Suck-ligate-unroof-biopsy by using a detachable 20-mm loop for the diagnosis and therapy of small...
6
ORIGINAL ARTICLE: Clinical Endoscopy Suck-ligate-unroof-biopsy by using a detachable 20-mm loop for the diagnosis and therapy of small subepithelial tumors (with video) Kenneth F. Binmoeller, MD, Janak N. Shah, MD, Yasser M. Bhat, MD, Steve D. Kane, BS San Francisco, California, USA Background: The diagnosis and therapy of subepithelial tumors (SETs) can be challenging. Objective: Proof-of-concept evaluation of the suck-ligate-unroof-biopsy (SLUB) technique for small ( !2 cm), non-pedunculated SETs. Design: Pilot feasibility study. Setting: Tertiary-care referral center. Patients: Twenty-three patients (median age 60 years) meeting the inclusion criteria after preliminary EUS. Intervention: SET ligation was performed with a detachable 20-mm loop deployed through an 18-mm diameter, soft, oblique, transparent, cap attachment. The SLUB technique comprised (1) suction to draw the SET into the cap; (2) ligation below the SET, confirmation by repeat EUS; (3) unroofing of the overlying mucosa with a needle- knife; and (4) biopsy specimens taken from the exposed tumor. Main Outcome Measurements: Technical success, histology and/or immunohistochemistry yield, adverse events, completeness of resection. Results: SLUB was attempted on 24 SETs and was technically successful in all. Location was the stomach (n Z 19), small bowel (n Z 1), colon (n Z 2), and rectum (n Z 2). Median size by EUS was 10 mm (range 6-15 mm). Biopsy specimens provided an immunohistologic diagnosis in all cases: GI stromal tumor (n Z 5), leiomyoma (n Z 8), carcinoid tumor (n Z 5), Vanek’s tumor (n Z 2), granuloma (n Z1), and pancreatic heterotopia (n Z 3). Follow-up endoscopy and EUS in 13 patients showed well-healed scars with no residual tumor, including all 9 patients with premalignant neoplastic lesions. The only adverse event was self-limited pain in 2 patients. Limitations: Single center, single operator, small sample size. Conclusions: Loop ligation of small, non-pedunculated SETs is feasible by using a cap attachment for suction. Un- roofing after ligation is safe and provides sufficient tissue for immunohistochemistry. Ligation combined with unroof- ing appears to lead to complete ablation by ischemia and tumor enucleation. (Gastrointest Endosc 2014;79:750-5.) Abbreviations: FNA, fine-needle aspiration; NIH, National Institutes of Health; SET, subepithelial tumor; SLUB, suck-ligate-unroof- biopsy. DISCLOSURE: All authors disclosed no financial relationships relevant to this publication. Use your mobile device to scan this QR code and watch the author in- terview. Download a free QR code scanner by searching “QR Scanner” in your mobile device’s app store. Copyright ª 2014 by the American Society for Gastrointestinal Endoscopy 0016-5107/$36.00 http://dx.doi.org/10.1016/j.gie.2013.09.028 Received July 5, 2013. Accepted September 30, 2013. Current affiliations: Paul May & Frank Stein Interventional Endoscopy Center, California Pacific Medical Center, San Francisco, California, USA. Presented at Digestive Disease Week, May 18-21, 2013, Orlando, Florida, USA. Reprint requests: Kenneth F Binmoeller, MD, Director, Interventional Endoscopy Services, California Pacific Medical Center, San Francisco, CA 94118, USA. If you would like to chat with an author of this article, you may contact Dr Binmoeller at [email protected]. 750 GASTROINTESTINAL ENDOSCOPY Volume 79, No. 5 : 2014 www.giejournal.org
Transcript of Suck-ligate-unroof-biopsy by using a detachable 20-mm loop for the diagnosis and therapy of small...

ORIGINAL ARTICLE: Clinical Endoscopy
Abbrof Hbiop
DISCto th
750
Suck-ligate-unroof-biopsy by using a detachable 20-mm loopfor the diagnosis and therapy of small subepithelial tumors(with video)
eviatioealth;sy.
