
SUCCESSES AND CHALLENGES OF VACCINATION PROGRAMS: … · SUCCESSES AND CHALLENGES OF VACCINATION...
44
SUCCESSES AND CHALLENGES OF VACCINATION PROGRAMS: FROM DEVELOPMENT TO IMPLEMEANTION Giuseppe Pantaleo, M.D. Professor of Medicine Head, Division of Immunology and Allergy Executive Director, Swiss Vaccine Research Institute Lausanne University Hospital, Lausanne, Switzerland 1
Transcript of SUCCESSES AND CHALLENGES OF VACCINATION PROGRAMS: … · SUCCESSES AND CHALLENGES OF VACCINATION...

SUCCESSES AND CHALLENGES OF VACCINATION PROGRAMS:FROM DEVELOPMENT TO IMPLEMEANTION
Giuseppe Pantaleo, M.D.
Professor of Medicine
Head, Division of Immunology and Allergy
Executive Director, Swiss Vaccine Research Institute
Lausanne University Hospital, Lausanne, Switzerland
1

Infectious Disease Burden and Vaccination
According to WHO reports
▪ “nearly 9 million children under 14 years of age die everyyear from infectious disease. And at least 1/3 (3 million)of them could be saved if existing vaccines were morewidely used, but the rest only if suitable new vaccineswere developed”

Continues Generation of Novel Vaccins

General Concepts
• Vaccine and acute infection
– If the disease follows the infection, the cure is associated with the elimination of the infection and of the pathogen
– The immune response induced by the disease is generally protective against the same the disease over time
– The vaccine must induce an immune response similar to that generatedby the natural infection
• Vaccine and chronic infection
– Persistence of a pathogen capable of evading the host immune response
– The immune response induced by the infection is not sufficient to prevent super-infection
– The vaccine must induce an immune response different from thatgenerated during the natural infection

General Concepts
• Ratio benefit/risk of the vaccination
– A vaccine is an immunologic active substance
– Side effects are expected but must be minimized
– The side effects should be compared to the benefits expected by
the vaccination
• All the components of the vaccine may contribute to the side
effects
– Active substance
– Adjuvant
– Formulation
General Concepts
• Preventative Vaccine
– Product administered to an healthy person to induce an immune responsespecific and persistent over time in order to prevent the occurrence of a certain disease
– Almost all the available vaccines have the above properties
• Therapeutic Vaccine
– Product administered to an ill person with the objective of
• Reducing the symptoms of the disease
• Blocking the progression of the disease
– It induces a novel immune response or modulates the existing immune response
– Only one therapeutic vaccine in the market (immunotherapy for prostate cancer)
• Sipileucel-T (PROVENGE™)
– Le BCG is used in the case of bladder cancer but the effec is non-specific(immunostimulation)

General Concepts• Active Immunization
– Induction of specific immune reponse(s) to
• One or multiple antigen(s) administered) (killed vaccine) or
• Produced by the pathogen itself (live vaccine)
– Achievement of a durable effect, induction of immunological memory
• Passive Immunization
– Transfert of the effector components of the immune system specific to
an antigen from one person to another person
• Antibodies
• Cells
– Effect waining over time, no immunological memory
• Immunostimulation/Immunomodulation
– For exemple Toll-like receptors
– Non-specific enhancement of the immune responses
– Effect limited over time
Types of Vaccines
• Live attenuated
– Replicate in the target species but have lost virulence
• Adaptation occurs through passages in artificial
conditions
– Different animal species/organ
– Fetal eggs
– Cell cultures
• Adaptation is associated with mutations
– Genetic stability to prevent reversion
• Contribution of the immune system to teh
attenuated phenotype
– No vaccination in immunodeficient patients
– Immune response qualitative similar to that induced by
the virulent pathogen but generally quantitative weaker
• Protection induced generally of limited durability
(re-call necessary)
Examples of live vaccines • BCG• Smallpox• Yellow fever• Measles, Rubella,
Mumps and Varicella• Oral Polio• Rotavirus• Flu intranasal
Types de vaccines
• Inactivated
– Whole killed organisms
• Heat
• Formaldehyde
• β-propiolactone
– Risk of denaturation of antigens
– Reponse broad against protective et
non protective antigens
– Integrated adjuvant
• Stimulation Toll-like receptors
Enhancement of immune response
• Side effects more severe than with
purified proteins
Exemples de vaccins inactivés• Pertussis (wP vaccine)• Tick-bone Encephalitis• Japonese Encephalitis• Inactivated Polio i• Hepatitis A• Rabbies• Fklu
Cutter Laboratories 1955: Plus de 200 000 enfants vaccinés, 40 000 cas de polio avec 200 enfants plus ou moins paralysés et 10 décès

