Support Devices for Acute CHF Destination LVADs to exclude .../media/Non-Clinical/Files-PDFs... ·...
50
Support Devices for Acute CHF Destination LVADs to exclude Transplant Expectations, Indications, Benefits ,Risks Donna Mancini, MD Mt Sinai School of Medicine
Transcript of Support Devices for Acute CHF Destination LVADs to exclude .../media/Non-Clinical/Files-PDFs... ·...

Support Devices for Acute CHFDestination LVADs to exclude Transplant
Expectations, Indications, Benefits ,Risks
Donna Mancini, MDMt Sinai School of Medicine
Conflict of Interest
• None

Refractory cardiogenic Shock
• 1. Use of temporary percutaneous devices in AHF/cardiogenic shock
• 2. Durable devices for Destination therapy
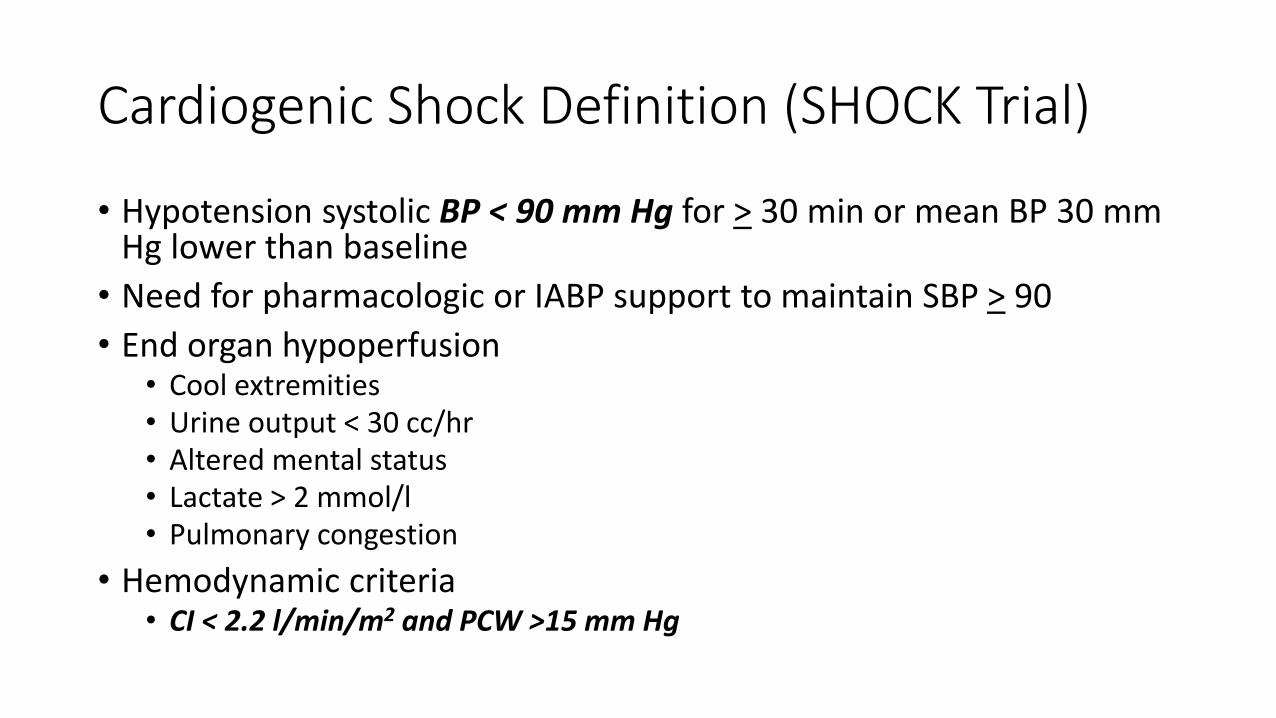
Cardiogenic Shock Definition (SHOCK Trial)
• Hypotension systolic BP < 90 mm Hg for > 30 min or mean BP 30 mm Hg lower than baseline
• Need for pharmacologic or IABP support to maintain SBP > 90
• End organ hypoperfusion• Cool extremities• Urine output < 30 cc/hr• Altered mental status• Lactate > 2 mmol/l• Pulmonary congestion
• Hemodynamic criteria• CI < 2.2 l/min/m2 and PCW >15 mm Hg

Etiology of Cardiogenic Shock
• Acute Myocardial Infarction• Large infarct• Moderate or small infarct w pre existing LV dysfn• Mechanical complication of MI- acute MR, VSD, LV rupture• RV infarct
• End Stage Cardiomyopathy
• Myocarditis
• Valvular Heart Disease
• Stress induced cadiomyopathy
• Cardiac Tamponade

Cardiogenic Shock
• AMI occurs in 1 million patients in US and 8 million patients annually worldwide
• Cardiogenic Shock occurs in 4-12% of AMI patients
• 1 yr Mortality rate is about 65%
• IABP-SHOCK II trial failed to show 30 day survival benefit in AMI patients w cardiogenic shock supported by IABP
• Shift now is to examine use of other percutaneous devices in these patients
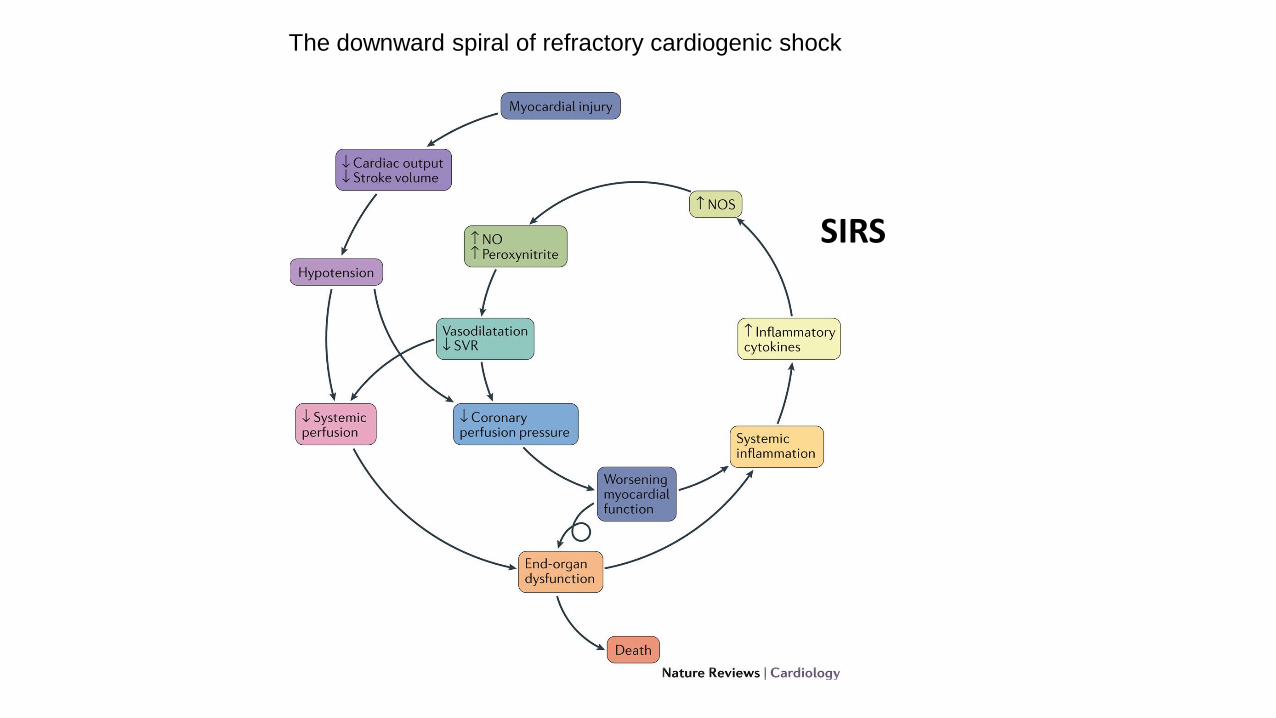
The downward spiral of refractory cardiogenic shock
SIRS

