Successful treatment of presumed death-adder neurotoxicity using anticholinesterases
5
Case Report Successful treatment of presumed death-adder neurotoxicity using anticholinesterases Mark Little and Peter Pereira Department of Emergency Medicine, Cairns Base Hospital Cairns, Queensland, Australia Emergency Medicine (2000) 12, 241–245 Correspondence: Dr Peter Pereira, Director, Department of Emergency Medicine, Cairns Base Hospital, PO Box 902, Cairns, Qld 4870, Australia. Email: [email protected] Mark Little, MB BS, DTM&H(Lon), FACEM, MPH&TM, Senior Registrar, Intensive Care; Peter Pereira, MB, BS, FACEM, Director, Department of Emergency Medicine. History A 49-year-old amateur herpetologist in rural Queensland was bitten over the fifth metacarpal of the left hand by his pet female death adder snake at 18.30 hours. He placed a bandage over the bite site but did not immobilize the limb. By 01.00 hours next morning he noticed worsening ptosis, slurred speech and respiratory difficulty, and presented himself to a country hospital where he was seen by a relieving 2nd- year resident medical officer. He had been bitten on at least 10 previous occasions, and had received antivenom on at least five of these. He reported previous allergic reactions to death-adder antivenom. On arrival at hospital, the patient was alert, with slurred speech, severe ptosis, generalized weakness and some respiratory difficulty. A suboptimal compression bandage was in place, without immobilization. The weakness and respiratory difficulty worsened rapidly in the department. A urine venom detection kit (VDK) was negative. One ampoule of polyvalent antivenom was given intravenously, resulting in immediate improvement of muscle power, but he developed a generalized pruritic, macular rash with partial upper-airway obstruction. He was given 100 µg i.v. adrenaline, with some improvement. Abstract We present the first reported case in Australia of anticholinesterases being used successfully in conjunction with antivenom to treat neurotoxicity following death-adder envenomation. A 49-year-old man was bitten by his pet death adder. He developed significant neurotoxicity due to delayed presentation and suboptimal first aid. Following one ampoule of polyvalent antivenom which produced an allergic reaction, administration of neostigmine and atropine facilitated aeromedical evacuation without the need for mechanical ventilation. After three ampoules of monovalent death-adder antivenom at the receiving hospital, antivenom supplies were exhausted. Further neostigmine and atropine resulted in complete resolution of paralysis, allowing discharge. Anticholinesterases may reduce the dose of antivenom required to treat death-adder envenomation. They may also be of use in cases of allergic reactions to antivenom, and in reducing the need for endotracheal intubation. Key words: anticholinesterases, death-adder envenomation, neurotoxicity.
-
Upload
mark-little -
Category
Documents
-
view
212 -
download
0
Transcript of Successful treatment of presumed death-adder neurotoxicity using anticholinesterases

Case Report
Successful treatment of presumed
death-adder neurotoxicity using
anticholinesterases
Mark Little and Peter Pereira
Department of Emergency Medicine, Cairns Base Hospital Cairns, Queensland, Australia
Emergency Medicine (2000) 12, 241–245
Correspondence: Dr Peter Pereira, Director, Department of Emergency Medicine, Cairns Base Hospital, PO Box 902, Cairns, Qld 4870,Australia. Email: [email protected]
Mark Little, MB BS, DTM&H(Lon), FACEM, MPH&TM, Senior Registrar, Intensive Care; Peter Pereira, MB, BS, FACEM, Director, Departmentof Emergency Medicine.
History
A 49-year-old amateur herpetologist in ruralQueensland was bitten over the fifth metacarpal of theleft hand by his pet female death adder snake at18.30 hours. He placed a bandage over the bite site butdid not immobilize the limb. By 01.00 hours nextmorning he noticed worsening ptosis, slurred speechand respiratory difficulty, and presented himself to acountry hospital where he was seen by a relieving 2nd-year resident medical officer.
He had been bitten on at least 10 previousoccasions, and had received antivenom on at least five
of these. He reported previous allergic reactions todeath-adder antivenom.
