Successful localization of parathyroid adenomas by magneticresonance imaging
4
IIIIIIIIIII ! I IIII II III SCIENTIFIC PAPERS Successful Localization of Parathyroid Adenomas by Magnetic Resonance Imaging Ralph Hamilton, MD, Burt M. Greenberg, MD, Warren Gefter, MD, Herbert Kressel, MD, and Charles Spritzer, MD, Philadelphia, Pennsylvania Current indications for operative intervention for localization of parathyroid adenomas include severe biochemical, asymptomatic hyperparathyroidism as manifested by a repeatable serum calcium level greater than 11 rag/100 ml, an increased parathy- reid hormone level, increased 24 hour urinary calci- um excretion of more than 150 rag, progressive loss of bone mass, or deterioration of renal function[/]. In addition, operation is likely to be beneficial in hypercalcemic menopausal patients threatened by postmenopausal osteoporosis and in those in whom compliance or follow-up presents a logistic problem [2]. TWenty-five percent of the 60,000 patients screened each year with asymptomatic hyperpara- thyroidism are at risk of complications if left un- treated for several years prior to definitive surgical therapy [3,4]. An enlarged adenomatous parathy- roid gland is thought to be the cause in over 90 percent of case s [5]. Localization of an abnorma ! parathyroid gland before initial operation benefits both the patient and the surgeon by limiting exploration to a specific region, thereby reducing the risk of complications such as damage to the regional laryngeal nerves and normal adjacent parathyroid glands. Furthermore, in one series, initial neck exploration was undertak- en without the benefit of localizing techniques, and in up to 40 percent of patients, it failed to reveal an adenoma. These patients eventually underwent one or more reexplorations [6]. In 10 to 17 percent of patients, reexploration requires a midline sterno- tomy [7,8]. Data suggest that by performing a more conservative operation for a known parathyroid ad: enema, the incidence of transient postoperative hy- Fromthe Department of Radiology, Division of Plastic Surgery, University of Pennsylvania, Philadelphia, Pennsylvania. Requests for reprints should be addressed to Ralph Hamilton, MD, Divisionof Plastic Surgery, Hospital of the University of Pennsylvania, 3400 Spruce Street, philadelphia, Pennsylvania 19104. pocalcemia can be decreased [9]. Radionuclide im- aging using cyanocobalamin, selenomethionine, and toluidine blue were extensively investigated in the 1960s and early 1970s, but results were disappoint- ing due to imaging difficulties and suboptimal sen- sitivity [1]. Interest in thallium-201 has reemerged with the observation that the radioactive potassium analog will localize in abnormal parathyroid glands. Although the proponents of this technique have reported a 70 percent accuracy rate in detecting adenomas, it requires injection of a radioactive iso- tope and an additional scan of the thyroid gland in order to obtain digital subtraction views [I0]. The combination of arteriography and venous parathy- reid hormone sampling has resulted in a 50 to 70 percent accuracy rate, particularly when performed for localization before a difficult reexploration is performed [11,12]. These invasive techniques are painful, risky, and expensive. High-resolution com- puterized tomography is very susceptible to streak artifact and requires an intravenous bolus contrast injection [13]. Prospective and blind retrospective computerized tomography readings correlated with operative findings have revealed an overall sensitiv- ity of between 39 and 78 percent [14-16]. High- resolution real-time ultrasonography is reputed to carry a high accuracy rate in locating large hyper- plastic glands and parathyroid adenomas, but large glands are not delineated when situated in the supe- riot mediastinum behind the trachea or esophagus or deep within the structures of the neck [17]. Magnetic resonance imaging has been shown to easily differentiate thyroid nodules, thyroid cysts, and parathyroid tumors from normal thyroid tissue [18]. It offers excellent soft-tissue resolution with- out the need for contrast agents, it is resistant to motion artifact, and in transverse, sagittal, or cor- onal views can distinguish enlarged parathyroid glands from normal surrounding neck structures. 37Q The American Journal of Surgery
-
Upload
ralph-hamilton -
Category
Documents
-
view
214 -
download
1
Transcript of Successful localization of parathyroid adenomas by magneticresonance imaging

I I I I I I I I I I I ! I I I I I I I I I I
SCIENTIFIC PAPERS
Successful Localization of Parathyroid Adenomas by Magnetic Resonance Imaging
Ralph Hamilton, MD, Burt M. Greenberg, MD, Warren Gefter, MD, Herbert Kressel, MD, and Charles Spritzer, MD, Philadelphia, Pennsylvania
Current indications for operative intervention for localization of parathyroid adenomas include severe biochemical, asymptomatic hyperparathyroidism as manifested by a repeatable serum calcium level greater than 11 rag/100 ml, an increased parathy- reid hormone level, increased 24 hour urinary calci- um excretion of more than 150 rag, progressive loss of bone mass, or deterioration of renal function[/]. In addition, operation is likely to be beneficial in hypercalcemic menopausal patients threatened by postmenopausal osteoporosis and in those in whom compliance or follow-up presents a logistic problem [2]. TWenty-five percent of the 60,000 patients screened each year with asymptomatic hyperpara- thyroidism are at risk of complications if left un- treated for several years prior to definitive surgical therapy [3,4]. An enlarged adenomatous parathy- roid gland is thought to be the cause in over 90 percent of case s [5].
