Substance Use Disorders and ASAM Patient...
69
Substance Use Disorders and ASAM Patient Placement Criteria Rochelle Head-Dunham, MD, FAPA Medical Director/Chief of Adult Services DHH/Office for Behavioral Health
Transcript of Substance Use Disorders and ASAM Patient...
Substance Use Disorders and ASAM Patient Placement Criteria
Rochelle Head-Dunham, MD, FAPA Medical Director/Chief of Adult Services DHH/Office for Behavioral Health
Objectives
1. Discuss defining criteria for Substance Use Disorders
2. Highlight General Principles of the Neurobiology of Addiction
3. Review the American Society of Addiction Medicine’s (ASAM) Patient Placement Criteria

SUBSTANCE USE DISORDERS
4

Terminology
• Dual-disorders vs Co-occurring Disorders • Use vs Misuse vs Abuse • Tolerance vs Physiological Dependence • Physiological Dependence vs Addiction • Pseudo-addiction • Assessment vs Patient Placement Criteria
5
General Principles & Considerations
• Heterogeneity of the addiction populations
• Diagnosing with expectation not exception • Holistic evaluations and comprehensive
treatment planning • Unique person-centered and family
focused treatment approaches are required to enhance outcomes
• Significant predictors of treatment success are continuous, empathic relationships and coordination of care
6
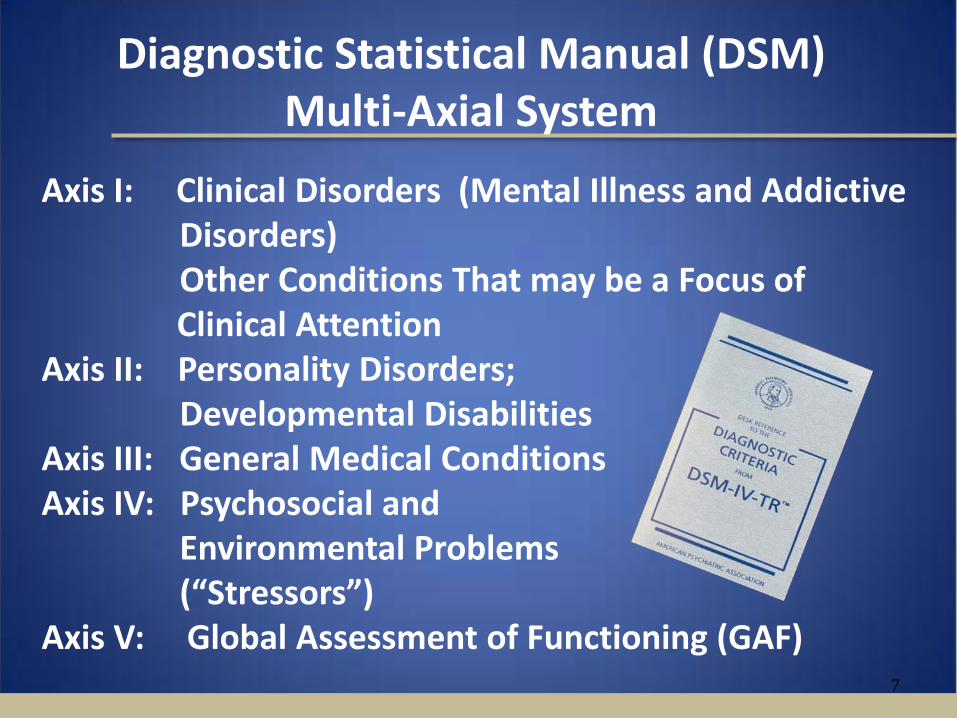
Diagnostic Statistical Manual (DSM) Multi-Axial System
7
Axis I: Clinical Disorders (Mental Illness and Addictive Disorders) Other Conditions That may be a Focus of Clinical Attention Axis II: Personality Disorders; Developmental Disabilities Axis III: General Medical Conditions Axis IV: Psychosocial and Environmental Problems (“Stressors”) Axis V: Global Assessment of Functioning (GAF)
8

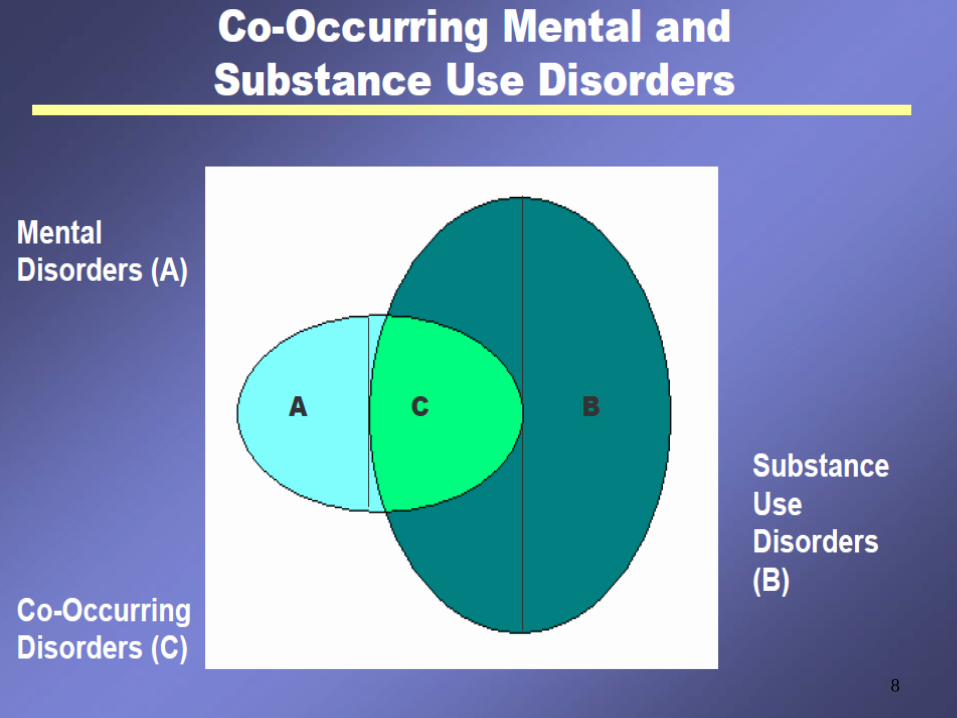
Interrelationship of Substance Use and Mental (Psychiatric) Disorders
Psychiatric disorders and substance use disorders can evolve independently through different, unrelated processes
Symptoms of psychiatric and substance use disorders can be expressed independently or simultaneously
Both disorders can mimic or mask symptoms of the other, i.e., cocaine intoxication can mimic schizophrenic; depression can mimic cocaine induced mood disorder.
A relapse of one disorder can precipitate acute symptoms of the other disorder.
Psychiatric symptoms may emerge with cessation of alcohol/drug use (i.e., first break schizophrenic).

