Substance Use Disorders and Cluster B Personality Disorders: Physiological, Cognitive, and...
21
Substance Use Disorders and Cluster B Personality Disorders: Physiological, Cognitive, and Environmental Correlates in a College Sample Jeanette Taylor, Ph.D. Department of Psychology, Florida State University, Tallahassee, Florida, USA Abstract: Substance use disorders (SUDs) and Cluster B personality disorders (PDs) are both marked by impulsivity and poor behavioral control and may result in part from shared neurobiological or executive cognitive functioning deficits. To examine the potential utility of such models in explaining variance in SUDs and PDs at the lower end of symptom expression and impairment, 123 (73 female) volunteer college students were administered 2 measures of executive cognitive functioning; a task assessing autonomic reactivity to aversive noise blasts; a life events and a peer substance use measure; and structured clinical interviews to assess symptoms of substance abuse/dependence and antisocial, borderline, histrionic, and narcissistic PDs. As expected, symptoms of SUDs and PDs were significantly positively correlated. Antisocial PD, alcohol and cannabis use disorder symptoms were significantly positively related to proportion of friends who use alcohol and drugs regularly and drug use among romantic partners. Number of negative life events was positively related to PD symptoms and to alcohol use disorder symptoms. Executive cognitive functioning was not related to SUD and PD symptoms in the expected direction. Findings suggest that, among higher functioning young adults, environ- mental factors may be particularly relevant to our understanding of SUDs and cer- tain PDs. Keywords: Substance use disorder, personality disorder, skin conductance, life events The author thanks Leonardo Bobadilla and Mark Reeves for their help with data collection. Address correspondence to Jeanette Taylor, Ph.D., Department of Psychology, Florida State University, Tallahassee, FL 32306-1270, USA; E-mail: taylor@psy. fsu.edu The American Journal of Drug and Alcohol Abuse, 31:515–535, 2005 Copyright D Taylor & Francis Inc. ISSN: 0095-2990 print / 1097-9891 online DOI: 10.1081/ADA-200068107 Order reprints of this article at www.copyright.rightslink.com Am J Drug Alcohol Abuse Downloaded from informahealthcare.com by Fordham University on 03/10/13 For personal use only.
Transcript of Substance Use Disorders and Cluster B Personality Disorders: Physiological, Cognitive, and...

Substance Use Disorders and Cluster BPersonality Disorders: Physiological, Cognitive,
and Environmental Correlates in aCollege Sample
Jeanette Taylor, Ph.D.
Department of Psychology, Florida State University, Tallahassee, Florida, USA
Abstract: Substance use disorders (SUDs) and Cluster B personality disorders (PDs)
are both marked by impulsivity and poor behavioral control and may result in part
from shared neurobiological or executive cognitive functioning deficits. To examine
the potential utility of such models in explaining variance in SUDs and PDs at the
lower end of symptom expression and impairment, 123 (73 female) volunteer college
students were administered 2 measures of executive cognitive functioning; a task
assessing autonomic reactivity to aversive noise blasts; a life events and a peer
substance use measure; and structured clinical interviews to assess symptoms of
substance abuse/dependence and antisocial, borderline, histrionic, and narcissistic
PDs. As expected, symptoms of SUDs and PDs were significantly positively
correlated. Antisocial PD, alcohol and cannabis use disorder symptoms were
significantly positively related to proportion of friends who use alcohol and drugs
regularly and drug use among romantic partners. Number of negative life events was
positively related to PD symptoms and to alcohol use disorder symptoms. Executive
cognitive functioning was not related to SUD and PD symptoms in the expected
direction. Findings suggest that, among higher functioning young adults, environ-
mental factors may be particularly relevant to our understanding of SUDs and cer-
tain PDs.
Keywords: Substance use disorder, personality disorder, skin conductance, life events
The author thanks Leonardo Bobadilla and Mark Reeves for their help with data
collection.
Address correspondence to Jeanette Taylor, Ph.D., Department of Psychology,
Florida State University, Tallahassee, FL 32306-1270, USA; E-mail: taylor@psy.
fsu.edu
The American Journal of Drug and Alcohol Abuse, 31:515–535, 2005
Copyright D Taylor & Francis Inc.
ISSN: 0095-2990 print / 1097-9891 online
DOI: 10.1081/ADA-200068107
Order reprints of this article at www.copyright.rightslink.com
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

INTRODUCTION
Substance abuse and dependence are common mental health disorders that
typically onset in young adulthood (1). Alcohol use problems are found in
10–25% of young adults (2, 3), and risk for heavy drinking and drug use that
may lead to substance use disorders (SUDs) is particularly high among young
adults (4). Costs associated with alcohol and drug abuse in the United States
(lost earnings, medical consequences, special services, accidents, etc.) are
estimated at $110–170 million annually (5), which underlines the importance
of SUDs as a mental health issue and as a focus of research.
SUDs are often comorbid with each other and with other mental
disorders, including personality disorders (PDs) (6), which are defined by
patterns of maladaptive responses related to one’s perceptions, cognitions,
emotional range/reactivity, or impulse control. Like SUDs, PDs are relatively
common and are found at high rates among young adults (7), In clinical
populations, comorbidity is especially high between SUDs and Cluster B
PDs, which are marked by erratic, dramatic behavior and includes antisocial
(ASPD), borderline (BPD), histrionic (HPD), and narcissistic (NPD). Cluster
B PDs are found at a high rate (>50%) among patients with various SUDs
(8, 9), and the association is strongest for ASPD and BPD. Around 30–50%
of patients with BPD have a SUD (10), and the link between ASPD and SUDs
is well documented with a widely used typology of alcoholism using ASPD
as a defining feature (11, 12). Onset of ASPD typically precedes onset of drug
dependence (13), indicating that ASPD may pose a risk for development of a
SUD. The association of SUDs to ASPD extends beyond clinical populations
to both college (14) and epidemiological ones (15).
Numerous explanatory models for SUDs and various Cluster B PDs have
been put forth, but few have focused on comorbidity. One model for the
comorbidity posits that high levels of the temperament factor novelty seeking
increases the likelihood of expressing features of both SUDs and Cluster B
PDs (16). Similar to this idea is that a common externalizing factor mediated
by genes contributes to the joint expression of SUDs and certain Cluster B
PDs (e.g., antisocial) (17). Gray’s (18) appetitive/aversive motivational
system has been offered as a factor in the expression of impulsivity and
behavioral inhibition, areas of dysfunction associated with SUDs and Cluster
B PDs. According to Fowles (19, 20), variation in the strength of Gray’s
(18, 21) behavioral inhibition system (BIS) and behavioral activation system
(BAS) may be reflected in physiological reactivity and in expressed
psychopathology. Gray (21) suggested that the neural structure of the BIS
includes inputs to the prefrontal cortex, the area of the brain associated
with executive cognitive functioning; the neural structure of the BAS is
thought to relate to the dopaminergic ‘‘reward circuit’’ (the circuit associated
with SUDs).
Skin conductance reactivity reflects autonomic nervous system arousal
that (like executive cognitive functioning) appears to be regulated by the
J. Taylor516
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

