay). The room must have an ‘Isolation clean’ before it is re-opened. MRSA on Medical wards Medical wards are considered a lower risk for MRSA. This risk though lower is not non-existent and it must be remembered that there are still vulnerable patients especially those with cancer and those with invasive devices. MRSA patients who have either throat carriage and a persistent cough; exudating wounds; or exfoliating skin conditions should be isolated in a side room with the door closed. MRSA patients may otherwise be admitted into bays, though staff must take barrier precautions including diligent hand decontamination, and use of gloves and aprons for personal care. Patients with MRSA must not be admitted into bays on Derwent ward
Highly Resistant Organisms e.g. ESBL, VRE, Acinetobacter
These are highly resistant organisms, which we do not wish to spread through the Trust. Often there are no antibiotics to be offered. It is essential that these patients be placed in a side room and the door kept closed. Rooms which have been occupied by patients with these organisms must have an ‘Isolation clean’ before being used for further patients.
Immunocompromised patients
Immunocompromised patients (i.e. neutropenic patients or patients receiving chemotherapy) will also require isolation to prevent them from picking up an infection. Patients in single rooms with infections should ideally be nursed away from patients in single rooms who are being isolated due to low immunity.

28
Appendix 2 – Severe Weather actions See Severe Weather Plan for full details
Severe Weather – Heavy snowfall Impact Transport disruption leading to issues with staff and patient attendance
Activation Procedure:
The On Call Director will activate a Business Continuity Incident and KHT Business Continuity Plan on receiving MET Office Reports of a 60% chance of the onset of severe weather conditions in the geographical area associated with Kingston Hospital. This will include the wider geographical area associated with the residential location of staff, location of key Trust suppliers etc. Silver will establish an Incident Management Team as required, with representation from, but not limited to:
o COO / On Call Manager o Head of Communications o Human Resources Manager o Estates / Facilities Manager o Service Line Managers o Emergency Planning Manager o Heads of Nursing and Midwifery o Radiology Manager o Bookings Manager o ISS Manager o Therapy Manager
