Substance Related Disorders Brian Smart, M.D. Harborview Medical Center.
Upload
rosamond-franklinCategory
view
225download
2
Substance-Related Disorders
Perspectives on Substance-Related Disorders
• The Nature of Substance-Related Disorders
– Problems related to the use and abuse of psychoactive substances
– Produce wide-ranging physiological, psychological, and behavioral effects
• Some Important Terms and Distinctions
– Substance use vs. substance intoxication
– Substance abuse vs. substance dependence
– Tolerance vs. withdrawal
Perspectives on Substance-Related Disorders (cont.)
• Five Main Categories of Substances
– Depressants – Result in behavioral sedation (e.g., alcohol, sedative, anxiolytic drugs)
– Stimulants – Increase alertness and elevate mood (e.g., cocaine, nicotine, caffeine)
– Opiates – Primarily produce analgesia and euphoria (e.g., heroin, morphine, codeine)
– Hallucinogens – Alter sensory perception (e.g., marijuana, LSD)
– Other drugs of abuse – Include inhalants, anabolic steroids, medications
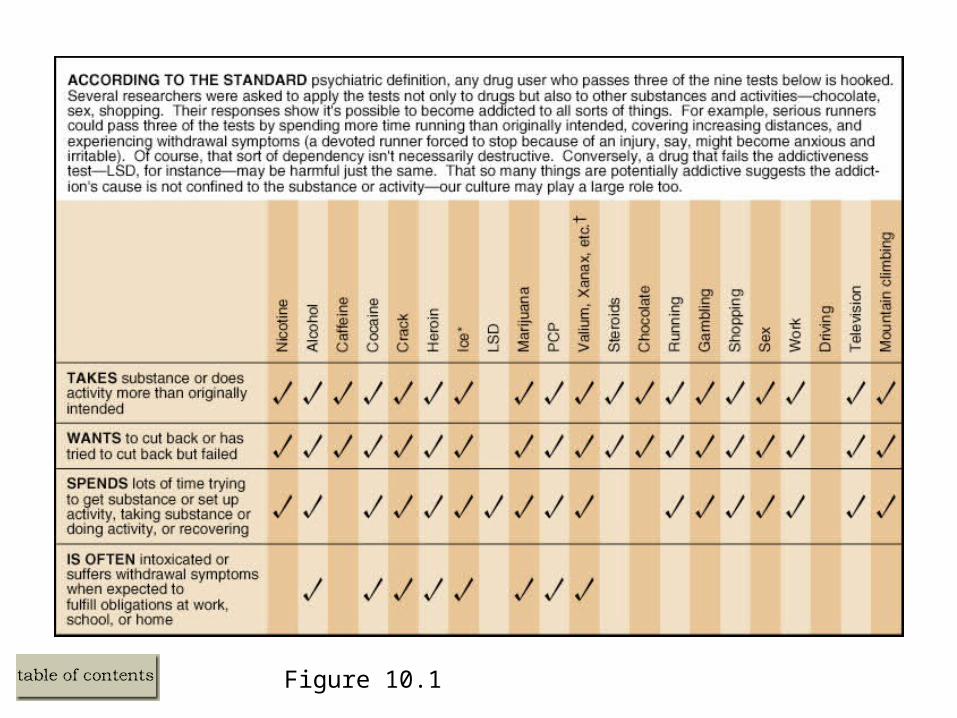
Figure 10.1
• **Ice, LSD, chocolate, TV: Is everything addictive?
