Sudden CardiacSudden Cardiac Deathukyce.cecentral.com/assets/1850/Presentation_TH...Jefferson Parish...
81
Sudden Cardiac Sudden Cardiac Sudden Cardiac Sudden Cardiac Death Death Michelle A. Grenier, MD Michelle A. Grenier, MD Associate in Pediatric Cardiology Associate in Pediatric Cardiology Texas Children’s Hospital Texas Children’s Hospital Financial Disclosures: None, but I do believe Prevention Financial Disclosures: None, but I do believe Prevention is a good thing. is a good thing. Unlabeled/Unapproved Uses Disclosures: None. Unlabeled/Unapproved Uses Disclosures: None.
Transcript of Sudden CardiacSudden Cardiac Deathukyce.cecentral.com/assets/1850/Presentation_TH...Jefferson Parish...
-
Sudden CardiacSudden CardiacSudden Cardiac Sudden Cardiac DeathDeath
Michelle A. Grenier, MDMichelle A. Grenier, MD,,Associate in Pediatric CardiologyAssociate in Pediatric Cardiology
Texas Children’s HospitalTexas Children’s HospitalFinancial Disclosures: None, but I do believe Prevention Financial Disclosures: None, but I do believe Prevention
is a good thing.is a good thing.Unlabeled/Unapproved Uses Disclosures: None.Unlabeled/Unapproved Uses Disclosures: None.
-
Athlete’s HeartAthlete’s HeartAthlete s HeartAthlete s Heart
•• HARVEY, La. HARVEY, La. ---- An autopsy An autopsy determined that LSU baseball determined that LSU baseball player player Wally PontiffWally Pontiff, found dead , found dead i hi h l ki hi h l kin his parents' home last week, in his parents' home last week, died of natural causes and no died of natural causes and no drugs were in his system, the drugs were in his system, the Jefferson Parish coroner saidJefferson Parish coroner saidJefferson Parish coroner said Jefferson Parish coroner said Monday. The autopsy found an Monday. The autopsy found an abnormality in the heartabnormality in the heart, which , which is still being tested so finalis still being tested so finalis still being tested, so final is still being tested, so final determination of exact cause of determination of exact cause of death may take several more days, death may take several more days, the coroner's report said.the coroner's report said.pp
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
Sudden cardiac death (SCD)Sudden cardiac death (SCD)Sudden cardiac death (SCD)Sudden cardiac death (SCD)Nontraumatic, nonviolent, Nontraumatic, nonviolent, unexpected event resulting fromunexpected event resulting fromunexpected event resulting from unexpected event resulting from sudden cardiac arrest within 6 sudden cardiac arrest within 6 hours of a previously witnessedhours of a previously witnessedhours of a previously witnessed hours of a previously witnessed state of normal health.state of normal health.
Maron BJ, Epstein SE, Roberts WC. JACC 1986;7:204-14
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
Warning signs during exerciseWarning signs during exercise–– PalpitationsPalpitationspp–– DizzinessDizziness–– Chest Pain/ Chest TightnessChest Pain/ Chest Tightness/ g/ g–– Shortness of BreathShortness of Breath–– SyncopeSyncopeSyncopeSyncopeIf there were warning signs, it may not be If there were warning signs, it may not be
“Sudden”“Sudden”
-
How frequently does it occur?How frequently does it occur?How frequently does it occur?How frequently does it occur?
l d h l ll d h l l•• Annual incidence in the general population Annual incidence in the general population 1/100,000 all comers1/100,000 all comers CDC, 2004, SenCDC, 2004, Sen--Chowdrhry, McKenna, Chowdrhry, McKenna, Cardiology 2006Cardiology 2006gygy
•• 2.3/100,000 athletes per year2.3/100,000 athletes per year Blangy, et al. Arch Mal Blangy, et al. Arch Mal Coeur Vaiss 2006Coeur Vaiss 2006
•• 4/100 000 hikers annually4/100 000 hikers annually B t h t l I t J S t M dB t h t l I t J S t M d•• 4/100,000 hikers annually4/100,000 hikers annually Burtscher, et al. Int J Sports Med Burtscher, et al. Int J Sports Med 20072007
•• Incidence higher in athletes 2.5:1 Incidence higher in athletes 2.5:1 Billes, et al. Eur J Billes, et al. Eur J C di P R h bil 2006C di P R h bil 2006Cardiovasc Prev Rehabil 2006Cardiovasc Prev Rehabil 2006
•• Incidence higher in males 9:1 Incidence higher in males 9:1 Billes et al. Eur J Cardiovasc Billes et al. Eur J Cardiovasc Prev Rehabil 2006Prev Rehabil 2006
-
More Numbers…Looking at Athletes More Numbers…Looking at Athletes ggunder 35 years of Ageunder 35 years of Age
•• >90% sudden death directly related to >90% sudden death directly related to cardiovascular causescardiovascular causes Bille, et al. Eur J Cardiovasc Prev Bille, et al. Eur J Cardiovasc Prev Rehabil 2006Rehabil 2006
•• 50% congenital anatomical/cardiomyopathy50% congenital anatomical/cardiomyopathy Bille, Bille, t l E J C di P R h bil 2006t l E J C di P R h bil 2006et al. Eur J Cardiovasc Prev Rehabil 2006et al. Eur J Cardiovasc Prev Rehabil 2006
•• 10% early atherosclerotic disease10% early atherosclerotic disease Bille, et al. Eur J Bille, et al. Eur J Cardiovasc Prev Rehabil 2006Cardiovasc Prev Rehabil 2006Cardiovasc Prev Rehabil 2006Cardiovasc Prev Rehabil 2006
•• 4% 164% 16--64 years no cause ID: arrhythmia? 64 years no cause ID: arrhythmia? SenSen--Chowdhry McKenna Cardiol 2006Chowdhry McKenna Cardiol 2006Chowdhry, McKenna Cardiol 2006Chowdhry, McKenna Cardiol 2006
-
The Invincible AdolescentThe Invincible AdolescentThe Invincible AdolescentThe Invincible Adolescent
•• 40% occurred in athletes
-
What is the relative cost of SCD?What is the relative cost of SCD?What is the relative cost of SCD?What is the relative cost of SCD?
