
Summer Training Option for Rural Medicine · Summer Training Option for Rural Medicine ... Name of...
28
Scott Zerger KU Endowment Printed On: 10 November 2017 Requests of more than $5,000 1 Summer Training Option for Rural Medicine Requests of more than $5,000 KU Endowment Mr. Scott Zerger PO Box 928 Lawrence, KS 66044 O: 785-832-7400 M: 913-484-1045 Mr. Scott Zerger PO Box 928 Lawrence, KS 66044 [email protected] O: 785-832-7426 M: 913-484-1045
-
Upload
hoangduong -
Category
Documents
-
view
216 -
download
0
Transcript of Summer Training Option for Rural Medicine · Summer Training Option for Rural Medicine ... Name of...

Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 1
Summer Training Option for Rural MedicineRequests of more than $5,000
KU EndowmentMr. Scott Zerger PO Box 928Lawrence, KS 66044
O: 785-832-7400M: 913-484-1045
Mr. Scott Zerger PO Box 928Lawrence, KS 66044
[email protected]: 785-832-7426M: 913-484-1045
Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 2
Application Form
Organization InformationVerification of tax-exempt status* Organization is:
501(c)(3) public charity
Verification of status Please note: Applications from public charities (501(c)3 organizations) are required to attach verification of charitable status in order to be considered. A state sales tax exemption DOES NOT complete this requirement. Applications from churches and/or government entities are not required to attach a verification document.
IRS Determination Letter 10-18-2010.pdf
Physical Address If the physical address of your organization is different than the mailing address, please enter your physical address below.
1891 Constant AveLawrence, KS 66047 - 3743
Project InformationProject Name* Name of Project.
Summer Training Option for Rural Medicine
Amount requested* $50,000.00
Primary objectives* The Foundation has six primary objectives. Which of these does your program or project best addresses:
Health Care

Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 3
County or Counties Served* Please check the primary county served by the program/project for which you are requesting funds.
CheyenneCloudDecaturEllisEllsworthGoveGrahamLoganMitchellNortonOsborneOttawaRawlinsRepublicRooksRussellSalineShermanSmithThomas
Communities Served* Please list the primary community served by the program/project for which you are requesting funds.
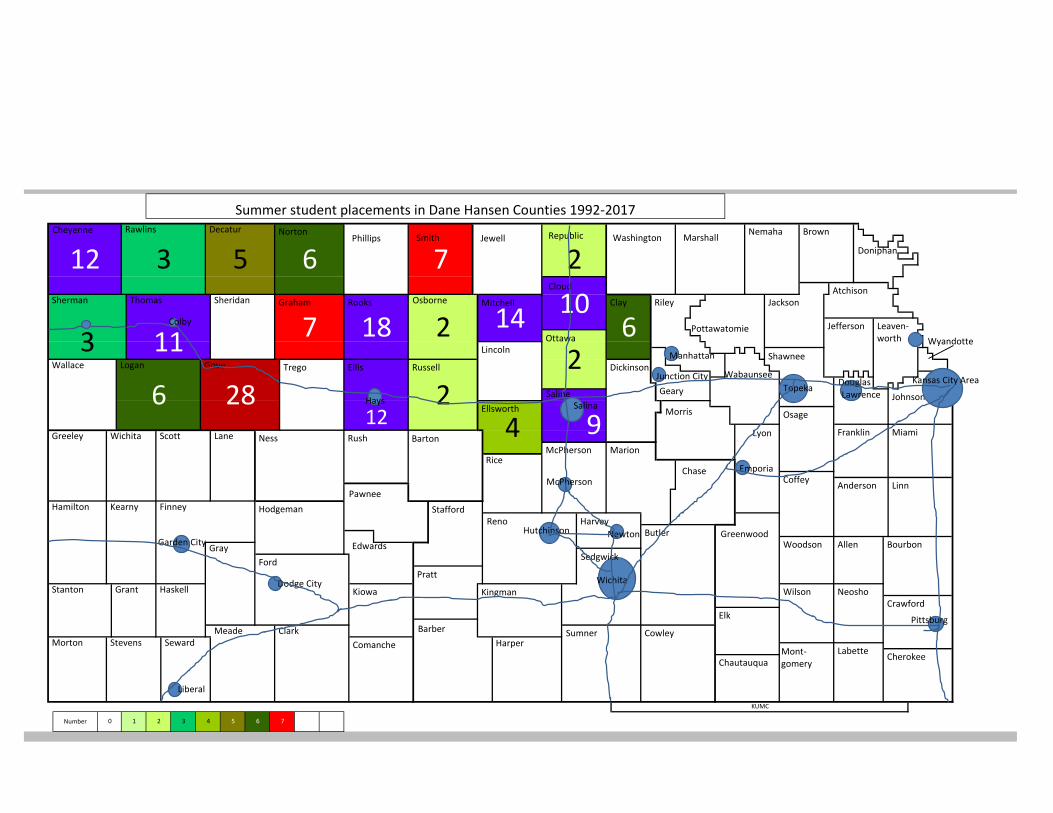
This year we placed students in the following counties (listed below and refer to attached map). There is work in several communities to have students in the years ahead. Over the duration of the program we have placed students in all the counties in the Hansen region except Wallace, Sheridan, Trego, Phillips, Jewel, and Lincoln. Wallace is covered by the doctors in Greeley County and there was a student with that physician this past year. Sheridan is covered by doctors in Quinter and we have had many students there over the years, including a student this past year. We are working on developing student rotations in the next year in Phillips, Trego and Lincoln counties.
• St Francis in Cheyenne County• Clay Center in Clay County • Concordia in Cloud County• Oberlin in Decatur County• Quinter in Gove County• Hill City in Graham County• Plainville in Rooks County• Stockton in Rooks County• Colby in Thomas County
Strategic Doing Project* Was this application generated through the Strategic Doing initiative?
No
Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 4
Target Population* Please check one or more populations served by the program/project for which you are requesting funds.
All
Project Description* Briefly describe the program/project for which you are requesting funds.
The program began in 1992, completing our 25th year. The Dane G Hansen Foundation has funded the program since 2015. In honor of the 25th year we changed the program name to the Summer Training Option for Rural Medicine (STORM). STORM is an elective for 2nd year medical students during the summer between1st and 2nd year.
Students complete an orientation week filled with skill building workshops. They then attend the Kansas Academy of Family Physicians annual meeting. They move to their host community after the meeting and live in housing provided. This allows an immersion experience. Students remain in this community for six weeks, participating in the clinical care of patients under the supervision of their preceptors. Students participate in surgery, obstetrical care, clinic visits, hospital visits and emergency room care.
Frequently, this is a life changing experience for students. They are witness to the unfiltered realities of birth, death, medical hardship, and celebrate the joys in a rural family medicine practice. They return to medical school charged for more. They describe personal and professional growth.
This program is only possible through the generosity of the volunteer clinical preceptors in hosting these students in their communities, practices and homes. Placements are limited to the availability of a doctor and a hospital in the host county. There are several places that do not meet that basic requirement, but over the years students have participated in every available county in northwest Kansas.
Students also participate in practice based research coordinated from KU. Many students have participated in writing articles and presenting the findings at local, state and national venues. This rural clinical elective is one of the most popular at KU. Reviews of the program are very high. It is offered at a critical time in their development as a physician. Students will use these rural experiences to shape their career and specialty choice.
Grant Request Description* If funded, how will you specifically use the Dane G. Hansen funds?
Selection of students is based on rural experience growing-up and interest in returning to rural sites for their practice. Students have returned to the sites where they completed this program after graduation.
Participation continues to increase. This year we had 38 students enrolled. Since its inception, the program has had 670 participants.
Dane G. Hansen funds will be used to provide stipends for students for the summer. Since students have to maintain their residence in the city of their school attendance and they are frequently not receiving scholarships during the summer, then students need funding for this purpose. Stipends are $2,800 for the entire 7 week summer program. Funds are not used for faculty salaries. We have secured funding for other aspects of the program to cover expenses of the orientation week of training (please refer to the budget spreadsheet).

Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 5
Project Objectives* What do you hope to achieve and how will it benefit the people of Northwest Kansas?
The main objective of this rural program is to introduce students to rural practice. Through this we hope to achieve a desire for students to return to rural communities in Kansas to practice primary care medicine.
Kansas is on the cusp of a significant rural physician workforce crisis. In 2007 a multi-stakeholder group participated in a comprehensive workforce analysis. The report discovered a number of issues. Kansas as a state is underserved in primary care medicine, we have significant challenges in the geographic distribution of physicians and, more importantly, future projections of workforce were very concerning. It is projected that we will not be able to keep pace with the expected attrition of physicians due to retirement in the next 10 years. To minimize the impact to access to health care and to the health of Kansans there are many initiatives to address the issues. Some of the more prominent programs are:
- Scholars in Rural Health- Salina Branch Campus- Kansas Medical Student Loan- Rural Medicine Interest Group- Summer Rural Research and Practice Program- Third year rural option for required clerkships- Fourth year rural preceptorship- Bridging Program- Recruitment and Retention CenterThe Summer Rural Research and Practice Program gives students the opportunity to live the lifestyle of a
rural practicing physician. It is important for the student to live in the community in order to understand the richness of life as a doctor integrated into their community. Students begin to understand the patient-doctor relationships that have developed over time. They are introduced not only to the patient care aspects but the multifaceted aspects of being a rural doctor. Students can envision their future practice life.
This program is often the first time that students are able to experience hands on clinical training. In order to prepare for this immersion experience, students are required to spend five days in an orientation with hands-on clinical skills training. The sessions include: introduction to the program, Human Subjects Training, head, ears, eyes, nose, and throat exam training, a casting workshop, suture workshop, neurology exam training, Advanced Life Support, and a musculoskeletal workshop. Near the end of the orientation week, the students are required to participate in the Kansas Academy of Family Physicians annual meeting.
This program comes at a time that is critical in medical student education. Students are yearning for clinical medicine at this point, instead of book work. Students have a high moral compass and a strong desire to serve people and working with these rural physicians provides just the ticket to reinforce their ideals. It reminds them of why they came to medical school in the first place.
Students are placed as close to their home community as possible. Many are looking for a way to return home and serve their community. We strive to make this happen. Many of them have done shadowing and have developed a mentor relationship with the hometown doctor and want to go back to do more.
Objective #1 – Increase the number of doctors in rural Kansas.Through the many KUMC Rural programs, repeated exposure to rural life and rural practice, and
continued mentorship/preceptorship with rural physicians the program has been successful. An analysis in 2014 revealed that of the 536 participants 81 are practicing in rural Kansas and 14 returned to where they did the summer rural program. There have been 154 students in the NW region of the state over the years and 23 practicing physicians, in this region, participated in this program as a student.
Objective #2 – Introduce students to rural medicineThrough placements of students in a clinical elective away from the main campuses and in rural locations,
students are exposed to rural practice and rural life. Many of these students come from rural hometowns and rural life is not something new. But, life as a doctor in a rural town is frequently a new concept.
Objective #3 – Introduce students to clinical medicineStudents at this stage have had minimal exposure to direct patient care. They have had lectures in clinical
skills and these are coupled with clinical skills labs. Students also have about 30-40 hours shadowing with a faculty preceptor. But, the summer rural program adds about 240-300 hours of patient contact and many students are involved in procedures with their supervising doctor.

Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 6
Objective #4 – Clinical Based research exposureAs part of the program students are part of a larger school of medicine based research program. They
learn human subjects protection. They learn various research techniques. They learn that rural clinical practice can be a very rich, highly intellectual, and professionally stimulating way to practice medicine. For some students the knowledge that they can have a rural practice and be involved in meaningful research for their patients is key to pursuing a rural career in medicine.
Timetable for the Project* When is the project projected to begin and end? For ongoing projects, when will the Dane G. Hansen funds be utilized?
The program runs from the first week of June through the 3rd week of July (7 weeks). The next cycle is projected to begin in June of 2018. Dane G Hansen funds would be utilized for student stipends. The stipends total $2800.00 per student. The payments are broken down into three allotments. The first check, for $1200.00 is given out at the conclusion of orientation week. The second check, for $1200.00, is mailed at the midway point of the rotation. The final check, for $400, is mailed at end of the rotation upon the completion of all assignments. Other funding has been secured to be utilized prior to the start of the program to buy supplies and clinical skills lab time to prepare for the orientation week.
Additional Support Describe additional sources of support (if any) that have been secured or that will be pursued for this project.
In addition to the Hansen Foundation, there are four additional sources. The H.L Baker Trust of LaCrosse, Kansas donates $36,000.00 annually, used exclusively for student stipends. The Kansas Academy of Family Physicians (KAFP) donates about $13,500.00, to purchase supplies, provide free registration, and provide free housing, for students at the annual June conference. The Sutton Family Endowed Account is utilized for the cost of training supplies, teaching support, and incidentals. The money donated by this fund varies yearly. Finally, the KU-SOM feels that this program is vital to the growth of physicians in rural Kansas. Due to the significant increase in popularity of this elective, the school has agreed to provide additional funding when necessary. Last year this elective had fifty two applicants, the largest number seen since the start of this program! The school of medicine also provided $10,000 to support the expansion last year. They have committed support in the future.
Evaluation* How will you evaluate the success of the project/program? Be specific. (If funded, this will be helpful when completing the final grant report.)
At the conclusion of the course we ask the students to write a reflection paper. This gives them the opportunity to take a retrospective look at their experience in rural Kansas. The students often comment that this rotation solidified, in their mind that they want to enter primary care in a rural location. In addition to the reflection assignment we ask the students to evaluate the orientation week. This allows for us to make necessary changes for future students. Finally, we plan to continue to gather data to help us track how many of the students that participate in the program eventually enter rural practice. Currently we track county level data on the number of participating students, the physicians that are involved each year, the downstream effect on workforce, residency specialty in which students match, student evaluation of the program and orientation, and evaluation of the preceptor and site. Our hope is that this program will continue to provide future physicians for rural Kansas.

Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 7
Sustainability* How will the project/program be sustained in the future? (For capital projects, how will you maintain or operate the item or facility?)
The Summer Rural Research and Practice Program will continue for years into the future. Started in 1992 it has a 25 year track record of success. There is a renewed interest in providing students with an early clinical exposure and in addressing rural physician workforce issues. This program provides both. In addition, there is a research component that is practice-based. This is an area of very active interest and growth on the research scene. The program is connected to the school of medicine in many ways and there is broad support. Funding is a limiting bottleneck, but with the recent development of broad-based funding support the financial future of the program is much more secure than in the past. We plan to continue to develop further diversification in the funding streams. The other historical bottleneck is the availability of rural physician preceptors to host students. We are currently on a campaign to gain new participants and last year there were 11 new preceptors for the program.
Supporting DocumentsProposal Budget* Complete the budget form attached on the Grant Criteria page under document requirements and upload here.
2018 DGH-Budget-Sheet.xlsx
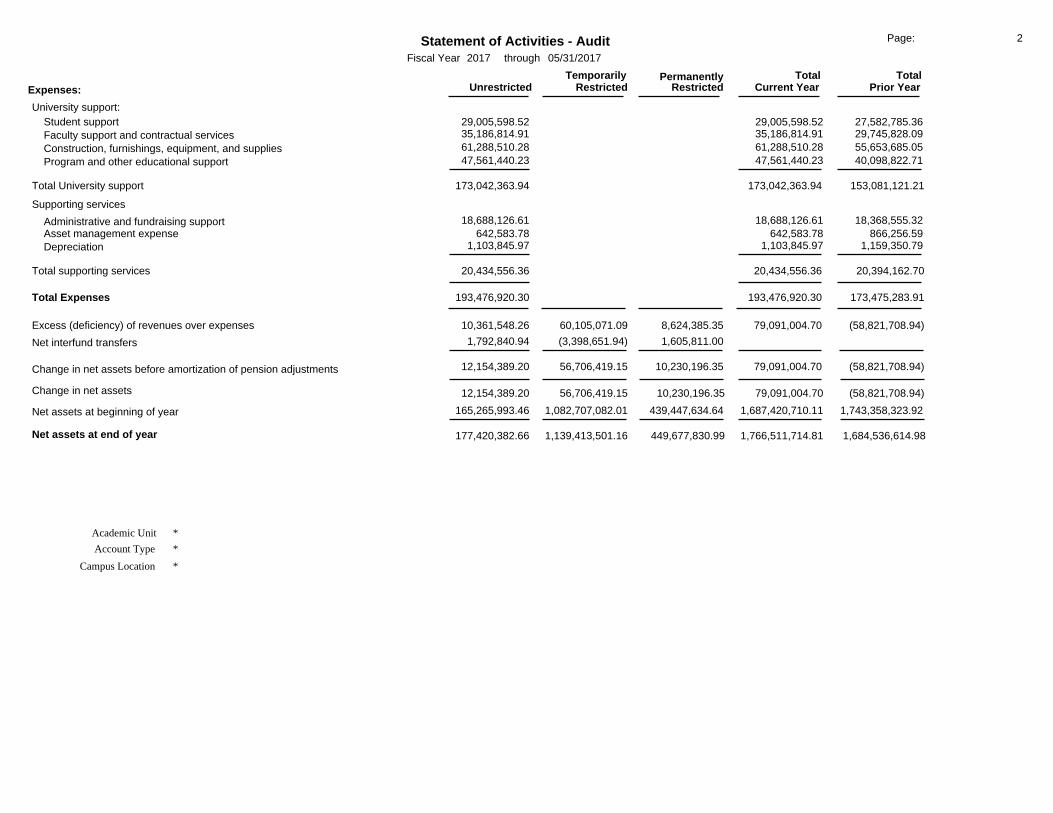
Balance Sheet* A detailed financial statement is required. Please do not attach your entire audit report. An example can be found on the Grant Criteria page, under document requirements.
YTD 2017 Statement of Financial Position Through 5-31-17.pdf
Income Statement* A detailed financial statement is required. Please do not attach your entire audit report. An example can be found on the Grant Criteria page, under document requirements.
YTD 2017 Summary of Activity Through 5-31-17.pdf
Board of Directors* Please attach a list of your board members. (Name and title, no biographies.)
2018- KU Endowment-Board of Directors.pdf
Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 8
Bid or Quote A copy of the bid or quote is required for a capital project or purchase.
Letter of Support 1 A letter of support may be attached, but is not required.
JLBrull KUMC Hansen Support Letter 2017-10-21.pdf
Letter of Support 2 A second letter of support may be attached, but is not required.
M Machen Support letter.pdf
Letter of Support 3 A third letter of support may be attached, but is not required.
Owings Support Letter.pdf
Additional Documents If there are additional documents that are critical to the trustees’ understanding of your proposal, upload them here.
Additional Documents.pdf
Electronic SignatureSignature of Applicant* By entering my full legal name here, I warrant the truthfulness of the information provided in this application.
Michael Kennedy, MD
Title of Applicant* Associate Dean for Rural Health Education, KU School of Medicine
Signature of Principal or College President (if required) By entering my full legal name here, I warrant that I have read and support this application.
Scott Zerger
Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 9
Title of Principal or College President Senior Director, Corporate & Foundation Development, KU Endowment
Signature of CEO, Director, Mayor, etc. If this request is for a City, 501 (c)(3) Organization, Government Entity, etc., the signature of the CEO, Director, Mayor, etc., is required.
By entering my full legal name here, I warrant that I have read and support this application.
Jerome Davies
Title of CEO, Director, Mayor, etc. SVP of Development & Secretary, KU Endowment
InternalTracking Number*
2017-12-6
501c3* Yes

Scott Zerger KU Endowment
Printed On: 10 November 2017 Requests of more than $5,000 10
File Attachment SummaryApplicant File Uploads• IRS Determination Letter 10-18-2010.pdf• 2018 DGH-Budget-Sheet.xlsx• YTD 2017 Statement of Financial Position Through 5-31-17.pdf• YTD 2017 Summary of Activity Through 5-31-17.pdf• 2018- KU Endowment-Board of Directors.pdf• JLBrull KUMC Hansen Support Letter 2017-10-21.pdf• M Machen Support letter.pdf• Owings Support Letter.pdf• Additional Documents.pdf

