Successfully Training A “Rookie” · PDF fileSuccessfully Training A...
10
10/27/2017 1 © 2017 Lehigh Valley Health Network Successfully Training A “Rookie” Registrar Robin L. Schrader, CSTR Trauma Registry PI Coordinator Trainer ▪ One Trainer-Too many too much! ▪ Approachable and Patient-Can be easily interrupted and be patient with repeated questions, etc. ▪ Accessible-Located close to trainee ▪ Knowledgeable (Seasoned Registrar)-Someone who has been doing the job for 5+ years
-
Upload
duongnguyet -
Category
Documents
-
view
226 -
download
2
Transcript of Successfully Training A “Rookie” · PDF fileSuccessfully Training A...

10/27/2017
1
© 2017 Lehigh Valley Health Network
Successfully Training A “Rookie” Registrar
Robin L. Schrader, CSTRTrauma Registry PI Coordinator
Trainer
▪ One Trainer-Too many too much!
▪ Approachable and Patient-Can be easily interrupted and be patient with repeated questions, etc.
▪ Accessible-Located close to trainee
▪ Knowledgeable (Seasoned Registrar)-Someone who has been doing the job for 5+ years

10/27/2017
2
What is the Trauma Registry? Why do we need Registrars?
▪ Explain why we collect data. • Registrars Role in Trauma Program• Who gets the Data
– PTSF– NTDB/TQIP– Institution
• What do they do with it– Research– Review Quality of Care– Compare Outcomes/PI– Peer Review
• Why is it important that data is clean/accurate
Getting Started
▪ Start with the Basics-Have an Orientation Packet ▪ Include copies of forms/information used often
– Trauma Registry Patient pick up criteria– Hospital Units/Floors– Consult List– Coding “cheat sheet”– List of Trauma/ED/Surgical residents with PGY listed– How to find EMS PCR’s – Currently in the process of making a step by step guide with screen shots of collector and where we find the
information in EPIC with a screenshot.• Daily Trauma patient pick up list
– What patient’s are Trauma Database “worthy”– What constitutes a “Trauma patient”– Specific injuries that are not picked up (i.e.. Fall same level-hip fx)– Use Teaching tools
– Patient pick up Algorithm– Daily check off sheet for pick up list duties

10/27/2017
3
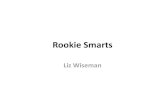
REGISTRY INCLUSION CRITERIA
Trauma Alert / Code Red / Trauma Transfer
Seen by Trauma (will have a trauma log)
Transfer In Admitted to Trauma Service (On census) Seen & Referred to Med. Svc Discharged from ED Or sent home for medical condition Pick up Pick up in registry no injury – pick up – Non PTOS NON PTOS **Can be PTOS or NON PTOS** (Burn – do not pick up) (Tfr Tilghman to CC & d/c from ED – do not pick up)*
Patient with traumatic mechanism seen in ED
Seen by Trauma (Trauma 18 consult or regular consult)
Cleared / no injury or Injury, must be at least concussion Admitted to treat Medical- Minor (lac, abrasion, strain &/or recorded LOC and sent No injury sprain, “closed” head injury home Traumatic Injury or admitted without LOC) for medical Pick up in registry condition with AND Sent Home Pick up in registry minor injury Do not pick up, even if (Do not pick up burn ED D/C) There is a log Do not pick up (CHI by ED dr does NOT= in registry Concussion)
Patient with traumatic mechanism seen in ED
Not seen by Trauma
Sent home Admitted on non-trauma svc Medical – no injury To treat Traumatic injury or admitted for medical Do not pick up condition with minor (Includes Transfer in Pick up in registry injury for another service) Do not pick up in Registry Drownings NOT seen by Trauma Do not pick up Rev. 2/2015* The only SDH we do NOT pick up are those proven to be from dialysis or cancer
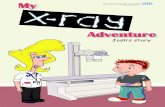
DAILY LIST CHECK/NOTE SHEET
DATE:____________________REGISTRAR:__________________
TASK ***remember to leave this on your desk for next day, and notes on back*** DONE
Run EPIC DC List
Mark the DC’s on the patient list and write Trauma #/Room/Registrar or __on the DC List
Email DC list to “Trauma daily dc list” group on copier
Pull DC’s from Active PT pile and write DC date on top of facesheet
Enter DC patient * date/time in collector *PTOS or NON (if known, by length of stay, etc.)
Assign charts to registrars (check calendar for who is working and who is on chart holiday)
Email charts to registrars and put facesheets on desks
Run EPIC BURN Census (my reports)
Print Trauma Census (under patient lists/shared/daily census)
Compare Burn and Trauma Census’ to our patient list/check for pts who may have moved off service or were dc’d and not removed, etc. (****remember to update any room # that still have ED or OR, and move any ED DCs to the unassigned dc list***)
Print new Trauma admission list (patient lists, shared, 24 hour adm)
Run LV ADT Daily Emergency Dept log‐Trauma‐review looking for trauma pick ups and off service pick ups
Flag “Trauma” patients in EPIC
Flag “Not a Trauma” for any Non Pick ups and add to non pick up sheet of patient list
Print FaceSheets from EPIC
Assign Trauma number to each patient on FaceSheet
Enter new patients in Collector‐ Name/MR#/Acct #/Sex/DOB/Age
Enter PTOS or NON PTOS if known (ie. ICU admission/Txfer in)
Type of injury‐Blunt‐Penetrating‐Burn
Two digit injury code
Admission Service
Transfer in‐yes or no/Transferring Facility
Admitting MD
Post ED Destination and Floor Number
ED Arrival Date/Time
Alert level‐ED Response Page; For Trauma Alert and Code Red, include MD times
Diagnoses‐From H&P and initial X‐Ray/Scans only
Go into Excel “Patient List” and Delete any DC’s that were already assigned to a registrar
Cut and Paste any DC’s, that were unassigned, to the Unassigned DC tab on the patient list‐remember to keep in admission date order
Delete any patients on the “unassigned dc” tab that have been given out
Add new patients to the Trauma, Burn, off service tabs (keep in date order, ie‐4/5, 4/6, 4/7, etc.)
Move any Mortalities to the Mortality tab, print, and hang on board
Update any “no pick up or re admit” patients to that tab (no need to print this page)
Complete the “dropped” tab if any patients were deleted, # reused, etc. (no need to print this page)
Print the Census‐Trauma, Burn, Off Service, and Unassigned DC tabs
Mark the Trauma number to start with on the top of the 1st page (Trauma pt census)
Highlight all new patients on Trauma, Burn, and Off service pages in Yellow

