
Stump appendicitis after laparoscopic appendectomy
2
267 Turkish Journal of Trauma & Emergency Surgery Case Report Olgu Sunumu Ulus Travma Acil Cerrahi Derg 2011;17 (3):267-268 Stump appendicitis after laparoscopic appendectomy: case report Laparoskopik apendektomiden sonra güdük apandisit: Olgu sunumu Omaima BU-ALI, 1 Mohamed AL-BASHIR, 1 Hashim A SAMIR, 2 Fikri M. ABU-ZIDAN 1 Güdük apandisiti, nadir bir geç apendektomi komplikasyo- nudur. Tanıda gecikme olması, genellikle daha önceden bir apendektomi öyküsü bulunması yüzündendir. Biz, laparos- kopik apendektomiden sonra bilgisayarlı tomografi (BT) ile ameliyat öncesi tanı konulan bir güdük apandisiti olgusu su- nuyoruz. On sekiz yaşında bir erkek, bir haftalık bir alt ka- rın ağrısı, bulantı ve kusma öyküsü ile başvurdu. Hastanın akut apandisit nedeniyle geçirilmiş bir laparoskopik apen- dektomi öyküsü vardı. Fiziksel incelemede alt karın bölge- sinde hassasiyet, defans ve ağrı belirlendi. BT ile, ileoçekal bileşkenin arkasına yerleşimli yaklaşık 2,5 cm uzunluğunda ve 0,78 cm çapında tübüler bir yapıya sahip serbest pelvik sıvı bulunduğu saptandı. Laparoskopik inceleme, bulguları doğruladı. Rezidüel bir apandiks güdüğü bulundu, yapşık- lıklardan ayrıldı ve rezeke edildi. Histopatoloji, multifokal hemorajik nekroz ile birlikte olan transmural nötrofilik in- filtrasyona sahip rezidüel bir apendiks bulunduğunu göster- di. Ameliyat sonrası sorun çıkmadı. Güdük apandisit tanısı zor olabilir. BT taraması, bu nadir durumun tanısına yönelik yararlı bir araç olduğunu kanıtlamıştır. Anahtar Sözcükler: Apandisit; BT tarama; laparoskopi; güdük. Stump appendicitis is a rare delayed complication of ap- pendectomy. The delay in diagnosis is usually because of a prior history of appendectomy. We report a case of stump appendicitis diagnosed pre-operatively with a computerized tomography (CT) scan after laparoscopic appendectomy. An 18-year-old male presented with a one-week history of lower abdominal pain, nausea and vomiting. He had a his- tory of laparoscopic appendectomy for acute appendicitis. Physical examination revealed tenderness and guarding in the lower abdomen. CT scan showed free pelvic fluid with a tubular structure of about 2.5 cm in length and 0.78 cm in diameter located posterior to the ileo-cecal junction. Lapa- roscopic exploration confirmed the findings. A residual ap- pendiceal stump was found and dissected from the adhesion and removed. Histopathology showed a residual appendix with transmural neutrophilic infiltration associated with mul- tifocal hemorrhagic necrosis. The postoperative period was uneventful. The diagnosis of stump appendicitis can be chal- lenging. CT scan has proven to be a useful tool for the diag- nosis of this rare condition. Key Words: Appendicitis; CT scan; laparoscopy; stump. Incomplete appendectomy may predispose to the development of stump appendicitis. Stump appendici- tis, the interval re-inflammation of the residual appen- diceal tissue, is a rare complication of appendectomy. The diagnosis of stump appendicitis in a patient post- appendectomy is challenging since it is rarely consid- ered prospectively. We report a case of stump appendicitis following laparoscopic appendectomy that was diagnosed pre-op- eratively with a computerized tomography (CT) scan. CASE REPORT An 18-year-old male presented with a one-week history of lower abdominal pain, nausea and vomit- ing followed by fever for one day. He had undergone laparoscopic appendectomy for acute appendicitis three months earlier with an uneventful postoperative course. Physical examination revealed tenderness and guarding in the lower abdomen. His white blood cell count was 9.8 x 10 9 /L. The CT scan showed free pelvic fluid with a tubu- Departments of 1 Surgery, 2 Clinical Imaging, Tawam Hospital in affiliation with Johns Hopkins Medicine, Al-Ain, United Arab Emirates. Tawam Hastanesi ve Johns Hopkins Tıp işbirliğiyle, 1 Cerrahi Kliniği, 2 Klinik Görüntüleme Bölümü, Al-Ain, Birleşik Arap Emirlikleri. Correspondence (İletişim): Fikri M. Abu-Zidan, M.D. PO Box 17666, Al-Ain, United Arab Emirates. Tel: +00971 50 8335390 e-mail (e-posta): [email protected] doi: 10.5505/tjtes.2011.47123
-
Upload
phanhuynhtiendat -
Category
Health & Medicine
-
view
812 -
download
1
Transcript of Stump appendicitis after laparoscopic appendectomy