Localization of an abnorma ! parathyroid gland before initial operation benefits both the patient and the surgeon by limiting exploration to a specific region, thereby reducing the risk of complications such as damage to the regional laryngeal nerves and normal adjacent parathyroid glands. Furthermore, in one series, initial neck exploration was undertak- en without the benefit of localizing techniques, and in up to 40 percent of patients, it failed to reveal an adenoma. These patients eventually underwent one or more reexplorations [6]. In 10 to 17 percent of patients, reexploration requires a midline sterno- tomy [7,8]. Data suggest that by performing a more conservative operation for a known parathyroid ad: enema, the incidence of transient postoperative hy-
From the Department of Radiology, Division of Plastic Surgery, University of Pennsylvania, Philadelphia, Pennsylvania.
Requests for reprints should be addressed to Ralph Hamilton, MD, Divisionof Plastic Surgery, Hospital of the University of Pennsylvania, 3400 Spruce Street, philadelphia, Pennsylvania 19104.
pocalcemia can be decreased [9]. Radionuclide im- aging using cyanocobalamin, selenomethionine, and toluidine blue were extensively investigated in the 1960s and early 1970s, but results were disappoint- ing due to imaging difficulties and suboptimal sen- sitivity [1]. Interest in thallium-201 has reemerged with the observation that the radioactive potassium analog will localize in abnormal parathyroid glands. Although the proponents of this technique have reported a 70 percent accuracy rate in detecting adenomas, it requires injection of a radioactive iso- tope and an additional scan of the thyroid gland in order to obtain digital subtraction views [I0]. The combination of arteriography and venous parathy- reid hormone sampling has resulted in a 50 to 70 percent accuracy rate, particularly when performed for localization before a difficult reexploration is performed [11,12]. These invasive techniques are painful, risky, and expensive. High-resolution com- puterized tomography is very susceptible to streak artifact and requires an intravenous bolus contrast injection [13]. Prospective and blind retrospective computerized tomography readings correlated with operative findings have revealed an overall sensitiv- ity of between 39 and 78 percent [14-16]. High- resolution real-time ultrasonography is reputed to carry a high accuracy rate in locating large hyper- plastic glands and parathyroid adenomas, but large glands are not delineated when situated in the supe- riot mediastinum behind the trachea or esophagus or deep within the structures of the neck [17].
Magnetic resonance imaging has been shown to easily differentiate thyroid nodules, thyroid cysts, and parathyroid tumors from normal thyroid tissue [18]. It offers excellent soft-tissue resolution with- out the need for contrast agents, it is resistant to motion artifact, and in transverse, sagittal, or cor- onal views can distinguish enlarged parathyroid glands from normal surrounding neck structures.
