Strengthening Communities - Flinders University communities 2008 STRENGTHENING COMMUNITIES A...
36
STRENGTHENING COMMUNITIES A mentoring program for adults with acquired brain injury Michelle Bellon, PhD*, Jaime Gardner† & Rebecca Riley† *Department of Disability Studies, Faculty of Health Sciences, Flinders University †Community Re-entry Program, South Australia October, 2008 CRP Research Report
Transcript of Strengthening Communities - Flinders University communities 2008 STRENGTHENING COMMUNITIES A...
Strengthening communities
2008
STRENGTHENING COMMUNITIES A mentoring program for adults with acquired brain injury
Michelle Bellon, PhD*, Jaime Gardner† & Rebecca Riley†
*Department of Disability Studies, Faculty of Health Sciences, Flinders University
†Community Re-entry Program, South Australia
October, 2008
CRP Research Report
CRP Research Report, 2008 Strengthening Communities
ABSTRACT
This pilot study presents the results of a 9-month mentor program for 7 adults with acquired brain injury (ABI).
Outcomes were measured using the Community Integration Questionnaire (CIQ) and interviews at pre and post program, and then repeated again at a six-month follow-up to provide three data collection points.
The mentor program sought to address the community support needs of adults with ABI, achieve individual goals, facilitate community reintegration and participation, develop robust networks, and enhance individual skills and coping strategies.
Case studies are presented describing each mentor relationship and the goals and outcomes for each couple.
Small but significant improvements were noted on the CIQ post-program, suggesting improvements in home integration, social integration, productivity, and total CIQ scores, with further research required to determine if these results generalize to a larger sample. These improvements were not sustained by 6-month follow-up, with scores falling back to baseline levels in all areas except productivity.
This report identifies the factors that influence the success of the mentor relationship, explores the impact on achievement of mentee goals and community inclusion, and indicates the benefits of participating in a mentor program for people with ABI. Recommendations for future mentor programs are highlighted.
The development and evaluation of this pilot study provides a useful model for mentor programs which may be applied to other areas of disability and community support.
This research project was funded by Community Benefit SA with the support of the Epilepsy Association of SA & NT.
Ethics approval received from Flinders University Social and Behavioural Research Ethics Committee (SBRE 3680)
A mentoring program for adults with ABI Page 1

CRP Research Report, 2008 Strengthening Communities
TABLE OF CONTENTS
INTRODUCTION ............................................................................................................................................ 2
Aim.............................................................................................................................................................. 3
What is Mentoring? ..................................................................................................................................... 3
The Role of Mentoring in Community Integration Following Acquired Brain Injury...................................... 4
Benefits and Limitations of Mentoring ......................................................................................................... 5
METHOD ........................................................................................................................................................ 6
Participants ................................................................................................................................................. 6
Procedures.................................................................................................................................................. 6
Outcome Measurement............................................................................................................................... 8
RESULTS ....................................................................................................................................................... 9
Demographic & Diagnostic Data ................................................................................................................. 9
Case Studies............................................................................................................................................... 9
Community Integration Questionnaire Scores........................................................................................... 24
DISCUSSION................................................................................................................................................ 27
What Factors Influence the Success of the Mentor Relationship? ............................................................ 27
What Impact does the Mentor Relationship have on Achievement of Mentee Goals?.............................. 30
What are the Benefits of a Mentor Program for People with ABI & Mentors? ........................................... 31
Recommendations .................................................................................................................................... 32
CONCLUSION .............................................................................................................................................. 33
REFERENCES ............................................................................................................................................. 33
A mentoring program for adults with ABI Page 2

CRP Research Report, 2008 Strengthening Communities
INTRODUCTION
One of the key concerns facing successful long-term community integration following acquired brain injury (ABI) is the experience of fractured social networks. These social networks are characteristically limited and diminished, resulting in social isolation and disconnection from the community (Rees, 2005; Tyerman, 1997). A useful way of assisting people with ABI to generate new supports is through the use of a mentor program. Mentors can play a vital role in assisting people with ABI in community reintegration (Jones, 1998). Through supporting and facilitating the development of a natural support network, opportunities for fulfilling personal goals can arise.
Mentoring support programs have been found to have a positive impact on personal sense of empowerment (regaining sense of mastery over situation, environment and life), and self-efficacy (enhancing perceptions of their capabilities for handling situations) across a number of disciplines. Mentor programs, also termed ‘buddy’ programs, have been widely used to support people with ABI, with the view to reduce isolation and increase community integration. However, despite the proliferation of mentor applications and research, there appears to be a distinct lack of research dedicated to evaluating the outcome of such a model in the area community integration following ABI.
Aim The aim of this project was to plan, conduct, measure and evaluate outcomes of a 9-month community based mentor program for 7 adults with ABI. The individualized program sought to address the community support needs of people with ABI, achieve individual goals, facilitate reintegration and participation, develop robust networks, and enhance individual skills and coping strategies.
What is Mentoring? The concept of mentoring has been in existence for thousands of years. In a historical context, the mentor was seen a trusted advisor who aided and trained the hero (Campbell, 1988). In Greek mythology, Athena acted as mentor and guide to Telemachus in Homer’s epic ‘The Odyssey’. In present day, this relationship still plays an important role and appears prominently in areas such as management (Eddy, Tannenbaum, Lorenzet & Smith-Jentsch, 2005), business (Heffernan & Joni, 2005), education (Dunn, 2005), medicine (Luckhaupt, Chin, Mangione et al 2005) and nursing (Tracey & Nicholl, 2006).