267
Turkish Journal of Trauma & Emergency Surgery
Case Report Olgu Sunumu
Ulus Travma Acil Cerrahi Derg 2011;17 (3):267-268
Stump appendicitis after laparoscopic appendectomy:case report
Laparoskopik apendektomiden sonra güdük apandisit: Olgu sunumu
Omaima BU-ALI,1 Mohamed AL-BASHIR,1 Hashim A SAMIR,2 Fikri M. ABU-ZIDAN1
Güdük apandisiti, nadir bir geç apendektomi komplikasyo-nudur. Tanıda gecikme olması, genellikle daha önceden bir apendektomi öyküsü bulunması yüzündendir. Biz, laparos-kopik apendektomiden sonra bilgisayarlı tomografi (BT) ile ameliyat öncesi tanı konulan bir güdük apandisiti olgusu su-nuyoruz. On sekiz yaşında bir erkek, bir haftalık bir alt ka-rın ağrısı, bulantı ve kusma öyküsü ile başvurdu. Hastanın akut apandisit nedeniyle geçirilmiş bir laparoskopik apen-dektomi öyküsü vardı. Fiziksel incelemede alt karın bölge-sinde hassasiyet, defans ve ağrı belirlendi. BT ile, ileoçekal bileşkenin arkasına yerleşimli yaklaşık 2,5 cm uzunluğunda ve 0,78 cm çapında tübüler bir yapıya sahip serbest pelvik sıvı bulunduğu saptandı. Laparoskopik inceleme, bulguları doğruladı. Rezidüel bir apandiks güdüğü bulundu, yapşık-lıklardan ayrıldı ve rezeke edildi. Histopatoloji, multifokal hemorajik nekroz ile birlikte olan transmural nötrofilik in-filtrasyona sahip rezidüel bir apendiks bulunduğunu göster-di. Ameliyat sonrası sorun çıkmadı. Güdük apandisit tanısı zor olabilir. BT taraması, bu nadir durumun tanısına yönelik yararlı bir araç olduğunu kanıtlamıştır. Anahtar Sözcükler: Apandisit; BT tarama; laparoskopi; güdük.
Stump appendicitis is a rare delayed complication of ap-pendectomy. The delay in diagnosis is usually because of a prior history of appendectomy. We report a case of stump appendicitis diagnosed pre-operatively with a computerized tomography (CT) scan after laparoscopic appendectomy. An 18-year-old male presented with a one-week history of lower abdominal pain, nausea and vomiting. He had a his-tory of laparoscopic appendectomy for acute appendicitis. Physical examination revealed tenderness and guarding in the lower abdomen. CT scan showed free pelvic fluid with a tubular structure of about 2.5 cm in length and 0.78 cm in diameter located posterior to the ileo-cecal junction. Lapa-roscopic exploration confirmed the findings. A residual ap-pendiceal stump was found and dissected from the adhesion and removed. Histopathology showed a residual appendix with transmural neutrophilic infiltration associated with mul-tifocal hemorrhagic necrosis. The postoperative period was uneventful. The diagnosis of stump appendicitis can be chal-lenging. CT scan has proven to be a useful tool for the diag-nosis of this rare condition. Key Words: Appendicitis; CT scan; laparoscopy; stump.
Incomplete appendectomy may predispose to the development of stump appendicitis. Stump appendici-tis, the interval re-inflammation of the residual appen-diceal tissue, is a rare complication of appendectomy. The diagnosis of stump appendicitis in a patient post-appendectomy is challenging since it is rarely consid-ered prospectively.
We report a case of stump appendicitis following laparoscopic appendectomy that was diagnosed pre-op-eratively with a computerized tomography (CT) scan.
CASE REPORTAn 18-year-old male presented with a one-week
history of lower abdominal pain, nausea and vomit-ing followed by fever for one day. He had undergone laparoscopic appendectomy for acute appendicitis three months earlier with an uneventful postoperative course. Physical examination revealed tenderness and guarding in the lower abdomen. His white blood cell count was 9.8 x 109/L.
The CT scan showed free pelvic fluid with a tubu-
Departments of 1Surgery, 2Clinical Imaging, Tawam Hospital in affiliation with Johns Hopkins Medicine, Al-Ain, United Arab Emirates.
Tawam Hastanesi ve Johns Hopkins Tıp işbirliğiyle, 1Cerrahi Kliniği, 2Klinik Görüntüleme Bölümü, Al-Ain, Birleşik Arap Emirlikleri.
Correspondence (İletişim): Fikri M. Abu-Zidan, M.D. PO Box 17666, Al-Ain, United Arab Emirates.Tel: +00971 50 8335390 e-mail (e-posta): [email protected]
doi: 10.5505/tjtes.2011.47123

