Summary (pediatric oral pathology)
107
ORAL PATHOLOGY ONLINE CONFERENCE Third year dental students Supervised by Dr.Dalal ALQahtani [email protected] College of Dentistry King Saud University SUMMARY
-
Upload
oralpathconf -
Category
Health & Medicine
-
view
574 -
download
4
Transcript of Summary (pediatric oral pathology)

ORAL PATHOLOGY
ONLINE
CONFERENCE Third year dental students
Supervised by Dr.Dalal ALQahtani
College of Dentistry
King Saud University
SUMMARY

TOPIC NAME:
PEDIATRIC ORAL PATHOLOGY
DONE BY:
Riham AlBusayes
Reem AlRabiah
Mariam AlShamali,
Maha AlJarboua
Amani AlMohaimeed

DONE BY XMIND 2013

DEVELOPMENTAL
• ORO-FACIAL CLEFTS
• PALATAL CYST OF THE
NEWBORN
• CONGENITAL EPULIS
• NATAL/NEONATAL TEETH
• ANKYLOGLOSSIA
• CONGENITAL ABSENCE OF
TEETH

ORO-FACIAL CLEFTS

ORO-FACIAL
CLEFTS• Orofacial clefts are birth defects where
the lip, palate or both may be involved.
• A cleft is a separation in a body
structure, often resulting from the
failure of tissues to grow together
properly.
• Cleft lip and cleft palate are the single
most common congenital deformity
affecting the orofacial structures and
constitute about 13% of all reported
anomalies.

• Cleft lip and cleft palate can occur
unilateral or bilateral. Because the lip
and the palate develop separately, it is
possible to have a cleft lip without a cleft
palate, a cleft palate without a cleft lip, or
both together.

ETIOLOGY
it’s multi-factorial, many factors may be involved:
• Genetics.
• Environmental factors; alcohol consumption,
• Smoking, hypoxia during pregnancy, dietary
and vitamins deficiencies (like folic acid and
vitamin A deficiency)
• Drugs: corticosteroids (anti-inflammatory),
phenytoin (anti-convulsant).
• Infections during pregnancy.
• Maternal age.

• Problems with
feeding can occur
with orofacial clefts
which requires
treatment.
So, How can we treat orofacial
clefts?

TREATMENT
• Surgery
• Obturator
PALATAL CYST OF THE NEWBORN
(EPSTEIN’S PEARLS; BOHN’S
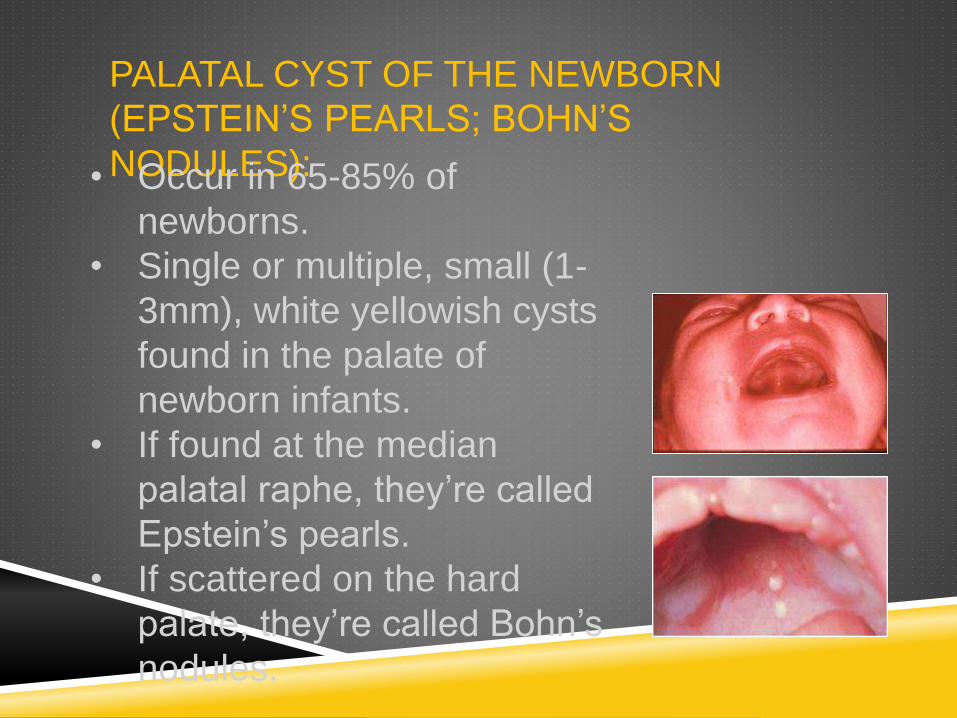
NODULES):• Occur in 65-85% of
newborns.
• Single or multiple, small (1-
3mm), white yellowish cysts
found in the palate of
newborn infants.
• If found at the median
palatal raphe, they’re called
Epstein’s pearls.
• If scattered on the hard
palate, they’re called Bohn’s
nodules.

PATHOGENESIS
• Researches have theorized that these
cysts may arise in one of two ways:
• First, epithelial entrapment at the midline
during the formation of secondary
palate. (Epistein’s pearls)
• Second, arise from epithelial remnants
derived from the development of the
minor salivary glands of the palate.
(Bohn’s nodules)

TREATMENT
• No treatment is required, as they’re
going to disappear several weeks after
birth.