Mentoring can be described as a nurturing process in which a skilled or more experienced person serves as a role model, teaches, supports, encourages and counsels an individual, providing direction and feedback regarding future plans and personal development (Hunt & Michael, 1983; Anderson & Shannon, 1988, cited in Lee, Theoharis, Kyeong-Hwa, Liss, Nix-Williams, Griswold & Walther-Thomas, 2006). This is a relationship which is based on mutual respect and agreed expectations that seeks to benefit all involved (Heartfield, Gibson & Nasel, 2005). Mentors are not expected to ‘know all the answers’, but assist by providing direction and guidance with problem solving. In addition, the mentor’s role is to assist, not assess (Duffy & Forgan, 2005).
One educational study describes the mentor as providing encouragement and support to enable the partner to improve personal effectiveness (Bush & Coleman, 1995). Coaching analogies have also been applied, with the mentor described as seeking to develop the mentee’s skill and capabilities, and prepare them for their future (Finn, 1993). Figure 1 below illustrates the variety of roles a mentor may hold.
The mentor relationship is not one that is static, but rather dynamic and evolving. Kram (1983) identifies four phases in the mentor relationship: initiation, cultivation, separation and redefinition. The mentor’s role is ideally seen as temporary, with the clear aim of developing autonomy and self-reliance (Barnett, 1995). In order for the mentoring relationship to be successful, it is advised that the mentee must first clearly identify their needs and goals (Heartfield, Gibson & Nasel, 2005). Having a clear view of what is to be achieved improves the chance of these outcomes being met by the end of the program.
A mentoring program for adults with ABI Page 3
CRP Research Report, 2008 Strengthening Communities
Figure 1 – Mentor roles
Provide feedback
Provide direction to resources
‘Open doors’
Act as a sounding
board
Provide support
Provide an alternative perspective
Facilitate problem solving
Assist to form goals
Mentor Roles
In order to develop and maintain such relationships, mentors require high levels of self-reflection, training and support (Jones, 1998). Reviews of strengths and weaknesses in teaching, guiding, counseling, behaviour management, personal communication, professional ethics and establishing relationship boundary skills are crucial (Lee et all, 2006).
The Role of Mentoring in Community Integration Following Acquired Brain Injury Acquired brain injury is defined by the Australian Institute of Health and Welfare as:
…“multiple disabilities arising from damage to the brain acquired after birth. It results in deterioration in cognitive, physical, emotional or independent functioning. It can be as a result of accidents, stroke, brain tumours, infection, poisoning, lack of oxygen, degenerative neurological diseases etc.” (AIHW, 2007)
ABI can result in a number of long term difficulties in a range of areas including:
• cognition (e.g. reduced concentration, memory, organizational skills), • behaviour (e.g. low frustration tolerance, reduced impulse control), • psychological functioning (e.g. anxiety and depression), • communication (e.g. reduced ability to listen, speak, read, write or interact socially), • physical functioning (eg reduced vision, hearing, balance, eye-hand coordination, mobility), and • health (e.g. fatigue, epilepsy, hydrocephalus)
(Sohlberg & Mateer, 2001, Ylvisaker & Feeney, 1998).
In particular, the experience of social isolation is common, and characterized by the breakdown of personal relationships, difficulty in making and sustaining relationships, anxiety and depression, reduced income, and limited job opportunities (Tyerman, 1997). The aim of the mentor in this context is to assist the individual to achieve personal goals, reduce isolation, and develop robust social networks for both the person with ABI and their family (Rees, 2005).
Close personal relationships play an important role in the development of self-esteem, mental health, academic achievement, social competence and social responsibility (DeVito, 2006). In contrast, life with few personal relationships can lead to feelings of social isolation, loneliness, reduced-self esteem, depression and emotional maladjustment, contributing to reduced physical and mental health and inability to resist disease (Green, Schleien, Mactavish & Benepe, 1995). In short, “we need friends for life; to make us – and keep us – whole” (Duck, 1991, p.8).
A mentoring program for adults with ABI Page 4

CRP Research Report, 2008 Strengthening Communities
The role of the mentor is to develop a supportive relationship with the person with ABI in order to motivate, guide and facilitate opportunities for the individual to participate in vocational, educational and social activities. In many ways, the mentor assists in the ‘frontal lobe’ functions for the person with brain injury by; (a) facilitating forward planning, (b) initiating constructive behaviour, (c) developing reality-based ideas in relation to their activity, (d) providing constructive language about the self and realistic language/ideas about others, (e) listening and reinforcing the positive behaviours, and (f) setting goals that are reality based (Rees, 2005). The long-term view must always be focused on developing strengths and talents, and enhancing community inclusion.
Jones’ (1998) paper on mentors for adults with ABI is one of the few published articles addressing issues in establishing a mentoring program in this context. In this paper, Jones identifies the mentor as someone who assists the individual with brain injury to acquire social and interpersonal skills, and develop awareness of new abilities and limitations through joint participation in activities. Through sustained support, regulation and regular cueing, the mentor can assist the person, particularly following frontal lobe damage, to inhibit impulsivity and facilitate problem solving, thereby increasing opportunities for successful goal achievement (Jones, 1998, p.57).
When constructing a mentoring program directly related to brain injury integration, research has highlighted the benefits of applying multidisciplinary approaches aimed at positive behaviour change (Hart & Evans, 2006). Interventions centered on goal achievement and self-regulation of goal-directed behaviour play an important role in enhancing the evidence base of brain injury rehabilitation (Hart & Evans, 2006). If the aim of rehabilitation is to enable people to identify and achieve relevant goals (Lawler, Dowswell, Hearn, Forster & Young, 1999; Wade, 1998), measuring the achievement of goals is a useful tool to determine the effectiveness of a particular intervention method (Kuipers, Foster, Carlson & Moy, 2003).