On arrival at hospital, the patient was alert, withslurred speech, severe ptosis, generalized weaknessand some respiratory difficulty. A suboptimalcompression bandage was in place, withoutimmobilization. The weakness and respiratorydifficulty worsened rapidly in the department. A urinevenom detection kit (VDK) was negative. One ampouleof polyvalent antivenom was given intravenously,resulting in immediate improvement of muscle power,but he developed a generalized pruritic, macular rashwith partial upper-airway obstruction. He was given100 µg i.v. adrenaline, with some improvement.
Abstract
We present the first reported case in Australia of anticholinesterases being usedsuccessfully in conjunction with antivenom to treat neurotoxicity following death-adderenvenomation. A 49-year-old man was bitten by his pet death adder. He developedsignificant neurotoxicity due to delayed presentation and suboptimal first aid. Followingone ampoule of polyvalent antivenom which produced an allergic reaction, administrationof neostigmine and atropine facilitated aeromedical evacuation without the need formechanical ventilation. After three ampoules of monovalent death-adder antivenom at thereceiving hospital, antivenom supplies were exhausted. Further neostigmine and atropineresulted in complete resolution of paralysis, allowing discharge. Anticholinesterases mayreduce the dose of antivenom required to treat death-adder envenomation. They may alsobe of use in cases of allergic reactions to antivenom, and in reducing the need forendotracheal intubation.
Key words: anticholinesterases, death-adder envenomation, neurotoxicity.
The Cairns Base Hospital Airmedical team (C-AIRMED) was contacted and a retrieval team wasactivated. On their arrival 45 min later, the patient hadgeneralized mild weakness (grade 4/5) and severeptosis. He was assessed as having moderaterespiratory difficulty due to muscle weakness with arespiratory rate of 30 /min. His SaO 2 was 98% on10 L/min via a non-rebreathing mask. Cardiovascularexamination was unremarkable. The macular eruptionwas resolving.
Given the requirement to ascend to 6000 ft for thereturn journey and the accompanying enforcedhypoxia, it was clear that it would be risky to attempttransport without an improved respiratory status. Themanagement choices were intubation and mechanicalventilation, further antivenom administration, and/orthe administration of an anticholinesterase (AChE) toimprove his muscle power. Neostigmine 1 mg and600 µg of atropine were subsequently administered.Although ptosis remained, the AChE resulted insignificantly improved chest expansion. It wasconsidered that there was sufficient improvement (onvisual and symptomatic assessment) to obviate theneed for intubation. The subsequent transport wasuneventful, however, on arrival at Cairns Base Hospitalhe had deteriorated. Although awake and alert, he haddeveloped paralysis of the extraocular muscles andrespiration was difficult.
Investigations revealed a normal full blood count,urea and electrolytes and coagulation profile. Creatinekinase (CK) was elevated at 275 IU. Arterial bloodgases performed on oxygen at 11 L/min non-rebreathing mask, showed pH 7.39, PC O 2 39 mmHg,PO 2 103, HCO3 23, base excess –0.8, SaO 2 98%. Repeaturine VDK was negative.
Due to the clinical picture, and given that thepatient had identified the snake as a death adder, thepatient was given an ampoule of monovalent death-adder antivenom and admitted to the intensive careunit. He showed initial improvement but thendeteriorated. He required a total of 3 ampoules ofdeath-adder antivenom over the next 7 h.
