Structure/function interface with sequential shortening of basal and apical components of the...
23
Structure/function interface with sequential shortening of basal and apical components of the myocardial band Gerald D. Buckberg a,c, * , Manuel Castella´ c , Morteza Gharib a , Saleh Saleh b a Option of Bioengineering, California Institute of Technology, Pasadena, CA, USA b Department of Medicine, David Geffen School of Medicine at UCLA, USA c Department of Surgery, Division of Cardiothoracic Surgery, David Geffen School of Medicine at UCLA, 10833 Le Conte Avenue, 62-258 CHS, Los Angeles, CA 90095-1701, USA Received 17 February 2006; accepted 27 February 2006 Abstract Objective: To study the sequential shortening of Torrent-Guasp’s ‘rope-heart model’ of the muscular band, and analyze the structure—function relationship of basal loop wrapping the outer right and left ventricles, around the inner helical apical loop containing reciprocal descending and ascending spiral segments. Methods: In 24 pigs (27—82 kg), temporal shortening by sonomicrometer crystals was recorded. The ECG evaluated rhythm, and Millar pressure transducers measured intraventricular pressure and dP/dt. Results: The predominant shortening sequence proceeded from right to left in basal loop, then down the descending and up the ascending apical loop segments. In muscle surrounded by the basal loop, epicardial muscle predominantly shortened before endocardial muscle. Crystal location defined underlying contractile trajectory; transverse in basal versus oblique in apical loop, subendocardial in descending and subepicardial in ascending segments. Mean shortening fraction average 18 3%, with endocardial exceeding epicardial shortening by 5 1%. Ascending segment crystal displacement followed descending shortening by 82 23 ms, and finished 92 33 ms after descending shortening stops, causing active systolic shortening to suction venous return; isovolumetric relaxation was absent. Conclusions: Shortening sequence followed the rope-like myocardial band model to contradict traditional thinking. Epicardial muscle shortened before endocardial papillary muscle despite early endocardial activation, and suction filling follows active systolic unopposed ascending segment shortening during the ‘isovolumetric relaxation’ phase. # 2006 Published by Elsevier B.V. Keywords: Helical ventricular myocardial band; Isovolumetric contraction and relaxation; Sonomicrometer crystals; Systolic ventricular filling 1. Introduction In spite of recent remarkable progress in understanding cellular myocardial function at the genetic/molecular level, the advancement in developing a comprehensive under- standing of ventricular structure has been limited to microscopic scales [1,2]. These concepts are mainly based on Streeter’s [3—5] two-dimensional measurements of a uniformly changing angle of orientation of myocardial microscopic fibers from epicadium to endocardium. Stre- eter’s findings have helped us to recognize the intricate nature of local fiber structure and perhaps function. However, in order to understand cardiac function and its efficiency from the point of view of vectors of force generated by cardiac sarcomeres, one needs to develop a global three-dimensional model of ventricular structure adhering to the local and global dynamics of myocardial spatial architecture. Streeter recognized the seminal conceptual framework of Krehl’s Treibwerk representation of the figure-of-eight oblique fiber pathways, connecting inner and outer cones, and verification of this idea by the dissection techniques of Torrent-Guasp that vindicates the Treibwerk, showing a highly ordered compact structure [6]. The re-introduction of a helical rope-like heart muscle concept by Torrent-Guasp et al. [7—9] offers a radically different view thus challenging the prevailing anatomical views of myocardial structure and function. In this concept, the ventricular structure consists of a single myofiber band, with a principal fiber pathway extending from the right ventricular muscle just below the pulmonary artery, to the left ventricular muscle attached to the aorta, twisted into a transverse outer shell and then wrapped into an oblique double helical coil. In this view (Fig. 1a—c, and on video on http://www.gharib.caltech.edu/ www.elsevier.com/locate/ejcts European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 * Corresponding author. Address: Department of Surgery, Division of Cardi- othoracic Surgery, David Geffen School of Medicine at UCLA, 10833 Le Conte Avenue, 62-258 CHS, Los Angeles, CA 90095-1701, USA. Tel.: +1 310 206 1027; fax: +1 310 825 5895. E-mail address: [email protected] (G.D. Buckberg). 1010-7940/$ — see front matter # 2006 Published by Elsevier B.V. doi:10.1016/j.ejcts.2006.02.065
Transcript of Structure/function interface with sequential shortening of basal and apical components of the...

Structure/function interface with sequential shortening of basaland apical components of the myocardial band
Gerald D. Buckberg a,c,*, Manuel Castella c, Morteza Gharib a, Saleh Saleh b
aOption of Bioengineering, California Institute of Technology, Pasadena, CA, USAbDepartment of Medicine, David Geffen School of Medicine at UCLA, USA
cDepartment of Surgery, Division of Cardiothoracic Surgery, David Geffen School of Medicine at UCLA,10833 Le Conte Avenue, 62-258 CHS, Los Angeles, CA 90095-1701, USA
Received 17 February 2006; accepted 27 February 2006
Abstract
Objective: To study the sequential shortening of Torrent-Guasp’s ‘rope-heartmodel’ of themuscular band, and analyze the structure—functionrelationship of basal loop wrapping the outer right and left ventricles, around the inner helical apical loop containing reciprocal descending andascending spiral segments. Methods: In 24 pigs (27—82 kg), temporal shortening by sonomicrometer crystals was recorded. The ECG evaluatedrhythm, and Millar pressure transducers measured intraventricular pressure and dP/dt. Results: The predominant shortening sequenceproceeded from right to left in basal loop, then down the descending and up the ascending apical loop segments. In muscle surrounded bythe basal loop, epicardial muscle predominantly shortened before endocardial muscle. Crystal location defined underlying contractile trajectory;transverse in basal versus oblique in apical loop, subendocardial in descending and subepicardial in ascending segments. Mean shortening fractionaverage 18 � 3%, with endocardial exceeding epicardial shortening by 5 � 1%. Ascending segment crystal displacement followed descendingshortening by 82 � 23 ms, and finished 92 � 33 ms after descending shortening stops, causing active systolic shortening to suction venous return;isovolumetric relaxation was absent. Conclusions: Shortening sequence followed the rope-like myocardial band model to contradict traditionalthinking. Epicardial muscle shortened before endocardial papillary muscle despite early endocardial activation, and suction filling follows activesystolic unopposed ascending segment shortening during the ‘isovolumetric relaxation’ phase.# 2006 Published by Elsevier B.V.
Keywords: Helical ventricular myocardial band; Isovolumetric contraction and relaxation; Sonomicrometer crystals; Systolic ventricular filling
www.elsevier.com/locate/ejctsEuropean Journal of Cardio-thoracic Surgery 29S (2006) S75—S97
1. Introduction
In spite of recent remarkable progress in understandingcellular myocardial function at the genetic/molecular level,the advancement in developing a comprehensive under-standing of ventricular structure has been limited tomicroscopic scales [1,2]. These concepts are mainly basedon Streeter’s [3—5] two-dimensional measurements of auniformly changing angle of orientation of myocardialmicroscopic fibers from epicadium to endocardium. Stre-eter’s findings have helped us to recognize the intricatenature of local fiber structure and perhaps function.However, in order to understand cardiac function and itsefficiency from the point of view of vectors of force
* Corresponding author. Address: Department of Surgery, Division of Cardi-othoracic Surgery, David Geffen School of Medicine at UCLA, 10833 Le ConteAvenue, 62-258 CHS, Los Angeles, CA 90095-1701, USA. Tel.: +1 310 206 1027;fax: +1 310 825 5895.
E-mail address: [email protected] (G.D. Buckberg).
1010-7940/$ — see front matter # 2006 Published by Elsevier B.V.doi:10.1016/j.ejcts.2006.02.065
generated by cardiac sarcomeres, one needs to develop aglobal three-dimensional model of ventricular structureadhering to the local and global dynamics of myocardialspatial architecture.
Streeter recognized the seminal conceptual framework ofKrehl’s Treibwerk representation of the figure-of-eightoblique fiber pathways, connecting inner and outer cones,and verification of this idea by the dissection techniques ofTorrent-Guasp that vindicates the Treibwerk, showing ahighly ordered compact structure [6]. The re-introduction ofa helical rope-like heart muscle concept by Torrent-Guaspet al. [7—9] offers a radically different view thus challengingthe prevailing anatomical views of myocardial structure andfunction. In this concept, the ventricular structure consists ofa single myofiber band, with a principal fiber pathwayextending from the right ventricular muscle just below thepulmonary artery, to the left ventricular muscle attached tothe aorta, twisted into a transverse outer shell and thenwrapped into an oblique double helical coil. In this view(Fig. 1a—c, and on video on http://www.gharib.caltech.edu/