Benefits and Limitations of Mentoring Despite well-documented advantages and disadvantages to the mentoring process, there are many opportunities for such programs to provide overall positive experiences. Benefits for mentees identified by Bush & Coleman (1995) and Jones (1998) include the opportunity to receive support, encouragement and feedback, develop opportunities to develop social networks and reduce isolation, develop confidence, encourage positive attitudes, and receive help in identifying personal goals and future pathways.
An ancient saying goes, ‘When the student is ready, the Master will appear.’ Readiness is an essential component of the mentor relationship (Seritan, 2005). If the mentee is not ready or prepared to learn with the mentor, the union will not succeed. In contrast, when the mentee is willing to enter the relationship, the benefits can be significant. Taking cue from the person with ABI is essential, by determining if this is the type of support the individual wants and can benefit from.
Benefits are certainly not limited to the mentee. Mentor benefits can include a sense of personal satisfaction and the opportunity to develop networking skills (Bush & Coleman, 1995). Mentoring can provide a deeply rewarding and stimulating experience.
The limitations of this process are equally important to identify. Key concerns include (a) limited time to develop the relationship properly, (b) the risk of the mentee becoming too dependent on the mentor, and (c) the possibility of a ‘mismatch’ leading to the failure of the relationship (Bush & Coleman, 1995).
The mentor/mentee relationship can also be placed at risk when relationship expectations are not clearly established from the outset (Conway, 2005). When mentors rely on intuition or improvisation as opposed to meeting clearly defined goals, there is no accountability for the success or failure of the relationship, and the program may fail. Clear objectives are essential to the long-term success of the partnership (Barker, 2006).
A mentoring program for adults with ABI Page 5
CRP Research Report, 2008 Strengthening Communities
METHOD
Participants Selection criteria for volunteers wishing to be involved in this study are presented below.
Mentee selection criteria:
• a diagnosed acquired brain injury • over 18 years of age at the commencement of the study • able to make a time commitment of a minimum of 2-3 hours per week to participate in the
