
Stroke: Diagnosis and Management Economics Burden of Stroke
9
1 Stroke: Diagnosis and Management .. e-mail:[email protected] Economics Burden of Stroke stroke 690 1 (.. ) 138,000 9,660 1 13,800 1. Sudden onset 2. Risk factors 3. Neuro-vascular Risk Factors for Cerebral Infarction Mechanism Etiology Hypertension Aging Hyperlipidemia Diabetes and so on Hypertension Hyperlipidemia Others Cardiac disease Hypertension Aging Others Cerebral thrombosis Cerebral embolism Hemodyna- mic Athero- thrombotic Cardio- embolic Lacunar Stroke Risk Factors Non-modifiable Modifiable • Older age • HT • Male sex • Smoking • Race • Carotid stenosis • Genetic • Exercise • DM • TIA • Hyperlipidemia • Cardiac disease Classification Ischemic Ischemic- occlusive occlusive Thrombosis Thrombosis major major vv vv minor minor vv vv Embolism Embolism cardiogenic cardiogenic artery artery-to to-artery artery cryptogenic cryptogenic Hemorrhagic Hemorrhagic Intraparenchymal Intraparenchymal Subdural Subdural Epidural Epidural Subarachnoid Subarachnoid
Transcript of Stroke: Diagnosis and Management Economics Burden of Stroke
1
Stroke: Diagnosis and Management��.��.�������� �� !���"#
�#$#%�&#'�(�#�%��!# )#*%�&#+#!,��#�-�.*/(0��!�#�-�. �1#%��!#2�!$+�0�"�
e-mail:[email protected]
Economics Burden of Stroke� *%#�&,�$+< stroke
� 690 �#!-"+'�(&#�� 1 0��*�(�.��.����B. �%<%�����.)� D�)#*-(%��++��E !<�1�F+ � GHI'J%! '�(�#/ 138,000 �#!� GHI'J%!�'N�OPQ#RQ#�%� 9,660 �#!-"+'S � *"#D&IR"#!��P<�#<-�<02(�#<+I+�'�(�#/ 1 0��T#�-"+*�-"+'S *���'N��<�� 13,800 2I#�T#�
� �HU�� !�#<���VW��R +!"#<!�X<
1. Sudden onset
2. Risk factors
3. Neuro-vascular
Risk Factors for Cerebral Infarction
Mechanism EtiologyHypertension
Aging
Hyperlipidemia
Diabetes and so on
Hypertension
Hyperlipidemia
Others
Cardiac
disease
Hypertension
Aging
Others
Cerebral
thrombosis
Cerebral
embolism
Hemodyna-mic
Athero-
thrombotic
Cardio-
embolic
Lacunar
Stroke Risk FactorsNon-modifiable Modifiable• Older age • HT• Male sex • Smoking• Race • Carotid stenosis• Genetic • Exercise
• DM• TIA• Hyperlipidemia• Cardiac disease
Classification IschemicIschemic--occlusiveocclusive
�� ThrombosisThrombosis
�� major major vvvv
�� minor minor vvvv
�� EmbolismEmbolism
�� cardiogeniccardiogenic
�� arteryartery--toto--arteryartery
�� cryptogeniccryptogenic
HemorrhagicHemorrhagic
�� IntraparenchymalIntraparenchymal
�� SubduralSubdural
�� EpiduralEpidural
�� SubarachnoidSubarachnoid
2
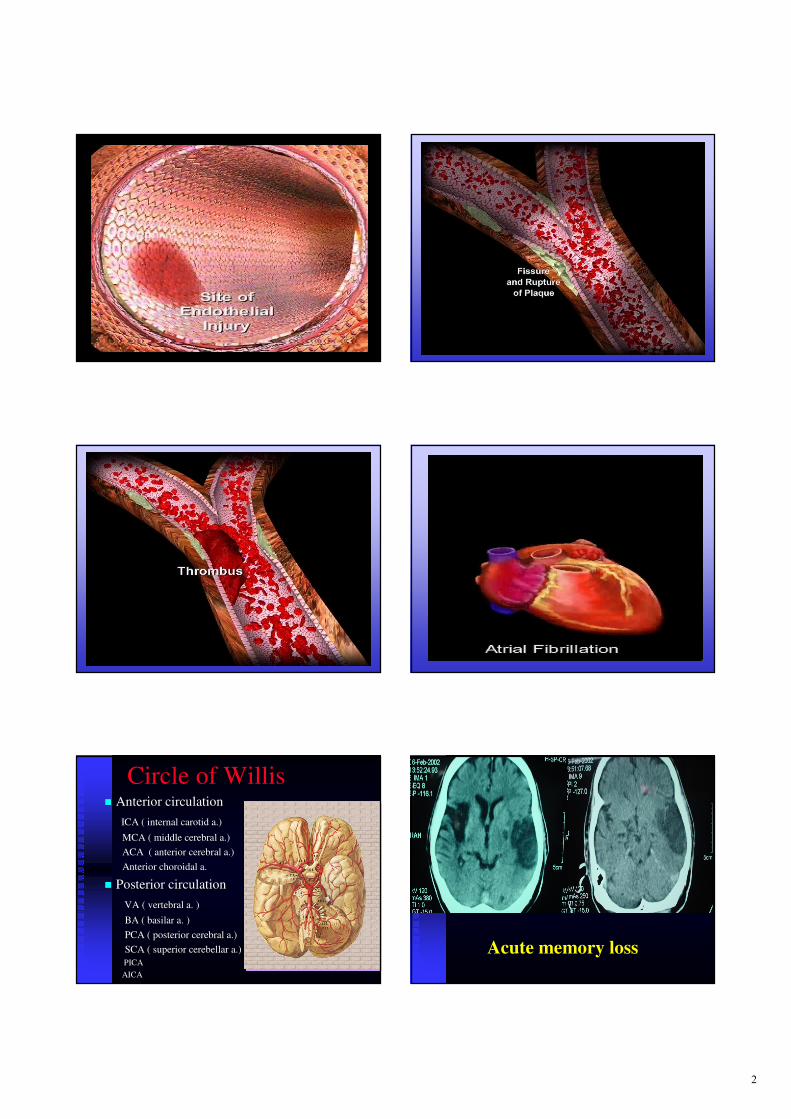
Circle of Willis�� Anterior circulationAnterior circulation
ICA ( internal carotid a.)ICA ( internal carotid a.)
MCA ( middle cerebral a.)MCA ( middle cerebral a.)
ACA ( anterior cerebral a.)ACA ( anterior cerebral a.)
Anterior Anterior choroidalchoroidal a.a.
�� Posterior circulationPosterior circulation
VA ( vertebral a. )VA ( vertebral a. )
BA ( basilar a. )BA ( basilar a. )
PCA ( posterior cerebral a.)PCA ( posterior cerebral a.)
SCA ( superior cerebellar a.)SCA ( superior cerebellar a.)