CONGINITAL EPULIS
Clinical features:
• A soft tissue tumor
that occurs almost
exclusively on the
alveolar ridge of
newborns.
• Pink to red, smooth-
surfaced mass.
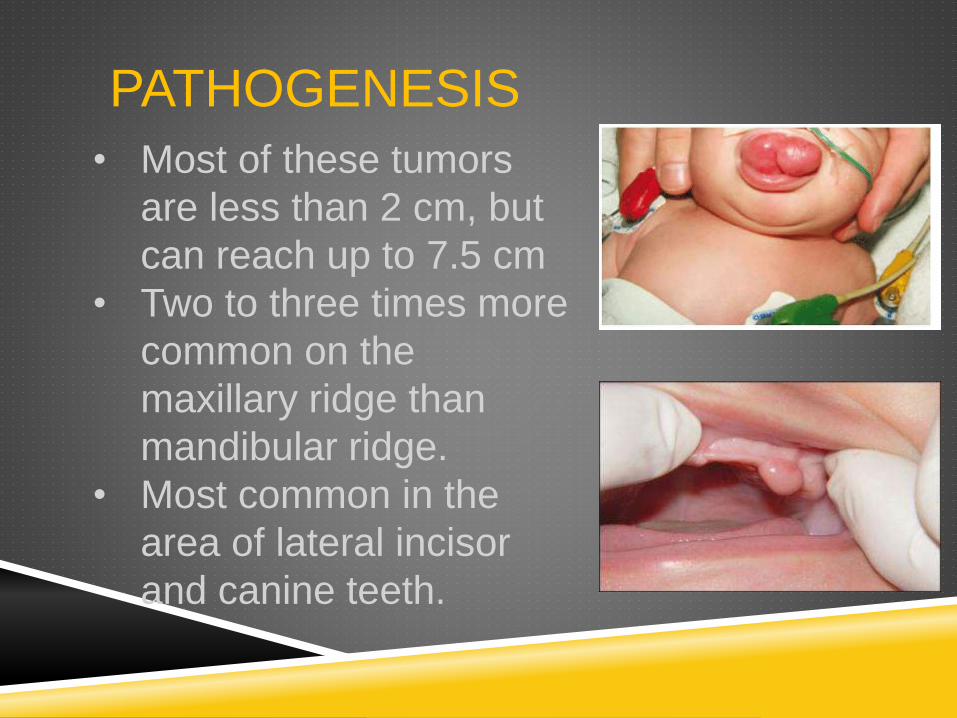
PATHOGENESIS
• Most of these tumors
are less than 2 cm, but
can reach up to 7.5 cm
• Two to three times more
common on the
maxillary ridge than
mandibular ridge.
• Most common in the
area of lateral incisor
and canine teeth.

• Shows a striking predilection for females
(90% of the cases), which suggest a
hormonal influence in its development.

HISTOPATHOLOGY:
• The overlying
epithelium shows
atrophy of rete
ridges
• Large-rounded
cells with granular
cytoplasm

TREATMENT:
• Surgical excision.
• Will not recur, even with incomplete
removal.
• In some patients, complete regression of
the tumor without treatment.

NATAL/NEONATAL
TEETH:• Natal teeth are teeth that are present at
birth.
• Neonatal teeth are teeth that emerge
through the gingiva during the first
month of life.
• Most common site:
mandibular central incisors area
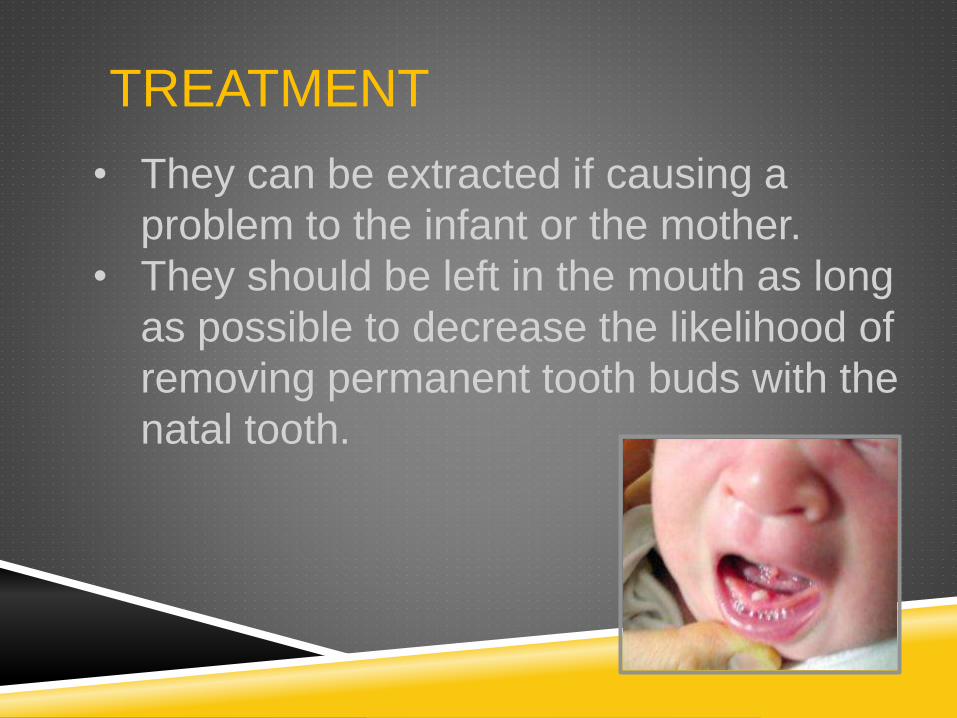
TREATMENT
• They can be extracted if causing a
problem to the infant or the mother.
• They should be left in the mouth as long
as possible to decrease the likelihood of
removing permanent tooth buds with the
natal tooth.