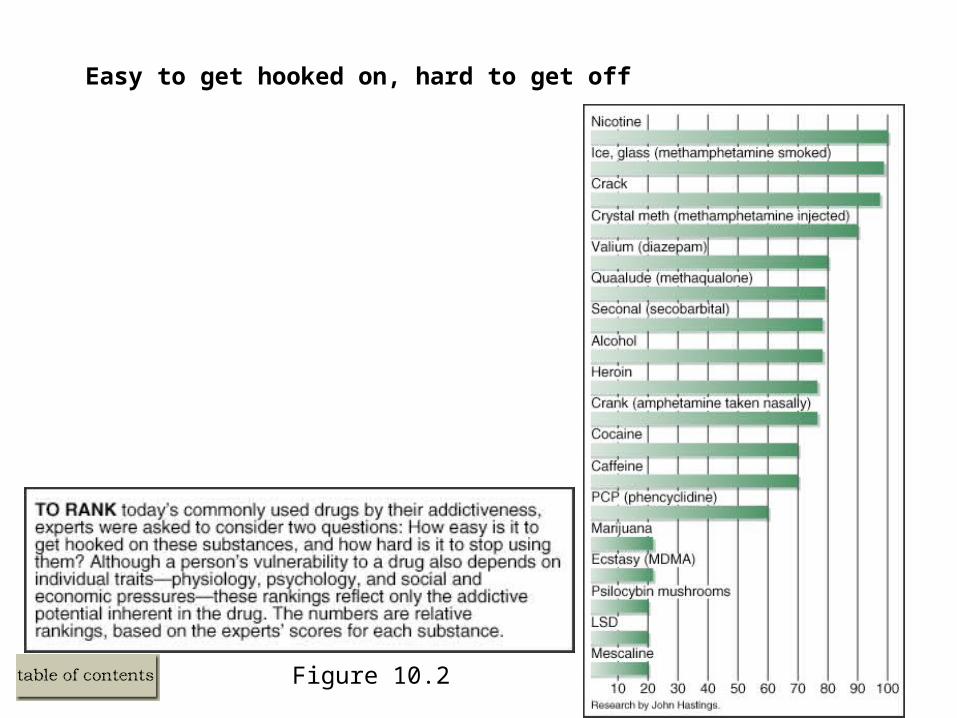
Figure 10.2
Easy to get hooked on, hard to get off
The Depressants: Alcohol Use Disorders
• Psychological and Physiological Effects of Alcohol
– Central Nervous system depressant
– Influences several neurotransmitter systems, but mainly GABA
• Effects of Chronic Alcohol Use
– Alcohol intoxication
– Alcohol withdrawal
– Associated brain conditions – Demenita and Wernicke’s disease
– Fetal alcohol syndrome
• DSM-IV Criteria for Disordered Alcohol Use
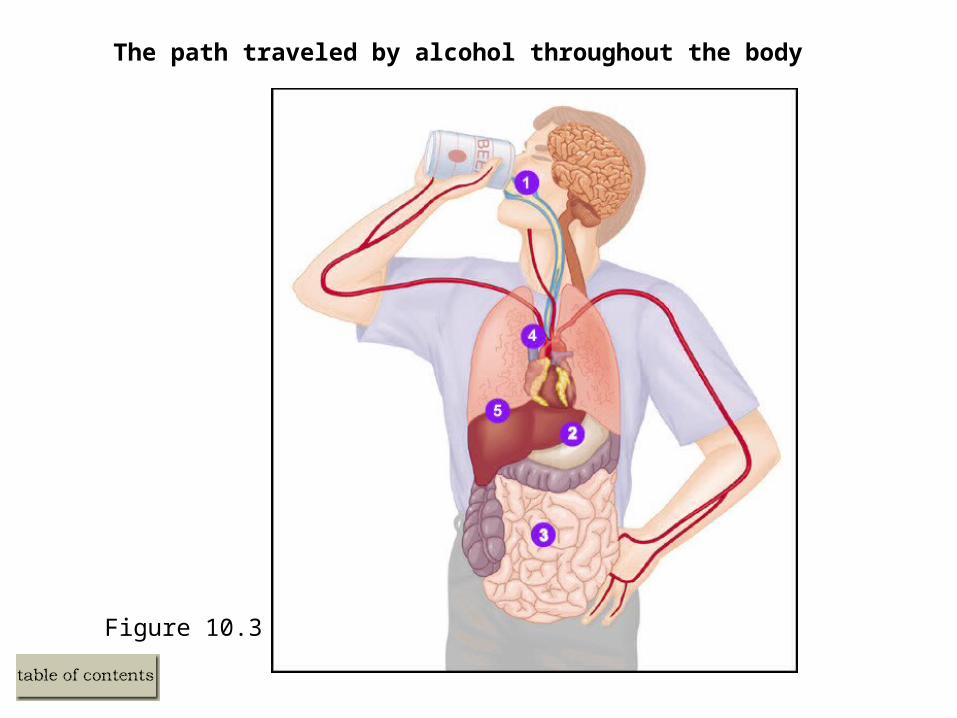
Figure 10.3
The path traveled by alcohol throughout the body
Alcohol: Some Facts and Statistics
• In the United States
– Most adults consider themselves light drinkers or abstainers
– Most alcohol is consumed by 11% of the U.S. population
– Alcohol use is highest among Caucasian Americans
– Males use and abuse alcohol more so than females
– Violence is associated with alcohol, but alcohol alone does not cause aggression
• Statistics on Abuse and Dependence
– 10% of Americans experience problems with alcohol
– Most persons with alcoholism can moderate or cease drinking
– 20% of those with alcohol problems experience spontaneous recovery
Sedative, Hypnotic, or Anxiolytic Substance use Disorders: An Overview
• The Nature of Drugs in This Class
– Sedatives – Calming
– Hypnotic – Sleep inducing (e.g., barbiturates)
– Anxiolytic – Anxiety reducing (e.g., benzodiazepines)
• Effects of Such Drugs Are Similar to Large Doses of Alcohol
– Combining such drugs with alcohol is synergistic
• All Exert Their Influence Via the GABA Neurotransmitter System
• DSM-IV Criteria for Sedative, Hypnotic, or Anxiolytic Substance Use Disorders
Stimulants: An Overview