frontal cortex (22, 23), the area associated with the BIS (18). According to
Fowles (20), a weak BIS and a strong BAS contribute to the expression of
SUDs and ASPD and this idea has been supported through findings of
autonomic hypo-reactivity among men at risk for alcoholism (24), adolescent
boys with SUDs (25, 26), young adult men and women with SUDs (27), and
people with psychopathy (28)—a construct related to ASPD. This model
could be extended to other Cluster B PDs to help explain their high
comorbidity with SUDs. For example, impulsivity and poor behavioral
control are prominent features of BPD and thus, the highly reactive BAS and
underactive BIS that lead to excessive substance use also may lead to
behaviors that characterize people with BPD. Consistent with this idea,
autonomic hyporeactivity has been observed in women with BPD (29).
Deficits in executive cognitive functioning can manifest as impaired
judgment, poor planning, and impulsivity: problems associated with SUDs
and Cluster B PDs. Executive cognitive functions are controlled by the frontal
cortex, which shows marked development in adolescence and early adulthood
(30)—the period in which SUDs and PDs typically onset—and are related to
motivation and learning (31)—domains associated with BIS/BAS functioning.
Given the idea that BIS/BAS strength could provide a liability toward SUDs
and Cluster B PDs, poorer executive functioning would likely enhance that
liability and perhaps contribute to other aspects of the disorder (e.g.,
impairment). Deficits in executive cognitive functioning have been linked to
SUDs (32–35) BPD (36–38), and ASPD (39); also see Ref. (40). However,
negative findings also exist for SUDs (41), BPD (42), and ASPD (34, 43).
Behavior stemming from motivation and learning (related to BIS/BAS
functioning) and from executive cognitive processes occur within the context
of the environment, which may further enhance the risk for SUDs and Cluster
B PDs, both individually and jointly. For example, poor judgment resulting
from executive cognitive functioning deficits may lead to excessive
substance use despite negative consequences and also to affiliation with a
deviant social group that enhances and reinforces the substance use problem
(or perhaps even introduces the person to substance use). Consistent with this
idea, peer deviance (drug use and/or antisocial behavior) has been robustly
associated with both substance use (44–49) and substance abuse (50–52) at
least among adolescents. Further, relationship between peer attributes and
substance abuse may be mediated by behavioral control (51).
Peer alcohol use continues to be a salient correlate of alcohol use into
early adulthood (53, 54). However, peer substance use has not been ade-
quately examined in relation to SUDs beyond adolescence or to Cluster B
PDs at any age and, therefore, it is not clear whether substance using peers
are an important contributor to SUDs in young adulthood or even a
significant correlate of associated disorders such as Cluster B PDs. The latter
may be an important link in that certain PDs (e.g., antisocial) may increase
the likelihood of an association with substance using peers that in turn
increases the risk for SUDs.
517Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

Stressful life events are another salient environmental factor that has
been linked to SUDs (55). Kendler (56) proposed a gene-environment
correlation such that genetic factors associated with the liability toward SUDs
also contribute to behaviors that make certain negative life events more
likely. Cluster B PDs are also associated with higher rates of negative life
events (57), but it is not clear if this relationship is independent of the one
between life events and SUDs. It is conceivable that people with Cluster B
PDs have chaotic lives as a result of their personality which in turn leads to
negative life events and an increased use of alcohol and drugs (perhaps as a
coping behavior).
The BIS/BAS model provides a neurobiological/motivational framework
for SUDs, ASPD, and BPD, and perhaps their comorbidity. The literature
suggests that an executive functioning deficit may be part of the cognitive
framework for these same disorders. Finally, the literature suggests at least 2
important environmental factors—negative life events and deviant peers—in the
environmental framework for SUDs and perhaps also Cluster B PDs. Both ASPD
and BPD have received vastly greater research attention than NPD and HPD
leaving their comorbidity to SUDs more of a mystery. Moreover, previous
research has not adequately examined nonclinical samples. Such investigations
are needed to test the appropriateness of etiological models in explaining
variance in SUDs and Cluster B PDs across the presentation spectrum.
The present study examined individual differences in symptoms of SUDs
and all 4 Cluster B PDs as they relate to individual differences in executive
cognitive functioning, autonomic reactivity, peer substance use, and negative
life events in early adulthood. Data were collected from a volunteer sample of
college students who, as a demographic group, are at risk for heavy substance
use and SUDs (3, 4) as well as PDs (1, 7). Importantly, college students who
are heavy substance users are unlikely to seek treatment even when their
substance use leads to problems (4). Thus, the present study examined
correlates of SUDs and Cluster B PDs in people who may not be seeking
treatment for these problems but who are at risk to experience them.
Given the documented comorbidity among SUDs and Cluster B PDs,
symptoms of those disorders were expected to correlate positively. Electro-
dermal response modulation was expected to correlate negatively with SUD
symptoms [based on findings from Taylor (27) and Taylor et al. (26)]. As per
the reviewed literature, both SUD and Cluster B PD symptoms were expected
to correlate negatively with indices of executive cognitive functioning and
positively with number of negative life events. Previous findings from ado-
lescent samples led to the expectation that SUD symptoms would correlate
positively with substance use among friends and romantic partners. Symp-
toms of Cluster B PDs were also expected to correlate positively with
substance use among peers based on the idea that people with Cluster B PDs
may select friends with similar levels of behavioral undercontrol (manifested
as substance use). Finally, it was assumed that behavioral undercontrol and
impulsivity would be most pronounced in people comorbid for SUDs and
J. Taylor518
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