Tongue-tie (Ankyloglossia)
Most of us think of tongue-tie as a situation we find ourselves in when
we are too excited to speak. Actually, tongue-tie is the non-medical
term for a
relatively common physical condition that limits the use of the tongue,
ankyloglossia.
THE
ETIOLOGY
Before we are born, a strong cord of tissue that guides development of
mouth structures is positioned in the center of the mouth. It is called a
frenulum.
After birth, the lingual frenulum continues to guide the position of
incoming teeth. As we grow, it recedes and thins. This frenulum is
visible and easily felt if you look in the mirror under your tongue. In
some children, the frenulum is especially tight or fails to recede and may
cause tongue mobility problems.
WHEN IS TONGUE-
TIE A PROBLEM
THAT NEEDS
TREATMENT?In Infants
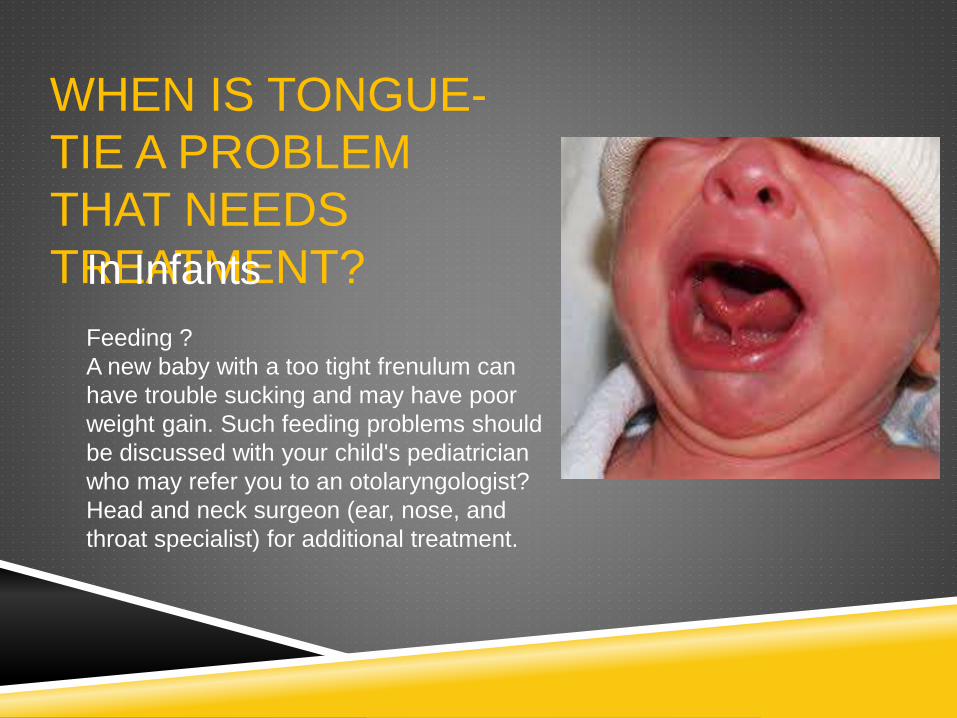
Feeding ?
A new baby with a too tight frenulum can
have trouble sucking and may have poor
weight gain. Such feeding problems should
be discussed with your child's pediatrician
who may refer you to an otolaryngologist?
Head and neck surgeon (ear, nose, and
throat specialist) for additional treatment.

In Toddlers and
Older ChildrenSpeech ?
While the tongue is remarkably able to compensate and
many children have no speech impediments due to tongue-
tie, others may. Around the age of three, speech problems,
especially articulation of the sounds - l, r, t, d, n, th, sh, and z
may be noticeable. Evaluation may be needed if more than
half of a three year old child's speech is not understood
outside of the family circle.
Although, there is no obvious way to tell in infancy which
children with ankyloglossia will have speech difficulties later,
the following associated characteristics are common:
• V-shaped notch at the tip of the tongue
• Inability to stick out the tongue past the upper gums
• Inability to touch the roof of the mouth
• Difficulty moving the tongue from side to side

As a simple test,
caregivers or parents might ask themselves if the child can lick
an ice cream cone or lollipop without much difficulty. If the
answer is no, they cannot, then it may be time to consult a
physician.
Appearance ?For older children with tongue-tie, appearance can
be affected by persistent dental problems such as a gap between
the bottom two front teeth. Your child's physician can guide you
in the diagnosis and treatment of tongue-tie. If he/she
recommends surgery, an otolaryngologist Head and neck
surgeon (ear, nose, and throat specialist), can perform a surgical
procedure called a frenulectomy.

CONGENITAL ABSENCE OF
TEETHCongenital absence of teeth is a
heritably phenomenon probably
most often passed to each
generation by an autosomal
dominant pattern with incomplete
penetrance and variable
expressivity. Correlation of
hypodontia with systemic
disease leads to the hypothesis
that this frequent dental anomaly
may in some cases be a
microform of systemic
ectodermal dysplasia.