•• “The term ‘sudden cardiac death’ (SCD) “The term ‘sudden cardiac death’ (SCD) implies the sudden and unexpected loss of implies the sudden and unexpected loss of a productive member of the community.” a productive member of the community.” Smith and Cain. J Interv Card Electrophysiol 2007Smith and Cain. J Interv Card Electrophysiol 2007
•• “The cost of SCD to society is incalcuable.” “The cost of SCD to society is incalcuable.” Smith and Cain. J Interv Card Electrophysiol 2007Smith and Cain. J Interv Card Electrophysiol 2007
If it i f il b it ff tIf it i f il b it ff t•• If it is your family member, it affects you If it is your family member, it affects you 100%.100%.
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
k f l f dd dk f l f dd dRisk profile for sudden cardiac Risk profile for sudden cardiac deathdeath
17 di17 di•• 17 years median age 17 years median age •• 90% male90% male•• 52% white, 44% black52% white, 44% black
68% l i f tb ll b k tb ll68% l i f tb ll b k tb ll•• 68% playing football or basketball68% playing football or basketball•• 90% collapsed during or shortly 90% collapsed during or shortly
after training session/competitive after training session/competitive eventeventeventevent
•• 85% cardiovascular cause85% cardiovascular cause
Maron BJ et al. JAMA 1996; 276: 199-204
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
Incidence of Sudden Cardiac Death by Sport
http://www.suddendeathathletes.org
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
Incidence of Sudden Cardiac Death by Month
http://www.suddendeathathletes.org
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
Incidence of Sudden Cardiac Death by Time of Day
http://www.suddendeathathletes.org
-
Sudden cardiac death in Sudden cardiac death in AthletesAthletesDistribution of cardiovascular causes of sudden death in 1435 young competitive athletes
Maron, B. J. et al. Circulation 2007;115:1643-1455
-
Athlete’s HeartAthlete’s HeartAthlete s HeartAthlete s Heart•• At age 18, just one At age 18, just one g , jg , j
month shy of his high month shy of his high school graduation, school graduation, Lil VicLil Vicwent into sudden cardiacwent into sudden cardiacwent into sudden cardiac went into sudden cardiac arrest while doing what arrest while doing what he loved best he loved best -- playing playing b k b ll db k b ll dbasketball. It turned out basketball. It turned out that Vic had that Vic had hypertrophic hypertrophic yp pyp pcardiomyopathy cardiomyopathy (HCM)(HCM) or an enlarged or an enlarged heart which had beenheart which had beenheart, which had been heart, which had been undetected. undetected.