• Nature of Stimulants
– Most widely consumed drug in the United States
– Such drugs increase alertness and increase energy
– Examples include amphetamines, cocaine, nicotine, and caffeine
Stimulants: Amphetamine Use Disorders
• Effects of Amphetamines
– Produce elation, vigor, reduce fatigue
– Such effects are followed by a “crash” (e.g., feeling depressed and tired)
– Enhance the release of dopamine and norepinephrine, while blocking reuptake
• DSM-IV Criteria for Amphetamine Intoxication
– Psychological symptoms
– Physiological symptoms
• Ecstasy and Ice
– Produces effects similar to speed, but without the crash
– 2% of college students report using Ecstasy
– Both drugs can result in dependence
Stimulants: Cocaine Use Disorders
• DSM-IV Criteria for Cocaine Intoxication and Withdrawal
– Psychological symptoms
– Physiological symptoms
– Most cocaine users cycle through patterns of tolerance and withdrawal
• Effects of Cocaine
– Produce short lived sensations of elation, vigor, reduce fatigue
– Cocaine use in the United States has declined over the last decade
– Effects result from blocking the reuptake of dopamine
– Cocaine is highly addictive, but addiction develops slowly
Stimulants: Nicotine Use Disorders
• Effects of Nicotine
– Stimulates the central nervous system, specifically nicotinic acetylcholine receptors
– Results in sensations of relaxation, wellness, pleasure
– Nicotine is highly addictive
• DSM-IV Criteria for Nicotine Withdrawal Only
– Psychological symptoms
– Physiological symptoms
– Nicotine users dose themselves to maintain a steady state of nicotine
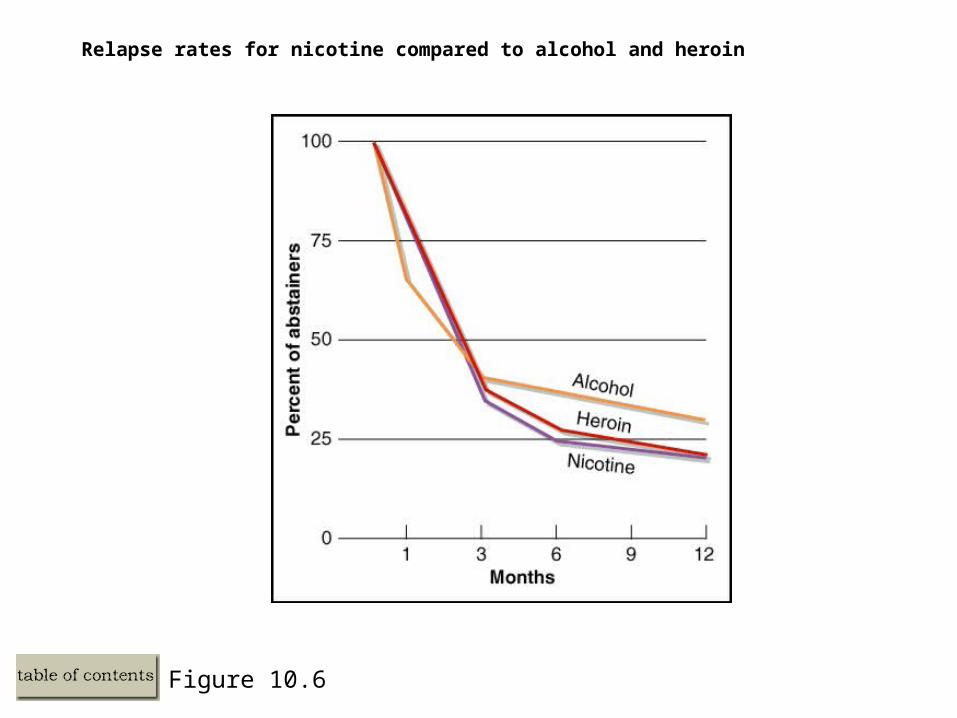
Figure 10.6
Relapse rates for nicotine compared to alcohol and heroin