In dentistry, hypodontia is the condition at which the patient
has missing teeth as a result of the failure of those teeth to
develop (also called tooth agenesis).
Hypodontia describes a situation where the patient is
missing up to five permanent teeth, excluding the 3rd molars.
Missing third molars occur in 9-30% of studied populations. In
primary dentition the maxilla is more affected, with the
condition usually involving the maxillary lateral incisor.
The condition of missing over 5 (six or more) permanent
teeth, excluding 3rd molars or wisdom teeth, has been called
oligodontia. The condition for missing all teeth, either primary
and/or permanent), is called anodontia. A similar condition is
hyperdontia, in which there are more than the usual number
of teeth, more commonly called as supernumerary teeth.
Many other terms to describe a reduction in number of teeth
appear in the literature: aplasia of teeth, congenitally missing
teeth, absence of teeth, agenesis of teeth and lack of teeth

(a) Developmental absence of the primary upper lateral
incisors in a 3-year-old child.
(b) Panoramic radiograph showing the absence of the
upper lateral incisors as well as of one lower

ODONTOGENIC :
• Parulis
• Eruption cyst

PARULIS :
• Parulis is the end of a draining fistulous
tract of a necrotic primary tooth.
• It is a soft , solitary, reddish papule
located apical and facial to
the abscessed tooth.
• Purulent drainage may be observe

PARULIS :
• Treatment is to extract the abscessed
tooth or preform root canal therapy

ERUPTION CYST :
1- Follicular enlargement appearing just
before the eruption of tooth.
2- Blue-black in color (may contain blood).

TREATMENT :
None unless infected, reassure the child
and parent, follicle will rupture, but may
need to surgically opened if infected.

REACTIVE
• Mucocele
• Chemical burn

MUCOCELE
• Mucocele is a benign
lesion characterized by
an extravasation or
retention of mucous in
submucosal tissue from
minor salivary glands.

MUCOCELE
• Mucoceles are known
to occur most
commonly on the lower
lip, followed by the floor
of mouth (Ranula) and
buccal mucosa being
the next most frequent
sites.

MUCOCELE
• Trauma and lip biting habits are the main
causes for these types of lesions.
• Mucocele is a common oral mucosal
lesion but it is rarely observed in the
infant.
• Clinically they are characterized by
single or multiple, spherical, fluctuant
nodules, ranging from normal pink to
deep blue in color, and are generally
asymptomatic.
HISTOPATHOLOGY

CHEMICAL BURN
• Aspirin & tetracyclin burn
• Caused by ingestion of household
chemicals by children
• Or by ingestion of dentifrices or
mouthwashes.
• Or iatrogenic burns, caused by acid etch
to tooth surface reaching the soft tissue.

CLINICAL FEATURES
• Thin, homogenous white film.
• Lateral pressure removes this white film
expose painful ulceraltion.

INFECTIONS
1- HIV infection
2- candidiasis
4-Primary Herpetic Gingivostomatitis
5- Scarlet fever

HIV INFECTION :1- Children most commonly acquire HIV infection during
pregnancy or at birth from an infected mother.
2- Blood products, transfusion, and breast milk are other
sources of pediatric HIV infection.
3- The fungal disease most commonly seen in children
with HIV is oral candidiasis
4-HIV gingivitis is characterized by a linear erythema of
the facial and interproximal gingival margins and is
unresponsive to improved oral hygiene
HIV INFECTION :
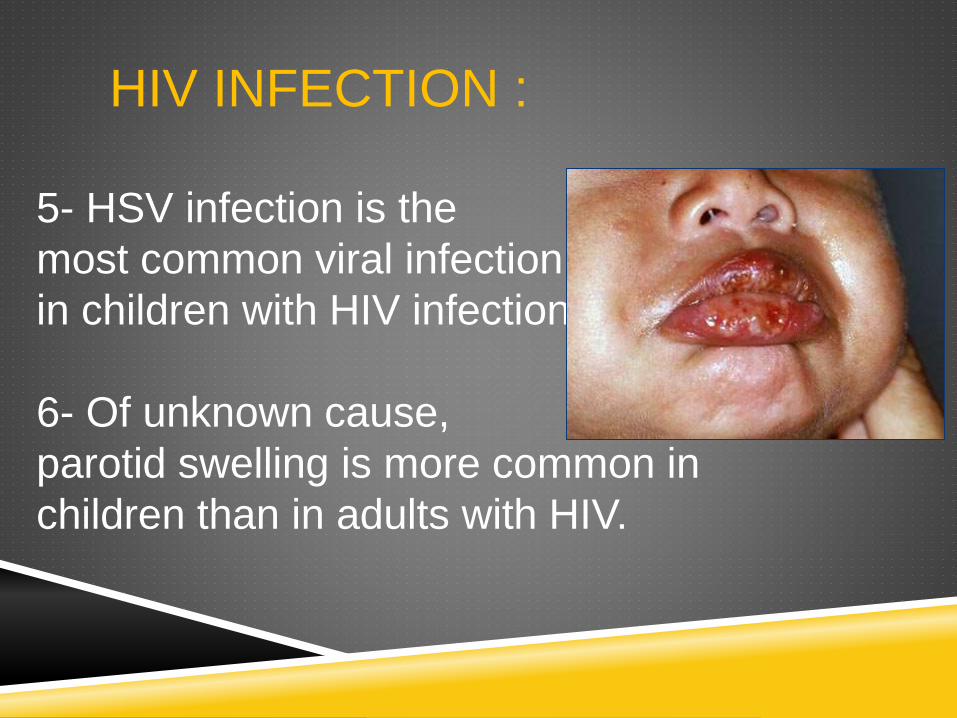
5- HSV infection is the
most common viral infection
in children with HIV infection.
6- Of unknown cause,
parotid swelling is more common in
children than in adults with HIV.
CANDIDIASIS :
1- Acute pseudomembranous candidiasis,
or.thrush, is the opportunis- tic overgrowth of the
fungus Cundidu ulbicuns.
2- candidiasis may be a sequelae of oral broad-
spectrum antibiotics or may reflect other systemic
alterations, such as immunode- ficiency.
3-Clinically, oral lesions are characterized by
creamy or curdy white plaques that can be wiped
off, leaving a red, raw, and painful surface. Any
mucosal surface in the oral cavity can be affected

CANDIDIASIS :

TREATMENT :
Topical or systemic antifungal agent usually
resolves the infection .