It is assumed that, given the regularity of MET Office warnings, there will be no need to invoke the BCP for Severe Weather ‘out of hours’. In the event that the 1st 60% MET Office warning is communicated at night, the Director On Call will invoke the plan and assume the role of Gold at 9.00 am on the following day.
Recovery Dependencies (on
other departments):
Effective recovery is dependent on Estates and facilities Department, HR Department, Communications Department, Bookings Department and all medical and non-medical clinical managers.
Resources required for recovery:
Additional financial resource may be required in support of ensuring staff availability, for example provision of free meals, taxis. This will be managed through consistent and careful communication and criteria of allocation. The total sum incurred will be included in the incident report.
No
. Action Responsibility
Completion Sign and time
1
Staff Availability Review existing rotas – likely availability of staff rostered to work
Nursing - Service Managers
Medical – Clinical Directors.
Contracted staff – ISS Manager.
Analysis of additional capacity likely to be available (extended duties/provision of accommodation etc)
Initiate swapping of shifts for those who are unlikely to be able to work.
Review additional capacity for childcare on site within staff nursery and allocate shifts accordingly.
As above - With HR Manager
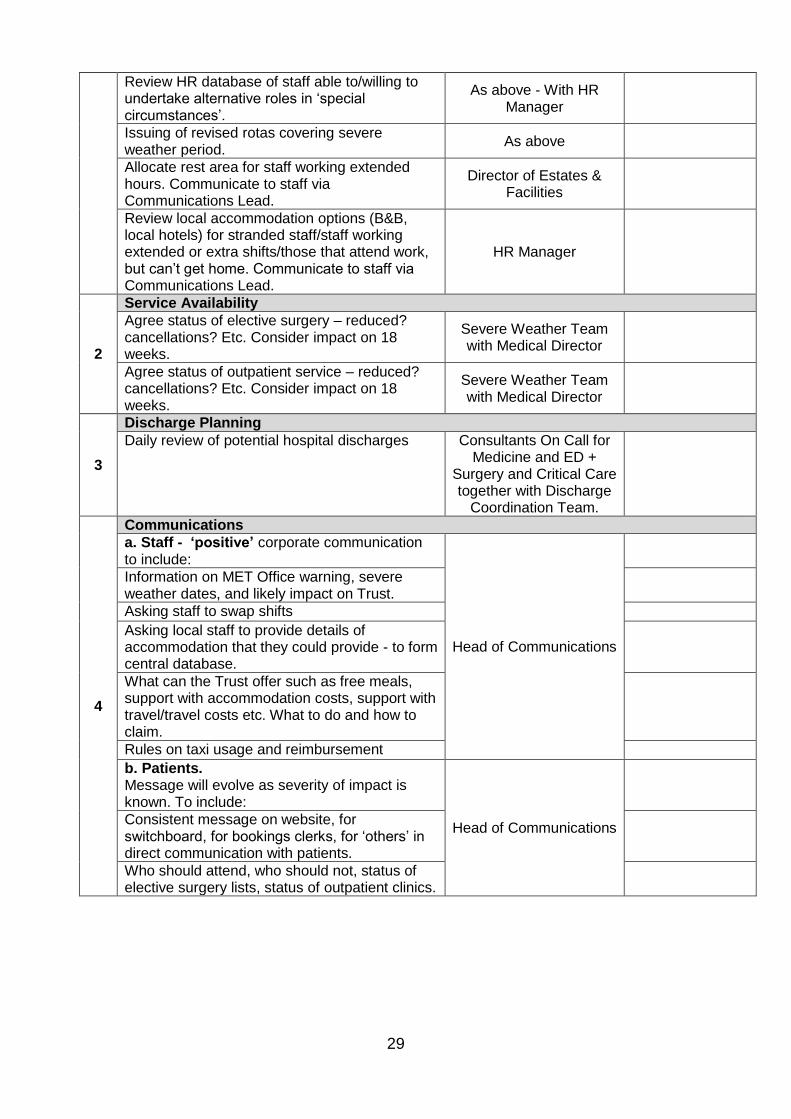
29
Review HR database of staff able to/willing to undertake alternative roles in ‘special circumstances’.
As above - With HR Manager
Issuing of revised rotas covering severe weather period.
As above
Allocate rest area for staff working extended hours. Communicate to staff via Communications Lead.
Director of Estates & Facilities
Review local accommodation options (B&B, local hotels) for stranded staff/staff working extended or extra shifts/those that attend work, but can’t get home. Communicate to staff via Communications Lead.
HR Manager
2
Service Availability Agree status of elective surgery – reduced? cancellations? Etc. Consider impact on 18 weeks.
Severe Weather Team with Medical Director
Agree status of outpatient service – reduced? cancellations? Etc. Consider impact on 18 weeks.
Severe Weather Team with Medical Director
3
Discharge Planning Daily review of potential hospital discharges Consultants On Call for
Medicine and ED + Surgery and Critical Care together with Discharge
Coordination Team.
4
Communications a. Staff - ‘positive’ corporate communication to include:
