Study of Chronic Pelvic Pain Research Network Study HHS ...
22
Toll-like Receptor 4 and Comorbid Pain in Interstitial Cystitis/ Bladder Pain Syndrome: A Multidisciplinary Approach to the Study of Chronic Pelvic Pain Research Network Study Andrew Schrepf 1 , Catherine S. Bradley 2,3 , Michael O'Donnell 2 , Yi Luo 2 , Steven E. Harte 4 , Karl Kreder 2,3 , Susan Lutgendorf 1,2,3 , and the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network 1 Department of Psychology, University of Iowa 2 Department of Urology, University of Iowa 3 Department of Obstetrics and Gynecology, University of Iowa 4 Departments of Anesthesiology and Internal Medicine-Rheumatology, University of Michigan Abstract Background—Interstitial Cystitis/Bladder Pain Syndrome (IC/BPS) is a condition characterized by pelvic pain and urinary symptoms. Some IC/BPS patients have pain confined to the pelvic region, while others suffer widespread pain. Inflammatory processes have previously been linked to pelvic pain in IC/BPS, but their association with widespread pain in IC/BPS has not been characterized. Methods—Sixty-six women meeting criteria for IC/BPS completed self-report measures of pain as part of the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP), collected 3 days of saliva for cortisol assays, and provided blood samples. Peripheral blood mononuclear cells (PBMCs) were stimulated with Toll-Like Receptor (TLR) 2 and 4 agonists and cytokines were measured in supernatant; IL-6 was also measured in plasma. Associations between inflammatory variables and the likelihood of endorsing extra-pelvic pain, or the presence of a comorbid syndrome, were tested by logistic regression and General Linear Models, respectively. A subset of patients (n=32) completed Quantitative Sensory Testing. Corresponding Author: Susan Lutgendorf, E11 Seashore Hall, Iowa City, IA 52242, 319-335-2432, [email protected]. Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. Financial Disclosures Dr. Harte has received consulting fees from Analgesic Solutions, DeCode genetics, and Pfizer, and has received grant support from Forest Laboratories and Cerephex, outside the submitted work; in addition, Dr. Harte has proprietary interest in the Multimodal Automated Sensory Testing system used in this research, including inventorship on United States and International patent applications, a licensing agreement, and the right to receive royalties from product commercialization. Dr. Kreder has received honorariums from Tengion and Medtronic, and served as a consultant for Tengion, Medtronic, and Symptelligence, which he has an equity interest in, outside the submitted work. Mr. Schrepf and Drs. Bradley, O'Donnell, Luo and Lutgendorf report no financial disclosures or potential conflicts of interest. HHS Public Access Author manuscript Brain Behav Immun. Author manuscript; available in PMC 2016 October 01. Published in final edited form as: Brain Behav Immun. 2015 October ; 49: 66–74. doi:10.1016/j.bbi.2015.03.003. Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Transcript of Study of Chronic Pelvic Pain Research Network Study HHS ...

Toll-like Receptor 4 and Comorbid Pain in Interstitial Cystitis/Bladder Pain Syndrome: A Multidisciplinary Approach to the Study of Chronic Pelvic Pain Research Network Study
Andrew Schrepf1, Catherine S. Bradley2,3, Michael O'Donnell2, Yi Luo2, Steven E. Harte4, Karl Kreder2,3, Susan Lutgendorf1,2,3, and the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network1Department of Psychology, University of Iowa
2Department of Urology, University of Iowa
3Department of Obstetrics and Gynecology, University of Iowa
4 Departments of Anesthesiology and Internal Medicine-Rheumatology, University of Michigan
Abstract
Background—Interstitial Cystitis/Bladder Pain Syndrome (IC/BPS) is a condition characterized
by pelvic pain and urinary symptoms. Some IC/BPS patients have pain confined to the pelvic
region, while others suffer widespread pain. Inflammatory processes have previously been linked
to pelvic pain in IC/BPS, but their association with widespread pain in IC/BPS has not been
characterized.
Methods—Sixty-six women meeting criteria for IC/BPS completed self-report measures of pain
as part of the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP), collected 3
days of saliva for cortisol assays, and provided blood samples. Peripheral blood mononuclear cells
(PBMCs) were stimulated with Toll-Like Receptor (TLR) 2 and 4 agonists and cytokines were
measured in supernatant; IL-6 was also measured in plasma. Associations between inflammatory
variables and the likelihood of endorsing extra-pelvic pain, or the presence of a comorbid
syndrome, were tested by logistic regression and General Linear Models, respectively. A subset of
patients (n=32) completed Quantitative Sensory Testing.
Corresponding Author: Susan Lutgendorf, E11 Seashore Hall, Iowa City, IA 52242, 319-335-2432, [email protected].
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Financial DisclosuresDr. Harte has received consulting fees from Analgesic Solutions, DeCode genetics, and Pfizer, and has received grant support from Forest Laboratories and Cerephex, outside the submitted work; in addition, Dr. Harte has proprietary interest in the Multimodal Automated Sensory Testing system used in this research, including inventorship on United States and International patent applications, a licensing agreement, and the right to receive royalties from product commercialization. Dr. Kreder has received honorariums from Tengion and Medtronic, and served as a consultant for Tengion, Medtronic, and Symptelligence, which he has an equity interest in, outside the submitted work. Mr. Schrepf and Drs. Bradley, O'Donnell, Luo and Lutgendorf report no financial disclosures or potential conflicts of interest.
HHS Public AccessAuthor manuscriptBrain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Published in final edited form as:Brain Behav Immun. 2015 October ; 49: 66–74. doi:10.1016/j.bbi.2015.03.003.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Results—A one standard deviation increase in TLR-4 inflammatory response was associated
with a 1.59 greater likelihood of endorsing extra-pelvic pain (p = .019). Participants with
comorbid syndromes also had higher inflammatory responses to TLR-4 stimulation in PBMCs (p
= .016). Lower pressure pain thresholds were marginally associated with higher TLR-4
inflammatory responses (p = .062), and significantly associated with higher IL-6 in plasma (p = .
031).
Conclusions—TLR-4 inflammatory responses in PBMCs are a marker of widespread pain in
IC/BPS, and should be explored in other conditions characterized by medically unexplained pain.
Keywords
Inflammation; Toll-Like Receptors; Functional Somatic Syndromes; Pain; Negative Affect; Interstitial Cystitis/Bladder Pain Syndrome
1. Introduction
Interstitial Cystitis/Bladder Pain Syndrome (IC/BPS) is a highly prevalent debilitating
chronic condition characterized by pelvic/bladder pain and urinary symptoms such as
frequency, urgency, and nocturia (Hanno et al., 2011). Additionally, IC/BPS patients have a
high prevalence of psychiatric comorbidities including depression and anxiety disorders
(Clemens et al., 2008). While some patients present with Hunner's ulcers, inflammatory
lesions found on the wall of the bladder, approximately 90% do not (Simon et al, 1997).
IC/BPS is therefore a diagnosis of exclusion, and is sometimes considered a cluster of
medically unexplained symptoms.
It has been proposed that there may be distinct subtypes of IC/BPS, as some patients appear
to experience pain and discomfort in the pelvic/bladder region only (i.e. local pain), while
others report extra-pelvic pain consistent with somatic syndromes like fibromyalgia, Irritable
Bowel Syndrome (IBS), Chronic Fatigue Syndrome (CFS), or Temporomandibular joint
disorder (TMD), suggesting a condition mediated by the central nervous system. A recent
investigation found that that comorbid IBS and CFS were present in 39% and 19% of
IC/BPS patients, respectively (Nickel et al., 2010). These findings are consistent with the
results of many studies finding high degrees of comorbidity between somatic syndromes
(Wessely et al., 1999). This suggests that there may be common physiological factors that
support global changes in central pain pathways and increased pain perception (Phillips &
Clauw, 2011). Furthermore, IC/BPS patients with comorbid somatic syndromes (e.g. CFS)
appear to be at risk of developing additional somatic syndromes in the future, suggesting a
progressive element of altered pain perception in some patients (Warren et al., 2013).