Types de vaccines
• Toxines
– Disease caused by the effect of toxins
– Toxin modification
• Preserved antigenicity
• Inactivation of toxic activity
– Heat
– Formaldehyde
– Glutaraldehyde
– Genetic
Examples of toxinvaccines• Diphtheria (D)• Tetanos (T)• Pertussis (PT dans
vaccin aP)
• The diphtheric et tetanos toxins are used as carrier proteines for conjugated polysaccharide vaccines
• CRM197 is a genetically attenuated diphteric toxinused as carrier protein within Prevenar-13

Types de vaccines
• Sub-unit– Purified proteins/Recombinant purified proteins
• Immunogenicity variable
• Generally transient response and need for multiple
administrations
– Pseudovirions
• Presentation of repetitive structures
– Optimal stimulation of B cells
• Often very immunogenic and long-lasting protection
Examples of sub-unit vaccines • Acelluar Pertussis
(aP vaccine)• Flu (Influvac)• HepB*• HPV*• HSV gB/gD (non
protective)• HIV gp120
*: Pseudovirions
pseudovirions of papillomavirus type 16 (University of Münster)

Types de vaccines
• Polysaccharides et conjugated
– Main antigens of capsulated bacteria
– Induction of reponses T-independent
• No immunological memory, non boostable
• Weak reponse in young chilidren
• Reponses of short durability
– Conjugation with a carrier protein (toxin, other bacterial
proteins)
• Immunological memory
• Good reponse in young children
• Boostable
Examples of vaccines polysaccharides et conjugated• Hemophilus influenzae type b
(Hib)• Streptococcus pneumoniae
(Prevenar-13)• Neisseria meningitidis group A, C,
Y, ou W135• Salmonella typhi
Properties Polysaccharide Conjugated
Immunogenicity in infants < 2 years Non Oui
Reponse dependent of B cells Oui Oui
Reponse dependent of T cells Non Oui
Memory Non Oui
Boosting Non Oui
Long-term protection Non Oui
Group immunity Non Oui

Types de vaccines
• Combinations
– Several serotypes of the same
pathogen
– Different mixtures of vaccines to
reduce the number of injections
– Absence of interaction to be verified
• Product
– Risk of loss of the
adjuvantation
• Immunological competition
between antigens
Examples of combined vaccines• DTP• Méningitis tetravalent (A, C,
W, Y135)• Pentavalents (D, T, aP, HepB,
Hib)• Hexavalents (D, T, aP, HepB,
polio, Hib)• pneumo conjugated 7- and
13-valent (Prevenar-7 and Prevenar-13
• pneumo conjugated 10-valent (Synflorix)
• pneumo conjugated 15-valent under development(V114)

Types de vaccines
• Recombinant Viruses– Highly attenuated non-replication competent viruses
expressing antigens of interest
• Poxvirus (vaccinia, canarypox, …)
• Adenovirus
• Virus de la rougeole
• CMV
– Chimeric virus
• Yellow Fever virus 17D / virus of the japonese encephalitis
• Yellow Fever virus 17D / Dengue virus
Examples of combinedvaccines• Several recombinant
poxvirusenregisregistered in veterinary medicine
• Vaccines underdevelpement against HIV, TB, etc.
• Vaccine against japoneseencephalitis (Imojev, commercialized in Asiasince 2013)
• Vaccine against Dengue
Brand Vector/Antigen Produceur
Raboral™ Vaccinia/Rage Merial 1994
VectorVax™ FP N Fowlpox/Newcastle Syntro Corp 1994
TROVAC™-NDV Fowlpox/Newcastle Merial 1995
TROVAC™-AIV H51 Fowlpox/Influenza aviaire Merial 1998
Recombitek™-CVD Canarypox/Mal. de Carré Merial 1997
Purevax™-Rabies Canarypox/Rage Merial 1998
Eurifel™ FeLV Canarypox/FeLV Merial 2000
Vectormune™ FP ILT Fowlpox/Inf laryngotracheitis CEVA 2002
Vectormune™ FP NDV Fowlpox/Newcastle CEVA 2002
Vectormune™ FP MG Fowlpox/Mycoplasma CEVA 2003
ProtEQ™ FLU Canarypox/Grippe équine Merial 2003
Recombitek™ WNV Canarypox/WNV Merial 2003
Veterinary recombinant vaccines rergistered
Types de vaccines
• Nucleic acids
– DNA
Gene Gun
Examples of DNA vaccines • Westnile fever(horse)• Necrosant
hematopoietic virus i (salmon)
• Melanoma (dog)• Experimental vaccines
for Vaccin HIV, HBV, and different cancers
Electroporation
Plasmide