LOSURis publi
GAST
Kenneth F. Binmoeller, MD, Janak N. Shah, MD, Yasser M. Bhat, MD, Steve D. Kane, BS
San Francisco, California, USA
Background: The diagnosis and therapy of subepithelial tumors (SETs) can be challenging.
Objective: Proof-of-concept evaluation of the suck-ligate-unroof-biopsy (SLUB) technique for small (!2 cm),non-pedunculated SETs.
Design: Pilot feasibility study.
Setting: Tertiary-care referral center.
Patients: Twenty-three patients (median age 60 years) meeting the inclusion criteria after preliminary EUS.
Intervention: SET ligation was performed with a detachable 20-mm loop deployed through an 18-mm diameter,soft, oblique, transparent, cap attachment. The SLUB technique comprised (1) suction to draw the SET into thecap; (2) ligation below the SET, confirmation by repeat EUS; (3) unroofing of the overlying mucosa with a needle-knife; and (4) biopsy specimens taken from the exposed tumor.
Main Outcome Measurements: Technical success, histology and/or immunohistochemistry yield, adverseevents, completeness of resection.
Results: SLUB was attempted on 24 SETs and was technically successful in all. Location was the stomach (nZ 19),small bowel (n Z 1), colon (n Z 2), and rectum (n Z 2). Median size by EUS was 10 mm (range 6-15 mm).Biopsy specimens provided an immunohistologic diagnosis in all cases: GI stromal tumor (n Z 5), leiomyoma(n Z 8), carcinoid tumor (n Z 5), Vanek’s tumor (n Z 2), granuloma (n Z1), and pancreatic heterotopia(n Z 3). Follow-up endoscopy and EUS in 13 patients showed well-healed scars with no residual tumor, includingall 9 patients with premalignant neoplastic lesions. The only adverse event was self-limited pain in 2 patients.
Limitations: Single center, single operator, small sample size.
Conclusions: Loop ligation of small, non-pedunculated SETs is feasible by using a cap attachment for suction. Un-roofing after ligation is safe and provides sufficient tissue for immunohistochemistry. Ligation combined with unroof-ing appears to lead to complete ablation by ischemia and tumor enucleation. (Gastrointest Endosc 2014;79:750-5.)
ns: FNA, fine-needle aspiration; NIH, National InstitutesSET, subepithelial tumor; SLUB, suck-ligate-unroof-
E: All authors disclosed no financial relationships relevantcation.
Use your mobile device to scan thisQR code and watch the author in-terview. Download a free QR codescanner by searching “QR Scanner”in your mobile device’s app store.
Copyright ª 2014 by the American Society for Gastrointestinal Endoscopy0016-5107/$36.00http://dx.doi.org/10.1016/j.gie.2013.09.028
Received July 5, 2013. Accepted September 30, 2013.
Current affiliations: Paul May & Frank Stein Interventional EndoscopyCenter, California Pacific Medical Center, San Francisco, California, USA.
Presented at Digestive Disease Week, May 18-21, 2013, Orlando, Florida, USA.
Reprint requests: Kenneth F Binmoeller, MD, Director, InterventionalEndoscopy Services, California Pacific Medical Center, San Francisco,CA 94118, USA.
If you would like to chat with an author of this article, you may contactDr Binmoeller at [email protected].
ROINTESTINAL ENDOSCOPY Volume 79, No. 5 : 2014 www.giejournal.org

Figure 1. 20-mm loop “prelooped” along the outer rim of the 18-mmoblique transparent cap, mounted on the endoscope tip.