10/27/2017
4
The Registrars “Bible”
▪ PTSF Data Dictionary • Review preface and instructions
• Discuss PTOS (PA Trauma Outcome Study) Inclusion Criteria
• Have the registrar read over the Data sections and answer questions
• Review occurrences briefly at this time
• Review Pre Existing Conditions
• Discuss the importance of following the Data dictionary
Collector Database
▪ Introduce to Collector-review pages• Explain NTDB/Burn and Custom tabs
• Starting a new chart
• Closing a chart
• Drop down boxes– Use, but do not replace coding book

10/27/2017
5
▪ EMS PCR’s• Explain where your facility locates trip sheets
– EMS Charts
– ImageTrend
– Request from EMS squads
• Explain importance of trip sheets
• Go over scene provider vs transport provider and helicopter vs ambulance-helicopter rendezvous
AIS (abbreviated injury scale)▪ Review the AIS book (all new Registrars should be sent to
AAAM AIS Course between 6-12 months of employment)• Review Coder Instructions• Body Regions-What’s included• Explain what the code means=Pre-Dot code(body region/type
of anatomic structure/specific anatomic structure/level of injury) Post-Dot code=Severity
• How to calculate an ISS (1-75)• Why sizes are important (i.e.. SDH, codes to specific size, not
small, moderate, or large)• How to look up codes

10/27/2017
6
CHARTS
▪ Start with easy, NON PTOS, charts• Abstract the chart from the hospital database (EPIC, EMR, Etc.)
– Explain where in the hospital database you find the information to abstract
• Use the PTSF Data Dictionary as you go through each screen– Have the registrar make notes– Explain the “rules” of the dictionary must be met to use the data (i.e.. Pre-
Existing conditions)– Let the new registrar enter a chart on their own
– Abstract and “Correct” the chart and review with the registrar and explain “why” and “where”, etc.
– As trainee progresses, move on to 2 day charts, PTOS charts, and continue to move to more complex cases (burns, if applicable), and longer LOS.
▪ Charts• As the trainee progresses with charts, you can begin to check
less and less data (i.e.. Demographics, ED stay information, etc.)– Progress until just DX and Procedures are being checked
– When trainee is consistently at 95-100% accurate with charts, progress to independent

10/27/2017
7

10/27/2017
8
Diagnosis Coding (Tricode)
▪ Discuss Traumatic Injuries
▪ Use of Tricode as a guide, always need to double check your codes!!!!
• Code only Traumatic Injury
• Laterality
• Open vs closed
• Descriptors, Grades, and sizes if known
• Review AIS codes in book