PICAPICA
AICAAICA
Acute memory loss

3
Global aphasia
Sudden right hemiplegia
Parietal lobe sign
�� AstereognosiaAstereognosia
�� Dressing Dressing apraxiaapraxia
�� Homonymous inferior quadrant Homonymous inferior quadrant anopiaanopia
�� GertmannGertmann’’ss syndromesyndrome
�� Sensory inattentionSensory inattention
Dressing apraxiaAcute cortical blindness
Sudden vertigo
4
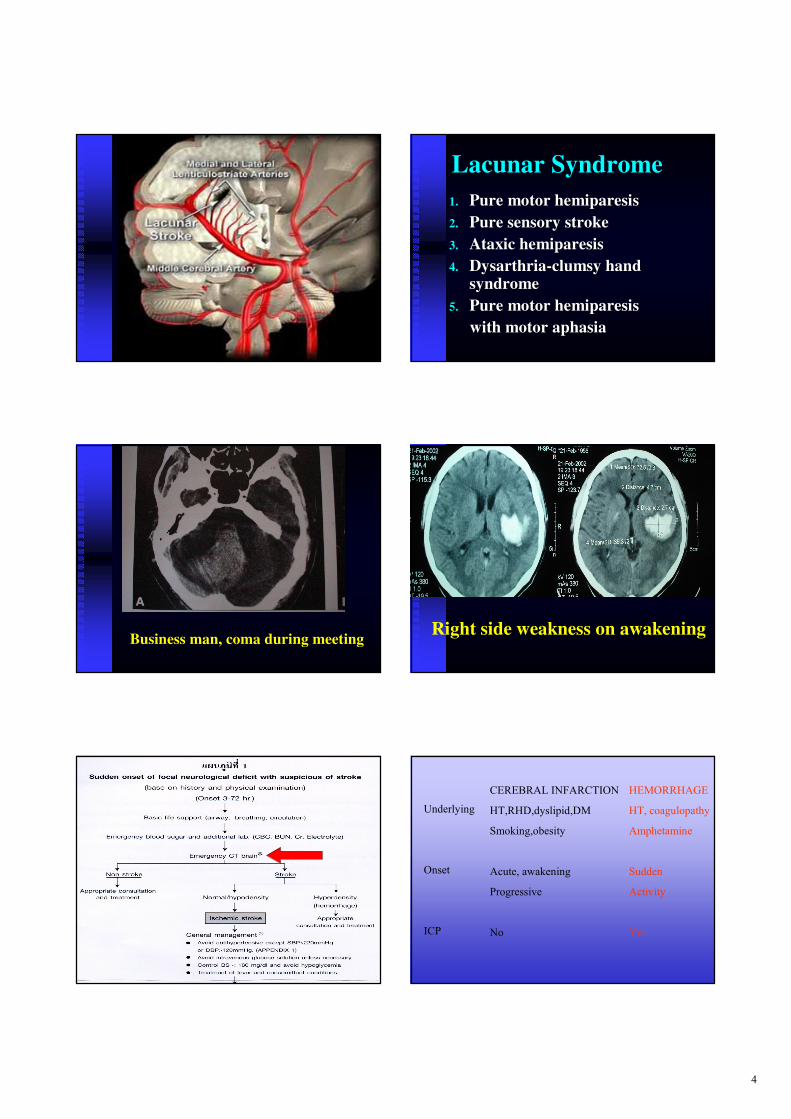
Lacunar Syndrome
1.1. Pure motor Pure motor hemiparesishemiparesis
2.2. Pure sensory strokePure sensory stroke
3.3. Ataxic Ataxic hemiparesishemiparesis
4.4. DysarthriaDysarthria--clumsy hand clumsy hand
syndromesyndrome
5.5. Pure motor Pure motor hemiparesishemiparesis
with motor aphasiawith motor aphasia
Business man, coma during meetingRight side weakness on awakening
CEREBRAL INFARCTION
HT,RHD,dyslipid,DM
Smoking,obesity
Acute, awakening
Progressive
No
Underlying
Onset
ICP
HEMORRHAGE
HT, coagulopathy
Amphetamine
Sudden
Activity