Head of Communications
Information on MET Office warning, severe weather dates, and likely impact on Trust.
Asking staff to swap shifts Asking local staff to provide details of accommodation that they could provide - to form central database.
What can the Trust offer such as free meals, support with accommodation costs, support with travel/travel costs etc. What to do and how to claim.
Rules on taxi usage and reimbursement b. Patients. Message will evolve as severity of impact is known. To include:
Head of Communications
Consistent message on website, for switchboard, for bookings clerks, for ‘others’ in direct communication with patients.
Who should attend, who should not, status of elective surgery lists, status of outpatient clinics.
30
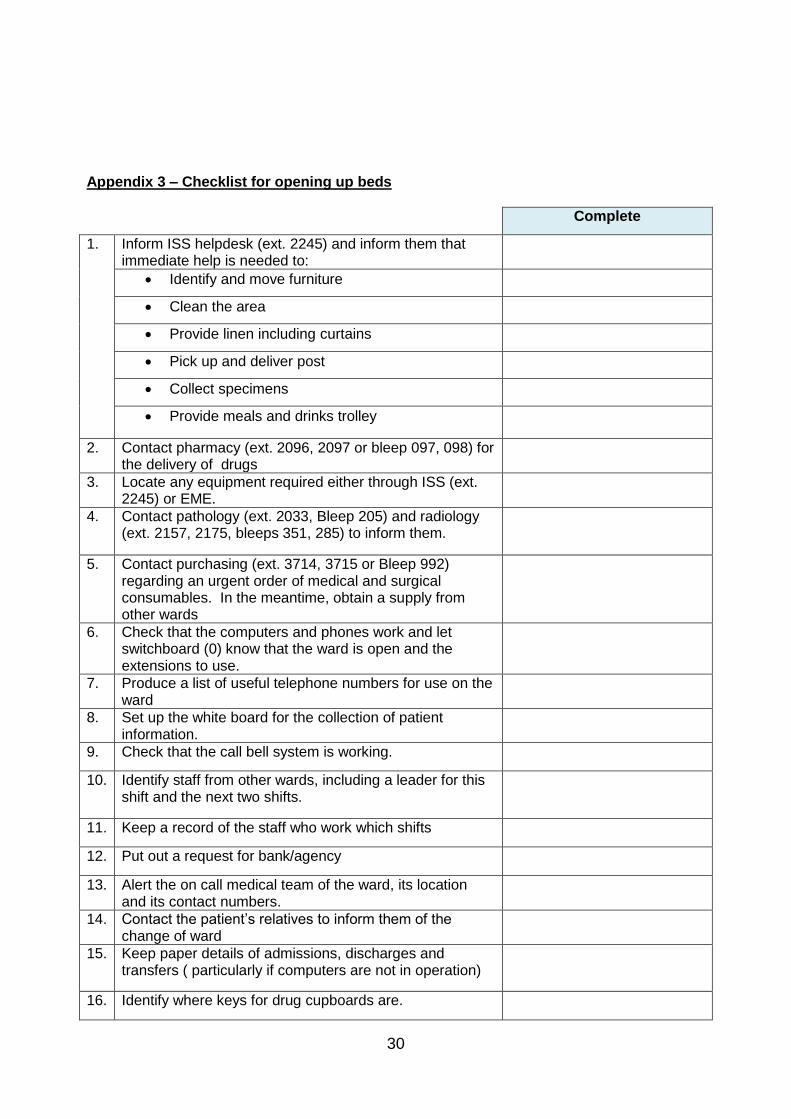
Appendix 3 – Checklist for opening up beds
Complete
1. Inform ISS helpdesk (ext. 2245) and inform them that immediate help is needed to:
Identify and move furniture
Clean the area
Provide linen including curtains
Pick up and deliver post
Collect specimens
Provide meals and drinks trolley
2. Contact pharmacy (ext. 2096, 2097 or bleep 097, 098) for the delivery of drugs
3. Locate any equipment required either through ISS (ext. 2245) or EME.
4. Contact pathology (ext. 2033, Bleep 205) and radiology (ext. 2157, 2175, bleeps 351, 285) to inform them.
5. Contact purchasing (ext. 3714, 3715 or Bleep 992) regarding an urgent order of medical and surgical consumables. In the meantime, obtain a supply from other wards
6. Check that the computers and phones work and let switchboard (0) know that the ward is open and the extensions to use.
7. Produce a list of useful telephone numbers for use on the ward
8. Set up the white board for the collection of patient information.
9. Check that the call bell system is working.
10. Identify staff from other wards, including a leader for this shift and the next two shifts.
11. Keep a record of the staff who work which shifts
12. Put out a request for bank/agency
13. Alert the on call medical team of the ward, its location and its contact numbers.
14. Contact the patient’s relatives to inform them of the change of ward
15. Keep paper details of admissions, discharges and transfers ( particularly if computers are not in operation)
16. Identify where keys for drug cupboards are.
31
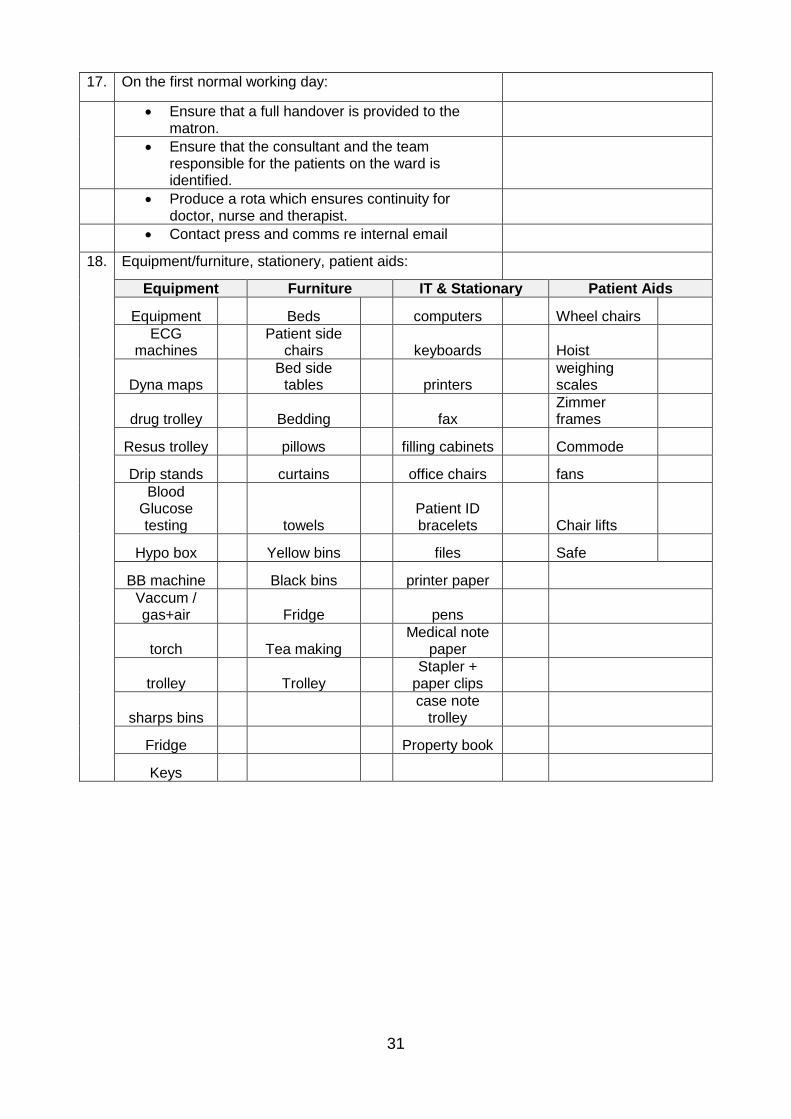
17. On the first normal working day:
Ensure that a full handover is provided to the matron.