Stimulants: Caffeine Use Disorders
• Effects of Caffeine – The “Gentle” Stimulant
– Used by over 90% of Americans
– Found in tea, coffee, cola drinks, and cocoa products
– Small doses elevate mood and reduce fatigue
– Regular use can result in tolerance and dependence
– Caffeine blocks the reuptake of the neurotransmitter adenosine
• DSM-IV Criteria for Caffeine Intoxication
– Psychological symptoms
– Physiological symptoms
Opiods: An Overview
• The Nature of Opiates and Opiods
– Opiate – Natural chemical in the opium poppy with narcotic effects (i.e., pain relief)
– Opiods – Refers to a class of natural and synthetic substances with narcotic effects
– Such drugs are often referred to as analgesics
– Examples include heroin, opium, codeine, and morphine
• Effects of Opiods
– Low doses induce euphoria, drowsiness, and slowed breathing
– High doses can result in death
– Withdrawal symptoms can be lasting and severe
– Activate body’s enkephalins and endorphins
• DSM-IV Criteria for Opiod Intoxication and Withdrawal
– Psychological symptoms
– Physiological symptoms
– Mortality rates are high for opiod addicts
Hallucinogens: An Overview
• Nature of Hallucinogens
– Substances that change the way the user perceives the world
– May produce delusions, paranoia, hallucinations, and altered sensory perception
– Examples include marijuana, LSD
• Marijuana
– Active chemical is tetrahydrocannabinol (THC)
– May produce several systems (e.g., mood swings, paranoia, hallucinations)
– Impairment in motivation is not uncommon (i.e., amotivational syndrome)
– Major signs of withdrawal and dependence do not typically occur
Hallucinogens: An Overview (cont.)