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S76
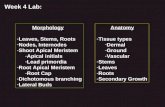
Fig. 1. Five successive phases in unwinding of the ventricularmyocardial band.In the first specimen (upper left), the band is in the normal position in theintact heart. In the last specimen (bottom) the band is fully expanded.
�heart/) both the outer circumferential wrap and innerhelical fiber bundle, which weave through myocardialsubstance, provide a preferential pathway for possiblesequential contractile dynamics.
The validity of any cardiac model relies upon showing thatthe structure can explain physiological function whenactivated. Torrent-Guasp’s concept, if correct, offers inter-esting opportunities to explain ventricular shape andmechanics based on realistic fiber shortening and dynamicrearrangement. Also, unlike the current views, it offers aunified concept of systolic ejection and the early suctionphase of ‘diastolic’ cardiac function. It provides a unifyingtheme because it can explain both phases of cardiac functionthrough a sequential contractile action. This is in contrastwith the conventional acceptance of elastic recoil fromstored potential energy during systole to explain isovolu-metric relaxation [10—13]. With Torrent-Guasp’s structuralmodel, a sequential contractile wave through the prefer-ential helical band can induce a coil-like twisting andreciprocal twisting in the opposite direction of the leftventricle and septum to cause the physiologic events ofejection and suction.
Torrent-Guasp’s model, with its main emphasis on thefiber architecture and dynamics, has been criticized for notbeing compatible with the Purkinje network of electricalactivation and its implications for the electromechanical andmechanical determinants of cardiac function. Also, the mereexistence of a preferential pathway for the contractile wavehas been questioned [14,15]. While the precise linking ofexcitation and contraction may require extensive under-taking, the latter concern over the time related contractileprocess can be possibly resolved through advanced MRItechniques [10,16] and, to a more limited extent, throughdirect mapping of contractile wave pathways by directmeasurement of local myocardium mass along Torrent-Guasp’s proposed helical fiber band.
The main objective of this paper is to mechanically probethe intact cardiac structure with sonomicrometer crystals[17,18], thus testing the hypothesis that the contractile wave
produces fiber shortening along Torrent-Guasp’s myocardialband and such contractile wave can move sequentially withits principle axis (maximum displacement orientation)aligned with local fiber bundle orientation. We used multiplesonomicrometer transducer-pairs to identify the principleangle of local fiber bundles at subendocardial/epicardialpositions throughout the left and right heart.
2. Material and methods
All animals received humane care in compliance with the‘Principles of Laboratory Animal Care’ formulated by theInstitute of Laboratory Animal Resources and the ‘Guide forthe Care and Use of Laboratory’ prepared by the NationalInstitutes of Health (NIH Publication No. 86-23, revised1985).
Twenty-four Yorkshire—Duroc pigs (27—82 kg) were pre-medicated (ketamine 15 mg/kg, diazepam 0.5 mg/kg intra-muscularly) and anesthetized with inhaled isoflurane 1.5%(MAC 1%) throughout the operation. Support with a volume-controlled ventilator (Servo 900C, Siemens-Elema, Sweden)was started after tracheostomy and endotracheal intubation.The femoral artery and vein were cannulated and arterialblood gases measured to keep oxygen tension, carbon dioxidetension, and pH values within the normal range. A balloon-tipped catheter (Model 132F5, Baxter Healthcare Corp.,Irvine, CA, USA) was advanced into the pulmonary arterythrough a jugular vein to measure cardiac output (thermo-dilution technique) and pulmonary artery pressure.
The pericardium was incised after median sternotomy anda solid-stated pressure transducer-tipped catheter (ModelMPC-500, Millar Instruments Inc., Houston, TX, USA) wasinserted through the apex to monitor left ventricularpressure (LVP). Regional contractility within the right andleft ventricles was measured with pairs of 2 mm ultrasonicmicrotransducer crystals (Sonometrics, London, Ont.,Canada). Each pair of crystals was oriented in order tomeasure contractility at a certain myocardial depth andorientation. The placement position of each crystal wasmade by using a 1 mm cut of the epicardium and introductionof the crystal to reach the depth selected. In the leftventricle two depths were chosen, endocardial, where thecrystals were positioned transmurally to reach the innersurface via the ventricular cavity, or subepicardial, byinsertion of 1 mm deep into the ventricular muscle. In theright ventricle, crystals were positioned in the endocardialwall, either in the outflow tract, or laterally by theatrioventricular groove. Aortic pressure, LVP, dP/dt, andsonomicrometer crystals data were digitally processed byspecific hardware and software (Sonometrics). Velocity ofsound through cardiac tissue was fixed to 1590 m/s.Sonomicrometer measurements were recorded with asampling rate of 95.8 samples per second, a transmitterspacing of 652 ms, transmit inhibit delay of 1.81 ms, andtransmit pulse length of 375 ns. Synchronicity betweenmyocardial contractility was compared to left ventricularperformance with 1 ms precision, by real-time plotting andprocessing of segment shortening, EKG, LVP, and dP/dt.Sequence of contraction of different segments of the heartwas then established and compared with ventricular

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S77
hemodynamics. All cases were performed and analyzed bythe same surgeon.
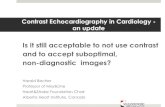
Fig. 2. The frontal view shows the aberrant fibers removed to define theunderneath musculature of the right ventricle. The trajectory of these aber-rant fibers, coming from the ascending segment of the apical loop, jump fromthe anterior surface of the left ventricle to cover the free wall of the rightventricle to then pass over the posterior face of the left ventricle (left arrow)to arrive again on the anterior surface (right arrow).
3. Experimental protocol
The insertion of pairs of sonomicrometer crystals indifferent positions/depth allowed the extent of segmentshortening to be measured in the anterior wall of the leftventricle, recording the dimension angle of contraction andmyocardial depth. Segmental shortening was calculated asfollows:
ðEDL� ESLÞEDL
� 100
where EDL and ESL are end diastolic and end systolic lengths,respectively.
The pattern of orientation is described in the Section 4.This dimension (angle of highest contractility relative to thelong axis of the heart) was registered for both endocardialand subepicardial contraction, and compared with synchro-nized EKG, LVP, and dP/dt. These measurements werecompared in real time with different pharmacologic changesof regional contractility, and position sites in the left andright ventricles.
4. Crystal orientation
Francisco Torrent-Guasp’s model of the helical heart ispresented in Fig. 1. In this model, the cardiac structureincludes two simple connected loops that start at thepulmonary artery and end in the aorta. The first loop, termedbasal loop, includes a horizontal basal band, which comprisesright and left segments surrounding the right and leftventricles. This basal band connects to the second apical loopthrough a downward spiral fold that causes an obliqueorientation of the band fibers that form the apical loop whichconsists of an endocardial or descending helical segment andan epicardial or ascending helical segment with opposing andoblique directional fiber pathways connected at the apicaltip. The oblique fibers of the ascending segment completetheir trajectory by bifurcating (as aberrant fibers) as shown inFig. 2 [19] to either the septal fibers coursing deeply towardthe aorta, or stay superficial and jump from the anterior leftventricular surface of the right ventricle to connect to thepulmonary artery, A-V rings and posterior perimeter of theventricular base Fig. 3 compares a silicon rubber cardiacmould [20] to the anatomic heart counterpart.
The sonomicrometer crystals were placed into the intactheart to test any relationship between sequential temporaland mechanical extent of fiber shortening between couplesof crystals to model shape and timing. Their orientation wasnested within and without the principal pathways comprisingthe suggested rope-like arrangement of the helical heart.Each of these internal and external suggested principaldirection trajectories of transverse and oblique muscle masswere assumed to comprise the architectural scaffold of theintact heart by inserting couples of micrometer crystals bothin the suspected pathway, and angles opposite this directionin the same site.
In order to better describe the orientation of the differentcouples of micrometer crystal pairs, their positions weredescribed by depth and angle of line connecting them. Tomeasure the angle of the line connecting the crystals in eachpair, a local coordinate was used (Fig. 3); the aortic annuluswas the highest point and the apex the lowest, in a North andSouth fashion. Following the North and South simile,contraction at 08 was considered when both crystals wereoriented North to South, 908 East to West, 458 Southwest toNortheast and 1358 Northwest to Southeast. The interchangeof angle orientation at a specific site allowed recording of thedifferent magnitude of contraction at the same location, butwith a varied angulation. For example, an endocardiallocation can be recorded at 08 and 908 to analyze if thesecrisscross, and different fiber planes determined howforcefully paired crystals shortened relative to one another.
5. Results
5.1. Anterior wall of the left ventricle
When searching for the orientation of the micrometercrystals with highest contraction in the endocardial wall,segment shortening wasmost powerful at angles between 808and 908, reaching 17—27%, with the more extensive short-ening in the apical than the basal position (Fig. 4, traces 1 and2). In contrast, placing the crystals at 08 showed reducedcontraction segment shortening (Fig. 5). The onset ofcontraction at this anterior wall myocardial depth precedesthe systolic rise of LVP and dP/dt, and occurred between theQ and R waves of the EKG (Fig. 6). Subendocardial muscleshows two distinct rates as it shortens. First, a short andsteep descent followed by a longer and less steep contractionphase. A notch was present on this curve, and divided thesephases. The magnitude of this notch increased as crystalswere placed closer to the papillary muscle (Figs. 7 and 8). Innormal hearts, the end of endocardial contraction consis-