Binmoeller et al Suck-ligate-unroof-biopsy
Subepithelial tumors (SETs) are commonly encounteredon routine endoscopies, but the exact prevalence is uncer-tain. One retrospective study reported a prevalence of 3.5%(188/5307 upper endoscopies). Although SETs are rarelysymptomatic and usually benign, an uncertain diagnosiscan be the source of significant anxiety for the patient. Sur-veillance is costly over time, and an argument can be madefor establishing a tissue diagnosis or removal. Stacked “bite-on-bite” forceps biopsy has a limited diagnostic yield,1 withone prospective study showing a diagnostic yield of only17% compared with 87% with endoscopic resection.2 EUSprovides valuable information regarding layer of originand can suggest a diagnosis, but it has been shown tohave limited accuracy.3-5 EUS-guided tissue sampling canbe technically challenging, with poor yields for small, mo-bile, SETs.6 Endoscopic resection by snaring and submuco-sal dissection secures a surgical specimen but is technicallydemanding and has been complicated by perforation andbleeding in most series.7-13 Ligation of SETs by using bandsand loops has been proposed to improve safety of treat-ment.14-20 We report our experience using a suck-ligate-unroof-biopsy (SLUB) technique for the diagnosis andtreatment of small SETs.
PATIENTS, MATERIALS, AND METHOD
A retrospective evaluation of a prospectively collectedcomputerized database (Provation Medical, Minneapolis,Minn) identifying all patients who underwent the SLUBprocedure since 2011 was approved by the CaliforniaPacific Medical Center Institutional Review Board. Inclu-sion criteria were intramural SETS !20 mm on EUS.Excluded were lesions with typical sonographic featuresof a lipoma, varix, or cyst. All procedures were performedon an outpatient basis by a single endoscopist (K.F.B.).Antithrombotic agents were generally stopped 5 daysbefore and for 7 to 10 days after the procedure, with insti-tution of “bridge” therapy with unfractionated or lowmolecular weight heparin as indicated. Informed consentwas obtained before the procedure in all patients. Thisincluded a discussion of the risk-benefit ratio of 3 manage-ment options: (1) surveillance in intervals, (2) surgery, or(3) SLUB. Patients were informed of the limitations of
www.giejournal.org
Take-home message
� The suck-ligate-unroof-biopsy method enablesacquisition of generous tissue samples forimmunohistochemical diagnosis with the potentialfor curative tumor ablation.
� Unroofing after ligation exposes the underlying tumorfor direct tissue sampling and promotes spontaneousenucleation.
SLUB and the need for close surveillance by EUS ofneoplastic lesions with malignant potential.
A wide, 18-mm-diameter, soft, oblique, transparent capwith a rim on the inside (Olympus D-206-05; OlympusMedical, Center Valley Pa) was fitted onto the tip of atherapeutic endoscope (GIF-1TQ160; Olympus). A ligatingdevice (HX-20U-1; Olympus) with a detachable nylon loop(MAJ-340; Olympus ) with a maximum diameter of 20 mmwas inserted into the accessory channel of the endoscopeand “prelooped” to open along the rim of the cap attach-ment (Fig. 1). A standardized technique was applied(Fig. 2A) (Video 1, available online at www.giejournal.org). All patients underwent preliminary EUS by using a12-MHz catheter US probe (MAJ-935; Olympus) (Fig. 2B).Lesion size was measured by EUS (maximum cross-section of lesion proper). Carbon dioxide was used forlumen insufflation. The cap was positioned around thecircumference of the tumor and suction was applied untilthe cap filled with tissue and a “red out” was seen(Fig. 2C). The loop was then tightened at the base of thelesion, suction was released, and the loop was deployedfrom the delivery sheath. After ligation, EUS was repeatedto confirm loop placement below the SET (Fig. 2D). Thetumor was then “unroofed” by incising the overlyingmucosa with a needle-knife (KD-10Q-1; Olympus) by usingpure cut current (auto cut, effect 5, 80 W, Erbe Vio 300D;Erbe, Marietta, Ga) (Fig. 2E). Two perpendicular incisionswere made along the mucosal surface above the ligationin a cross formation. Freehand incision was directedfrom the outside to the center to avoid injury to the neigh-boring wall. Multiple biopsy specimens (at least 3 withvisible tissue yields) were obtained from the exposed tu-mor by using a standard biopsy forceps (Fig. 2F). All spec-imens were submitted for histopathologic andimmunohistochemical analysis (Fig. 2G). In cases wherea GI stromal tumor was suspected, the analysis includeda mitotic count per 50 high-power fields in order to deter-mine the malignant potential according to the National In-stitutes of Health (NIH) classification.21
Depending on the pathology of the tumor, surveillanceendoscopy and EUS were scheduled at 3 to 6 months afterthe index procedure (Fig. 2). Follow-up endoscopies werenot performed in patients with benign pathology andabsence of symptoms.