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
Hypertrophic Cardiomyopathy
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Etiologies of SCDEtiologies of SCD–– Hypertrophic CardiomyopathyHypertrophic Cardiomyopathy
••Leading cause of sudden Leading cause of sudden ead g cause o suddeead g cause o suddecardiac death in young cardiac death in young athletesathletes
••Estimated prevalence of the Estimated prevalence of the disease 1:500 (not all high disease 1:500 (not all high risk) risk)
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• HypertrophicHypertrophic•• Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
Disorder caused byDisorder caused by––Disorder caused by Disorder caused by mutations of the cardiac mutations of the cardiac sarcomere unitsarcomere unitsarcomere unitsarcomere unit
––Autosomal dominant Autosomal dominant hhinheritanceinheritance
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Detection of HCMDetection of HCM–– HistoryHistory
••F il hi tF il hi t••Family historyFamily history––autosomal dominantautosomal dominant
••SymptomsSymptomsy py p––exertional dyspnea, orthopnea, exertional dyspnea, orthopnea,
fatigue: diastolic dysfunction fatigue: diastolic dysfunction ––chest pain: ischemiachest pain: ischemiachest pain: ischemiachest pain: ischemia
••ExamExam––murmur murmur (present in only 25%)(present in only 25%)
-
SCD In Young AthletesSCD In Young AthletesSCD In Young AthletesSCD In Young Athletes
Hypertrophic cardiomyopathyHypertrophic cardiomyopathy
No murmur on exam Possible murmur on exam
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
i f Ci f C•• Detection of HCMDetection of HCM–– MurmurMurmur
••SEM at the left lower to mid sternalSEM at the left lower to mid sternal••SEM at the left lower to mid sternal SEM at the left lower to mid sternal edge, radiates along the LVOTedge, radiates along the LVOT
••Harsh in quality, but may be vibratoryHarsh in quality, but may be vibratory••Increases with exercise Increases with exercise
––increased contractilityincreased contractilityI ith V l l t diI ith V l l t di••Increases with Valsalva, standing Increases with Valsalva, standing
––decreased volumedecreased volume
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Detection of HCM: Detection of HCM: Inherent difficultiesInherent difficulties–– Children may not yet show Children may not yet show
LVHLVHLVH tLVH t–– LVH may appear at any LVH may appear at any age, and change.age, and change.
–– It may not appear untilIt may not appear untilIt may not appear until It may not appear until adolescence, as the normal adolescence, as the normal LV remodeling process LV remodeling process appears to be most activeappears to be most activeappears to be most active appears to be most active thenthen
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Sudden Death in HCMSudden Death in HCM–– Lethal ventricular arrhythmiaLethal ventricular arrhythmia–– May be associated with extreme May be associated with extreme
physical exertion physical exertion M l b i it t d bM l b i it t d b–– May also be precipitated by May also be precipitated by volume depletion (dehydration).volume depletion (dehydration).
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Risk Factors for SCD in HCMRisk Factors for SCD in HCM–– Prior cardiac arrestPrior cardiac arrest–– Sustained or repetitive non sustained VT Sustained or repetitive non sustained VT –– Hypotensive BP response to exerciseHypotensive BP response to exercise
F il hi t f SCDF il hi t f SCD–– Family history of SCDFamily history of SCD–– Syncope (particularly exrtional)Syncope (particularly exrtional)–– Extreme LVH (>30mm)Extreme LVH (>30mm)Extreme LVH (>30mm)Extreme LVH (>30mm)
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
i f SC i Ci f SC i C•• Prevention of SCD in HCMPrevention of SCD in HCM–– Medications have not been Medications have not been
h t ff t th t ff t tshown to affect outcomeshown to affect outcome–– One study from Italy, where One study from Italy, where
th i ti id ith i ti id ithere is nationwide screening, there is nationwide screening, showed a diminished incidence showed a diminished incidence in SCD (ARVD), with exercisein SCD (ARVD), with exercisein SCD (ARVD), with exercise in SCD (ARVD), with exercise restrictionrestriction
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
•• Sudden Death in HCMSudden Death in HCML th l h t h th b litL th l h t h th b lit–– Lethal heart rhythm abnormalityLethal heart rhythm abnormality
–– Association with extreme physical Association with extreme physical exertionexertionexertion exertion
–– Autosomal Dominant/Spontaneous Autosomal Dominant/Spontaneous mutationsmutations
–– Warrants disqualification from Warrants disqualification from competitive sports competitive sports
-
HCM versus Athlete’s HeartHCM versus Athlete’s HeartHCM versus Athlete s HeartHCM versus Athlete s Heart
•• Pathologic descriptions of myocardial Pathologic descriptions of myocardial hypertrophy in trained individuals from hypertrophy in trained individuals from Ki h d Li b h i 1958Ki h d Li b h i 1958Kirch and Linzbach in 1958Kirch and Linzbach in 1958
•• The heart of the trained athlete can be The heart of the trained athlete can be t i th l i b t hi t l it i th l i b t hi t l itwice the normal size, but histologic twice the normal size, but histologic structure remains intactstructure remains intact
•• Th i ht f th t i d h t d tTh i ht f th t i d h t d t•• The weight of the trained heart does not The weight of the trained heart does not usually surpass the limit of 500g, defined usually surpass the limit of 500g, defined as the critical heart weightas the critical heart weightas the critical heart weightas the critical heart weight
-
Athlete’s HeartAthlete’s HeartAthlete s HeartAthlete s Heart•• Cardiac enlargement in athletes may Cardiac enlargement in athletes may
represent a physiologic phenomenon represent a physiologic phenomenon (controversial for many years)(controversial for many years)
•• Concerns about longConcerns about long--term consequences term consequences of morphologic left ventricular remodelingof morphologic left ventricular remodelingp g gp g g
•• Concern of sudden cardiac deaths in Concern of sudden cardiac deaths in athletes with hypertrophic cardiomyopathyathletes with hypertrophic cardiomyopathyathletes with hypertrophic cardiomyopathy athletes with hypertrophic cardiomyopathy (HCM) accounting for majority of (HCM) accounting for majority of catastrophescatastrophescatastrophescatastrophes
-
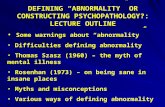
Ambiguity with HCMAmbiguity with HCMAmbiguity with HCMAmbiguity with HCM
Figure 1. Echocardiograms in parasternal long-axis view from an elite athlete (Olympic rower) (left) and a young asymptomatic patient with hypertrophic cardiomyopathy (HCM) (right). Magnitude of anterior ventricular septal (VS) hypertrophy is similar in each, demonstrating the morphological gray zone into which a highly trained athlete may fall and the diagnostic ambiguity that may ensue. Calibration dots are 1 cm apart. Leftdiagnostic ambiguity that may ensue. Calibration dots are 1 cm apart. Left panel is reprinted by permission of the New England Journal of Medicine(1991;324:295-301).