Commonly Co-Occurring Mental Disorders (Axis I)
1. Mood Disorders are disorders that present with a disturbance in
mood as a predominant feature; Major Depressive Disorders, Bipolar Disorders, substance Induced Mood Disorders, commonly co-occur with addictive disorders
2. Anxiety Disorders are disorders that present with anxiety (fear) as
the predominant feature. Panic disorder, Social Anxiety Disorder, Generalized Anxiety Disorder, and Post-Traumatic Stress Disorder, commonly co-occur with addictive disorders.
3. Psychotic Disorders are disorders which typically present with
“psychosis” or gross impairment in reality testing evidenced by delusional thinking, disorganized speech, or disorganized/ catatonic behavior. Schizophrenia, Schizoaffective disorder, and Delusional disorder, co-occur with addictive disorders.
10
Personality Disorders Co-occur with Substance Use (Axis II)
A Personality Disorder is an enduring
pattern of inner experience and behavior that deviates markedly from the
expectations of the individual’s culture, is pervasive and inflexible, has an onset in
adolescence or early adulthood, is stable over
time, and leads to distress or impairment, and is
manifested in at least two of the following areas:
Cognition, Affectivity, Interpersonal functioning or Impulse Control.
DSM-IV TR

Medical Co-morbidity and Substance Use (Axis III)
12
Inhalant use among 12 – 17 year olds and depression are increasing;
Patients in chemical dependency programs are 18 times more likely to have major psychosis, 15 times more likely to have depression and 9 times more likely to have an anxiety disorder;
Substance use increases the risk for hypertension (x2), congestive heart failure (x9) and pneumonia (x12);
HIV patients with a substance use disorder are more likely to be non-adherent;
Medicaid patients with a substance use disorder are more likely to be readmitted to a hospital within 30 days;

Medical Co-morbidity and Substance Use (Axis III)
13
Substance use creates increased rates of complications with hip replacements;
Patients treated with medication for alcoholism had fewer detoxification, alcohol related inpatient days and emergency room visits;
High cost Medicaid recipients with HIV had an average annual cost of $157,000, with 40% higher costs for treatment of co-morbid MH/SU disorders , the most common co-morbidities
Treating patients with substance use related medical disorders in an integrated setting can achieve cost savings;
Definition of Substance Related Disorders
Substance Related Disorders are disorders resulting from ingestion of a drug of abuse (including alcohol), along with the development of the side effects of a medication, or from toxin exposure.” “Substance” can refer to a drug of abuse, a medication, or a toxin. Patterns of use have been researched for eleven substances: Alcohol, Amphetamine, Caffeine, Cannabis, Cocaine, Hallucinogens, Inhalants, Nicotine, Opioids, Phencyclidines and Sedative hypnotics/Benzodiazepines.
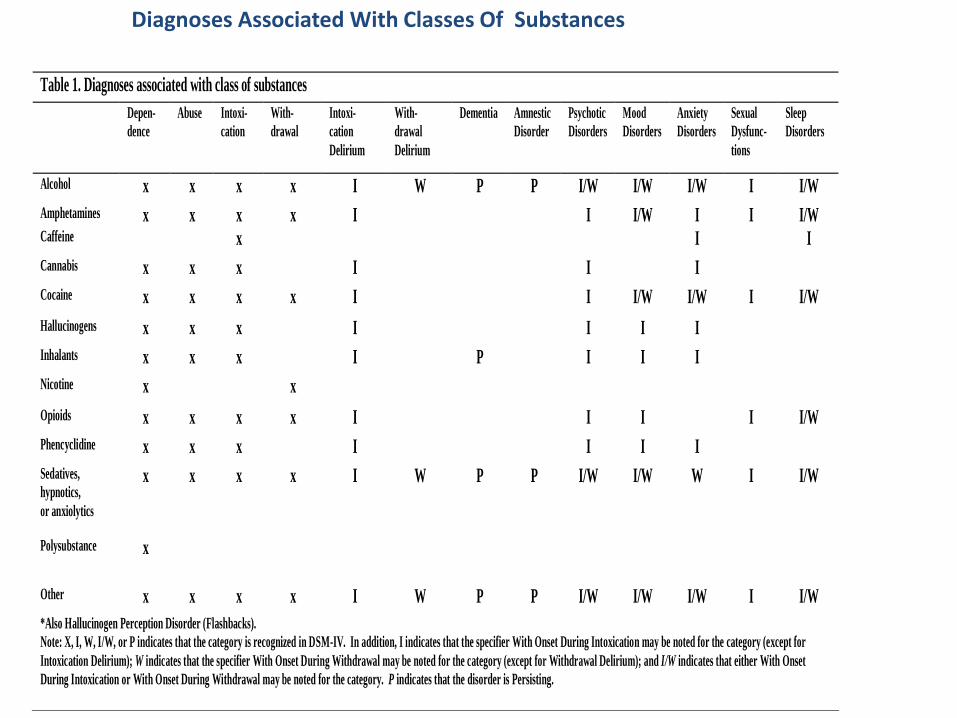
Diagnoses Associated With Classes Of Substances
Table 1. Diagnoses associated with class of substances Depen-
dence Abuse Intoxi-
cation With- drawal
Intoxi- cation Delirium
With- drawal Delirium
Dementia Amnestic Disorder
Psychotic Disorders
Mood Disorders
Anxiety Disorders
Sexual Dysfunc- tions
Sleep Disorders
Alcohol x x x x I W P P I/W I/W I/W I I/W Amphetamines x x x x I I I/W I I I/W Caffeine x I I Cannabis x x x I I I Cocaine x x x x I I I/W I/W I I/W Hallucinogens x x x I I I I Inhalants x x x I P I I I Nicotine x x Opioids x x x x I I I I I/W Phencyclidine x x x I I I I Sedatives, hypnotics, or anxiolytics
x
x x x I
W P P I/W I/W W I I/W
Polysubstance
x
Other x x x x I W P P I/W I/W I/W I I/W *Also Hallucinogen Perception Disorder (Flashbacks). Note: X, I, W, I/W, or P indicates that the category is recognized in DSM-IV. In addition, I indicates that the specifier With Onset During Intoxication may be noted for the category (except for Intoxication Delirium); W indicates that the specifier With Onset During Withdrawal may be noted for the category (except for Withdrawal Delirium); and I/W indicates that either With Onset During Intoxication or With Onset During Withdrawal may be noted for the category. P indicates that the disorder is Persisting.