• LSD and Other Hallucinogens
– LSD is most common form of hallucinogenic drug
– Tolerance tends to be rapid, and withdrawal symptoms are uncommon
– Psychotic delusional and hallucinatory symptoms can be problematic
• DSM-IV Criteria for Marijuana and Hallucinogen Intoxication
– Psychological and physiological symptoms are similar
Other Drugs of Abuse: Inhalants
• Nature of Inhalants
– Substances found in volatile solvents that are breathed into the lungs directly
– Examples include spray paint, hair spray, paint thinner, gasoline, nitrous oxide
– Such drugs are rapidly absorbed with effects similar to alcohol intoxication
– Tolerance and prolonged symptoms of withdrawal are common
– DSM-IV criteria for inhalant intoxication
Other Drugs of Abuse: Anabolic Steroids
• Nature of Anabolic-Androgenic Steroids
– Steroids are derived or synthesized from testosterone
– Used medicinally or to increase body mass
– Users may engage in cycling or stacking
– Steroids do not produce a high
– Steroids can result in long-term mood disturbances and physical problems
Other Drugs of Abuse: Designer Drugs
• Designer Drugs
– Drugs produced by pharmaceutical companies for diseases
– Ecstasy, MDEA (“eve”), BDMPEA (“nexus”), ketamine (“special K”) are examples
– Such drugs heighten auditory and visual perception, sense of taste/touch
– Becoming popular in nightclubs, raves, or large social gatherings
– All designer drugs can produce tolerance and dependence
Causes of Substance-Related Disorders: Family and Genetic Influences
• Results of Family, Twin, and Adoption Studies
– Substance abuse has a genetic component
– Much of the focus has been on alcoholism
– Genetic differences in alcohol metabolism
– Multiple genes are involved in substance abuse
Causes of Substance-Related Disorders: Neurobiological Influences
• Results of Neurobiological Research