Volume 79, No. 5 : 2014 GASTROINTESTINAL ENDOSCOPY 751
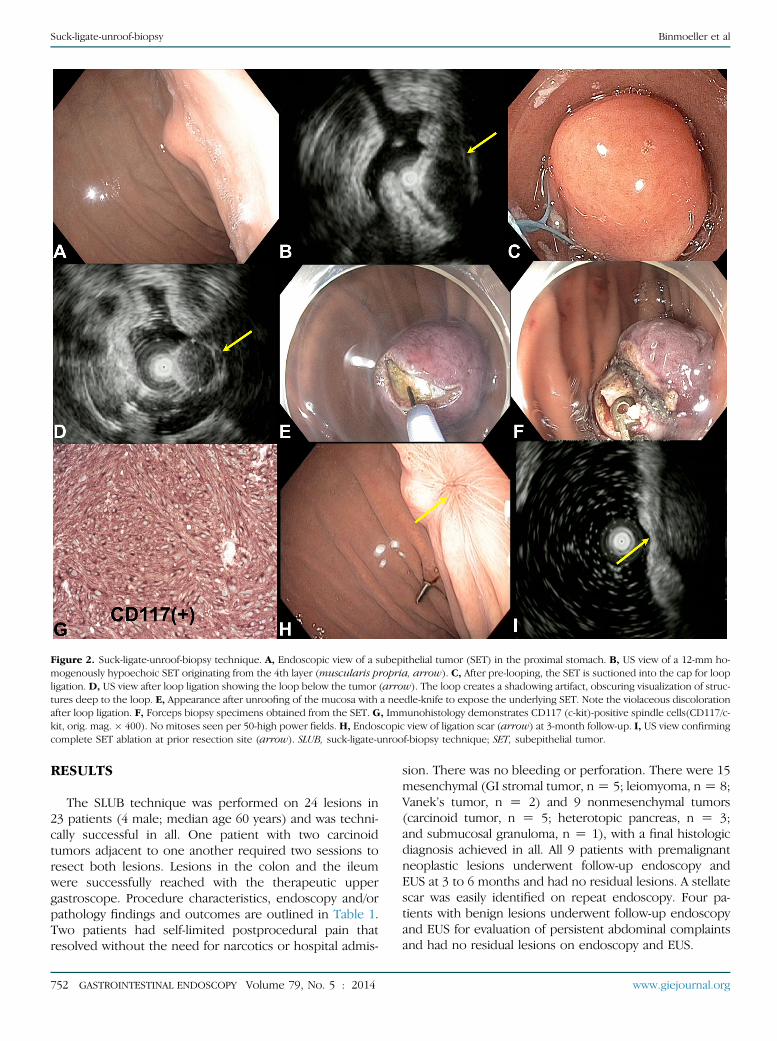
Figure 2. Suck-ligate-unroof-biopsy technique. A, Endoscopic view of a subepithelial tumor (SET) in the proximal stomach. B, US view of a 12-mm ho-mogenously hypoechoic SET originating from the 4th layer (muscularis propria, arrow). C, After pre-looping, the SET is suctioned into the cap for loopligation. D, US view after loop ligation showing the loop below the tumor (arrow). The loop creates a shadowing artifact, obscuring visualization of struc-tures deep to the loop. E, Appearance after unroofing of the mucosa with a needle-knife to expose the underlying SET. Note the violaceous discolorationafter loop ligation. F, Forceps biopsy specimens obtained from the SET. G, Immunohistology demonstrates CD117 (c-kit)-positive spindle cells(CD117/c-kit, orig. mag. � 400). No mitoses seen per 50-high power fields. H, Endoscopic view of ligation scar (arrow) at 3-month follow-up. I, US view confirmingcomplete SET ablation at prior resection site (arrow). SLUB, suck-ligate-unroof-biopsy technique; SET, subepithelial tumor.