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S78
Fig. 3. Orientation of crystal position to define angle of contraction, which compares the silicon rubber mold of the heart to the intact heart with intact heart showingsignposts of angles for positioning.
tently coincided with the beginning the descent phase of theleft ventricular pressure, which also coincided with theappearance of the negative slope of dP/dt (Fig. 3).
At the same position (same distance from apex)subepicardial contraction averaged 12 � 2% segment short-
Fig. 4. Different segment shortening tracings of the endocardial and epicardial sites otracing) and intact ventricle (lower tracing) with position of sonomicrometer crystalssegment is superficial (solid line). (B) Segment shortening of the anterior wall of the(descending segment), compared to left ventricular pressure and dP/dt. See text for(first dotted line), and its termination after descending segment stopped (second dsegment, the start contraction of ascending segment, the stop contraction of desce
ening (Fig. 4), when the angle of crystal placement wasoriented at 150 � 108%, and placed approximately 608opposite endocardial placement. Conversely, the extent ofcontraction was 6% at a 458 angulation, so that the 908crisscross angulation between the subendocardial and
f the anterolateral left ventricle. These sites conform to (A) the model (upper. The descending segment is deep, with hatched lines, whereas the ascendingleft ventricle at subepicardial side (ascending segment) and endocardial sidedescription of events. Note the delayed start of ascending segment contractionotted line). The longitudinal lines show the start of shortening of descendingnding segment, and the stop contraction of ascending segment.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S79
Fig. 5. Example of multi-site crystal positioning, with samples taken from descending (endocardial) and ascending (epicardial) muscle segments. The maximumdisplacement orientation occurred in the regions shown in the upper two ascending segment record, and lower three descending positions.
subepicardial crystal pairs usually produced the greatestcontractile force. We observed a delay of 82 � 23 ms for theonset of subepicardial segment shortening with respect tothat of the subendocardial segment. Typically, subepicardialsegment shortening started at the maximum value of dP/dt,
Fig. 6. Comparison of simultaneous recording of tracings from the descendingand ascending segments of the apical loop, left ventricular pressure (LVP), theelectrocardiogram (EKG) and dP/dt analysis of LVP from recordings from Millarcatheters.
and finished 92 � 31 ms after subendocardial contractionsended (Fig. 4).
The extent of contraction was more intense whenthe crystal pairs were situated near the apex in both theendocardial and epicardial sides of the left ven-tricle (Fig. 9). This reflected an anisotropic contractileeffort as we compared basal and apical segment short-ening. For example, basal contraction averaged 35 � 5%less than apical contraction, and this general trend wasconsistent for both the endocardial and the epicardialmuscles.
5.2. Posterior wall of the left ventricle
In contrast to the anterior wall of the left ventricle,endocardial and epicardial sides of the posterior wallpresented near similar amount of contraction. Segmentshortening ranged 20 � 3% in the endocardial wall and18 � 3% in the epicardial one. However, the orientation ofcontraction was opposite in each side: better angle ofcontraction of the endocardial side was found at 08, while atthe epicardial side was 908 (Fig. 10). This fractionalshortening variance was most evident at the epicardial site,as the transverse, or horizontal positioning showed 19%versus 7% for vertical placement. With endocardial place-ment the vertical crystal pair showed 23% versus 17% withtransverse positioning. This continuum of contractionchanged its organized pattern when the crystal touchedthe papillary muscle with a different fiber pathway (Figs. 7and 8).
Despite these differences in the vigor of shorteningbetween endo- and epicardial sites in the posterior inferior LVwall, the starting point of contraction was similar, shown inFig. 10, a finding different from the �80 ms time delay ininitiating shortening by crisscross sites of crystal placementevident on the anterior call, shown in Fig. 3.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S80
Fig. 7. Circumferential sonomicrometer endocardial sites around the left ventricular mid wall, showing a notch in the tracings. A predominant notch occurs in thethird tracing, where there is absent coordinated shortening. These surface placement recordings (upper image, anterior view, and lower image, apical view) arecompared to internal sites shown in Fig. 10.
5.3. Right ventricle
Two main types of contraction are found in the rightventricular free wall, depending upon site of crystalplacement. In the right ventricular outflow tract beneaththe pulmonary artery, contraction pattern with an orienta-tion of 150 � 108 started later than the lateral wall, and issimilar to the epicardial side of the anterior wall of the leftventricle (Fig. 11a). This fiber orientation matches theoblique direction seen by cardiac unraveling (Fig. 11b). In therest of the free wall of the right ventricle, contraction isoriented between 100 � 58. In the lateral free wall, close tothe atrioventricular junction, contraction started at the timeof LV anterior shortening, and was more prominent when thecrystals were placed in a transverse (shortening fraction23 � 1% at 1008), compared to a vertical direction (SF%10 � 1% at 08). When crystal pairs were placed at 458,contraction was 6% (Fig. 12a and b).
Fig. 8. The endocardial sites of placement are displayed, together with evidence thdisplacement occurred by papillary muscle crystal positioning, where fiber angle di
5.4. Sequence of contraction
Contraction starts initially in the lateral free wall of theright ventricle, and simultaneously in the endocardial side ofthe antero-septal wall of the left ventricle. This observationis evident in Fig. 13, showing that the initial contraction slopeis most vigorous in the endocardial segment of the leftventricle. The initiation of this early contraction corre-sponded with the Q wave of the EKG and initial slow LVP rise,as pressure rise remained below 15 mmHg. The sequence ofevents continues after a delay of 10 � 5 ms with thecontraction of the posterior wall of the left ventricle. Thecontraction of right and posterior left ventricular, andanterior endocardial wall segments began before contractionof the rest of the myocardium resulted in the rapid ascent inventricular pressure recording that exceeded aortic diastolicpressure. Consequently, the early steep segmental short-ening of the right free wall, posterior LV and endocardial
at the location of the predominant notch, with absent recording of maximumffers from endocardial fibers.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S81
Fig. 9. These sites are in the fiber orientation plane showing maximum shortening force during probing for the best crystal angle. The descending or endocardialsegment positioning near the apex of the LV wall cone, shows evidence of more forceful shortening than sites in body of cone position. Note that both sequences ofshortening begin at the same time.
regions (Fig. 13) occurred while there was no contractiondetected in the subepicardial sites of the segments located inthe subepicardial anterior wall of the left ventricle, asreflected by Fig. 14 in the right ventricular outflow tract.
Contraction at epicardial segments began 82 � 23 msafter the initial muscle contraction (free wall of the rightventricle and the endocardial wall of the left ventricle), andcorresponded to the peak of the positive dP/dt wave, the Swave on the QRS complex of the EKG signal (Fig. 6), and mostimportantly, the steep rise (equivalent to the peak dP/dt) inleft ventricular pressure for ejection of blood. For the rest ofsystole during ejection, contraction was present in allsegments of the heart resulting in ‘co-contraction’ of bothendocardial and epicardial fibers. The initiation of contrac-tion in the subepicardial fibers was maximal in a 908 oppositedirection from endocardial ones, and coincided with areduction of the slope of contraction of the subendocardial
Fig. 10. Comparison of crystal positioning in ascending segment (optimum site angulatwall. Note (a) early and similar start of signal in the posterior wall, with more forcefuepicardial ascending segment and (b) delayed start of ascending segment shortenin
fibers (Fig. 4). Conversely, the contraction of the epicardialfibers did not change the slope of segmental contraction ofeither the lateral free wall of the right ventricle, or theposterior free wall of the left ventricle, as shown in Figs. 11—14.
We evaluated the sequential temporal and spatialrelationships between the endocardium, posterior inferiorLV wall, and epicardium, shown in Fig. 15 by comparing siteswith the angle of maximum displacement between pairs ofcrystals in these regions. This time-related course ofshortening started by displacement of endocardial muscle,followed �10 ms later by the posterior inferior wall, withinitiation �80 ms later in epicardial muscle. The anterior LVmuscle crystal angles, recording the maximal extent ofcrystal displacement, were in a superimposed crisscross (808and 1508) pattern for deep and superficial, while a similarextent of the posterior LV wall maximal shortening occurred
ion) of the anterior LV, and the vertical and transverse positions in the posteriorl shortening transverse than vertical placement, and later start of shortening ing.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S82
Fig. 11. (1) Segmental shortening in the right ventricle, showing (a) early contraction in the lateral free wall (top tracing), (b) delayed shortening in RVoutflow tract(lower tracing), that is similar to (c) epicardial segment tracing of LV ascending segment (middle tracing). (2) Image of fiber orientation of unfolded RV muscle,showing that the oblique fibers of LVascending segment proceeding, as aberrant fibers, to aorta (seen on LV) also proceed along RVoutflow tract. This is evident alongunfolded fibers going to pulmonary artery, where LV and RV vessels are separated during muscular band dissection.
in deep and superficial muscle at 908 and 08, with the samestarting time in deep and superficial sites as seen in Fig. 10.Consequently, we could use this evaluation of the super-imposed crisscross endo- and epicardial pathways todistinguish between the posterior LV and anterior LV wall,because the anterior wall showed an earlier endocardialstarting point and �80 ms delay in epicardial shortening.Conversely, the posterior wall deep and superficial fibersstarted together, about �10 ms later (Fig. 15), with theabsence of any time delay (Fig. 10) in the endocardial andepicardial regions.
As shown in Fig. 4, the first regions to stop shortening werethe segments that started first, located in the endocardialside of the antero-septal left ventricle wall, and the free wallof the right ventricle (Fig. 14), and then 10 ms later byposterior free left ventricle wall. The end of contraction forthese segments coincided with the end of the flat peak regionin the left ventricular pressure tracing, corresponding to theonset of the negative dP/dt (Fig. 4). However, the epicardialcomponent of left anterior wall and right ventricular outflowtract fibers continued their contraction phase for 92 � 33 msafter the RV free wall, posterior LV, and endocardial LVsegments ceased their contraction phase.
This extended time interval during which the epicardialsegment that continues its contraction corresponds to the so-
called ‘LV isovolumetric relaxation’ phase. In addition, thistime interval, also, overlaps the LV’s rapid pressure decreaseor otherwise known as the ‘suction’ phase (Fig. 4).
Analysis of the pressure recordings, coupled withsimultaneous analysis of regional recordings of contractionin endocardial, epicardial, lateral right ventricular andposterior left ventricular segments, shows a linkagebetween the acceleration and deceleration phases ofdeveloped pressure (i.e., the slope velocity of the pressurerecording) and regions of contraction. During the initialrapid acceleration, or isovolumetric contraction of leftventricular pressure, all segments shortened simulta-neously, whereas during the later deceleration of LVpressure, only the subepicardial segment was activelyshortening. Consequently, there was no interval of isovolu-metric relaxation.
The prolonged contraction of the anterior wall epicardialfibers during the cessation of endocardial shortening wasassociated with a reversal, or upward slope of theendocardial crystal tracing as shown in Fig. 4. Simulta-neously, the basal segments of the free posterior wall of theleft ventricle presented an increased distance betweencrystals (Figs. 14 and 16), resulting in a rapid reversal of theslope of the crystal recording during endocardial noncon-traction or relaxation (i.e., zero contraction). This separa-

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S83
Fig. 12. (a) Crystal angle orientation in RV lateral wall, showing a greater shortening if the trajectory is horizontal (upper tracing) rather than vertical (secondtracing). Early shortening is similar in lateral free wall tracings. (b) Comparison of early shortening in RV lateral free wall (upper tracing) compared to later origin(hatched line) of contraction in RV outflow tract (middle tracing) that mirrors LV epicardial segment of ascending segment (lower tracing) of apical loop.
tion or widening between crystals reached the point ofmaximum fiber stretch (i.e., separation between crystals),only surpassed by the added stretch due to ventricular fillingby atrial contraction, as shown in Fig. 4.
The relationship between contraction of endo- andepicardial segments was examined by use of infusions ofinotropes or b-blockers (Fig. 17). The time delay between thestart of contraction in the endocardial and epicardial musclesof the anterior wall of the left ventricle decreased to26 � 7 ms when dopamine at 10 mg/(kg min) was given.Simultaneously the extent of shortening increased from 25.7to 29.1% in the endocardial wall, and heart rate rose from 88to 112 beats per minute to confirm the inotropic stimulation.
In contrast, propranolol, a negative inotrope, prolonged thetime delay between initiation of contraction in endocardial,and epicardial segments to 121 � 20 ms, reduced the extentof shortening to 19%, and slowed the heart rate to 78 beatsper minute.
This pharmacologic prolongation, induced by propranolol,increased phase separation of the onset of contractionbetween the endocardial and epicardial segments. There wasalso an associated prolongation of the duration of theendocardial contraction. Thus, the interval or hiatus ofseparation shortened between the ends of endocardialcontraction with ongoing epicardial contraction. The phasictime frame for end of contraction of endocardial and

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S84
Fig. 13. Comparison of early segmental shortening of the three components contributing to the isometric phase of contraction, that includes (a) RV lateral wall (toptracing), (b) a 0.10 ms delay (hatched line) at the onset of posterior basal loop LV freewall (second tracing), and (c) a combined rapid and slower phase of shortening indescending (endocardial) segment of LV wall.
epicardial fibers occurred at a closer interval (in contrast tothe prolongation existing during the rapid ascent of the leftventricular pressure curve), so that there was prolongation ofthe slope of the rapid descent of the left ventricular pressurecurve.
5.5. Negligible movement of the apex
When a pair of crystals was positioned close to one anotherat the point of the apex (Fig. 18), we found irregular, butnoneffective contraction. The selected but noneffective
Fig. 14. Sequential contraction of the basal loop, showing (a) a widening between crfree wall segments, of the horizontal basal loop, and (b) later onset of initiation and pfor description.
shortening sites were adjacent and 1 cm apart, to includelocations either toward or away from the septum, or in deepor superficial placement to evaluate endocardial andepicardial fibers. This positioning could not measure rotationof the apex.
5.6. Abnormal contractile movement of apex, with moredistal fiber placement
A different pattern appeared when one crystal was placedinto the tip of apex, with the other inserted into muscle (at a
ystals (with upward trajectory) after completion of shortening of the RV and LVersistent shortening of RV outflow tract during widening of basal loop. See text