Virus reassortant
• Une autre forme de virus chimérique (non recombinant)
• Concerne les virus à génome segmenté– Rotavirus: 11 segments d’ARN double brin
• Protéines structurales: VP1, 2, 3, 4, 6 et 7
• VP4 et VP6 impliquées dans la protection
– Influenza: 8 segments d’ARN simple brin de polarité négative
• Protéines structurales: HA, NA, M1, M2, NP
• HA et NA impliquées dans la protection
• Souche A/Puerto Rico/8/34 utilisée comme base pour la production à haut rendement dans les oeufs
• Obtention des virus réassortis– La co-infection de cellules par deux virus
résulte en la production de virions comprenant toutes les combinaisons viables de segments
– La combinaison recherchée est sélectionnée (neutralisation ou hybridation sur plages de lyse)
Source: NIAIDSource: Wikipedia
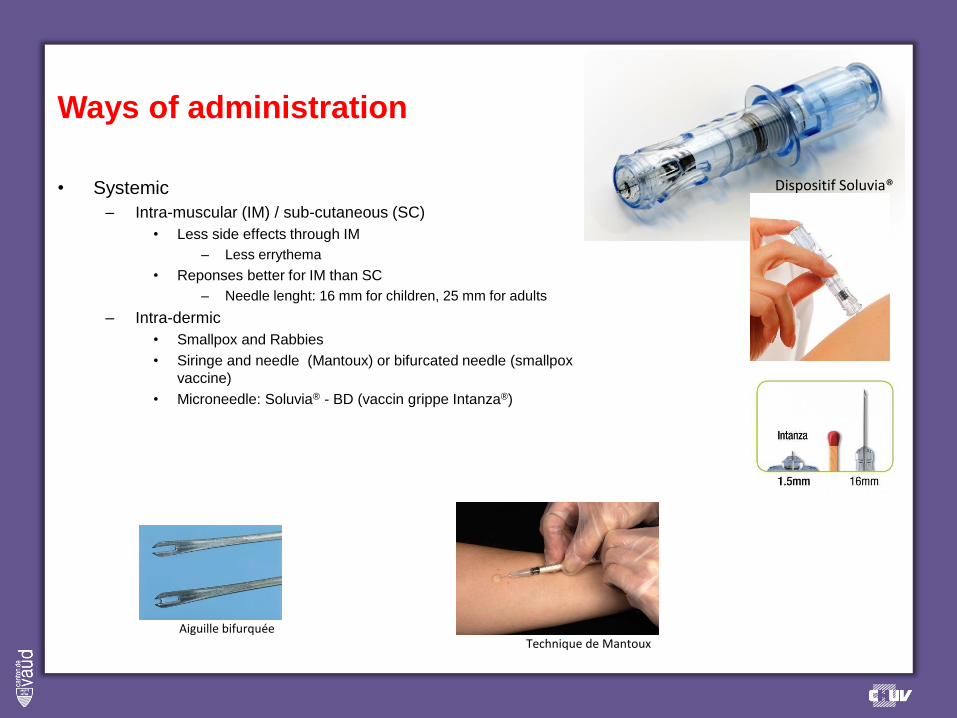
Ways of administration
• Systemic
– Intra-muscular (IM) / sub-cutaneous (SC)
• Less side effects through IM
– Less errythema
• Reponses better for IM than SC
– Needle lenght: 16 mm for children, 25 mm for adults
– Intra-dermic
• Smallpox and Rabbies
• Siringe and needle (Mantoux) or bifurcated needle (smallpox
vaccine)
• Microneedle: Soluvia® - BD (vaccin grippe Intanza®)
Technique de MantouxAiguille bifurquée
Dispositif Soluvia®

Ways of administration
• Oral: Induction mucosal immunity
– Live attenuated vaccine against polio
• One serotype or a mixte of 3 serotypes
– Live attenuated vaccine against rotavirus (Rotateq, Rotarix)
• Virus attenuated or ressortants
– Inactivated vaccine inactivé against cholera (Dukoral)
• Whole kilkled bacteria of V. cholerae O1 Classical et El Tor
• The non toxic B sub-unit of the cholera toxin

Ways of administration
• Nasal
– Mucosal immunization
– Natural way of infection better response ?
– Explored for Flu
• Live attenuated vaccine: Flumist® (MedImmune)
• Inactivated trivalent yearly vaccine with adjuvant (LT)
– Neurologic side effects: facial paralysis of Bell
– Product retired from the market
Conclusion• Acceptable only for des live vaccines (Flumist®)• For the adjuvant, risk linked to the sensitivity of the facial nerve • Protection similar to a systemic vaccination

Comment les vaccins protègent-ils?
• Une infection est un processus exponentiel La prévention d’une infection doit privilégier la
rapidité d’action, l’inactivation du pathogène avant qu’il ne puisse se répliquer ou infecter les
cellules
– C’est typiquement le rôle des anticorps!
• Neutralisation directe
• Opsonisation pour élimination par les phagocytes
• Opsonisation pour lyse du pathogène médiée par le complément
– Les cellules T cytotoxiques ne peuvent agir que si des cellules sont infectées
• Dans le cas des vaccins préventifs, c’est la préexistence de la réponse immunitaire qui est
critique
– Anticorps sériques: effet immédiat (pour infections aigües)
– Mémoire immunitaire: induction rapide d’une réponse effectrice (pour infection lentes)
• Hépatite B
• Rage
• Dans le cas d’un vaccin thérapeutique, la réponse préexistante naturelle doit être modulée pour
augmenter en efficacité, le facteur temps est moins critique
• Dans tous les cas les deux bras de l’immunité sont nécessaires, il n’y a pas d’anticorps sans
cellules T!

