Subnormal parasympathetic activity after cardiac transplantation
4
Subnormal Parasympathetic Activity After Cardiac Transplantation Michael L. Smith, POD, Kenneth A. Ellenbogen, MD, Dwain I-. Eckberg, MD, Helen M. Sheehan, BSN, and Marc D. Thames, MD Heart period variability (standard deviation of 120 - consecutive RR or PP intervals) was used to assess baseline parasympathetic activtty in 18 pattents wlth congestive heart failure before and after or- thotoplc cardiac transplantatton, and was com- pared to that of 16 age-matched control subjects. Mean heart period variabtltty (f standard error of the mean) was significantly greater (p <O.OS) in control subjects (58 f 5 ms) than in the patients at any time before or after transplantation. Heart pe- rlod variabillty of innervated recipient atria did not change significantly early (1 to 4 weeks) after transplantation (16 f 2 to 24 f 5 ms; p = O.ll), but increased significantly between weeks 15 and 37 after transplantation (30 & 5 ms, p <0.002 ver- sus before transplantation). A stepwise regression model (R* = 0.35; p = 0.01) showed that heart pe- riod variability was directly related to time after transplantation and inversely related to systolic ar- terial pressure after transplantation and degree of rejection. Heart period variability of the denervated donor atria did not change from early to late peri- ods after transplantation, suggesting that vagal re- innervation of the donor heart had not occurred. These data indicate that baseline parasympathetic activity does not increase significantly during the first month after transplantation but increases sig- nificantly between months 3 and 6. (AmJ Cardiol 1990;66:1243-1246) From the Departments of Medicine and Physiology, McGuire Veterans Administration Medical Center and Medical College of Virginia, Rich- mond, Virginia. ‘Ihis study was supported in part by National Institutes of Health Grants HL-30506, IX-22296 and HL-07556, Bethesda, Maryland, and by funds from the Veterans Administration, Washing- ton, DC!. Manuscript received April 11, 1990; revised manuscript re- ceived June 25.1990, and accepted June 26. Address for reprints: Kenneth A. Ellenbogen, MD, Department of Cardiology, 111J, McGuire Veterans Administration Medicai Center, 1201 Broad Rock Boulevard, Richmond, Virginia 23249. aselineparasympathetic activity and arterial baro- reflex gain are attenuated in humans and experi- ental animals with congestive heart failure.‘-” Ellenbogen et al5 showed that arterial baroreflex gain was normal in normotensive cardiac transplant patients. More recently, we found that baseline parasympathet- ic activity (heart period variability) was significantly greater in cardiac transplant patients than in heart fail- ure patients, but remained subnormal.6 These previous data were derived from cross-sectional studies of differ- ent groups of patients. To date, a longitudinal study on the same patient cohort has not been used to assess di- rectly the effect of cardiac transplantation on autonom- ic function. This study usesa longitudinal design to (1) determine if cardiac transplantation accounts for the improvement of baseline parasympathetic activity to the innervated recipient atria (suggested by the previous cross-sectionalstudy); and (2) determine how changes in baseline parasympathetic activity after transplanta- tion relate to changes in clinical parameters. METHODS Subjects: Eighteen men with congestive heart failure (aged 24 to 62 years, mean f standard error of the mean 46 f 2) who underwent orthotopic cardiac trans- plantation were prospectively studied before and after this surgical procedure, Orthotopic cardiac transplanta- tion was performed with techniques describedprevious- l~.~ Each subject gave written informed consent. The study was approved by the Medical College of Virginia and Veterans Administration Hospital Committees on the Conduct of Human Research. Sixteen healthy age- matched subjects free of organic heart disease were studied as control subjects. Me~~urem~~t$: Measurements were obtained at the same time of day to avoid circadian variation. Patients with dyspneaor frequent (>4 beats/min) ventricular or atria1 premature beats were excluded from the study. A standard limb lead rhythm strip was obtained in control subjectsand patients before transplantation. An esopha- geal lead or intracavitary quadripolar catheter was used to record donor and recipient atria1 activity in patients after transplantation. After 20 minutes of supine rest, an electrocardiographic rhythm strip was obtained for determination of mean PP interval and heart period variability. Rhythm strips were obtained from a strip- chart recorder at a paper speedof 100 mm/s (accuracy f 5 ms). Breathing rate was measuredin 8 patients and was not significantly different between each measure- ment period. SHE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER 15, 1990
-
Upload