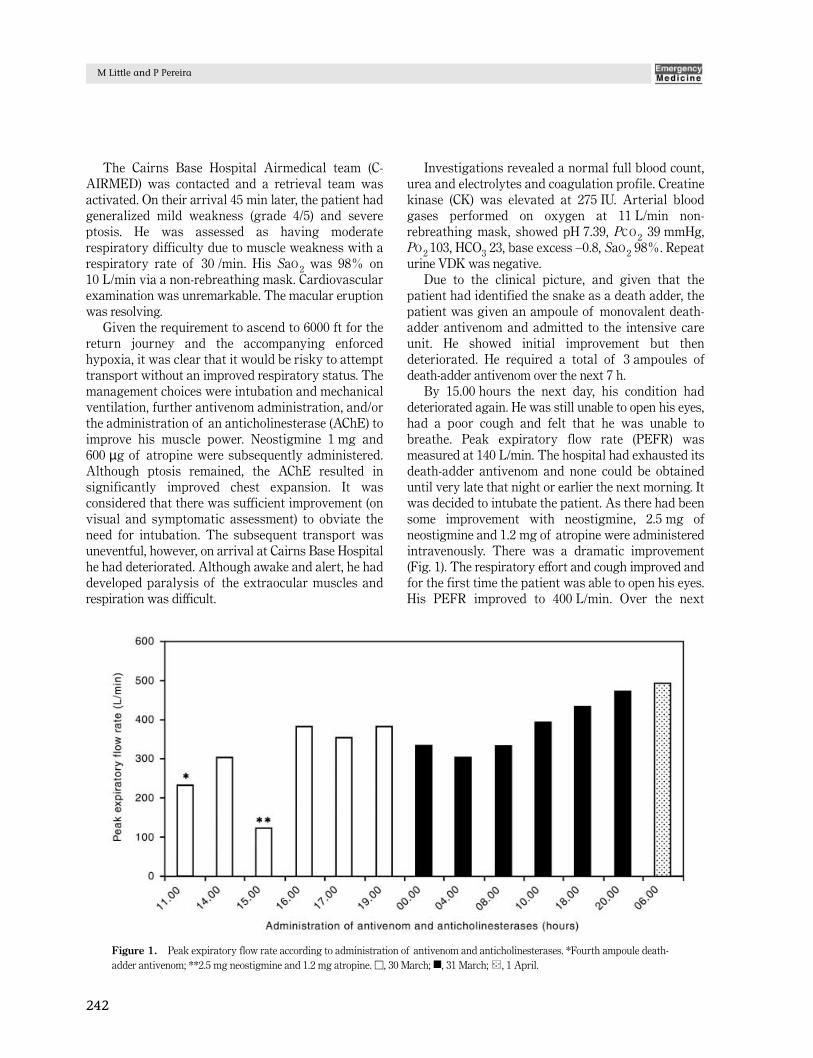
By 15.00 hours the next day, his condition haddeteriorated again. He was still unable to open his eyes,had a poor cough and felt that he was unable tobreathe. Peak expiratory flow rate (PEFR) wasmeasured at 140 L/min. The hospital had exhausted itsdeath-adder antivenom and none could be obtaineduntil very late that night or earlier the next morning. Itwas decided to intubate the patient. As there had beensome improvement with neostigmine, 2.5 mg ofneostigmine and 1.2 mg of atropine were administeredintravenously. There was a dramatic improvement(Fig. 1). The respiratory effort and cough improved andfor the first time the patient was able to open his eyes.His PEFR improved to 400 L/min. Over the next
M Little and P Pereira
242
Figure 1. Peak expiratory flow rate according to administration of antivenom and anticholinesterases. *Fourth ampoule death-adder antivenom; **2.5 mg neostigmine and 1.2 mg atropine. □, 30 March; �, 31 March; , 1 April.

12–24 h he had mild ptosis and weakness but hisgeneral condition was considerably improved and hedid not require any further antivenom. His PEFRremained above 320 L/min. He was discharged home60 h after admission with no symptoms to take a 5-daycourse of oral steroids.
Discussion
The death adder (Acanthophis) is found throughout alarge part of mainland Australia and Papua NewGuinea (PNG). The venom of the death adder is highlyneurotoxic, but has no significant coagulant ormyolytic action.1 A potent neurotoxin, acanthophin-d,has been isolated from the venom. In neuro-physiological experiments this toxin has demonstratedirreversible post-synaptic neuromuscular blockade.2
Envenomation due to Australian and PNG deathadders demonstrates a corresponding clinical picture.Lalloo et al.3 prospectively studied all snakebitespresenting to the Port Moresby General Hospital(PMGH), between March 1990 and June 1992. Of the32 patients presenting with snakebite, 18 had evidenceof envenomation by the death adder. Of thoseenvenomed by the death adder, 17 (94%) hadneurotoxicity, with all demonstrating ptosis. Fivepatients (28%) required ventilation with a median timeof 13 h (range 2–23.5 h) after the bite. Five patients didnot receive antivenom. Of those who did not receiveantivenom, two patients presented late with stableneurological symptoms and three had minor neuro-logical symptoms. There were no deaths reported inthe cases envenomed by the death adder.