Corrélats de protection
• Les anticorps sont utilisés par défaut comme corrélats de protection (CoP) pour les vaccins en
développement
– Pour des raisons pratiques, un CoP de protection doit être choisi avant de commencer le développement de
la dose et du calendrier d’immunisation d’un nouveau vaccin
– Ce choix doit être justifié par la biologie de l’infection
– La réponse humorale est un bon CoP pour des raisons pratiques et théoriques
• Il est spécifique et a une forte probabilité d’être directement impliqué dans le mécanisme de protection
• Il peut être mesuré de manière spécifique, précise et reproductible
• Les anticorps sont au minimum un bon indicateur que le système immunitaire a vu l’antigène
• Toutes les études réalisées à ce jour montrent que les anticorps fonctionnels sont des CoP pour
tous les vaccins préventifs existants excepté pour le vaccin BCG
– N’exclut pas l’existence d’autres CoP (cas du vaccin contre le zona)
– Un corrélat n’est pas nécessairement impliqué dans le mécanisme responsable de la protection
– Ne signifie pas que d’autres effecteurs ne sont pas importants (il faut des Th pour obtenir des IgG)
– Pour beaucoup de pathogènes, l’apparition de symptômes nécessite la dissémination du pathogène par la
voie sanguine et une généralisation de l’infection
Corrélat
Pro
tect
ion

Corrélats de protection
• Un corrélat de protection est défini
par deux paramètres
– Type de mesure
– Seuil de protection
• Sans surprise, les anticorps
corrèlent avec la protection pour
pratiquement tous les vaccins
existants
• Cela ne veut pas dire l’immunités
cellulaire ne contribue pas à la
protection
• Les cellules B mémoire peuvent
médier la protection si la réponse
anamnestique est plus rapide que le
pathogène. C’est le cas pour
l’hépatite B et peut-être pour la rage
Vaccin Corrélat de protection Seuil
Variole Neutralisation 1/20 dil
Diphtérie Neutralisationd e la
toxine
0.01-0.1 IU/mL
Hépatite A ELISA 10 mIU/mL
Hépatite B ELISA 10 mIU/mL
Rougeole microneutralization 120 mIU/mL
Grippe HAI 1/40 dil
Coqueluche ELISA 5 units
Pneumocoque ELISA;
Opsonophagocytose
0.20-0.35 µg/mL
(enfants); 1/8 dil
Meningocoque Bactéricidie 1/4 dil (human
complement)
Fièvre jaune Neutralisation 1/5 dil
Zona Neutralisation; cellules
T CD4+
Non défini
Varicelle Neutralisation, ELISA
(gp)
1/64 dil; 5 IU/mL
Virus du papillome
humain
Anticorps neutralisants Non définis

Antigène polysaccharidique
• Epitopes répétés qui permettent une stimulation des cellules B par regroupement des récepteurs à la surface des cellules B
• Absence d’engagement des cellules T car l’antigène est non protéique (pas d’épitope T)– Réponse non associée à un centre germinatif dans un ganglion lymphatique ou dans la rate
– Induction d’une réponse IgM et IgG mais sans maturation d’affinité
• Réponse de courte durée, au mieux quelques années
• La protection est plus faible et de moins longue durée chez les enfants que chez les adultes
• La revaccination permet d’augmenter le titre en anticorps mais généralement pas au même niveau qu’après la première injection
• Exemples– Vaccin contre la méningite à méningocoque (Neisseria meningitidis)
– Vaccin contre la pneumonie (Streptococcus pneumoniae)
Exemple de vaccin polysaccharidique
Seuil de protection
Titr
e A
nti
corp
s
Temps
Dose 1 Dose 2
Réponse primaire