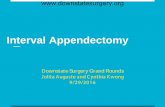
lar structure measuring 2.5 cm in length and 0.78 cm in diameter located posterior to the ileo-cecal junction (Fig. 1). Laparoscopic exploration revealed purulent fluid in the pelvis with multiple adhesions in the right iliac fossa. A residual appendiceal stump was found and dissected from the adhesion and removed. Histo-pathology showed a residual appendix with transmu-ral neutrophilic infiltration associated with multifocal hemorrhagic necrosis. The postoperative period was uneventful. The patient was followed for nine months without any complaints.
DISCUSSIONThe cause of stump appendicitis is incomplete re-
moval of the appendix during the initial surgery. The re-inflammation of the residual appendiceal tissue is reported to occur as early as two months and as late as 50 years after the initial surgery.[1]
The diagnosis of stump appendicitis in a patient with previous appendectomy presents a diagnostic di-lemma likely leading to delayed diagnosis and high perforation rate.[1] It requires a high index of suspicion to be determined early. Ultrasonography and CT scan may be helpful in establishing the diagnosis prospec-tively.[2] Interestingly, CT scan showed the presence of gas in the proximal part of the lumen of the appendix in our patient. About 15% of acute appendicitis cases will have gas in their lumen.[3] There are a variety of possible explanations: the obstruction may have been limited to the distal part; the diagnosis may have been reached before the gas was absorbed; the gas may have been produced by bacteria distal to the obstruc-tion; or the inflammation may have occurred without obstruction.[3]
The reports of stump appendicitis are rare and no relationship to a particular surgical technique can be made. It has been reported in patients following open appendectomy with stump ligation,[4] open ap-pendectomy with stump inversion[5] and laparoscopic appendectomy.[1,2] In laparoscopic appendectomy, the appendiceal stump is closed with an Endoloop or by stapling. In our case, the stump was closed with an Endoloop in the initial surgery and with staples in the second operation. There is no reported difference be-tween the two surgical techniques except for the lower risk of postoperative intra-abdominal surgical site infection and need for readmission to hospital when staples are used.[6]
Regardless of the surgical technique used, identifi-cation of the appendiceal base by tracing the taenia coli down to the appendix is crucial in preventing such a complication. Stump appendicitis should be considered in the differential diagnosis of any patient with a previ-ous history of appendectomy who presents with signs and symptoms of appendicitis. CT scan has proven to be a useful tool for the diagnosis of this rare condition.
REFERENCES1. Liang MK, Lo HG, Marks JL. Stump appendicitis: a compre-
hensive review of literature. Am Surg 2006;72:162-6.2. Shin LK, Halpern D, Weston SR, Meiner EM, Katz DS.
Prospective CT diagnosis of stump appendicitis. AJR Am J Roentgenol 2005;184:62-4.
3. Rettenbacher T, Hollerweger A, Macheiner P, Rettenbacher L, Frass R, Schneider B, et al. Presence or absence of gas in the appendix: additional criteria to rule out or confirm acute appendicitis--evaluation with US. Radiology 2000;214:183-7.
4. Thomas SE, Denning DA, Cummings MH. Delayed pathol-ogy of the appendiceal stump: a case report of stump appen-dicitis and review. Am Surg 1994;60:842-4.
5. Mangi AA, Berger DL. Stump appendicitis. Am Surg 2000;66:739-41.
6. Beldi G, Vorburger SA, Bruegger LE, Kocher T, Inderbitzin D, Candinas D. Analysis of stapling versus endoloops in ap-pendiceal stump closure. Br J Surg 2006;93:1390-3.
268 Mayıs - May 2011
Ulus Travma Acil Cerrahi Derg
Fig. 1. Axial CT (A) shows the thickened and enhanced ap-pendix stump (arrow) with peripheral mesenteric fat stranding. Curved multi-planar reconstruction (B) along the long axis of the appendix stump (arrow), measuring 2.5 cm in length, shows enhanced and in-flamed distal segment. A small fluid collection is seen nearby. Note the presence of gas in the proximal part of the lumen of the appendix.




![The current management of acute uncomplicated appendicitishub.hku.hk/bitstream/10722/251485/1/content.pdf · of acute uncomplicated appendicitis with promising re-sults [6–8]. Appendectomy,](https://static.fdocuments.us/doc/165x107/5c9dec6588c993d8368bb27a/the-current-management-of-acute-uncomplicated-of-acute-uncomplicated-appendicitis.jpg)



![Case Report Stump Appendicitis: An Uncompleted Surgery, a ...downloads.hindawi.com/journals/cris/2013/972596.pdf · CaseReportsinSurgery [] L. O. Baumgardner, Rupture of appendiceal](https://static.fdocuments.us/doc/165x107/605e04e918aee32c2626f671/case-report-stump-appendicitis-an-uncompleted-surgery-a-casereportsinsurgery.jpg)



![Clinical Study Laparoscopic-Assisted Single-Port ...Appendicitis is the most common cause of acute abdom-inaldiseaseinchildren[ ]. Despite several advantages of laparoscopic appendectomy](https://static.fdocuments.us/doc/165x107/60c5d0c53cc0b00b80379732/clinical-study-laparoscopic-assisted-single-port-appendicitis-is-the-most-common.jpg)
![Case Report Stump Appendicitis: An Uncompleted Surgery, a ... · a er appendectomy, but our case presented only four and half ((/)) months a er laparoscopic appendectomy [, ]. With](https://static.fdocuments.us/doc/165x107/60df3a7ef0e58c30304e41fe/case-report-stump-appendicitis-an-uncompleted-surgery-a-a-er-appendectomy.jpg)