PRIMARY HERPETIC GINGIVOSTOMAT
ITIS1- The initial infection with herpes simplex virus
(HSV) occurs in young children after contact with
an infected child or adult.
2- The manifestations of primary herpetic
infection may be flulike symptoms or subclinical.
In primary gingivostomatitis, after an incubation
period of approximately 1 week, the patient
complains of fever, malaise, and irritability.

PRIMARY HERPETIC GINGIVOSTOMAT
ITIS3- Marginal gingivae become fiery red,
edematous, and may bleed easily. Clusters of
small vesicles erupt throughout the mouth, then
burst to form yellow vesicles surrounded by a red
halo.
4- The vesicles coalesce to form large ulcers of
the oral and perioral tissues. The lesions are
accompanied by pain, fever, arthralgia,
headache, and cervical lymphadenopathy.

SCARLET FEVER :
1- Most commonly affects children
2- Scarlet fever is usually spread by inhalation.
3- Most of the clinical features are caused by
erythrogenic toxin, a substance produced by the
bacterium Streptococcus pyogenes when it is
infected by a certain bacteriophage.
SCARLET FEVER :
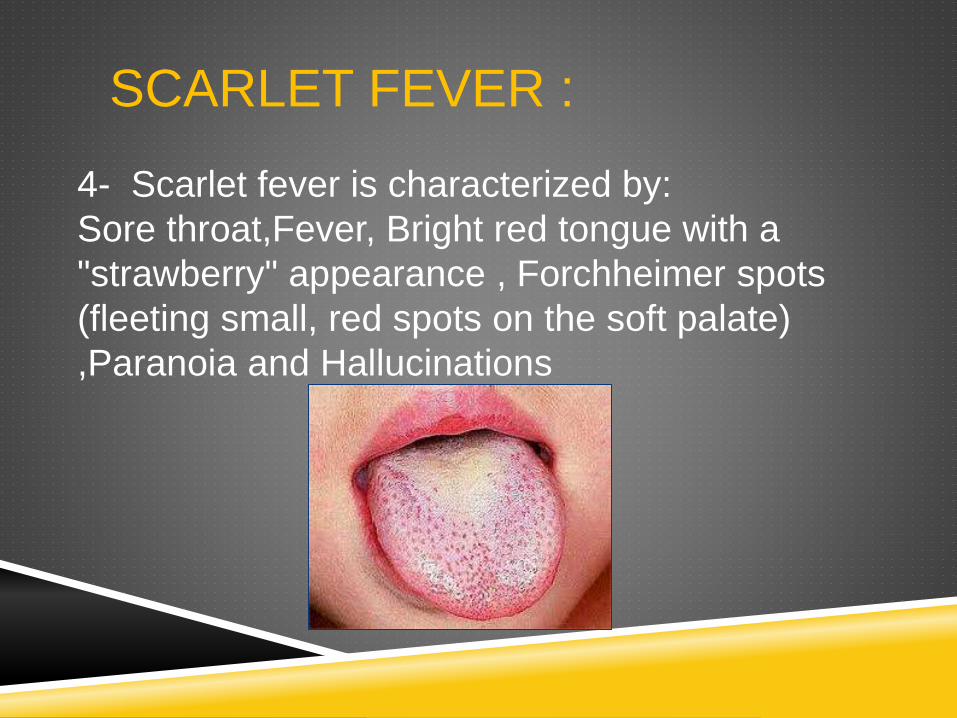
4- Scarlet fever is characterized by:
Sore throat,Fever, Bright red tongue with a
"strawberry" appearance , Forchheimer spots
(fleeting small, red spots on the soft palate)
,Paranoia and Hallucinations

TREATMENT :
There is no vaccine, but the disease is effectively
treated with antibiotics.
ULCERATIONS
• Recurrent apthous ulcer

RECURRENT APTHOUS
ULCER • The initial infection with herpes simplex
virus (HSV) occurs in young children after
contact with an infected child or adult.
• The manifestations of primary herpetic
infection may be flulike symptoms or
subclinical. In primary gingivostomatitis,
after an incubation period of approximately
1 week, the patient complains of fever,
malaise, and irritability.

BENIGNTUMORS
• Marginal gingivae become fiery red, edematous,
and may bleed easily. Clusters of small vesicles
erupt throughout the mouth, then burst to form
yellow vesicles surrounded by a red halo.
• The vesicles coalesce to form large ulcers of the
oral and perioral tissues. The lesions are
accompanied by pain, fever, arthralgia, headache,
and cervical lymphadenopathy.

BENIGNTUMORS
• HAEMANGIOMA
• LYMPHANGIOMA
• GIANT CELL FIBROMA
(RETROCUSPIC PAPILLA)

HAEMANGIOMA
• Infantile haemangiomas are benign
vascular neoplasms that have a
characteristic clinical course marked by
early proliferation and followed by
spontaneous involution.
• Haemangiomas are the most common
tumors of infancy and usually are
medically insignificant.

CLINICAL FEATURES:
• Bluish- red or purple colour.
• Homogeneous, sharp border, sessile
prominence.
• Spongy to palpation, blanching( +ve).
• Asymptomatic.