-
Differentiating from HCMDifferentiating from HCMDifferentiating from HCMDifferentiating from HCM•• LV cavity enlarged in athlete’s heartLV cavity enlarged in athlete’s heartLV cavity enlarged in athlete s heartLV cavity enlarged in athlete s heart•• Hypertrophy symmetric and homogenousHypertrophy symmetric and homogenous•• LV cavity maintains ellipsoid shapeLV cavity maintains ellipsoid shape•• LV cavity maintains ellipsoid shapeLV cavity maintains ellipsoid shape•• LV mass regresses with deconditioningLV mass regresses with deconditioning•• LV filling pattern remains normalLV filling pattern remains normal•• Acoustic pattern of myocardium remainsAcoustic pattern of myocardium remainsAcoustic pattern of myocardium remains Acoustic pattern of myocardium remains
normalnormal•• Restricted to certain sportsRestricted to certain sports•• Restricted to certain sportsRestricted to certain sports
-
Cardiac FunctionCardiac FunctionCardiac FunctionCardiac Function•• Echo exams on 286 cyclists in Tour de Echo exams on 286 cyclists in Tour de yy
France and 52 matched sedentary France and 52 matched sedentary volunteers volunteers
•• 148 in 1995 race, 138 in 1998 race, and 148 in 1995 race, 138 in 1998 race, and 37 in both37 in both37 in both37 in both
•• 51% had substantial LV enlargement 51% had substantial LV enlargement (LVIDd > 60mm up to 73mm)(LVIDd > 60mm up to 73mm)(LVIDd > 60mm, up to 73mm)(LVIDd > 60mm, up to 73mm)
•• 9% had increased LVWT (>13 mm)9% had increased LVWT (>13 mm)
-
A Heavy HeartA Heavy HeartA Heavy HeartA Heavy Heart
•• Left Ventricular Mass (PennLeft Ventricular Mass (Penn--cube formula)cube formula)
ControlsControls 174 g174 gEnduranceEndurance trainedtrained 249 g249 gEnduranceEndurance--trainedtrained 249 g249 gCombinedCombined 288 g288 gStrengthStrength--trainedtrained 267 g267 g
-
A Summary Table to ClarifyA Summary Table to ClarifyA Summary Table to Clarify A Summary Table to Clarify
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
Commotio cordisCommotio cordisCommotio cordisCommotio cordis••Direct, nonpenetrating Direct, nonpenetrating trauma to the chest wall trauma to the chest wall t au a to t e c est at au a to t e c est a––baseball, hockey puck, baseball, hockey puck, opponentopponent
O d i l i iO d i l i i••Occurs during repolarizationOccurs during repolarization––electrically vulnerableelectrically vulnerable
••10% survival10% survival••10% survival10% survival••Softer baseballs shown to Softer baseballs shown to reduce riskreduce riskreduce riskreduce risk
-
SCD In Young AthletesSCD In Young AthletesSCD In Young AthletesSCD In Young Athletes
Commotio Cordis (20%)Commotio Cordis (20%)
http://www.suddendeathathletes.org
-
SCD In Young AthletesSCD In Young AthletesSCD In Young AthletesSCD In Young Athletes
C ti C di V l bl i d iC ti C di V l bl i d iCommotio Cordis: Vulnerable microseconds in Commotio Cordis: Vulnerable microseconds in the cardiac cyclethe cardiac cycle
Ventricular Fibrillation
-
SCD in Young AthletesSCD in Young Athletesgg–– Long QT SyndromeLong QT Syndrome
C it l i d fC it l i d f••Congenital, acquired formsCongenital, acquired forms••Classically defined by:Classically defined by:
QT 440QT 440––QTc > 440 msecQTc > 440 msec––Bizarre T wave morphologyBizarre T wave morphologyT ltT lt––T wave alternansT wave alternans
––Predisposition to lethal cardiac Predisposition to lethal cardiac arrhythmias (arrhythmias (torsade de pointes)torsade de pointes)arrhythmias (arrhythmias (torsade de pointes)torsade de pointes)
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes•• Long QT syndrome and SCDLong QT syndrome and SCDg Q yg Q y
–– 287 patients287 patients••Mean age at death 6.8 +/Mean age at death 6.8 +/-- 5.6 yrs5.6 yrs
W i iW i i••Warning signs:Warning signs:––syncope (26%), seizures (10%), syncope (26%), seizures (10%),
cardiac arrest (9%) preceded bycardiac arrest (9%) preceded bycardiac arrest (9%) preceded by cardiac arrest (9%) preceded by emotion or exerciseemotion or exercise
••Family historyFamily history39% f Q S 3 % f SC39% f Q S 3 % f SC––39% positive for LQTS, 31% for SCD39% positive for LQTS, 31% for SCD
Garson et al. Circulation 1993; 87(6): 1866-72
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
•• Coronary Artery AnomaliesCoronary Artery Anomalies–– Second leading cause of SCDSecond leading cause of SCDSecond leading cause of SCDSecond leading cause of SCD–– Mechanism of sudden deathMechanism of sudden death
•• Abrupt lack of oxygen to the heart muscleAbrupt lack of oxygen to the heart muscle•• Heart rhythm abnormalityHeart rhythm abnormality
–– No known inheritance patternNo known inheritance pattern
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
Coronary Artery Abnormalities (14%)Coronary Artery Abnormalities (14%)
The right coronary artery arises from the right cusp, the left from the left cusp
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
Acute angle takeoff and course between the aortaAcute angle takeoff and course between the aorta and pulmonary artery. Both exacerbated by y
aortic root dilation with exercise.