Shock Trial
Hochman JAMA 2001;285:190
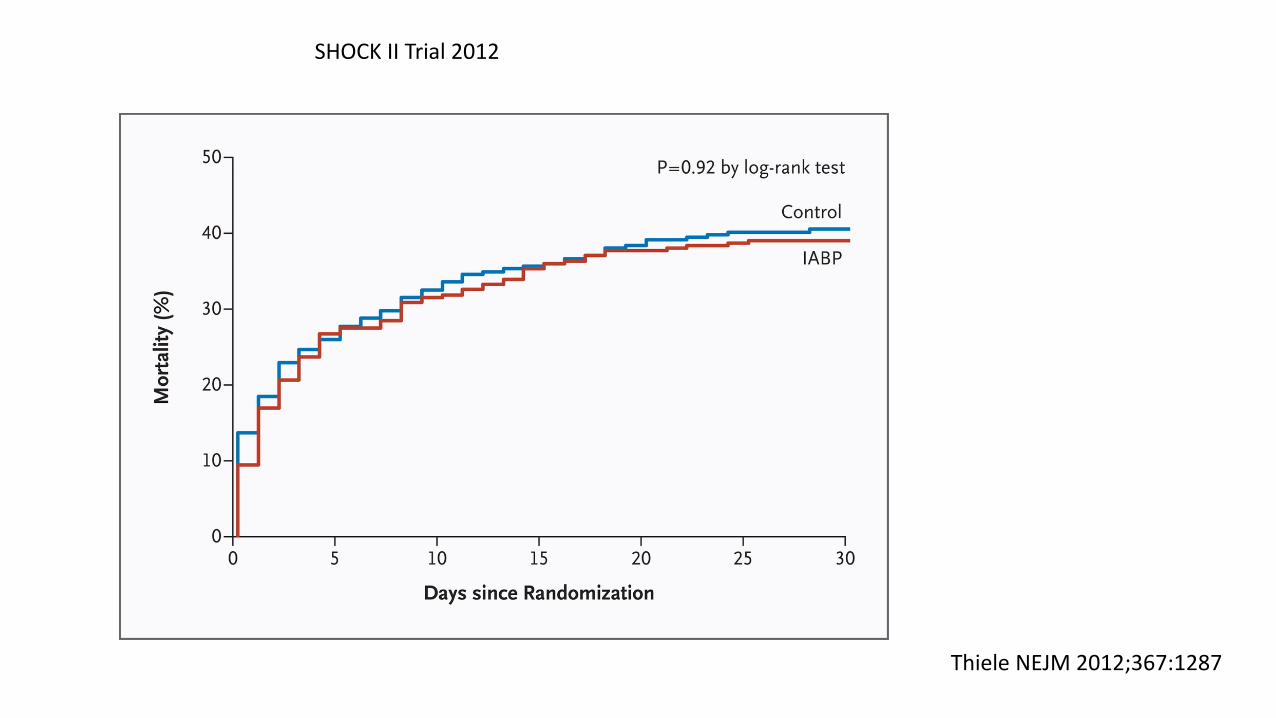
SHOCK II Trial 2012
Thiele NEJM 2012;367:1287