Diagnoses Associated With Classes Of Substances (Illustrated)
Table 1. Diagnoses associated with class of substances Depen-
dence Abuse Intoxi-
cation With- drawal
Intoxi- cation Delirium
With- drawal Delirium
Dementia Amnestic Disorder
Psychotic Disorders
Mood Disorders
Anxiety Disorders
Sexual Dysfunc- tions
Sleep Disorders
Classes of Substances Alcohol
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W
Amphetamines
x
x
x
x
I
I
I/W
I
I
I/W
Caffeine
x
I I
Cannabis
x
x
x
I
I
I
Cocaine
x
x
x
x
I
I
I/W
I/W
I
I/W
Hallucinogens
x
x
x
I
I
I
I
Inhalants
x
x
x
I
P
I
I
I
Nicotine
x
x
Opioids
x
x
x
x
I
I
I
I
I/W
Phencyclidine
x
x
x
I
I
I
I
Sedatives, hypnotics, or anxiolytics
x
x
x
x
I
W
P
P
I/W
I/W
W
I
I/W
Polysubstance
x
Other
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W

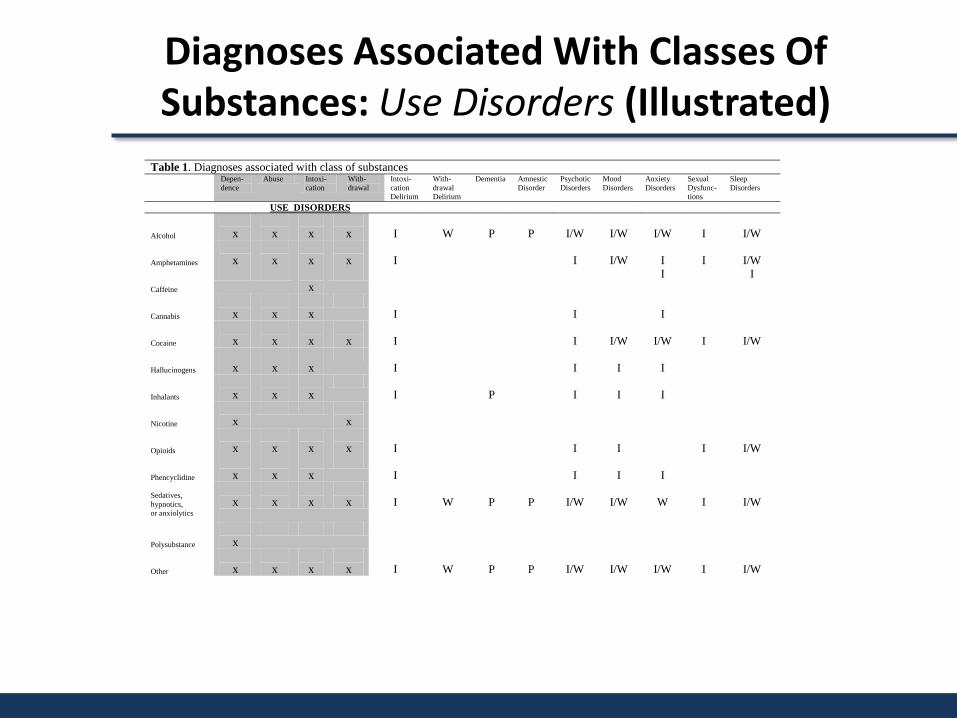
Diagnostic Considerations DSM IV-TR
The Diagnostic and Statistical Manual (DSM-IV) has established two broad categories for the
distinction of Addictive Disorders: A. “Use Disorders” are those diagnostic states which
name the substance of abuse and assign severity (i.e., alcohol abuse or dependence…) or acuity (cocaine intoxication or withdrawal).
B. “Induced Disorders” are those diagnostic states which occur as a result of the psychological consequences of ingested chemicals (i.e.., cocaine induced psychosis, methamphetamine induced mood disorder…).
17

Diagnostic Determinants
• Diagnostic determinants of “Abuse” versus “Dependence”, “Withdrawal” versus “Intoxication” are drug pharmacology and behavioral patterns/consequences of use
• Rationale for appropriate placement decisions must take into consideration, all of the above as determinants of severity and acuity.