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes•• Coronary ArteryCoronary ArteryCoronary Artery Coronary Artery
AnomaliesAnomalies••Second leading disease of the Second leading disease of the gg
heart resulting in SCDheart resulting in SCD••Mechanism of sudden death: Mechanism of sudden death:
lethal ventricular arrhythmialethal ventricular arrhythmialethal ventricular arrhythmialethal ventricular arrhythmia––sudden onset critical sudden onset critical
ischemiaischemiat i f tit i f ti––recurrent infarctionsrecurrent infarctions
––neurocardiogenic syncopeneurocardiogenic syncope
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Marfan SyndromeMarfan Syndrome–– Incidence of SCD 5Incidence of SCD 5--8/10008/1000–– Ruptured aortic aneurysmRuptured aortic aneurysm
Disproportionate representationDisproportionate representation–– Disproportionate representation Disproportionate representation among basketball & volleyball players among basketball & volleyball players (Flo Hyman)(Flo Hyman)
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
M f S dMarfan Syndrome
Long, spider-like fingers
Photos courtesy of Harold Chen, MD. Emedicine: Marfan Syndrome
Tall stature, long arms Hyperflexible joints
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes–– Marfan SyndromeMarfan Syndrome
A l d iA l d i••Autosomal dominantAutosomal dominant••Prevalence 1:10,000Prevalence 1:10,000••Defect in the fibrillin geneDefect in the fibrillin gene••Defect in the fibrillin geneDefect in the fibrillin gene••Tall habitus, arachnodactyly, Tall habitus, arachnodactyly,
pectus excavatum, high arched pectus excavatum, high arched p , gp , gpalate, pes planus, scoliosis, palate, pes planus, scoliosis, ectopia lentis, hyperextensibiliity, ectopia lentis, hyperextensibiliity, dilated aortic root, mitral valvedilated aortic root, mitral valvedilated aortic root, mitral valve dilated aortic root, mitral valve prolapseprolapse
••LoeysLoeys--Dietz: TGF b abnormalityDietz: TGF b abnormality
-
Sudden Cardiac DeathSudden Cardiac Death–– MyocarditisMyocarditis
••Viral infection of the heart muscleViral infection of the heart muscle••Heritable predispositionHeritable predisposition
–– Long QT syndromeLong QT syndrome••Abnormality of the electrical systemAbnormality of the electrical system••60% heritable (may be higher)60% heritable (may be higher)
A ti t iA ti t i–– Aortic stenosisAortic stenosis••Birth defect of the heart resulting in Birth defect of the heart resulting in
progressive obstruction of blood flow fromprogressive obstruction of blood flow fromprogressive obstruction of blood flow from progressive obstruction of blood flow from the heart to the bodythe heart to the body
••May be inherited 30May be inherited 30--50%, NODAL and 50%, NODAL and ay b d 30ay b d 30 50%, O a d50%, O a dNOTCH 1NOTCH 1
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
OC SOC S••MYOCARDITISMYOCARDITIS••1818--29% of childhood SCD29% of childhood SCDI fl ti di tI fl ti di t••Inflammation predisposes to Inflammation predisposes to arrhythmia up to months laterarrhythmia up to months later
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
•• Arrhythmogenic right ventricular Arrhythmogenic right ventricular cardiomyopathycardiomyopathy
••F tt i filt ti d fib i f th i htF tt i filt ti d fib i f th i ht••Fatty infiltration and fibrosis of the right Fatty infiltration and fibrosis of the right ventricleventricle
••Predisposed to exercisePredisposed to exercise--induced induced ppventricular arrhythmiasventricular arrhythmias