37Q The American Journal of Surgery

Localization of Parathyroid Adenomas
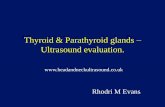
Figure I. ~ Magnetic resonance cross.sectional view of the neck showing parathyroid adenoma (PA), the thyroid lobe ( T), the carotid artery (C), and the Infernal Jugular vein ( J). The view was taken 3.5 cm Inferior to the vocal cords.
Though previous reports have repor ted the identifi- cation of para thyroid glands, the use of a powerful magnetic resonance imaging scanner as a specific preoperat ive localizing technique for pr imary hy- perpara thyroidism has not been repor ted previous- ly [18].
Patients and Methods
Preoperative magnetic resonance imaging scans were obtained in 10 patients. Positive diagnosis required an elevated serum calcium level on at least two separate occasions and an elevated C-terminal parathyroid hor- mone level measured by radioimmunoassay. The preoper- ative serum calcium level ranged from 10.9 to 15 mg/dl (normal range 8.5 to 10.5 mg/dl) and the parathyroid hormone level ranged from 392 to 18,000 pg/ml (normal range less than 340 pg/ml). Malignancy, sarcoidosis, vita- min D intoxication, and idiopathic hypocalciuric hyper- calcemia were excluded by appropriate clinical evalua- tion. No patient had previous exploration of the neck. Physical examination of the neck failed to detect a cervi- cal mass in any patient. Studies on all 10 patients were performed on a General Electric 1.5 tesla superconduc- ting magnet. Spin echo images utilizing both short and long repetition times and echo time were acquired in all cases. Short repetition and echo time (repetition time 600 ms, echo time 20 to 25 ms) pulse sequences were consid- ered spin-lattice relaxation time (T1)-weighted images, whereas long repetition and echo time (repetition time 2,000 to 2,500 ms, echo time 60 to 80 ms) pulse sequences were considered spin-spin relaxation time (T2)-weighted images. Surface coils were routinely used. Using a field of view of 16 cm, pixel size was 0.6 mm by 0.6 mm or 0.6 mm by 1.25 mm, depending on whether a 256 by 256 or a 256
Figure 2. At operation the midpoint of the parathyroid adenoma (tip of forceps) Is measured to be 5 cm Inferior to the superior thyroid notch (not the same patient as In Figure 1).
by 128 matrix was chosen. Images were acquired in the axial plane in all cases. Coronal and sagittal images were obtained selectively to assist in localizing suspected ab- normalities. Distance measurements from the vocal cords to the image thought to represent a parathyroid gland were recorded by sequential imaging at known distances (Figure 1).
The operative approach consisted of a transverse cervi- cal incision with careful midline separation of the pre- thyroidal musculature. Systematic exploration was per- formed with careful attention devoted to the region con- taining the suspected enlarged gland. Normal-sized para- thyroid glands were located and biopsied with care taken to preserve the vascular pedicle. The distance from the thyroid notch, which anatomically correlates with the level of the vocal cords, to the enlarged gland was record- ed, and the enlarged gland was completely removed (Fig- ure 2). The intraoperative anatomic location and size of the gland were correlated with the scan results. Normal postoperative calcium levels confirmed successful resec- tion in all cases, and in no patient was a secondary neck dissection required.
Results
The magnetic resonance imaging scan correct ly predicted the location of the para thyro id adenoma. within a 1.5 cm area in 90 percent of the pat ients (9 of 10 patients). The adenomas ranged in size f rom 2 by 0.2 by 0.4 cm to 4.5 by 1.5 by 1.5 cm (Table I). All glands were found within the predic ted region of para thyroid tissue, and no glands were located in aber rant locations, such as the t racheoesophageal groove, thymus, thyroid gland, or at the m e d i a s t i n a l inlet. In 4 of 10 patients , the abnormal small adeno- ma tha t was present would have been very difficult to localize in the absence of magnetic resonance imaging. A single benign para thyro id adenoma and
Volume 155, March 1988 371

Hamilton et al
TABLE I Clinical and MRI Findings in Eight Patients With Parathyroid Adenomas
Preoperative Serum Values* MRI Findings Operative Findin~ls Calcium C-terminal PTH Distance Distance Size (rag/all) (pg/ml) (cm) Side (cm) Side (cm)
11.9 583 3.5 Right 2 Right 2 by 1.5 by 0.6 11.4 557 3 Right 3.5 Left 1.5 by 1 by 0.4 10.9 1,521 4.5 Left 5 Left 4.5 by 1.5 by1.5 11.9 989 2.5 Right 2.8 Right 1.3 by 0.7 by 1 12.1 302 3.9 Right 3.8 Right 2 by 0.4 by 0.2 13.5 1,315 3.5 Right 5 Right 2.5 by 1.5 by 1 11.8 1,031 3 Right 3,5 Right 1 by 1.5 by 1 !2.8 6,000 1 Rigl~t 1 Right 1.2 by 0.7 by 0.5 12.5 466 1 Left 0,7 Left 0.8 by 0.6 by 0.3 15 18,000 5.5 Right 4 Right 4 by 2 by 1
* Normal values: calcium 8.5 to 10.5 mg/dl and C-terminal parathyroid hormone less than 340 pg/ml. MRI = magnetic resonance imaging; PTH = parathyroid hormone.
