SUPPORT PACKAGE FOR REHABILITATION€¦ · Person centered/integrated care ... Maturity Model Based...
43
SUPPORT PACKAGE FOR REHABILITATION
Transcript of SUPPORT PACKAGE FOR REHABILITATION€¦ · Person centered/integrated care ... Maturity Model Based...

SUPPORT PACKAGE FOR REHABILITATION

Governance

SUPPORT PACKAGE FOR REHABILITATION
SUPPORT PACKAGE FOR REHABILITATION – MANUAL
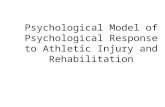
FOUR-STEP PROCESS
ACCOMPANYING TOOLS
1. Determine situation Standard Assessment of Rehabilitation
Systems (STARS)
2. Develop rehabilitation strategic plan Guidance for Rehabilitation Strategic
Planning (GRASP)
3. Establish rehabilitation monitoring
framework and evaluation and review
processes
Framework for Rehabilitation Monitoring
and Evaluation (FRAME)
4. Implement
Action on Rehabilitation (ACTOR)

FRAME STARS
GRASP
ACTOR

Rehabilitation Strengthening Process
Year 1 2* 3 4* 5 Year 6
* Countries may operate on a 1 or 2 year planning cycle and the review process could occur annually or every two years.

SUPPORT PACKAGE FOR REHABILITATION
SUPPORT PACKAGE FOR REHABILITATION – MANUAL
FOUR-STEP PROCESS
ACCOMPANYING TOOLS
1. Determine situation Standard Assessment of Rehabilitation
Systems (STARS)
2. Develop rehabilitation strategic plan Guidance for Rehabilitation Strategic
Planning (GRASP)
3. Establish rehabilitation monitoring
framework and evaluation and review
processes
Framework for Rehabilitation Monitoring
and Evaluation (FRAME)
4. Implement
Action on Rehabilitation (ACTOR)

The Manual
• Introduction to Package
• practical resource
• flexible and adaptable to country situation
• Overview to the four steps and tools
• Health System Strengthening
• Planning - National Health Strategic Plans & Rehabilitation Strategic Plan
• Conceptual Framework for Rehabilitation
• Principles to guide process

Four-step process Phases of each step Step 1. Determine the situation Phase A: Prepare for situation assessment
Phase B: Complete rehabilitation capacity questionnaire
Phase C: Assess in the country
Phase D: Write and finalize report, disseminate and communicate
findings
Step 2. Develop a strategic plan Phase E. Prepare for strategic planning
Phase F. Identify priorities, undertake planning and drafting
Phase G. Consult and finalize plan and complete costing of plan
Phase H. Endorse and disseminate the strategic plan
Step 3. Establish monitoring, evaluation and
review processes
Phase I. Develop monitoring framework with indicators, baselines and
targets
Phase J. Establish evaluation and review process
Step 4. Implement Phase K. Establish an annual action cycle
Phase L. Increase capacity of rehabilitation leadership and governance

The Six Building Blocks of the Health System
Rehabilitation components within the health system
1. Leadership and governance
Laws, policies, plans and strategies that address rehabilitation
Governance structures, regulation mechanism and accountability processes that address rehabilitation
Planning, collaboration and coordination processes for rehabilitation
2. Financing Health expenditure earmarked for rehabilitation
Health financing and payment structures inclusive of rehabilitation
3. Health workforce Health workforce that delivers rehabilitation interventions - primarily
rehabilitation medicine and therapists and nursing
4. Service delivery All the health services that deliver rehabilitation interventions
5. Medicines and technology
Medicines and technology utilized commonly by people accessing rehabilitation services, primarily assistive products
6. Health information systems
Health information systems that includes data relevant to rehabilitation, for example, population functioning and rehabilitation needs data, rehabilitation service availability and utilization data.

Principles for Strengthening Rehabilitation
Strengthening governance and leadership for rehabilitation within ministries of health
Integrating into health policies and plans
Advancing integrated, people-centered care
Improving equity and human rights
Ensure evidence-informed policies and planning

STARS – Standard Assessment of Rehabilitation Systems
1. Preparation, preparation, preparation
• Ensure the government is informed, committed and leading the assessment
• Establish the scope of the assessment
• Identify key stakeholders, clarify their roles and responsibilities
• Confirm timelines and availability of resources
• Identify participants for the Rehabilitation Technical Working Group
2. Rehabilitation Capacity Questionnaire
3. In-country assessment period
• Together - government, rehabilitation technical working group and assessor
• Interviews, consultation meetings, focus group discussion, site visits
• Maturity model assessment
4. Write, finalize, communicate the Situation Assessment Report