Diagnostic Determinants
“Use Disorders” Intoxication and Withdrawal
Diagnoses Associated With Classes Of Substances: Use Disorders (Illustrated)
Table 1. Diagnoses associated with class of substances Depen-
dence Abuse Intoxi-
cation With- drawal
Intoxi- cation Delirium
With- drawal Delirium
Dementia Amnestic Disorder
Psychotic Disorders
Mood Disorders
Anxiety Disorders
Sexual Dysfunc- tions
Sleep Disorders
USE DISORDERS Alcohol
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W
Amphetamines
x
x
x
x
I
I
I/W
I
I
I/W
Caffeine
x
I I
Cannabis
x
x
x
I
I
I
Cocaine
x
x
x
x
I
I
I/W
I/W
I
I/W
Hallucinogens
x
x
x
I
I
I
I
Inhalants
x
x
x
I
P
I
I
I
Nicotine
x
x
Opioids
x
x
x
x
I
I
I
I
I/W
Phencyclidine
x
x
x
I
I
I
I
Sedatives, hypnotics, or anxiolytics
x
x
x
x
I
W
P
P
I/W
I/W
W
I
I/W
Polysubstance
x
Other
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W
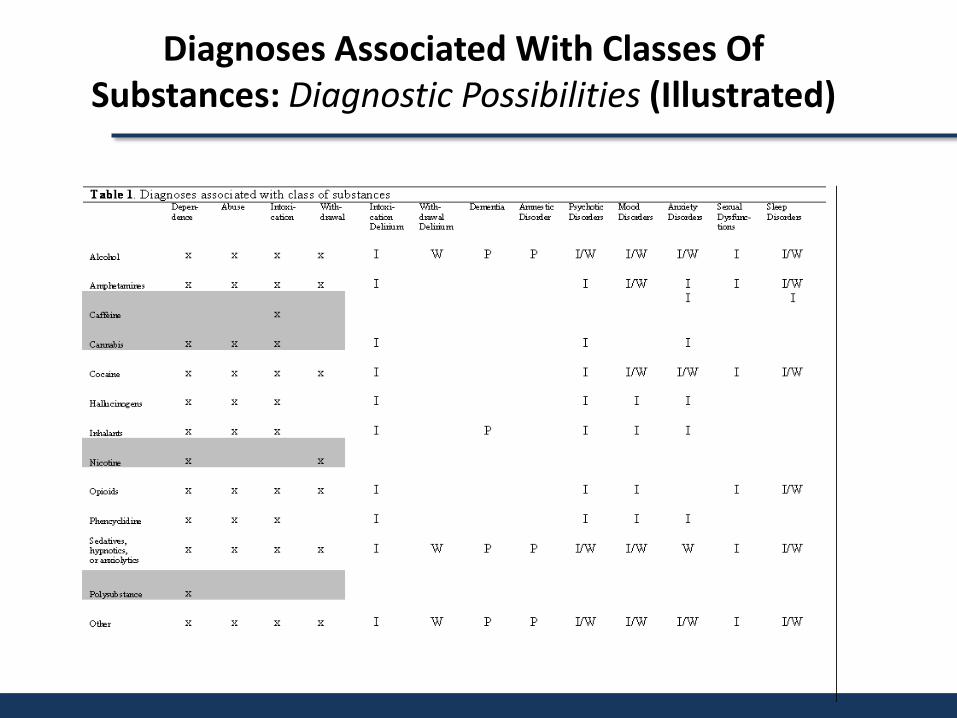
Diagnoses Associated With Classes Of Substances: Diagnostic Possibilities (Illustrated)
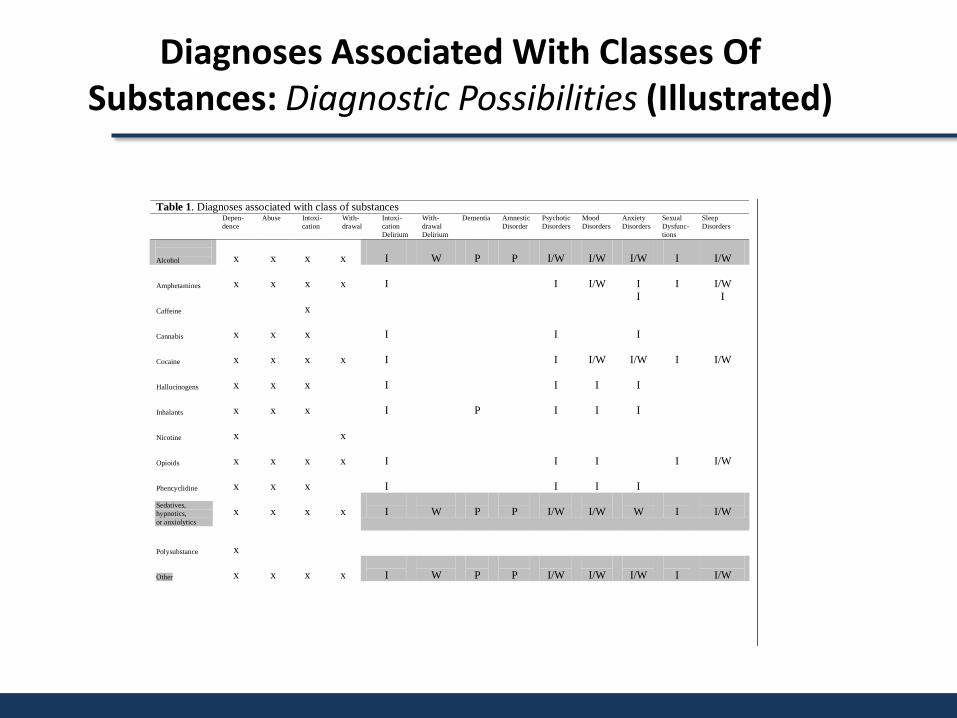
Diagnoses Associated With Classes Of Substances: Diagnostic Possibilities (Illustrated)
Table 1. Diagnoses associated with class of substances Depen-
dence Abuse Intoxi-
cation With- drawal
Intoxi- cation Delirium
With- drawal Delirium
Dementia Amnestic Disorder
Psychotic Disorders
Mood Disorders
Anxiety Disorders
Sexual Dysfunc- tions
Sleep Disorders
Alcohol
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W
Amphetamines
x
x
x
x
I
I
I/W
I
I
I/W
Caffeine
x
I I
Cannabis
x
x
x
I
I
I
Cocaine
x
x
x
x
I
I
I/W
I/W
I
I/W
Hallucinogens
x
x
x
I
I
I
I
Inhalants
x
x
x
I
P
I
I
I
Nicotine
x
x
Opioids
x
x
x
x
I
I
I
I
I/W
Phencyclidine
x
x
x
I
I
I
I
Sedatives, hypnotics, or anxiolytics
x
x
x
x
I
W
P
P
I/W
I/W
W
I
I/W
Polysubstance
x
Other
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W

Medication Options
“Induced Disorders”

Medication Considerations
Medications and Induced States • Drugs and Alcohol induce a complex array of
symptoms which are very similar to mental disorders in those who do not use drugs and alcohol.
• Use of psychotropic medications is therefore indicated to manage the psychiatric symptoms, independent of the cause for their expression. (Some cautions are necessary.)
24

Diagnoses Associated With Classes Of Substances: Induced Disorders (Illustrated)
Table 1. Diagnoses associated with class of substances Depen-
dence Abuse Intoxi-
cation With- drawal
Intoxi- cation Delirium
With- drawal Delirium
Dementia Amnestic Disorder
Psychotic Disorders
Mood Disorders
Anxiety Disorders
Sexual Dysfunc- tions
Sleep Disorders
INDUCED DISORDERS Alcohol
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W
Amphetamines
x
x
x
x
I
I
I/W
I
I
I/W
Caffeine
x
I I
Cannabis
x
x
x
I
I
I
Cocaine
x
x
x
x
I
I
I/W
I/W
I
I/W
Hallucinogens
x
x
x
I
I
I
I
Inhalants
x
x
x
I
P
I
I
I
Nicotine
x
x
Opioids
x
x
x
x
I
I
I
I
I/W
Phencyclidine
x
x
x
I
I
I
I
Sedatives, hypnotics, or anxiolytics
x
x
x
x
I
W
P
P
I/W
I/W
W
I
I/W
Polysubstance
x
Other
x
x
x
x
I
W
P
P
I/W
I/W
I/W
I
I/W