Ensure that the consultant and the team responsible for the patients on the ward is identified.
Produce a rota which ensures continuity for doctor, nurse and therapist.
Contact press and comms re internal email
18. Equipment/furniture, stationery, patient aids:
Equipment Furniture IT & Stationary Patient Aids
Equipment
Beds
computers
Wheel chairs
ECG machines
Patient side chairs
keyboards
Hoist
Dyna maps Bed side
tables
printers weighing
scales
drug trolley
Bedding
fax Zimmer
frames
Resus trolley
pillows
filling cabinets
Commode
Drip stands
curtains
office chairs
fans
Blood Glucose testing
towels
Patient ID bracelets
Chair lifts
Hypo box
Yellow bins
files
Safe
BB machine
Black bins
printer paper
Vaccum / gas+air
Fridge
pens
torch
Tea making Medical note
paper
trolley
Trolley Stapler +
paper clips
sharps bins
case note
trolley
Fridge
Property book
Keys
32
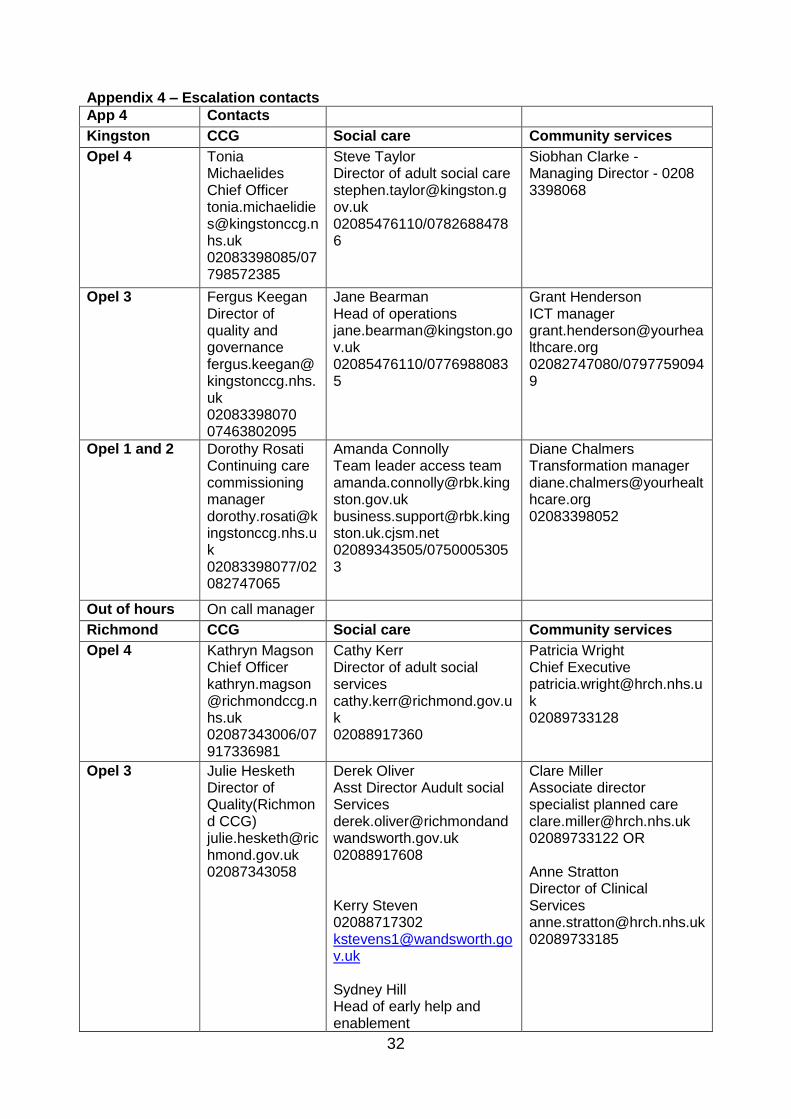
Appendix 4 – Escalation contacts
App 4 Contacts
Kingston CCG Social care Community services
Opel 4 Tonia Michaelides Chief Officer [email protected] 02083398085/07798572385
Steve Taylor Director of adult social care [email protected] 02085476110/07826884786
Siobhan Clarke - Managing Director - 0208 3398068
Opel 3 Fergus Keegan Director of quality and governance [email protected] 02083398070 07463802095
Jane Bearman Head of operations [email protected] 02085476110/07769880835