Rehabilitation System - Conceptual Framework
Input to Rehabilitation System
Rehabilitation System Capacity & Processes
1. Governance
2. Information
3. Financing
4. Human Resources
Output of Rehabilitation System
Rehabilitation System Services & Processes
A. Rehabilitation Services Available
B. Rehabilitation Service Quality
Outcome of Rehabilitation System
Rehabilitation System Performance Attributes
• Accessibility
• Equity
• Efficiency
• Sustainability
Impact of Rehabilitation
Services
Better Population Health
and Functioning
with Protection from
Financial hardship

Rehabilitation System – Measurement Items
Health System Building Block (Inputs) Dimensions Assessed
Governance
Legislation, Policy, Regulation Planning Accountability Coordination
Information & Research
Rehabilitation Data Rehabilitation Research
Financing
Rehabilitation Expenditure Financing Mechanisms Service Payment Systems
Workforce
Number & Specialties Professional Mobility Training

Rehabilitation System – Measurement Items
Services (Outputs) Dimensions Assessed
Service Availability
Services & facilities across health care levels Services across stages of care Services for target populations; complex, child, older Assistive Products
Service Quality
Effectiveness Timeliness Person centered/integrated care Safety

Rehabilitation System – Measurement Items
Rehabilitation Services Performance Attributes (Outcomes)
Dimensions Assessed
Accessibility
Availability & Affordability & Acceptability
Equity
Equity measured through access to rehabilitation for population groups
Efficiency
Allocative Efficiency, Technical Efficiency
Sustainability
Institutional Sustainability Financial Sustainability Disaster/Crisis Resilience

STARS – Standard Assessment of Rehabilitation Systems
Maturity Model
Based on the Rehabilitation Conceptual Model
1. Governance
2. Financing
3. Information
4. Human resources
5. Services – Availability / Quality
6. Outcome Attributes – Accessibility / Equity / Efficiency / Sustainability

STARS – Standard Assessment of Rehabilitation Systems
Maturity Model
Based on the Rehabilitation Conceptual Model
1. Governance
a. Rehabilitation policies and plans are formulated
b. The levers for rehabilitation policy and plan implementation function well
c. There is accountability and transparency across rehabilitation governance
d. There is regulation of the sector
e. There is collaboration and coalition building
f. Evidence and intelligence is utilized to inform decision making






Guidance for Strategic Planning – GRASP
Phases
1. Preparation, preparation, preparation
• Mobilise support from
• Scope, process, budget, timeframes, drafting group,
costing, endorsement process
2. Identify priorities, undertake the planning and
drafting
• Prioritising exercise
• Drafting process – drafting group
3. Consult, finalise and complete
• Consultation process
4. Endorse and disseminate
• Endorsement process within the government
Other Components to GRASP Considerations for rehabilitation strategic planning – Q&A • Policy, plans, legislation • Scope • Assistive products • MOH / MOSA • National / sub-national
Sample rehabilitation strategic plan



Framework for Rehabilitation Monitoring and Evaluation – FRAME
Phases
1. Establishing Monitoring framework
• Aligned to Strategic plan
2. Establishing Evaluation and Review
processes
• Complementary to framework
• Guidance for reporting on implementation of
strategic plan activities
• Guidance for evaluation and review processes
Other Components to FRAME Menu of Rehabilitation System Indicators Core and expanded

CONTENTS OF FRAME TOOL
1. Guidance for development of a monitoring framework that measures change in rehabilitation within health systems
2. Guidance for development of a monitoring process on the implementation of activities of the strategic plan
3. Guidance for development of overarching evaluation and review processes
4. A menu of indicators – core and expanded set, with definition, measurement, data sources etc

Developing a National Rehabilitation Monitoring Framework
1. Based on strategic plan, identify priority areas for results
2. Identify relevant, reliable and feasible indicators for the country – select indicators from the FRAME rehabilitation menu.
3. Confirm feasibility of data collection and management for indicators
4. Adjust templates/mechanisms for data collection, collation and management.
5. Train relevant people on new data collection and collation.
6. Plan reporting regularity for indicators and commence
7. Undertake annual or two yearly review of results from the monitoring framework.

Common Priority Areas in a Rehabilitation Strategic Plan
• Strengthening leadership, governance, planning and coordination for rehabilitation
• Building stronger integration of rehabilitation across health system planning
• Strengthening the information, evidence and research in rehabilitation
• Expanding the financing to rehabilitation and reducing out of pocket costs
• Increasing the availability and quality of the rehabilitation workforce
• Expanding the availability of rehabilitation services across all levels of healthcare
• Increasing access to rehabilitation services at the community level
• Improving the quality of rehabilitation services
• Developing early identification and intervention services for children with developmental delays and disabilities
• Developing specialized rehabilitation services for prioritized groups, such as people with complex rehabilitation needs, older people, people with non-communicable disease, people with mental health conditions and people with vision and hearing impairments.
• Increasing provision of assistive products
But what does success look like?
And how do we measure it?