michael-l-smith -
Category
Documents
-
view
212 -
download
0
Transcript of Subnormal parasympathetic activity after cardiac transplantation

Subnormal Parasympathetic Activity After Cardiac Transplantation
Michael L. Smith, POD, Kenneth A. Ellenbogen, MD, Dwain I-. Eckberg, MD, Helen M. Sheehan, BSN, and Marc D. Thames, MD
Heart period variability (standard deviation of 120 - consecutive RR or PP intervals) was used to assess baseline parasympathetic activtty in 18 pattents wlth congestive heart failure before and after or- thotoplc cardiac transplantatton, and was com- pared to that of 16 age-matched control subjects. Mean heart period variabtltty (f standard error of the mean) was significantly greater (p <O.OS) in control subjects (58 f 5 ms) than in the patients at any time before or after transplantation. Heart pe- rlod variabillty of innervated recipient atria did not change significantly early (1 to 4 weeks) after transplantation (16 f 2 to 24 f 5 ms; p = O.ll), but increased significantly between weeks 15 and 37 after transplantation (30 & 5 ms, p <0.002 ver- sus before transplantation). A stepwise regression model (R* = 0.35; p = 0.01) showed that heart pe- riod variability was directly related to time after transplantation and inversely related to systolic ar- terial pressure after transplantation and degree of rejection. Heart period variability of the denervated donor atria did not change from early to late peri- ods after transplantation, suggesting that vagal re- innervation of the donor heart had not occurred. These data indicate that baseline parasympathetic activity does not increase significantly during the first month after transplantation but increases sig- nificantly between months 3 and 6.
(AmJ Cardiol 1990;66:1243-1246)
From the Departments of Medicine and Physiology, McGuire Veterans Administration Medical Center and Medical College of Virginia, Rich- mond, Virginia. ‘Ihis study was supported in part by National Institutes of Health Grants HL-30506, IX-22296 and HL-07556, Bethesda, Maryland, and by funds from the Veterans Administration, Washing- ton, DC!. Manuscript received April 11, 1990; revised manuscript re- ceived June 25.1990, and accepted June 26.
Address for reprints: Kenneth A. Ellenbogen, MD, Department of Cardiology, 111 J, McGuire Veterans Administration Medicai Center, 1201 Broad Rock Boulevard, Richmond, Virginia 23249.
aseline parasympathetic activity and arterial baro- reflex gain are attenuated in humans and experi-
ental animals with congestive heart failure.‘-” Ellenbogen et al5 showed that arterial baroreflex gain was normal in normotensive cardiac transplant patients. More recently, we found that baseline parasympathet- ic activity (heart period variability) was significantly greater in cardiac transplant patients than in heart fail- ure patients, but remained subnormal.6 These previous data were derived from cross-sectional studies of differ- ent groups of patients. To date, a longitudinal study on the same patient cohort has not been used to assess di- rectly the effect of cardiac transplantation on autonom- ic function. This study uses a longitudinal design to (1) determine if cardiac transplantation accounts for the improvement of baseline parasympathetic activity to the innervated recipient atria (suggested by the previous cross-sectional study); and (2) determine how changes in baseline parasympathetic activity after transplanta- tion relate to changes in clinical parameters.
METHODS Subjects: Eighteen men with congestive heart failure
(aged 24 to 62 years, mean f standard error of the mean 46 f 2) who underwent orthotopic cardiac trans- plantation were prospectively studied before and after this surgical procedure, Orthotopic cardiac transplanta- tion was performed with techniques described previous- l~.~ Each subject gave written informed consent. The study was approved by the Medical College of Virginia and Veterans Administration Hospital Committees on the Conduct of Human Research. Sixteen healthy age- matched subjects free of organic heart disease were studied as control subjects.
Me~~urem~~t$: Measurements were obtained at the same time of day to avoid circadian variation. Patients with dyspnea or frequent (>4 beats/min) ventricular or atria1 premature beats were excluded from the study. A standard limb lead rhythm strip was obtained in control subjects and patients before transplantation. An esopha- geal lead or intracavitary quadripolar catheter was used to record donor and recipient atria1 activity in patients after transplantation. After 20 minutes of supine rest, an electrocardiographic rhythm strip was obtained for determination of mean PP interval and heart period variability. Rhythm strips were obtained from a strip- chart recorder at a paper speed of 100 mm/s (accuracy f 5 ms). Breathing rate was measured in 8 patients and was not significantly different between each measure- ment period.