Grant Henderson ICT manager [email protected] 02082747080/07977590949
Opel 1 and 2 Dorothy Rosati Continuing care commissioning manager [email protected] 02083398077/02082747065
Amanda Connolly Team leader access team [email protected] [email protected] 02089343505/07500053053
Diane Chalmers Transformation manager [email protected] 02083398052
Out of hours On call manager
Richmond CCG Social care Community services
Opel 4 Kathryn Magson Chief Officer [email protected] 02087343006/07917336981
Cathy Kerr Director of adult social services [email protected] 02088917360
Patricia Wright Chief Executive [email protected] 02089733128
Opel 3 Julie Hesketh Director of Quality(Richmond CCG) [email protected] 02087343058
Derek Oliver Asst Director Audult social Services [email protected] 02088917608 Kerry Steven 02088717302 [email protected] Sydney Hill Head of early help and enablement
Clare Miller Associate director specialist planned care [email protected] 02089733122 OR Anne Stratton Director of Clinical Services [email protected] 02089733185

33
[email protected] 020088715271
Opel 1 and 2 Ana Costinas Commissioning manager [email protected] 02088316136/07985482463
Emiliya Ivanova Social work team manager [email protected] Telephone:
Jeanne Davey Team manager [email protected] [email protected] 07940466898/02087144060 or Tom Penman Urgent Care manager [email protected] 02089733123/07415649916
Out of hours
Surrey CCG Social care Community services
Opel 4 Steve Hams Director of Clinical performance [email protected] 01372 201538 Mob 07507531558
Sonya Sellar Area director [email protected] 07968834010
Jo Pritchard Chief Executive [email protected] 01372384943 Mob 07979594414
Opel 3 James Blyth Director of commissioning [email protected] 01372201538 Mob 07765147196
Teresa Hawkings Senior Manager [email protected] 07791423513
Helen Cook Head of Adult Services [email protected] 07506729030

34
Opel 1 and 2 Lorna Hart Deputy Director of Commissioning [email protected] or [email protected] 01372201751 07747476530
Tracey Pope-warren Team Manager [email protected] 07805757179 Suzannah Townsend Assistant team manager [email protected] 07805845404
Fiona Mooney Head of Epsom community hub [email protected] 01372734871/07506732311
On call manager
Wandsworth CCG Social care Community services
Opel 4 Kathy Kerr Director of adult social services [email protected] 02088917360
Opel 3 Rebecca Welburn Director of Commissioning [email protected] 02088126675
Sydney Hill Head of early help and enablement [email protected] 020088715271
Opel 1 and 2 Jane French Commissioning redesign manager [email protected] 02088126731/07825845403