Suck-ligate-unroof-biopsy Binmoeller et al
RESULTS
The SLUB technique was performed on 24 lesions in23 patients (4 male; median age 60 years) and was techni-cally successful in all. One patient with two carcinoidtumors adjacent to one another required two sessions toresect both lesions. Lesions in the colon and the ileumwere successfully reached with the therapeutic uppergastroscope. Procedure characteristics, endoscopy and/orpathology findings and outcomes are outlined in Table 1.Two patients had self-limited postprocedural pain thatresolved without the need for narcotics or hospital admis-
752 GASTROINTESTINAL ENDOSCOPY Volume 79, No. 5 : 2014
sion. There was no bleeding or perforation. There were 15mesenchymal (GI stromal tumor, nZ 5; leiomyoma, nZ 8;Vanek’s tumor, n Z 2) and 9 nonmesenchymal tumors(carcinoid tumor, n Z 5; heterotopic pancreas, n Z 3;and submucosal granuloma, n Z 1), with a final histologicdiagnosis achieved in all. All 9 patients with premalignantneoplastic lesions underwent follow-up endoscopy andEUS at 3 to 6 months and had no residual lesions. A stellatescar was easily identified on repeat endoscopy. Four pa-tients with benign lesions underwent follow-up endoscopyand EUS for evaluation of persistent abdominal complaintsand had no residual lesions on endoscopy and EUS.
www.giejournal.org

TABLE 1. Patient characteristics, endoscopy and/orpathology findings, outcomes (n [ 23)
Male, no. (%) 4 (17)
Indication, no.
Abdominal pain/incidental 19
Bleeding 2
Dysphagia 2
Tumors, no. 24
Tumor location, no.
Antrum 4
Cardia 4
Fundus 3
Gastric body 8
Ileum 1
Transverse colon 2
Rectum 2
Size on EUS, median, (range) mm 10 (6-15)
Procedure time, median, (range) min 15 (5-42)
Histology, no.
Carcinoid tumor 5
GI stromal tumor 5
Vanek’s tumor 1
Leiomyoma 8
Pancreatic heterotopia 3
Granuloma 2
Adverse events, no. (%)
Postprocedural pain 2 (9)
Bleeding 0
Perforation 0
Patients with follow-up 13 (56)
Residual tumor at follow-up 0
Binmoeller et al Suck-ligate-unroof-biopsy
DISCUSSION
Ligation-assisted treatment of small SETs has been pro-posed to improve the safety of treatment. Chang et al15
first described the adjunctive use of band ligation of agastric subepithelial lesion before electrosurgical resection.Sun et al20 reported band ligation without electrosurgeryfor the treatment of 64 small upper GI leiomyomas origi-nating from the muscularis propria, previously diagnosedby EUS-FNA or “stack” biopsies. Spontaneous sloughing
www.giejournal.org
was observed in 95% within 3.6 to 4.5 weeks after endo-scopic band ligation, with no adverse events. Huanget al16 performed ligation of 8 small (!20 mm) gastric stro-mal tumors by using bands and detachable 30-mm loopsfollowed by resection, with no reports of perforation orbleeding. No adverse events were reported in these series.