PDs and result in more severe problems (e.g., more negative life events).
Consistent with this idea, people with comorbid SUD and Cluster B PD
diagnoses were expected to show poorer electrodermal response modulation,
poorer executive cognitive functioning, more negative life events, and more
friends and partners using alcohol and drugs than those with only a SUD and
controls (who were expected to differ from those with only a SUD).
METHOD
Participants
Participants were 123 (73 female) students attending a large southeastern
U.S. university. Persons aged 18 or older without a self-reported history of
head injury, neurological disorder, or hearing problems were recruited
through advertisement fliers for a paid ($25) study of psychological and
physiological functioning. The sample was primarily White (59.3%), African
American (16.3%), and Hispanic/Latino (13.8%) with a mean age of 20.8
(SD=4.15). Informed written consent was obtained from each participant and
the study was approved by the IRB.
Procedures and Measures
Data were collected from individuals during a 2.5-hour laboratory session;
measures are described below in the order in which they were administered.
Psychophysiological Measurement
Participants washed their hands with Ivory soap and rubbing alcohol was
swabbed on the medial phalanx of the middle and ring finger of each hand prior
to placement of silver-silver chloride (Ag-AgCl) electrodes that were filled
with commercially available SC electrode cream and attached using electrode
collars (8 mm diameter opening). The SC from the right and left hands were
recorded through two DC amps connected to separate 24-bit digitizing SC
couplers from Contact Precision Instruments (Cambridge, MA). The system
used constant 0.5-V electrode excitation as specified by Lykken and Venables
(58). Data were digitized online at 128 Hz. All physiological data were
acquired and scored with the PSYLAB 7 software program from Con-
tact Precision Instruments running on two interfaced IBM-compatible PCs.
Participants were seated alone in a darkened room equipped with a
microphone, a video camera for monitoring participation, and a computer
monitor for visual stimulus presentation.
Participants received experimenter communications and auditory stimuli
through stereo headphones. Participants were asked about irregularities in
519Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

food, drug, nicotine, and caffeine intake prior to the study session.
Psychophysiological recording began with a 2-minute relaxation period
followed by a 90-second task in which participants received a single 2-second
unpredictable blast of 92 or 1101 dB white noise that served to orient them to
the aversive sound used in the Cooltest.
In the Cooltest, participants were given 6 presentations of a video clip of
a numberless, unmarked clock with a sweep second hand and a 2-second blast
of white noise. Participants were told that the noise would be unpredictable
on some trials and that on other trials there would be a red hash mark on the
clock face to make the noise predictable (during the instructions, participants
were shown a still image of the predictable clock with a red hash mark in a
position not used in the actual test). Participants were told that the type of
trial coming next would be indicated on the computer screen just before each
trial began and their task was to ‘‘stay cool’’ and not react to any of the
noises. Consistent with an earlier Cooltest study (26), trials 1, 4, and 6 were
predictable; trials 2, 3, and 5 were unpredictable and blast times were
invariant across subjects and occurred between the 18th and 50th s of each 1-
minute trial (each trial was associated with a particular, unrepeated blast
time). No stimuli were presented in the 5 seconds between trials.
The SCR amplitude for each of the Cooltest trials, defined as the
difference (in msiemens) between the SCL preceding the response and the
SCL at the peak of the response, was scored from each hand via automated
procedures or by people blind to the participant’s other data. Electrodermal
response modulation, reflecting the percent change in SCR when the blast is
predictable, was quantified as follows (using raw SCR data given the built-in
range correction):
100 � ðMean SCRUnpredictable � Mean SCRPredictableÞ=Mean SCRUnpredictable
A t-test showed no significant difference between scores across hands and,
therefore, the scores were averaged for a mean electrodermal response
modulation score that was used in analyses.
Executive Cognitive Functioning Measures
The 64-card computerized research version of the Wisconsin Card Sorting
Test (WCST) (59, 60) and the Stroop test (61) were administered next. The
1A problem with the calibration of the white noise generator’s output inadvertently
caused a reduced noise of 92 dB to be delivered for all stimuli to the first 42
participants through the study. A t-test comparing the electrodermal response
modulation score of those who received all stimuli at 92 (n=36) versus 110 dB
(n=77) showed no significant difference, t (110)=�0.73, p=.47. Thus, data were not
excluded on participants who received the 92 dB noises.
J. Taylor520
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

Stroop test yields an interference score reflecting the extent to which a
previously learned response (reading color names) interfered with ability to
inhibit the learned response (naming an ink color that is mismatched to the
target color word, e.g., ‘‘red’’ is printed in blue ink). The WCST requires the
sorting of cards by an unidentified preset criterion using trial and error with
only minimal feedback (i.e., ‘‘correct’’ or ‘‘incorrect’’ after each card is
sorted). The criterion changes after a preset number of successful responses.
The WCST produces t-scores for perseverative responses and errors (which
reflect the extent to which the examinee continued using a previously
successful strategy after the criterion changed), nonperseverative errors, and
total errors. Indices of executive cognitive functioning included these t-scores
from the WCST and interference score from the Stroop test.
Symptoms of Substance Use Disorders and Cluster B
Personality Disorders
Lifetime occurrence of symptoms of SUDs (alcohol, cannabis, sedatives,
stimulants, cocaine, opioids, hallucinogens, PCP, and ‘‘other’’ [inhalants,
steroids, non-prescription sleep or diet pills]) and other Axis I disorders was
assessed using the Structured Clinical Interview for DSM-IV, Non-patient
Edition [SCID-I/NP; Ref. (62)]. Symptoms of HPD, NPD, BPD, and ASPD
were assessed with the Structured Interview for DSM-IV Personality
Disorders (SIDP-IV) (63). Trained graduate students (who were blind to
the participant’s other study data) administered the interviews.
Symptoms of each disorder were assigned via consensus of at least 2
clinical graduate student interviewers examining all available clinical
information (including audio tapes of the interviews). Symptom data were
entered into a computer and a count of the symptoms met at threshold level
was generated for each diagnosis using a computer algorithm. This symptom
count was combined with the requisite other clinical criteria (e.g., duration)
to produce diagnoses via a computer algorithm. Diagnoses were generated at
the definite (all criteria met) and probable (all but one criteria met) certainty
levels to identify subthreshold diagnostic cases and avoid classifying them as
diagnostically clean. Symptom counts further captured the presence of
clinically significant problems at even subthreshold levels of diagnosis.
Reliability of diagnoses (probable or definite) using the consensus procedure
was good (kappas ranged from .61 to 1.0 for both the Cluster B PDs and the
SUDs). Similarly, reliability correlations for symptom counts were high
ranging from .84 to .96 for Cluster B PDs and .69 to 1.0 for SUDs.
An examination of the data indicated that alcohol and cannabis abuse and
dependence were the most common SUDs. As such, they were examined
separately from the remainder of the illicit drugs. Symptoms of abuse and
dependence were combined yielding counts of abuse/dependence symptoms
of alcohol, cannabis, and other (non-cannabis) illicit drugs.
521Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