••Genetic basisGenetic basis
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes•• Conduction AbnormalitiesConduction Abnormalities•• Conduction AbnormalitiesConduction Abnormalities
••WolffWolff--ParkinsonParkinson--White syndromeWhite syndrome––Ventricular preVentricular pre--excitationexcitationVentricular preVentricular pre excitationexcitation––Supraventricular tachycardiaSupraventricular tachycardiaincidence same in athletes andincidence same in athletes andincidence same in athletes and incidence same in athletes and nonnon--athletesathletes
––Sudden deathSudden deathSudden deathSudden deathatrial fibrillation with rapid atrial fibrillation with rapid conduction along the bypass conduction along the bypass g ypg yptract (VF)tract (VF)
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes•• Miscellaneous Causes of SCDMiscellaneous Causes of SCDs a ous Caus s o SCs a ous Caus s o SC
–– Cocaine/OtherCocaine/OtherRx, Steroids, “Huffing”Rx, Steroids, “Huffing”, , g, , g–– Atherosclerotic coronary artery Atherosclerotic coronary artery
diseasedisease22 3% f SCD i thl t 403% f SCD i thl t 40••22--3% of SCD in athletes < 40 years3% of SCD in athletes < 40 years
••Is this on the rise?Is this on the rise?Ano e i ne o /b lemiAno e i ne o /b lemi–– Anorexia nervosa/bulemiaAnorexia nervosa/bulemia••electrolyte imbalances, conduction electrolyte imbalances, conduction abnormalitiesabnormalitiesabnormalitiesabnormalities
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes
How do we How do we costcost--effectivelyeffectivelycostcost effectively effectively
reduce the reduce the i id fi id fincidence of incidence of
sudden death sudden death sudde deatsudde deatin our athletes?in our athletes?
-
Primary PreventionPrimary PreventionPrimary Prevention Primary Prevention •• Do not let anyone Do not let anyone
participate inparticipate inparticipate in participate in sportssports
-
Primary PreventionPrimary PreventionPrimary PreventionPrimary Prevention
SS•• PrePre--participation Screeningparticipation Screening–– Padua, Italy:Padua, Italy: Nationwide systematic athletic Nationwide systematic athletic
screening implemented in 1982 (ages 12screening implemented in 1982 (ages 12 –– 3535screening implemented in 1982 (ages 12 screening implemented in 1982 (ages 12 35 35 years)years)
–– There was a There was a significant reductionsignificant reduction of SCD in of SCD in this population (0 56 vs 0 21)this population (0 56 vs 0 21)this population (0.56 vs. 0.21)this population (0.56 vs. 0.21)
–– The causes of SCD differ in Italy (ARVD, HCM)The causes of SCD differ in Italy (ARVD, HCM)–– Stringent disqualificationStringent disqualificationStringent disqualificationStringent disqualification–– The Lausanne RecommendationsThe Lausanne Recommendations
(International Olympic Committee)(International Olympic Committee)f d lf d l–– European Society of Cardiology Consensus European Society of Cardiology Consensus
StatementStatement
-
What is the US Consensus?What is the US Consensus?What is the US Consensus?What is the US Consensus?
•• 19961996, the , the American Heart Association American Heart Association consensus panelconsensus panel recommended prerecommended pre--participation cardiovascular screening for participation cardiovascular screening for young, competitive athletes based on young, competitive athletes based on “ethical, legal and medical grounds”.“ethical, legal and medical grounds”.
