Superantigens in dermatology
24
-
Upload
mohammad-adil-s -
Category
Health & Medicine
-
view
124 -
download
1
Transcript of Superantigens in dermatology


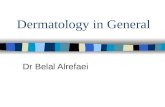
INTRODUCTION• Superantigens are a group of microbial and viral
proteins that cause polymorphic T cell stimulation and massive release of cytokines.
• Unlike conventional antigens, superantigens:
Exert their effects as globular intact proteins.
Are not MHC restricted.
Recognize and bind to variable region of T cell receptor(Vβ).
Have a high responding frequency for T cells(20-30%) against antigens(0.01- 0.1%).
• Generate large number of T cells with skin homing receptors (Cutaneous Lymphocyte Antigen).

APC
MHC 2
Ag
T cell
Cα Cβ
Vα Vβ
APC
MHC 2
T cell
Cα Cβ
Vα vβ
S
A
IL-6
IL-1
TNFα

CLASSIFICATION

TOXIC SHOCK SYNDROME
• Inflammatory response characterized by fever, rash,
hypotension and multiorgan dysfunction
• Represents the severe end of spectrum of superantigen
mediated diseases.
• First described in 1978 in children with Staph. aureus
infection.
• 1980s…… reports of epidemics in women using highly
absorbable vaginal tampons.

CAUSES
Staphylococcus aureus
Toxic Shock Syndrome Toxin(TSST-1):
• Predominant toxin associated with menstrual related cases.
• Unique ability to cross mucosal surfaces.
• Also causes less than half of the cases of non- menstrual TSS.
Staphylococcal Enterotoxin B & C (SEB & SEC):
• Cause of half of the cases of non-menstrual TSS.
Group A Streptococcus
Streptococcal Pyrogenic Exotoxin A (SPEA):
• Accounts for majority of Streptococcal TSS cases
Streptococcal Pyrogenic Exotoxin B & C (SPEB & SPEC)
Non Group A Streptococcus

CLINICAL FEATURES OF STAPHYLOCOCCAL TSS
• Menstrual TSS ---- associated with use of highly absorbent vaginal
tampons.
• Non- menstrual TSS ---- associated with post surgical wounds,
sinusitis, osteomyelitis, influenza, intravenous drug abuse, burn
wounds and gynaecological post partum infection.
• TSS begins with symptoms of fever, sore throat, myalgia and diarrhoea
or vomiting.
• Macular rash begins on the trunk and extends to the periphery & can
involve palms and soles. Later changes to scrletiniform rash.
• Non purulent conjunctival hyperemia, pharyngeal inflammation and
strawberry tongue are invariably present.
• Hypotension, altered mentation, fainting and overt shock occur.
• Rash desqumates in 1-2 weeks.
• Blood cultures positive in 10% cases only



CLINICAL FEATURES OF STREPTOCOCCAL TSS
• Streptococcal TSS ---- result of skin infection in 80% cases.
• Wounds appear to be the most common type of causative
infections.
• Also described as a complication of Varicella and influenza A.
• Initial presentation is skin pain localized to an extremity.
• Later erythema with edema develops, then cellulitis with
necrotising fasciitis and myositis occurs with concomitant
bloodstream invasion and herald of Toxic Shock Syndrome.
• Blood cultures are positive in more than 50% cases.

DIFFERENTIAL DIAGNOSIS
• Septic shock
• Staphylococcal exfoliative syndromes
• Rocky Mountain Spotted Fever
• Viral Hemorrhagic shock
• Measles
• Leptospirosis
• Stevens Johnson syndrome
• Kawasaki syndrome
• Scarlet fever

TREATMENT
• Remove the inciting cause
• Supportive care
• β-lactamase resistant antibiotics (e.g. Nafcillin): cause bacterial lysis and cause initial rise in TSST-1, so given with clindamycin (which inhibit bacterial protein toxin production).
• Vancomycin: due to rise in MRSA cases.
• IVIG in severe and recalcitrant cases.
• Systemic corticosteroids?

PROGNOSIS
• Mortality rate in Staphylococcal TSS is
approximately 5%, mostly because majority of
cases occur in otherwise healthy young individuals.
• Mortality rate in Streptococcal TSS is more than
30%.
• Recurrences seen in upto 20% cases.