Antigène protéique
• Stimulation des cellules B
• Engagement des cellules T et– Formation de centres germinatifs dans un ganglion lymphatique ou dans la rate
– Induction d’une réponse IgM et IgG avec maturation d’affinité
• Réponse de durée variable, de plusieurs mois à plusieurs années
• Généralement deux injections distantes d’environ un mois pour maximiser la réponse primaire
• La réponse anticorps décroît dans le temps et atteint un plateau en 2 à 3 ans
• La nécessité de rappels dépend du seuil de protection, du plateau et de l’antigène
• Exemples– Protection de courte durée: vaccin coqueluche acellulaire (PT, FHA, PRN, FIM-2, FIM-3)
– Protection de durée moyenne: anatoxine tétanique ou diphtérique
– Protection de longue durée: vaccin hépatites A et B et papillomavirus humains
Titr
e A
nti
corp
s
Temps
Dose 1+2 Rappel 1 Rappel 2
Seuil de protection
Réponse anamnestique
Réponse primaire
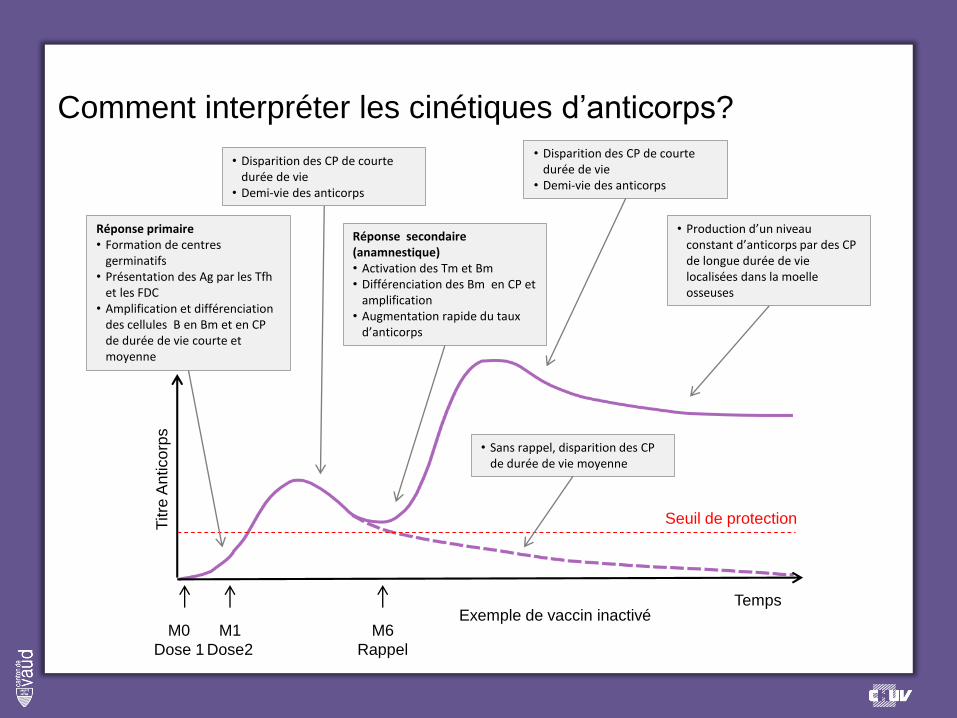
Comment interpréter les cinétiques d’anticorps?
M0
Dose 1
M1
Dose2
M6
Rappel
Titre
An
tico
rps
Temps
Seuil de protection
Exemple de vaccin inactivé
Réponse primaire• Formation de centres
germinatifs• Présentation des Ag par les Tfh
et les FDC• Amplification et différenciation
des cellules B en Bm et en CP de durée de vie courte et moyenne
• Disparition des CP de courte durée de vie
• Demi-vie des anticorps
Réponse secondaire (anamnestique)• Activation des Tm et Bm• Différenciation des Bm en CP et
amplification• Augmentation rapide du taux
d’anticorps
• Sans rappel, disparition des CP de durée de vie moyenne
• Disparition des CP de courte durée de vie
• Demi-vie des anticorps
• Production d’un niveau constant d’anticorps par des CP de longue durée de vie localisées dans la moelle osseuses

Small Pox
26
Very Contagious disease caused by variola virus(orthopoxvirus)
The most devastating disease known to humanity
No treatment ever developed, killed as much as 30% ofthose infected, 65 to 85% of survivors marked with deeppitted scars on the face, blindness was a commoncomplication
When Spanish conquistadors introduced smallpox in theNew World, the indigenous population shrank from 25millions down to 1.6 millions in less than a 100 years

Smallpox: Immune correlates of protection
27
Specific antibodies induced can prevent smallpoxinfection
Against disseminated disease both antibodies andspecific CD4 and CD8 responses are necessary. Whenantibodies are waning after smallpox vaccination, diseasemay occur. However the disease is milder. This resistanceto clinically typical smallpox depends on memory T cells

Promotion of vaccination over variolationFirst mass vaccination oversea expedition (to Spanish colonies in the New World) living chain
Establishment of the National vaccine Institute 28
1796 -1798
Edward JennerInoculation of Cowpox to James Phipps followed by variolation. No reactiongto variolation observed
1898-1902
Regulation of Vaccine supply IncreasesContamination Leads to Stronger Regulations: Adoption of The Biologics Control Act
First US vaccination LawMassachusetts passed the first U.S. law mandating vaccination for schoolchildren.
1855
Waterhouse bring vaccination to the United StatesAround 100 000 people vaccinated worldwide
1800-1815 1820
Decrease in mortality due to smallpox in London
Development of Freeze-Dried Vaccine The Vaccine Institute in Paris produced a freeze-dried vacuum-packed smallpox vaccine used in tropical climates
1918
28
Advances in Vaccine ProductionVaccine FarmsAddition glycerin to lymph as germicide reducing transmission of harmful microbes
1891
Publication of Jenner’s results“Inquiry” at his own expense
French Doctors Investigate Animal VaccineAwareness of the danger of the spread of diseases such as syphilis via arm-to-arm transmission The use of calves for vaccine material came to be widespread
1864