DSM V Eliminates the Multi-Axial System
• Axis I, II, and III (all diagnosis) are combined • Axis IV Stressors are eliminated, replaced by
– ICD-9-CM V codes – ICD-10-CM Z codes after October 2014
• Axis V GAF is eliminated-new options are – World Health Organization Disability Assessment
Schedule (WHO-DAS 2.0)
26
DSM-V Diagnostic Considerations
• Substance-Related and Addictive Disorders • Substance Abuse and Substance Dependence now
consolidated into “Substance Use Disorder”, with severity continuum of mild, moderate, or severe
• Legal consequences criterion removed and craving criterion added to “Substance Use Disorder”
• Tolerance and Withdrawal criteria are not counted if the substance is prescribed by a physician
• “Gambling Disorder” has been moved from the Impulse-Control Disorders chapter in DSM-IV to this chapter in DSM-5
27

NEUROBIOLOGY OF ADDICTION
28

What is Addiction?
The repetitive compulsive use of anything in spite of adverse consequences and
ineffectiveness. This is regardless of the drug
or behavior used.
What are we Addicted to?
Below the level of the cortex the brain has a reward center. This center is necessary for us to learn what we should do again. It is a necessary survival mechanism. It can go awry and when it does we can be addicted. The main neurotransmitter active at this
site is DOPAMINE. Wetsman, 2007

The Dopamine Spike
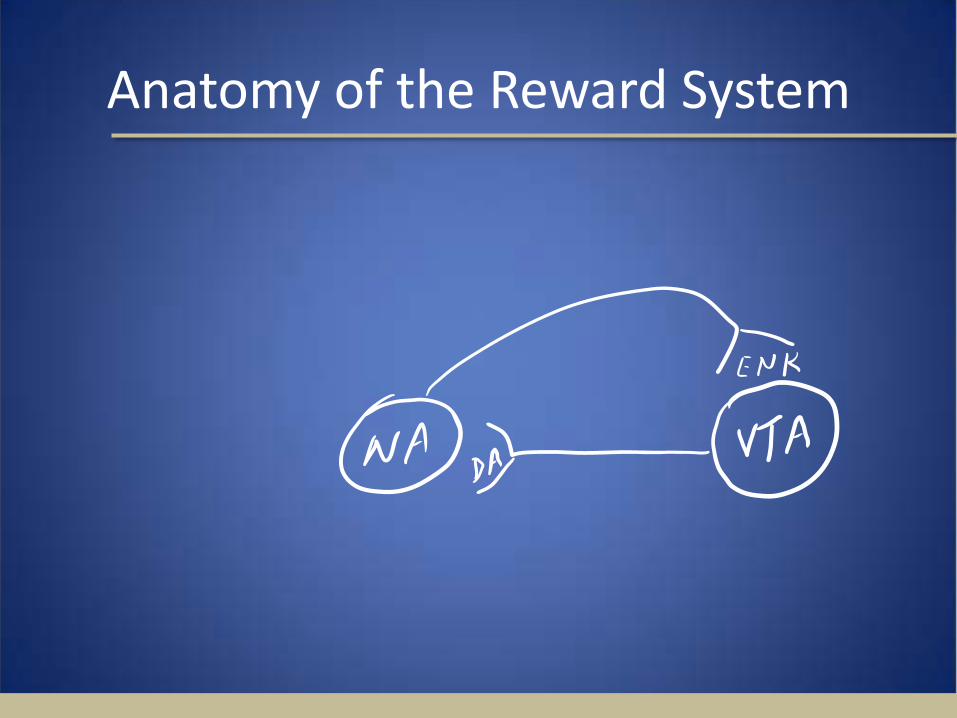
Anatomy of the Reward System

Dopamine Spike
• Electrical stimulation of the MFB in humans
• Electrical self stimulation of the MFB in mammals
• Degree of reward varies with rate of rise • Craving starts on the way down • Everyone has enough at the peak
Wetsman, 2007

The Reward System
Non-selective and
Indiscriminant

Addiction Definitions
• Impaired control • Preoccupation with the drug • Use despite adverse consequences • Distortions in cognition (denial and others)
ASAM • Addiction can be defined as compulsive
drug seeking and drug taking, with a loss of control over drug use. APA
• Maladaptive pattern of use • Significant impairment or distress • Three or more of the following within any 12 month
period: DSMIV
35

Definitions DSMIV (cont’d)
Tolerance
Withdrawal
Broken limits
Persistent desire or unsuccessful efforts
Excessive time spent
Important activities given up
Use despite adverse consequences
36

Why Addiction, Not Dependence?
History of the term “Dependence” and the APA. WHO and physically vs psychologically
“addicting.” Addiction without physical dependence. Dependence without addiction. Dependence vs. Tolerance
Wetsman, 2007
So What About Abuse?
Addiction is a sick brain doing it’s best to feel better. Abuse is a healthy brain doing stupid
things with drugs. There is no evidence of one leading to
the other. You can have one or the other first and then develop the other one.
Wetsman, 2007
So What About Abuse
Abuse is to “won’t” -- as addiction is to “can’t”. Abuse is a normal brain needing no
medicines (other than for whatever else is wrong with it) and addiction is an ill brain that often needs medical help. Treatments for Abuse vs Dependence
are Different!
Wetsman, 2007

DSM IV-TR Abuse (Cont)
Key Point: THE SYMPTOMS HAVE NEVER MET
THE CRITERIA FOR SUBSTANCE DEPENDENCE FOR THIS CLASS OF
SUBSTANCE. Wetsman, 2007

American Society of Addiction Medicine -
Patient Placement Criteria (ASAM–PPC)
41

42
What is happening in some programs in America?
• Clients are being referred to the wrong levels of care.
• Clients are often referred to, and treated in the agency conducting the
assessment.
• Clinical Assessments do not justify the recommendations being made.
• Clinical Justifications are not required.
• If provided clinical justifications do not include clinical rationale / evidence supporting the recommendation.
• There are little to no policies or procedures that address the format and or quality of assessments, patient placement decisions, and clinical justifications

43
Why Do We Need to Improve Patient Placement and Clinical Justifications?
• Improved Performance and Treatment Outcomes
• Increase Initiation, Engagement & Retention Rates
• More Efficient & Effective Utilization of Resources
• Shift to Performance Based Contracting
• Positions Organizations for Medicaid and Private Insurance Reimbursement
44
Question
QUESTION: How does this lack of consistency interpreting clinical information impact treatment?
45
Treatment Implications
Answer: Client’s receive the Wrong……… 1. Diagnosis or Diagnostic Impression 2. Level of Care Recommendation 3. Services and Interventions
As a result, the client’s chances of being
successful in treatment are compromised right from the beginning of the treatment process.