Non Selective NOS inhibitor

Cardiogenic Shock

IABP
ECMO

LV to Aorta LA-Aorta V-A
Short Term Mechanical Circulatory Support Devices

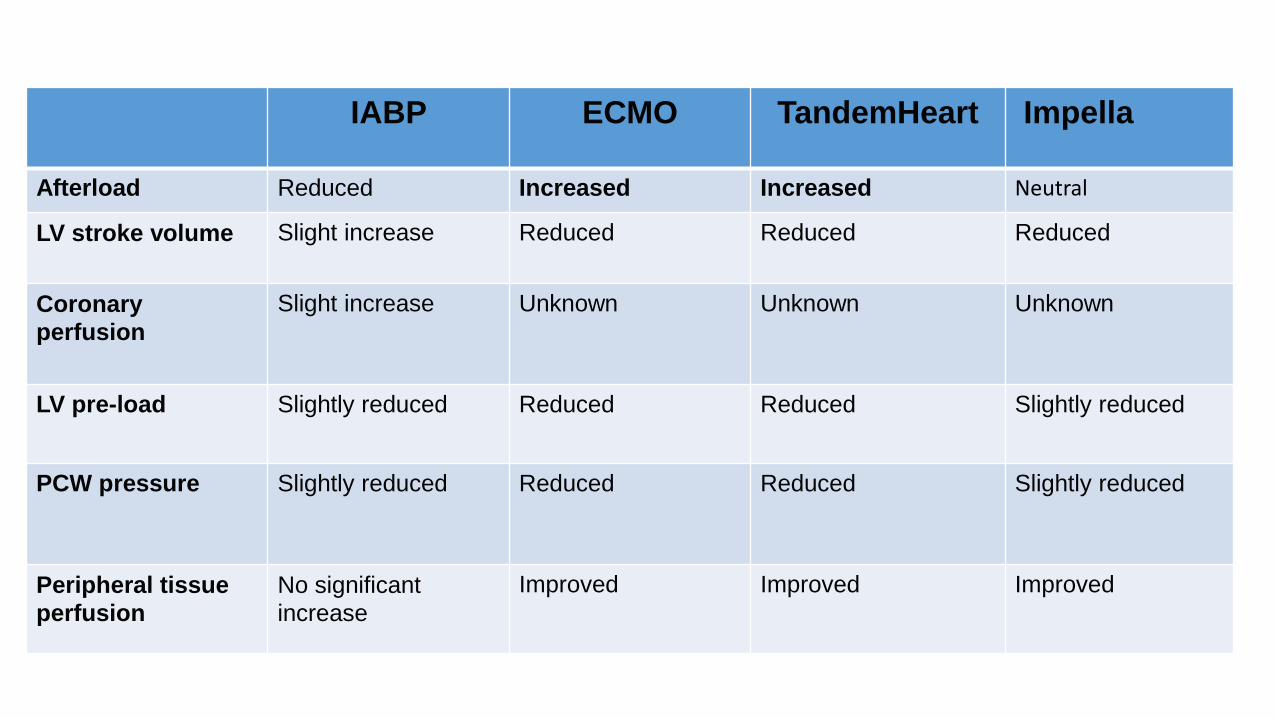
IABP ECMO TandemHeart Impella
Afterload Reduced Increased Increased Neutral
LV stroke volume Slight increase Reduced Reduced Reduced
Coronary
perfusion
Slight increase Unknown Unknown Unknown
LV pre-load Slightly reduced Reduced Reduced Slightly reduced
PCW pressure Slightly reduced Reduced Reduced Slightly reduced
Peripheral tissue
perfusion
No significant
increase
Improved Improved Improved
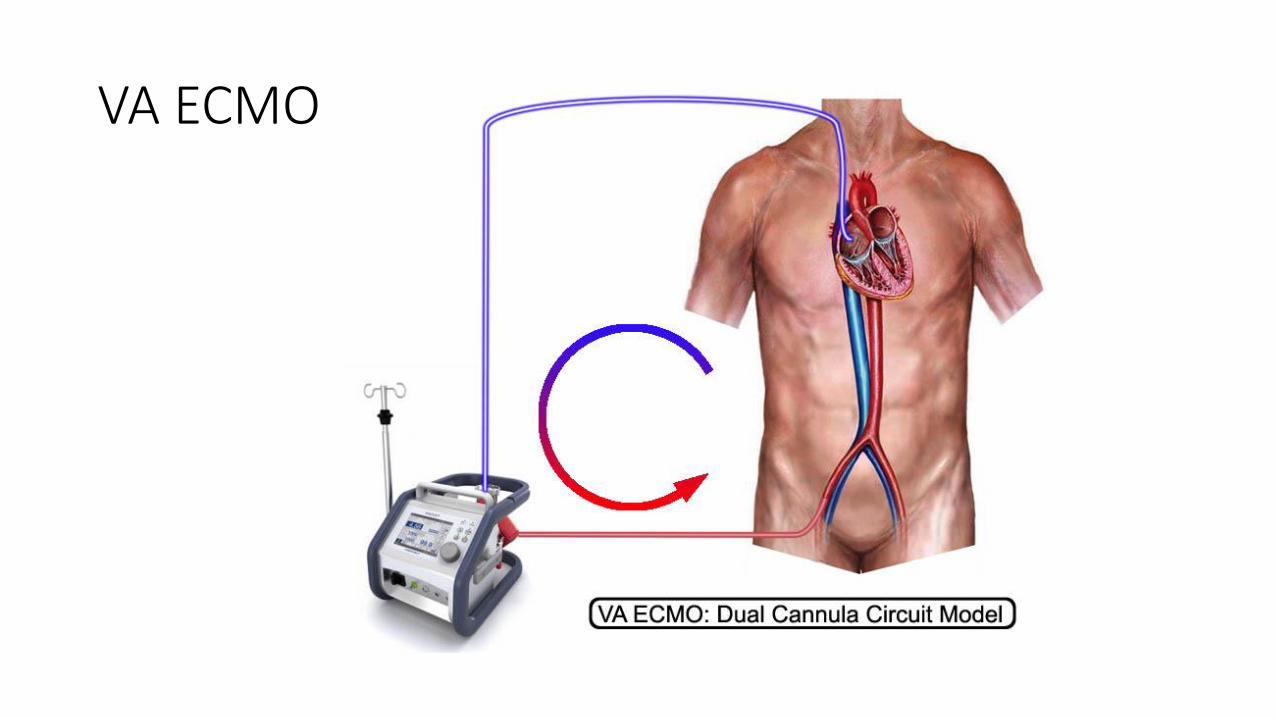
VA ECMO

J Am Coll Cardiol. 2015;66(23):2663-2674.
EDP and arterial elastase as ECMO flow
TPR
ECMO + IABPEcpella
Elastase EDV to ESP
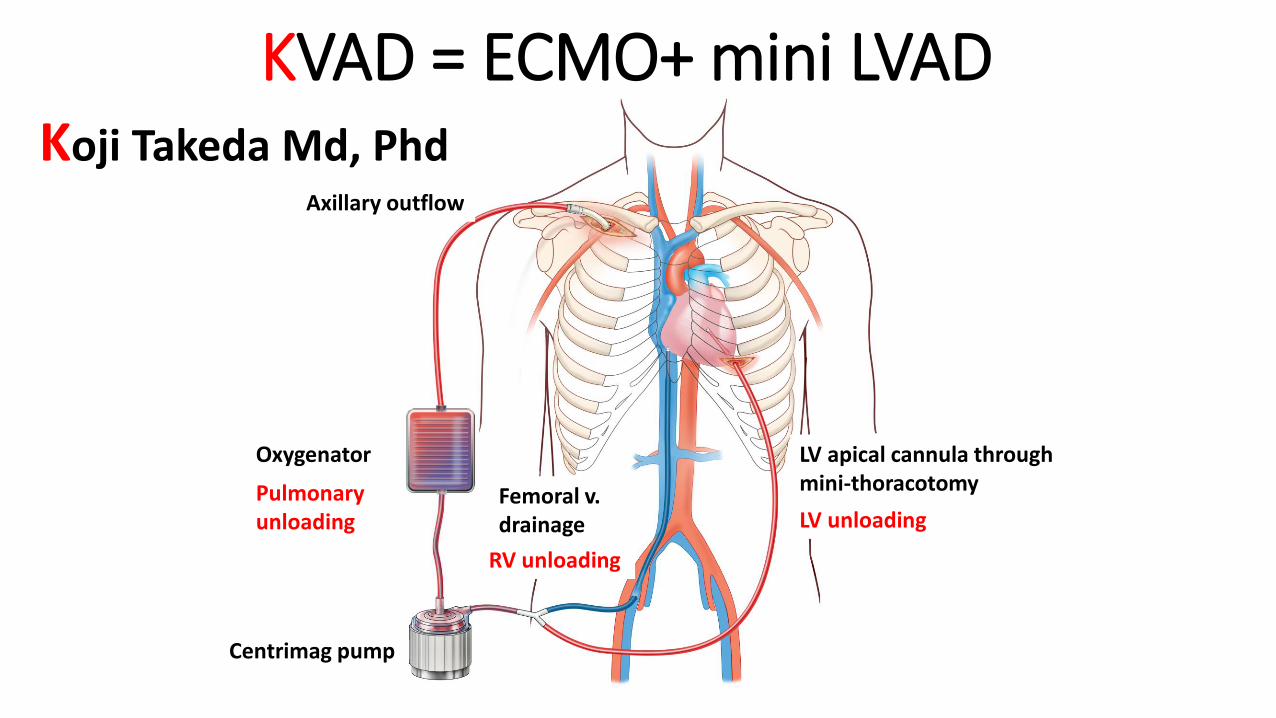
KVAD = ECMO+ mini LVAD
Centrimag pump
Oxygenator LV apical cannula through mini-thoracotomy
Axillary outflow
Femoral v. drainage LV unloading
RV unloading
Pulmonary unloading
Koji Takeda Md, Phd
J Am Coll Cardiol. 2015;66(23):2663-2674.
.
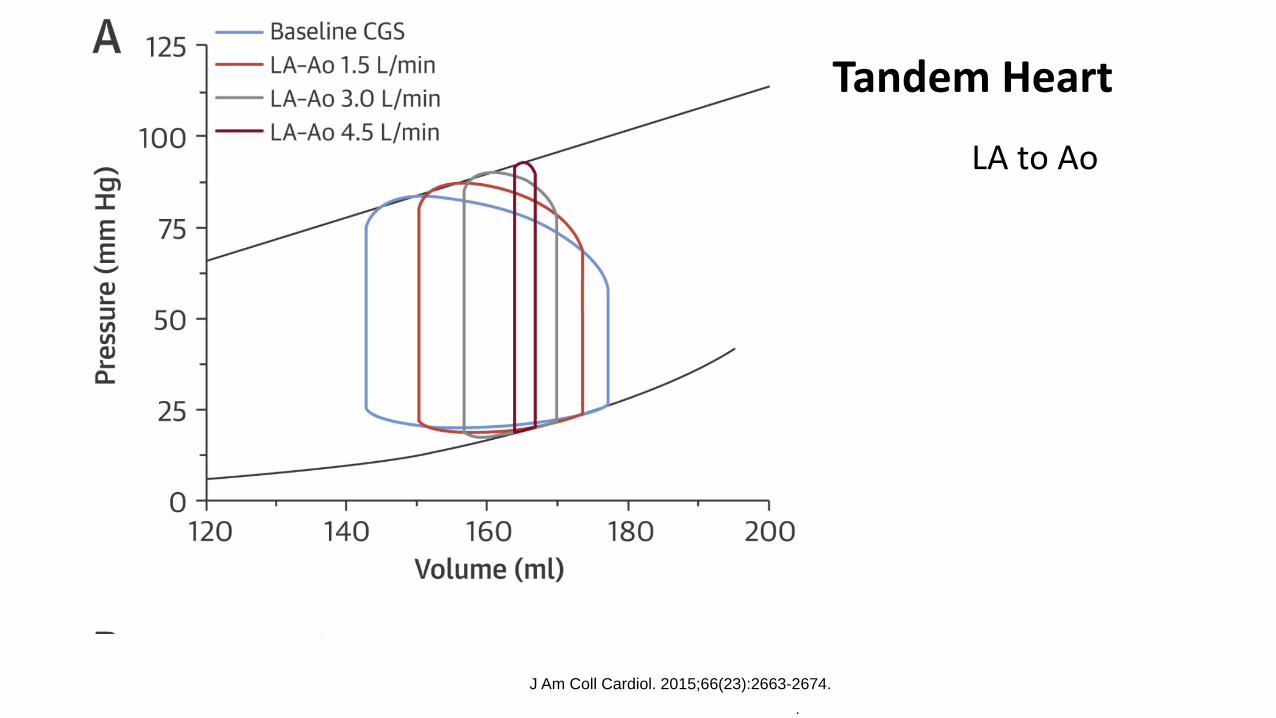
LA to Ao
Tandem Heart