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S85
Fig. 15. Simultaneous tracings of the posterior and inferior LV wall (top tracing), and anterior epicardial (middle tracing) and anterior endocardial segments (lowertracing). Note (a) earliest onset of shortening (solid line) in descending endocardial segment, (b) 10 ms delay (doted line) in onset of shortening in posterior, inferior LVwall and (c) longer delay in onset (hatched line), together with ongoing shortening in ascending (epicardial) area after descending and posterior shortening stops.
greater distance of 2—3 cm from the apex) that hadpreviously shown a contractile pattern (Fig. 19). The secondmuscular crystal placement sites (distant from apex)evaluated deep subendocardial and more superficial epicar-dial positions.
These tracings, defined in Fig. 20a, showed absence of theexpected endocardial pattern sequence consistently presentin themidwall (Figs. 4 and 19). The normal starting point thatpreviously coincided with the beginning of ventricularpressure rise, shifted to the (�80 ms) starting point of theepicardial fibers. However, this endocardial contractionended normally, with termination �90 ms before theexpected completion of the epicardial fiber contraction.Similarly, the expected epicardial contractile patternsequence reflected reverse mirroring of the endocardialpattern. Contraction began �80 ms earlier, resemblinginitiation of endocardial placed crystals in other studies,with a normal completion point, typically �90 ms later than
Fig. 16. Comparison between early shortening of posterior basal loop free wall (top)trajectory) in LV free wall, while their ongoing shortening and downward trajectory colines. This widening event transpires during the phase of deceleration of LV pressur
the stoppage point of endocardial crystals. Consequently, aparadox exists when an apex tip becomes the one placementpoint and normally contracting muscle becomes the other;the endocardial contractile pattern becomes�80 ms shorter,and the epicardial pattern becomes �90 ms longer than inexpected sequences without an apical tip starting site.
6. Discussion
The intent of this study was to use sonomicrometercrystals with high temporal and spatial resolutions [21,22] todetermine if the timing and maximum extent of shorteningbetween crystal probes relates to the principal fiber pathwayorientation suggested by Torrent-Guasp’s helical heart model[8,20,23]. We explored the relationship of how these twodimensional devices could identify function in the underlyingthree dimensional muscle, which comprises an oblique
and ascending (epicardial) LV free wall. Note the widening of crystals (upwardntinues in LVepicardial muscle, shown by distance between dotted and hatchede associated with the isovolumetric period.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S86
Fig. 17. Sequence of contraction of different segments during a study in one subject during (a) basal conditions (top) and with dopamine (middle) or propranololinfusion (bottom). Black and hatched lines mark the start and end of shortening of endocardial and epicardial muscle, respectively. There is a delay between start ofthe endocardial and the epicardial myocardia of the anterior wall that decreases with dopamine from 84 � 10 ms to 26 � 7 ms and increases with propranolol to121 � 20 ms. The termination of endocardial shortening is prolonged with propranolol to (a) reduce the separation during baseline, and (b) associated with a fall inthe downslope of the LV pressure tracing.
double helix called the apical loop, that is surrounded by atransverse basal loop acting like a buttress covering thedouble spiral endocardial and epicardial apical components.
The crystal dimension gauges provide a local view of aglobal concept, exploring all cardiac regions, by probing howthe maximal extent of fiber shortening in preferentialpathways is governed by the orientation between couplesof these crystals. These local barometers do not measureeither thickening [21,24], twisting [10,11], torsion[12,25,26], cross fiber shearing forces [21,22], or inceptionof the calcium trigger of contraction [27,28]. These localshortening measurements are influenced by transmuralshearing forces, yet they do reflect how deformation fromposition orientation receives substantial interactions fromneighboring fibers. Consequently, each change in time-related regional function comprises how three-dimensionalspatial architecture alters function within the ventricularwall. The consequence of unraveling the functional implica-tions of a novel architectural pattern, is that, if correct, alinking will exist during conventional hemodynamic measure-ments, between the electrical signal, formation of upslope
Fig. 18. Recordings at the endocardial and epicardial regions of LV apex, with crystalsthat does not resemble tracings obtained in all other regions of the LV as shown in
and downslope of ventricular pressure waves, and rate ofmaximal acceleration and deceleration of these standardsignals.
Distinction between each of the varied factors thatinfluence the term ‘contractility’ is not the intent of thismanuscript, since no effort wasmade tomeasure deformation[24,29], as it influences strain of the cross fiber or transmuralshearing forces [22,29] that may result in a motion that maynot be aligned with local myofibers. However, such measure-mentsweremadeby others [30], wherefindings of shear stressand torsion that is maximal in the endocardial and approxi-mately twice [16,30,31] that of the epicardial region, ismatched and consistentwith themaximal extent of shorteningduring our comparisons of displacement between couples ofcrystals. Additionally, our observation of the anisotropicshortening showing the heterogeneous contractile action ofboth endocardial andepicardial regions, that increases towardtheapex, compares favorablywith tagging-relatedMRI reportsof deformation [30].
Consequently, despite the limitations of the crystals usedfor sonomicrometric measurements, these local records take
placed closely together, and tracings showing an irregular, nonuniform patternFig. 21, when crystals are placed in a nonapical, slightly higher position.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S87
Fig. 19. Simultaneous recordings of tracings 2 cm above the LV apex, showing the typical recordings of tracings obtained in the maximal fiber direction of theascending and descending, epicardial and endocardial muscles. Note the (a) earlier origin and termination of contraction in the descending segment, (b) similarstarting point for RV contraction, and (c) later origin and end of shortening in the ascending segment.
Fig. 20. (a) Simultaneous tracings of recordings obtained by one crystal in the tip of the apex, and the other in either the endocardium or epicardium of the upper LV.These crystals were placed either medially or laterally in the upper LV wall. Note that (a) the ascending (epicardial) segment starts early and ends at the normal latertime frame, while (b) the descending (endocardial) site starts late and ends at the expected early time interval. These starting and stopping intervals, marked by solidlines for the descending segment, and hatched lines for ascending segment, can be compared to the tracings in Fig. 19, showing the proper intervals. (b) The helicalconfiguration is shown on the left, and the right image of the apex is expanded to show the crystals that are placed at apex, and then inserted either deeply into thedescending segment or superficially into the ascending segment. These are the positions responsible for generating the sonomicrometer tracings shown in (a).

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S88
Fig. 21. The successive stages of unwinding of the ventricular myocardial band are compared to the rope model. The intact heart is the normal position in (A), and (E)shows the unfolded heart where the band is fully extended. The text provides a description of these segments.
maximal advantage of their temporal and spatial resolutionthat we recognize is also influenced by the overlying crossfiber strain and shearing forces of the inner and outer halvesof the ventricular wall. The point of maximal directionalshortening or widening of opposing crystal pairs defines thecomposite geometric action of the either overlying orunderlying ventricular muscle mass containing natural crossfiber connections. The centerpiece of this shorteningobservation is that the location where opposing crystalsshow maximum reduction of distance between them is atright angles to their angle of placement [22]. We suspect thatthe perpendicular angular shortening of a spring within eachprincipal fiber pathway may become a clear example of thisaction, whereby limited shortening follows analyzing thecross-sectional site, with amajor vector developing along theprincipal direction.
The study tested several factors, and these includeddefining the correct angle orientation between crystals ateach site to determine maximal displacement. Eachventricular site was selected to determine if the principalfiber course shown in the unraveled heart described inFigs. 1, 21 and 22, and on video on http://www.gharib.cal-tech.edu/�heart/, could, when refolded into the intact
muscle, reflect a consistency with (a) known anatomy, (b)the recognized course of the Purkinje electrical cablesystem, and (c) simultaneously follow the novelmodel of theventricular band. After pairs of probes within a spatialconfiguration that selected the point of maximum displace-ment at regions within basal and apical loops were tested,we then evaluated if a sequence of time and position relatedforce displacement was consistent with progression of thecontractile wave around the unrolled rope by a trajectorymoving from right to left in the basal loop, and then down thedescending and up the ascending segments of the apicalloop.
Clearly, any deviation from this expected sequencereflects either (a) an error in the model or (b) failure totake the conduction system into account. We determined ifan anisotropic increment in contractile force followed theelliptical shape of the ventricular chamber, and alsoevaluated if these sequential contractions relate to inter-action of calcium dynamics with the myocardial massconfronted with either positive or negative inotropicinfluences by dopamine or propanalol. Finally, we definedhow (a) the apex itself, that visibly rotates, contributes tonormal contractile force since it forms the tip or vortex of the

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S89
Fig. 22. Unscrolling of the myocardial band, whereby the intact heart isunwrapped in (e) to define the stretched out band. Note the oblique fold inthe center of the band that separates the basal and apical loops. Note also (1)the transverse fiber orientation in the basal loop in (b—e); (2) the helix of theapical loop contains oblique fibers, with an apical reciprocal spiral as shown in(c); and (3) the twisting nature of the helix at the junction of the basal andapical loop.
double helix, and (b) how the apical tip of the ventricularhelical coil becomes influenced by the principal fiberdirection actions of the distant endocardial or epicardialcomponents whose overlapping forms the helix producingthis conical tip.
6.1. Sonomicrometer evidence for the myocardial band
6.1.1. Identification for the proper contraction angleThe angle defining the maximum contraction between
crystal gauges conformed closely with themain fiber pathwayevident on the helical model. In every instance the maximalextent of contraction was in a direction perpendicular toevident macroscopic direction. For example, epicardial fibershortening was greatest 12% at 1358 angle, with crystalsmoving closer together at this angulation, with markedlydiminished contraction of 6% at 458. The more extensiveendocardial vs. epicardial shortening (20% vs 12%) shown bycrystal sonomicrometer of the anterior LV free wallintroduces data consistent with measurements in MRIrecordings [30,31]. Furthermore, the extent of shorteningdiminished in each area as crystal placement was made at offangles to the probed site of maximal force of shorteningselected from the model. Of course, the points of bothmaximal and minimal crystal displacement varied indifferent regions, as we segmentally probed the intact heartto search for the underlying scaffolding that may uncoverprincipal and preferential fiber pathways.
6.2. Anterior left ventricle
In the anterior LV free wall, the crisscross nature definingthe most active sites supported the suspicion of dualunderlying descending and ascending segments. Of criticalimportance is the time-related difference in both appear-ance and end of contraction, showing a �80 ms delaybetween the origin of endocardial versus epicardial short-ening. The counterpoint to these observations is a similar�90 ms delay between end of endocardial and ongoingepicardial contraction. The timing and spatial shorteningmeasurements find a functional counterpart in LV pressuretracings and dP/dt events related to rapid ventricular fillingdescribed in Fig. 6, and summarized in the Section 5. Thesecrystal observations are consistent with the ventricularrotational movements reported by McDonald [32], suggestingassociation with early activation and contraction of endo-cardium, with later contraction and persistence of epicardialcontraction.
Aside from the temporal and maximum displacement forcontraction, codified by the downslope of the crystalrecordings of the deep and superficial muscle, an upslope(or widening between endocardial crystals) developed duringthe interval between cessation of deep shortening of ongoingascending shortening. This stretching is consistent with theslight epicardial lengthening observed by Rademakers [10]during what he termed ‘isovolumetric relaxation’. Wesuspect Rademaker’s epicadial observation reflects howthe widened endocardial region causes transmural transmis-sion to overlying surface muscle.
6.3. Circumferential studies
One alternate avenue included crystal placement aroundthe circumferential perimeter of the left ventricle, where wedid not search for the principal pathway directly, but probeda cross-sectional region to try to search for interactionbetween sites, in a manner similar to transverse heartsections evaluated by MRI [33] or echocardiography [34]. Weuncovered one site that showed an area of negligible overallcontraction, but developed an augmentation of the notch inthe slope of the endocardial recordings made throughout theanterior left ventricle. This region matched the point ofcontraction of the papillary muscle proven at autopsy (Figs. 6and 7) where papillary muscle fibers move in a differentdirection compared to free wall fibers. This structural findingthus accounts for the sudden loss or the expected normallygraded contraction seen in Figs. 7 and 9. Simultaneously,normal contraction persisted in the overlying epicardialmuscle where visible fibers are more transverse [35].
6.4. Posterior wall
Placement of crystals in the posterior wall defined theabsence of two overlying layers, due to early and similarorigin time of contraction. In this posterior location, theinner descending segment wraps around to form the apex andrise to become the ascending segments shown in Figs. 1 and11, thereby removing the concept of two layer super-imposition (as exists in the anterior LV free wall) to provide afunctional equivalent to the single principal pathway evident