46
Question
QUESTION: What Does Research Say About Mismatching Clients to Treatment?

Louisiana Department of Health and 47
Treatment Implications
ANSWER: Clients that are mismatched to treatment have lower retention rates and poorer outcomes. Less treatment is NOT Good. More treatment is NOT Good. One study found that No Treatment was better than the wrong treatment. (Knight, K., 2009)
48
• Uniform Patient Placement Criteria (e.g., ASAM, LOCUS …) describe in detail the levels of care along the continuum of care, and provide specific guidelines for Patient Placement Decisions, a.k.a., Level of Care recommendations.
General Components of UPPC Level of Care Continuum Dimensions of Assessment Criteria (e.g., admission, continued stay & discharge)
Uniform Patient Placement Criteria Defined
49
ASAM Dimensions
• ASAM Six (6)Dimensions: The client’s risk status in each of the six dimensions collectively inform the patient
placement decision.
1. Acute Intoxication and/or Withdrawal Potential.
2. Biomedical Conditions and Complications.
3. Emotional, Behavioral, or Cognitive Problems and Complications.
4. Readiness to Change.
5. Relapse, Continued Use, or Continued Problem Potential
6. Recovery Environment.
50
Benefits of UPPC • Uniform Patient Placement Criteria:
1. Guides proper patient placement.
2. Promotes individualized care.
3. Identifies critical information to be collected during an assessment.
4. Influences multidimensional treatment planning.
5. Establishes a common language.
6. Identifies gaps in a continuum of care.

51
IMPORTANT !!!
Criteria are NOT substitutes for GOOD Clinical Judgment.
Tools, and Criteria’s support, guide
and enhance GOOD Clinical Judgment!

ASAM PPC - 2R
ASAM Historical and Theoretical Foundations
The ASAM PPC – 2 is published by the American Society of Addiction Medicine. Used as a clinical guide in matching patients
to the correct level of care. Expands use of multidimensional assessments
in developing objective patient placement decisions at various levels of care. Emphasis on intensities of along a continuum,
in a variety of program types and levels of care
52

ASAM PPC - 2R
ASAM Historical and Theoretical Foundations
• The continuing development and refinement of the criteria continue a shift from:
Uni-dimensional to multidimensional assessment.
Program-driven to clinically driven treatment.
Fixed length of service to variable length of service.
A limited number of discrete levels of care to a continuum of care.
53
ASAM PPC - 2R
Theoretical Foundations of the ASAM PPC
• Goals of Treatment: Tailored to individuals needs (length, choice) Guided by individualized treatment plan. Client directed treatment plan. Based on comprehensive bio-psychosocial assessment
of person and when possible, family. Should list problems, strengths, priorities, goals,
methods or strategies. Safety first
54
ASAM Placement Considerations
• Placement decisions are determined based upon consideration of:
Level of Service/Care most appropriate to meet the clinical needs
Dimensional Assessments “Primary” and “Secondary “ Determinants
Louisiana Department of Health and Hospitals 55

ASAM PPC - 2R
Exceptions to PPC There are 3 exceptions which override the PPC match: Lack of the availability of the appropriate selected care.
Failure of a patient to progress at a given level of care so
as to warrant a reassessment of the treatment plan with a view to modification of the treatment approach.
State laws regulating requiring different criteria.
56

ASAM PPC - 2R
ASAM Levels of Service
• Levels of Care: Level 0.5 Early Intervention Level I Outpatient Treatment Level II Intensive Outpatient / Partial Hospitalization Level III Residential/Inpatient Treatment Level IV Medically Managed Intensive Hospital/Inpatient Treatment
• (Note: .1 to .9 represents graduated intensity within an existing level of care.)
57
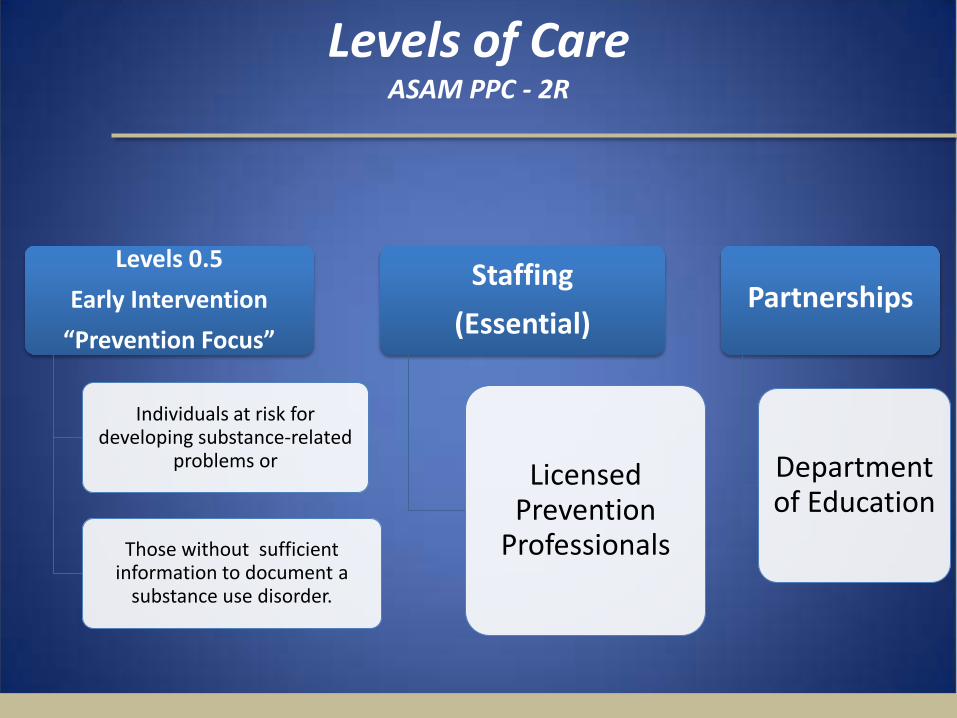
Levels of Care ASAM PPC - 2R
Levels 0.5 Early Intervention
“Prevention Focus”
Individuals at risk for developing substance-related
problems or
Those without sufficient information to document a
substance use disorder.
Staffing (Essential)
Licensed Prevention
Professionals
Partnerships
Department of Education