Identifying markers of pain sensitization in IC/BPS may improve early phenotyping of
vulnerable patients and lead to novel therapeutic targets with the potential to prevent disease
progression. Furthermore, identifying markers of central sensitization in chronic pain
patients may further prevent psychiatric comorbidity as chronic pain has recently been
shown to induce dysfunction in the locus coeruleus and subsequent depression and anxiety
like behaviors in an animal model (Alba-Delgado et al., 2013). Much research has been
devoted to identifying altered mechanisms of pain perception (i.e. sensitized pathways), and
Schrepf et al. Page 2
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

whether reliable markers of these alterations can be identified. Candidate markers include
changes in pain processing networks identified through functional magnetic resonance
imaging (fMRI), and hyperalgesia/allodyina identified by quantitative sensory testing
(QST), both of which have identified abnormal responses to stimuli in chronic pain patients,
including patients with IC/BPS (Kilpatrick et al., 2014; Ness et al., 2014). Another
promising biomarker is the inflammatory response to Toll-Like Receptor (TLR) stimulation
in peripheral immune cells, as we have recently found these responses to be associated with
heightened pelvic pain in IC/BPS (Schrepf et al., 2014).
TLRs are highly conserved receptors on sentinel immune cells that respond to both Microbe
Associated Molecular Patterns (MAMPs) and Damage Associated Molecular Patterns
(DAMPs; Hutchinson et al., 2009). We have recently reported that TLR-2 inflammatory
responses distinguish IC/BPS patients from healthy controls, and that the magnitude of
TLR-4 inflammatory responses in stimulated PBMCs are associated with the extent of
painful urinary and pelvic symptoms reported by IC/BPS patients. PBMCs have been
hypothesized to mark pain sensitization in humans since it was demonstrated that
proliferation of PBMCs incubated with morphine is strongly associated with tolerance for
noxious cold stimuli (Hutchinson et al., 2004). Additionally, we found that IC/BPS patients
had higher serum levels of Interleukin (IL)-6, a marker of systemic inflammation, and
altered diurnal cortisol patterns (Schrepf et al., 2014). These finding echo a recent
investigation that found that TLR-2 and TLR-4 inflammatory responses in PBMCs
differentiate chronic pain patients from healthy controls (Kwok et al., 2012) and other work
identifying altered TLR inflammatory responses as features of other conditions
characterized by persistent pain such as Inflammatory Bowel Disease and Rheumatoid
arthritis (Kovarik et al., 2011; Kowalski et al., 2008). However, it is unknown if
inflammatory responses in PBMCs can differentiate subtypes of painful syndromes such as
IC/BPS, particularly those characterized by pain not typically considered part of the IC/BPS
syndrome (i.e. widespread, extra-pelvic pain.).
The purpose of the current study was to determine if inflammatory processes, especially
TLR-2 and TLR-4 inflammatory responses in PBMCs, are differentially associated with
pelvic vs. extra-pelvic pain in IC/BPS. Additionally, we examined relationships between
TLR-mediated inflammation, pain intensity/interference with daily life, and pressure pain
sensitivity determined by QST. We also examined the relationship between TLR-mediated
inflammation and the presence of comorbid pain conditions in IC/BPS patients, as these
conditions are characterized by pain outside the pelvic region, and contribute substantially to
the difficulty of treating the IC/BPS syndrome (Nickel et al., 2010). In line with the results
of our earlier work and results from animal models of chronic pain, we hypothesized that
greater TLR inflammatory responses in PBMCs would be associated with pain outside the
pelvic region, increased pain sensitivity by QST, and comorbid somatic syndromes.
2. Methods
2.1 MAPP Study and Recruitment
The Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) is a National
Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) sponsored research
Schrepf et al. Page 3
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

initiative comprising several sites with the objective of characterizing the epidemiology,
symptom trajectories, phenotypes and biological correlates of chronic pelvic pain (Clemens
et al. 2014). The University of Iowa is a participating institution emphasizing biomarker
research. Participants were eligible if they were at least 18 years of age, female, not
pregnant, and reported chronic pain/pressure/discomfort associated with the bladder or
pelvic region in the preceding three months. Participants had negative urine cultures for
uropathogens. Exclusion criteria included conditions which might result in tissue damage to
areas relevant to IC/BPS symptomology (e.g. history of urethral stricture, neurological
disorder affecting the bladder or bowel). Additional information about the MAPP project,
including patient characterization, study aims, and full exclusion criteria is available
(Clemens et al., 2014; Landis et al., 2014; Schrepf et al., 2014).
2.2 Demographic and Symptom Information
The sample was composed of an expanded group of participants from a previously reported
study (Schrepf et al. 2014) who provided additional information on pain and comorbid
syndromes. In addition, a subsample completed QST. Sixty-six women provided
demographic information at the time of eligibility screening, including information about
income, education, employment, race and ethnicity. Upon study entry, participants had a
blood draw, urine collection, physical examination and completed a battery of
questionnaires relating to pain and urological symptoms. These included the Brief Pain
Inventory (BPI), a measure of pain intensity, interference with daily life, and a body map for
selection of painful areas (Cleeland & Ryan, 1994) which has previously been validated in
chronic pain populations (Tan et al., 2004). The body map was modified so that patients
could select regions where pain was experienced from a standardized form of 45 distinct
areas. Participants were also administered self-report screens to assess the presence of
comorbid somatic syndromes. These included the Rome III criteria for IBS (Drossman &
Dumitrascu, 2006), the American College of Rheumatology diagnostic criteria for
Fibromyalgia (Wolfe et al., 2010), International Chronic Fatigue Syndrome Study Group
criteria for CFS (Fukuda et al., 1994), an 8 question MAPP specific diagnostic tool for
symptoms of vulvodynia (e.g. “experience constant burning or raw feeling at the opening of
the vagina,”) and the Research Diagnostic Criteria for TMD (Dworkin et al., 2002). These
diagnostic criteria show adequate reliability and validity (Dworkin et al., 2002; Ford et al.,
2013; Komaroff et al., 1996; Wolfe et al., 2010;) excepting the criteria for vulvodynia,
which is necessarily exploratory. Additionally, participants completed the reliable and
validated Positive and Negative Affect Scale (PANAS; Watson et al. 1988). Use of non-
steroidal anti-inflammatory drugs (NSAIDs), tricyclic antidepressants, opioids, selective
serotonin/norepinephrine reuptake inhibitors (SSRI/SNRI), and pentosan polysulfate, and
duration of symptoms in years, were collected by patient self-report.
2.3 Cortisol
Salivary cortisol was collected in salivettes by participants at 3 time points (upon waking:
4-9am, afternoon: 5 pm, and bedtime: 8pm-12am) for three consecutive days prior to the
baseline visit. Samples collected outside this time frame were excluded to maintain
homogeneity. Individual waking and bed times have been demonstrated to better
approximate diurnal cortisol rhythms than scheduled collection times (Kraemer et al., 2006).
Schrepf et al. Page 4
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Participants were instructed not to eat, exercise or consume caffeine for thirty minutes prior
to collecting a sample. Participants wrote the time of each collection on the salivette tubes.
Self-report of collection time has been demonstrated to be reliable and salivary cortisol is
stable at room temperature (Kraemer et al., 2006). Salivettes were analyzed by
chemiluminescence immunoassay (IBL, Hamburg, Germany) at the Technical University of
Dresden. The lower detection limit is 0.41 nmol/L and inter-assay and intra-assay
coefficients of variance are less than 10%.
2.4 Inflammatory Measures
Blood samples were collected between approximately 11:30am and 12:30pm. PBMCs were
separated by Ficoll-paque gradient centrifugation within 30 minutes of blood collection and
cultured in RPMI 1640 medium containing 10% fetal bovine serum, 100 U/ml penicillin and
100 ug/ml streptomycin for 3 days with TLR agonists at 37°C in a humidified incubator
with 5% CO2. TLR-2 and TLR-4 agonists were selected on the basis of the role of these
receptors in chronic pain in animal models and our previous findings linking them to
symptoms in IC/BPS (Bastos et al., 2013; Hutchinson et al., 2008; Schrepf et al., 2014;). For
stimulation of TLR-4, 50 ng/ml of Lipopolysaccharide (LPS) was used; for TLR-2
stimulation, 0.04 ng/ml of Staphylococcus aureus Cowan I (SAC) was used. Conditioned
media was then harvested and frozen at −80°C prior to batch ELISA analysis. Each well
contained 1×106 cells in 24 well plates, with one well per subject for TLR-4 and TLR-2
stimulation. Cytokines IL-6 and IL-1β were assayed in duplicate by DuoSet ELISAs (R&D
Systems) according to instructions included with the kit. Plasma IL-6 was assayed with a
high sensitivity Quantikine ELISA (R & D Systems).