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S90
in the myocardial band dissection (Fig. 1). A tracing of thestructural sequence of ventricular band allowed simulta-neous recording of shortening in the descending, posterior,and ascending regions (shown in Fig. 15) where a simulta-neous timing sequence of contraction of the wrapped bandbecame evident with the earliest shortening in thedescending segment, slightly later in the posterior muscle,and latest in the ascending segment. Further study of theposterior wall confirmed the predominant maximal contrac-tion in the transverse direction, thereby following theevident visible fiber direction, with lesser contraction whenthe vertical angle was used (shown in Fig. 10). This transversevector identifies the predominant pathway of the super-imposed overlapping fibers, the posterior wall [as shown inthe fiber strand peel off technique (SPOT)], and ‘shingle roof’undercrossing of subjacent fibers described by Lunkenheimerand co-workers [23,36]. Such transverse principal directionof contractile shortening in the inferior posterior LV providesa functional equivalent to the principal circumferentialstructural fibers described by Greenbaum [37] in anatomicpostmortem dissections. Perhaps the crisscross extent ofdisplacement reflects the spring-like twisting within a singlepredominant pathway, thus contributing to the deformationseen by MRI and regional studies.
6.5. Right ventricle
Thedifference in timing and angle of temporal and spatialshortening in the RV free wall and outflow tract preciselyfollowed the model; the lateral RV wall shortened simulta-neously with the descending segment of the left ventricle,and RV outflow tract shortening was consistent with theascending segment of the apical loop. The circumferentialnature of fiber direction in the lateral free wall was alsoconfirmed by the more effective shortening within thetransverse predominant fiber course in the lateral RVfree wall of the RV, with lesser shortening evident aftervertical crystal placement as shown in Fig. 12a. This earlyshortening pattern would favor a constrictive motion duringthe isometric phase of systole that precedes ventricularejection.
We confirmed evidence of the aberrant fibers [9] runningover the RV outflow tract, originating from the LV obliqueascending segment, by finding a delay in the beginning of theshortening signal In the RV anterior and lateral walls. Theanterior RV delay precisely paralleled the later origin at theLV free wall shortening, shown in Fig. 12a, with anatomicconfirmation defined in Figs. 2 and 11b showing to the obliquecourse of the aberrant fibers that jump onto the rightventricle from the anterior left ventricle. These fibers thenfollow a similar course within the deep and superficialtrajectories along the pulmonary artery outflow tract. Theoblique nature of the fiber orientation would be consistentwith a later twisting motion during ejection.
6.6. Basal loop during late ventricular isovolumetriccontraction
Additional functional information was provided by widen-ing of the right and posterior LV free wall basal loop crystals(Figs. 14 and 16) during the hiatus of ongoing ascending
segment shortening responsible for suction generated rapidventricular filling. This widening between outer rim basalloop crystals implies a stretching of noncontracting muscleduring the presumed reciprocal clockwise direction twisting,as the ventricle prepares to suck blood into its cavity duringisovolumetric systolic contraction. This stretch and wideningbetween crystals is also clear in Fig. 4, where we presume thenoncontracting stiff endocardial fibers are pulled apartduring the active ongoing contraction during continuingascending segment shortening.
6.7. The conical ventricle
The anisotropic quality of heterogeneous contraction ofdifferent regions is evident from MRI recordings [16,30],where the force vector of contraction increases as segmentsare followed from base to apex. Our crystal recordings lookedat both endocardial and epicardial regions, and confirmedthis improved shortening as we moved towards the ellipticalchamber apex, with 35% reduced contraction when basalendocardial segment bases were compared to the near apicalrecords (shown in Fig. 9). The dynamic change in MRI tracingscompare the base and apex to define increased strain anddeformation as the radius of curvature narrows and theextent of intracavitary thickening increases towards the tipof the conical chamber [22,24].
Our studies did not measure clockwise or counterclock-wise rotation but the sequence of initial contraction of theright, then the left circumferential basal loop regions wouldproduce the slight clockwise rotation, described initially byprior vector analysis by Coghlan and coworkers [38], recentMRI studies [33], and characterized as ‘cocking of the heart’in the comprehensive reports by Ingels and co-workers[26,39,40]. This clockwise basal loop motion precedes thepredominant counter clockwise twist responsible for ven-tricular shortening during ejection. Our analysis indicatesthat the shortening caused by subsequent endocardial andthen co-contraction of both descending and ascendingsegments of the oblique helical apical loop will shortenthe heart by pulling downward the attached basal loop. Thiscounterclockwise pathway is evident on MRI [10,11] andother twisting analysis defining torsion of the macroscopicheart [41] as it twists during ventricular ejection.
6.8. The apex
Visualization of the apex shows that it rotates, as it isformed by the vortex of the criss-crossing descending andascending segments. Anatomically, it is thin at cross-sectionalobservation [9,42]. Placement of a crystal at the apex withconnection to the second of these couples at adjacent deep ofsuperficial muscle showed only an irregular contraction(shown in Fig. 18). These movements were consistent, thusoccurring with and without the Millar catheter in the apex, tothereby exclude a traumatic cause for these movements.Moreover, the contour of this contraction was ineffective, andthe pattern did not reflect tracings gathered from the othersegments. We could only interpret this record to confirmexistence of some motion that varied markedly from theconsistent and coordinated contractile scheme evident fromall three angular patterns in nonapical regions (Fig. 4).

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S91
This regional evaluation of only the apex, rather than howit interacts with other distal regions, may follow prior studiesof apical rotation done by placing only one isolated probethat is restricted to studying the tip region alone [43,44]. Weamended this isolation by selecting two points, but limitedour analysis to closely adjacent regions. These local measuresdefined irregular shortening patterns in the tip, and set thestage to determine how the tip of the helix interacts with thesegments that form the apical tip. These include the inside-out wrap of the functional descending segment, and theoutside-in wrap of the ascending segments [45—47].
An unusual pattern was seen in Fig. 20a when one crystalwas placed into the apical tip, and then connected to asecond distal crystal attached to functional endocardial orepicardial muscle. These functional observations contradictexpected patterns from nontip connected endocardial orepicardial recordings shown in Fig. 4. Each apical tracingshowed insights of how the nonefficient contractile apexbecame influenced by attachment to the descending andascending segments whose inside-out and outside-in vortexforms the cone tip. The apical recording connected to theactive descending segment started at�80 ms later time thanepicardium initiation, and ended normally, approximately�90 ms before completion of the ascending segment short-ening. Conversely, the apical tip to the ascending segmentstarted �80 ms early, at precisely the time of expected earlystart of the descending segment, but ended normally�90 msafter the descending segment stopped.
We suspect how these tracings illustrate the helical coil ofthe apex, formed by these segments, and influenced byreciprocal shortening of the two components that create theventricular tip (as shown in Fig. 20b). Perhaps thesecontractile changes reflect the transition point, whereopposing contractile forces nullify each other, and producethe evident rotation. With the apex and descending segment,rotation was clockwise due to the pull of the ascendingsegment on the apex, with the normal completion due to thecorrect position of the distal endocardial crystal. Conversely,with the apex and ascending segment, the early start is dueto the early pull of the descending segment in a counter-clockwise direction, coupled with a normal ending point,�80 ms beyond expected descending segment stoppage ofcontraction. We believe the apex thus rotates due to how theopposing segments effect the helix, and this pattern is onlyvisible when one of the crystals is placed into the rotating,but noneffective contracting apex, while the other is in acorrect position in either deep or superficial descending orascending muscle can be shortened considerably.
6.9. Implications of myocardial band analysis
The first concept that is forthcoming from the dataanalysis is that systolic contraction exists both during thephase of ejection, and during the time-related periodpreviously termed as isovolumetric relaxation. This intervalcoincides with the rapid deceleration of ventricular pressurethought previously to reflect elastic recoil from isovolumetricrelaxation related to potential energy stored during thesystolic contraction [10,48—52] but is produced by ongoingcontraction of the epicardial muscle forming ascendingsegment. This muscle continues to shorten beyond the end
contraction phase of the endocardial muscle forming thedescending segment. Consequently, a contractile phaseexists throughout LV pressure acceleration during systolicejection as well as during the early LV pressure decelerationthat precedes the time of rapid filling.
Review of the pressure, dP/dt, and sonomicrometertracings in Figs. 4 and 15 defines three contractile phasesresponsible for (a) isovolumetric contraction prior toejection, (b) contraction and co-contraction for ejection,and (c) contraction for early rapid filling. These muscularshortenings for systolic action during both ejection and rapidfilling will involve a shortening wave in each of the segmentsof the basal and apical loops, but our findings contradict (a)the concept of longitudinal progression along the sequentialfour segments of the band, i.e., right to left in basal loop,then descending followed by ascending in the apical loop[7,9,17,18], and (b) the prevailing notion that elastic recoilfrom stored potential energy from systole is responsible forthe isovolumetric relaxation that generates suction for rapidfilling [10].
Crystal shortening follows changes in wall motion withoutreference to electrical events, and analysis of these temporaland spatial findings that comprise the data must includeinsight into (a) connections of the electric cable system forthe Purkinje neural penetration distribution, (b) myocardialspread of impulses to fibers in relation to muscle thicknessalong themyocardial band, and (c) a concept of matching theelectric and mechanical interaction along the visiblesequential muscular segments progressing through theunfolded, then rewrapped band. This matching of theelectrically defined depolarization and repolarization mustthen be correlated with the evidence of ongoing contractionduring the period of repolarization, since a contractile efforttakes place during the entire QRS and T waves on the EKG.Clearly, an explosion of electricity comprises the QRSpattern, but ongoing contraction is evident during theelectrical interval of repolarization as the Twave appears, sothat a more complete understanding of excitation—contrac-tion linking is essential.
The genesis of ventricular contraction during the isovolu-metric contraction phase of systole shows that shorteningbegins immediately after the Q wave on the EKG, andinvolves both left ventricular endocardial the right lateralfree wall fibers, to be followed�10 ms later with LV posteriorcontraction in the distribution of the basal loop. These threesegments contract before the rapid acceleration of LVpressure for ejection. The predominant force becomescircumferential compression, thereby explaining the �25%narrowing of the mitral valve annulus during the isovolu-metric contraction that precedes ventricular emptying, asdefined by Shah and co-workers [53]. Contraction of theepicardial segment follows �80 ms later, and correlates withthe rapid acceleration of pressure, the peak of the positivedP/dt and the end of the QRS complex.
Consequently, isovolumetric contraction involves onlythree segments, while the rapid ascent of pressure forejection involves all four segments, bringing into play thelater contribution of the epicardial or ascending segment.Based upon the direction of crystals, we think that the RVand posterior LV basal loop shortenings are dominant atthe initiation of contraction, and cause compression and