Effect of LV to arterial MCS
J Am Coll Cardiol. 2015;66(23):2663-2674.
Impella; durable VADs

Reyentovich, A. et al. (2016)
Nat. Rev. Cardiol.
Tandem Heart n=33
Impella 2.5 n=26
Tandem Heart n=41
Randomized trials of Percutaneous MCS vs IABP in AMI
3 trials totaling 100 patients
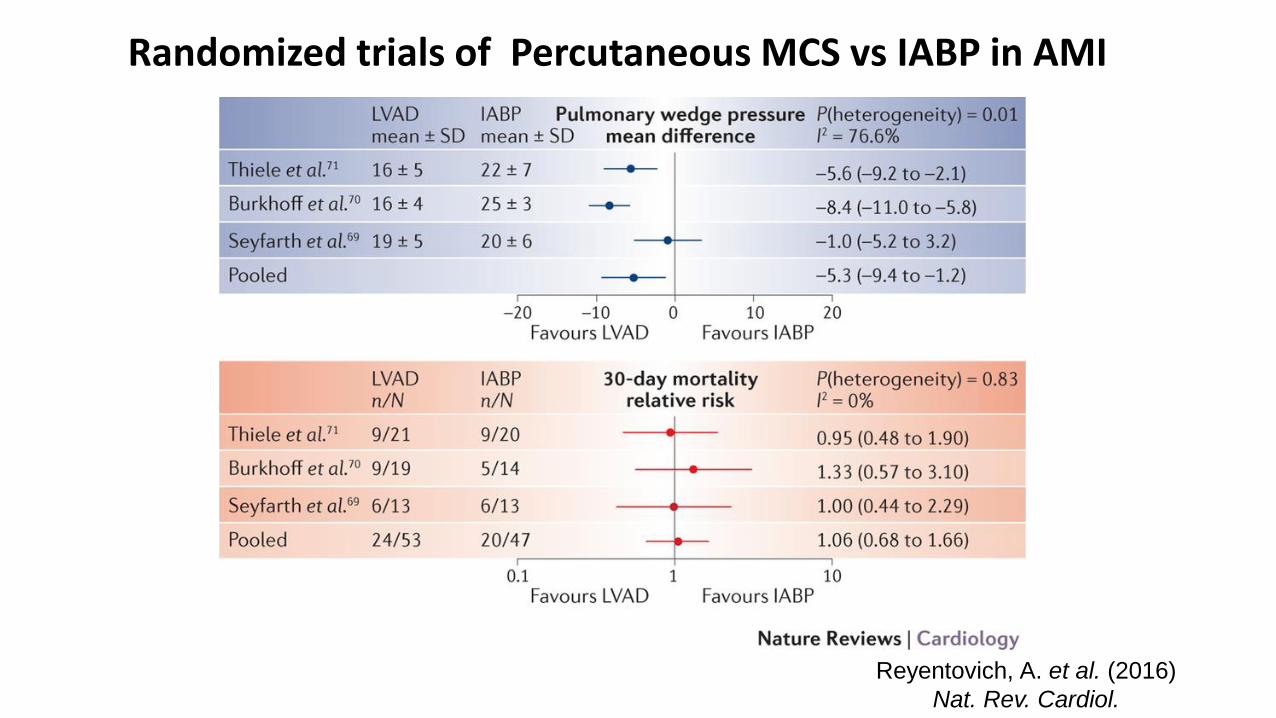
Reyentovich, A. et al. (2016)
Nat. Rev. Cardiol.
Randomized trials of Percutaneous MCS vs IABP in AMI

Guideline Recommendations of Short Term MechanicalAssist Devices in Cardiogenic shock
ACC/AHA/SCAI ESC/EACTS
IABP Class IIA Hemodynamic instability after AMI
IIb Hemodynamic instability after AMI
ECMO none none none ECMO implantation should be considered for temporary support in patients with acute heart failure with potential for functional recovery following revascularization.
Tandem Heart IIB Same as IABP IIb Routine use of percutaneous centrifugal pumps is not recommended.
Impella IIB Same as IABP none none

NYHA I II IIINYHA
IV
NYHA Symptom Class:Back and forth
ARisk
BAsx
Structural dx
CSx ever
ACC/AHA Stages: One-way progression
D= IV sxRefractory to
Optimal Med Rx
INTERMACSProfiles
e.g. Tx, VAD,Continuous Inotropes onlyindicated for Stage D
Evolution of Heart Failure Classification
INTERMACS: Interagency Registry for Mechanically
Assisted Circulatory Support