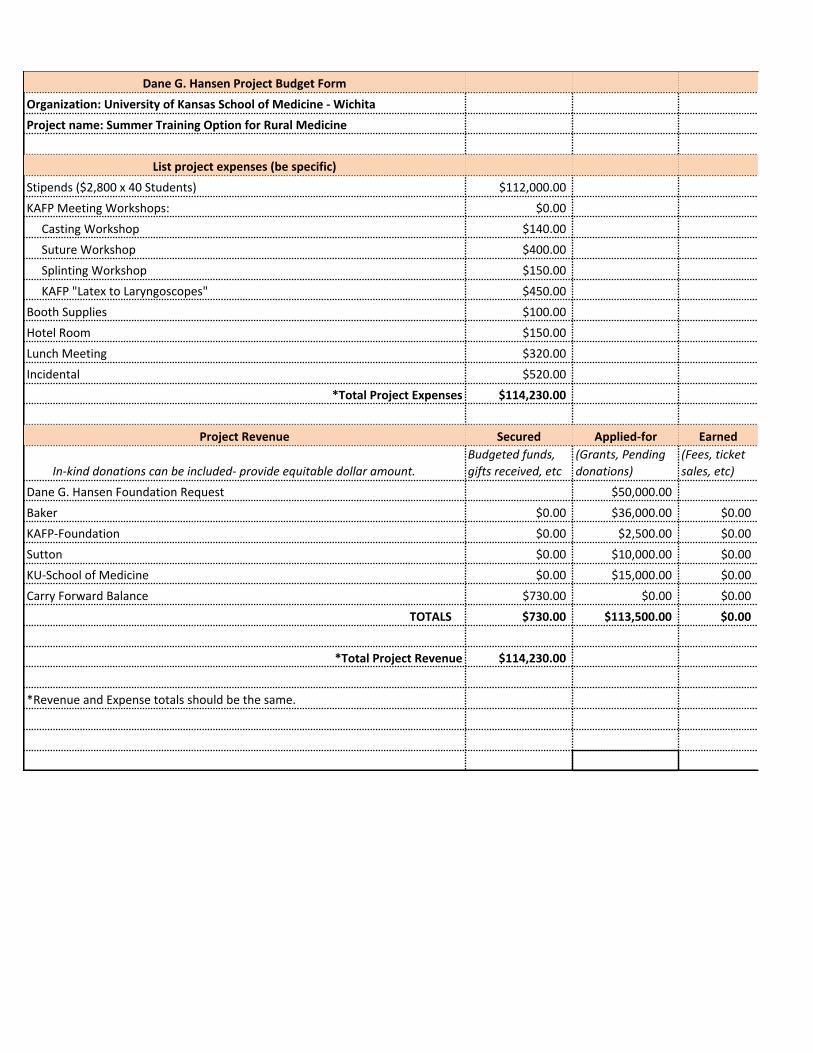
Dane G. Hansen Project Budget FormOrganization: University of Kansas School of Medicine - WichitaProject name: Summer Training Option for Rural Medicine
List project expenses (be specific)Stipends ($2,800 x 40 Students) $112,000.00KAFP Meeting Workshops: $0.00 Casting Workshop $140.00 Suture Workshop $400.00 Splinting Workshop $150.00 KAFP "Latex to Laryngoscopes" $450.00Booth Supplies $100.00Hotel Room $150.00Lunch Meeting $320.00Incidental $520.00
*Total Project Expenses $114,230.00
Project Revenue Secured Applied-for Earned
In-kind donations can be included- provide equitable dollar amount. Budgeted funds,gifts received, etc
(Grants, Pendingdonations)
(Fees, ticketsales, etc)
Dane G. Hansen Foundation Request $50,000.00Baker $0.00 $36,000.00 $0.00KAFP-Foundation $0.00 $2,500.00 $0.00Sutton $0.00 $10,000.00 $0.00KU-School of Medicine $0.00 $15,000.00 $0.00Carry Forward Balance $730.00 $0.00 $0.00
TOTALS $730.00 $113,500.00 $0.00
*Total Project Revenue $114,230.00
*Revenue and Expense totals should be the same.


As of
05/31/17
As of
05/31/16Assets
Statement of Financial PositionKansas University Endowment Association
734,820.668,040,687.29Cash and cash equivalentsReceivables
45,862.0883,728.40 Receivables from investment activities91,167.2122,797.70 Other receivables
21,977,287.8821,973,008.57 Student loans receivable, less allowance for uncollectible loans79,843,635.0063,456,710.00 Contributions pledged, less allowance for uncollectible pledges
8,458,142.028,681,102.63 Real estate loans receivable
Total receivables 94,217,347.30 110,416,094.19
Investments
1,574,232,645.441,684,478,148.77 Securities43,509,355.4142,077,569.56 Trusts held by others
3,693,840.203,516,295.99 Interest in other KU Endowment Entities13,491,570.2513,199,169.08 Real estate
1,634,927,411.301,743,271,183.40Total investments
Property and facilitites on or adjacent to University campus
13,900,521.4613,700,240.46 Land26,157,884.4626,014,750.47 Buildings
3,803,737.023,074,038.43 Equipment and furnishings
43,862,142.9442,789,029.36
(13,173,344.54)(13,631,688.05)Less accumulated depreciation
Net property and facilities on or adjacent to the University campus 29,157,341.31 30,688,798.40
5,952,118.846,554,975.33Deposits and other assets
1,782,719,243.391,881,241,534.63Total Assets
Liabilities and Net Assets
Liabilities
11,544,083.0020,132,651.34 Accounts payable and accrued expenses27,895.9326,647.57 Payables from investment activities
804,672.96868,587.68 Trust payable19,197,326.3824,442,383.91 Life income payables
66,608,650.1569,259,549.32 Agency funds
98,182,628.42114,729,819.82Total liabilities
Net assets
197,557,355.89177,420,382.66 Unrestricted1,045,419,347.941,139,413,501.16 Temporarily restricted
441,559,911.15449,677,830.99 Permanently restricted
1,684,536,614.98Total net assets 1,766,511,714.81
11:11:5407/13/2017
1,782,719,243.401,881,241,534.63Total Liabilities and Net Assets
FS_Stmt_Finan_Pos_Audit_1yr