2.5 Quantitative Sensory Testing
A subsample of participants completed the MAPP network QST protocol. Pressure pain
sensitivity was evaluated at the thumbnail (As-Sanie et al., 2013; Giesecke et al., 2004;
Petzke et al., 2001) using the Multimodal Automated Sensory Testing (MAST) system
(Harte et al., 2013). The MAST system consists of a control computer that executes testing
algorithms and stores testing data, and a touch-screen interface for participant feedback.
Computer-controlled pressure stimuli are applied to the thumbnail bed via a 1 cm2 rubber
probe housed within a wireless, pistol-grip style handset. Probe movement is driven by a
miniature servo-motor. A closed-looped control system measures applied pressures and
dynamically self-adjusts motor output to the resistance of the thumb and any movement to
ensure accurate and repeatable force delivery.
Participants received scripted instructions, and MAST system familiarization and practice
testing prior to data collection. During testing, an ascending series of 5-s duration pressures
were delivered at a rate of 4 kg/cm2/s to the dominant thumbnail beginning at 0.50 kg/cm2
and increasing in 0.50 kg/cm2 steps, with a minimum inter-stimulus interval of 20 s. Pain
intensity was rated after each stimulus on a 0-100 numerical rating scale (NRS) displayed on
the interface screen (0 = no pain; 100 = worst pain imaginable). Testing terminated when the
first of three possible stop conditions were met: 1) participant reached her personal pain
tolerance (i.e., requested to stop the test), 2) patient reported a pain intensity rating of ≥
80/100, or 3) the maximum pressure of 10 kg/cm2 was delivered. A modified three-
Schrepf et al. Page 5
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

parameter logistic model was used to fit the stimulus-response data obtained from this
procedure. The midpoint between the minimum and maximum stimulus intensity was
estimated within-person using the SAS NLIN procedure to derive an overall measure of
supra-threshold pressure pain sensitivity, referred to as Pain50. Additional outcome
variables included pressure pain threshold, defined as the first pressure in a string of at least
two consecutive pressures that elicited a NRS pain rating > 0, and pressure pain tolerance,
defined as the last pressure recorded in the stimulus response profile.
2.6 Data Analysis
Statistical analyses were performed using SPSS v. 21 and R v. 3.1.1. Cytokine values were
log-10 transformed, and cortisol values natural log transformed, to normalize their
distribution. The Inflammatory response scores for stimulated cytokines were calculated by
summing the z-scores ([individual score- group mean]/ group standard deviation) for the
IL-6 and interleukin-1 beta (IL-1β) response in PBMCs following stimulation with LPS
(TLR-4) or SAC (TLR-2. This inflammatory response score was then standardized for ease
of interpretation. Both IL-6 and IL-1β have been implicated in enhanced pain processing
when released by spinal glia, and both are released following TLR-2 and 4 stimulation, in
part, by transcription of nuclear factor-kappaB (NFκB; Milligan & Watkins, 2009). The
composite score, therefore, is likely more reflective of the inflammatory response to TLR
stimulation than either cytokine alone. Distributions of transformed variables were examined
for confirmation of normality. Salivary cortisol values at each of the collection points were
regressed on the time of collection over the three-day period to calculate cortisol slope, a
measure of the average hourly decrease in cortisol over the course of the day as described
previously (Kraemer et al., 2006).
To determine if inflammatory variables were associated with a greater likelihood of
endorsing extra-pelvic sites as painful, mixed-effects logistic regression models were used.
Higher probabilities of endorsing pain outside the pelvic region reflect pain not typically
considered part of the IC/BPS syndrome. Thus, endorsement of pain at any of the 44 sites
outside the pelvic region was considered indicative of extra-pelvic pain. In these models the
dependent variable of interest was the probability of a patient selecting any extra-pelvic site
(44 sites) as painful, with inflammatory variables as predictors. Subject and site specific
intercepts were tested as random effects, with the maximum random effects structure
retained by likelihood testing. Modeling subject specific variance (e.g. if some patients are
more likely to endorse any site as painful) and site-specific variance (e.g. if lower back pain
is more likely to be endorsed than pain in the hands across subjects) can allow more accurate
estimation of fixed effects (Baayen et al., 2008). Random intercept terms were retained for
subject and pain site. BMI, age, use of medications, presence of a comorbid condition, and
inflammatory variables were used in univariate analyses to determine which, if any
variables, were associated with a greater likelihood of endorsing extra-pelvic pain.
Significant variables (p < .05) were retained in multivariate analyses. Relationships between
pain severity/interference (from the BPI) and inflammation were tested in multivariate
General Linear Models with the same set of covariates. To explore the relationships between
inflammatory variables (e.g. TLR-4 inflammatory responses and cortisol slope) and duration
of symptoms in years Pearson correlations were used.
Schrepf et al. Page 6
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Group differences between IC/BPS only and IC/BPS comorbid patients (IBS, CFS,
fibromyalgia, TMD, vulvodynia) with respect to inflammatory variables were tested with
one-way ANOVAs, and between IC/BPS only and IC/BPS comorbid patients with
individual conditions (IBS, fibromyalgia, CFS, TMD and vulvodynia). The association
between number of comorbid conditions and inflammatory variables was tested by
Spearman's Rank correlations. Relationships between inflammatory variables and pain
intensity and interference were assessed using General Linear Models controlling for
negative affect, comorbid condition status, and use of SSRI/SSNIs, following the results of
the univariate analyses. Due to the non-normal distribution of QST Spearman's rank
correlation tests were used to test the association with inflammatory variables.
3. Results
3.1 Demographic Characteristics and Covariates
Participants were on average approximately 42 years old (range 20-74), and the vast
majority were non-Hispanic and white. See Table 1. Higher TLR-4 inflammatory responses
were associated with a greater likelihood of endorsing extra-pelvic pain (p= .006). SSRI/
SNRI use was associated with a greater likelihood of endorsing extra-pelvic pain (p < .001).
Tricyclic antidepressant use was marginally associated with a lower likelihood of endorsing
extra-pelvic pain (p = .081) whereas older age was marginally associated with a greater
likelihood of endorsing extra-pelvic pain (p =.071). Greater negative affect and presence of a
comorbid condition were both associated with a greater likelihood of endorsing extra-pelvic
pain (both p <.001). BMI, opioid use, NSAID use, Pentosan Polysulfate use, cortisol slope,
and duration of symptoms in years were not associated with the likelihood of endorsing
extra-pelvic pain (all p > .15; univariate analyses for covariate selection not shown).
Additionally, the inflammatory response to TLR-2 stimulation was not associated with a
greater likelihood of endorsing pain outside the pelvic region (Odds Ratio = 1.03, 95% CI
= .72, 1.49, p = .86). Therefore, multivariate analyses included comorbid status, SSRI/SNRI
use, and negative affect in addition to the TLR-4 inflammatory response.