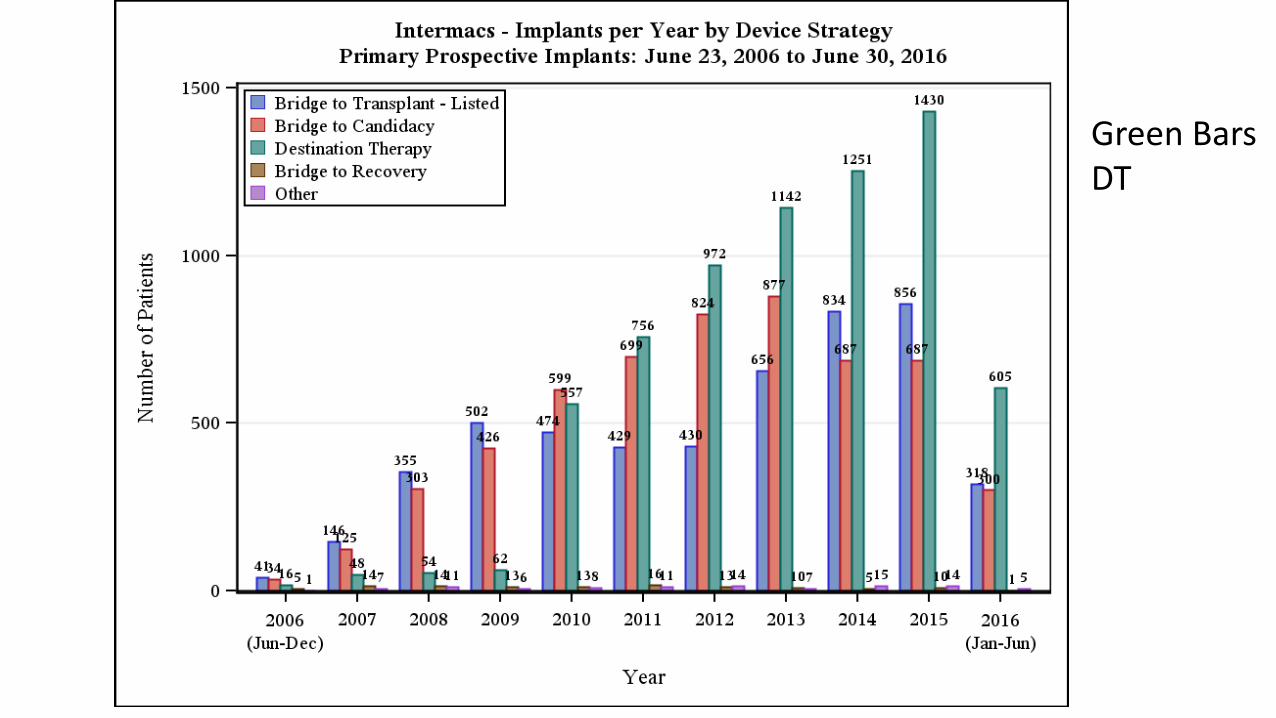
Green Bars DT


LVAD vs TxLVAD Tx
Body Size Still w limits
BSA<1.3 ??
All sizes
Age No age limit 70
RV failure RVSWI PVR< 6 Wood U
Restrictive CM Inadequate Yes
Urgent
Situations
Yes No
Assess Neuro
Status
Yes No

Patient Selection for VADs
• Severity of CHF• INTERMACS; HFSS; Seattle HFM
• Exclude significant co-morbidity:
if unclear support with short term device
• Assess need for biventricular support
• Assess need for short vs long term support
• Assess peri-operative risk
No severe end-organ dysfunction/failure
Ability to tolerate anticoagulant or antiplatelet therapieswithout plans for correction

ADULT PROFILES IV Ino IABP/V
ent
Official Shorthand NYHA
CLASS
INTERMACS
LEVEL 1
X X “Crash and burn” IV
INTERMACS
LEVEL 2
X X “Sliding fast” on inotropes IV
INTERMACS
LEVEL 3
X “Stable” Continuous Ino-”Dependent” * IV
INTERMACS
LEVEL 4
Resting symptoms on oral therapy at
home.
ambul
IV
INTERMACS
LEVEL 5
“Housebound”,
Comfortable at rest, symptoms with
minimum activity ADL
ambuI
IV
INTERMACS
LEVEL 6
“Walking wounded”-ADL possible but
meaningful activity limited
IIIB
INTERMACS
LEVEL 7
Advanced Class III III

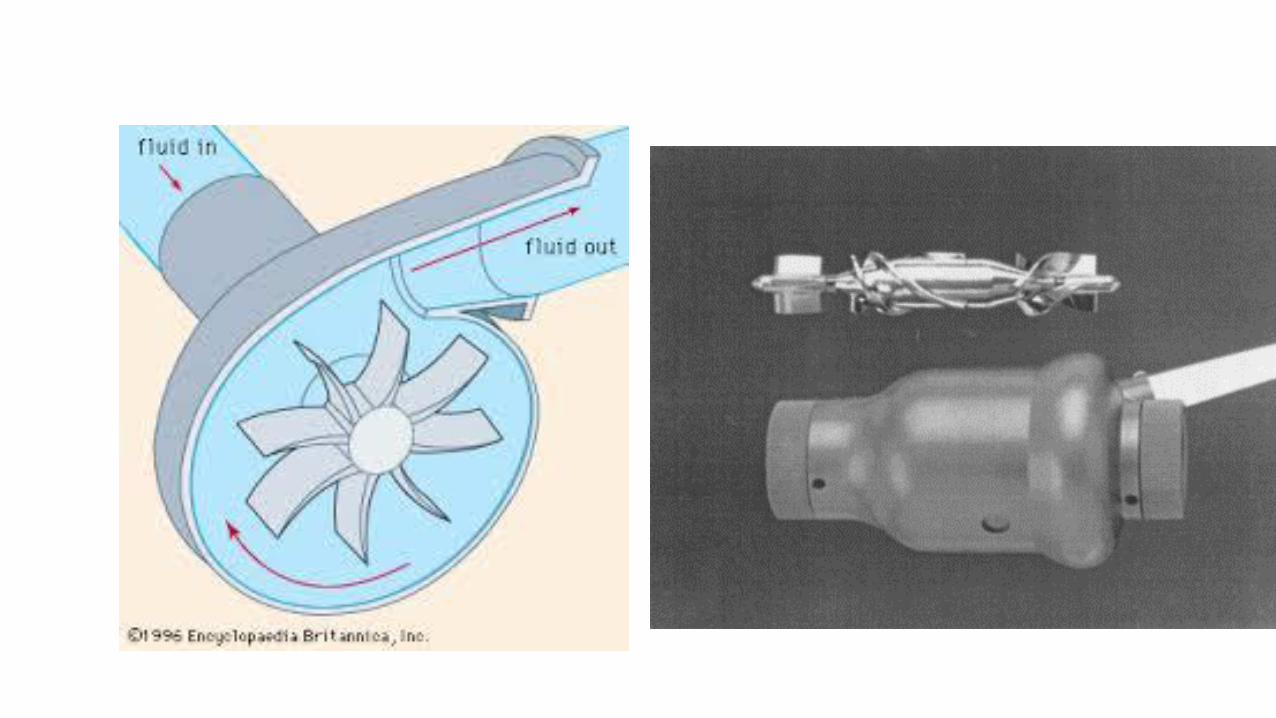
HeartMate IITM LVAS
The HeartMate II LVAS (St. Jude Medical, Inc.) is a mechanical
bearing axial continuous-flow blood pump;
only device in the US approved for both Bridge-To-Transplant
(BTT) and Destination Therapy (DT) patients
Mehra MR, Naka Y, et al. Published Nov 16, 2016 at
NEJM.org