Unrestricted RestrictedTemporarily
Revenues, gains (losses) and other support: RestrictedPermanently Total
Current Year Prior YearTotal
Statement of Activities - AuditFiscal Year through 05/31/20172017
Page: 1
Fundraising:(494,813.46) 98,948,215.77 4,190,974.33 106,449,124.09102,644,376.64 Contributions and grants received and pledged
794,092.07 7,304,399.22 4,365,222.38 16,478,717.1712,463,713.67 Bequests1,044,488.14 32,298.50 270,012.411,076,786.64 Life income gifts
(45,029.31) 188,204.94 35,890.14 992,350.23179,065.77 Change in value of life income gifts(88,723.84) Change in net interest in other KU Endowment Entities
Total fundraising 254,249.30 107,485,308.07 8,624,385.35 116,363,942.72 124,101,480.06
Income from asset holdings3,318,929.79 9,155,098.40 17,834,803.5112,474,028.19 Investment income
31,104,572.92 107,629,326.09 (32,446,568.25)138,733,899.01 Realized and unrealized gains (losses) on investments and trusts held by others612,003.32 872,644.63 1,153,974.961,484,647.95 Loan interest income304,161.87 385,736.86 647,316.19689,898.73 Agricultural and mineral income
(1,442,301.30) 349,283.38 1,182,613.73(1,093,017.92) Rental, gain (loss) on sale of assets and other income
Total income (losses) from asset holdings 33,897,366.60 118,392,089.36 152,289,455.96 (11,627,859.86)
340,499.59 3,574,026.73 2,179,954.773,914,526.32Other Receipts
Net assets released from restrictions:169,346,353.07 (169,346,353.07) Satisfaction of program restrictions
Total revenues, gains and other support 203,838,468.56 60,105,071.09 8,624,385.35 272,567,925.00 114,653,574.97
16:46:5707/12/2017Run Date: Stmt_Activities_Audit_2Report ID:
Unrestricted RestrictedTemporarily
Expenses: RestrictedPermanently Total
Current Year Prior YearTotal
Statement of Activities - AuditFiscal Year through 05/31/20172017
Page: 2
University support:29,005,598.52 27,582,785.3629,005,598.52 Student support35,186,814.91 29,745,828.0935,186,814.91 Faculty support and contractual services61,288,510.28 55,653,685.0561,288,510.28 Construction, furnishings, equipment, and supplies47,561,440.23 40,098,822.7147,561,440.23 Program and other educational support
Total University support 173,042,363.94 173,042,363.94 153,081,121.21
Supporting services
18,688,126.61 18,368,555.3218,688,126.61 Administrative and fundraising support642,583.78 866,256.59642,583.78 Asset management expense
1,103,845.97 1,159,350.791,103,845.97 Depreciation
Total supporting services 20,434,556.36 20,434,556.36 20,394,162.70
Total Expenses 193,476,920.30 193,476,920.30 173,475,283.91
Excess (deficiency) of revenues over expenses 60,105,071.0910,361,548.26 8,624,385.35 79,091,004.70 (58,821,708.94)
1,792,840.94 (3,398,651.94) 1,605,811.00Net interfund transfers
12,154,389.20 79,091,004.70 (58,821,708.94)56,706,419.15 10,230,196.35Change in net assets before amortization of pension adjustments
Change in net assets (58,821,708.94)79,091,004.7012,154,389.20 56,706,419.15 10,230,196.35
165,265,993.46 1,082,707,082.01 439,447,634.64 1,743,358,323.921,687,420,710.11Net assets at beginning of year
*
*Academic Unit
Account Type
*
Net assets at end of year 177,420,382.66 1,684,536,614.981,766,511,714.811,139,413,501.16 449,677,830.99
Campus Location

Executive Committee of the Board of Trustees
Deanell Reece Tacha, Chair Dean, School of Law Pepperdine University Malibu, California Current Term: 2017-2018 Initial Appointment: 2003 John B. Dicus Chairman, President & CEO Capitol Federal Savings Topeka, Kansas Current Term: 2014-2018 Initial Appointment: 2014 David B. Dillon, Vice Chair Chairman of the Board—Retired The Kroger Company Kansas City, Missouri Current Term: 2014-2018 Initial Appointment: 2014 William R. Docking Chairman & CEO The Union State Bank Arkansas City, Kansas Current Term: 2014-2018 Initial Appointment: 2000 A. Drue Jennings, Immediate Past Chair Senior Counsel--Retired Polsinelli Shughart, PC Leawood, Kansas Current Term: 2017-2018 Initial Appointment: 2003
M. D. Michaelis Chairman of the Board Emprise Financial Corporation Wichita, Kansas Current Term: 2016-2020 Initial Appointment: 2003 Linda Ellis Sims Mgr., US 3rd Party Basestock Sales—Retired ExxonMobil Corporation Independence, Missouri Current Term: 2014-2018 Initial Appointment: 2010 Steve Sloan President and CEO Midwest Minerals, Inc. Pittsburg, Kansas Current Term: 2014-2018 Initial Appointment: 2014 Todd L. Sutherland President The University National Bank Lawrence, Kansas Current Term: 2015-2019 Initial Appointment: 2005 Robert D. Taylor Chairman Emeritus & Founder—Retired Executive AirShare Corporation Mission Hills, Kansas Current Term: 2014-2018 Initial Appointment: 2010 Kurt D. Watson President & COO IMA Financial Group, Inc. Andover, Kansas Current Term: 2014-2018 Initial Appointment: 1994
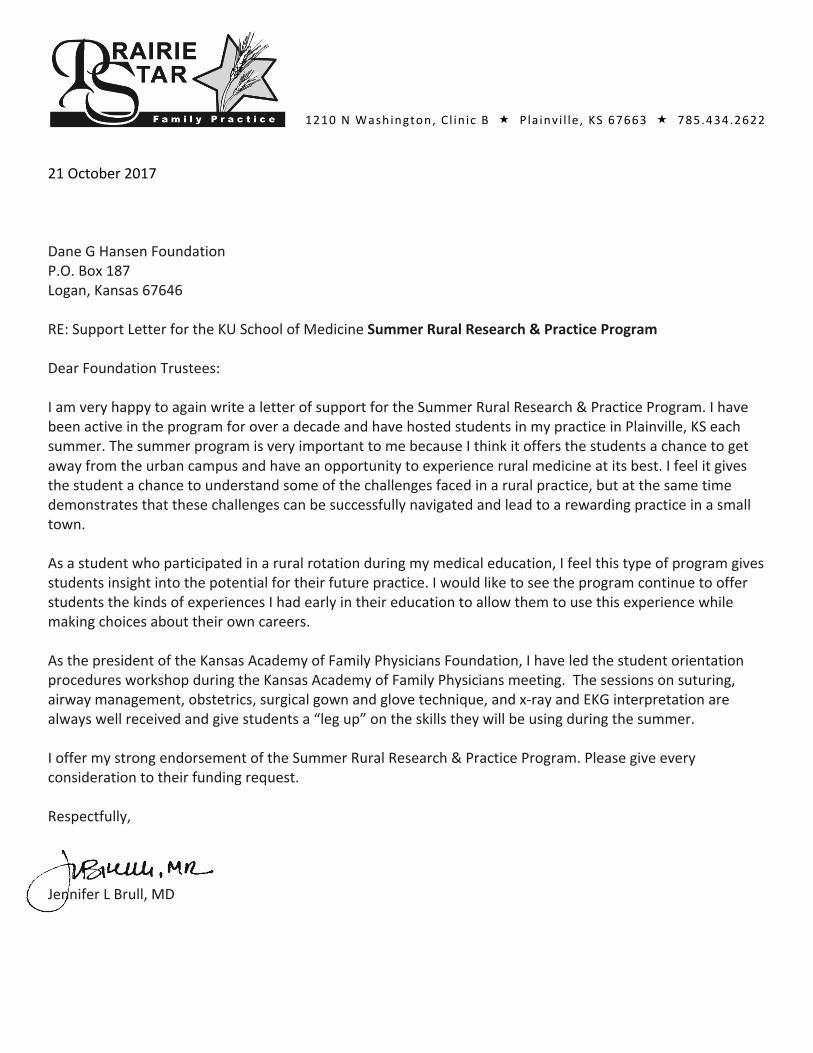
1210NWashington, C l in ic B « P la invi l le , KS 67663 « 785.434.2622
21October2017DaneGHansenFoundationP.O.Box187Logan,Kansas67646RE:SupportLetterfortheKUSchoolofMedicineSummerRuralResearch&PracticeProgramDearFoundationTrustees:IamveryhappytoagainwritealetterofsupportfortheSummerRuralResearch&PracticeProgram.IhavebeenactiveintheprogramforoveradecadeandhavehostedstudentsinmypracticeinPlainville,KSeachsummer.ThesummerprogramisveryimportanttomebecauseIthinkitoffersthestudentsachancetogetawayfromtheurbancampusandhaveanopportunitytoexperienceruralmedicineatitsbest.Ifeelitgivesthestudentachancetounderstandsomeofthechallengesfacedinaruralpractice,butatthesametimedemonstratesthatthesechallengescanbesuccessfullynavigatedandleadtoarewardingpracticeinasmalltown.Asastudentwhoparticipatedinaruralrotationduringmymedicaleducation,Ifeelthistypeofprogramgivesstudentsinsightintothepotentialfortheirfuturepractice.IwouldliketoseetheprogramcontinuetoofferstudentsthekindsofexperiencesIhadearlyintheireducationtoallowthemtousethisexperiencewhilemakingchoicesabouttheirowncareers.AsthepresidentoftheKansasAcademyofFamilyPhysiciansFoundation,IhaveledthestudentorientationproceduresworkshopduringtheKansasAcademyofFamilyPhysiciansmeeting.Thesessionsonsuturing,airwaymanagement,obstetrics,surgicalgownandglovetechnique,andx-rayandEKGinterpretationarealwayswellreceivedandgivestudentsa“legup”ontheskillstheywillbeusingduringthesummer.IoffermystrongendorsementoftheSummerRuralResearch&PracticeProgram.Pleasegiveeveryconsiderationtotheirfundingrequest.Respectfully,JenniferLBrull,MD