•• The Bethesda Conference The Bethesda Conference JACC 2005JACC 2005
-
Screening athletesScreening athletesScreening athletesScreening athletes
•• AHAAHA recommends “a complete and recommends “a complete and targeted personal and family history and targeted personal and family history and physical examination (including brachial physical examination (including brachial artery blood pressure measurement) artery blood pressure measurement) performed by performed by a qualified examinera qualified examiner and and include include 12 key AHA12 key AHA--recommended recommended elementselements as well as parental verification of as well as parental verification of medical history for high school and middle medical history for high school and middle school athletes”school athletes”
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes
•• The 12 Element AHA Recommendations The 12 Element AHA Recommendations for Preparticipation CV Screening of for Preparticipation CV Screening of C titi Athl t (2006C titi Athl t (2006 7)7)Competitive Athletes (2006Competitive Athletes (2006--7)7)
•• Medical HistoryMedical History•• Personal HistoryPersonal History
–– Exertional chest pain/DiscomfortExertional chest pain/Discomfort–– Unexplained Syncope/Near syncopeUnexplained Syncope/Near syncope–– Prior recognition of heart murmurPrior recognition of heart murmur
l d bl dl d bl d–– Elevated systemic blood pressureElevated systemic blood pressure
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes
–– Is there Family History?Is there Family History?•• Premature deathPremature death (sudden, and unexpected, or (sudden, and unexpected, or
otherwise) before age 50 years due to heartotherwise) before age 50 years due to heartotherwise) before age 50 years due to heart otherwise) before age 50 years due to heart disease, in > 1 relativedisease, in > 1 relative
•• Disability from heart diseaseDisability from heart disease in a close relative in a close relative < 50 years of age< 50 years of age< 50 years of age< 50 years of age
•• Specific knowledge of Specific knowledge of certain cardiac certain cardiac conditionsconditions in family members: hypertrophic or in family members: hypertrophic or d l d d h l dd l d d h l ddilated cardiomyopathy, long QT syndrome or dilated cardiomyopathy, long QT syndrome or other ion channelopathies, Marfan syndrome, or other ion channelopathies, Marfan syndrome, or clinically important arrhythmiasclinically important arrhythmias
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes•• Physical ExamPhysical Examyy
––Heart murmurHeart murmurF l l l d iF l l l d i––Femoral pulses to exclude aortic Femoral pulses to exclude aortic coarctationcoarctation
––Physical stigmata of Marfan Physical stigmata of Marfan syndromesyndromesyndromesyndrome
––Brachial artery blood pressure Brachial artery blood pressure (sitting position)(sitting position)
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes•• NBANBA requires echo and ECG on all requires echo and ECG on all qq
players on an annual basisplayers on an annual basis•• NFLNFL teams generally perform ECG’steams generally perform ECG’s•• NFL NFL teams generally perform ECG s teams generally perform ECG s
and obtain echos if clinically indicatedand obtain echos if clinically indicated•• US Olympic CommitteeUS Olympic Committee
administers preparticipation H & Padministers preparticipation H & Padministers preparticipation H & P administers preparticipation H & P and further noninvasive testing is and further noninvasive testing is performed only when warrantedperformed only when warrantedperformed only when warrantedperformed only when warranted
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes•• International Olympic Committee andInternational Olympic Committee andInternational Olympic Committee and International Olympic Committee and
European Society of CardiologyEuropean Society of Cardiologyrecommend ECG’s in all young competitiverecommend ECG’s in all young competitiverecommend ECG s in all young competitive recommend ECG s in all young competitive athletesathletes
•• AHA panelAHA panel does not believe it to be eitherdoes not believe it to be either•• AHA panelAHA panel does not believe it to be either does not believe it to be either prudent or practical to recommend the prudent or practical to recommend the routine use of tests such as 12routine use of tests such as 12--lead ECGlead ECGroutine use of tests such as 12routine use of tests such as 12 lead ECG lead ECG or echocardiography in the context of or echocardiography in the context of mass universal screeningmass universal screeningmass, universal screeningmass, universal screening
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes•• More than More than 5 million5 million competitive competitive pp
athletes in high schoolathletes in high school•• Greater thanGreater than 500 000500 000 collegiatecollegiate•• Greater than Greater than 500,000500,000 collegiate collegiate
athletes athletes •• Greater than Greater than 5,0005,000 professional professional
athletesathletesathletesathletes•• Population available for screening Population available for screening
may be as large asmay be as large as 10 million10 millionmay be as large as may be as large as 10 million10 million
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes•• ECGECG abnormal in > 90% HCMabnormal in > 90% HCM•• Detects ARVC, ion channelopathiesDetects ARVC, ion channelopathies
Mi h l i i l hiMi h l i i l hi•• Misses catecholaminergic polymorphic Misses catecholaminergic polymorphic ventricular tachycardiaventricular tachycardia
•• ECGECG has low specificity as a has low specificity as a screening test in athletic populationsscreening test in athletic populationsscreening test in athletic populationsscreening test in athletic populations
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes•• Concerns re: widespread use of Concerns re: widespread use of