HAEMANGIOMA
MANAGEMENT
• Excisional biopsy, unless the lesion is
too large then injection of sclerosing
solutions or cryosurgery are preformed,
because biopsy to large hematomas
lead to haemorrhage.
LYMPHANGIOMA
• Lymphangiomas are uncommon congenital
hamartomas of the lymphatic system, usually
diagnosed in infancy and early childhood.
• Commonly located at head and neck, they are rarely
situated in the oral cavity.
• Preferred site of oral involvement is the tongue. In the
absence of proper therapy, lymphangiomas of the
tongue are extremely recurrent.

LYMPHANGIOMA
PATHOGENETIC
THEORIES:Three theories have been proposed to explain the origin
of this abnormality:
• The first suggests that a blockage or arrest of normal
growth of the primitive lymph channels occurs during
embryogenesis.
• The second that the primitive lymphatic sac does not
reach the venous system.
• While the third advances the hypothesis that, during
embryogenesis, lymphatic tissue lays in the wrong
area.

HISTOPATHOLOGY:
• Let’s watch this video to better understand the
histopathology for lymphangioma:
http://www.youtube.com/watch?v=x2-a2SyeI24

MANAGEMENT
• Surgical intervention represents the treatment of choice.
• Lesion extension and involvement of vital structures can
reduce, in some cases, the possibility of complete
resection.
• Sclerosing therapy should be considered for recurrences.
GIANT CELL FIBROMA
(RETROCUSPIC PAPILLA) • Asymptomatic sessile or pedunculated nodule
• Usually less than 1cm in size
• Occurs more in females than males.
• Occurs more in maxilla than mandible.
• Not associated with trauma (not reactive)
• 60% of lesion diagnosed during the first 3 decades of life.
• Occurs more in mandible than maxilla.
• 50% of cases occur in gingiva
• Can also occur on tongue and palate

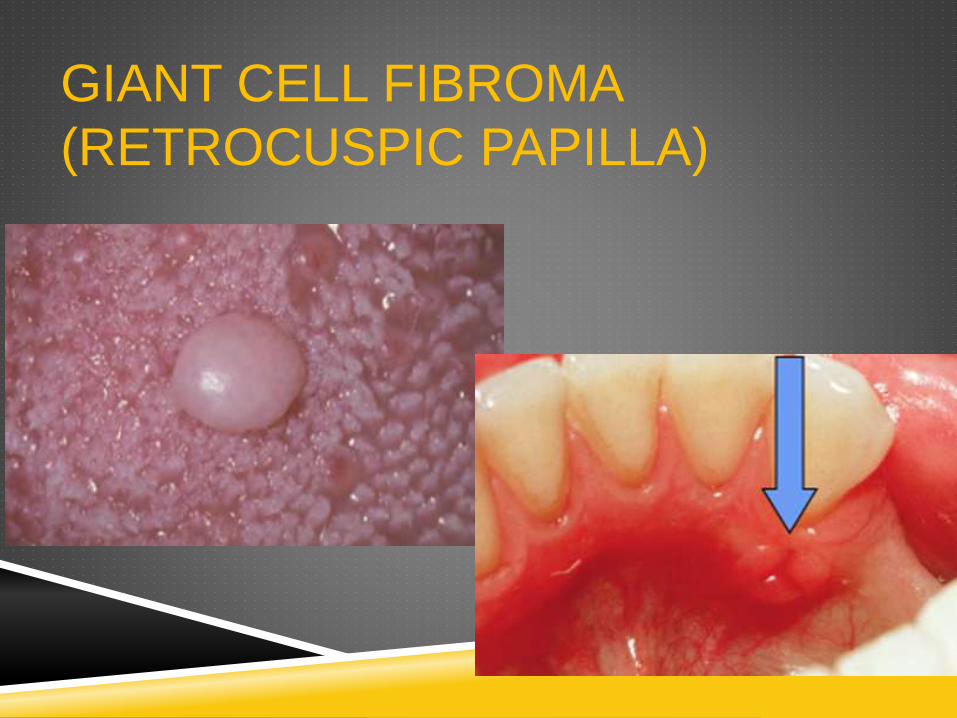
GIANT CELL FIBROMA
(RETROCUSPIC PAPILLA) • Retrocuspid papilla is a giant cell fibroma that occurs on
the gingiva lingual to mandibular cuspids (canines).
• It’s usually bilateral, small pink papule.
• Retrocuspid papilla are quite common, they have been
reported in 25% - 99% of children and young adults.
GIANT CELL FIBROMA
(RETROCUSPIC PAPILLA)

HISTOPATHOLOGY:
• Connective tissue mass with Pseudoepitheliumatous
hyperplasia
• Different giant cells; large stellate fibroblasts within the
connective tissue

HISTOPATHOLOGY:

MALIGNANT
TUMORS:• EMBRYONIC
RHABDOMYOSARCOMA
• MUCOEPIDERMOID CARCINOMA
EMBRYONIC
RHABDOMYOSARCOMA• Rhabdomyosarcoma (RMS) is an aggressive malignant
neoplasm of skeletal muscle origin that represents 50% of
all soft tissue sarcomas in childhood, with most cases
occurring in the head and neck 40%.
• Within the microscopical patterns, the embryonal type is
the most frequent in the oral cavity.

EMBRYONIC
RHABDOMYOSARCOMA
HISTOPATHOLOGY
• Embryonal RMS is characterized by a mixture of
pleomorphic and skeletal immature muscle cells, the so-
called rhabdomyoblasts.
• These cells have a distinctive eosinphilic-rich cytoplasm
and proliferate in a myxoid loose stroma.