In this study, we performed suction-assisted ligation byusing a detachable nylon ligation device in conjunctionwith an 18-mm oblique, soft, transparent cap. Huanget al16 used standard 30-mm loops in conjunction withan 18-mm cap, but we have found the 30-mm loop difficultto pre-loop in the cap. We encountered no major technicaldifficulties with cap insertion or loop deployment. Thedeformability of the soft cap allowed easy passage acrossthe cricopharynx and the esophagogastric junction. Weperformed endoscopic unroofing by needle-knife incisionto expose the underlying tumor for endoscopicallydirected forceps biopsy. This differs from the originaldescription of the unroofing technique by Mimuraet al,22 which involves snaring at the middle of the mass(ie, resecting the upper half). Lee et al23 modified the un-roofing technique by first removing 2 or 3 fragments of theoverlying mucosa with a snare, followed by partial resec-tion of the exposed tumor. We did not use a snare forunroofing, because we have found it difficult to selectivelyremove the mucosa; the snare either slips off the surfaceduring closure or captures too much tissue, which mayinclude the loop. de la Serna-Higuera et al24 commentedon similar technical difficulties during use of a snare forunroofing and used a needle-knife to perform a singleincision over the tumor.
The unroofing technique used in our study served thedual objective of tumor exposure for directed biopsies aswell as partial enucleation. We made two incisions in across formation to expose a maximum amount of underly-ing tissue. Unroofing has been described previously as apreliminary step to tumor enucleation by submucosaldissection technique.25,26 Although we did not dissectout the tumor after unroofing, we sometimes enucleatedthe tumor from its ligation bed while obtaining biopsyspecimens, owing to the pulling force on the tumor(Fig. 3). This observation supports the hypothesis thatunroofing after ligation promotes enucleation.
The only adverse event we encountered was self-limitedpostprocedure pain in two patients. Procedural bleedingafter unroofing was not seen, which we attribute to ligationbefore unroofing. By using unroofing alone, Lee et al23
reported procedural bleeding that required endoscopichemostasis in 56% of patients. de la Serna-Higuera et al24
prophylactically closed needle-knife incisions with clips.Biopsies were diagnostic in all cases (yield of 100%).
Of these, there was sufficient material for immunohistol-ogy in all mesenchymal tumors and mitotic index calcula-tion in all c-kit–positive GI stromal tumor lesions. All GIstromal tumors were!2 cm and showed!5 mitoses per50 high-power fields, so they were categorized as “very
Volume 79, No. 5 : 2014 GASTROINTESTINAL ENDOSCOPY 753

Figure 3. Enucleation of an encapsulated subepithelial tumor with biopsyforceps after unroofing.
Suck-ligate-unroof-biopsy Binmoeller et al
low risk” according to the NIH risk table.21 The high yieldof biopsies after unroofing is consistent with findings byde la Serna-Higuera et al,24 who reported a diagnostic yieldof 93% in a cohort of 14 patients with SETs. In 8 patientswith stromal cell tumors, there was sufficient material forimmunohistochemical analysis in 7 patients (87%) andmitotic index determination in 5 patients (71.4%). Ofnote, the diagnostic yield of EUS-FNA in 8 patients whounderwent both EUS-FNA and biopsies was only 12.5%.
Patients were selected for the SLUB procedure based onthe EUS findings. In this respect, the procedure was EUSguided. We used a 12-MHz catheter US probe insertedthrough the working channel of the endoscope. All SETSwere intramural and did not exceed 20 mm in size. SLUBwas not performed when the EUS was sufficiently diag-nostic of a lipoma (homogenously hyperechoic), varix, orcyst (homogenously anechoic). We considered suspectedpancreatic heterotopia to be an appropriate indicationfor SLUB, because the endoscopic and EUS findings arenot sufficiently diagnostic. Neoplastic growths such as acarcinoid tumor, GI stromal tumor, and lymphoma canmimic pancreatic heterotopia.27 In addition, pancreaticheterotopia can be symptomatic, causing abdominal pain,dyspepsia, and pancreatitis,28,29 and warrant treatment.One of the 3 patients with pancreatic heterotopia in ourcohort had abdominal pain, which resolved after ablation.Although rare, malignant transformation of pancreatic het-erotopia has been reported and may warrant treat-ment.30,31 The strength of the SLUB procedure is theability to acquire large tissue samples for immunohisto-chemical diagnosis with the potential for curative tumorablation in a single procedure. The main weakness is theinability to provide an en bloc specimen of the entire tu-mor for surgical pathology and evaluation of the resectionmargins. However, the need for confirmation of radical
754 GASTROINTESTINAL ENDOSCOPY Volume 79, No. 5 : 2014
resection by surgical pathology is mitigated by the benignnature of most small SETs, including GI stromal tumorsand the ability of EUS to interrogate for residual or recur-rent tumor. Any neoplastic lesion with malignant potentialwill need close serial follow-up by EUS. Patients should beinformed that surveillance is imperative because of theinability to assess for negative margins after the tumorhas sloughed off.