Life Events and Substance Use Among Friends and Partners
Self-reports to assess life events and substance use among peers were
created for this study. The life events measure included 20 events that were
rated on frequency of occurrence within the past 12 months (0, 1, 2, or 3
times or more coded 0 to 3, respectively) and how stressful the event was
on a scale from 0 (not at all) to 3 (very stressful) (for events occurring more
than once, the most stressful occurrence was rated). Twelve events were
rationally selected as negative (e.g., ‘‘Experienced a break-up in a sig-
nificant romantic relationship’’) and responses were summed within that
category. Internal consistency reliability was acceptable for number of
negative life events (alpha=.67). The stress ratings of the 12 negative life
events were averaged to produce an average level of stress associated with
negative life events.
An 8-item self-report was created to assess substance use among peers.
Participants indicated the number of friends they had (defined as people they
‘‘talk to or see regularly’’) on a scale from 0 (coded 0) to 10 or more (coded
5) within the past 12 months and the proportion of their friends (from 0=none
to 4=almost all) that drank alcohol, drank alcohol once a week or more, used
an illicit drug, and used an illicit drug once a week or more. Using those same
metrics, participants indicated the number of romantic partners they had
(defined as people they ‘‘had dated’’) within the past 12 months and the
proportion of partners who drank alcohol and used an illicit drug. Given that
the definition of romantic partner could easily include people the participant
did not know very long or very well, the validity of responses regarding
regular use of alcohol and drugs by partners was potentially low and was
therefore not assessed.
Diagnostic Groups Used to Examine Comorbidity
Participants were placed into groups based on the presence of any SUD
diagnosis (abuse at the definite level or dependence at the probable or definite
level) and any Cluster B PD diagnosis (at the probable or definite level).
Participants without an SUD or Cluster B PD diagnosis (and no anxiety
disorder or depression) formed the control group (n=27; 17 female); 10
participants (7 female) with at least one SUD diagnosis (and no other
diagnosis) formed the SUD only group; and 18 participants (7 female) with at
least one SUD and at least one Cluster B PD diagnosis formed the comorbid
group. Diagnoses related to alcohol and cannabis made up the vast majority
of SUD diagnoses for the SUD only and comorbid groups and ASPD and
BPD made up the majority of PD diagnoses in the comorbid group.
Furthermore, adult antisocial behavior (ASPD without conduct disorder) was
included as a PD diagnosis based on research showing that people with ASPD
are similar to those with adult antisocial behavior on various correlates
(64, 65). Finally, there were not a sufficient number of cases to form a Cluster
J. Taylor522
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

B PD only group, which precluded a test of the unique association of Cluster
B PDs with the various dependent variables.
Analyses
First, descriptive data on symptom counts and rates of diagnoses were
calculated for each disorder. Next, Pearson interclass correlations were
calculated between the symptom counts for SUDs and Cluster B PDs, and
the psychophysiological, cognitive, and environmental variables to index the
strength of the associations. Partial correlations were used to investigate the
impact of these variables on the association between symptoms of PDs and
SUDs. A Bonferroni correction for the total number of correlations to be
calculated would have been prohibitively conservative; therefore, a
Bonferroni correction was made for each disorder category. Alpha for the
4 Cluster B PDs was corrected (.05/4) yielding an alpha of .013 for
correlations with those disorders. Similarly, the alpha for correlations with
the three SUDs was set to .017. The maximum sample size for the
correlational analyses for PDs was 123, which yielded adequate power
(83%) to detect medium effects [d� .3 using conventions put forth by
Cohen (66)] at the corrected alpha of .013. Data were missing on some
measures (e.g., on electrodermal modulation score due to recording failures)
leaving a minimum of 107 cases for some of the correlations with PD
symptoms, which still left adequate power (76%) to detect medium-sized
correlations at the corrected alpha. The maximum sample size for the SUD
correlational analyses was 120 due to some missing interview information,
which yielded adequate power (85%) to detect medium effects (d� .3) at
the corrected alpha of .017. Missing data on the correlates led to a minimum
of 97 cases for some of the correlations with SUD symptoms, which still
left adequate power (75%) to detect medium-sized correlations at the cor-
rected alpha.
Finally, comorbidity between SUDs and Cluster B PDs was examined in
relation to executive cognitive functioning, physiological reactivity, life
events, and substance use among friends and romantic partners by comparing
scores on those variables among 3 diagnostic groups (control, SUD only, and
comorbid SUD-Cluster B PD). Groups were compared using one-way
ANOVA with post hoc Least Significant Difference follow-up tests. (The
sample was underpowered for tests of gender effects and thus no factorial
ANOVA models were tested.) A total of 55 participants were classified into
the 3 groups, which allowed detection of large effects [d� .45 using
conventions put forth by Cohen (66)] with adequate power (84%) at alpha set
to .05. Missing data for some dependent variables led to a minimum sample
of 48 for the group analysis, which still provided adequate power (77%) to
detect large effects. Power analyses were conducted using the G*Power
program (67).
523Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

RESULTS
Table 1 presents the mean and standard deviation for raw symptom counts of
each disorder. As is often the case in nonclinical samples, the symptom count
distribution for each disorder was positively skewed and the data were
submitted to a log-transformation (log10 [x=1]) prior to analyses. Table 1
also presents rates of SUDs and Cluster B PDs, which were largely consistent
with general prevalence rates for those disorders (1–3). The rate of ASPD
was high and was not attributable to low diagnostic reliability. Instead, the
inclusion of probable cases of adult antisocial behavior (i.e., people meet-
ing just 2 ASPD criteria) may have contributed to the higher rate for
that disorder.
Table 2 presents interclass correlations among log-transformed symptom
counts of PDs and SUDs and psychophysiological and environmental
variables. As expected, correlations among the Cluster B PDs and among
SUDs were significant with the exception of HPD and NPD symptoms, which
did not correlate with SUD symptoms. As expected, electrodermal response
modulation showed a significant inverse relationship to drug use disorder
symptoms. Consistent with the report by Taylor (27) using this same sample,
symptoms of Cluster B PDs were not significantly associated with
electordermal response modulation. As expected, SUD, ASPD, and NPD
symptoms were significantly positively associated with peer substance use.
Partial correlations were used to investigate the influence of peer
substance use on the association between ASPD and SUD symptoms. The
correlation between ASPD and alcohol use disorder symptoms remained
significant and ranged in magnitude from .24 (when controlling for drug use
Table 1. Symptom count means (and standard deviations) and prevalence rate for
each disorder
Disorder N Mean (SD) % with Diagnosisa
Narcissistic personality disorder 123 0.43 (0.98) 3.3
Histrionic personality disorder 123 0.41 (0.90) 2.4
Borderline personality disorder 122 0.78 (1.25) 4.1
Antisocial personality disorderb 121 0.64 (1.17) 18.2
Alcohol abuse/dependencec 116 1.81 (2.53) 37.9
Cannabis abuse/dependencec 120 1.04 (2.04) 29.2
Non-cannabis illicit drug
abuse/dependencec120 1.00 (3.16) 14.2
aIncludes cases diagnosed at a probable or definite certainty level.bIncludes adult antisocial behavior in the mean and in the rate of diagnosis.cMean includes symptoms of abuse and dependence; rate of diagnosis reflect the
percent of the sample that met criteria for abuse at a definite level or dependence at a
probable or definite level.
J. Taylor524
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