A Massive Vaccination EffortNew York City Mayor William O’Dwyer to residents who had not been recently vaccinated to be vaccinated against the disease. In the next month, 80% of the city’s residents were vaccinated—some 6.35 million people
1947
2929
1922
SchoolVaccination RequirementsUnited States schools required smallpox vaccination before children could attend
1958
Assembly Aims for EradicationThe Twelfth World Health Assembly adopted a goal of global smallpox eradication
29
Changes in Vaccine ProductionThe newly established World Health Organization issued a report praising the freeze-dried vacuum-packed vaccine from the Vaccine Institute in Paris. Production of the vaccine soon spread around the world
1948 1972
Routine U.S. Smallpox Vaccination CeasesContamination Leads to Stronger Regulations: Adoption of The BiologicsControl Act
The Bifurcated NeedleWyeth Laboratories patented the bifurcated needle for delivery of smallpox vaccine.Rrequiredslessvaccine material for each dose, easier than previous methods. large implications for smallpox vaccination campaigns
1965
WHO Pushes Eradication Effortslaunched the Intensified Smallpox Eradication Programmesmallpox was endemic in 30 countries (mainly in developing countries). • Mass vaccinations using freeze-dried vaccine material• Development of a system to detect, monitor, and investigate smallpox cases and contain outbreaks. Three principles were vital to the program’s success: participation from all countries, with solid coordination; adaptability as national programs were implemented; and ongoing research to evaluate progress and deal with problems that might arise
1969
Smallpox DeclaredEradicatedThe World Health Assembly accepted the WHO Global Commission’s recommendation and declared the world free from smallpox
8th May1980
1950s: 50 million cases of small pox per year worldwide
Last Wild Case of Variola MinorAli Maow Maalin, a cook in Merca, Somalia
1977

Small pox eradication
Vaccine (live vaccinia virus) is very effective in preventingdisease even administered up to 4 days after virusexposure
High vaccine coverage worldwide, easy to administer
No animal reservoir
Smallpox does not survive if it does not go from person toperson
From vaccine discovery to eradication: 84 years30

Poliovirus
31
Highly infectious RNA virus belonging to the human enterovirusof the Picornaviridae family, causing for poliomyelitis
Isolated in 1909 by Dr Landsteiner and Dr Popper
3 serotypes of poliovirus, PV1, PV2, and PV3; each with a slightlydifferent capsid protein
Most poliovirus infections cause asymptomatic viral replicationthat is limited to the intestinal tract. Around 25 % of infected willdeveloped minor illness and 1% will develop paralyticpoliomyelitis. Persistent paralysis and deformities are commonsequeleas of polio

Poliovirus: immune correlates of protection
32
▪ Individuals who are exposed to poliovirus, either through infection or by immunization with the vaccine develop immunity. Antibodies are present in the tonsils and gastrointestinal tract (IgA) and are able to block poliovirus replication. IgG and IgM Abs prevent spread of the virus to motor neurons of the central nervous system
▪ Infection with one serotype of poliovirus does not provide immunity against the other serotypes
▪ Vaccines: ▪ Salk vaccine, or inactivated poliovirus vaccine (IPV), based on three wild
reference strains, Mahoney (type 1 poliovirus), MEF-1 (type 2 poliovirus), and Saukett (type 3 poliovirus)
▪ Oral polio vaccine (OPV), live-attenuated, produced by the passage of the virus through non-human cells at a sub-physiological temperature, which produces spontaneous mutations in the viral genomes

3333
1894
First U.S. Polio Epidemic
Early Polio Vaccine Trialstwo separate teams were at work developing and testing a polio vaccine. Both projects came to disastrous ends.At New York University, Dr Maurice Brodie, prepared a killed poliovirus vaccine. He enrolled about 11,000 individuals (in both control and vaccine groups) in his trial.Dr John Kolmer, of Temple University in Philadelphia developed an attenuated poliovirus vaccine, which he tested in about 10,000 children.The tests proved a disaster. Several subjects died of polio many were paralyzed, made ill, or suffered allergic reactions to the vaccines.
19351908
Poliovirus IdentifiedDr Karl Landsteiner and Dr Erwin Popper, announced that the infectious agent in polio was a virus
33
1905
Contagious Nature of Polio DiscoveredDr Ivar Wickman (1872-1914) suggested that polio was a contagious disease that could be spread from person to person and recognized that polio could be present in people who did not appear to have a severe form of the disease.
Breakthrough in Culturing VirusesIn Boston, the team of Dr John Enders showed that they could grow polioviruses in non-nervous tissue—namely human embryonic skin and muscle tissue
1949
More Than One Type of Poliovirus Proposed
1931
Salk Begins Early Polio Vaccine Testsfirst tests in humans of their killed-virus polio vaccine.
1952
Massive Polio Vaccine Trial Begins in U.S. Salk’s polio vaccineover 1.3 million children participated in the trial.randomized, double-blind test
1954 1955
Polio Vaccine Results AnnouncedDr Thomas Francis announced the results of the Salk poliovirus vaccine trial. The vaccine, they said, was 80-90% effective against paralytic polio.The U.S. government licensed Salk’s vaccine later this same day.
1950
Koprowski Tests Polio Vaccine in Childrenfirst human trial of his attenuated oral poliovirus vaccine