In conclusion, the diagnosis and treatment of small SETsby using the SLUB procedure is technically feasible andappears to be safe. A limitation of this study is the biasinherent in the performance of procedures at a single cen-ter by a single endoscopist. Further study is needed todetermine whether results are reproducible elsewhere.
REFERENCES
1. Hunt GC, Smith PP, Faigel DO. Yield of tissue sampling for submucosallesions evaluated by EUS. Gastrointest Endosc 2003;57:68-72.
2. Cantor MJ, Davila RE, Faigel DO. Yield of tissue sampling for subepithe-lial lesions evaluated by EUS: a comparison between forceps biopsiesand endoscopic submucosal resection. Gastrointest Endosc 2006;64:29-34.
3. Hwang JH, Saunders MD, Rulyak SJ, et al. A prospective studycomparing endoscopy and EUS in the evaluation of GI subepithelialmasses. Gastrointest Endosc 2005;62:202-8.
4. Karaca C, Turner BG, Cizginer S, et al. Accuracy of EUS in the evaluationof small gastric subepithelial lesions. Gastrointest Endosc 2010;71:722-7.
5. Rösch T, Kapfer B, Will U, et al. Accuracy of endoscopic ultrasonogra-phy in upper gastrointestinal submucosal lesions: a prospective multi-center study. Scand J Gastroenterol 2002;37:856-62.
6. Philipper M, Hollerbach S, Gabbert HE, et al. Prospective comparisonof endoscopic ultrasound-guided fine-needle aspiration and surgicalhistology in upper gastrointestinal submucosal tumors. Endoscopy2010;42:300-5.
7. Binmoeller KF, Grimm H, Soehendra N. Endoscopic closure of a perfo-ration using metallic clips after snare excision of a gastric leiomyoma.Gastrointest Endosc 1993;39:172-4.
8. Park YS, Park SW, Kim TI, et al. Endoscopic enucleation of upper-GIsubmucosal tumors by using an insulated-tip electrosurgical knife.Gastrointest Endosc 2004;59:409-15.
9. von Renteln D, Riecken B, Walz B, et al. Endoscopic GIST resectionusing FlushKnife ESD and subsequent perforation closure by meansof endoscopic full-thickness suturing. Endoscopy 2008;(40 suppl 2):E224-5.
10. Waterman AL, Grobmyer SR, Cance WG, et al. Is endoscopic resectionof gastric gastrointestinal stromal tumors safe? Am Surg 2008;74:1186-9.
11. Hwang JC, Kim JH, Kim JH, et al. Endoscopic resection for the treat-ment of gastric subepithelial tumors originated from the muscularispropria layer. Hepatogastroenterology 2009;56:1281-6.
12. Li QL, Yao LQ, Zhou PH, et al. Submucosal tumors of the esophagogas-tric junction originating from the muscularis propria layer: a largestudy of endoscopic submucosal dissection (with video). GastrointestEndosc 2012;75:1153-8.
13. Bialek A, Wiechowska-Kozlowska A, Pertkiewicz J, et al. Endoscopicsubmucosal dissection for treatment of gastric subepithelial tumors(with video). Gastrointest Endosc 2012;75:276-86.