i i t tii i t tinoninvasive testingnoninvasive testing––FalseFalse--positive test resultspositive test results
••unnecessary anxietyunnecessary anxiety••unjustified exclusion fromunjustified exclusion fromunjustified exclusion from unjustified exclusion from sportssports
••unjustified exclusion fromunjustified exclusion fromunjustified exclusion from unjustified exclusion from life insurance coveragelife insurance coverage
-
Screening AthletesScreening AthletesScreening AthletesScreening Athletes
Screening for SCDScreening for SCD8,000,0008,000,000 competitive sports participants competitive sports participants
in the U.S. (high school & college)in the U.S. (high school & college)
200,000200,000 estimated to be screened to estimated to be screened to detect 1000 at risk and 1 who would diedetect 1000 at risk and 1 who would diedetect 1000 at risk and 1 who would diedetect 1000 at risk and 1 who would die
-
SCD in Young AthletesSCD in Young AthletesSCD in Young AthletesSCD in Young Athletes•• Cost of NonCost of Non--Invasive ScreeningInvasive Screening
–– 6,000,000 high school athletes6,000,000 high school athletes••Screening exam $100Screening exam $100••ECG $70ECG $70••Echocardiogram $1500Echocardiogram $1500••Total cost / participant $1670Total cost / participant $1670
Total US health care cost Total US health care cost $10,020,000,000$10,020,000,000
-
Screening athletesScreening athletesScreening athletesScreening athletes•• Cost of NonCost of Non--Invasive ScreeningInvasive Screeninggg
–– 10 million high school athletes10 million high school athletes•• Screening exam $25Screening exam $25•• ECG $50ECG $50•• ECG $50ECG $50•• Echocardiogram $400Echocardiogram $400
Total US health care cost Total US health care cost $2 billion$2 billion to to prevent each preventable death.prevent each preventable death.p pp p
(Per suspected athlete (Per suspected athlete $330,000$330,000))
-
Normal Conduction Pathway Normal Conduction Pathway yyin the Heart and the ECGin the Heart and the ECG
Sinoatrial (SA) NodeSinoatrial (SA) NodeAtrioventricular (AV) Node
Left Bundle Branches
Right Bundle Branch
Purkinje Fibers
P = Atrial Depolarization
P T
QRS pQRS = Ventricular DepolarizationT = Ventricular Repolarization
QRS
-
Normal Sinus RhythmNormal Sinus RhythmNormal Sinus RhythmNormal Sinus Rhythm
Sinoatrial NodeSinoatrial NodeSinoatrial NodeSinoatrial Node
12:56 29MAR96 PADDLES X1.0 HR = 74
-
Ventricular TachycardiaVentricular TachycardiaVentricular TachycardiaVentricular Tachycardia
12:57 29MAR96 PADDLES X1.0 HR = 214
-
Ventricular FibrillationVentricular FibrillationVentricular FibrillationVentricular Fibrillation
12:57 29MAR96 PADDLES X1.0 HR = ---
-
Defibrillation: The OnlyDefibrillation: The OnlyDefibrillation: The Only Defibrillation: The Only Effective Treatment for Effective Treatment for
i l ib ill ii l ib ill iVentricular FibrillationVentricular Fibrillation
300 JOULES DEFIB 20:29 01APR96 PADDLES X1.0 HR = ---
-
AsystoleAsystoleAsystoleAsystole
15:17 29MAR96 PADDLES X1.0 HR = ---
-
LIFEPAK® 500
Automated External DefibrillatorsDefibrillators
-
How to DefibrillateHow to DefibrillateHow to DefibrillateHow to Defibrillate
•• Verify the victim is unconscious, not Verify the victim is unconscious, not breathingbreathingbreathing, breathing, without a pulse or signs of circulation without a pulse or signs of circulation
•• Turn on AED and attach electrodesTurn on AED and attach electrodes•• Turn on AED and attach electrodesTurn on AED and attach electrodes•• ANALYZE heart rhythmANALYZE heart rhythm•• Follow the voice prompts and screenFollow the voice prompts and screen•• Follow the voice prompts and screen Follow the voice prompts and screen
messagesmessages
-
Defibrillation Electrode Defibrillation Electrode PlacementPlacement
Anterior
Lateral
AnteriorAnterior--lateral placementlateral placement
-
Defibrillation Electrode Defibrillation Electrode PlacementPlacement
Correct electrode position Incorrect electrode position
•• Correct electrode position optimizes the amount of Correct electrode position optimizes the amount of current flowing through the ventriclescurrent flowing through the ventricles
Correct electrode position Incorrect electrode position
-
Sudden Cardiac DeathSudden Cardiac DeathSudden Cardiac DeathSudden Cardiac Death
•A public health crisis:
200000
250000
House fire
100000
150000Prostate cancer
Breast cancer
50000
100000Car accidents
Sudden cardiacarrest
0Annual incidence
arrest
-
S dd C di D thS dd C di D thSudden Cardiac DeathSudden Cardiac Death
Why is early defibrillation so important?Chance of survival Chance of survival from SCA from SCA diminishes 7diminishes 7--10%10%diminishes 7diminishes 7 10% 10% with every minute with every minute after collapseafter collapse
-
Averting SCD in Young AthletesAverting SCD in Young AthletesAverting SCD in Young AthletesAverting SCD in Young Athletes
•• “Play Ball!” “Just DO it!”“Play Ball!” “Just DO it!”•• ScreenScreen appropriately with expert providersappropriately with expert providersScreenScreen appropriately with expert providersappropriately with expert providers•• Sometimes old Sometimes old ––fashioned fashioned H&PH&P are the are the
bestbestbestbest•• Keep Keep AEDAED handy, in working condition, handy, in working condition,
and educate usersand educate usersand educate usersand educate users
-
FINFINFINFIN
•• USA USA in Beijingin BeijingMarch 2008!March 2008!
-
ECG FindingsECG FindingsECG FindingsECG Findings
Distribution of 3 ECG categories with respect to sporting disciplines among 1005 athletes. ECGs that were distinctly abnormal (black bars), mildly abnormal (gray bars), and normal or with minor alterations (white bars) are depicted as proportions of all the athletes participating in each sporting discipline. Only sports with 12 participants are shown. X-C indicates cross-country.