In the present case, the patient presented withsignificant symptoms of neurotoxicity. In Australia,the mainstay of treatment of death-adderenvenomation is administration of antivenom, usingmonovalent (if available) or polyvalent. The end-pointfor administration is resolution of neurological signsand symptoms. However, in less developed countries,such as PNG where there is a limited health budget,AChE in combination with antivenoms have been usedto optimize management and decrease treatment costs.4
Death-adder neurotoxicity due to post-synapticacetylcholine receptor blockade has been demonstratedin vitro and in vivo to be susceptible to competitiveinhibition by AChE, such as neostigmine andedrophonium. In one animal study, Wistar rats wereinjected with a lethal dose of crude death adder venom.At the onset of symptoms of envenomation, an AChE
together with atropine, was administered to the rats. Ata minimum lethal dose of venom, all animals survivedas a result.5
The clinical relevance of these experiments hasbeen demonstrated by various authors,1,3,4,6–8 who havesuccessfully used AChE to treat neurotoxicity fromdeath adders and cobras.
In a placebo-controlled, double-blind cross-over trialof intravenous edrophonium in 10 aduts withneurotoxicity as a result of being bitten by thePhilippine cobra, all patients had reversal ofneurotoxic signs.6 Gold,8 reported the successfultreatment of a patient who developed significantneurotoxcity within 3 h of being bitten by his petcobra. Due to a delay in the arrival of antivenom,neostigmine (0.5 mg) was given. This resulted indramatic and complete reversal of symptoms. Thepatient received four doses, approximately every20 min until antivenom was available.
Currie et al.4 reported a case of a PNG man whowas bitten by a death adder. He had a compressionbandage applied for 18 h with no significantsymptoms. Four hours after the bandage was loosened,the patient developed significant symptoms ofneurotoxicity, with ptosis, inability to talk and swallow,and some respiratory difficulty. Death-adderenvenomation was confirmed using the VDK, and thepatient was given 2.5 mg neostigmine and 0.6 mgatropine intravenously. The symptoms resolved in5 min and, 20 min later, he received one ampoule ofantivenom of death adder antivenom with no return ofneurotoxicity.
In another case7 from PNG, a 55-year-old womanpresented 22 h after being bitten by a death adder. Shehad symptoms of mild ptosis and dysarthria whichhad not progressed. Due to the mild neurotoxicsymptoms, she was given neostigmine 2.5 mg, whichproduced complete resolution of symptoms and she didnot require antivenom.
Although it has not been conclusively demonstratedthat our patient suffered his symptoms as a result of adeath-adder bite, it seems almost certain, given the factthat he was an amateur herpetologist who only keptdeath adders and he was bitten by his pet whileattempting to feed it. His clinical presentation ofmuscular weakness in the absence of myotoxicity,coagulopathy or haemolysis is entirely in keeping withthis presumptive diagnosis. Additionally, AChE wouldnot be expected to be of benefit for venoms withpredominantly presynaptic neurotoxicity, such as tigersnakes and taipans. It is of some concern that both
243
Death-adder neurotoxicity

VDK tests proved negative for any antigen; however,this is not uncommon.
We believe this is the first reported Australian casewhere an AChE was used in the management ofsnakebite specifically to competitively inhibit the post-synaptic neurotoxic effects in a case of death-adderenvenomation. Its initial administration allowed the airmedical retrieval team to transfer the patient withoutresorting to intubation and mechanical ventilation. Thedose of 1 mg neostigmine was administered as a testdose and could have been repeated as its effectssubsided. It certainly should have been administeredon arrival at the receiving hospital prior to orconcurrently with the death-adder antivenom, given itsdramatic beneficial effect.