Yes
5
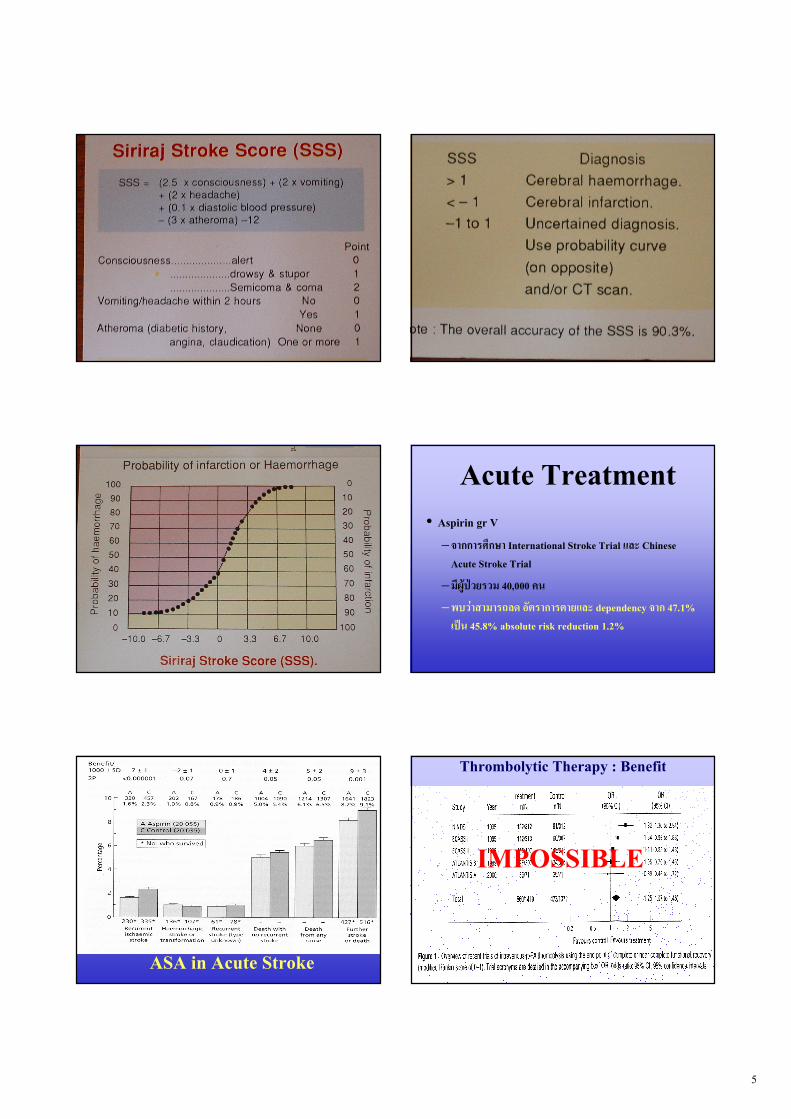
Acute Treatment• Aspirin gr V
– R#��#��h�V# International Stroke Trial 02( Chinese Acute Stroke Trial
–� GHI'J%!�%� 40,000 *�
–�T%"#�#�#�j2� +�-�#�#�-#!02( dependency R#� 47.1% �'N� 45.8% absolute risk reduction 1.2%
ASA in Acute Stroke
Thrombolytic Therapy : Benefit
IMPOSSIBLE

6
Anticoagulant in Stroke
NO BENEFIT
Acute Treatment• Outcome �#����V#� X2��#�-#!02(�#� dependents 1 �#!• Aspirin
– -�%+!"#<�#�*Q#�%�• Death or dependency 47.0%• ASA 45.8%• Absolute risk reduction (ARR) 1.2%• Number needed to treat (NNT) 100/1.2 = 83 �#! • *"#D&IR"#! 83 x 0.5 x 28 = 1, 160 T#�
• Thrombolytic therapy – ARR 6.3% NNT 16 *"#D&IR"#! 800,000 T#�
Ref : Hankey GJ and Warlow CP, 1999
Male, 70 years, DM, HT, IHD, dyslipidemiaDysphagia, dysarthia
What to do about BP in
acute ischemic stroke is
unclear: raise it, lower it or
leave it alone? We trend to
leave it alone unless there is
evidence of end-organ
damage.