343434
Goal Set for Polio Eradication in the AmericasPan American Health Organization (PAHO), announced a campaign to achieve polio eradication in the Americas by 1990.
1985
34
1959
Soviet Trials of Sabin's Live Attenuated Poliovirus VaccineAlbert Sabin forged a bond with Soviet health officials, who were interested in a cheaper alternative to Salk’s vaccine.
2000
99% Reduction in Polio Cases worldwide
2012
Polio Vaccination Programs ContinueAs of the end of 2012, polio remained endemic in only three countries: Afghanistan, Nigeria and Pakistan
1997
IPV Returns to U.S. ScheduleAn improved version of Jonas Salk’s inactivated poliovirus vaccine began to be given to U.S. children before giving the OPV. An average of 8-10 cases of vaccine-derived polio per year were caused by the OPV (about 1 case per 2.4 million doses distributed). In the absence of wild-type disease, the public and authorities began to deem the risk from the vaccine unacceptable.By 2000, transition to an all-IPV schedule would be complete.
WHO Global Polio Eradication InitiativeAt the time, polio was endemic in 125 countries. The initiative called for the eradication of the disease by the year 2000.
1988 1994
Polio Declared Eliminated from the Americas
1968
OPV : standard part of the immunization schedule in U.S.
2002
Polio Declared Eliminated in Europe
1960
Sabin's Polio Vaccine Licensed (OPV)

Polio eradication
35
▪ No long term carrier state for poliovirus in immunocompetentindividuals
▪ Polioviruses have no non-primate reservoir in nature, and survival of the virus in the environment for an extended period of time appears to be remote
▪ Interruption of person to person transmission of the virus by vaccination is the critical step in global polio eradication
▪ Eradication of wild type polio will be followed by minimizing the emergence of circulating vaccine-derived poliovirus (cVDPV), by stopping routine use of oral polio vaccine (OPV) and developing
affordable options for inactivated polio vaccine (IPV) use.

Polio eradication
36
▪ From vaccine discovery to 99% reduction in polio cases worldwide: 50 years
▪ From vaccine discovery to eradication of polio in the Americas: 44 years

Hepatitis B virus (HBV)
▪ DNA virus discovered in 1965 (by Dr. Blumberg)
▪ Non-cytopatic, hepatotropic virus
▪ Spread by contact with infected blood and body fluids
▪ Mode of transmission: Parenteral (blood to blood)-I.V. drug users, health workers are at
increased risk
By contact with an infected person (horizontal)
By sexual contact - sex workers and homosexuals are particular at risk
Perinatal (Vertical) - mother to child at birth37
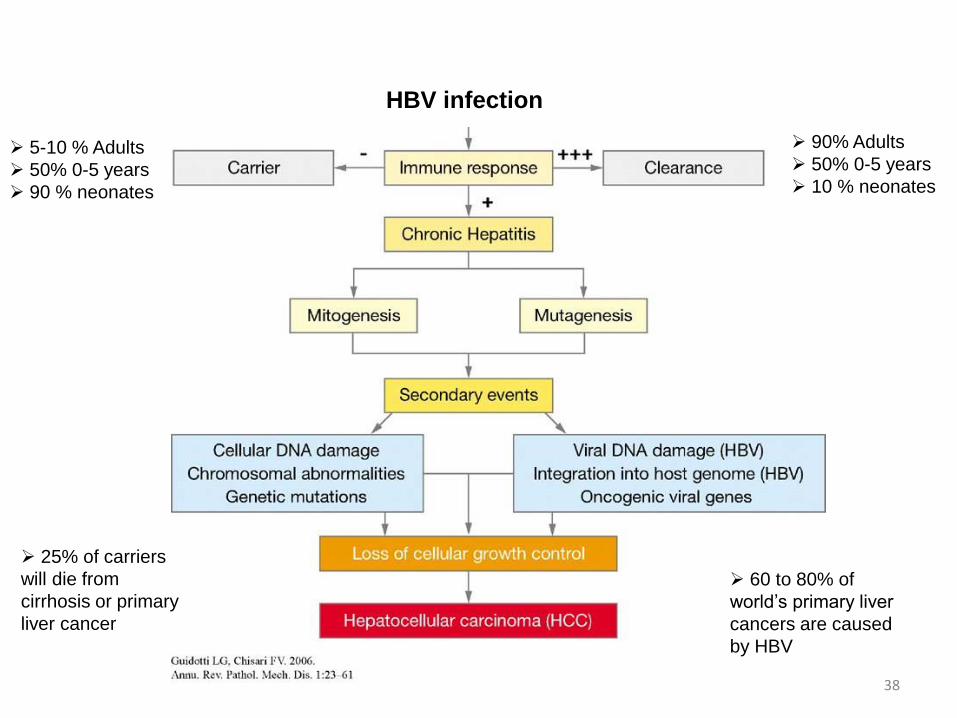
HBV infection
➢ 90% Adults
➢ 50% 0-5 years
➢ 10 % neonates
➢ 5-10 % Adults
➢ 50% 0-5 years
➢ 90 % neonates
➢ 25% of carriers
will die from
cirrhosis or primary
liver cancer
38
➢ 60 to 80% of
world’s primary liver
cancers are caused
by HBV