mentor program • agreed to allow the researcher access to relevant medical and psychological records • accessible and available to participate in the study for 15 months • were not at-risk for suicidal or violent behaviour and/or have serious psychiatric or substance
abuse problems • lived in metropolitan Adelaide
Mentor selection criteria:
• over 18 years of age at the commencement of the study
• accessible and available to participate in the study for 15 months
• able to make a time commitment of a minimum or 2-3 hours per week to participate in the mentor program, in addition to attending a preliminary information seminar, and weekly support/debriefing meetings with supervisor
• did not have an offender history (satisfy police clearance check)
• had a current first aid certificate
• were not at-risk for suicidal or violent behaviour and/or have serious psychiatric or substance abuse problems.
Information on this study was circulated to participants in a community based integration program for adults with ABI and students at Flinders University. Eight individuals with ABI and 9 volunteers seeking to be mentors indicated interest in the study and were recruited. One mentor withdrew from the study shortly after matching due to personal reasons. The mentee partner decided not to continue in the program or meet a new mentor due to family health difficulties. Despite a small sample size, 7 couples were considered representative, with data collection and supervision of the sample manageable and appropriate in terms of the research goals (Graziano & Raulin, 2004).
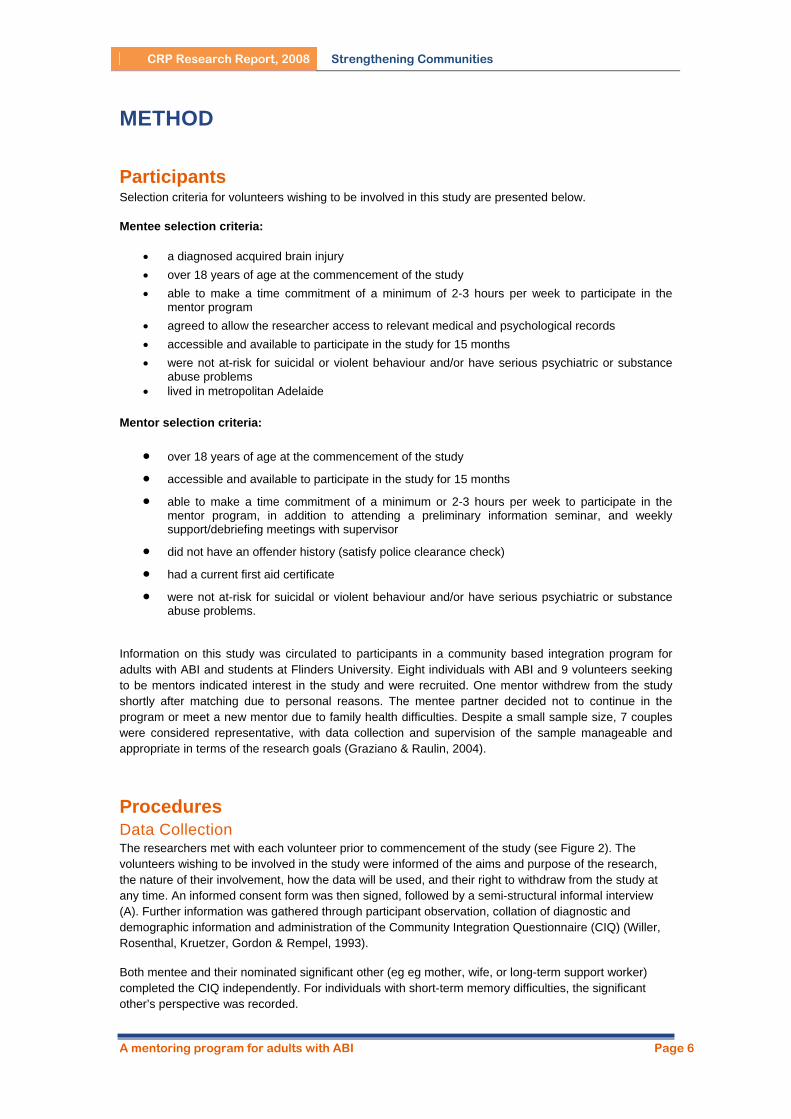
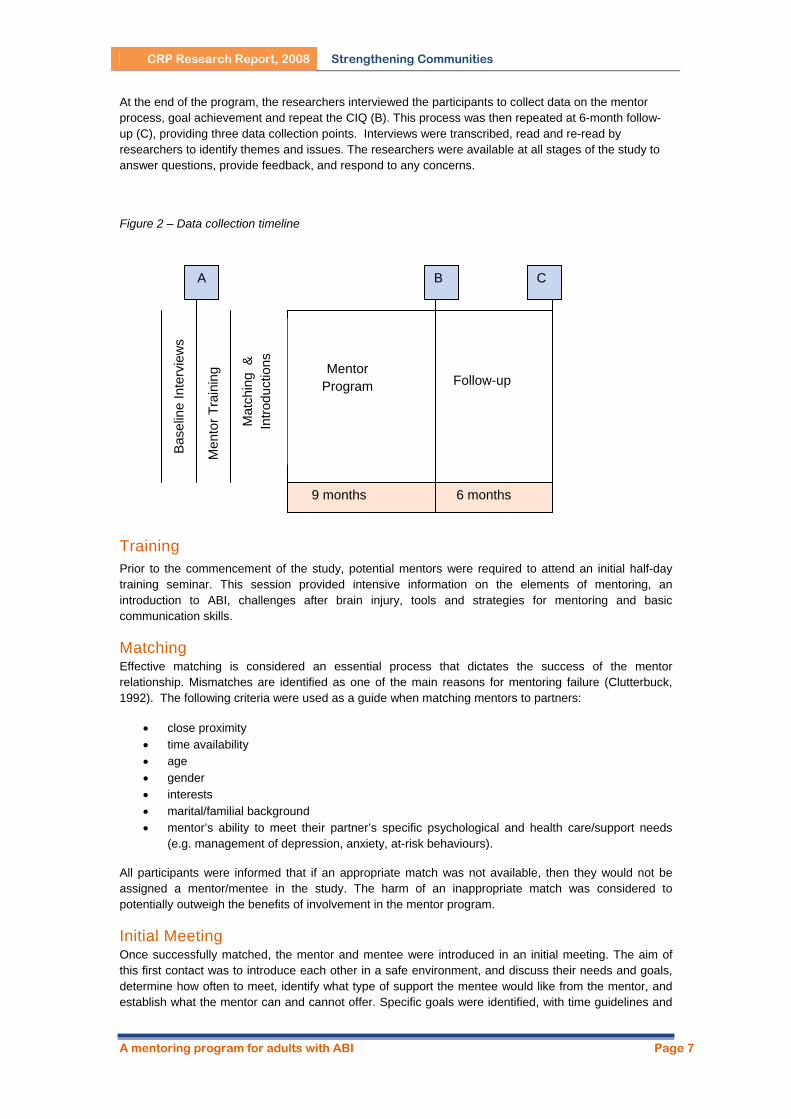
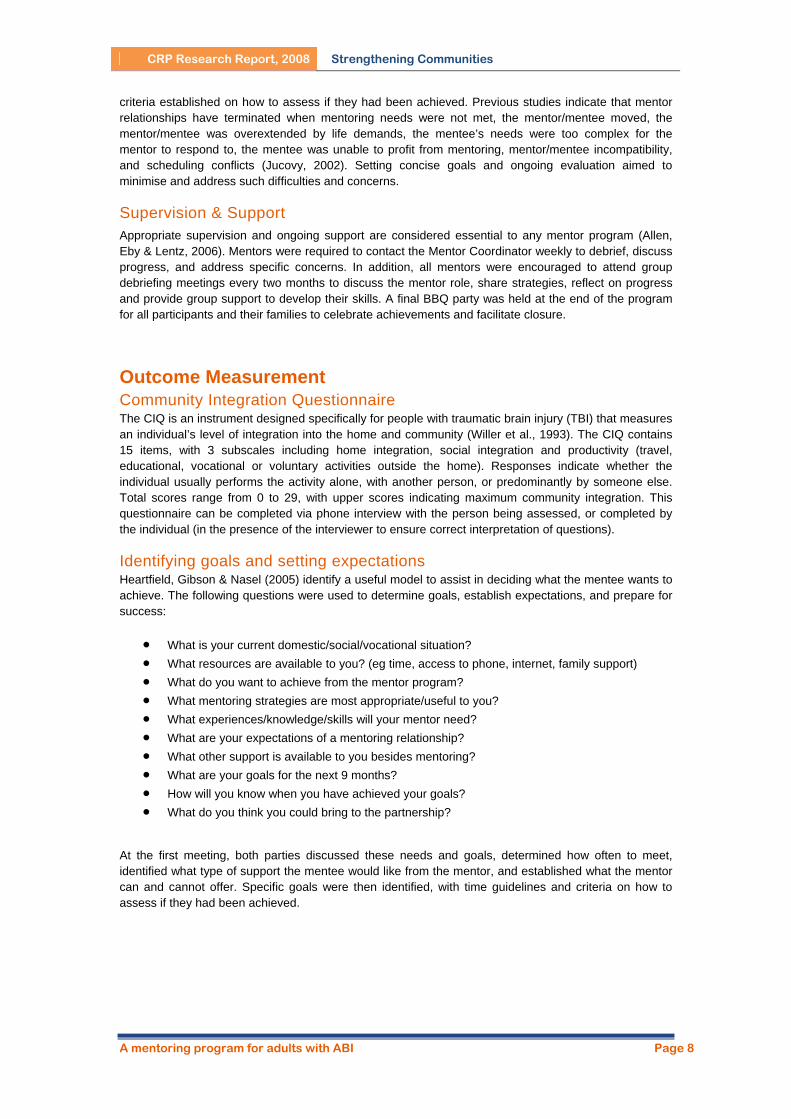
Procedures Data Collection The researchers met with each volunteer prior to commencement of the study (see Figure 2). The volunteers wishing to be involved in the study were informed of the aims and purpose of the research, the nature of their involvement, how the data will be used, and their right to withdraw from the study at any time. An informed consent form was then signed, followed by a semi-structural informal interview (A). Further information was gathered through participant observation, collation of diagnostic and demographic information and administration of the Community Integration Questionnaire (CIQ) (Willer, Rosenthal, Kruetzer, Gordon & Rempel, 1993).