– Drugs affect the pleasure or reward centers in the brain
– The pleasure center – Dopamine, midbrain, frontal cortex
– GABA turns off reward-pleasure system
– Neurotransmitters responsible for anxiety/negative affect may be inhibited
Causes of Substance-Related Disorders: Psychological Dimensions
• Role of Positive and Negative Reinforcement
– Most see substance abuse as a means to cope with negative affect
– The self-medication and the tension reduction hypotheses
• Opponent-Process Theory
– Explains why the crash after drug use fails to keep people from using
• Role of Expectancy Effects
– Expectancies influence drug use and relapse
Causes of Substance-Related Disorders: Social and Cultural Dimensions
• Exposure to Drugs in a Prerequisite for Use of Drugs
– Media, family, peers
– Parents and the family appear critical
• Societal Views About Drug Abuse
– Sign of moral weakness – Drug abuse is a failure of self-control
– Sign of a disease – Drug abuse is caused by some underlying process
• The Role of Cultural Factors
– Influence the manifestation of substance abuse
An Integrative Model of Substance-Related Disorders
• Exposure or Access to a Drug Is a Necessary, but not Sufficient
• Drug Use Depends on Social and Cultural Expectations
• Drugs Are Used Because of Their Pleasurable Effects
• Drugs Are Abused for Reasons That Are More Complex
– The premise of equifinality
– Stress may interact with psychological, genetic, social, and learning factors
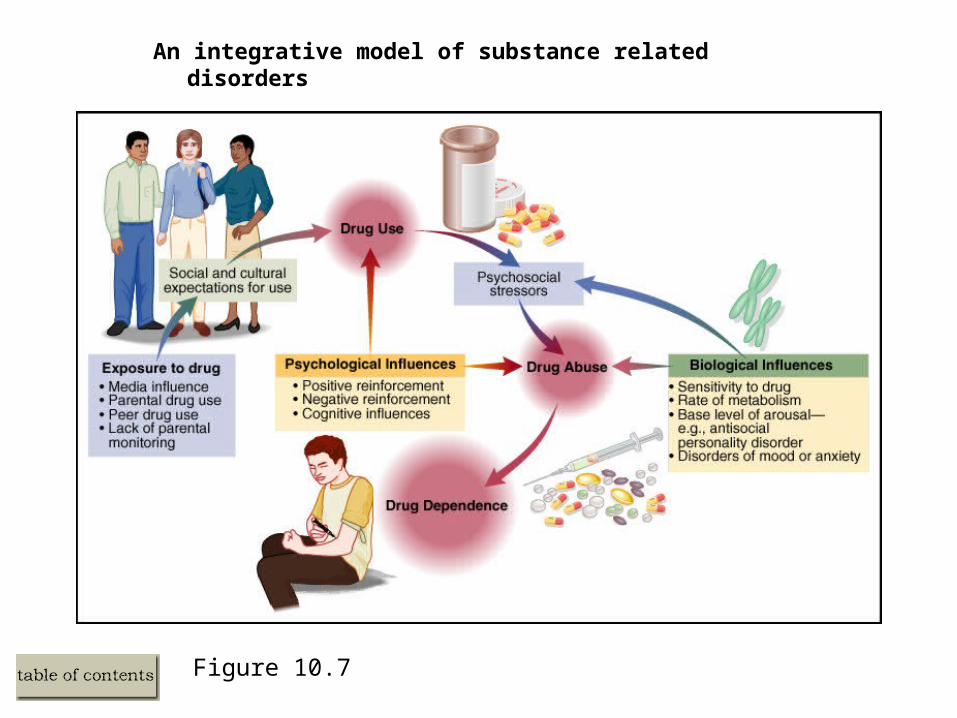
Figure 10.7
An integrative model of substance related disorders
Biological Treatment of Substance-Related Disorders
• Agonist Substitution
– Safe drug with a similar chemical composition as the abused drug
– Examples include methadone for heroin addiction, and nicotine gum or patch
• Antagonistic Treatment