Hepatitis B virus (HBV)
▪ Often asymptomatic infection
▪100 times more infectious than HIV
▪ Outcome of infection
Adult: in 10 % of cases: chronic hepatitis which can lead to liver cancer (25 % of chronically HBV infected patients develop hepatocellular carcinoma (HCC). HBV causes 80% liver cancers, 9th
leading cause of death)
After birth up to 5 years old: 30 to 50 % cases: chronic hepatitis
At birth: 90% of cases: chronic hepatitis 39

HBV Distribution
Geographic distribution of chronic hepatitis B virus (HBV) infection — worldwide 2008
In 2010, 1/3 of the 6 billion people have been infected at one point in their life with HBV and over 350 million are chronically infected
worldwide: 1 million death from late chronic HBV complication every year. Half of these are due to liver cancers.
Primary liver cancer is the 8th most common cancer in the world
40

HBV: immune correlates of protection
▪ Passive immunization with Hepatitis B immunoglobulin (HBIG) prepared from plasma containing high titers of HBsAg, prevents infection and disease before and after exposure to HBV
41

Efficacy Clinical trials in high risk populations US (1978-1980)Szmuness et al (1980), Francis DP et al (1982)Highly purified Hepatitis B surface antigen (HBsAg) vaccine from human plasma
Efficacy Clinical trials newborns Tawain (1980-1982)Beasley el al (1983)(HBsAg) vaccine from human plasma
1981
“Heptavax”Approved by FDA, produced by Merck (discontinued in 1990)Plasma-derived HBV vaccine, (100$ a dose)World first cancer vaccine
1965
HBV virus discovery by Dr Blumberg
1969
First experimental HBV VaccineDr Blumberg and MillmanHeat-treated form of HBV
1986
“RECOMBIVAX HB® First recombinant subunit vaccine”Approved by FDA, produced by Chiron Corporation and MerKRecombinant HBsAg + alum (10 $ a dose)
WHO called for all children to receive the HBV vaccine116 countries added the vaccine to their immunization program
1991-19921976
First experimental HBV Vaccine tested in ChimpanzeesBuynak, HillemanHighly purified Hepatitis B surface antigen (HBsAg) vaccine from human plasma
Preclinical development of therapeutic vaccine for chronic HBV
HBV routinely used for children in 171 out of 193 WHO member states
2012
Evaluation of Vaccine efficacyin countries that added the vaccine to their immunization program
42

Immunological correlates of protection in HBV vaccination
▪ Efficacy of vaccine: induction of specific antibodies tohepatitis surface antigen (anti-HBs) antibodies andInduction of T cell memory
▪ Vaccine is administered intramuscular injection, ofprimary 3 doses of vaccines induces protective Ab in 95%of the vaccinees. Protection is achieved when HBsAGantibodies titers are above 10 mlU/ml. Long termprotection (>22 years) with no requirement of boosting
▪ Vaccine greatly reduces mother to child transmission aswell as the incidence of HCC and mortality from HCC
43

First Anti-Cancer Vaccine
Incidence of symptomatic hepatitis B in AN children, 1981-2010.
Prevalence of HBsAg in children <20 years of age: 1988
to 2008 Annual incidence of HCC in AN children <20 years of age.
Elimination of hepatocellular carcinoma
and acute hepatitis B in children 25 years
after a hepatitis B newborn and catch-up
immunization program.
McMahon BJ, Bulkow LR, Singleton RJ, Williams J, Snowball M, Homan C,
Parkinson AJ.
Hepatology. 2011 Sep 2;54(3):801-7.
44









![2019 ANNUAL REPORTSculpture of Father Mario Pantaleo – “Patio de la Solidaridad” [Patio of Solidarity] LIFE AND WORK OF FATHER MARIO 05 Giuseppe Mario Pantaleo was born in Pistoia,](https://static.fdocuments.us/doc/165x107/60e61d3dbe59bd291c4af00a/2019-annual-report-sculpture-of-father-mario-pantaleo-a-aoepatio-de-la-solidaridada.jpg)