3.2 TLR-4 Inflammatory Response and Pain
In multivariate analyses, a one standard deviation increase in the TLR-4 inflammatory
response was associated with 1.59 greater odds (95% CI = 1.08, 2.33) of endorsing pain
outside the pelvic area on the body map (p = .019), controlling for negative affect, comorbid
status, and SSRI/SNRI use. This one standard deviation increase in TLR-4 inflammatory
response corresponds to a 63% increase in the likelihood of a participant endorsing pain
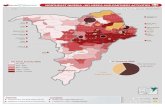
outside the pelvic region at any site on the body map.1 See Table 2. Figure 1 illustrates the
higher likelihood of endorsing extra-pelvic pain among those with higher TLR-4
inflammatory response. The TLR-4 inflammatory score was associated with greater self-
report of pain severity (p = .013) and pain interference (p = .046) on the BPI, controlling for
negative affect, comorbid status, and SSRI/SNRI use. See Table 3. Additionally, the TLR-4
1As a conservative measure, an additional analysis was conducted including tricyclic antidepressant use and patient age in addition to the above mentioned covariates. Neither tricyclic antidepressant use nor patient age were significantly associated with extra-pelvic pain (both p > .08) and their inclusion did not attenuate the association between TLR-4 mediated inflammation and extra-pelvic pain (odds ratio: 1.63, p = .013).
Schrepf et al. Page 7
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

inflammatory response was associated with higher TLR-2 inflammatory responses (r = .304,
p = .013) and longer duration of symptoms in years (r = .295, p=.017) but not with cortisol
slope (r = .165, p = .23 (n=56) or plasma IL-6 (r = .064, p = .61).
3.3 QST
In the subsample of 32 patients (13 IC/BPS only, 19 IC/BPS comorbid) who underwent
QST, higherTLR-4 inflammation scores were marginally associated with lower pressure
pain thresholds (Spearman's Rho= −.334, p = .062) and increased levels of IL-6 in plasma
were significantly associated with lower pressure pain thresholds (Spearman's Rho = −.381,
p = .031). In contrast, the TLR-2 inflammation score was not associated with pressure pain
thresholds (p =.30), nor was cortisol slope (p = .84). Pain50 and pressure pain tolerance
were not associated with inflammatory variables (all p > .19).
3.4 Inflammatory Measures and Comorbid Conditions
The TLR-4 inflammatory response was significantly greater in IC/BPS comorbid patients (p
= .016) compared to the IC/BPS patients without comorbid conditions. Additionally, a
higher TLR-4 inflammatory response distinguished IC/BPS + IBS patients (n=28, p = .018),
IC/BPS + TMD (n=23, p = .007), and IC + vulvodynia (n=14, p = .049), from IC/BPS only
participants (n=26). The TLR-4 inflammatory response was higher in IC/BPS + CFS
participants (n=8) and IC/BPS + fibromyalgia participants (n=2) but not significantly so
(both p > .18), possibly due to small sample sizes. IL-1β measured in supernatant of LPS
(TLR-4) stimulated PBMCs was significantly higher in IC/BPS patients with comorbid
conditions (p = .008) whereas IL-6 was not significantly elevated (p = .21). IL-1β and IL-6
measured in the supernatant of SAC (TLR-2)-stimulated PBMCs did not differ significantly
between groups (both p > .20) nor did the TLR-2 composite inflammatory score (p = .50).
IL-6 measured in plasma was marginally higher in IC/BPS comorbid participants (p = .097,
while cortisol slopes did not differ between groups (p = .96). See Table 4. Greater numbers
of comorbid syndromes were associated with a greater TLR-4 inflammatory response
(Spearman's Rho = .311, p = .011). No other inflammatory variable was associated with
number of comorbid conditions or presence of individual comorbid conditions (all p >.10).
4.1 Discussion
The key finding of this study is that TLR-4-mediated inflammatory responses in PBMCs are
associated with extra-pelvic pain in a chronic pelvic pain population. This is demonstrated in
the association between LPS evoked inflammation and an increasing likelihood of endorsing
pain outside the pelvic region, and by the ability of this inflammatory response to distinguish
between patients meeting criteria for IC/BPS only and patients meeting criteria for IC/BPS
who also had comorbid syndromes. Use of medications was not associated with measures of
pain, while greater negative affect was strongly associated with pain measures independent
of TLR-4 inflammation. While exploratory, QST data suggest that TLR-4 inflammation may
also be associated with lower pressure pain thresholds measured at a non-symptomatic site
remote from the pelvic region (i.e., the thumb), further suggesting a central mechanism of
pain hypersensitivity in this population. These findings build on our previous finding that
TLR-4 inflammation is associated with pelvic pain in IC/BPS (Schrepf et al., 2014) by
Schrepf et al. Page 8
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

demonstrating that TLR-4 inflammation is associated with comorbid pain not typically
considered part of the IC/BPS syndrome.
This is the first study to our knowledge which has shown TLR-mediated inflammation to be
associated with comorbid pain in a chronic pain population. Further, these differences in
TLR-4 mediated inflammation were not associated with a particular comorbid condition, as
each condition that was well-represented in our sample (IBS, TMD, and vulvodynia) was
characterized by higher TLR-4 mediated inflammation compared to patients with IC/BPS
only. This suggests that TLR-4 inflammation may reflect a broad mechanism by which pain
signaling is enhanced in IC/BPS. This extends our earlier finding that TLR-4 inflammation
predicts non-specific pain severity and frequency of pelvic pain symptoms in IC/BPS but
was not associated with pain in particular anatomical regions or during particular activities.
A recent investigation in an animal model of visceral pain found that TLR-4 regulates stress-
induced pain (Tramullas et al., 2014). This is notable given the high prevalence of IBS in
IC/BPS patients, and because stressful events frequently precipitate symptom flares
(Rothrock et al., 2001). QST data indicating lower pressure pain thresholds (increased pain
sensitivity) in patients with higher TLR-4 inflammatory responses and higher IL-6 in blood
suggest that these inflammatory processes are related to global pain sensitivity, not pain
associated with IC/BPS only, and are consistent with other findings that higher pro-
inflammatory cytokines in blood are associated with altered pain sensitivity on QST in
osteoarthritis patients (Lee et al., 2011). While the presence of a comorbid syndrome was
associated with an increased likelihood of endorsing extra-pelvic pain in a univariate model,
this was no longer true in the multivariate model including TLR-4 inflammation and
negative affect. This provides further evidence that TLR-4 inflammation may play a critical
role in the painful symptoms associated with comorbid conditions in IC/BPS, though it is
not possible to determine from these results what role, if any, TLR-4 inflammation may play
in centrally mediated pain sensitization.
The fact that TLR-2 stimulation distinguished patients from comparison participants in our
previous study, but did not distinguish between patients with and without comorbid
syndromes, is of interest. One possibility is that hypersensitivity to TLR-2 is an early or
universal feature of IC/BPS while TLR-4 sensitivity is not. Previous research has
demonstrated that higher TLR-2 density on PBMCs, but not TLR-4 density, distinguishes
IBS patients from controls (Ohman et al., 2012). Another recent study found that TLR-2 and
TLR-4 mRNA were up-regulated in the colonic mucosal tissue of IBS patients with
heterogeneous symptom presentation compared to those with symptoms of diarrhea or
constipation only (Belmonte et al. 2012). It is unknown if TLR-4 density on PBMCs or other
tissue may differ between IC/BPS patients with and without comorbid conditions, or if
TLR-4 responses are heightened in patients with comorbid syndromes due to a “priming”
effect of prior MAMP or DAMP exposure. Another possibility is that intracellular signaling
and subsequent cytokine production may differ significantly following TLR-4 vs. TLR-2
stimulation; a recent investigation of stimulated human whole blood found that both TLR-2
and TLR-4 stimulation resulted in NF-κB family activity, but that a distinct IFN
upregulation occurred following TLR-4 stimulation only (Blankley et al., 2014). Another
recent investigation used principal component analysis to analyze various cytokine and
chemokine responses to both TLR-2 and TLR-4 receptor stimulation in human whole blood;
Schrepf et al. Page 9
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

the results indicated that different TLR agonists (including TLR-2 and TLR-4), evoked
distinct protein signatures, suggesting divergent intracellular signaling pathways (Duffy et
al., 2014). Thus it appears that though TLR2 and 4 ligands may signal through the same
receptor, each cytokine is capable of eliciting unique signaling patterns. Another possibility
is that unexplored vulnerabilities (e.g. genetic factors) could mask the relationship between
TLR-2 mediated inflammation and pain, if such a relationship exists. Clearly, more research
is needed to identify relevant cellular and intracellular differences in TLR-4 vs. 2 responses
in the context of IC/BPS.