Neostigmine also proved to be an alternative toadministration of a second ampoule of polyvalentantivenom given the presumed allergic reaction to thefirst ampoule. Its use when the hospital death-adderantivenom stock had been depleted allowed resolutionof the patient’s symptoms, dramatically reflected in theimproved PEFR.
The administration of AChE has particularrelevance to the Australian rural setting wheremonovalent antivenom is rarely available, and thenonly in limited quantities. Given the scattered ruralpopulation and the great distances between populationcentres, the administration of an AChE such asneostigmine could prove an important adjunct to themanagement of snakebite where death-adderenvenomation is certain. This would include thesituation of a junior doctor, with limited airway skills,relieving in country hospitals. Here the use of AChEmay help in the short-term relief of significantneurotoxicity until a more experienced practitionerarrives. As neutralization of the venom must takepriority, AChE must not be used to replace antivenom
M Little and P Pereira
244
as the primary mode of treatment. Instead, itsjudicious use may assist in resolving symptomatologyand preventing complications from respiratory failureand generalized skeletal weakness. Additionally, itsadministration may reduce the required dosage ofantivenom.
Both Lalloo3 and Currie et al.4,7 reported caseswhere the administration of neostigmine andantivenom dramatically improved the condition oftheir patients such that they required only one ampouleof antivenom. One patient had no further symptoms,one required ventilation for only 2 h and wasasymptomatic 14 h after antivenom. These casessuggest that there is some potential for reducedantivenom requirements. It is certain that our casewould have required further antivenom shouldneostigmine not have been administered. The financialsavings are obvious in our case because it also allowedthe patient to avoid intubation on two occasions duringthe episode of care.
Conclusion
Although the mainstay of the treatment of snakebite isantivenom, there are situations in the treatment ofdeath-adder envenomation where the use of AChE mayplay a role (Table 1).
Accepted 5 May 2000.
References
1. Hudson BJ. Positive response to edrophonium in death adder(Acanthophis antarcticus) envenomation. Aust. N.Z. J. Med. 1988;18: 792–4.
2. Scheumack DD, Spence J, Tyler MI et al. The complete aminoacid sequence of a post synaptic neurotoxin isolated from thevenom of the Australian death adder snake Acanthophisantarcticus. Comp. Biochem. Physiol. B Comp. Biochem. 1990;95: 45–50.
3. Lalloo DG, Trevett AJ, Black J et al. Neurotoxicity, anticoagulantactivity and evidence of rhabdomyolysis in patients bitten bydeath adders (Acanthophis sp.) in southern Papua New Guinea.QJM 1996; 89: 25–35.
4. Currie B, Fitzmaurice M, Oakley J. Resolution of neurotoxicitywith anticholinesterase therapy in death adder envenomation.Med. J. Aust. 1988; 148: 522–5.
5. Flachsenberger W, Mirtschin P. Anticholinesterases as antidotesto envenomation of rats by the death adder (Acanthophisantarcticus). Toxicon 1994; 32: 35–9.
Table 1. Indications for use of anticholinesterases in thetreatment of death-adder envenomation*
1. Significant envenomation with limited supply of antivenom.2. Envenomed patients with respiratory distress, and medical staff
with limited airway skills.3. Aeromedical transfer, with clinical deterioration, especially in
cases with known significant reactions to antivenom.4. An adjunct in the symptomatic treatment of death-adder
toxicity particularly in the acute setting with severe respiratorycompromise prior to or during antivenom administration.
*The use of an anticholinesterase, such as neostigmine, shouldnever be advocated ahead of death-adder antivenom.

8. Gold BS. Neostigmine for the treatment of neurotoxicityfollowing envenomation by the Asiatic Cobra. Ann. Emerg. Med.1996; 28: 87–9.
245
Death-adder neurotoxicity
6. Watt G, Theakston RDG, Hayes CG et al. Positive response toedrophonium in patients with neurotoxic envenoming by cobras(Naja naja philuippinensis). N. Engl. J. Med. 1986; 315: 1444–8.
7. Currie BJ, Richens J, Korinihona A et al. Anticholinesterasetherapy for death adder envenomation. Aust. N.Z. J. Med. 1990;20: 190.