Levels of Care ASAM PPC - 2R
Levels I
Outpatient Care (<9hrs/week Adults <6hrs/week Adols)
Organized services delivered in a wide variety of outpatient settings.
Prescriptive services, regularly scheduled sessions, a defined set of policies and
procedures or medical protocols.
Accommodates high severity D4, unmotivated mandated persons;
expanded for COD
Staffing (Essential)
MD, Nurse, Clinicians/
Counselors, Care
Coordinator, Peer Mentors
(strongly recommended)

Levels of Care ASAM PPC - 2R
Level II Intensive
Outpatient/Partial Hospitalization (>9hrs/wk)
Partial 9-20hrs/wk; IOP 20hrs/</wk
Organized, clinically intensive services delivered during the day, before or after
work/school, in the evening or on weekends.
Provides essential education and treatment components while allowing patients to apply their newly acquired skills within “real world”
environments.
Staffing (Essential)
MD, Nurse, Clinicians/
Counselors, Care
Coordinator, Peer Mentors
(strongly recommended
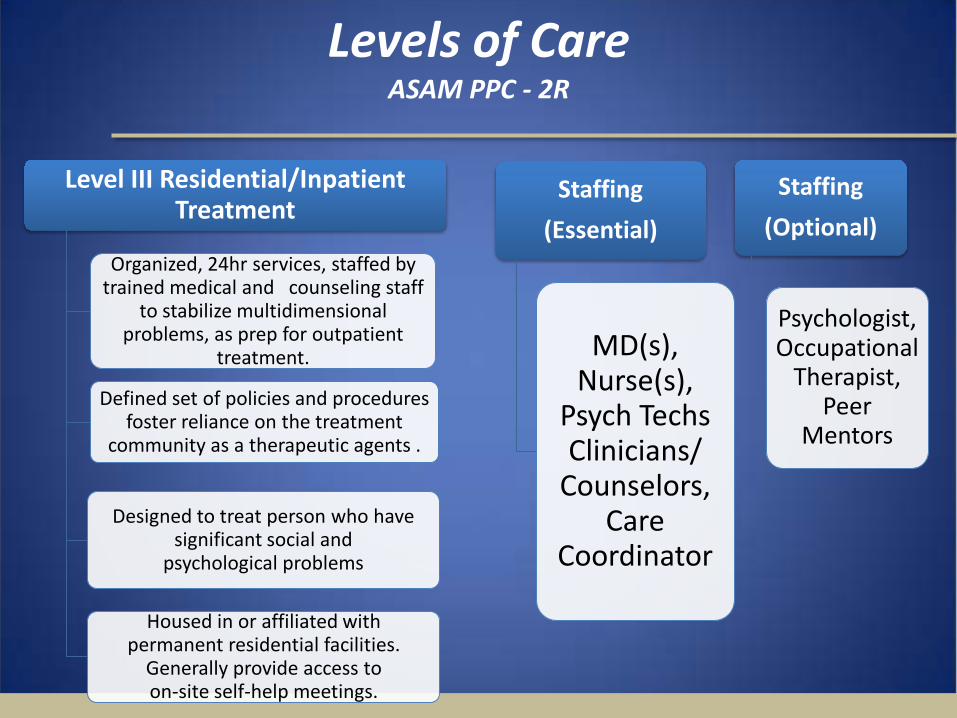
Levels of Care ASAM PPC - 2R
Level III Residential/Inpatient
Treatment
Organized, 24hr services, staffed by trained medical and counseling staff
to stabilize multidimensional problems, as prep for outpatient
treatment.
Defined set of policies and procedures foster reliance on the treatment
community as a therapeutic agents .
Designed to treat person who have significant social and
psychological problems
Housed in or affiliated with permanent residential facilities.
Generally provide access to on-site self-help meetings.
Staffing (Essential)
MD(s), Nurse(s),
Psych Techs Clinicians/
Counselors, Care
Coordinator
Staffing (Optional)
Psychologist, Occupational
Therapist, Peer
Mentors
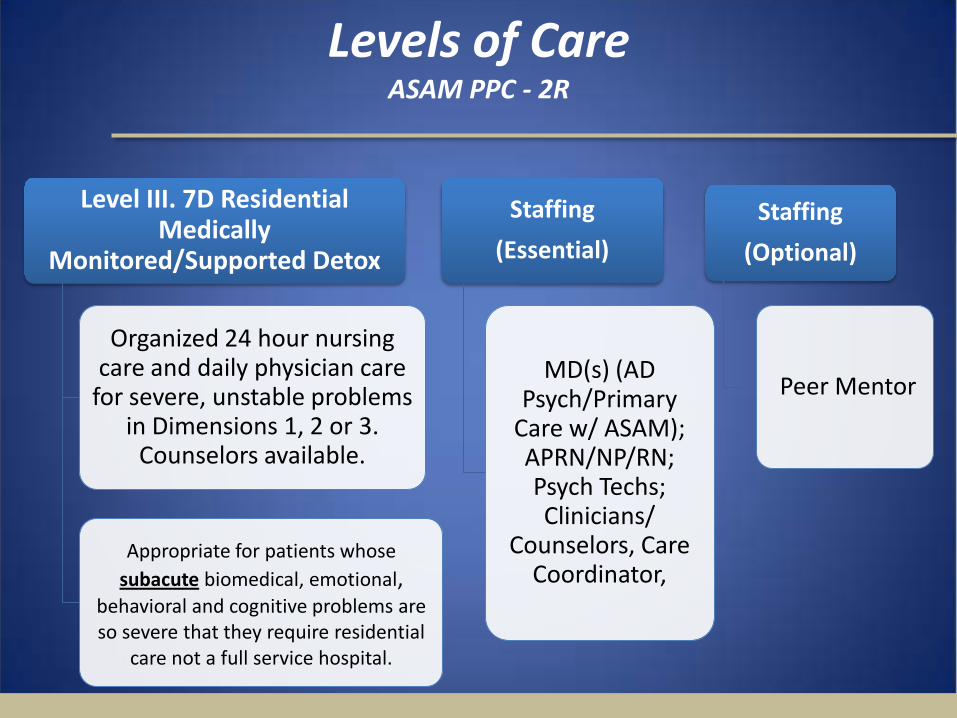
Levels of Care ASAM PPC - 2R
Level III. 7D Residential
Medically Monitored/Supported Detox
Organized 24 hour nursing care and daily physician care
for severe, unstable problems in Dimensions 1, 2 or 3.
Counselors available.
Appropriate for patients whose
subacute biomedical, emotional, behavioral and cognitive problems are so severe that they require residential
care not a full service hospital.
Staffing (Essential)
MD(s) (AD Psych/Primary
Care w/ ASAM); APRN/NP/RN; Psych Techs; Clinicians/
Counselors, Care Coordinator,
Staffing (Optional)
Peer Mentor