Angela Kelly Acting team leader [email protected] 02084876811/02088718583
Out of hours
Merton CCG Social care Community services
Opel 4 Kim Carey Interim Executive, head of access and assessment [email protected] 02085454535
Opel 3 Sarah wells Service manager [email protected] 02082745301
35
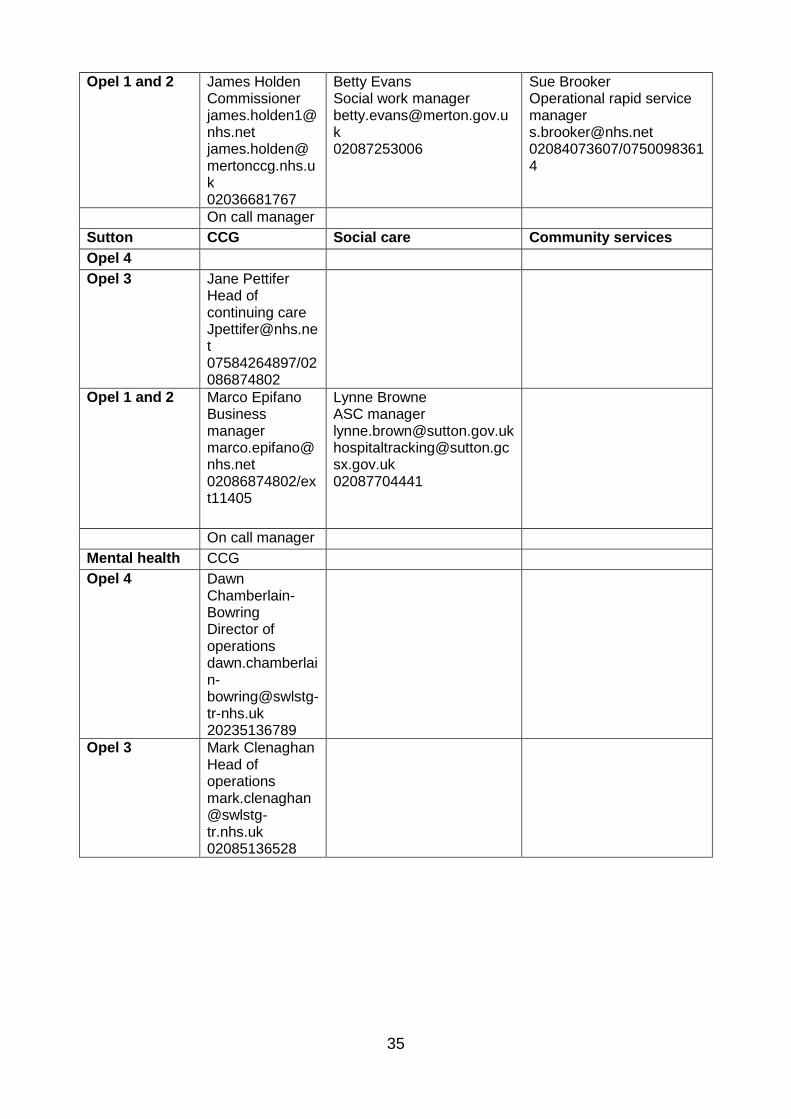
Opel 1 and 2 James Holden Commissioner [email protected] [email protected] 02036681767
Betty Evans Social work manager [email protected] 02087253006
Sue Brooker Operational rapid service manager [email protected] 02084073607/07500983614
On call manager
Sutton CCG Social care Community services
Opel 4
Opel 3 Jane Pettifer Head of continuing care [email protected] 07584264897/02086874802
Opel 1 and 2 Marco Epifano Business manager [email protected] 02086874802/ext11405
Lynne Browne ASC manager [email protected] [email protected] 02087704441
On call manager
Mental health CCG
Opel 4 Dawn Chamberlain-Bowring Director of operations [email protected] 20235136789
Opel 3 Mark Clenaghan Head of operations [email protected] 02085136528
36
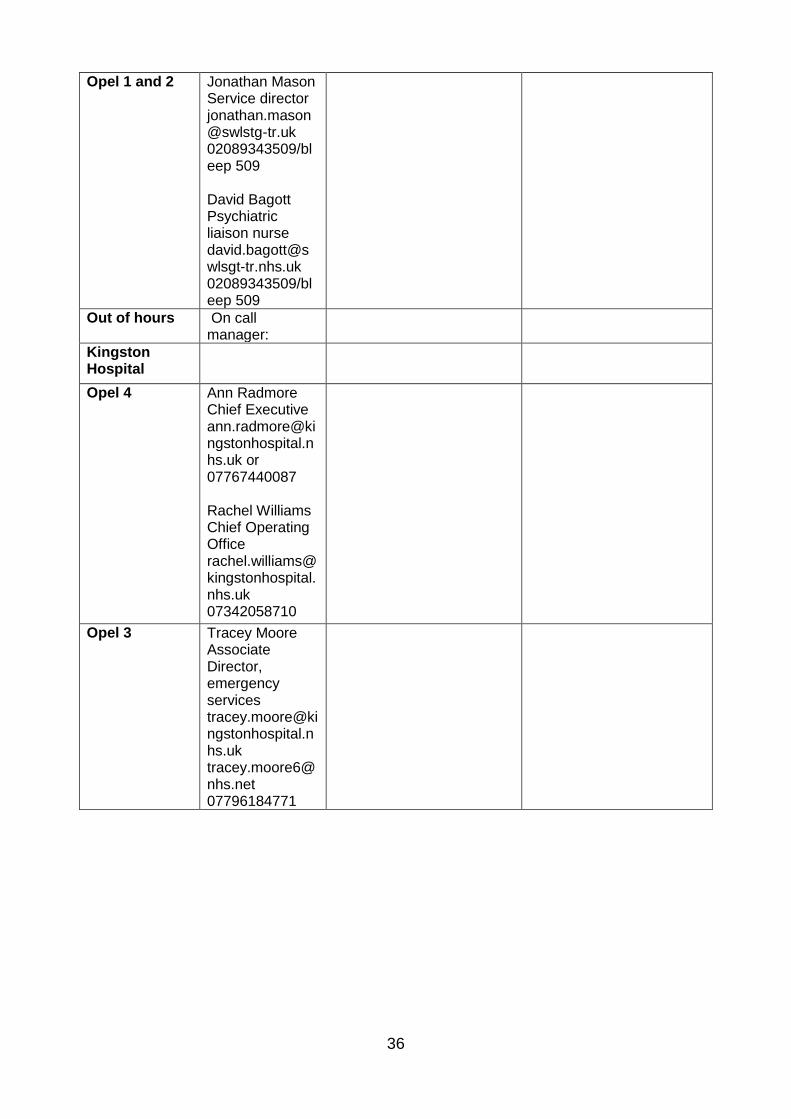
Opel 1 and 2 Jonathan Mason Service director [email protected] 02089343509/bleep 509 David Bagott Psychiatric liaison nurse [email protected] 02089343509/bleep 509
Out of hours On call manager:
Kingston Hospital