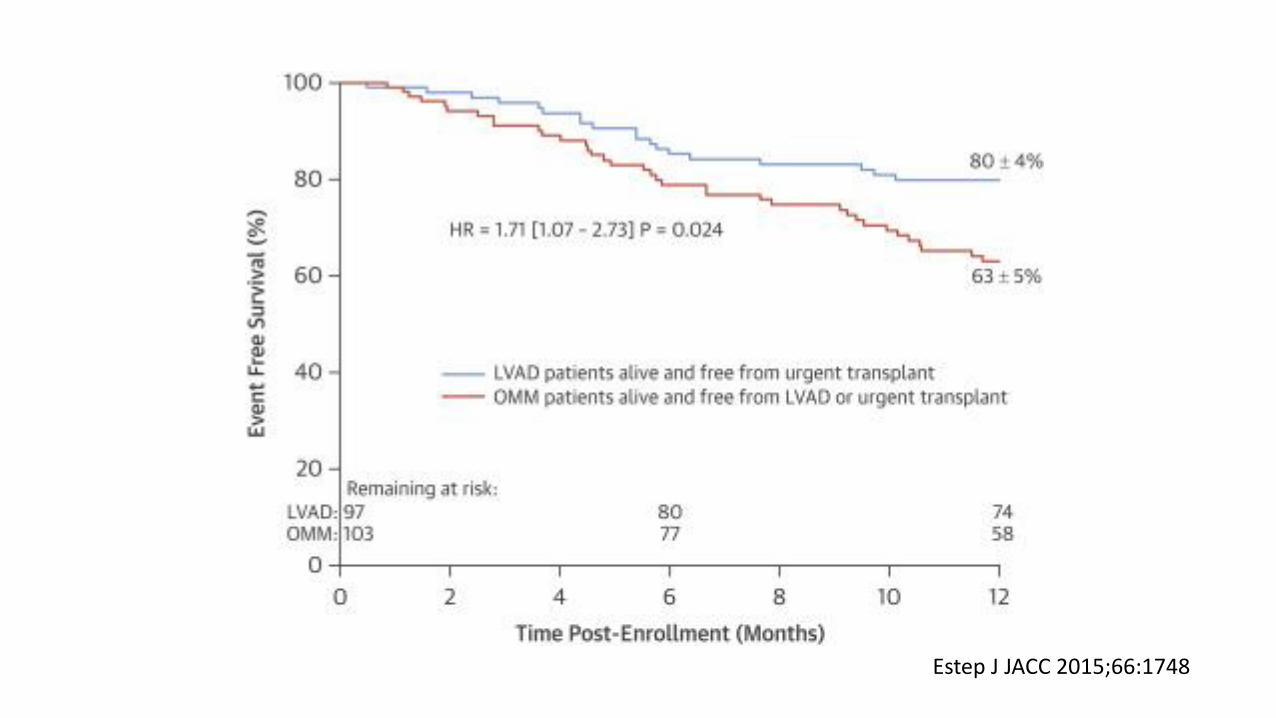
Estep J JACC 2015;66:1748
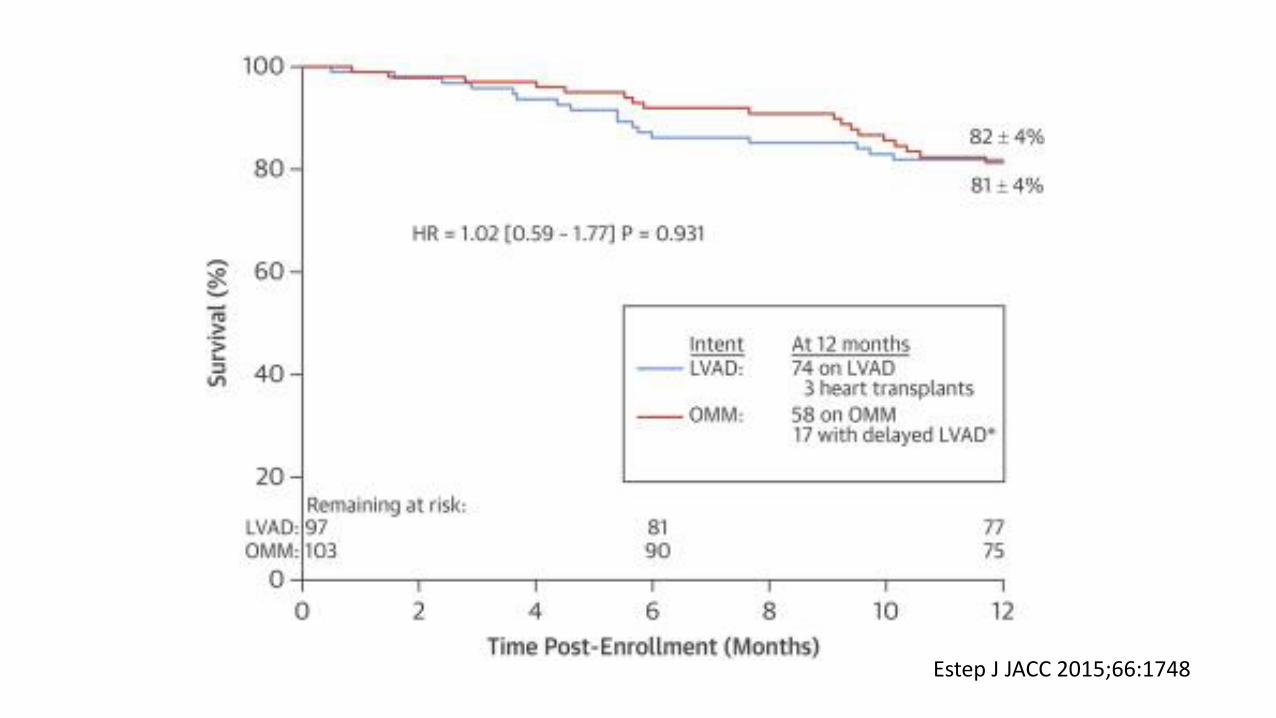
Estep J JACC 2015;66:1748


Adverse Events OMM (n = 103) LVAD (n = 94) DT Trial§(EPPY)
Bleeding 1 (1) [0.02] 44 (47) [1.22]‡ 1.13
GI bleeding 1 (1) [0.02] 29 (31) [0.76]‡‖ —
Driveline infection — 9 (9.6) [0.14]‡ 0.22
Pump thrombus — 6 (6.4) [0.08]† 0.07¶
Pump exchange yr 1 — 4 (4.3) 2.10%
Stroke 2 (2) [0.02] 8 (8.5) [0.09]∗ 0.08
Arrhythmias VT/VF 6 (5.8) [0.12] 17 (18.1) [0.23]∗ 0.46
Worsening HF# 36 (35) [0.68] 10 (10.6) [0.12]‡ —
Rehospitalizations 64 (62) [1.43] 75 (79.8) [2.49]‡ 2.64∗∗
Composite event rate†† 39 (38) [0.83] 62 (66) [1.89]‡ 2.09
Relative Risk (95% CI):OMM/LVAD: 0.44 (0.35-).56)
Adverse Events in ROADMAP