among friends) to .27 (when controlling for alcohol use among friends).
Similarly, the correlation between ASPD and cannabis use disorder
symptoms remained significant and ranged from .34 (when controlling for
drug use among friends) to .40 (when controlling for alcohol use among
friends). Finally, ASPD was significantly correlated with non-cannabis illicit
drug use disorder symptoms when controlling for drug use among friends
(r = .35). Narcissistic PD symptoms were significantly correlated with peer
drug use, which may have resulted from the association between NPD and
Table 2. Interclass correlations among symptom counts of personality disorders,
substance use disorders, substance use among friends and romantic partners, and
life events
NPD HPD BPD ASPD ALC CAN ILLIC
Histrionic personality
disorder (HPD)
.40
Borderline personality
disorder (BPD)
.42 .31
Antisocial personality
disorder (ASPD)
.25 .19 .38
Alcohol abuse/
dependence (ALC)
.18 � .01 .32 .35
Cannabis abuse/
dependence (CAN)
.15 .02 .33 .45 .46
Illicit drug abuse/
dependence (ILLIC)
.10 .07 .32 .43 .34 .35
Electrodermal response
modulation
.03 .21 .03 � .09 � .22 � .25 � .23
Number of friends .12 .05 � .06 .00 .26 .03 � .03
Friends drink alcohol .20 .11 .10 .25 .48 .35 .17
Friends drink 1� /week
or more
.17 .05 .10 .24 .58 .38 .19
Friends use drugs .30 .11 .19 .38 .40 .45 .34
Friends use drugs
1� /week or more
.28 .06 .15 .31 .45 .45 .20
Number of romantic
partners
.33 .21 .17 .12 .23 .11 � .03
Partners drink alcohol .10 � .07 .00 .15 .39 .15 .06
Partners use drugs .26 .06 .13 .34 .36 .44 .22
Number of negative
life events
.21 .24 .26 .30 .24 .19 � .01
Average stress for
negative events
� .02 .11 .23 � .12 � .05 � .04 .07
Note: ILLIC=non-cannabis illicit drug abuse/dependence. Drinking and drug use
variables for friends and partners refers to proportion of friends and partners who use
substances. Significant correlations ( p<.013 for personality disorders; p<.017 for
substance use disorders) are in bold type.
525Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

ASPD (the latter of which was significantly correlated with peer drug use).
To test this, symptoms of NPD were correlated with the peer drug use
variables while controlling for ASPD symptoms and the correlations
remained significant at p < .05, indicating that people with NPD features
have higher proportions of friends and romantic partners who use drugs and
the association is not accounted for by antisocial or SUD symptomatology.
Finally, the correlations in Table 2 revealed that negative life events
were related as expected to most PDs and to alcohol use disorder symptoms.
When controlling for number of negative life events, the correlations between
alcohol use disorder symptoms and symptoms of BPD (r = .27) and ASPD
(r = .30) remained significant (p < .005).
Correlations between PD and SUD symptoms and executive cognitive
functioning variables were largely nonsignificant (most were <.10 in
magnitude) and, therefore, were not presented in detail. Total errors on the
WCST correlated significantly with symptoms of BPD (r = .23) and alcohol
use disorders (r = .24), which were also significantly associated with
nonperseverative errors (r = .27). These correlations were not in the expected
direction such that symptoms were associated with higher T-scores (i.e.,
better performance or fewer errors).
The results of the ANOVA analyses were consistent with the results of
the correlational analyses. As expected, diagnostic groups differed signifi-
cantly (p < .001) on number of negative life events, F (2, 53) = 7.52. Also
consistent with expectations, post hoc follow-up tests showed that the
comorbid group had significantly (p < .004) more negative life events than
both the controls and the SUD only group. On average, the comorbid group
reported nearly 7 negative life events within the past 12 months compared to
an average of about 2.7 for the SUD only and control groups. Groups did not
differ significantly on any of the executive cognitive functioning indices or
electrodermal modulation score.
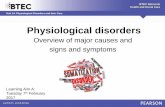
Figure 1 presents the mean proportion of friends and romantic partners
within the past 12 months who used alcohol and drugs. A significant group
effect was found for regular (once a week or more) use of alcohol, F (2,
52) = 3.48, p = .04, and illicit drugs, F (2, 50) = 5.35, p = .008, among friends.
A significant (p = .001) group effect was also found for drug use among
friends, F (2, 512) = 7.86, and romantic partners, F (2, 48) = 8.77. Differences
between groups were only partly consistent with expectations. As illustrated
in Figure 1, post hoc follow-up tests revealed that, as expected, the comorbid
group had significantly (p<.05) more friends and partners using substances
than controls. The SUD only group also differed significantly from controls
in the proportion of friends who regularly use alcohol (p <.03) and romantic
partners who use illicit drugs (p<.02). The difference between the SUD only
group and controls on the proportion of friends who use drugs and those who
use drugs regularly showed a trend toward significance (p<.08). However,
contrary to expectations, the comorbid group did not differ significantly from
the SUD only group in any of the post hoc tests. There was not a significant
J. Taylor526
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

effect for group on number of friends or proportion of friends who drink
alcohol. A group effect was found for number of romantic partners, F (2,
54)= 4.59, p = .02, with the SUD only and comorbid groups evidencing
significantly (p< .04) more romantic partners than the control group.
DISCUSSION
Substance use disorders and Cluster B PDs may share neurobiological,
cognitive, and environmental risk factors that contribute to their individual
and joint manifestations. However, few studies have examined variables
tapping each of these domains in relation to SUDs and Cluster B PDs within
the same sample. The present study examined multivariable data in a young
adult sample to provide insights into factors that relate to SUDs and Cluster B
PDs individually and jointly and to shed light on whether various risk factors
are significantly associated with SUDs and PDs at the lower end of the
spectrums of severity and impairment. Certain environmental factors may be
particularly relevant to understanding SUDs, Cluster B PDs, and their
comorbidity in nonclinical populations.
Figure 1. Mean proportion of friends and romantic partners within the past 12
months who used alcohol and illicit drugs. The vertical line with cross bars
represents±1 SE. SUD = substance use disorder; PD = Cluster B personality disorder.
Descriptors for the scale values are given on the y-axis. Ratings were made only if the
participants indicated any friends or romantic partners within the past 12 months.
Control group n = 24–27; SUD only group n = 9–10; Co-morbid SUD-PD group
n = 17–18.
527Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