Levels of Care ASAM PPC - 2R
Level IV.D Medically Managed Intensive Hospital/ Inpatient
Treatment
Organized 24 hour nursing care and daily physician care for
severe, unstable problems in Dimensions 1, 2 or 3. Counselors available.
Appropriate for patients whose acute biomedical, emotional, behavioral and cognitive problems are so severe that
they require primary medical and nursing care
Full resources of a general
acute care psychiatric hospital are available.
Staffing (Essential)
MD(s) (AD Psych/Primary
Care w/ ASAM); APRN/NP/RN; Psych Techs; Clinicians/
Counselors, Care Coordinator,
Staffing (Optional)
Peer Mentor
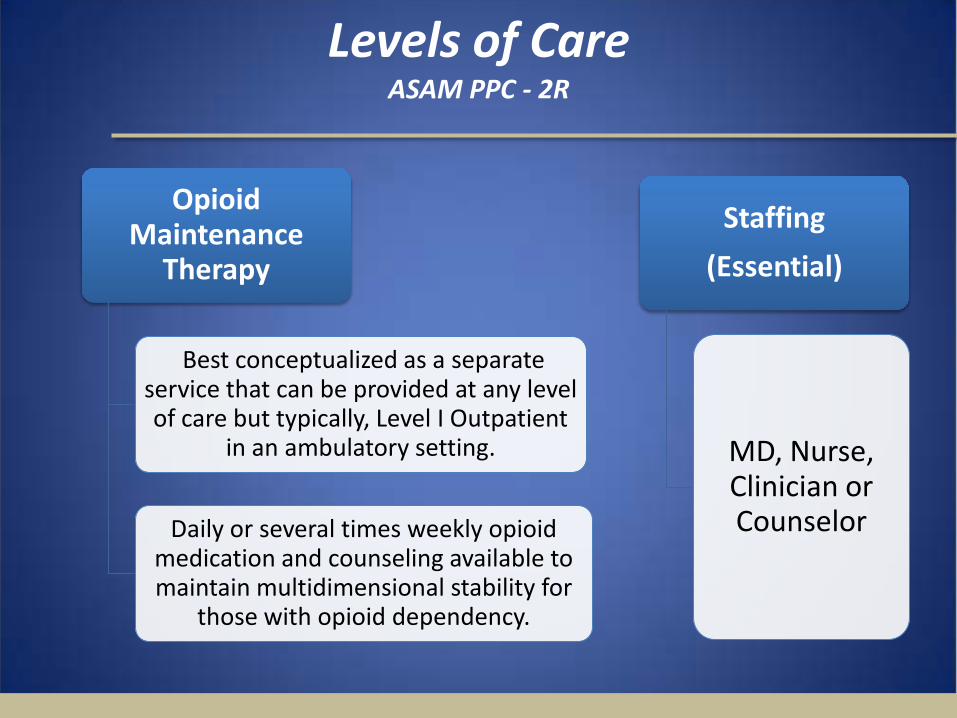
Levels of Care ASAM PPC - 2R
Opioid
Maintenance Therapy
Best conceptualized as a separate service that can be provided at any level of care but typically, Level I Outpatient
in an ambulatory setting.
Daily or several times weekly opioid medication and counseling available to maintain multidimensional stability for
those with opioid dependency.
Staffing (Essential)
MD, Nurse, Clinician or Counselor

Dimensional Criteria ASAM’s 6 assessment dimensions allow for
multidimensional considerations in the determination of best level of care placements.
Primary Determinants • Acute Detox • Medical Complications • Psychiatric Difficulties
Secondary Determinants • Change readiness • Relapse, continued use, continued
problem potential • Recovery/Living Environment
Summary
• Addiction populations are heterogeneous • Neurobiology of addiction supports a chronic,
relapsing condition and the disease concept • Diagnose with expectation not exception • Holistic evaluations and comprehensive
treatment planning with care coordination are critical
• Appropriate “dosing” of care is critical to successful outcomes
• Unique person-centered, family focused empathic treatment approaches are required to enhance outcomes
66

Louisiana Department of Health and Hospitals 67
References • American Psychiatric Association, Diagnostic and Statistical manual of Mental
Disorders, Fourth Edition, Text Revision. Washington DC, American Psychiatric Association, 2000.
• Carroll, K.M. Methodological issues and problems in the assessment of substance use. Psychological Assessment 7:349–358, 1995.
• Donovan, D.M., and Marlatt, G.A., eds. Assessment of Addictive Behaviors. New York: Guilford Press, 1988.
• McLellan, A.T.; Kushner, H.; Metzger, D.; Peters, R.; Smith, I.; Grissom, G.; Pettinati, H.; and Argeriou, M. The fifth edition of the Addiction Severity Index. J Substance Abuse Treat 9:199–213, 1992b.
Louisiana Department of Health and Hospitals 68
References • Mee-Lee, D.; Shulman, G.D.; Fishman, M.; Gastfriend, D.R.; and Grifith, J.H. Patient Placement
Criteria for the Treatment of Substance-Related Disorders. 2d ed., rev. Chevy Chase, MD: American Society of Addiction Medicine, 2001.
• Meyers, A. Thomas McLellan, J. Jaeger, H. Pettinati ,The development of the comprehensive addiction severity index for adolescents (CASI-A) An interview for assessing multiple problems of adolescents. Journal of Substance Abuse Treatment, Volume 12, Issue 3, Pages 181-193 K.
• Spitzer, R.L., Williams, J.B.W., Gibbon, M. & First, M.B. Structured Clinical Interview for DSM- III-R-Patient Version. New York: New York State Psychiatric Institute, Biometrics Research Department, 1988.
• Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R., & Dunbar, G.C. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-1V and ICD-10. Journal of Clinical Psychiatry, 59 (suppl. 20), 1998.