HISTOPATHOLOGY

MANAGEMENT
• Overall 5-year survival rates have improved to more than
80% with the combined use of surgery, radiation therapy,
and chemotherapy.
• However, in patients with metastatic disease, little
progress has been made in survival rates, with a 5-year,
event-free survival rate of less than 30%

MUCOEPIDERMOID CARCINOMA
• Salivary gland tumors are rare in children but when they
involve the minor salivary glands, there is an increased
risk that they will be malignant, and it is the palatal region
that is the most common site.

CLINICAL PRESENTATION:
• The presentation of this malignancy is a painless,
persistent enlargement. When the major salivary
glandsand tongue are involved, pain, paresthesia, and
difficulty with swallowing are noted more frequently.
• Intraoral lesions appear as a localized fluctuant nodule
with a bluish or reddish-purple, smooth, mucosal surface.

CLINICAL PRESENTATION:

HISTOPATHOLOGY
• These tumors are determined to be low, intermediate and
high grade based on defined microscopic criteria, which
are correlated with prognosis.
• Most pediatric cases of mucoepidermoid carcinoma are
diagnosed as low or intermediate grade tumors.
• Consisting of multicystic spaces and duct-like structures
in a fibrous connective tissue. The cysts and small islands
are composed of mucous, intermediate and epidermoid
cells with evidence of mucus pooling.

HISTOPATHOLOGY

MANAGEMENT:
• Management of a low grade mucoepidermoid of the minor
salivary glands involves wide local excision with adequate
tumor-free margins.
• High grade tumors require more aggressive surgery with
or without postoperative radiotherapy and chemotherapy.
• Individuals with low grade tumors have a good prognosis
with greater than a 90% cure rate. In contrast, high grade
tumors have a poor prognosis with only a 20 to 30%
survival rate.

SYNDROMES
Down Syndrome.
Papillon-Lefevre Syndrome

DOWN SYNDROME
also known as trisomy 21, is a
genatic disorder caused by the
presence of all or part of a third copy
of chromosome 21. It is typically
associated with physical growth
delays, characteristic facial features,
and mild to moderate intellectual
disability.

• DENTAL MANIFESTATIONS IN DOWN SYNDROME:
. DELAYED ERUPTION OF BOTH PRIMARY AND PERMANENT DENTITIONS MICRODONTIAENAMEL HYPOCALCIFICIATION AND HYPOPLASIA COMMON 1/3 MORE CARIES RESISTANT THAN THEIR NON-DS SIBLINGS GINGIVITIS DEVELOPS EARLIER AND MORE RAPIDLY V-SHAPED PALATE, INCOMPLETE DEVELOPMENT OF THE MIDFACE COMPLEX, SOFT PALATE INSUFFICIENCYABSENT INCISORS MAKE ARTICULATION DIFFICULT SCALLOPED, FISSURED TONGUE WITH BIFID UVULA, CLEFT LIP/PALATE, ENLARGED TONSILS/ADENOIDSREDUCED SALIVARY FLOW HIGHER INCIDENCE OF BRUXISM, PARTICULARLY IN AGES 0-6 YEARS. BRUXISM TENDS TO DECREASE AFTER AGE SIX


DENTAL MANAGMENT
An aggressive preventive dental program is recommended for
patients with Down syndrome. The program should include:
Three to four month recalls: Consistent preventive care can help
reduce periodontal disease
Dietary counseling and encouragement of good oral hygiene:
Practical advice to minimize consumption of cariogenic foods
and the effects of such foods on tooth structure
Topical fluoride application: For caries prevention and/or
reduction of dentinal hypersensitivity
Chlorexidine gluconate 0.12% rinse: For reduction of bacteria that
cause periodontal disease

• PAPILLON-LEFEVRE SYNDROME :
also known as
palmoplantar keratoderma
with periodontitis, is an
autosomal recessive genetic
disorder caused by a
deficiency in cathepsin C

charecter of the syndrome:
1- hyperkeratosis of the palms and soles
2- premature loss of the primary and permanent dentitions
3- Hyperkeratotic lesions of the elbows and knees also may be found
4- Periodontal inflammation begins soon after the primary teeth erupt
5- Bone loss is severe, so that primary teeth are lost by 5 years of age (, permanent teeth also were lost within a few years of eruption)
MANAGMENT:
conventional therapy with oral hygiene instruction, professional
cleanings, frequent recalls, and antibiotics have failed to prevent
tooth loss.

TEETH ANOMALIES
1-Enamel hypoplasia
2-amelogensis imperfecta
3-dentinogenesis imperfecta
4-tetracyclin staining of teeth

ENAMEL HYPOPLASIA
Enamel hypoplasia is a defect of the teeth in
which the enamel is hard but thin and deficient
in amount,caused by defective enamel matrix
formation with a deficiency in the
cementing substance. Usually the condition
involves
part of the tooth having a pit in it. In some
cases, the natural enamel crown has a hole in
it, and in extreme cases, the tooth has no
enamel, which doesn't mean the tooth doesn't
exist
because dentin is also a component of teeth.