The expected interrelations were found among symptoms of SUDs and
among symptoms of Cluster B PDs, indicating covariance of these problems
in nonclinical samples. These data from clinical interviews were consistent
with studies using self-reports that found significant comorbidity among
Cluster B PDs in nonclinical samples (68). Also as expected, symptoms of
Cluster B PDs and SUD were significantly related, but only with regard to
BPD and ASPD. Histrionic and NPD symptoms, while related to each other
and to the other PDs, were not related significantly to SUD symptoms in this
young adult college sample. Thus, consistent with research from clinical
samples, BPD and ASPD were the Cluster B disorders that were most
strongly related to SUDs. An important caveat to this conclusion is that BPD
and ASPD were more common in this sample and the restricted range of
symptoms of HPD and NPD may have attenuated their associations with the
other variables, including SUD symptoms.
The data were fairly consistent with previous work showing positive
associations between SUDs and number of negative life events experienced.
However, the association with negative life events was significant only for
alcohol use disorder symptoms in the present study. Also consistent with
previous work [e.g., Ekselius et al. (7)], symptoms of most Cluster B PDs
were significantly related to negative life events. Furthermore, the findings
from the group comparisons suggested that Cluster B PDs contributed
substantially to the likelihood of experiencing negative life events given that
the people with both an SUD and a comorbid Cluster B PD diagnosis reported
more than twice as many negative life events as those with only an SUD
diagnosis and those without a psychiatric diagnosis. Thus, the data suggest
that young adults with substance use problems and features of PDs marked by
impulsivity and erratic behavior are likely to experience higher numbers of
negative life events (e.g., having a serious fight with a close friend) than even
those with just substance use problems. The present data cannot address the
direction of causation and no single obvious causal pattern exists because
negative life events could conceivably be either a consequence of or a
contributor to a substance use problem or a maladaptive personality style.
The present data suggest that further study of life events as they relate to
SUDs and Cluster B PDs individually and jointly is warranted.
Consistent with research conducted largely in adolescent samples, the
present study found significant associations between symptoms of SUDs and
the substance use habits of friends and romantic partners in early adulthood
and extended earlier research findings to certain Cluster B PDs. Cannabis and
alcohol use disorder symptoms and ASPD symptoms were all significantly
associated with alcohol use among friends and drug use among friends and
romantic partners. Narcissistic PD symptoms also were significantly
associated with drug use among friends and romantic partners despite the
lack of association of narcissism with SUDs in this sample. Unlike with
negative life events, the comorbidity between SUDs and Cluster B PDs did
not relate to an increase in substance use among peers, suggesting that having
J. Taylor528
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

an SUD increases the likelihood of hanging around with friends and getting
involved with romantic partners who use alcohol and/or illicit drugs in young
adulthood regardless of co-morbid Cluster B PD pathology. Again, the
present data do not address the direction of causation and various scenarios
are plausible including the possibility that SUDs lead to seeking friends and
romantic partners with similar levels of substance use or, alternatively,
substance use among friends and romantic partners increases one’s own use
thereby increasing the chances of developing an SUD. The nature of the
relationship between peer substance use and SUDs is an important area
for future study because of it has potential implications for intervention
and prevention.
Consistent with the notion that a weak BIS contributes to the liability
toward SUDs, symptoms of illicit drug use disorders (including cannabis)
were inversely related to electrodermal response modulation. However,
similar support was not found for Cluster B PD symptoms. Not surprisingly,
the present data were consistent with another report from this same sample
showing poor electrodermal response modulation to be associated with SUDs
and not Cluster B PDs (27). Thus, these findings do not represent independent
evidence for a potentially specific link between SUDs and electrodermal
response modulation, but are nonetheless consistent with that idea. The group
analyses failed to show a significant association between electrodermal
response modulation and SUD, suggesting a possible inconsistency with
earlier reports (26, 27). An examination of effect sizes revealed a large
difference (d=.69) between controls and the comorbid group and only small
differences (d=.23) between controls and the SUD only group and between
the SUD only and comorbid groups. Therefore, although other research
suggests that SUDs may be particularly strongly related to poor electrodermal
response modulation, more work is needed before ruling out the possibility
that Cluster B PDs are also related to this biological factor.
Negative findings from this study on the association between executive
cognitive functioning and SUDs may provide insights into the mixed picture
presented by the extant literature. The present study failed to find worse
performance on 2 widely used measures of executive cognitive functioning
among people with symptoms of SUDs and/or Cluster B PDs. Even the group
analyses, where participants met criteria for SUD and/or PD diagnoses, failed
to show an effect. In fact, the only significant findings indicated that college
students with more alcohol use disorder and/or BPD symptoms had better
performance on the WCST in terms of total errors and non-perseverative
errors compared to students with fewer such symptoms. The obvious caveat
to these negative findings is that the present sample was arguably high
functioning as evidenced by their enrollment in college and perhaps not
particularly severe in the SUD and PD pathology as evidenced by some
meeting diagnostic criteria at a probable certainty level. Thus, although
executive cognitive functioning deficits may be related to risk for SUD and
Cluster B PD, they may not characterize people with less severe
529Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

presentations. The present study suggests the possibility that higher executive
cognitive functioning may help young adults who experience SUDs and BPD
features to avoid global impairment in occupational functioning (as
evidenced by their enrollment in college).
This study examined individual differences in SUD and Cluster B PDs as
they relate to empirically supported correlates that reflect neurobiological and
cognitive models for understanding these disorders and perhaps their
comorbidity. The findings suggested that young adults with SUD and ASPD
features are likely to experience more negative life events and to associate
with friends and romantic partners who drink and use illicit drugs, indicating
that environmental factors (not deficits in neurobiology and cognitive
functioning) may be particularly relevant to understanding SUDs and certain
PDs in higher functioning young adults. The findings from this study must be
taken within the context of several limitations. First, the sample did not
permit adequate test of gender effects, which may be particularly important in
understanding SUDs and Cluster B PDs (which differ in prevalence by
gender). Second, the present sample was clearly high functioning and there-
fore results cannot necessarily be generalized to other nonclinical popula-
tions. The use of a nonclinical sample also limited the range of psychiatric
symptoms and the number of people who fit into diagnostic groups but this
is a disadvantage of any nonclinical sample, not just those drawn from col-
lege populations.
The present study highlights the potential importance of environmental
variables in understanding phenomenology of SUDs and certain Cluster B
PDs, particularly at the less severe end of the spectrum of symptom ex-
pression and impairment. Although the etiology of SUDs and Cluster B PDs
may share a common underlying genetic liability (17), temperament (16), or
motivational structure (20), the environment may be crucial in determining
which disorder manifests. Future work is needed to understand what factors
pose risk for SUDs and Cluster B PDs individually and jointly to help answer
questions about their etiology and perhaps inform treatment.
REFERENCES
1. American Psychiatric Association. Diagnostic and Statistical Manual of
Mental Disorders. 4th ed. Washington, DC: American Psychiatric
Association, 1994.
2. Clements R. Prevalence of alcohol-use disorders and alcohol-related
problems in a college student sample. J Am Coll Health 1999; 48:111–
118.
3. Grant BF, Harford TC, Dawson DA, Chou P. Epidemiologic Bulletin
No. 35: prevalence of DSM-IV alcohol abuse and dependence, United
States 1992. Alcohol Health Res World 1994; 18:243–248.
4. Feigelman W, Gorman BS, Lee JA. Binge drinkers, illicit drug users,
J. Taylor530
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