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S92
narrowing of the chamber. The oblique squeeze of theendocardial segment initiates the twisting responsible forejection with shortening of the cavity, due to an initiation ofthe torsion-like counterclockwise twisting, or wringing of atowel or with a wine press, as suggested by Borrelli [41] in1660, and now codified by noninvasive MRI recordings withtagging studies [10,11,33]. The downward movement of theventricle during this later phase of ejection implies that theendocardial or descending segment muscle carries thedominant force during contraction for ejection.
With consideration of only the rope model, this contrac-tile phase sequence defeats Torrent-Guasp’s concept ofprogression of contraction sequentially along the visiblemyocardial band [8,9,17,24,38,54], since endocardial con-traction would be expected to begin after the left posteriorLV contraction. There must be a matching with nerve andmuscle anatomy, since the earliest muscle contact of thePurkinje penetration is via the massive fan type neuraldistribution described by Tawara [55] that directly touchesendocardial fibers. Sodi-Pallares and Calder [56] and Lewis
Fig. 23. Chronologic sequence of contraction of both segments of the apical loop as rarea) is already shortening. In (A) the descending segment contracts first, to begin ejecshortly after descending segment contraction, the ascending segment starts to shdirections to shorten the ventricle for the rest of ejection. In (C) when the descendisegment continues shortening to begin to lengthen the ventricle at the start of the
et al. [57,58] have described this early activation ofendocardial muscle that is translated into immediatecontraction.
We suspect there is a delay between the initial excitationof endocardial fibers in a direct neural myocyte connection,and the later contraction of fibers in the thicker endocardialmuscle mass that does not have Purkinje cells touching eachfiber, and thus must get its excitation by transmission via amatrix transmission [59]. We know from the studies byDelhaas et al. [60] that transient ischemia does not alter theQRS interval during reperfusion, but slows the transmuralcontraction scheme, presumably by slowing the conductionpathway through the muscle. Further testing of this matrixconcept is needed in the normal heart to define therelationship of spread of the impulse for contraction of thewall.
The early rapid downslope of the crystal recordmay definehow the obliquely oriented fibers have a more forcefulcontraction, as postulated by Sallin [61], while the lesserslope in the free wall of the RV may reflect reduced force by
ecorded by sonomicrometer crystals. The basal loop (circumferential darkenedtion (first solid longitudinal line), while the ascending segment is relaxed. In (B)orten (hatched line) to reflect both segments ‘co-contraction’ in reciprocalng segment reaches its maximal contraction (second solid line), the ascendingisovolumetric contractile phase, which stops at the dotted line.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S93
the transverse fibers, whose maximal circumferential courseis codified by the alignment of transverse crystal anglesduring RV recording (Fig. 11a and 12a). These mechanicalobservations may help explain why the predominant fiberangle orientation may allow the 15% shortening found inisolated fibers without scaffolding connections, to change asthey exist in the wrapped heart with scaffolded spatialarchitecture, to show more forceful shortening (i.e., 60%)when predominant fiber orientation is oblique, rather thantransverse (i.e., 30%), as exists in the predominant pathwaysof fibers comprising the two segments of the apical and basalloops [61,62].
Another gap in conventional thinking is the evidence ofearly contraction of the entire base of the heart beforeejection occurs. This separation between basal contractionbefore papillary muscle shortening for rapid ejection startswas reported by Armour and Randall [63] in 1970, whoconfirmed the work of Roy and Adami [64] in 1890. Our datasupports the concept of Armour and Randall that the base ofthe heart forms a stiff outer shell around the bulk ofmyocardium (really the endocardial and epicardial ordescending and ascending regions of the apical loop)responsible for ejection. Armour documented the laterstimulation of the base, as also shown by Sodi-Pallares andCalder [56], who confirmed a ‘mismatch’ in excitation—contraction coupling.
We have recently [17,18,59] considered this concept, andour observations support the work of Robb and Robb [65], thatcorrelates the axial flow spread of the impulse along the fiberbundles, with more rapid transmission along thinner thanthicker fibers. Consequently, the more slender RV and LV freewall basal loop segments shortenmorequickly than the thickerpapillary muscle and outer LV wall. We suspect that excitationimpulse spreads through a matrix system [59] along these finefibrous sheaths that extend from the termination of thePurkinje conduction fibers to escape and interweave with
Fig. 24. Simultaneous tracings of the ascending and descending segments of the apicaland during reperfusion (right column). Note the (a) separation between end of descesegments during ischemia, and (c) propagation of systolic contraction to allow matcduring reperfusion.
muscle fibers beyond the transition between conduction tissueand the remaining working myocardium.
These observations thereby also contradict the concept oftransmission of the contraction wave impulse from the innerto the outer wall, since the direct penetration of the Purkinjefibers extends only to inner wall muscle. Clearly, conductionalong cell—cell via low resistance gap junctions, at amaximum velocity of 0.3 mm/ms could not occur along the80 mmdescending segment, and 130 mmascending segment,since 433 ms would be needed in the epicardium to completeactivation [59]. The beginning of excitation of most fibersthat enter into contraction is only �105 ms, and only �80 msin this study. Most likely the impulse transmission spreadsalong spiral pathways, as suggested by Taccardi et al. [66,67]to explain the spread of activation beyond the superficialPurkinje network.
The endocardial very rapid shortening phase becomes lesssteep with the onset of shortening of the oppositely directedepicardial or ascending segment. Consequently, there is then‘co-contraction’ of all areas (including the basal loop rightventricle and posterior LV, and endocardial and epicardial, ordescending and ascending segments of the apical loop) duringejection. The crystals when paced in a crisscross mannerdefined maximal shortening force along principal fiberpathways but did not measure the torsion confirmed byMRI [10] and in isolated segment recordings by Ingels et al.[26] and Beyar et al. [48,49]. We suspect the change in slopeof the crystal tracing during co-contraction reflects theoblique and clockwise counterforce and dominant counter-clockwise twist of the descending segment (shown in Fig. 23)that becomes opposed by the reciprocal twisting of theascending segment in a different direction. This reciprocalforce may become unleashed when there is cessation ofdescending segment active contraction, so the reciprocallytwisting ascending segment can then predominate andproduce the clockwise twisting so characteristic of abrupt
loop during control (left column), (a) 15-min ischemic interval (middle column)nding and ascending shortening during baseline at control, (b) bulging of bothhing of the time frames of shortening in endocardial and epicardial segments

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S94
Fig. 25. (a) This diagram is taken from the 1760 text of Senac, showing hisconception of the cardiac internal helical formation. (b) This apical view of theheart, from Mall’s text in 1911 [83], shows the reciprocal spiral arrangement offibers, moving from the epicardium to within the chamber from the surface,and how internal fibers emerge from the endocardium to wrap around theepicardial surface.
lengthening during rapid ventricular filling described in thefollowing sections.
The final phase of contraction relates to the hiatusbetween loss of contraction in the RV, posterior LV andendocardial or descending segment records, and ongoingcontraction in the epicardial or ascending segment. This timeinterval is linked to the deceleration of LV pressure and theonset of the negative phase of dP/dt recording. Conse-quently, there is an active period of epicardial or ascendingcontraction during the period previously termed isovolu-metric relaxation. A more precise term is late isovolumetriccontraction [17,18]. Fig. 23 displays the theme for dominantinteraction between endocardial and epicardial segmentsand directional displacement.
This active and ongoing epicardial systolic muscularshortening after active endocardial or descending systolicshortening has stopped, specifically contradicts the conceptthat the rapid descent of pressure, and negative dP/dt isfrom recoil of stored potential energy [48,68—72], sincesystole persists [17,18]. This contractile cause differs fromthe interaction between the contracting myofilaments andelastic collagen surrounding the muscle fibers [48]. As aproposed mechanism for lengthening, we suspect thatdespite completion of active endocardial contraction inthe descending segment, tension persists in this muscle,allowing it to act as a fulcrum [17,18] for ascent of theventricle during the rapid filling phase [73]. We believe thisongoing twist of epicardial muscle, occurring in an oppositedirection from the endocardium or descending region, makesthis contractile effort govern the rapid clockwise rotationseen by MRI [33] during lengthening during rapid filling.
This active contractile role was also suggested byRademakers and co-workers [10,11] by MRI studies, definingthat 50% of filling develops during this time frame, andaccentuation of speed and rate untwisting (or reciprocaltwisting in a reverse direction) for rapid filling by can beincreased by inotropic drug infusion. Brutsaert and co-workers [27,28,74] further amended the infrastructure forrapid filling by a suggesting contractile phase of systole. Ourfindings tested this concept with sonomicrometer crystals,and characterized the role of calcium dynamics in thisprocess by infusion with dopamine or propranolol. Thenegative inotropic effect of propranolol, aside from reducingpressure and heart rate, widened the onset of contraction ofthe epicardium versus the contraction of the endocardium tothereby slow ejection, while simultaneously narrowing thehiatus for rapid filling, by decreasing the time frame forotherwise unbridled epicardial contraction while the remain-der of the chamber muscle was not contracting. The resultwas a delay or prolongation of the downslope of LV pressureand less negative dP/dt. Clearly, further advancement of thestoppage of the endocardial contraction relative to theongoing epicardial shortening will increasingly compromisethe contractile forces responsible for rapid filling and derailthe mechanisms for suction, so that pressure, rather thatmuscle motion now becomes the principal filling determi-nant. The consequence is that these tracings introduce acontractile mechanism that both contributes to suction fillingin the normal heart, and more importantly implies that whenthis action becomes disrupted, a contractile cause fordiastolic dysfunction may prevail.
Evidence for this prolongation of late systole in heartswith diastolic dysfunction is evident in studies of stunning(Fig. 24) after ischemia [75—77], hypertrophy during aorticstenosis [78], posttransplant dilatation [79], and tachycar-dia-induced cardiomyopathy [40]. Our findings show that thisis an active phenomena, related to loss of the critical gapbetween stoppage of shortening in the circumferential andendocardial region, and ongoing contraction of the epicardialor ascending segment. The pertinent MRI findings that wouldsupport this concept is that there is loss of the normal actionof rapid ascent of the muscle, so that vigorous shortening andrapid lengthening becomes replaced by a lesser lengthdistance of movement, and slower return to the normaldiastolic filling position.
6.10. The integrated cardiac spiral
The reciprocal spiral pattern is heralded by the macro-scopic double helical cardiac form defining the ascending anddescending loops, and interface with the collagen weave-like