SHE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER 15, 1990

TABLE I Summary of Physiologic Data
PP Heart Interval Period Systolic at Rest Variability Pressure
Group (ms) 0-W (mm W
Control (n = 16) 984 f 39 58*5 129f3 Transplants (n = 18)
Pretransplant, 760 f 31 16+2 117*3 Recipient
Posttransplant, 782 f 36 24f5” 132&4* Recipient (early)
Posttransplant. 811 f45 30f5” 145f4” Recipient (late)
Posttransplant, 707 f 34 6fl -
donor (early) Posttransplant, 721 f 28 7fl -
donor (late)
All values are mean f standard error of the mean. * Significantly different from values before transplantation (p <0.05). I Heart period variability was characterized as the
standard deviation of 120 consecutive sinus rhythm PP intervals of the innervated recipient artia with a cali- brated digitizing tablet (Sigma&an, Jandel Scientific). Measurement reliability was determined in 8 control subjects studied on 2 occasions, 7 days apart (paired t test). Heart period variability was unchanged in these subjects (day 0 = 41 f 7 ms, day 7 = 39 f 6 ms; p = 0.43).
Data analysis: Time of measurement was divided into 2 periods after transplantation: “Early” represent- ing the first 4 weeks, and “Late” representing a period ranging from 15 to 37 weeks after transplantation. The data were normally distributed, and parametric analy- ses were performed. Pretransplantation and early or late posttransplantation were compared by analysis of vari- ance with repeated-measures design and contrasts to discern differences between time periods. A probability <0.05 was considered significant. A stepwise regression analysiq7 with a model entry significance level of 0.25 was used to develop a model of pre- and posttransplan- tation clinical characteristics for the prediction of the
dependent heart period variability change from before to after transplantation. The independent variables test- ed for the model were time after transplantation, dura- tion of class III/IV heart failure, ejection fraction be- fore transplantation, degree of rejection at the time of study (on a 0 to 3 scale, where 0 = no rejection and 3 = severe rejection), systolic or diastolic arterial pressures after transplantation, and age. The model R2 value rep resents the percent variation of the data explained by the model. The model R2 was used to describe the sta- tistical findings because it provides more succinct infor- mation about the model than the partial correlation co- efficients.
RESULTS All transplant patients received both cyclosporine
and azathioprine as immunosuppressive therapy. The average duration of class III/IV heart failure and mean ejection fraction before transplantation was 6.6 f 0.8 months (range 3 to 12) and 17.1 f 1.9% (range 8 to 30), respectively.
Table I summarizes physiologic data for control sub- jects and for transplant patients for each measurement period in the transplant patients. Baseline PP interval (984 f 39 ms) and heart period variability (58 f 5 ms) was significantly greater in control subjects than in transplant patients at any period. Neither recipient PP intervals nor donor P’P’ intervals of transplant patients changed (p >0.05) after transplantation. Arterial pres- sure increased significantly during the first month after transplantation (p = 0.01) and increased further during the late measurement period (p = 0.04).
Mean heart period variability of the control group was significantly greater than that of all other groups. Heart period variability of the innervated recipient atria of the transplant patients (Table I) did not increase significantly by the early posttransplantation study (p = 0.1 l), but did increase significantly by the late study (p = 0.02 compared to early posttransplantation; p = 0.002 compared to before transplantation). Three pa- tients showed dramatic increases in heart period vari-
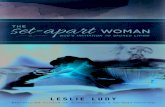
loo- pre , early, late
E
B-L 75- ;tl E n .z
z 50- x ‘C iti tf 25- x I:
0 20 4c
Dost-transplant time, weeks
I
FIGURE 1. Individual heart period vari- ability data for each patient before (pre), during the first 4 weeks (early) and during weeks 15 to 37 (late).
1244 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 66

ability. The analyses were repeated excluding these pa- tients to determine if differences before and after trans- plantation were attributable to these patients alone. Heart period variability increased from 15 f 2 to 17 f 4 ms between pre- and early posttransplantation (p = 0.17), and to 24 f 3 ms at late posttransplantation (p = 0.003) in the 15 patients. Heart period variability of the denervated donor atria was unchanged from early to late posttransplantation (p = 0.79).