and polydrug users: an epidemiological study of American collegians.
J Alcohol Drug Educ 1998; 44:47–69.
5. Harwood H, Fountain D, Livermore G. The Economic Costs of Alcohol
and Drug Abuse in the United States, 1992. Analysis by the Lewin
Group. NIH Publication No. 98-4327, Bethesda, Maryland: DHHS,
NIH, 1998.
6. Skodol AE, Oldham JM, Gallaher PE. Axis II comorbidity of substance
use disorders among patients referred for treatment of personality
disorders. Am J Psychiatry 1999; 156:733–738.
7. Ekselius L, Tillfors M, Furmark T, Fredrikson M. Personality disorders
in the general populations: DSM-IV and ICD-10 defined prevalence as
related to sociodemographic profile. Pers Individ Differ 2001; 30:311–
320.
8. Ross S, Dermatis H, Levounis P, Galanter M. A comparison between
dually diagnosed inpatients with and without Axis II comordidity and
the relationship to treatment outcome. Am J Drug Alcohol Abuse 2003;29:263–279.
9. Verheul R, Kranzler HR, Poling J, Tennen H, Ball S, Rounsaville BJ.
Axis and Axis II disorder in alcoholics and drug addicts: fact or artifact?
J Stud Alcohol 2000; 61:101–110.
10. Trull TJ, Sher KJ, Minks-Brown C, Durbin J, Burr R. Borderline
personality disorder and substance use disorders: a review and inte-
gration. Clin Psychol Rev 2000; 20:235–253.
11. Babor TF, Hofmann M, DelBoca FK, Hesselbrock V, Meyer RE,
Dolinsky ZS, Rounsaville B. Types of alcoholics, I. Evidence for an
empirically derived typology based on indicators of vulnerability and
severity. Arch Gen Psychiatry 1992; 49:599–608.
12. Cloninger CR, Bohman M, Sigvardsson S. Inheritance of alcohol abuse:
cross-fostering analysis of adopted men. Arch Gen Psychiatry 1981;38:861–868.
13. Compton WM, Cottler LB, Phelps DL, Abdallah AB, Spitznagel EL.
Psychiatric disorders among drug dependent subjects: are they primary
or secondary? Am J Addict 2000; 9:126–134.
14. Casillas A, Clark LA. Dependency, impulsivity, and self-harm: traits
hypothesized to underlie the association between cluster B personality
and substance use disorders. J Pers Disord 2002; 16:424–436.
15. Taylor J, Elkins IJ, Legrand L, Peuschold D, Iacono WG, McGue M.
Construct Validity of Adoloscent Antisocial Personality Disorder.Tallahassee, FL: Florida State University, 2003. Manuscript submitted
for publication.
16. Battaglia M, Przybeck TR, Bellodi L, Cloninger CR. Temperament
dimensions explain the comorbidity of psychiatric disorders. Compr
Psychiatry 1996; 37:292–298.
17. Kreuger RF, Hicks BM, Patrick CJ, Carlson SR, Iacono WG, McGue
M. Etiologic connections among substance dependence, antisocial
531Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

behavior, and personality: modeling the externalizing spectrum. J
Abnorm Psychology 2002; 111:411–424.
18. Gray JA. Perspectives on anxiety and impulsivity: a commentary. J Res
Pers 1987; 21:493–509.
19. Fowles DC. The three arousal model: implications of Gray’s two-factor
learning theory for heart rate, electrodermal activity, and psychopathy.
Psychophysiology 1980; 17:87–104.
20. Fowles DC. Pscyhophysiology and psychopathology: a motivational
approach. Psychophysiology 1988; 25:373–391.
21. Gray JA. Elements of a Two-Process Theory of Learning. New York:
Academic Press, 1975.
22. Bechara A, Damasio H, Tranel D, Damasio AR. Deciding advanta-
geously before knowing the advantageous strategy. Science 1997;275:1293–1295.
23. Raine A, Reynolds GP, Sheard C. Neuroanatomical correlates of skin
conductance orienting in normal humans: a magnetic resonance im-
aging study. Psychophysiology 1991; 28:548–558.
24. Finn PR, Kessler DN, Hussong AM. Risk for alcoholism and classical
conditioning to signals for punishment: evidence for a weak behavioral
inhibition system? J Abnorm Psychology 1994; 103:293–301.
25. Iacono WG, Carlson SR, Malone SM. Identifying a multivariate
endophenotype for substance use disorders using psychophysiological
measures. Int J Psychophysiol 2000; 38:81–96.
26. Taylor J, Carlson SR, Iacono WG, Lykken DT, McGue M. Individual
differences in electrodermal responsivity to predictable aversive
stimuli and substance dependence. Psychophysiology 1999; 36:193–
198.
27. Taylor J. Poor electrodermal reactivity and its association to substance
use disorders. Psychophysiology 2004; 41:982–989.
28. Fowles DC, Missel KA. Electrodermal hyporeactivity, motivation, and
psychopathy: theoretical issues. In: Fowles D, Sutker P, Goodman S,
eds. Progress in Experimental Personality and Psychopathology Re-
search 1994: Special Focus on Psychopathy and Antisocial Behavior: A
Developmental Perspective. New York: Springer Publishing, 1994:263–
283.
29. Herpertz SC, Kunert HJ, Schwenger UB, Sass H. Affective respon-
siveness in borderline personality disorder: a psychophysiological
approach. Am J Psychiatry 1999; 156:1550–1556.
30. Sowell ER, Thompson PM, Tessner KD, Toga AW. Mapping continued
brain growth and gray matter density reduction in dorsal frontal cortex:
inverse relationships during postadolescent brain maturation. J Neurosci
2001; 15:8819–8829.
31. Rolls ET, Hornak J, Wade D, McGrath J. Emotion-related learning in
patients with social and emotional changes associated with frontal lobe
damage. J Neurol Neurosurg Psychiatry 1994; 57:1518–1524.
J. Taylor532
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