Both mentee and their nominated significant other (eg eg mother, wife, or long-term support worker) completed the CIQ independently. For individuals with short-term memory difficulties, the significant other’s perspective was recorded.
A mentoring program for adults with ABI Page 6
CRP Research Report, 2008 Strengthening Communities
At the end of the program, the researchers interviewed the participants to collect data on the mentor process, goal achievement and repeat the CIQ (B). This process was then repeated at 6-month follow-up (C), providing three data collection points. Interviews were transcribed, read and re-read by researchers to identify themes and issues. The researchers were available at all stages of the study to answer questions, provide feedback, and respond to any concerns.
Figure 2 – Data collection timeline
A
Bas
elin
e In
terv
iew
s
Men
tor T
rain
ing
B C
9 months
Mat
chin
g &
In
trodu
ctio
ns
Mentor Program
Follow-up
6 months
Training Prior to the commencement of the study, potential mentors were required to attend an initial half-day training seminar. This session provided intensive information on the elements of mentoring, an introduction to ABI, challenges after brain injury, tools and strategies for mentoring and basic communication skills.
Matching Effective matching is considered an essential process that dictates the success of the mentor relationship. Mismatches are identified as one of the main reasons for mentoring failure (Clutterbuck, 1992). The following criteria were used as a guide when matching mentors to partners:
• close proximity • time availability • age • gender • interests • marital/familial background • mentor’s ability to meet their partner’s specific psychological and health care/support needs
(e.g. management of depression, anxiety, at-risk behaviours).
All participants were informed that if an appropriate match was not available, then they would not be assigned a mentor/mentee in the study. The harm of an inappropriate match was considered to potentially outweigh the benefits of involvement in the mentor program.
Initial Meeting Once successfully matched, the mentor and mentee were introduced in an initial meeting. The aim of this first contact was to introduce each other in a safe environment, and discuss their needs and goals, determine how often to meet, identify what type of support the mentee would like from the mentor, and establish what the mentor can and cannot offer. Specific goals were identified, with time guidelines and
A mentoring program for adults with ABI Page 7
CRP Research Report, 2008 Strengthening Communities
criteria established on how to assess if they had been achieved. Previous studies indicate that mentor relationships have terminated when mentoring needs were not met, the mentor/mentee moved, the mentor/mentee was overextended by life demands, the mentee’s needs were too complex for the mentor to respond to, the mentee was unable to profit from mentoring, mentor/mentee incompatibility, and scheduling conflicts (Jucovy, 2002). Setting concise goals and ongoing evaluation aimed to minimise and address such difficulties and concerns.
Supervision & Support Appropriate supervision and ongoing support are considered essential to any mentor program (Allen, Eby & Lentz, 2006). Mentors were required to contact the Mentor Coordinator weekly to debrief, discuss progress, and address specific concerns. In addition, all mentors were encouraged to attend group debriefing meetings every two months to discuss the mentor role, share strategies, reflect on progress and provide group support to develop their skills. A final BBQ party was held at the end of the program for all participants and their families to celebrate achievements and facilitate closure.
Outcome Measurement Community Integration Questionnaire The CIQ is an instrument designed specifically for people with traumatic brain injury (TBI) that measures an individual’s level of integration into the home and community (Willer et al., 1993). The CIQ contains 15 items, with 3 subscales including home integration, social integration and productivity (travel, educational, vocational or voluntary activities outside the home). Responses indicate whether the individual usually performs the activity alone, with another person, or predominantly by someone else. Total scores range from 0 to 29, with upper scores indicating maximum community integration. This questionnaire can be completed via phone interview with the person being assessed, or completed by the individual (in the presence of the interviewer to ensure correct interpretation of questions).
Identifying goals and setting expectations Heartfield, Gibson & Nasel (2005) identify a useful model to assist in deciding what the mentee wants to achieve. The following questions were used to determine goals, establish expectations, and prepare for success:
• What is your current domestic/social/vocational situation? • What resources are available to you? (eg time, access to phone, internet, family support) • What do you want to achieve from the mentor program? • What mentoring strategies are most appropriate/useful to you? • What experiences/knowledge/skills will your mentor need? • What are your expectations of a mentoring relationship? • What other support is available to you besides mentoring? • What are your goals for the next 9 months? • How will you know when you have achieved your goals? • What do you think you could bring to the partnership?
At the first meeting, both parties discussed these needs and goals, determined how often to meet, identified what type of support the mentee would like from the mentor, and established what the mentor can and cannot offer. Specific goals were then identified, with time guidelines and criteria on how to assess if they had been achieved.