Heart period variability of recipient atria was widely distributed after transplantation. Individual data before and after transplantation are illustrated in Figure 1. Stepwise regression analyses were performed to deter- mine clinical and physiologic correlates of heart period variability changes associated with cardiac transplanta- tion. A significant model was obtained in which time after transplantation was directly related, and systolic arterial pressure and degree of rejection were inversely related to the change in heart period variability. The model, although significant, was a poor predictor of heart period variability (R2 = 0.35, p = 0.01).
DISCUSSION Previously, we reported on cross-sectional compari-
sons in which baroreflex gain is normal and heart period variability is near normal in cardiac transplant pa- tients.jJj The present study is the first longitudinal study of the effect of cardiac transplantation on baseline para- sympathetic activity. Our data show that heart period variability of innervated recipient atria of transplant pa- tients, used as an index of baseline parasympathetic ac- tivity, can increase after cardiac transplantation, but usually remains subnormal. The degree of restoration of heart period variability is inversely related, in part, to arterial pressure after transplantation and the degree of rejection. These data suggest that baseline parasympa- thetic activity improves, but usually does not return to normal after cardiac transplantation.
We used heart period variability during quiet breathing to assess baseline cardiac parasympathetic ac- tivity in humans. This measure is considered a reason- able estimate of parasympathetic activity when respira- tion is regular and physiologic conditions are stable.8
eline levels and changes of heart period variability related directly to cardiac parasympathetic efferent
nerve activity in dogs.9 The heart period variability measure used in the present study, standard deviation of BP interval, correlates with other measures of cardiac parasympathetic activity; therefore, this measure is a simple, yet powerful estimate of baseline parasympa- thetic activity.8
Parasympathetic activity in eart failure before ransplantation: Reduced baseline parasympathetic ac-
tivity and arterial baroreflex gain,1-3 elevated baseline parasympathetic activity and elevated plasma norepi- nephrine concentrationlO~ll are hallmarks of congestive heart failure. Furthermore, cardiac parasympathetic ac- tivity is related inversely to the severity of heart failure and prognosis of heart disease.r,‘2313 Our patients had profoundly subnormal heart period variability associ- ated with heart failure before transplantation, suggest-
ing a severe abnormality of baseline parasympathetic activity (Figure 1). These findings support previous re- ports of reduced parasympathetic activity in congestive heart failure.1,2
Parasympathetic activity after transplantation: Heart period variability of the innervated recipient atria did not increase significantly during the first month af- ter transplantation, but increased significantly between weeks 15 and 37 (late posttransplant period). However, only 4 of the 18 patients showed increases >lO ms; thus, these data suggest that heart period variability does not necessarily improve after transplantation. In our previous cross-sectional study,6 a diverse patient population was studied with posttransplant time ranging from 2 weeks to 5 years. Those data suggested that heart period variability increased substantially after transplantation and continued to increase progressively over time. However, few patients were studied in the first 6 weeks after transplantation. The present data support the previous study in showing that an increase in heart period variability usually occurs with time after transplantation. However, these data also show that the improvement is delayed and is not usually very dra- matic.
Ellenbogen et al5 reported that arterial baroreflex gain is normal in transplant patients. Their findings imply normal parasympathetic responsiveness in the presence of impaired baseline parasympathetic activity. Therefore, we hypothesize that the subnormal baseline activity is not due to an impairment along the efferent vagal pathway; rather, it is best explained by a change in the total afferent input to the cardiac vagal motor nuclei in the brain.
A stepwise regression model indicated that changes in heart period variability after transplantation correlate directly with time after transplant, and inversely with systolic arterial pressure and degree of rejection. This analysis supports the hypothesis that heart period vari- ability tends to increase with time after transplantation. Furthermore, these data support our previous conclu- sion6 that hypertension after transplantation adversely affects baseline parasympathetic activity. However, the predictive power of the model (R2 = 0.35) was poor, indicating that other factors confound the measurement of heart period variability after cardiac transplantation. Other factors probably contributed to the variation of responses: (1) Patients were receiving a variety of medi- cations that could affect parasympathetic activity; and (2) the rates of patient recovery from cardiac transplan- tation are highly individual and difficult to assess.