CRITERIA DEFINITION
Valid Sufficient (scientific) evidence exists to support a link between the value of an indicator and one or more aspects of rehabilitation within health systems
Reliable Repeated measurements of a stable phenomenon get similar results and are sensitive to change
Relevant An indicator measures an aspect of rehabilitation within health systems with high importance
Actionable
An indicator measures an aspect of rehabilitation within health systems that is subject to control by providers and/or the health care system and is actually used at a national level for policy making or strategy development
Internationally feasible An indicator can be derived for international comparisons without substantial additional resources
Internationally comparable
Reporting countries comply with the relevant data definition and where differences in the indicator values between countries reflect issues in health systems rather than differences in data collection methodologies, coding or other measurement or health system reasons
OECD Criteria for Healthcare Quality Indicators Criteria used to score HCQI
Adapted from OECD report of quality of healthcare indicators

• Indicator name:
• Domain: Based on the global 100 categorization
• Domain of conceptual framework: Based on Conceptual framework for the Rehab.
• Rationale:
• Definition:
• Numerator:
• Denominator:
• Disaggregation and additional dimension:
• Method of measurement:
• Method of estimation/variation: /
• Measurement frequency:
• Monitoring and evaluation framework: Log frame
• Preferred data sources:
• Other possible data sources and related links:
• Limitations:

2). Indicator name: Public Rehabilitation Expenditure
Domain of Global Reference List: Health Systems
Dimension of Rehabilitation System Conceptual Framework: Rehabilitation Financing
Rationale: Public expenditure on rehabilitation per capita demonstrates the level of government expenditure for rehabilitation. This includes from all
government agencies, ministries of health and social affairs/veterans etc. This removes the contribution being made by international non-government
organizations/development partners and private expenditure.
Definition: Public health expenditure are the funds for rehabilitation that are from Public sources, as defined through SHA, and calculated on per capita
basis.
Numerator: Public rehabilitation expenditure
Denominator: Total population as measured through national records. Alternative to this is population as based on World Bank figures.
Disaggregation and additional dimension: Public expenditure for specialist rehabilitation services
Method of measurement: Data from Ministry of Health, National health accounts
Method of estimation/variation: /
Measurement frequency: Two yearly
Monitoring and evaluation framework: Input
Preferred data sources: National from Ministry of Health
Other possible data sources and related links: World bank or other international sights.
Limitations: Attaining public health expenditure for rehabilitation is a challenge and it most likely does not include the rehabilitation services that are
integrated into hospitals.

5). Indicator name: Rehabilitation in health information system
Domain of Global Reference List: Health Systems
Dimension of Rehabilitation System Conceptual Framework: Rehabilitation Information Systems
Rationale: The inclusion of rehabilitation data in the district health management information system (DHMIS), or the reporting system/dashboards of the
health management information system indicates rehabilitation data is being collected and managed.
Definition: One or more rehabilitation information points being collated in the district health management information system (DHMIS), or the reporting
system/dashboards of the health management information system. This indicator is not reflecting rehabilitation data collected in individual client records
only, it must be data collated and managed and synthesized to enable reporting.
Numerator: Number of rehabilitation information points
Denominator: /
Disaggregation and additional dimension: /
Method of measurement: Data from Ministry of Health DHMIS
Method of estimation/variation: /
Measurement frequency: Annually
Monitoring and evaluation framework: Input
Preferred data sources: National from Ministry of Health DHMIS, DHIS2 system in countries
Other possible data sources and related links: DHIS2

11). Indicator name: Rehabilitation personnel per 10,000
Domain of Global Reference List: Health Systems
Dimension of Rehabilitation System Conceptual Framework: Rehabilitation Workforce
Rationale: The number of workforce per 10,000 is an indication of the density of workforce which also indicates rehabilitation service availability. If it is
compared to medicine and nursing and interpreted based on evidence of proportions of high performing health systems then this also contributes to
understanding of prioritization rehabilitation services compared with other health services.
Definition: Rehabilitation personnel include rehabilitation doctors, rehabilitation nurses and therapists, including physiotherapy, occupational therapy,
speech language therapy, prosthetists, orthotists and psychologists. It does not include social workers as a significant proportion of their interventions are
not rehabilitation interventions. This includes those working in government, private practice and NGO services.
Numerator: Total number of rehabilitation workforce
Denominator: Per 10,000 of the population
Disaggregation and additional dimension: Employed in government services only. Separate disciplines. Add another indicator: number of rehabilitation
disciplines.
Method of measurement: Health workforce data and demographic data.
Method of estimation/variation: /
Measurement frequency: Annually
Monitoring and evaluation framework: Input
Preferred data sources: National from Ministry of Health
Other possible data sources and related links: Global professional associations – WCPT, WFOT, ISPRM
Limitations: For countries without credentialing reliable data it is often not available and government data more reliable.