– Drugs that block or counteract the positive effects of substances
– Examples include naltrexone for opiate and alcohol problems
• Aversive Treatment
– Drugs that make the injection of abused substances extremely unpleasant
– Examples include antabuse for alcoholism and silver nitrate for nicotine addiction
• Efficacy of Biological Treatment
– Such treatments are not generally not effective when used alone
Psychosocial Treatment of Substance-Related Disorders
• Inpatient vs. Outpatient Care
– Data suggest little difference in terms of overall effectiveness
• Community Support Programs
– Alcoholics Anonymous and related groups
– Seem helpful and are strongly encouraged
• Debate Over Controlled Use vs. Complete Abstinence as Treatment Goals
Psychosocial Treatment of Substance-Related Disorders
• Components of Comprehensive Treatment and Prevention Programs
– Individual and group therapy
– Aversion therapy and convert sensitization
– Contingency management
– Community reinforcement
– Relapse prevention
– Preventative efforts via education
Summary of Substance-Related Disorders
• DSM-IV and DSM-IV TR Substance Related Disorders Cover Four Classes
– Depressants, stimulants, opiates, and hallucinogens
– Specific diagnoses include dependence, abuse, intoxication, or withdrawal
• Most Psychotropic Drugs Activate the Dopaminergic Pleasure Pathway in the Brain
• Psychosocial Factors Interact with Biological Influences to Produce Substance Disorders
• Treatment of Substance Dependence Is Largely Unsuccessful
– Highly motivated persons do best when part of combined treatment programs
• Substance-Related Disorders Are 100% Preventable
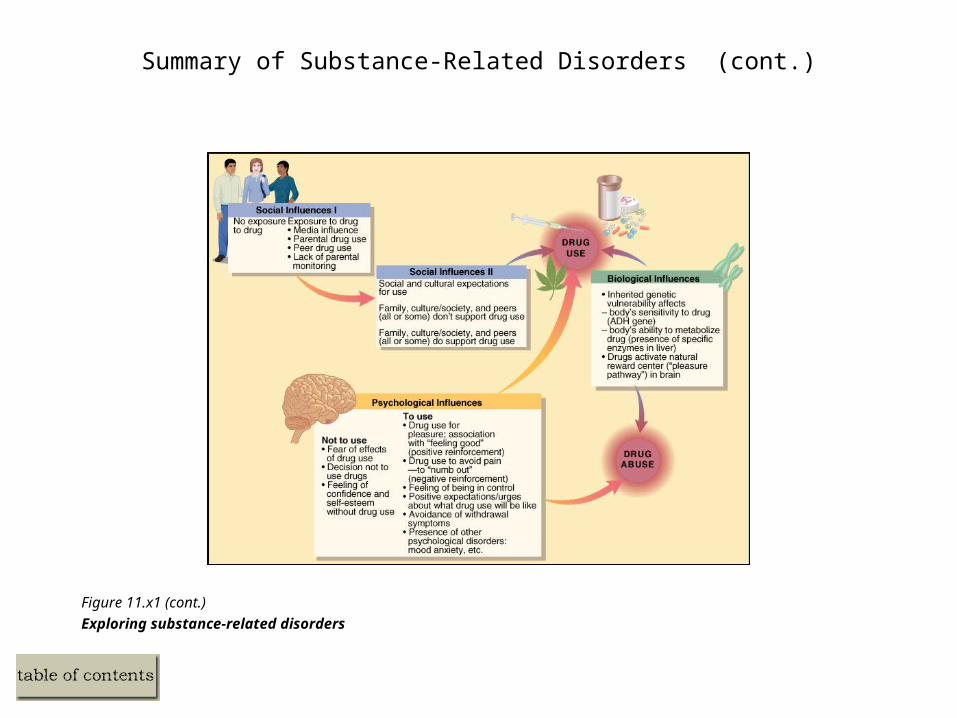
Summary of Substance-Related Disorders (cont.)
Figure 11.x1 (cont.)
Exploring substance-related disorders
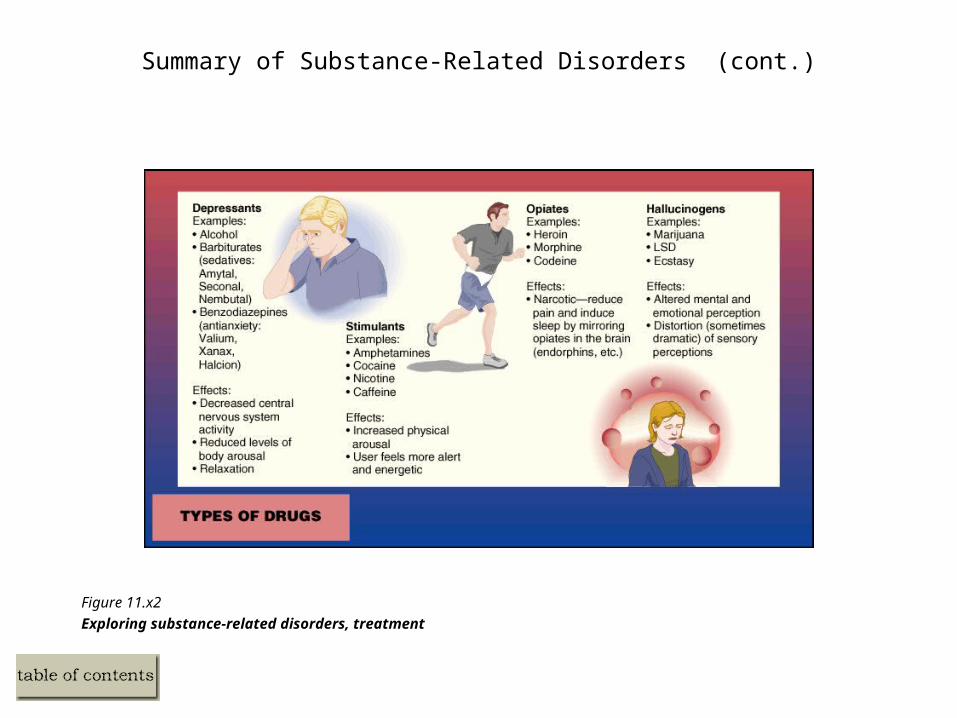
Summary of Substance-Related Disorders (cont.)