32. Giancola P, Moss H, Martin C, Kirisci L, Tarter R. Executive cognitive
functioning predicts reactive aggression in boys at high risk for sub-
stance dependence: a prospective study. Alcohol Clin Exp Res 1996;20:740–744.
33. Giancola PR, Tarter RE. Executive cognitive functioning and risk for
substance abuse. Psychol Sci 1999; 10:203–205.
34. Stevens MC, Kaplan RF, Hesselbrock VM. Executive-cognitive
functioning in the development of antisocial personality disorder.
Addict Behav 2003; 28:285–300.
35. Shoal GD, Giancola PR. Executive cognitive functioning, negative
affectivity, and drug use in adolescent boys with and without a family
history of a substance use disorder. J Child Adolesc Subst Abuse 2001;10:111–121.
36. Dinn WM, Harris CL, Aycicegi A, Greene PB, Kirkley SM, Reilly C.
Neurocognitive function in borderline personality disorder. Prog Neuro-
Psychopharmacol Biol Psychiatry 2004; 28:329–341.
37. Monarch ES, Saykin AJ, Flashman LA. Neuropsychological impair-
ment in borderline personality disorder. Psychiatr Clin North Am 2004;27:67–82.
38. Stein DJ, Hollander E, Cohen L, Frenkel M. Neuropsychiatric
impairment in impulsive personality disorders. Psychiatry Res 1993;48:257–266.
39. Dolan M, Park I. The neuropsychology of antisocial personality
disorder. Psychol Med 2002; 32:417–427.
40. Morgan AB, Lilienfeld SO. A meta-analytic review of the relation
between antisocial behavior and neuropsychological measures of
executive function. Clin Psychol Rev 2000; 20:113–136.
41. Peterson JB, Finn PR, Pihl RO. Cognitive dysfunction and the
inherited predisposition to alcoholism. J Stud Alcohol 1992; 53:154–
160.
42. Sprock J, Rader TJ, Kendall JP, Yoder CY. Neuropsychological
functioning in patients with borderline personality disorder. J Clin
Psychol 2000; 56:1587–1600.
43. Crowell TA, Kieffer KM, Kugeares S, Vanderploeg RD. Executive and
nonexecutive neuropsychological functioning in antisocial personality
disorder. Cogn Behav Neurol 2003; 16:100–109.
44. Bray JH, Adams GJ, Getz JG, McQueen A. Individuation, peers, and
adolescent alcohol use: a latent growth analysis. J Consult Clin Psychol
2003; 71:553–564.
45. Curran PJ, Stice E, Chassin L. The relation between adolescent alcohol
use and peer alcohol use: a longitudinal random coefficients model.
J Consult Clin Psychol 1997; 65:130–140.
46. Howard MO, Jenson JM. Inhalant use among antisocial youth:
prevalence and correlates. Addict Behav 1999; 24:59–74.
47. Jessor R, Van Den Bos J, Vanderryn J, Costa FM, Turbin MS.
533Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

Protective factors in adolescent problem behavior: moderator effects
and developmental change. Dev Psychol 1995; 31:923–933.
48. Kandel DB. The parental and peer contexts of adolescent deviance: an
algebra of interpersonal influences. J Drug Issues 1996; 26:289–315.
49. Mason WA, Windle M. Family, religious, school and peer influences on
adolescent alcohol use: a longitudinal study. J Stud Alcohol 2001;62:44–53.
50. Barnow S, Schuckit MA, Lucht M, John U, Freyberger HJ. The
importance of a positive family history of alcoholism, parental rejection
and emotional warmth, behavioral problems and peer substance use for
alcohol problems in teenagers: a path analysis. J Stud Alcohol 2002;63:305–315.
51. Dawes M, Clark D, Moss H, Kirisci L, Tarter R. Family and peer
correlates of behavioral self-regulation in boys at risk for substance
abuse. Am J Drug Alcohol Abuse 1999; 25:219–237.
52. Spooner C. Causes and correlates of adolescent drug abuse and
implications for treatment. Drug Alcohol Rev 1999; 18:453–475.
53. Jones-Webb R, Short B, Wagenaar A, Toomey T, Murray D, Wolfson
M, Forster J. Environmental predictors of drinking and drinking-related
problems in young adults. J Drug Educ 1997; 27:67–82.
54. Leonard KE, Mudar PJ. Alcohol use in the year before marriage:
alcohol expectancies and peer drinking as proximal influences on
husband and wife alcohol involvement. Alcohol Clin Exp Res 2000;24:1666–1679.
55. Anisman H, Merali Z. Understanding stress: characteristics and caveats.
Alcohol Res Health 1999; 23:241–249.
56. Kendler KS. Twin studies of psychiatric illness: an update. Arch Gen
Psychiatry 2001; 58:1005–1014.
57. Moran P, Mann A. The prevalence and 1-year outcome of cluster B
personality disorders in primary care. J Forensic Psychiatr 2002;13:527–537.
58. Lykken DT, Venables PH. Direct measurement of skin conductance: a
proposal for standardization. Psychophysiology 1971; 8:656–672.
59. Heaton RK. WCST-64: Computer Version for Windows—Research
Edition [Computer Program]. Odessa, Florida: Psychological Assess-
ment Resources, Inc., 2000.
60. Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtiss G. Wisconsin
Card Sorting Test Manual: Revised and Expanded. Odessa, Florida:
Psychological Assessment Resources, Inc., 1993.
61. Golden CJ. Stroop Color and Word Test: A Manual for Clinical
and Experimental Uses. Wood Dale, Illinois: Stoelting Company,
1978.
62. First MB, Spitzer RG, Gibbon M, Williams JBW. Structured Clinical
Interview for DSM-IV Axis I Disorders, Research Version, Non-Patient
J. Taylor534
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.

Edition (SCID-I/NP). New York: Biometrics Research, New York State
Psychiatric Institute, 2001.
63. Pfohl B, Blum N, Zimmerman M. Structured Interview for DSM-IV
Personality Disorders (SIDP-IV). Iowa City, Iowa: University of Iowa,
1995.
64. Cottler LB, Price RK, Compton WM, Mager DE. Subtypes of adult
antisocial behavior among drug abusers. J Nerv Ment Dis 1995;183:154–161.
65. Elkins IJ, Iacono WG, Doyle AE, McGue M. Characteristics associated
with the persistence of antisocial behavior: results from recent
longitudinal research. Aggress Violent Behav 1997; 2:101–124.
66. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed.Hillsdale, NJ: Lawrence Erlbaum Associates, 1988.
67. Faul F, Erdfelder E. GPOWER: A Priori, Post-Hoc, and Compromise
Power Analyses for MS-DOS [Computer Program]. Bonn, FRG: Bonn
University, Department of Psychology, 1998.
68. Watson DC, Sinha BK. Comorbidity of DSM-IV personality disorders
in a nonclinical sample. J Clin Psychol 1998; 54:773–780.
535Substance Use Disorder Correlates
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Fo
rdha
m U
nive
rsity
on
03/1
0/13
For
pers
onal
use
onl
y.