Dane G Hansen Foundation P.O. Box 1B7 Logan, Kansas 67646 785·689-4832 RE: Support letter for the KU School of Medici ne Summer Rural Research & Practice Program Dear Foundation Trustees: This is to serve as a letter of support for the Summer Rural Research & Practice Program. As Associate Dean of Clinical Sciences on the KUSoM Salina Campus and Associate Director of the Smoky Hill Family Medicine Residency Program, I am very invested in our mission to provide excellent physicians for rural Kansas. This program is one of the key instruments in achieving this mission. I have been active in the program a number of years, hosting and helping in placement of participating students in Salina and the surrounding areas. The summer program offers the students a chance to get away from the urban campus and have an opportunity to experience rural medicine at its best. While the Salina campus typically attracts students with an interest in rural practice, there are a great number of medical students on the other campuses who share this interest and need opportunities for further exploration. This program offers students a chance to understand some of the challenges faced in a rural practice, but at the same time demonstrates that these challenges can be successfully navigated and lead to a rewarding practice in a small town. As a family physician and a member of the leadership team at the KUSoM Salina, I have a somewhat unique perspective in the full spectrum of experience for the program. Students are eager to seek out clinical experiences after their first year of medical school. I would like to see the program continue to offer students the kinds of experiences that allow them to make more informed choices about their own careers. Therefore, I offer my strongest endorsement of the Summer Rural Research & Practice Program. Respectfully, C. Scott Owings, MD Associate Dean, KU School of Medicine - Salina Associate Director, Smoky Hill Family Medicine Residency Program
8-19 >20
Summer student placements in Dane Hansen Counties 1992-2017
KUMC
4
7Number 10 2 3 4 5 6
12 7
2
228
63
3 11
6
7 18
12
5
2
9
14 6
210
CheyenneWashington MarshallRepublic
Cloud
Ottawa
Saline
McPherson
Harvey
Sedgwick
Sumner
Jewell
Mitchell
Lincoln
Ellsworth
Rice
Reno
Kingman
HarperBarber
Pratt
Stafford
Barton
Russell
Osborne
SmithPhillips
Comanche
Kiowa
Edwards
Pawnee
Rush
Ellis
Rooks
Norton
Graham
Trego
Ness
Hodgeman
Ford
ClarkMeade
Gray
Lane
Gove
Sheridan
DecaturRawlins
Thomas
Logan
Scott
Finney
Haskell
SewardStevens
Grant
Kearny
Wichita
Sherman
Wallace
Greeley
Hamilton
Stanton
MortonCowley
ChautauquaMont-gomery
Labette Cherokee
CrawfordNeoshoWilson
Woodson Allen Bourbon
Nemaha Brown
Doniphan
AtchisonJackson
Pottawatomie
Shawnee
Jefferson Leaven-worth Wyandotte
JohnsonDouglas
MiamiFranklin
Osage
Coffey
Lyon
Anderson Linn
Greenwood
Chase
Morris
Wabaunsee
Butler
Marion
Geary
RileyClay
Dickinson
Elk
Kansas City Area
Liberal
Dodge City
Hutchinson
Manhattan
Junction City
Emporia
Garden City
Wichita
Hays Salina
McPherson
Topeka
Pittsburg
Lawrence
Newton
Colby

0
5
10
15
20
25
30
35
40
45
50
Number of Summer Rural Research and Practice Students