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S95
Fig. 26. Natural coils within coils in a ram like animal (eland) in upper image. Note (a) the external reciprocal spirals of the horns, and (b) how the strength of eachhorn is created by the occurrence of internal spirals within this external spiral scaffold. This double spiral arrangements amplified in the lower tracings of the apicalloop, colored white, that reflects how the descending and ascending segments of the apical loop interact for ejection and suction. These segments are in repose indiastole in A, Note in B, that during the initiation of ejection, the descending loop becomes dominant and shortens from base to apex, while this motion stretches theascending segment. The later contraction of the ascending segment will initially cause co-contraction, and then will lengthen the chamber in C while thenoncontracting descending segment stops contraction and retains tension to act as a fulcrum for lengthening.
structure forming the connective tissue scaffold for thismuscle mass [80]. A similar dual helicoid configuration existsmicroscopically in myosin, actin, tropomyosin, and confo-cally in the coil arrangement in calcium distribution within asingle cell, as well as the coil arrangement within a singlecalcium ion [81]. The helical cardiac formation is well knownanatomically, with Senec describing the internal helix (shownin Fig. 25a) from his text in 1760 [82,83], Pettigrew describingthe apex (shown in Fig. 25b) to contain reciprocal spirals withthe epicardium going from without to within, and theendocardium going from within to without [82]. This spatialanalysis also provides a functional confirmation to theobservations of Lower [84], in 1669, who described musclefibers of the inner wall that ran opposite the fibers of theouter wall, and that contraction can be compared ‘. . . to thewringing of a cloth to squeeze out the water’. Our functionalanalysis shows that the lengthening is due to the reciprocaltwist of the outer wall fibers that continue to contract afterthe inner wall fibers stop in the normal heart.
We suspect the heart borrows a trick from nature, wherethe reciprocal spiral horns of a ram or eland, gain internalstrength from the internal spring-like coil arrangement. Forthese reasons, the arrangement shown in Fig. 26a and b[17,18,85] may reflect the cardiac spiral within spiralarrangement. The spatial arrangements of these coils mayalso help explain why a muscle can contract and shorten, yetlengthen its longitudinal position when we consider theascending segment. This role of contraction of a spring withina spring, like coils within coils, connected in a helical mannerintroduces some insight into how a muscle can both contractand lengthen. Review of Fig. 26b shows how the noncon-tracting ascending segment may become stretched during
the beginning of descending segment contraction and how bysubsequent wringing can both shorten the distance betweenindividual springs, yet lengthen due to its spatial helicalorientation.
This spatial configuration parallels the structure of DNAwhere this recipe for an interweaving spiral configuration isplanned. If this concept is correct, the natural framework forour search into understanding has been mapped before ourarrival, and our task is find the new helical pathways requiredfor us to understand novel mechanisms to explain ourfunctional observations in the living heart.
References
[1] LeGrice IJ, Smaill BH, Chai LZ, Edgar SG, Gavin JB, Hunter PJ. Laminarstructure of the heart: ventricular myocyte arrangement and connectivetissue architecture in the dog. Am J Physiol 1995;269:H571—82.
[2] Spotnitz HM, Spotnitz WD, Cottrell TS, Spiro D, Sonnenblick EH. Cellularbasis for volume related wall thickness changes in the rat left ventricle. JMol Cell Cardiol 1974;6:317—31.
[3] Streeter DD, Torrent-Guasp F. Geodesic paths in the left ventricle of themammalian heart. Circulation 1973;48(Suppl. 4):4—14.
[4] Streeter DD, Powers WE, Ross MA, Torrent-Guasp F. Three-dimensionalfiber orientation in the mammalian left ventricular wall. In: Baan J,Noordergraaf A, Raines J, editors. Cardiovascular system dynamics. Cam-bridge: M.I.T. Press; 1978. p. 73—84.
[5] Streeter DD. The cardiovascular system. I. American PhysiologicalSociety. Handbook of physiology Baltimore: Williams and Wilkins; 1979.p. 61—112.
[6] Krehl L. Kenntniss der fallung und entleerung des herzens. Abhandl MathPhys 1891;29:341—62.
[7] Torrent-Guasp F. Sobre morfologia y funcionalismo cardiacos. Rev EspCardiol 1967;20:1.
[8] Torrent-Guasp F, Ballester M, Buckberg GD, Carreras F, Flotats A, Carrio I,Ferreira A, Samuels LE, Narula J. Spatial orientation of the ventricular