14). Indicator name: Tertiary healthcare with rehabilitation integrated
Domain of Global Reference List: Service Coverage
Dimension of Rehabilitation System Conceptual Framework: Rehabilitation Services - Availability
Rationale: The percentage of tertiary hospitals with 3+ disciplines of therapy available is a basic reflection of the availability of
rehabilitation in those settings, a tertiary hospital offers more specialized services so multiple disciplines are needed.
Definition: 3+ therapy disciplines in tertiary level hospitals (tertiary defined through countries own approach)
Numerator: Number of tertiary hospitals with 3+ therapy disciplines
Denominator: Total number of tertiary hospitals
Disaggregation and additional dimension: All hospitals / government hospitals only.
Method of measurement: Data from Ministry of Health
Method of estimation/variation: To include rehabilitation medicine and nursing as one of the disciplines.
Measurement frequency: Two yearly
Monitoring and evaluation framework: Output
Preferred data sources: National from Ministry of Health
Other possible data sources and related links: Tertiary-level hospitals
Limitations: Where countries have rehabilitation disciplines that cover two therapy disciplines such as PT and OT
References: /

19). Indicator name: Assistive product list (APL) financed through public sources
Domain of Global Reference List: Service Coverage
Dimension of Rehabilitation System Conceptual Framework: Rehabilitation Services / Availability
Rationale: The percentage of APL that is funded through public sources is an indication of overall availability to the
population
Definition: The % of the WHO APL that is financed through public sources, this includes all government agencies who
finance AP.
Numerator: Number financed through public sources
Denominator: Total number of the 50 APL
Disaggregation and additional dimension: /
Method of measurement: Ministry of health
Method of estimation/variation: /
Measurement frequency: Two yearly
Monitoring and evaluation framework: Output and processes
Preferred data sources: National from Ministry of Health
Other possible data sources and related links:
Limitations: This is unlikely to be sensitive to change for many high-income countries

26). Indicator name: Functioning outcome assessment on admission and discharge from specialist rehabilitation facility
Domain of Global Reference List: Health Systems
Dimension of Rehabilitation System Conceptual Framework: Rehabilitation Services – Quality
Rationale: This indicator serves as a measure to gain a picture of the amount of people who are assessed in terms of their function on
admission and discharge. It indicates the quality of a service. Using a standardized outcome measure on admission and discharge also
indicates the impact of the treatment.
Definition: On admission to a specialist facility a standardized outcome measure is used to assess function and the same outcome
measure is used on discharge to measure the change.
Numerator: Number of people who have a functioning outcome assessment on admission and discharge
Denominator: Total number of people admitted to specialist rehabilitation facilitation
Disaggregation and additional dimension: sex, age, non-communicable disease, communicable disease, trauma, paediatrics.
Method of measurement: Data from Ministry of Health
Method of estimation/variation: Survey estimation possible if 90% of results are available with an equal geographical coverage
Measurement frequency: Annually
Monitoring and evaluation framework: Output
Preferred data sources: National from Ministry of Health
Other possible data sources and related links: Data directly from specialist rehabilitation facilities
Limitations: There will need to be consensus as to which outcome assessments are used in order to be able to compare and bench-
mark



Action on Rehabilitation – ACTOR
Phase
1. Establish Annual Action Cycle
• Plan, do, review
Other Component to ACTOR
Increase capacity of rehabilitation leadership and
governance
• Resourcing government structures
• Leadership and rehabilitation training
• Engaging peoples of influence
• Mentoring champions
• Undertaking study tours
• Country to country support

Support Package on Rehabilitation How it can work
• Government request support for process, likely over 12+ months • Government lead with assistance from WHO and possibly Development Partner. • Likely external consultant undertake rehabilitation situation assessment, support
strategic planning and development of performance monitoring framework.
Estimated Budget for Process • Initial cost for consultant to provide technical support and undertake rehabilitation
situation assessment and development of strategic plan and monitoring framework. Approx. 2@ 4 week contracts, including 2 in-country missions, $20,000 each – total $40,000
• Additional cost of government meetings and events – $1000-2000. • The cost to implement rehabilitation strategic plan is not included – primarily gvt. • Anticipated cost-sharing Government, WHO and Development Partners

2018 • WPRO:
• Laos • Solomon Islands
• AFRO: • Senegal • Zambia
• EMRO: • Afghanistan • Jordon
• SEARO • Myanmar • Bangladesh
• PAHO: • Guyana • Bolivia • 3 States of Brazil
• EURO • Montenegro • Turkmenistan

Pauline Kleinitz Rehabilitation Programme World Health Organization Email: [email protected] Website: http://www.who.int/rehabilitation
43
Thank you!