HeartMate II LVASHeartMate 3TM LVAS Magnetic Levitation Technology
The HeartMate 3 LVAS (St. Jude Medical, Inc.) is a
centrifugal-flow, fully magnetically levitated blood pump
engineered to minimize destruction of red blood cells and
thrombosis
• Wide blood-flow passages to reduce shear stress
• Frictionless with absence of mechanical bearings
• Intrinsic Pulse designed to reduce stasis and avert thrombosis
Mehra MR, Naka Y, et al. Published Nov 16, 2016 at
NEJM.org


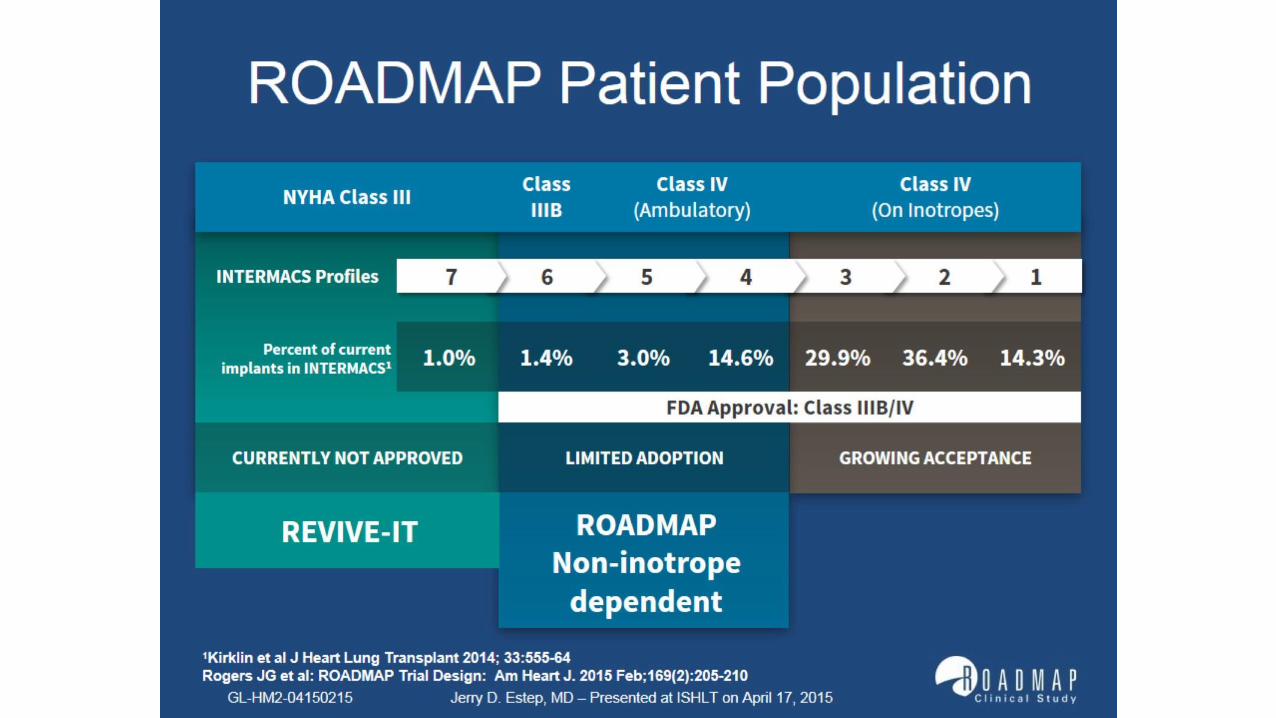
• Patients with advanced heart failure and severe limitations (NYHA IIIB or IV), refractory to standard medical therapy and deemed as necessary candidates for left ventricular assist device implantation, irrespective of the intended goal of pump support (BTT or DT)
• Key exclusion criteria included planned biventricular support, irreversible end-organ dysfunction, or active infection
Target Population
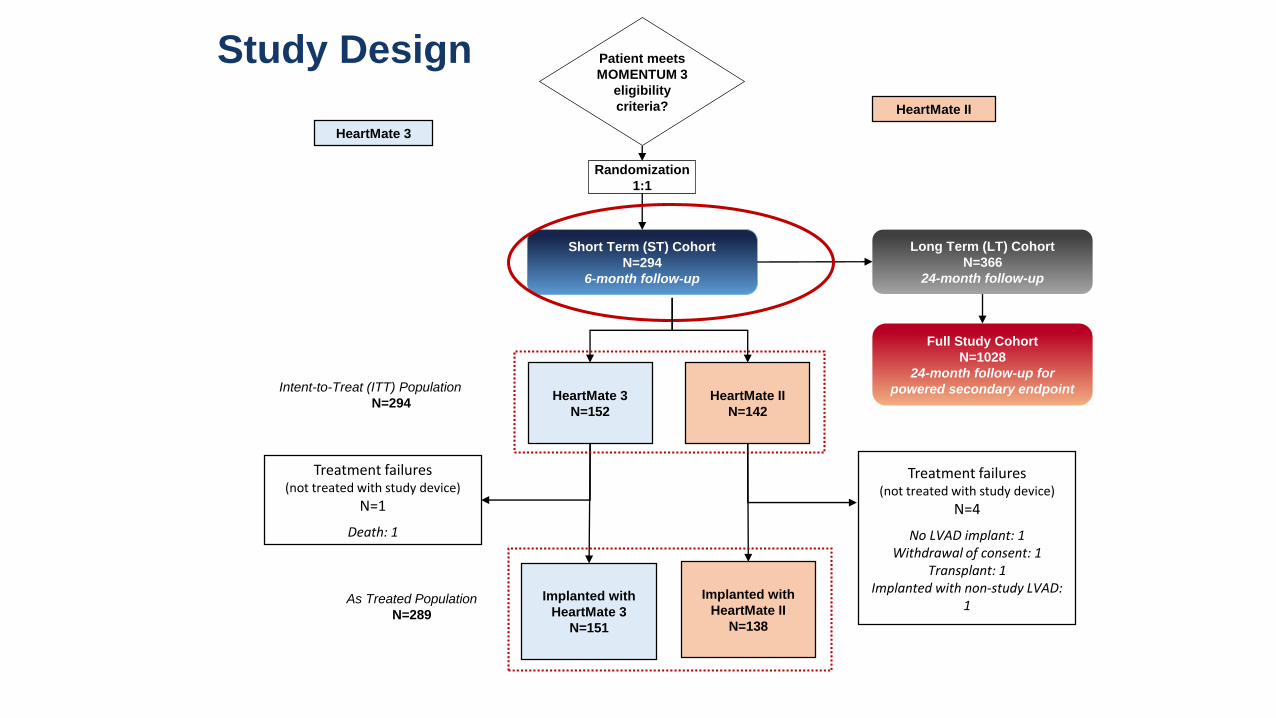
Patient meets
MOMENTUM 3
eligibility
criteria?
Short Term (ST) Cohort
N=294
6-month follow-up
Randomization
1:1
Study Design
HeartMate II
HeartMate 3
Long Term (LT) Cohort
N=366
24-month follow-up
Full Study Cohort
N=1028
24-month follow-up for
powered secondary endpointHeartMate 3
N=152
HeartMate II
N=142
Treatment failures(not treated with study device)
N=4
No LVAD implant: 1Withdrawal of consent: 1
Transplant: 1Implanted with non-study LVAD:
1
Treatment failures(not treated with study device)
N=1
Death: 1
Implanted with
HeartMate 3
N=151
Implanted with
HeartMate II
N=138
Intent-to-Treat (ITT) Population
N=294
As Treated Population
N=289

• Primary Endpoint (composite, by ITT):
• Survival at 6 months free of disabling stroke (modified Rankin score >3) or reoperation to replace or remove the pump (other than for recovery)
• Demonstration of non-inferiority of HeartMate3™ LVAS to HeartMate II™ LVAD
Study Endpoint
Caution – HeartMate 3 LVAS is an investigational device. Limited by Federal (United States) law to investigational use
SJM-HM3-1116-0003 | Item approved for global use.