A mentoring program for adults with ABI Page 8
CRP Research Report, 2008 Strengthening Communities
RESULTS
Demographic & Diagnostic Data Demographic and diagnostic information of all participants are presented in Tables 1 and 2 (pseudonyms used to maintain confidentiality).
Table 1 – Demographic and diagnostic information for each participant
Mentee Gender Age Ave at trauma
Cause of ABI
GCS Mentor Gender Age
Alan M 32 30 MVA 3 Steve M 27 Julia F 33 12 MVA 5 Mina F 25 Jim M 60 52 MVA 7 Philip M 47 Simon M 29 20 MVA 5 Wayne M 23 Bonnie F 48 27 MVA 3 Kay F 47 Leon M 34 29 Drug o/d 14 Trevor M 22 Colin M 49 14 Fall N/A Marie F 42 Mean 41 26 33
Table 2 – Demographic information for each participant
Mentee Living arrangement Marital status
Transport Vocational/educational activities
Alan With carer Divorced Guardian Part time work & volunteer Julia Independent Divorced Own Unemployed Jim With carer Married Public Unemployed
Simon Independent Single Public/car Part time work Bonnie Independent Single Public Unemployed Leon Shared accommodation Single Guardian Unemployed Colin Shared accommodation Single Public Part time work
Case Studies Alan & Steve Alan is a 33 year-old man who experienced a traumatic brain injury in a motor vehicle accident at the age of 30 (GCS = 3). As a result of the injury, Alan experiences some difficulty with short-term memory and uses a variety of prompts and cues (including a whiteboard, daily planner, note pad and mobile phone) to compensate and provide structure. Alan can become very fatigued, although he is often unaware that this is the case. This may become more obvious with signs such as yawning, confusion, low concentration, and changes in mood, affecting Alan’s chances of returning to employment. Prior to his injury, Alan ran his own business as a tradesman and was newly married. He worked for a period of time in the Army Reserves, and enjoyed the physical and mental challenges of leading others. In particular, Alan has had many ranks of leadership and is still enthused by motivating people to achieve their full potential.
Two years after his brain injury, Alan’s relationship with his wife ended, and he is now living on his own. His relationship with his mother is of particular importance, as she plays a key role in helping him negotiate plan and organize his routine. Alan has carers provide 10 hours of support per week to help with meals and housework. Before starting the mentor program, his weekly activities included attending a community ‘shed’ program for men with ABI, martial arts classes for people with ABI, volunteer work twice a week at a local Aged Care home, and chess at an over 50’s centre. Alan describes that a lot of friends and relationships have ‘dropped by the wayside’ since the accident, and he is looking forward to developing a relationship which would help reduce the loneliness, increase his social stimulation and provide companionship from outside of the family.
A mentoring program for adults with ABI Page 9
CRP Research Report, 2008 Strengthening Communities
Steve is a 28 year-old male who is very sociable and enjoys physical activity. Steve has recently finished a University degree, and is now employed full-time in the disability sector. Steve initially met Alan through a community based integration program, where Steve was a University student on placement. Both men had a number of common interests and backgrounds, including experience in the Army, a competitive nature, and easy-going personalities. Steve wanted to maintain the positive relationship with Alan that he had built, and enthusiastically joined the mentor program. By coincidence, Steve and his fiancé had recently moved into a house on the same street as Alan’s parents. He enjoys lifting weights, running, bush walking, cycling, outdoor activities, as well as socialising with friends.
Goal Descriptions
Alan identified the following goals:
• Weekly visits to the gym to increase stamina, fitness and strength • Improve self-esteem and expand social networks • Reduce the amount of time needed to rest during the day • Explore either open or supported work opportunities
Relationship Development and Outcomes Both Alan and Steve started the program with energy and enthusiasm. For the first few months, Alan met Steve at his house, and they traveled to a nearby University gym together. Alan was also familiar with the location, as his martial arts workshops were held in the same building. Steve created a personal weights and cardio program for Alan which they followed when working out each week. After a few months, Alan began catching the bus and meeting Steve at the gym. Alan discussed with Steve the details of his recent divorce, how he was coping, as well as seeking advice on appropriate social behaviour and interactions with women.
Gradually, Alan and Steve extended their workout sessions to up to 2 hours. Alan and Steve progressed to meeting at the gym at the same time, but doing separate routines. Alan appeared confident in his workout, looked comfortable and socialized with other patrons of the gym. In addition, Alan began expressing new goals to Steve, including organising a walk to increase community awareness of ABI. Alan’s mother expressed that he was really benefiting from the mentor program, both physically and emotionally.
Alan’s confidence in the gym increased, and on a number of occasions he brought his friend Tim (a friend he met in rehabilitation) to the gym and encouraged him to join. This was seen as a very positive opportunity for peer mentoring in the future. Both Steve and Alan laughingly reported examples of increases in Alan’s self-esteem and body image, including a change from wearing baggy clothes to more tight fitting cut-off shirts which showed off his ‘guns’ (biceps). He would also bring magazines with ideas for different workout routines. By the end of the program, Alan had built a positive rapport with staff members at the gym who now knew him and asked where he was if he missed a session. On one occasion when Steve was sick, Alan took the initiative to go to the gym on his own accord – a positive indication that he felt confident enough to go to the gym alone.
Two months before the scheduled end of the mentor program, Steve spoke with Alan and his mother about future plans. It was decided that Steve would start to fade out the scheduled weekly meetings slowly and Alan would be encouraged to attend gym increasingly on his own. Steve and Alan planned on seeing each other in a more natural, unscheduled fashion after the end of the mentor program for occasional bike rides etc. Alan had recently invited Steve to his PATH (Plan to Achieve Tomorrow’s Hope) meeting (a goal-based program which includes all significant people in his life and aims to achieve his future goals in time framed steps). This allowed for greater coherence between all Alan’s supports, and strengthened his social networks.