one to three normal parathyroid glands were con- firmed by intraoperative pathologic examination. A false-positive reading occurred in a patient in whom a 7 mm adenoma was predicted in the posterior aspect of the right lobe of the thyroid gland; how- ever, a small adenoma was found in the posterior aspect of the left lobe. Few normal parathyroid glands were noted preoperatively, although on ret- rospective review, several additional glands could be identified on magnetic resonance imaging.
Since our operative technique entails localization and biopsy of all four glands, the average operative time of 2 to 3 hours was not significantly reduced. Complications did not develop in any of the pa-. tients.
Comments More traditional techniques of preoperative lo-
calization have been fraught with technical compli- cations, have a low sensitivity rate, and have carried a fair risk to the patient [1,10-17]. Magnetic reso- nance imaging is a safe, noninvasive study that is becoming increasingly available in clinical practice.
Magnetic resonance imaging produces cross-sec- tional tomographic images with higher soft-tissue resolution when compared with cQmputerized to- mography or ultrasonography. Magnetic resonance imaging images derive from the interaction of ra- diowaves and atomic nuclei with an odd number of protons. The hydrogen nucleus, a single proton atom, is the most abundant, and yields the strongest signal. T1 is the measure of the time it takes for protons to resume their random state after excita- tion from administered radiowaves, T2 is a measure of the time it takes for atoms to assume perfect lock- Step procession after initial excitation [I9]. The val- ues of both of these parameters change with tissue type and with disease process. The magnetic reso- nance imaging technique is particularly well suited in an area such as the neck, where juxtaposition of
soft-tissue masses is complex but the relaxation time of each structure is discrete. Magnetic reso- nance imaging has the combined advantages of computerized tomography and ultrasonography in that both the neck and the thoracic inlet can be examined without streak artifacts, and vascular structures can be separated from soft-tissue masses without the infusion of intravenous contrast materi- al. Furthermore, the anatomic resolving power of the new 1.5 tesla scanner is equal or superior to computerized tomography and ultrasonography.
Magnetic resonance imaging is a clinically signifi- cant diagnostic modality that is becoming available to head and neck surgeons. Based on the early expe- rience presented herein, enlarged and often normal- sized parathyroid glands can be localized. No pa- tient presented with thoracic inlet tumors, nor was any parathyroid gland or adenoma found in aber- rant locations. We encourage centers with magnetic resonance capability to continue to expand the knowledge base in assessing the neck and to help determine the role of magnetic resonance in identi- fying parathyroid adenomas that may not be found in the standard neck dissection. With improve- ments in spatial resolution, an even greater increase in electromagnetic field strength, and further expe- rience with tissue characterization, it appears likely that magnetic resonance imaging may be able to accurately localize both normal-sized and ectopic parathyroid glands.
Summary Exploration of the neck for primary hyperpara-
thyroidism is facilitated if the parathyroid glands can b.e localized preoperatively. Magnetic resonance imaging is a noninvasive and relatively safe proce- dure that is capable of distinguishing and differenti- ating small soft-tissue structures.