Opel 4 Ann Radmore Chief Executive [email protected] or 07767440087 Rachel Williams Chief Operating Office [email protected] 07342058710
Opel 3 Tracey Moore Associate Director, emergency services [email protected] [email protected] 07796184771
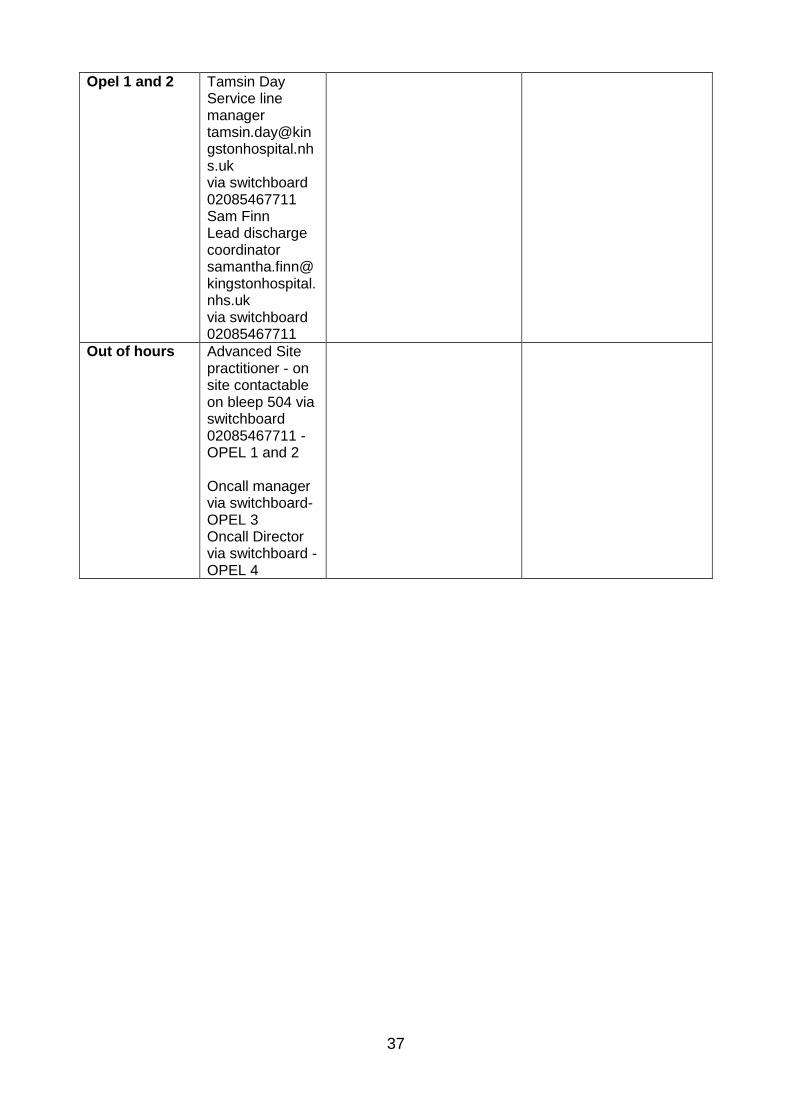
37
Opel 1 and 2 Tamsin Day Service line manager [email protected] via switchboard 02085467711 Sam Finn Lead discharge coordinator [email protected] via switchboard 02085467711
Out of hours Advanced Site practitioner - on site contactable on bleep 504 via switchboard 02085467711 - OPEL 1 and 2 Oncall manager via switchboard- OPEL 3 Oncall Director via switchboard - OPEL 4
38
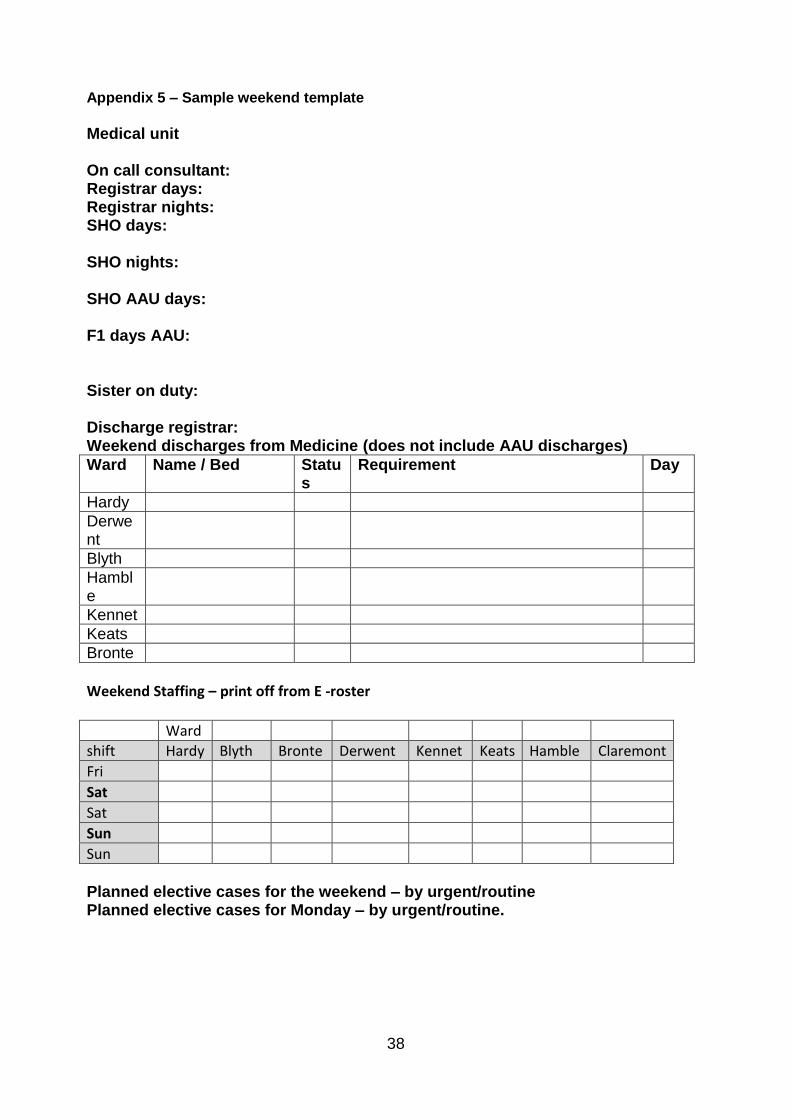
Appendix 5 – Sample weekend template
Medical unit On call consultant: Registrar days: Registrar nights: SHO days:
SHO nights: SHO AAU days: F1 days AAU:
Sister on duty: Discharge registrar: Weekend discharges from Medicine (does not include AAU discharges)
Ward Name / Bed Status
Requirement Day
Hardy
Derwent
Blyth
Hamble
Kennet
Keats
Bronte
Weekend Staffing – print off from E -roster
Ward shift Hardy Blyth Bronte Derwent Kennet Keats Hamble Claremont Fri Sat
Sat
Sun
Sun
Planned elective cases for the weekend – by urgent/routine Planned elective cases for Monday – by urgent/routine.

39
Appendix 6 – Emergency Department Capacity Management, Redirect and Closure Protocol(ED Policy) v 8


