Microglia and astrocytes express TLRs including TLR-2 and TLR-4, and stimulation of
TLR-4 on microglia induces release of pro-inflammatory cytokines IL-6, IL-1β- and TNF-
alpha in the spinal cord (Milligan & Watkins, 2009). TLR-4-mediated inflammation released
by glia cells in the dorsal horn of the spinal cord is thought to be one contributing
mechanism for central pain amplification in rodent models of chronic pain (Ellis et al., 2014;
Grace et al., 2014; Hutchinson et al., 2008), though this effect may be sex specific, as recent
work suggests that LPS promotes hyperalgesia when delivered to the brain or periphery, but
not the spinal cord, in female mice (Sorge et al. 2011). Regardless, TLR-4 is essential in
LPS induced hyperalgesia as LPS injection fails to promote hyperalgesia in TLR-4 deficient
mice (Mattioli et al., 2014). Importantly for this study, the amplification of pain signaling
sometimes involves extension of pain from the original site of injury, termed “extra-
territorial” pain (Wieseler-Frank et al., 2005). Whether circulating PBMCs reflect neuro-
inflammatory processes remains an open question; recent work suggests that TLR-mediated
inflammation in PBMCs corresponds to the same TLR-mediated inflammation in the spinal
cord, in a rodent model of chronic pain (Kwok et al., 2013). However, relevant animal
models of IC/BPS will need to be developed before concordance between inflammatory
responses in PBMCs and spinal microglia can be formally tested.
While rodent models that investigate the role of TLRs in pain have typically used
neuropathic injury models (e.g. sciatic constriction), studies of human pain populations with
little evidence of peripheral tissue damage have also identified differential responses to TLR
stimulation in PBMCs (Kowalski et al., 2008; Schrepf et al., 2014). If sensitization of TLR-
induced inflammation is a mechanism for pain amplification in IC/BPS, this raises the
question of what the initiating events may be in this population, given the generally low
proportion of patients with evidence of peripheral tissue damage. One large twin study
implicated both genetic factors (approximately one third) and non-shared environmental
factors (approximately two thirds) in the risk of IC/BPS (Altman et al., 2011). At least two
large studies have identified an increased number of antecedent urogenital infections as a
risk factor for IC/BPS in women raising the possibility that recurrent or severe infections
might serve as initiating events in IC/BPS (Díaz Mohedo et al., 2014; Li et al. 2010). TLRs
including TLR-4 are pattern recognition receptors that respond to PAMPs and DAMPs; they
play a critical role in expelling bacteria from the urinary tract and are expressed on both
bladder epithelial cells and phagocytic cells that migrate into the bladder during infections
(Song & Abraham, 2008). Purified LPS infused directly into the bladder induces pain in the
pelvic region in a rodent model of urinary tract infection (Rudick et al., 2010). One
possibility, therefore, is that sustained local inflammatory events precipitate TLR
sensitization in migrating immune cells that then begin to modulate central pain processing
Schrepf et al. Page 10
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

after evidence of local infection is gone. This concept is supported by experiments
demonstrating that a single peripheral inflammatory challenge (e.g. formalin) or peripheral
trauma (e.g. laparotomy) can prime spinal microglia activation and subsequent LPS induced
allodynia for as long as two weeks (Hains et al., 2010). More direct implications for IC/BPS
symptoms have been demonstrated in an animal study that found a demyelination injury to
the sciatic nerve increased the sensitivity of bladder-associated sensory neurons to
chemokines and increased the frequency of micturition (Foster et al., 2011).
4.2 Limitations
This sample of IC/BPS patients was disproportionately non-Hispanic and white compared to
the general population. These findings require replication in a more diverse sample. Isolated
PBMCs were stimulated at a single dose-level of LPS and SAC. It is possible that
characterizing TLR-2 inflammatory responses at a wide range of doses might reveal
differences between IC/BPS only patients and those suffering comorbid conditions (Kwok et
al., 2013). These analyses are cross-sectional and cannot determine causal directions
between pain measures and TLR-mediated inflammation. A large number of statistical tests
were performed in exploring these novel hypotheses; these associations require replication
in other samples of IC/BPS patients.
4.1 Conclusions and Future Directions
TLR-4 mediated inflammation is a promising biomarker of comorbid pain in IC/BPS
patients and may be associated with pain in other somatic syndromes. Putative TLR-4
antagonists that have been shown effective at suppressing pain in animal models may have
application in IC/BPS populations. In addition to characterizing TLR-mediated
inflammatory responses at a wider range of concentrations, more research is required to
delineate the relationship between local inflammatory events and central pain sensitivity. As
IC/BPS is often characterized by symptom fluctuation, termed “flares,” future studies should
consider TLR-mediated inflammation in relation to these events.
Acknowledgments
The authors gratefully acknowledge the assistance of Mary Eno in carrying out this project. This research was funded by grant UO1DK082344 to K.K. from the National Institute of Diabetes Digestive and Kidney Diseases and by the Institute for Clinical and Translational Science at the University of Iowa, grant 2 UL1 TR000442-06 . The authors gratefully acknowledge the MAPP research network:
MAPP Network Executive Committee: J. Quentin Clemens, MD, FACS, MSci, Network Chair, 2013-, Philip Hanno, MD, Ziya Kirkali, MD, John W. Kusek, PhD, J. Richard Landis, PhD, M. Scott Lucia, MD, Chris Mullins, PhD, Michel A. Pontari, MD. Northwestern University Discovery Site : David J. Klumpp, PhD, Co-Director, Anthony J. Schaeffer, MD, Co-Director, Apkar (Vania) Apkarian, PhD, David Cella, PhD, Melissa A. Farmer, PhD, Colleen Fitzgerald, MD, Richard Gershon, PhD, James W. Griffith, PhD, Charles J. Heckman II, PhD, Mingchen Jiang, PhD, Laurie Keefer, PhD, Darlene S. Marko, RN, BSN, CCRC, Jean Michniewicz, Todd Parrish, PhD, Frank Tu, MD, MPH. University of California, Los Angeles Discovery Site and PAIN Neuroimaging Core: Emeran A. Mayer, MD, Co-Director, Larissa V. Rodríguez, MD, Co-Director, Jeffry Alger, PhD, Cody P. Ashe-McNalley, Ben Ellingson, PhD, Nuwanthi Heendeniya, Lisa Kilpatrick, PhD, Jason Kutch, PhD, Jennifer S. Labus, PhD, Bruce D. Naliboff, PhD, Fornessa Randal, Suzanne R. Smith, RN, NP. University of Iowa Discovery Site: Karl J. Kreder, MD, MBA, Director, Catherine S. Bradley, MD, MSCE, Mary Eno, RN, RA II, Kris Greiner, BA, Yi Luo, PhD, MD, Susan K. Lutgendorf, PhD, Michael A. O’Donnell, MD, Barbara Ziegler, BA. University of Michigan Discovery Site: Daniel J. Clauw, MD, Co-Director; Network Chair, 2008-2013, J. Quentin Clemens, MD, FACS, MSci, Co-Director; Network Chair, 2013-, Suzie As-Sanie, MD, Sandra Berry, MA, Megan E. Halvorson, BS, CCRP, Richard Harris, PhD, Steve Harte, PhD, Eric Ichesco, BS, Ann Oldendorf, MD, Katherine A. Scott, RN, BSN, David A. Williams, PhD. University of Washington, Seattle Discovery Site: Dedra Buchwald, MD, Director,
Schrepf et al. Page 11