Indication to Reduction BP• Before and post rt-PA ( 24 hr )
• Hypertensive encephalopathy
• AMI
• Aortic dissection
• Hemorrhagic transformation
Drug : Nitroglycerine , Nitroprusside ,Nicardipine , Labetarol ,Captopril
NO ADALAT SUBLINGUAL
7
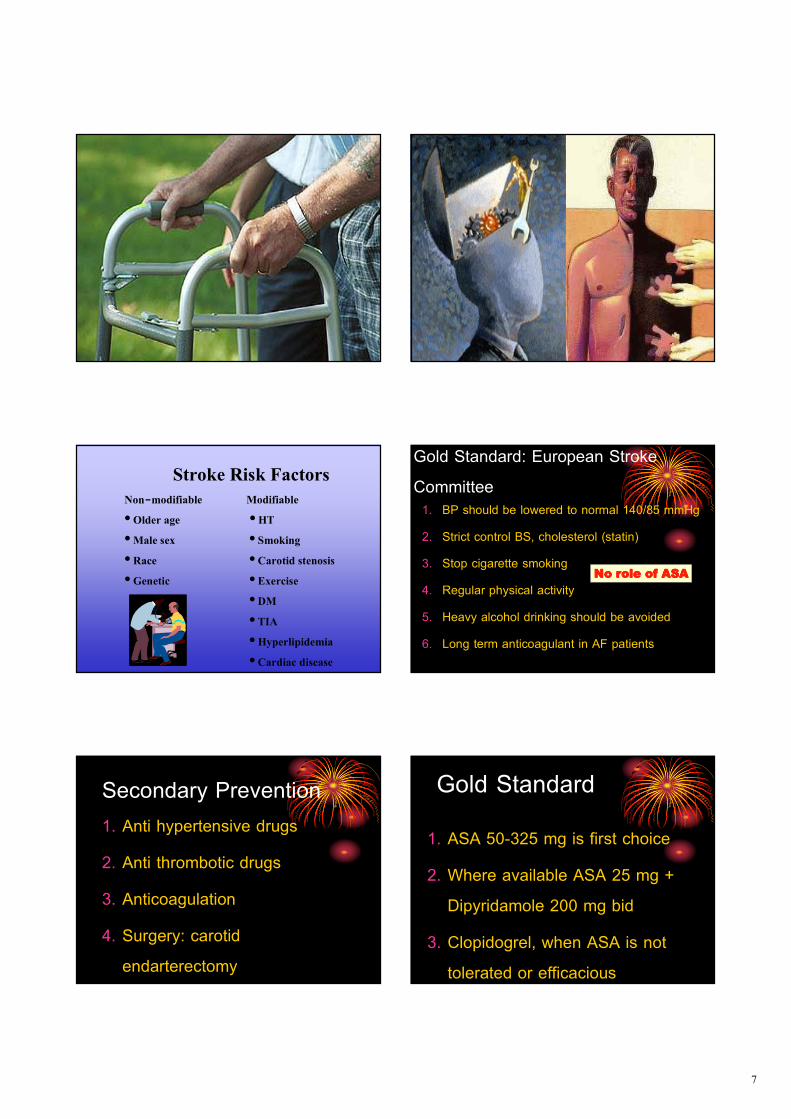
Stroke Risk FactorsNon-modifiable Modifiable• Older age • HT• Male sex • Smoking• Race • Carotid stenosis• Genetic • Exercise
• DM• TIA• Hyperlipidemia• Cardiac disease
Gold Standard: European Stroke
Committee 1. BP should be lowered to normal 140/85 mmHg
2. Strict control BS, cholesterol (statin)
3. Stop cigarette smoking
4. Regular physical activity
5. Heavy alcohol drinking should be avoided
6. Long term anticoagulant in AF patients
No role of ASANo role of ASANo role of ASANo role of ASA
Secondary Prevention
1. Anti hypertensive drugs
2. Anti thrombotic drugs
3. Anticoagulation
4. Surgery: carotid
endarterectomy
Gold Standard
1. ASA 50-325 mg is first choice
2. Where available ASA 25 mg +
Dipyridamole 200 mg bid
3. Clopidogrel, when ASA is not
tolerated or efficacious

8
Anticoagulantion: 5 Rheumatic
5 MI
5 CHF
5 Cardiomyopathy
5 Arrhythmia, AF
5 PFO
Gold Standard
1. Stroke with AF, INR 2-3
2. Prosthetic heart valve, INR 3-4
3. Cardioembolic stroke, INR 2-3
Risk FactorsRisk FactorsRisk FactorsRisk Factors

9
� Smoking cessation � ARR 2.3%� NNT -"+'S 43 �#!� *"#D&IR"#!
� <��+< 0 T#� � '�(1!���<��*"#T,1� Xw�I 12,700 T#�
Secondary prevention


