From the day I arrived she had me going to see patients by myself, jumping in on procedures, and helping around the clinic. I was very fortunate that Dr. Brown was especially interested in OB because it allowed me to take part in 3 deliveries over the summer (two of which were C-sections). Until this summer, I had never experienced a birth. The first baby we delivered was birthed via C-section. It was my first time scrubbing into surgery along with being my first birth, so I was extremely nervous. Dr. Brown and Dr. Walz, the other doctor in town, did most of the procedure but I got to help cut sutures and hold the baby for a second before she was swooped up by the nurses. I will always remember the birth of that little girl. She was extremely cute. I also got to do a ton of suturing this summer both at the clinic and in the E.R. I repaired lacerations, took punch biopsies, and cut out potential skin cancers, all of which required suturing. I also got to inject a couple knees with steroids and give some immunizations to babies. Although I had a lot of fun while in St. Francis, I also experienced the more sobering side of medicine. During my stay, I got called on a coroner call with Dr. Walz. We went out in the country and met the sheriff where we encountered a man who lived alone in his early 60’s who had died the night before while watching TV. It was eerie to see the man still sitting in his messy trailer with the TV still on, but it was our job to inspect him for signs of foul-play. Overall, I had a great experience in St. Francis and I would highly encourage other students to shadow Dr. Brown.
Andrew Hatfield
I was not sure what to expect from the Rural Health Elective when I started 6 weeks ago. In reflection on my experience in Concordia, I cannot imagine a better way to spend my summer break. It gave me the opportunity to participate in unique and exciting clinical care, greatly improve my clinical skills, and understand what the professional and personal life is like for a physician. The ability to devote my time solely to clinical care without worrying about a grade made it unique and rewarding for me, and in addition I got to experience what makes rural medicine special. I really valued the bond formed with the patients, the extra time you get to focus on an individual's needs, and the spectrum of patient care provided in rural Kansas these past 6 weeks.
As examples of the many memorable patients from this summer, two people stand out. We will call them Mr. Blue and Mr. June. Mr. Blue had been losing weight and not eating well for some time. He reported feeling a blockage in the esophagus to where he could not eat much and was very discouraged and distressed. We did an EGD and found no blockage, but instead an incredibly irritated stomach - the worst my preceptor had ever seen. My preceptor told me privately after the EGD that he was not sure Mr. Blue would make it out of the hospital alive as he also had heart failure in addition to his failure to thrive. Nevertheless, we reassured Mr. Blue there was no blockage and started the slow work of treating his gastritis, getting him back to eating and coping with his heart failure. He ended up eventually staying for about 3 weeks, including the hospital and “swing bed” stays (the use of rural hospital beds as “swing beds” was a new concept for me). I was overjoyed when I got to see him leave the hospital to go home with his wife, having gained weight and strength. The transformation in him that occurred with me as a witness truly hit on what a great physician can do through medication, reassurance, and good care. Seeing the whole health care team of MD, OT, PT, nursing, and nutrition truly turn

around this case was very encouraging for me as to what we can do for someone who comes in suffering. Mr. June came into the Emergency Department early one morning after he woke up with his air mattress deflated and lying on the floor. Due to Spina Bifida, he had no feeling below his ribs and both his legs had been amputated below the hip. I was warned about his sacral and ischial wounds before I went in, but nothing could have prepared me for the severity of his wounds. Although he had no feeling in the area, the wounds were so bad that laying directly on the floor woke him up and prompted him to come in. He had 3 wounds with each at least the size of a baseball and obviously severely infected. We could not see the depth of one, with another being so deep that you had to push the tissue back a great deal to get to see the bottom of the wound. He said the home health aide who bathed him the day before had not mentioned that anything was wrong to him. He was transferred to Wichita and I have not heard since how he is doing. However, I was told at the time of the transfer that he was not expected to live due to the severity of the infected wounds. It was disheartening to see how much the health care system can fail, especially when it is mainly due to poverty and a rural location. If people do not get the health care that they need early on, the system cannot always compensate later and solve the issue. It was a stark reminder of why preventative and primary care can play such a big role in health and wellness, even though they can be overlooked by some as important.
Concordia afforded me so many opportunities this summer and I am beyond grateful. Outside of the hospital, I went to softball games, a dirt racetrack, many firework displays, a patient’s home to get cross stitch tips, museums, local restaurants, and much more. It truly cemented for me that rural medicine is about individuals, the community, and medicine intertwining and that all three together make rural practice the special experience that it is.
Hannah Swagerty
Having lived in a larger city my entire life, I have to admit that I was a little nervous to be spending 6 weeks in a town with a population of less than 1,500. As I reflect on my time spent here, I can honestly say that this experience solidified my desire to become a family medicine physician. I have shadowed many different physicians in different states and countries, but none of them provided me with the hands-on training that I was able to experience throughout this summer.
Every person I encountered in Oberlin, from the hospital staff, healthcare professionals, administrative leaders, patients, to the general community, welcomed me into their town and made me feel comfortable. I attended a community-wide meeting with over 150 community members where I was able to learn about the different grant opportunities and how the community wanted to distribute the funds to make the largest impact. It was great to watch an entire community come together to discuss how they can make their community a better place.
An 86 year old man was brought into the hospital after his wife found him unconscious in their shed. When he arrived, he had a body temperature of 108.9°F. He was groaning in pain, but was not responsive. He lied there naked as we worked to cool him down, using Ziploc bags filled with ice cubes, because there was a lack of resources and a cooling blanket was not available.
Although we were able to get his temperature down to normal, his body had become stiff as a rock and he was not neurologically intact. His wife, son, and daughter sat there and cried while holding his hand and rubbing his head, waiting for even the smallest response. Although we did everything we could do for him, the nurse practitioner and physician assistant decided that we did not have the appropriate resources to do anything else and he had to be transferred elsewhere to an ICU. We contacted the flight crew and called surrounding hospitals to see where we could send him and after being turned down by three other facilities, we were finally able to get an acceptance to Wichita, which would be another 45min to an hour in transportation time. The flight crew came and intubated him and we were finally able to get him transferred.
All weekend this patient and his family were on my mind. I could not sleep that night because I was going through everything in my head about what we did and what we could have done differently. When I came back to the clinic on Monday, I was devastated to learn that the patient had passed away. I was able to talk with the providers who reassured me that we all did everything we could possibly do with the resources we had and that his body temperature was too high for too long of a period and that he was likely brain dead before even getting to the emergency department. This entire situation was very difficult for me to handle because I was essentially watching the family witness their loved one dying in front of their eyes and there was nothing anyone could do to save his life. Although devastating, I was able to learn first-hand some of the challenges that rural communities face: lack of resources, increased waiting time for care (due to transportation issues), and compromised patient care. However, this experience also taught me the level of compassion that can be seen in such a small town. All of the health professionals here have close relationships with their patients and their families and they truly work as hard as they can to provide the best care possible with whatever resources they have. In an emergency situation, they worked very well together and made sure to keep the family both informed and comfortable every step of the way. After the patient had passed over the weekend, the family came into the clinic and the providers provided emotional support to them, which I’ve never seen elsewhere.
As stated earlier, this summer confirmed my desire to work as a family medicine physician in a rural or underserved community. Emergency medicine was emotional for me and I realized that it is not a field that I want to go into. With family medicine, I can focus on preventive care and I hope to have the same type of relationship with my patients that these health providers have with theirs. They provide a comfortable, non-judgmental, safe space where the patients can address their health concerns. In being here for six weeks, I was able to see some patients multiple times and I enjoy the continuity of care. Having the ability to do small outpatient procedures in family practice like: incising and draining cysts, suturing wounds, removing toenails, etc. helps keep things exciting.
Vanessa Amandariz