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Niloofar Afari, PhD, Univ. Of California, San Diego, John Krieger, MD, Jane Miller, MD, Stephanie Richey, BS, Susan O. Ross, RN, MN, Roberta Spiro, MS, TJ Sundsvold, MPH, Eric Strachan, PhD, Claire C. Yang, MD. Washington University, St. Louis Discovery Site: Gerald L. Andriole, MD, Co-Director, H. Henry Lai, MD, Co-Director, Rebecca L. Bristol, BA, BS, Coordinator, Graham Colditz, MD, DrPH, Georg Deutsch, PhD, Univ. of Alabama at Birmingham, Vivien C. Gardner, RN, BSN, Coordinator, Robert W. Gereau IV, PhD, Jeffrey P Henderson, MD, PhD, Barry A. Hong, PhD, FAACP, Thomas M. Hooton, MD, Univ of Miami, Timothy J. Ness, MD, PhD, Univ. of Alabama at Birmingham, Carol S. North, MD, MPE, Univ. Texas Southwestern, Theresa M. Spitznagle, PT, DPT, WCS, Siobhan Sutcliffe, PhD, ScM, MHS. University of Pennsylvania Data Coordinating Core (DCC): J. Richard Landis, PhD, Core Director, Ted Barrell, BA, Philip Hanno, MD, Xiaoling Hou, MS, Tamara Howard, MPH, Michel A. Pontari, MD, Nancy Robinson, PhD, Alisa Stephens, PhD, Yanli Wang, MS, University of Colorado Denver Tissue Analysis & Technology Core (TATC): M. Scott Lucia, MD, Core Director, Adrie van Bokhoven, PhD, Andrea A. Osypuk, BS, Robert Dayton, Jr, Karen R. Jonscher, PhD, Holly T. Sullivan, BS, R. Storey Wilson, MS. Drexel University College of Medicine: Garth D.Ehrlich, PhD. Harvard Medical School/Boston Children's Hospital: Marsha A. Moses, PhD, Director, Andrew C. Briscoe, David Briscoe, MD, Adam Curatolo, BA, John Froehlich, PhD, Richard S. Lee, MD, Monisha Sachdev, BS, Keith R. Solomon, PhD, Hanno Steen, PhD. Stanford University : ,Sean Mackey, MD, PhD, Director, Epifanio Bagarinao, PhD, Lauren C. Foster, BA, Emily Hubbard, BA, Kevin A. Johnson, PhD, RN, Katherine T. Martucci, PhD, Rebecca L. McCue, BA, Rachel R. Moericke, MA, Aneesha Nilakantan, BA, Noorulain Noor, BS. Queens University: J. Curtis Nickel, MD, FRCSC, Director. National Institutes of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institutes of Health (NIH): Chris Mullins, PhD, John W. Kusek, PhD, Ziya Kirkali, MD, Tamara G. Bavendam, MD
References
Alba-Delgado C, Llorca-Torralba M, Horrillo I, Ortega JE, Mico JA, Sánchez-Blázquez P, Meana JJ, Berrocoso E. Chronic pain leads to concomitant noradrenergic impairment and mood disorders. Biol Psychiatry. 2013; 73:54–62. [PubMed: 22854119]
Altman D, Lundholm C, Milsom I, Peeker R, Fall M, Iliadou AN, Pedersen NL. The genetic and environmental contribution to the occurrence of bladder pain syndrome: an empirical approach in a nationwide population sample. Eur Urol. 2011; 59:280–285. [PubMed: 21056533]
As-Sanie S, Harris RE, Harte SE, Tu FF, Neshewat G, Clauw DJ. Increased pressure pain sensitivity in women with chronic pelvic pain. Obstet Gynecol. 2013; 122:1047–1055. [PubMed: 24104772]
Baayen RH, Davidson DJ, Bates DM. Mixed-effects modeling with crossed random effects for subjects and items. J Mem Lang. 2008; 59:390–412.
Bastos LF, Godin AM, Zhang Y, Jarussophon S, Ferreira BC, Machado RR, Maier SF, Konishi Y, de Freitas RP, Fiebich BL, Watkins LR, Coelho MM, Moraes MF. A minocycline derivative reduces nerve injury-induced allodynia, LPS-induced prostaglandin E2 microglial production and signaling via toll-like receptors 2 and 4. Neurosci Lett. 2013; 543:157–162. [PubMed: 23523650]
Belmonte L, Beutheu Youmba S, Bertiaux-Vandaële N, Antonietti M, Lecleire S, Zalar A, Gourcerol G, Leroi AM, Déchelotte P, Coëffier M, Ducrotté P. Role of toll like receptors in irritable bowel syndrome: differential mucosal immune activation according to the disease subtype. PLoS One. 2012; 7:e42777. [PubMed: 23028414]
Blankley S, Graham CM, Howes A, Bloom CI, Berry MP, Chaussabel D, Pascual V, Banchereau J, Lipman M, O'Garra A. Identification of the key differential transcriptional responses of human whole blood following TLR2 or TLR4 ligation in-vitro. PLoS One. 2014; 9:e97702. [PubMed: 24842522]
Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994; 23:129–138. [PubMed: 8080219]
Clemens JQ, Meenan RT, O'Keeffe Rosetti MC, Kimes TA, Calhoun EA. Case-control study of medical comorbidities in women with interstitial cystitis. J Urol. 2008; 179:2222–2225. [PubMed: 18423759]
Clemens JQ, Mullins C, Kusek JW, Kirkali Z, Mayer EA, Rodríguez LV, Klumpp DJ, Schaeffer AJ, Kreder KJ, Buchwald D, Andriole GL, Lucia MS, Landis JR, Clauw DJ. The MAPP research network: a novel study of urologic chronic pelvic pain syndromes. BMC Urol. 2014; 14:57. [PubMed: 25085007]
Díaz Mohedo E, Wärnberg J, Barón López FJ, Mera Velasco S, Cabello Burgos A. Chronic pelvic pain in Spanish women: prevalence and associated risk factors. A cross-sectional study. Clin Exp Obstet Gynecol. 2014; 41:243–248. [PubMed: 24992769]
Schrepf et al. Page 12
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Drossman DA, Dumitrascu DL. Rome III: New standard for functional gastrointestinal disorders. J Gastrointestin Liver Dis. 2006; 15:237–241. [PubMed: 17013448]
Duffy D, Rouilly V, Libri V, Hasan M, Beitz B, David M, Urrutia A, Bisiaux A, Labrie ST, Dubois A, Boneca IG, Delval C, Thomas S, Rogge L, Schmolz M, Quintana-Murci L, Albert ML, Milieu Intérieur Consortium. Functional analysis via standardized whole-blood stimulation systems defines the boundaries of a healthy immune response to complex stimuli. Immunity. 2014; 40:436–50. doi:10.1016/j.immuni.2014.03.002. [PubMed: 24656047]
Dworkin SF, Sherman J, Mancl L, Ohrbach R, LeResche L, Truelove E. Reliability, validity, and clinical utility of the research diagnostic criteria for Temporomandibular Disorders Axis II Scales: depression, non-specific physical symptoms, and graded chronic pain. J Orofac Pain. 2002; 16:207–220. [PubMed: 12221737]
Ellis A, Wieseler J, Favret J, Johnson KW, Rice KC, Maier SF, Falci S, Watkins LR. Systemic administration of propentofylline, ibudilast, and (+)-naltrexone each reverses mechanical allodynia in a novel rat model of central neuropathic pain. J Pain. 2014; 15:407–421. [PubMed: 24412802]
Ford AC, Bercik P, Morgan DG, Bolino C, Pintos-Sanchez MI, Moayyedi P. Validation of the Rome III criteria for the diagnosis of irritable bowel syndrome in secondary care. Gastroenterology. 2013; 145:1262–1270. e1. doi: 10.1053/j.gastro.2013.08.048. [PubMed: 23994201]
Foster R, Jung J, Farooq A, McClung C, Ripsch MS, Fitzgerald MP, White FA. Sciatic nerve injury induces functional pro-nociceptive chemokine receptors in bladder-associated primary afferent neurons in the rat. Neuroscience. 2011; 183:230–237. doi: 10.1016/j.neuroscience.2011.03.035. [PubMed: 21458542]
Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann Intern Med. 1994; 121:953–959. [PubMed: 7978722]
Giesecke J, Reed BD, Haefner HK, Giesecke T, Clauw DJ, Gracely RH. Quantitative Sensory Testing in Vulvodynia Patients and Increased Peripheral Pressure Pain Sensitivity. Obstet.Gynecol. 2004; 104:126–133. [PubMed: 15229011]
Grace PM, Hutchinson MR, Maier SF, Watkins LR. Pathological pain and the neuroimmune interface. Nat Rev Immunol. 2014; 14:217–31. doi: 10.1038/nri3621. [PubMed: 24577438]
Hains LE, Loram LC, Weiseler JL, Frank MG, Bloss EB, Sholar P, Taylor FR, Harrison JA, Martin TJ, Eisenach JC, Maier SF, Watkins LR. Pain intensity and duration can be enhanced by prior challenge: initial evidence suggestive of a role of microglial priming. J Pain. 2010; 11:1004–1014. [PubMed: 20434956]
Hanno PM, Burks DA, Clemens JQ, Dmochowski RR, Erickson D, Fitzgerald MP, Forrest JB, Gordon B, Gray M, Mayer RD, Newman D, Nyberg L Jr, Payne CK, Wesselmann U, Faraday MM. AUA guideline for the diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J Urol. 2011; 185:2162–2170. [PubMed: 21497847]