Alan’s description of the mentor relationship is of a mutual friendship “I help Steve and he helps me – a lot of give and take”. Steve also positively described their time together “I really enjoyed it. Some days I might not want to go to gym, but I will because I know he’ll be there and we have a laugh, debrief, and watch the hot chicks – they’re very motivating!”
A mentoring program for adults with ABI Page 10
CRP Research Report, 2008 Strengthening Communities
Both described the mentor program as an opportunity to get to know each other better. Alan said “Steve is a good friend now. Not just like a mentor (someone who comes and goes), but a friend… I don’t want to let him down because we do have a good friendship now. And I see the benefit of gym. Having a goal is personally important. You have to use it or lose it!”
Alan felt he has succeeded in achieving his goals. “I can see my goals being met…to look like Arnie [Schwartzanigger]! [laughs]. I can see little improvements.” He reported increases in fitness and strength, his weight has increased, and he has gained increased movement in his right arm. During this time, Alan started work 2 days per week (4 hours per day) in a sheltered employment setting. Although Alan saw this as a positive step, he also felt “tired all the time. But I still made time for gym cause it’s a priority”. At the end of the program, Alan reported that he felt his endurance had improved – he noticed the fatigue less, and had increased his hours at work to 6 hours per day. “This week at work I wasn’t so tired. I can’t say what this is due to, but I’d like to think gym helped out a bit”.
By the 6-month follow-up period, Alan and Steve maintained phone contact as Steve and his partner had a baby. Although Alan understood Steve now had different family commitments, there had been no other social involvement or leisure activities in his routine. Alan did not continue attending the gym without Steve. However, Alan had successfully continued with his job, and reported a high level of satisfaction with his work. He also began a series of public awareness talks about ABI to primary schools with the support of a paid carer, which he found very rewarding.
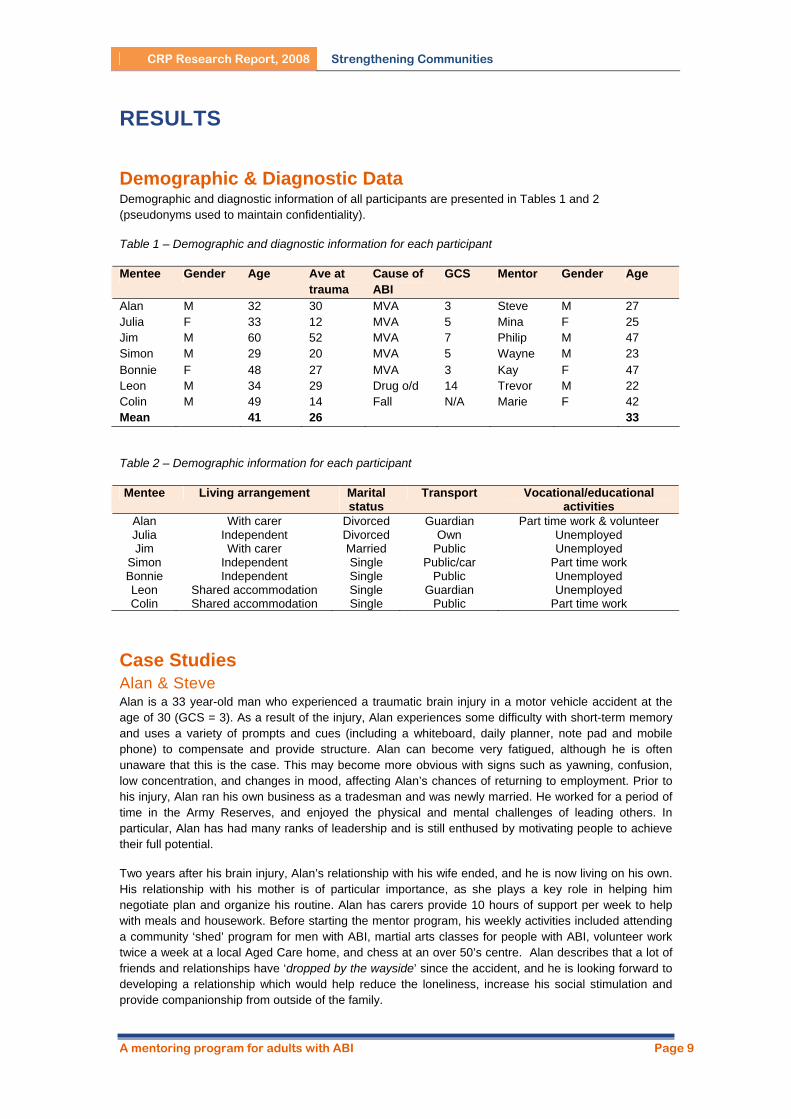
The graphs below illustrate Alan’s CIQ sub-score results from baseline to 6-month follow-up. By the end of the mentor program, there was no measured change in home or social integration scores, however the improvement of 2 points in productivity reflects his shift from unemployment to part-time work. Alan’s total CIQ score increased from 18 to 20 by the end of the program. However, changes are noted by the follow-up period. Home integration scores dropped slightly, as Alan identified that over this period he had less involvement in planning social arrangements, and a carer or family member had taken over this role. By the 6-month follow-up, Alan’s social integration scores dropped, reflecting a decrease in the number of leisure activities and visits to friends and relatives each month. Alan also identified that he no longer felt he had a best friend with whom to confide. In contrast, his productivity score was maintained as he successfully continued with part time work. It could be considered that his work has replaced the social contact and leisure time he once enjoyed.