This summer was an invaluable experience with so many great stories that I could probably write an entire book about it. However, to simplify my “Quinterssential” summer to fit on one page, I will focus on 3 common aspects of medicine: the good, the bad, and the ugly. The Good: Personal relationships are everywhere in small towns, and everywhere in family medicine. I was amazed at how quickly I was immersed and welcomed into the community. An office administrator invited me to ride her husband’s combine during wheat harvest, a nurse invited me to church, the Gove County Advocate put a column on me in their newspaper, community members invited us to little league games, Dr. Doug and Dr. Shelly regularly invited us over for dinner, Dr. Machen took me to the Buffalo Bill statue on the way to a deposition in Oakley, and I went with a fellow medical student to explore Quinter’s best attractions, Castle Rock and Ray’s Pharmacy’s chocolate malts. I loved that I received as much feedback on my work from patients as I did from the physicians. Quinter made me feel like I was a valued member of their community, which isn’t always the case for young medical students elsewhere. I am now able to imagine myself as a family med doc in a peaceful, rural community, which is leaps and bounds from where I started never having even been to a town so small before! The Bad: The world isn’t perfect, and neither is medicine. This summer I got to experience the great joy of being called into the ER at 3am for patients who had things like an ingrown toe nail and really didn’t need to be there that late at night. I also got to talk to drug seeking patients, and patients on drugs – all new experiences for me. We removed staples from a man’s head who was being charged with murder. However, the memory that will always stick with me from this summer will be the delivery of one of my favorite patient’s first child. After trying to push for almost 3 hours, even with the help of a kiwi, the baby would not budge, so an emergency C-section had to be called. I was relieved that the mother would be able to relax and perhaps lessen her pain. However, I hadn’t seen how scary an operation could be yet. The patient was laying on the table crying like she was still feeling quite a bit of pain, which was more distracting than I ever thought it could be. Due to the long labor, the baby was wedged down and stuck in the birth canal. We had to push up on the head and pull back on the shoulders with all our might to deliver this baby, which then was blue with an APGAR of one and a misshapen head. The baby came out with such force that it caused her intestines to bulge out of the incision too, and the long labor had caused her uterus to become extremely boggy. It was in that moment that I really understood the true scope of rural medicine – there were no specialists to call in. Dr. Doug was the only person in an hour’s radius any direction that could keep them alive. Dr. Machen was on a fishing trip, and I found out in that moment that Dr. Shelly had left for Seattle as one of their best medical school friends had just committed suicide. It was overwhelming. I was awed by Dr. Doug’s ability to find a calm focus and just work, and soon the mother was all stitched back up and the baby was crying in its bassinet. All was well, and I pray that will always be the case. The Ugly: Not everything is as expected. On my first day working in Quinter, Dr. Machen handed me a blue croquet ball asking me what it was. He followed this up by handing me a pamphlet with an article titled “A Novel Use of a Vacuum Extractor,” and chuckled, “welcome to family medicine.” Little did I know, the ball I was currently holding was previously vacuum extracted from a patient’s rectum! As shocking as this was, I could only admire Dr. Machen’s ingenuity in sparing this patient a visit to the OR. Later in the summer, I was able to witness one of the most disgusting moments of his long career, and surprisingly it was not the appointment with a chief complaint of “bug in ear.” We were unsuspectingly removing a large lipoma from a patient’s back when it suddenly exploded upon first contact with the scalpel, spewing a foul

smelling, cheesy, white substance all over our faces, hair, scrubs, and even the ceiling of the procedure room! It was actually a sebaceous cyst, and the patient then remembered that he used to be able to “squeeze stuff out of it.” There was nothing to do except just laugh at each other and our current predicament as we finished sewing up the patient. There was never a dull day this summer. Even with these ups and downs, I would sign up to do this program time and time again. While I’m studying for Step 1 this year, I know I will be able to motivate myself by looking back and remembering what I’m working toward at the end of all of these years of schooling
Katherine Sensenich
There’s a certain level of anxiety associated with any large transition in life. As I was packing my bags to leave for Quinter, I was battling my feelings of fear and apprehension because I knew the experience I would get this summer would be unlike any other. These feelings quickly dissipated just a couple hours into my first day at the office. In just the morning, I was able to perform a punch biopsy, practice some suturing, and see an IUD insertion. I thought for sure these would be the highlight of the day, but soon I learned otherwise. One of Dr. Shelly’s patients went into labor, and I had the distinct honor of watching the delivery Monday night, just a mere twenty-four hours after I arrived. The experiences I had my first day were all new and exciting, and considering it was just my first day, I knew I had my work cut out for me.
The next five weeks were some of the best experiences of my life. Between clinic visits, ER shifts, vaginal deliveries, surgeries, procedures, and C-sections, I learned more than I could have ever predicted. I learned how to drive a scope in both a colonoscopy and an EGD. I delivered three babies myself. I scrubbed in on multiple C-sections and walked away, hands dirty, and face grinning with the beauty of new life. I saw children and even did follow-ups on babies I had delivered myself. I saw women and men who were ninety-eight years and above. I saw every scope of life and every kind of emergency, big or small. More than anything, I learned that being a doctor extends far beyond the patients you see in clinic. Being a doctor in a small town means you’re a role model, an authority figure, a friend, and most importantly, someone your patients depend on. Being a doctor in a small town is as rewarding and life-changing as I could have ever imagined.
In summary, the six weeks I spent in Quinter changed me in so many positive ways. They inspired me to keep trekking along in medical school, comforted by the knowledge that someday I would get to do what I truly loved. It reminded me that being a physician is not a job, but a life-calling. It encouraged me to face my fears and dare myself to step outside my comfort zone. It taught me more medicine than I could have ever imagined, and the hands-on-experience I gained will follow me for the rest of my life. As I pack my bags to head back, I consider the student I was before and after this experience. As I say goodbye to the community I fell in love with, I remember why medicine is the practice I have devoted my life to. And that memento is the most important and rewarding of all.
Emily Lenherr

The STORM program allowed me to grow as a person and as a physician. It was a great reminder and an inspiration to dedicate myself to my preclinical studies so I will feel more knowledgeable in my later years. Seeing how fast decisions had to be made or all the “calculations” involved with providing the best medicine possible reminded me that I had signed up for a life of learning. Dr. Atkins was with me every step of the way with watching how I interacted with patients in clinic or in the ER, providing me with a Pharmacology book so I could understand the different types of medications patients were receiving, explaining some of the burdens of reimbursement and asking me to stop and think about some of the experiences I had.
While there I lost my first patient as a Student Doctor. He was an older man with end stage cancer and I went with Dr. Atkins to see him for a few days without asking why he was in the hospital. We made a deal with him that if he did PT on Friday that we would bring him a cupcake. He did and when Dr. Atkins and I returned on Monday he was displaying Cheyne-Stokes breathing pattern. His wife found out that we had brought him that cupcake and showed a lot of gratitude. A patient I had come so close with was dying the next time I saw him and by the time a return for lunch he was gone. Dr. Atkins expressed to me that it is always the little things in life that make the most difference in people’s lives and this is a lesson I will carry forward with me the rest of my career.
Another eventful day in Hill City began with a Code Blue of a 40 year old women. We attempted everything we could but after an hour there was nothing left we could do. Dr. Atkins broke the news to the family and we let them come see their loved one who had just passed. I never really thought about the fact that as future physicians, being around death will be second nature to us and each person has their own way of dealing with that. The issue comes with being the person that shares these experiences with the family of your patients. In my eyes death in old age is usually a great thing to experience; but when you pass away earlier in you life there were some many experiences planned and left undone that it can really take a toll on those around you.
Terrance Mabry


