Harte SE, Mitra M, Ichesco EA, Halvorson ME, Clauw DJ, Shih AJ, Kruger GH. Development and validation of a pressure-type automated quantitative sensory testing system for point-of-care pain assessment. Med Biol Eng Comput. 2013; 51:633–644. [PubMed: 23381890]
Hutchinson MR, La Vincente SF, Somogyi AA. In vitro opioid induced proliferation of peripheral blood immune cells correlates with in vivo cold pressor pain tolerance in humans: a biological marker of pain tolerance. Pain. 2004; 110:751–755. [PubMed: 15288416]
Hutchinson MR, Zhang Y, Brown K, Coats BD, Shridhar M, Sholar PW, Patel SJ, Crysdale NY, Harrison JA, Maier SF, Rice KC, Watkins LR. Non-stereoselective reversal of neuropathic pain by naloxone and naltrexone: involvement of toll-like receptor 4 (TLR4). Eur J Neurosci. 2008; 28:20–29. [PubMed: 18662331]
Hutchinson MR, Ramos KM, Loram LC, Wieseler J, Sholar PW, Kearney JJ. Evidence for a role of heat shock protein-90 in toll like receptor 4 mediated pain enhancement in rats. Neuroscience. 2009; 164:1821–1832. [PubMed: 19788917]
Kilpatrick LA, Kutch JJ, Tillisch K, Naliboff BD, Labus JS, Jiang Z. Alterations in resting state oscillations and connectivity in sensory and motor networks in women with interstitial cystitis/painful bladder syndrome. J Urol. 2014; 192:947–955. [PubMed: 24681331]
Schrepf et al. Page 13
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Komaroff AL, Fagioli LR, Geiger AM, Doolittle TH, Lee J, Kornish RJ, Gleit MA, Guerriero RT. An examination of the working case definition of chronic fatigue syndrome. Am J Med. 1996; 100:56–64. [PubMed: 8579088]
Kovarik JJ, Tillinger W, Hofer J, Hölzl MA, Heinzl H, Saemann MD, Zlabinger GJ. Impaired anti-inflammatory efficacy of n-butyrate in patients with IBD. Eur J Clin Invest. 2011; 41:291–298. [PubMed: 21070220]
Kowalski ML, Wolska A, Grzegorczyk J, Hilt J, Jarzebska M, Drobniewski M, Synder M, Kurowski M. Increased responsiveness to toll-like receptor 4 stimulation in peripheral blood mononuclear cells from patients with recent onset rheumatoid arthritis. Mediators Inflamm. 2008; 2008:132732. [PubMed: 18584044]
Kraemer HC, Giese-Davis J, Yutsis M, O'Hara R, Neri E, Gallagher-Thompson D, Taylor CB, Spiegel D. Design decisions to optimize reliability of daytime cortisol slopes in an older population. Am J Geriatr Psychiatry. 2006; 14:325–333. [PubMed: 16582041]
Kwok YH, Hutchinson MR, Gentgall MG, Rolan PE. Increased responsiveness of peripheral blood mononuclear cells to in vitro TLR 2, 4 and 7 ligand in chronic pain patients. PLoS One. 2012; 7:e44232. [PubMed: 22937165]
Kwok YH, Tuke J, Nicotra LL, Grace PM, Rolan PE, Hutchinson MR. TLR 2 and 4 responsiveness from isolated peripheral blood mononuclear cells from rats and humans as potential chronic pain biomarkers. PLoS One. 2013; 8:e77799. [PubMed: 24204973]
Landis JR, Williams DA, Lucia MS, Clauw DJ, Naliboff BD, Robinson NA, van Bokhoven A, Sutcliffe S, Schaeffer AJ, Rodriguez LV, Mayer EA, Lai HH, Krieger JN, Kreder KJ, Afari N, Andriole GL, Bradley CS, Griffith JW, Klumpp DJ, Hong BA, Lutgendorf SK, Buchwald D, Yang CC, Mackey S, Pontari MA, Hanno P, Kusek JW, Mullins C, Clemens JQ. The MAPP research network: design, patient characterization and operations. BMC Urol. 2014; 14:58. [PubMed: 25085119]
Lee YC, Lu B, Bathon JM, Haythornthwaite JA, Smith MT, Page GG, Edwards RR. Pain sensitivity and pain reactivity in osteoarthritis. Arthritis Care Res. 2011; 63:320–327.
Li GZ, Zhang N, Du P, Yang Y, Wu SL, Xiao YX, Jin R, Liu L, Shen H, Dai Y. Risk factors for interstitial cystitis/painful bladder syndrome in patients with lower urinary tract symptoms: a Chinese multi-center study. Chin Med J. 2010; 23:2842–2846. [PubMed: 21034594]
Mattioli TA, Leduc-Pessah H, Skelhorne-Gross G, Nicol CJ, Milne B, Trang T, Cahill CM. Toll-like receptor 4 mutant and null mice retain morphine-induced tolerance, hyperalgesia, and physical dependence. PLoS One. 2014; 9:e97361. [PubMed: 24824631]
Milligan ED, Watkins LR. Pathological and protective roles of glia in chronic pain. Nat Rev Neurosci. 2009; 10:23–36. [PubMed: 19096368]
Ness TJ, Lloyd LK, Fillingim RB. An endogenous pain control system is altered in subjects with interstitial cystitis. J Urol. 2014; 191:364–370. [PubMed: 23973521]
Nickel JC, Tripp DA, Pontari M, Moldwin R, Mayer R, Carr LK. Interstitial cystitis/painful bladder syndrome and associated medical conditions with an emphasis on irritable bowel syndrome, fibromyalgia and chronic fatigue syndrome. J Urol. 2010; 184:1358–1363. [PubMed: 20719340]
Ohman L, Lindmark AC, Isaksson S, Posserud I, Strid H, Sjövall H, Simrén M. Increased TLR2 expression on blood monocytes in irritable bowel syndrome patients. Eur J Gastroenterol Hepatol. 2012; 24:398–405. [PubMed: 22273988]
Petzke F, Khine A, Williams D, Groner K, Clauw DJ, Gracely RH. Dolorimetry performed at 3 paired tender points highly predicts overall tenderness. J Rheumatol. 2001; 28:2568–2569. [PubMed: 11708444]
Phillips K, Clauw DJ. Central pain mechanisms in chronic pain states--maybe it is all in their head. Best Pract Res Clin Rheumatol. 2011; 25:141–154. [PubMed: 22094191]
Rothrock NE, Lutgendorf SK, Kreder KJ, Ratliff T, Zimmerman B. Stress and symptoms in patients with interstitial cystitis: a life stress model. Urology. 2001; 57:422–427. [PubMed: 11248609]
Rudick CN, Billips BK, Pavlov VI, Yaggie RE, Schaeffer AJ, Klumpp DJ. Host-pathogen interactions mediating pain of urinary tract infection. J Infect Dis. 2010; 201:1240–9. [PubMed: 20225955]
Schrepf A, O'Donnell M, Luo Y, Bradley CS, Kreder K, Lutgendorf S, Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network. Inflammation and inflammatory
Schrepf et al. Page 14
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

control in interstitial cystitis/bladder pain syndrome: Associations with painful symptoms. Pain. 2014; 155:1755–1761. [PubMed: 24907404]
Simon LJ, Landis JR, Erickson DR, Nyberg LM. The Interstitial Cystitis Data Base Study: concepts and preliminary baseline descriptive statistics. Urology. 1997; 49:64–75. [PubMed: 9146004]
Song J, Abraham SN. TLR-mediated immune responses in the urinary tract. Curr Opin Microbiol. 2008; 11:66–73. [PubMed: 18243043]
Sorge RE, LaCroix-Fralish ML, Tuttle AH, Sotocinal SG, Austin JS, Ritchie J, Chanda ML, Graham AC, Topham L, Beggs S, Salter MW, Mogil JS. Spinal cord Toll-like receptor 4 mediates inflammatory and neuropathic hypersensitivity in male but not female mice. J Neurosci. 2011; 31:15450–15454. [PubMed: 22031891]
Tan G, Jensen MP, Thornby JI, Shanti BF. Validation of the Brief Pain Inventory for chronic nonmalignant pain. J Pain. 2004; 5:133–137. [PubMed: 15042521]
Tramullas M, Finger BC, Moloney RD, Golubeva AV, Moloney G, Dinan TG, Cryan JF. Toll-like receptor 4 regulates chronic stress-induced visceral pain in mice. Biol Psychiatry. 2014; 76:340–8. [PubMed: 24331544]
Warren JW, Langenberg P, Clauw DJ. The number of existing functional somatic syndromes (FSSs) is an important risk factor for new, different FSSs. J Psychosom Res. 2013; 74:12–17. [PubMed: 23272983]
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988; 54:1063–1070. [PubMed: 3397865]
Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many? Lancet. 1999; 354:936–939. [PubMed: 10489969]
Wieseler-Frank J, Maier SF, Watkins LR. Central proinflammatory cytokines and pain enhancement. Neurosignals. 2005; 14:166–174. [PubMed: 16215299]
Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010; 62:600–610.