10/27/2017
9
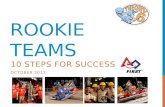
Procedure Coding (ICD-10-PCS)
▪ Review the ICD-10-PCS book
▪ Explain procedures picked up as per PTSF and as per your institution
• Have a handy list with codes available (“Cheat Sheet”)
• Discuss the “locations” at your facility where procedures may be done
• Many procedures are “learn as you go” with each chart
IMAGING CT HEAD NO CONTRAST BW28ZZZ CT HEAD WITH CONTRAST BW281ZZ CT BRAIN NO CONTRAST B020ZZZ CT BRAIN WITH CONTRAST B0201ZZ CT NECK BW2FZZZ CT HEAD AND NECK BW29ZZZ CT NECK (NO CONTRAST) BW2FZZZ CT ABDOMEN NO CONTRAST BW20ZZZ CT ABDOMEN WITH CONTRAST
BW201ZZ
CT CHEST AND ABDOMEN NO CONTRAST
BW24ZZZ
CT CHEST AND ABDOMEN WITH CONTRAST
BW241ZZ
CT CHEST/ABD/PELVIS WITH CONTRAST
BW251ZZ
CT ABD/PELVIS WITH CONTRAST
BW211ZZ
CT CHEST NO CONTRAST BW24ZZZ CT CHEST WITH CONTRAST BP2W1ZZ CT FACE NO CONTRAST BN25ZZZ CT FACE WITH CONTRAST BN251ZZ CT C SPINE NO CONTRAST BR20ZZZ CT C SPINE WITH CONTRAST BR201ZZ CT T SPINE NO CONTRAST BR27ZZZ CT T SPINE WITH CONTRAST BR271ZZ CT L SPINE NO CONTRAST BR29ZZZ CT L SPINE WITH CONTRAST BR291ZZ CT PELVIS NO CONTRAST BR2CZZZ CT PELVIS WITH CONTRAST BW2G1ZZ CT SI JOINTS BR2DZZZ CT SI JOINT WITH CONTRAST BR2D1ZZ CT SACRUM AND COCCYX BR2FZZZ CT SACRUM AND COCCYX WITH CONTRAST
BR2F1ZZ
CTA HEAD AND NECK BW291ZZ CTA NECK/w/wo contrast BW2F10Z CTA THORAX BW2410Z MRI BRAIN NO CONTRAST B030ZZZ
MRI BRAIN WITH CONTRAST B030Y0Z MRI C SPINE NO CONTRAST BR30ZZZ MRI C SPINE WITH CONTRAST BR30Y0Z MRI T SPINE NO CONTRAST BR37ZZZ MRI T SPINE WITH CONTRAST BR37Y0Z MRI L SPINE NO CONTRAST BR39ZZZ MRI L SPINE WITH CONTRAST BR39Y0Z MRI BRACHIAL PLEXUS WITH CONTRAST
BW3PY0Z
MRI BRACHIAL PLEXUS NO CONTRAST
BW3PZZZ
MRA NECK WITH CONTRAST MRA NECK WITHOUT CONTRAST
BW3FY0Z BW3FZZZ
MRA HEAD NO CONTRAST B33RZZZ XR RIBS RIGHT BP0XZZZ XR RIBS LEFT BP0YZZZ X RAY RIGHT FEMUR BQ03ZZZ PLAIN CHEST XRAY BW03ZZZ PLAIN XRAY PELVIS BR0CZZZ BABYGRAM WHOLE BODY BW0MZZZ XR ABDOMEN BW00ZZZ BRAIN DEATH NUC MED SCAN C0201ZZ EKG 4A02X4Z FAST BW41ZZZ ECHO LEFT AND RIGHT HEART B246ZZZ XR HIP R‐BQ00…/L‐BQ01 XR FEM R‐BQ03 /L‐BQ04 XR KNEE R‐BQ07/L‐BQ08 VENOUS DUPLEX BIL LE’S VEINS (DOPPLER)
B54DZZZ
VENOUS DUPLEX BIL UE’S VEINS
B54PZZZ
US BIL KIDNEYS BT43ZZZ US BIL KIDNEYS AND BLADDER BT4JZZZ CAROTID DUPLEX HEAD AND NECK
BH4CZZZ
US PELVIS BW4GZZZ US GI TRACT BD47ZZZ
US GALLBLADDER AND BILE DUCTS
BF43ZZZ
US BLADDER BT40ZZZ US UTERUS 1ST TRIMESTER 1‐12
BY49ZZZ
US UTERUS 2ND TRIMESTER 13‐28
BY4CZZZ
US UTERUS 3RD TRIMESTER 29+
BY4FZZZ
U/S ABD AND PELVIS BW41ZZZ U/S BRAIN (TRANS CRANIAL DOPPLER)
B040ZZZ
Fetal Heart Tones (RATE) 4A0HXCZ SUTURE/STAPLE/REPAIR
SUTURE SKIN SCALP 0HQ0XZZ SUTURE SKIN FACE 0HQ1XZZ SUTURE EXTERNAL EAR RIGHT
09Q0XZZ
SUTURE EXTERNAL EAR LEFT 09Q1XZZ SUTURE NOSE 09QKXZZ SUTURE UPPER LIP 0CQ0XZZ SUTURE LOWER LIP 0CQ1XZZ SUTURE BUCCAL MUCOSA 0CQ4XZZ SUTURE UPPER GINGIVA 0CQ5XZZ SUTURE LOWER GINGIVA 0CQ6XZZ Suture upper eyelid R‐08QNXZZ/L‐
08QPNXZZ Suture lower eyelid R‐08QQXZZ/L‐
08QRXZZ SUTURE MUSCLE 0JQ…. SUTURE SKIN 0HQ….

10/27/2017
10
▪ One Trainer-BE PATIENT!▪ Explain the Registrar Role in
the Trauma Program▪ Have “cheat sheets”/examples
available▪ Review PTSF data dictionary,
NTDB dictionary, AIS book, and ICD-10 coding books
▪ ***BE POSTIVE AND ENCOURAGING TO YOUR REGISTRY ROOKIE****
Contact Information:
Robin L. Schrader, CSTRTrauma PI Coordinator