It can be caused by any of the following:
1-Trauma
2-Bacterial infection
3-Slow enamel formation
4-Celiac disease
CAUSES

Amelogenesis imperfecta (AI) presents with a rare abnormal
formation of the enamel or external layer of the crown of teeth.
Enamel is composed mostly of mineral, that is formed and regulated by
the proteins in it.
Amelogenesis imperfecta is due to the malfunction of the proteins in the
enamel: ameloblastin,
enamelin, tuftelin and amelogenin.
People afflicted with amelogenesis imperfecta have teeth with abnormal
color:
yellow, brown or grey; this disorder can afflict any number of teeth of both
dentitions.
The teeth have a higher risk for dental cavities and are hypersensitive to
temperature changes
as well as rapid attrition, excessive calculus deposition, and gingival
hyperplasia.
AMELOGENESIS IMPERFECTA

GENETICS
Mutations in the AMELX, ENAM,MMP20, KLK-4,FAM83H,
WDR72,
C4orf26, SLC24A4 LAMB3 and ITGB6 genes have been
found to
cause amelogenesis imperfecta (non-syndromic form).
About 5% of amelogenesis imperfecta cases are caused by
mutations in the AMELX gene and
are inherited in an X-linked pattern.
A condition is considered X-linked
if the mutated gene that causes the disorder is located on
the X chromosome, one of the two
sex chromosomes. In most cases, males
with an X-linked form
of this condition experience more severe
dental abnormalities than affected females.

TREATMENT
Preventive and restorative dental care is very important as
well as considerations
for esthetic issues since the crown are yellow from
exposure of dentin due to enamel loss.
Full-coverage crowns are sometimes being used to
compensate for the abraded enamel. Usually
stainless steel crowns are used in children which may be
replaced by porcelain once they
reach adulthood. In the worst-case scenario, the teeth may
have to be extracted and implants or
dentures are required.

DENTENOGENESIS IMPERFECTA
Dentinogenesis imperfecta is a disorder of tooth
development. This condition causes the teeth to be
discolored (most often a blue-gray or yellow-brown color)
and translucent. Teeth are also weaker than normal, making
them prone to rapid wear, breakage, and loss. These
problems can affect both primary (baby) teeth and
permanent teeth.

Type I: Type of dentinogenesis imperfecta with similar
dental abnormalities usually an autosomal dominant trait
with variable expressivity but can be recessive if the
associated osteogenesis imperfecta is of recessive type.]
Type II : Occurs in people without other inherited disorders
(i.e. Osteogenesis imperfecta). It is an autosomal dominant
trait. .
Type III: Type is rare; its predominant characteristic is bell-
shaped crowns, especially in the permanent dentition.
Unlike Types I and II, it involves teeth with shell-like
appearance and multiple pulp exposures
TYPE OF DI :

The objectives of early treatment of DI in the primary
dentition are as follows: 1. Maintain dental health and
preserve vitality, form, and size of the dentition. 2. Provide
the patient with an esthetic appearance at an early age, in
order to prevent psychological problems. 3. Provide the
patient with a functional dentition. 4. Prevent loss of
vertical dimension. 5. Maintain arch length. 6. Avoid
interfering with the eruption of the remaining permanent
teeth. 7. Allow normal growth of the facial bones and
temporomandibular joint (TMJ). 8. Establish a rapport with
the patient and the patient’s family early in the treatment.
TREATMENT :

TETRACYCLIN STAINING OF
TEETH Tetracycline can stain the teeth anywhere from a bright
yellow shade to dark brown. Usually the staining starts
out as a yellow color. Over time, as the tooth is exposed
to light, a chemical reaction occurs and the yellow turns to
a dark brown color.

DRUGS THAT CAUSE STAINING OF
TEETHMany of tetracycline’s homologues (similar drugs) are all
associated with discoloration. Chlortetracycline,
demethylchlortetracycline and oxytetracycline can all
cause brown/gray/yellow staining of the teeth.
Ciprofloxacin is an antibiotic that can be given
intravenously to infants for treatment of a Klebsiella
infection. It can stain the teeth a green color, but the
staining is usually more mild than tetracycline staining.
Minocycline hydrochloride is an antibiotic used to treat
acne and rheumatoid arthritis.

PREVENTION :
Tetracycline can cross the placental barrier and
incorporate into the developing tooth. It should be
avoided (if possible) by mothers who are pregnant and
also in kids until they are at least seven or eight years of
age.

TREATMENT OF TETRACYCLINE STAINED
TEETH :It is very difficult to treat internal staining of teeth because
it affects the dentin layer underneath the enamel.
CASE 1
• What is you diagnosis?
• How are you going to manage it?

CASE 2

CASE 2
• Excisional biopsy was
taken showing fibrous
c.t
• High power
magnification showing
which type of cells?

REFERENCES:https://pedclerk.sites.uchicago.edu/sites/pedclerk.uchicago.ed
u/files/uploads/1-s2.0-S0031395505702601-main.pdf
http://www.columbia.edu/itc/hs/dental/d7710/client_edit/Oral_P
athology.pdf
http://www.dentalcare.com/en-US/dental-education/continuing-
education/ce4/ce4.aspx?ModuleName=coursecontent&PartID
=2&SectionID=3
http://emedicine.medscape.com/article/909213-overview
-http://www.entnet.org/content/tongue-tie-ankyloglossia
http://jada.ada.org/content/96/2/266.long
http://ejo.oxfordjournals.org/content/27/5/443
http://en.wikipedia.org/wiki/Amelogenesis_imperfecta
http://en.wikipedia.org/wiki/Enamel_hypoplasia

REFERENCESPediatric Gastroenterology: A Color Handbook
http://emedicine.medscape.com/article/1083849-overview
http://www.rjme.ro/RJME/resources/files/470406373377.pdf
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2640069/
http://www.hindawi.com/journals/crid/2014/723130/
http://www.sciencedirect.com/science/article/pii/S1741940905000907
http://sarcomahelp.org/rhabdomyosarcoma.html
http://www.aapd.org/assets/1/25/Flaitz-22-04.pdf
http://www.hindawi.com/journals/crid/2012/370242/fig1/
Oral and maxillofacial pathology, 3rd edition, Neville