SCARLET FEVER
• ‘Scarlatina’ in older literature.
• Characterised by exudative pharyngitis, fever and rash.
• Caused by Pyrogenic exotoxin producing Group A beta hemolytic Steptococcus.
• Disease of school going children, children <2 yrsprotected by maternal antiexotoxin antibodies.
• 80% children have antibodies by 10yrs
• Seen in winter & spring, associated with close contact & overcrowding.
• Transmission: Aerosol / Fomites / contaminated food.
• Combination of delayed type hypersensitivity and superantigen mediated processes.

• Usually evolves from a tonsillar/pharyngeal focus.
• 10% children with strep throat will develop scarlet fever.
• Can arise from infections of skin & soft tissue, surgical wounds(Surgical Scarlet fever) or the uterus (Puerperal Scarlet fever).
• Incubation period: 12 hours – 7 days.
• PRODROME: pharyngitis, headache, vomiting, abdominal pain & fever.
• SANDPAPER LIKE & BLANCHING RASH (1-2 days later): starts from neck, then to trunk & extremities, spares the palms & soles. ‘SUNBURN WITH GOOSE PIMPLES’
• Flushed face with CIRCUMORAL PALLOR
• PASTIA’S LINES: Confluent petechiae due to increased capillary fragility along the skin folds.

• Tonsils: edematous & erythematous
• FORCHHEIMER’S SPOTS: petechiae & red macules on soft
palate & uvula.
• WHITE STRAWBERRY TONGUE (0-2 days): White coated
tongue with red, edematous papillae.
• RED STRAWBERRY TONGUE (after 2 days): After
desquamation red tongue with prominent papillae.
• Tender anterior cervical lymphadenopathy.
• DESQUAMATIVE PHASE starting from face, involving
fingers & palms. Lasts from 1 – 4 wks.
• Diagnosis confirmed by Rapid Streptococcal Test or throat
culture.

DIFFERENTIAL DIAGNOSIS
• SSSS
• Kawasaki syndrome
• Atypical drug hypersensitivity reactions
• Staphylococcal scarlet fever
COMPLICATIONS
• Suppurative: Peritonsillar abscess, pneumonia, sinusitis, meningitis
• Non-suppurative: Acute Rheumatic fever, Glomerulonephritis

TREATMENT & PROGNOSIS
• Antibiotics: Penicillin & Erythromycin group
• Supportive Care
• Pre- antibiotic era: 20% mortality
• Presently: <1% mortality

STAPHYLOCOCCAL SCARLET FEVER
• Caused by Staphylococcal Enterotoxin B (SEB),
homologous to SPEA.
• Lack of pharyngitis.
• Scarlatiniform rash, but tender.
• Within few days, thick flakes develop & entire skin
desquamates.
• Not associated with rheumatic fever or glomerulonephritis.
• Previously considered to be a milder / abortive form of
Staphylococcal Scalded Skin Syndrome.

RECALCITRANT ERYTHEMATOUS
DESQUAMATING DISORDER(REDD)
• First described in 1992.
• Majority of patients have AIDS.
• Clinical features resemble Toxic Shock Syndrome,
but diagnostic criteria is not met
• Prolonged disease lasting for months with delayed
desquamation of diffuse, macular, erythematous
rash.

TOXIN MEDIATED ERYTHEMA
• Also called RECURRENT TOXIN
MEDIATED PERINEAL EYTHEMA.
• First described in 1996.
• Striking diffuse macular perineal
erythema within 24-48 hours of
pharyngitis with toxin producing
Group A Streptococcus or
Staphylococcus aureus.
• Clinical findings of Scarlet fever.
• Fever, hypotension and other
systemic signs of Scarlet fever /
TSS are ABSENT.
• Recurrences are common.

DISEASES INITIATED AND/OR
EXACERBATED BY SUPERANTIGENS
1. PSORIASIS
a) Guttate Psoriasis:
• Develops after Group A Stretococcal pharyngitis
• Superantigen mediated systemic activation of T cells and
resultant oligoclonal activation of keratinocytes.
b) Flaring of Psoriasis:
• Increased levels of keratinocyte MHC II expression in
patients of psoriasis, increasing cutaneous reactivity to
superantigens

2. AUTOECZEMATIZATION (ID) RESPONSE
• Because of ability of superantigens to home T cells to the skin,
superantigen producing Staphylococcus aureus or group A
Streptocoocus are believed to be the trigger for id response.
3. ATOPIC DERMATITIS
• Atopic patients have universally been found to harbor Staph.
aureus. Many atopic patients have Ig E antibodies that recognize
superantigens. Thus, they act as allergens in atopic patients and
cause disease flares.