14. Cariani G, Di Marco M, Roda E. Endoloop-assisted polypectomyfor large peduncolated colorectal polyps. Surg Endosc 2007;21:1676-7.
www.giejournal.org
Binmoeller et al Suck-ligate-unroof-biopsy
15. Chang KJ, Yoshinaka R, Nguyen P. Endoscopic ultrasound-assistedband ligation: a new technique for resection of submucosal tumors.Gastrointest Endosc 1996;44:720-2.
16. Huang WH, Feng CL, Lai HC, et al. Endoscopic ligation and resectionfor the treatment of small EUS-suspected gastric GI stromal tumors.Gastrointest Endosc 2010;71:1076-81.
17. Huang WH, Peng CY, Yu CJ, et al. Endoloop-assisted unroofing for thetreatment of symptomatic duodenal lipomas. Gastrointest Endosc2008;68:1234-6.
18. Lee SH, Park JH, Park doH, et al. Endoloop ligation of large pedunculatedsubmucosal tumors (with videos). Gastrointest Endosc 2008;67:556-60.
19. Papalambros A, Petrou A, BrennanN, et al. GIST suture-line recurrence ata gastrojejunal anastomosis 8 years after gastrectomy: Can GIST ever bedescribed as truly benign? A case report. World J Surg Oncol 2010;8:90.
20. Sun S, Ge N, Wang C, et al. Endoscopic band ligation of small gastricstromal tumors and follow-up by endoscopic ultrasonography. SurgEndosc 2007;21:574-8.
21. Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastrointes-tinal stromal tumors: a consensus approach. Hum Pathol 2002;33:459-65.
22. Mimura T, Kuramoto S, Hashimoto M, et al. Unroofing for lymphangio-ma of the large intestine: a new approach to endoscopic treatment.Gastrointest Endosc 1997;46:259-63.
23. Lee CK, Chung IK, Lee SH, et al. Endoscopic partial resection withthe unroofing technique for reliable tissue diagnosis of upper GI
www.giejournal.org
subepithelial tumors originating from the muscularis propria on EUS(with video). Gastrointest Endosc 2010;71:188-94.
24. de la Serna-Higuera C, Pérez-Miranda M, Diez-Redondo P, et al.EUS-guided single-incision needle-knife biopsy: description and resultsof a new method for tissue sampling of subepithelial GI tumors (withvideo). Gastrointest Endosc 2011;74:672-6.
25. Katoh T, Itoh Y, Mohri T, et al. Endoscopic enucleation of gastrointes-tinal stromal tumors of the stomach: report of five cases. World J Gas-troenterol 2008;14:2609-11.
26. Zhang JS, Ye LP, Wang CY, et al. Endoscopic submucosal enucleationof small gastric gastrointestinal stromal tumors with cross-shaped inci-sion: report of sixty-nine cases. Hepatogastroenterology 2012;59:440-3.
27. Thoeni RF, Gedgaudas RK. Ectopic pancreas: usual and unusual fea-tures. Gastrointest Radiol 1980;5:37-42.
28. Rimal D, Thapa SR, Munasinghe N, et al. Symptomatic gastric hetero-topic pancreas: clinical presentation and review of the literature. IntJ Surg 2008;6:e52-4.
29. De Beule T, Ardies L, Van Hoe L, et al. Ectopic gastric pancreatitis:unusual cause of epigastric pain. JBR-BTR 2011;94:295-6.
30. Ura H, Denno R, Hirata K, et al. Carcinoma arising from ectopicpancreas in the stomach: endosonographic detection of malignantchange. J Clin Ultrasound 1998;26:265-8.
31. Guillou L, Nordback P, Gerber C, et al. Ductal adenocarcinoma arisingin a heterotopic pancreas situated in a hiatal hernia. Arch Pathol LabMed 1994;118:568-71.
Volume 79, No. 5 : 2014 GASTROINTESTINAL ENDOSCOPY 755


