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97S96
muscle band: physiologic contribution and surgical implications. J ThoracCardiovasc Surg 2001;122(2):389—92.
[9] Torrent-Guasp F, Buckberg GD, Clemente C, Cox JL, Coghlan HC, GharibM. The structure and function of the helical heart and its buttresswrapping. I. The normal macroscopic structure of the heart. SeminThorac Cardiovasc Surg 2001;13(4):301—19.
[10] Rademakers FE, Buchalter MB, Rogers WJ, Zerhouni EA, Weisfeldt ML,Weiss JL, Shapiro EP. Dissociation between left ventricular untwisting andfilling. Accentuation by catecholamines. Circulation 1992;85(4):1572—81.
[11] Shapiro EP, Rademakers FE. Importance of oblique fiber orientation forleft ventricular wall deformation. Technol Health Care 1997;5:21—8.
[12] Ingels NB, Hansen D, Daughters II GT, Stinson EB, Alderman E, Miller DC.Relation between longitudinal, circumferential, and oblique shorteningand torsional deformation in the left ventricle of the transplanted humanheart. Circ Res 1989;64:915—27.
[13] Moon MR, Ingels NB, Daughters II GT, Stinson EB, Hansen DE, Miller DC.Alterations in left ventricular twist mechanics with inotropic stimulationand volume loading in human subjects. Circulation 1994;89:142—50.
[14] Jouk PS, Usson Y, Michalowicz G, Grossi L. Three-dimensional cartographyof the pattern of themyofibres in the second trimester fetal human heart.Anat Embryol (Berl) 2000;202:103—18.
[15] Lunkenheimer PP, Redmann K, Scheld H, Dietl KH, Cryer C, Richter KD,Merker J, Whimster W. The heart muscle’s putative ‘‘secondary struc-ture’’. Functional implications of a bandlike anisotropy. Technol HealthCare 1997;5:53—64.
[16] Buchalter M, Rademakers FE, Weiss JL, Rogers WJ, Weisfeldt ML. Rota-tional deformation of the canine left ventricle measured by magneticresonance tagging: effects of catecholamines, ischaemia, and pacing.Cardiovasc Res 1994;28:629—35.
[17] Buckberg GD, Clemente C, Cox JL, Coghlan HC, Castella M, Torrent-GuaspF, Gharib M. The structure and function of the helical heart and itsbuttress wrapping. IV. Concepts of dynamic function from the normalmacroscopic helical structure. Semin Thorac Cardiovasc Surg2001;13(4):342—57.
[18] Buckberg GD, Coghlan HC, Torrent-Guasp F. The structure and function ofthe helical heart and its buttress wrapping. V. Anatomic and physiologicconsiderations in the healthy and failing heart. Semin Thorac CardiovascSurg 2001;13(4):358—85.
[19] Torrent-Guasp F. Un modelo elastico del corazon. Rev Esp Cardiol1996;49:516—22.
[20] Torrent-Guasp F, Whimster WF, Redmann K. A silicone rubber mould of theheart. Technol Health Care 1997;5:13—20.
[21] Villarreal FJ, Lew WY, Waldman LK, Covell JW. Transmural myocardialdeformation in the ischemic canine left ventricle. Circ Res 1991;68:368—81.
[22] Waldman LK, Nosan D, Villarreal F, Covell JW. Relation between trans-mural deformation and local myofiber direction in canine left ventricle.Circ Res 1988;63:550—62.
[23] Schmid P, Niederer P, Lunkenheimer PP, Torrent-Guasp F. The anisotropicstructure of the human left and right ventricles. Technol Health Care1997;5(1—2):29—43.
[24] LeGrice IJ, Takayama Y, Covell JW. Transverse shear along myocardialcleavage planes provides a mechanism for normal systolic wall thicken-ing. Circ Res 1995;77:182—93.
[25] Hansen DE, Daughters GT, Alderman EL, Ingels Jr NB, Miller DC. Torsionaldeformation of the left ventricular midwall in human hearts with intra-myocardial markers: regional heterogeneity and sensitivity to the ino-tropic effects of abrupt rate changes. Circ Res 1988;62(5):941—52.
[26] Ingels Jr NB, Hansen DE, Daughters GT, Stinson EB, Alderman EL, MillerDC. Relation between longitudinal, circumferential, and oblique short-ening and torsional deformation in the left ventricle of the transplantedhuman heart. Circ Res 1989;64(5):915—27.
[27] Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and diastolicheart failure: Part II: causal mechanisms and treatment. Circulation2002;105(12):1503—8.
[28] Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and diastolicheart failure: Part I: diagnosis, prognosis, and measurements of diastolicfunction. Circulation 2002;105(11):1387—93.
[29] Waldman LK, Fung YC, Covell JW. Transmural myocardial deformation inthe canine left ventricle: normal in vivo three-dimensional finite strains.Circ Res 1985;57:152—63.
[30] Buchalter MB, Weiss JL, Rogers WJ, Zerhouni EA, Weisfeldt ML, Beyar R,Shapiro EP. Noninvasive quantification of left ventricular rotational
deformation in normal humans using magnetic resonance imaging myo-cardial tagging. Circulation 1990;81(4):1236—44.
[31] Kvam G, Dahle H, Nordrehaug JE, Randa TI, Tillung T. The shorteningfraction of myocardial fibers and its layered distribution, as derived fromcine-MR imaged left ventriculograms. An approach for evaluating globarleft ventricular function. Acta Radiol 1997;38(3):391—9.
[32] McDonald IG. The shape and movements of the human left ventricleduring systole. A study by cineangiography and by cineradiography ofepicardial markers. Am J Cardiol 1970;26(3):221—30.
[33] Lorenz CH, Pastorek JS, Bundy JM. Delineation of normal human leftventricular twist throughout systole by tagged cine. J Cardiovasc MagnReson 2000;2(2):97—108.
[34] Spotnitz WD, Welker RL. Update on myocardial contrast echocardiogra-phy: a surgeon’s perspective. Semin Thorac Cardiovasc Surg1998;10(4):265—72.
[35] Greenbaum RA, Ho SY, Gibson DG, Becker AE, Anderson RH. Left ven-tricular fibre architecture in man. Br Heart J 1981;45:248—63.
[36] Lunkenheimer PP, Redmann K, Dietl KH, Cryer C, Richter KD, WhimsterWF, Niederer P. The heart’s fibre alignment assessed by comparing twodigitizing systems. Methodological investigation into the inclination angletowards wall thickness. Technol Health Care 1997;5(1—2):65—77.
[37] Coghlan C, Prieto G, Harrison TR. Movement of the heart during theperiod between the onset of ventricular excitation and the start of leftventricular ejection. Am Heart J 1961;62:65—82.
[38] Buckberg GD, Coghlan C, Torrent-Guasp F. The structure and function ofthe helical heart and its buttress—Anatomic and physiologic considera-tions in the healthy and failing heart. Sem Thorac Cardiovasc Surg2001;13(4):358—85.
[39] Ingels Jr NB, Daughters GT, Stinson EB, Alderman EL. Measurement ofmidwall myocardial dynamics in intact man by radiography of surgicallyimplanted markers. Circulation 1975;52(5):859—67.
[40] Tibayan FA, Lai DT, Timek TA, Dagum P, Liang D, Daughters GT, Ingels NB,Miller DC. Alterations in left ventricular torsion in tachycardia-induceddilated cardiomyopathy. J Thorac Cardiovasc Surg 2002;124(1):43—9.
[41] Borelli GA. In: Bishop LF, Neilson Jr J, editors. History of cardiology. NewYork: Medical Life Press; 1927.
[42] Robb JS, Robb RC. The normal heart: anatomy and physiology of thestructural units. Am Heart J 1942;23:455—67.
[43] Gibbons Kroeker CA, Tyberg JV, Beyar R. Effects of load manipulations,heart rate, and contractility on left ventricular apical rotation. Anexperimental study in anesthetized dogs. Circulation 1995;92(1):130—41.
[44] Gibbons Kroeker CA, Ter Kerus HE, Knudtson ML, Tyberg JV, Beyar R. Anoptical device to measure the dynamics of apex rotation of the leftventricle. Am J Physiol 1993;265:H1444—9.
[45] Pettigrew J. On the arrangement of the muscular fibres of the ventricularportion of the heart of the mammal. Proc R Soc Lond 1860;10:433—40.
[46] Pettigrew JB. On the arrangement of the muscular fibres of the ventriclesof the vertebrate heart with physiological remarks. Phil Trans1865;154:445—500.
[47] Keith A. The functional anatomy of the heart. Br Med J 1918;1:361—3.[48] Beyar R, Yin F, Hausknecht M, Weisfeldt ML, Kass D, Beyar R, Yin F.
Dependence of left ventricular twist-radial shortening relations on car-diac cycle phase. Am J Physiol 1989;257:H1119—26.
[49] Beyar R, Sideman S. The dynamic twisting of the left ventricle: acomputer study. Ann Biomed Eng 1986;14:547—62.
[50] Beyar R, Shapiro EP, graves WL, Rogers WJ, Guier WH, Carey GA, soulenRL, Zerhouni EA,Weisfeldt ML,Weiss JL. Quantification and validation ofleft ventricular wall thickening by a three-dimensional volume elementmagnetic resonance imaging approach. Circulation 1990;81(1):297—307.
[51] Arts T, Hunter WC, Douglas A, Muijtjens Am Reneman RS. Description ofthe deformation of the left ventricle by a kinematic model. J Biomech1992;25:1119—27.
[52] Arts T, Meerbaum S, Reneman RS, Corday E. Torsion of the left ventricleduring the ejection phase in the intact dog. Cardiovasc Res1984;18(3):183—93.
[53] Ormiston JA, Shah PM, Tei C, Wong M. Size and motion of the mitral valveannulus in man. I. A two-dimensional echocardiographic method andfindings in normal subjects. Circulation 1981;64(4):113—20.
[54] LeGrice IJ, Takayama Y, Holmes JW, Covell JW. Impaired subendocardialfunction in tachycardia-induced cardiac failure. Am J Physiol1995;268:H1788—94.
[55] Tawara S. Dos Reizfeitungsystem des Saugethierherzens Jena: GustavFischer; 1906.

G.D. Buckberg et al. / European Journal of Cardio-thoracic Surgery 29S (2006) S75—S97 S97
[56] Sodi-Pallares D, Calder RM. New bases of electrocardiography, 388. St.Louis: Mosby; 1956.
[57] Lewis MJ, Shah AM, Smith JA, Henderson AH. Does endocardiummodulatemyocardial contractile performance? Cardioscience 1990;1:83—7.
[58] Lewis T, Rothschild MA. Series B. 1915; 181—226.[59] Coghlan HC, Coghlan AR, Buckberg GD, Gharib M, Cox JL. The structure
and function of the helical heart and its buttress wrapping. III. Theelectric spiral of the heart: the hypothesis of the anisotropic conductingmatrix. Semin Thorac Cardiovasc Surg 2001;13(4):333—41.
[60] Delhaas T, Arts T, Prinzen FW, Reneman RS. Regional electrical activationand mechanical function in the partially ischemic left ventricle of dogs.Am J Physiol 1996;271:H2411—20.
[61] Sallin EA. Fiber orientation and ejection fraction in the human ventricle.Biophys J 1969;9:954—64.
[62] Ingels Jr NB. Myocardial fiber architecture and left ventricular function.Technol Health Care 1997;5:45—52.
[63] Armour JA, Randall WC. Electrical and mechanical activity of papillarymuscle. Am J Physiol 1970;218(6):1710—7.
[64] Roy CS, Adami JG. Heartbeat and pulsewave. Practitioner 1890;44:81—94.[65] Robb JS, Robb RC. The excitatory process in themammalian ventricle. Am
J Physiol 1936;115:43—52.[66] Taccardi B, Lux RL, Ershler PR, MacLeod R, Dustman TJ, Ingebrigtsen N.
Anatomical architecture and electrical activity of the heart. Acta Cardiol1997;52(2):91—105.
[67] Taccardi B, Macchi E, Lux RL, Ershler PR, Spaggiari S, Baruffi S, VyhmeisterY. Effect of myocardial fiber direction on epicardial potentials. Circula-tion 1994;90(6):3076—90.
[68] Robinson TF, Factor SM, Sonnenblick EH. The heart as a suction pump. SciAm 1986;254(6):84—91.
[69] Yamasaki R, Wu Y, McNabb M, Greaser M, Labeit S, Granzier H. Proteinkinase A phosphorylates titin’s cardiac-specific N2B domain and reducespassive tension in rat cardiac myocytes. Circ Res 2002;90(11):1181—8.
[70] Bell SP, Nyland L, Tischler MD, McNabb M, Granzier H, LeWinter MM.Alterations in the determinants of diastolic suction during pacing tachy-cardia. Circ Res 2000;87(3):235—40.
[71] Gibson DG, Brown DJ. Continuous assessment of left ventricular shape inman. Br Heart J 1975;37(9):904—10.
[72] Kass DA, Traill TA, Keating M, Altieri PI, Maughan WL. Abnormalities ofdynamic ventricular shape change in patients with aortic and mitral
valvular regurgitation: assessment by Fourier shape analysis and globalgeometric indexes. Circ Res 1988;62(1):127—38.
[73] Karwatowski SP, Brecker SJ, Yang GZ, Firmin DN, St John SM, Under-wood SR. A comparison of left ventricular myocardial velocity indiastole measured by magnetic resonance and left ventricular fillingmeasured by Doppler echocardiography. Eur Heart J 1996;17(5):795—802.
[74] Brutsaert DL, Szoka FC. Relaxation and diastole of the heart. Physiol Rev1989;69:1228—315.
[75] Takayama M, Norris RM, Brown MA, Armiger LC, Rivers JT, White HD.Postsystolic shortening of acutely ischemic canine myocardium predictsearly and late recovery of function after coronary artery reperfusion.Circulation 1988;78(4):994—1007.
[76] Davidoff R, Picard MH, Force T, Thomas JD, Guerrero JL, McGlew S,Weyman AE. Spatial and temporal variability in the pattern of recovery ofventricular geometry and function after acute occlusion and reperfusion.Am Heart J 1994;127:1231—41.
[77] Castella M, Buckberg GD. Diastolic dysfunction in stunned myocardiumand its prevention by Na+—H+ exchange inhibition. Eur J CardiothoracSurg 2006.
[78] Stuber M, Scheidegger MB, Fischer SE, Nagel E, Steinemann F, Hess OM.Alterations in the local myocardial motion pattern in patients sufferingfrom pressure overload due to aortic stenosis. Circulation 1999;100:361—8.
[79] Yun KL, Niczyporuk MA, Daughters GT, Ingels Jr NB, Stinson EB, AldermanEL, Hansen DE, Miller DC. Alterations in left ventricular diastolic twistmechanics during acute human cardiac allograft rejection. Circulation1991;83(3):962—73.
[80] Caulfield JB, Janicki JS. Structure and function of myocardial fibrillarcollagen. Technol Health Care 1997;5(1—2):95—113.
[81] Lipp P, Niggli E. Microscopic spiral waves reveal positive feedback insubcellular calcium signalling. Biophys J 1993;65(6):2272—6.
[82] Cook T. The curves of life New York: Dover Publications Inc.; 1979.[83] Mall FP. On the muscular architecture of the ventricles of the human
heart. Am J Anat 1911;11:211—78.[84] Lower R. Tractus de Corde 1669. In: Gunther RT, editor. Early science in
Oxford. Sawsons: Oxford; 1932.[85] Buckberg GD. Basic science review: the helix and the heart. J Thorac
Cardiovasc Surg 2002;124(5):863—83.