Schrepf et al. Page 15
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Highlights
• We measured inflammatory responses in PBMCs to TLR stimulation in IC/BPS
patients
• Greater responses to TLR-4 stimulation were associated with widespread pain
• Greater responses to TLR-4 stimulation were associated with comorbid
conditions
• TLR-4 mediated inflammation may be a therapeutic target in unexplained
chronic pain
Schrepf et al. Page 16
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Figure 1. Prevalence of pain reported in the first tertile (low) of the TLR-4 composite inflammatory
score versus the third tertile (high) for each site on the body map.
Schrepf et al. Page 17
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schrepf et al. Page 18
Table 1
Participant Characteristics.
Participant Characteristics N=66
Age Mean(SD) 42.03 (15.12)
BMI Mean(SD) 27.18 (5.65)
PANAS negative affect 22.27 (8.56)
Race % (n)
White 97 (64)
Asian 1 (1)
Multi Race 1 (1)
Ethnicity % (n)
Non-Hispanic 98 (65)
Hispanic 1 (1)
Education % (n)
High School or GED 13 (9)
Some College 27 (18)
Graduated College 32 (21)
Graduate Degree 27 (18)
Employment % (n)
Employed 62 (41)
Unemployed 11 (7)
Disabled 8 (5)
Retired 9 (6)
Full Time Homemaker 9 (6)
Not Answered 1 (1)
Annual Income/$ % (n)
<10,000 14 (9)
<25,000 6 (4)
<50,000 23 (15)
<100,000 33 (22)
>100,000 20 (13)
Prefer not to answer 5 (3)
Comorbid Conditions % (n)
None 39 (26)
Irritable Bowel Syndrome 42 (28)
Fibromyalgia 3 (2)
Chronic Fatigue Syndrome 12 (8)
TMD 35 (23)
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schrepf et al. Page 19
Participant Characteristics N=66
Vulvodynia 21 (14)
Number of Comorbid Conditions % (n)
0 39 (26)
1 26 (17)
2 23 (15)
3 6 (4)
4 6 (4)
Tricyclic anti-depressants
No 56 (37)
Yes 44 (29)
Opioids
No 83 (55)
Yes 17 (11)
Pentosan Polysulfate
No 56 (37)
Yes 44 (29)
NSAIDs
No 89 (59)
Yes 11 (7)
SSRI/SNRIs
No 86 (57)
Yes 14 (9)
IC/BPS=Interstitial Cystitis/Bladder Pain Syndrome. BMI=Body Mass Index. NSAID= non-steroidal anti-inflammatory drug. SSRI/SNRI = selective serotonin reuptake inhibitor/serotonin-norepinephrine reuptake inhibitor. TMD = temporomandibular disorders.
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schrepf et al. Page 20
Table 2
Relationship of TLR-4 inflammatory response and covariates (logistic regression) with extra-pelvic pain.
Outcome Measure Predictor Est. S.E. Z value Odds Ratio 95% CI p
Extra-Pelvic Pain
TLR-4 inflammation response (one SD above mean) .46 .20 2.34 1.591.08, 2.33
.019
Use of SSRI/SNRI .41 .57 .73 1.51.50, 4.59
.47
Comorbid Condition .39 .43 .92 1.48.64, 4.59
.36
PANAS negative affect (one SD above mean) .66 .21 3.12 1.94, 1.28, 2.95 .002
BPI= Brief Pain Inventory. IL-6=Interleukin-6. PANAS=Positive and Negative Affect Scale. TLR=Toll-Like Receptor.
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schrepf et al. Page 21
Table 3
General Linear Models testing relationship of TLR-4 inflammatory response and covariates with BPI
symptom scores.
Outcome Measure Predictor B. S.E. F1,65 95% CI p
Pain Severity (BPI)
TLR-4 inflammatory response .503 .197 6.53 .109,.896 .013
Comorbid condition .204 .429 .23 −1.063, .655 .64
Use of SSRI/SNRI −.156 .615 .06 −1.075, 1.386 .97
PANAS negative affect .096 .025 14.83 .046,.145 <.01
Pain Interference (BPI)
TLR-4 inflammatory response .567 .278 4.17 .012, 1.123 .046
comorbid condition .200 .607 .50 −1.414, 1.014 .74
Use of SSRI/SNRI −.028 .832 .01 −1.635, 1.691 .97
PANAS negative affect .171 .035 23.67 .101,.241 <.01
BPI= Brief Pain Inventory. IL-6=Interleukin-6. PANAS=Positive and Negative Affect Scale. TLR=Toll-Like Receptor.
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schrepf et al. Page 22
Table 4
Means, standard deviations and 95% confidence intervals of biomarkers in participants with IC/BPS only and
those with additional comorbid conditions (Fibromyalgia, Irritable Bowel Syndrome, vulvodynia, Chronic
Fatigue Syndrome, Temperomandibular Disorder)
Variable Mean (S.D.) 95% CI Inflammatory Variables IC Only n=26 IC Comorbid n=40 p
TLR-4 inflammatory response −.36 (1.13)−.82, .09
.24 (.85)−.03, .51
.016
IL-1β + LPS 3.11 (.93)2.73,3.48
3.58 (.44)3.44, 3.72
.008
IL-6 + LPS 4.15 (.40)3.99, 4.31
4.28 (.42)4.14, 4.41
.205
TLR-2 inflammatory response −.10 (1.06)−.53, .32
.07 (.97)−.24, .38
.501
IL-1β + SAC 1.17 (1.19).69, 1.65
1.44 (1.14)1.08, 1.81
.365
IL-6 + SAC 1.68 (1.37)1.13, 2.24
1.79 (1.22)1.40, 2.19
.719
Cortisol Slope (ln transformed) n=22−.11 (.06)−.14, −.08
n=34−.11 (.07)−.13, −.08
.955
IL-6 plasma (log10 transformed) .33 (.35)−.75, 0.84
.46 (.26).00, .97
.097
Duration of Symptoms (years) 6.91 (7.48)3.89, 9.93
8.3 (8.00)5.71, 10.90
.48
IL-6=Interleukin-6. IL-1β=Interleukin-1 beta. LPS= lipopolysaccharide. SAC= Staphylococcus aureus Cowan. TLR = Toll-Like Receptor.
Brain Behav Immun. Author manuscript; available in PMC 2016 October 01.