Figure 11.x2
Exploring substance-related disorders, treatment
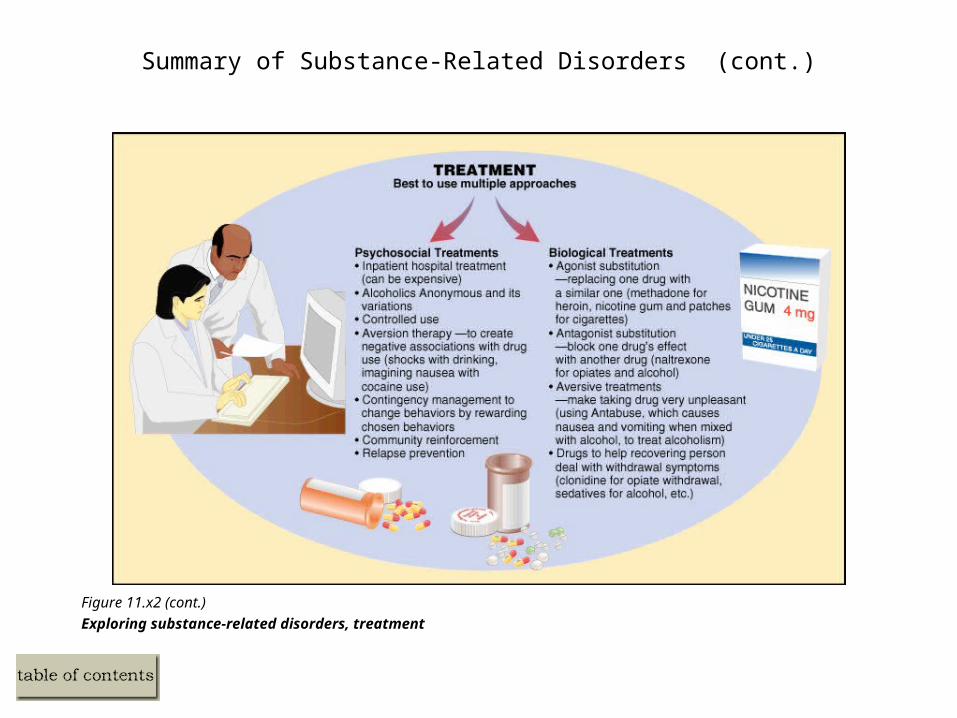
Summary of Substance-Related Disorders (cont.)
Figure 11.x2 (cont.)
Exploring substance-related disorders, treatment
Web sites
• National Clearinghouse for Alcohol and Drug Information
– www.health.org
• National Institute on Drug Abuse
– www.nida.nih.gov
• Inhalants
– www.inhalants.org
• Substance Abuse and Mental Health Services Administration
– www.samhsa.gov

Impulse-Control Disorders
• DSM-IV-TR
– Intermittent explosive disorder
– Kleptomania
– Pyromania
– Pathological gambling
– Trichotillomania
Impulse-Control Disorders (continued)
• Each is Characterized by
– Increased tension/anxiety prior to the act
– A sense of relief following the act
– Impairment of social and occupational functioning
Impulse-control Disorders: Intermittent Explosive Disorder
• Intermittent Explosive Disorder
– Rare condition
– Characterized by frequent aggressive outbursts
– Leads to injury and/or destruction of property
– Few controlled treatment studies
Impulse-control Disorders: Kleptomania
• Kleptomania
– Failure to resist urge to steal unnecessary items
– Seems rare, but it is not well studied
– Highly comorbid with mood disorders
– Also co-occurs with substance-related problems
Impulse-control Disorders: Pyromania, Pathological Gambling
• Pyromania
– Involves having an irresistible urge to set fires
– Diagnosed in less than 4% of arsonists
– Little etiological and treatment research
• Pathological Gambling
– Affect 3-5% adult Americans
– Treatment is similar to that for substance dependence
Trichotillomania (continued)
• Trichotillomania
– Inability to resist the urge to pull hair
– Observed in 1-5% of college students, mostly female
– Clomipramine (Anafranil) and CBT have been shown to be helpful