Ten patients with primary hyperparathyroidism underwent preoperative diagnostic magnetic reso-
372 The American Journal of Surgery

Localization of Parathyroid Adenomas
nance imaging followed by cervical exploration. In 9 of these patients (90 percent), imaging correctly predicted the location of a single enlarged parathy- roid gland, and in one patient the findings were misleading. All 10 patients proved to have single adenomas in orthotopic locations. Based on this early experience, magnetic resonance imaging ap- pears to be a promising technique for preoperative localization of an enlarged parathyroid gland.
References
1. LaRose JH, Whitaker RH, Reba RC. Radioiodinated toluidine blue: an unsatisfactory scanning agent. J Nucl Mad 1970; 11: 731-2.
2. Gaz RD, Wang C. Management of asymptomatic hyperpara- thyroidism. Am J Surg 1984; 147: 498-501.
3. Hodgson SF, Heath H. Asymptomatic primary hyperparathy- roidism: treat or follow. Mayo Clin Proc 1981; 56: 521-2.
4. Scholz DA, Purnell DC. Asymptomatic primary hyperparathy- roidism. Mayo Clin Proc 1981; 56: 473-8.
5. SaubierEL, FaysseE, GouillaC. Surgical treatment of primary hyperparathyroidism. Evaluation of 263 cases. J Chir (Par- is) 1983; 120: 693-9.
6. MacFarlane SC, Hanelin LG, Taft DA, Ryan JA, Fredlund PN. Localization of abnormal parathyroid glands using thallium- 201. Am J Surg 1984; 148: 7-11.
7. Wang C, Parathyroid reexploratlon. A clinical and pathological study of 112 cases. Am J Surg 1977; 186: 140-5.
8. Edis AJ, Sheedy DF, Beahrs OH, van Heerden JA. Results of reoperation for hyperparathyroldism with evaluation of pre- operative localization studies. Surgery 1978; 84: 384-93.
9. Kaplan EZ, Suglmoto J, Bartlett S, Fredlund A. Postoperative
hypocalcemia: its relation to operative technique. Ann Chir Gynaecol 1983; 72: 146-52.
10. MacFarlane SD, Hanelin LLG, Taft DA, Ryan JA, Fredlund PN. Localization of abnormal parathyroid glands, Am J Surg 1984; 148: 7-11.
11. Makaraimen H, Lahde S, Kairaluoma MI, Leinonen A. Preoper- ative localization of enlarged parathyroid glands. Ann Clin Re s 1984; 40: 51-4,
12. Brennan MT, Doppman JL, Kirdy AG, Marx SJ, Spiegel AM, Aurbach GD. Assessment of techniques for preoperative parathyroid gland localization in patients undergoing reo- peration for hyperparathyroidism. Surgery 1982; 91: 6-11.
13. Stark PD, Moss AA, Gooding GA, Clark OH. Parathyroid scan- ning by computed tomography. Radiology 1983; 148: 297- 9.
14. McMillan NC, Smith L, McKellar N J, et al. The localization of parathyroid tumors: a comparison of computed tomogra- phy with cervical vein hormone assay. Scott Med J 1983; 28: 153-6.
15. Skibber JM, Reynolds JC, Spiegel AM, eta!. Computerized technetium thallium scans and parathyroid reexploration. Surg Gynecol Obstet 1985; 161: 101-5.
16. Stark DD, Gooding HA, Moss AA, Clark OH, Orefors CO. Parathyroid imaging: comparison of high resolution CT and high resolution sonography. Am J Radio11983; 141: 633-8.
17. Clark OH, Stark DA, Duh AY, Arnaud CD, Goodlng GA. Value of high resolution real-time ultrasonography in secondary hyperparathyroidism. Am J Surg 1985; 150: 9-17.
18. Stark DD, Clark OH, Moss AA. Magnetic resonance imaging of the thyroid, thymus, and parathyroid glands. Surgery !984; 96: 1083-90.
19. Greenberg BM, Mezrlch R, Prymak C, Kressel H, LaRossa D. Application of magnetic resonance imaging technique in determining canine muscle and human free flap viability. Plast Reconstr Surg 1987; 79: 959-65.
Volume 155, March 1988 373