Baseline Characteristics
Characteristic
HeartMate 3
(n=152)
HeartMate II
(n=142)Age - years
Mean 60 ± 12 59 ± 12
Left ventricular ejection fraction - % 17.1 ± 5.0 17.3 ± 4.9
Male sex - no. (%) 121 (80) 114 (80)
Race – no. (%)
White 104 (68) 107 (75)
Black or African American 37 (24) 24 (17)
Other* 11 (8) 11 (8)
Body surface area - m2 2.1 ± 0.3 2.1 ± 0.3
Ischemic cause of heart failure - no. (%) 68 (45) 72 (51)
History of stroke - no. (%) 12 (8) 14 (10)
Concomitant medication or intervention - no (%)
Intravenous inotropic agents 132 (87) 121 (85)
IABP 18 (12) 21 (15)
INTERMACS 2 50 (33) 44 (31)
INTERMACS 3 76 (50) 69 (49)
Bridge to Transplant (BTT) 41 (27) 37 (26)
Bridge to Candidacy 27 (18) 27 (18)
Destination Therapy (DT) 84 (55) 78 (55)

Primary End Point Analysis (ITT)
0.00
0.20
0.40
0.60
0.80
1.00
0 1 2 3 4 5 6
Pro
bab
ility
of
Even
t Fr
ee
Surv
ival
Months no. at risk
HeartMate 3 152 146 138 135 130 128 127
HeartMate II 142 125 119 116 110 106 103
HeartMate II
HeartMate 3
77%
86%
Survival at 6 months free of disabling stroke or
reoperation to replace or remove the pump
Non-inferiority Analysis
Absolute difference +9.4% (95% LCB -2.1%), P<0.0001
Superiority Analysis
HR 0.55, (95% CI 0.32-0.95), P=0.037
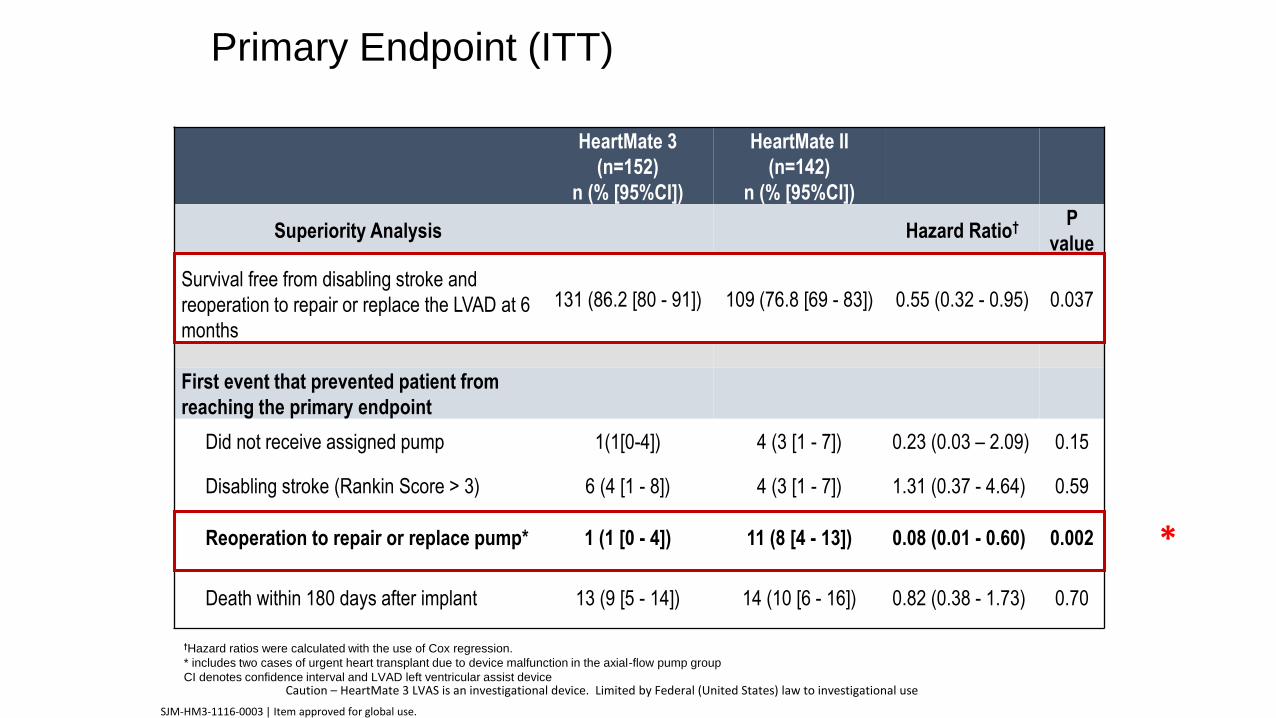
Primary Endpoint (ITT)
HeartMate 3
(n=152)
n (% [95%CI])
HeartMate II
(n=142)
n (% [95%CI])
Superiority Analysis Hazard Ratio† P
value
Survival free from disabling stroke and
reoperation to repair or replace the LVAD at 6
months
131 (86.2 [80 - 91]) 109 (76.8 [69 - 83]) 0.55 (0.32 - 0.95) 0.037
First event that prevented patient from
reaching the primary endpoint
Did not receive assigned pump 1(1[0-4]) 4 (3 [1 - 7]) 0.23 (0.03 – 2.09) 0.15
Disabling stroke (Rankin Score > 3) 6 (4 [1 - 8]) 4 (3 [1 - 7]) 1.31 (0.37 - 4.64) 0.59
Reoperation to repair or replace pump* 1 (1 [0 - 4]) 11 (8 [4 - 13]) 0.08 (0.01 - 0.60) 0.002
Death within 180 days after implant 13 (9 [5 - 14]) 14 (10 [6 - 16]) 0.82 (0.38 - 1.73) 0.70
†Hazard ratios were calculated with the use of Cox regression.
* includes two cases of urgent heart transplant due to device malfunction in the axial-flow pump group
CI denotes confidence interval and LVAD left ventricular assist deviceCaution – HeartMate 3 LVAS is an investigational device. Limited by Federal (United States) law to investigational use
SJM-HM3-1116-0003 | Item approved for global use.
*

Conclusions
• Short and long term mechanical support devices are being used for the treatment of cardiogenic shock and Stage D Heart Failure
• There are continued improvements in pump design
• Short term devices have not yet been shown to improve survival in cardiogenic shock but clearly provide greater hemodynamic support
• Adverse events remain common in the use of durable device support