Heart period variability in denervated donor atria: The denervated donor hearts of the transplant patients demonstrated minimal heart period variability, consis- tent with previous reports of little or no respiratory sinus arrhythmia in such patients.t4,15 This lack of heart peri- od variability suggests that parasympathetic reinnerva- tion of the heart does not occur during the first 6 months after transplantation. Reinnervation occurs as early as 2 months16 and autonomic innervation appears to be functionally effective within 9 monthsr7 in auto- transplanted dogs. However, in human transplant pa-
THE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER 15. 1990

tients, evidence from heart period variability6 and heart rate responses to exercise14 suggest that no reinnerva- tion occurs during the first 2 years after transplantation. Fallen et all* recently showed that the power spectrum of heart rate variability of 1 transplant patient was normal, including both low frequency and respiratory peaks, at 33 months after transplantation. This finding is indicative of normal parasympathetic innervation of the heart. This is the only isolated finding of possible reinnervation in humans of which we are aware.
REFERENCES 1. Eckberg DL, Drabinsky M, Braunwald E. Defective cardiac para%ympathetic control in patients with heart disease. N Engl J Med 1971;285:877-883. 2. Saul JP, Arai Y, Berger RD, Lilly LS, Colucci WS, Cohen RJ. Assessment of autonomic regulation in chronic contestive heart failure by heart rate spectral analysis. Am J Cardiol 1988;61:1292-1299. 3. Olivari MT, Levine TB, Cohn JN. Abnormal neurohumoral response to nitro- prusside infusion in congestive heart failure. JAm CON Cardiol 1983;2:41 I-417. 4. White CW. Reversibility of abnormal arterial baroreflex control of heart rate in heart failure. Am J Physiol 1981;241:H778-H782. 5. Ellenbogen KA, Mohanty PK, Szentpetery S, Thomas MD. Baroreflex abnor- malities in heart failure: reversal after orthotopic cardiac transplantation. Circu- lation 1989;79:51-58. 6. Smith ML, Ellenbogen KA, Eckberg DL, Szentpetery S, Thames MD. Sub- normal heart period variability in heart failure: Effect of cardiac transplantation. J Am Coil Cardiol 1989;14:106-111.
7. Draper NR, Smith H. Applied Regression Analysis. New York: John Wiley & Sons, 198 1:294-352. 8. Eckberg DL. Respiratory sinus arrhythmia: a window on central autonomic regulation in man. In: Hunyor S, Ludbrcok J, Shaw J, McGrath M, eds. The Peripheral Circulation. Amsterdam: Elsevier, 1984~267-274. 9. Katona PG, P&as JW, Barnett GO, Terry BS. Cardiacvagal efferent activity and heart period in the carotid sinus reflex. Am J Physiol 1970;218:1030-1037. 10. Leimbach WN Jr, Wallin BG, Victor RG, Aylward PE, Sundlof G, Mark AL. Direct evidence from intraneural recordings for increased central sympathet- ic outflow in patients with heart failure. Circulation 1986;73:913-919. 11. Cohn JN, Levine TB, Olivari MT, Garberg V, Lura D, Francis GS, Simon AB, Rector T. Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med 1984;3 11:8 19-823. 12. Wolf MM, Varigos GA, Hunt D, Sloman JG. Sinus arrhythmia in acute myocardial infarction. Med J Austr 1978;2:52-53. 13. Hinkle LE, Carver ST, Plakun A. Slow heart rates and increased risk of cardiac death in middle-aged men. Arch Intern Med 1972;129:732-750. 14. Stinson EB, Griepp RB, Schroeder JS, Dong E Jr, Shumway NE. Hemody- namic observations one and two years after cardiac transplantation in man. Circulation 1972;45:1183-1194. 15. Beck W, Barnard CN, Schrire V. Heart rate after cardiac transplantation. Circulation 1969;40:437-445. LB. Mohanty PK, Thames MD, Capehart JR, Kawaguchi A, Ballon B, Lower RR. Afferent reinnervation of the autotransplanted heart in dogs. J Am CON Cardiol 1986;7:414-418. 17. Kaye MP, Randall WC, Hageman GR, Geis WP, Priola DV. Chronology and mode of reinnervation of the surgically denervated canine heart: functional and chemical correlates. Am J Physiol 1977;233:H43 I-H437. 18. Fallen EL, Kamath MV, Ghista DN, Fitchett D. Spectral analysis of heart rate variability following human heart transplantation: evidence for functional reinnervation. J Auton Nern Syst 1988;23:199-206. 19. Adair JR, Manning JW. Hypothalamic modulation of baroreceptor afferent unit activity. Am J Physiol 1975;229:1357-1364.
1246 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 66