A mentoring program for adults with ABI Page 11

CRP Research Report, 2008 Strengthening Communities
Julia & Mina Julia is a 34 year-old woman who, at 12 years of age, was hit by a car while riding her bicycle. She was in coma for 27 days with a GCS of 5. Long-term effects of this ABI include severe left-sided hemiplegia, and difficulty with short-term memory, initiating and persisting at tasks, motivation, planning, monitoring her social behavior and impulsivity. She often experiences dramatic mood swings, resulting in uncontrolled aggressive behaviour and language one moment, then sincerely apologetic the next. In addition to the effects of her brain injury, further medical complications including obesity, cellulitis, endrometriosis and reset bones limit Julia’s ability to move without pain. She is physically restricted to activities that do not require prolonged periods of exercise or movement (e.g. walking distances or climbing multiple stairs). These limitations have greatly affected Julia’s self-image and impacted further on levels of isolation.
Julia lives with her six-year old son in a house near her parents. She receives considerable support from her mother and father, including assistance in dressing, motivation to do daily tasks and support in parenting. Julia shares custody of her son with her ex-husband, who has access every second weekend. An important facet of her independence is her continued ability to drive, however she frequently receives support from her parents with transport when pain and fatigue limit her ability to drive herself. She frequently experiences severe depressive states which lead to feelings that no one cares for her, isolation, and thoughts of suicide. These periods come and go in cycles, and often follow ‘highs’ where her bubbly personality and enthusiasm are accompanied by a desire to be socially active and achieve. Julia engages in some risk-taking behaviours including binge eating, which are linked to her feelings of low self-esteem, poor body image, and periods of disinhibition.
Mina is a 25 year-old full time doctoral student. Mina and Julia met through the community integration program 3 years previously, and had developed a friendly relationship. Mina volunteered to participate in the program in order to strengthen her relationship with Julia, develop a routine, and help her to achieve her goals.
Goal Descriptions
Julia identified the following goals:
• Organise and run a beauty workshop • Find and maintain regular volunteer work • Increase physical activity and manage weight • Identify other ongoing social and community activities to develop and maintain motivation.
Julia wanted to re-engage in regular activities that help her feel proud and increase her motivation and confidence. “It would be great to get some motivation in my life, and make some more friends.”
Relationship Development and Outcomes
Julia and Mina met regularly once per fortnight for the nine month period. Their contact included meeting for coffee, dinners, shopping at the markets, cooking together, visiting the local library and phone conversations. According to Julia, “We hit it off straight away, and it’s continued like that”. Julia initiated most of the contact throughout the program, and Mina touched base with her via phone or SMS contact when needed. When organizing a social outing, Mina would also occasionally invite two or more of her friends.
An important facet of their relationship was providing feedback and support during periods of depression and stress. They would speak about her son and how Julia can support him, how Julia can positively interact with her parents, and manage her depression and binge eating patterns. Managing appropriate language and communication was a priority, as Julia would at times send multiple messages to Mina requesting they go out immediately. Mina felt this was inappropriate and excessive, and boundaries were addressed.
A major success for Julia included developing and successfully running a beauty workshop during this period. Together with Mina, Julia wrote down her ideas and they discussed what was realistic. They then wrote down step-by-step instructions for the workshop, and designed a flyer. Julia independently typed
A mentoring program for adults with ABI Page 12

CRP Research Report, 2008 Strengthening Communities
and printed her notes and handouts, and together they organized the catering. Unfortunately, on the eve of the workshop, Julia cancelled the event due to ill health. However, they successfully worked to reschedule the workshop, and Julia actively invited people from her social network to attend. With support to plan this event, Julia was able to achieve her goal of teaching others the skills she has learned in make-up and beauty. The workshop was received very positively, and the event was a success. Photos were taken to remind Julia of her achievement in times of depression and self-doubt.
Other goals were not so successful. With encouragement, Julia wrote her resume and filled out a job application at a local store, however she did not finish and send it off. This goal was not pursued due to Julia’s health difficulties (multiple hospital admissions) and her change in motivation. At this time, Mina traveled overseas for 6 weeks which may have impacted on the momentum of goal achievement, and interrupted the development of their relationship. Similarly, the goal to increase physical activity and manage Julia’s weight was not achieved. This is an ongoing issue, with long-term established patterns in binge eating closely corresponding with periods of low self-esteem and depression. Mina did report that by the end of the program, Julia would no longer binge eat in front of her.
Mina described the mentor relationship as natural and felt their friendship has strengthened. “I liked spending time with Julia. We always did something we BOTH wanted to do.” Mina felt that Julia and herself made a good match as they had an established friendship before the program. However, at times Julia would forget they were participating in a formal and managed mentor relationship, and when Mina would mention attending mentor program meetings, Julia would ask “what program?” Mina described having an established friendship before entering a mentor relationship as having a downside. She felt that mentors could set clearer boundaries in a professional relationship, with a greater chance of the mentee responding positively to being challenged. She found establishing this change in relationship difficult, however felt that they had achieved a number of successful outcomes. These included reducing her social isolation by introducing a range of social activities and interests, providing positive social reinforcement for appropriate behaviours, developing reality-based ideas, regulating negative self-talk and encouraging positive language about her-self and others. At the end of the program, the two intended to continue their relationship.
At 6-month follow-up, they had maintained contact. They both continued to call and go to lunch and shopping dates, however this contact became more irregular. Julia had also moved to live in a new home in the level above her parents. This decision was made by her family to reduce the costs of maintaining two homes, and to provide ongoing support for Julia and her son. Julia was excited and supportive of the move to a new house, and not overly concerned at the changes to her independence, as she would maintain a separate kitchen, living, bathroom and bedroom areas in her section of the house.
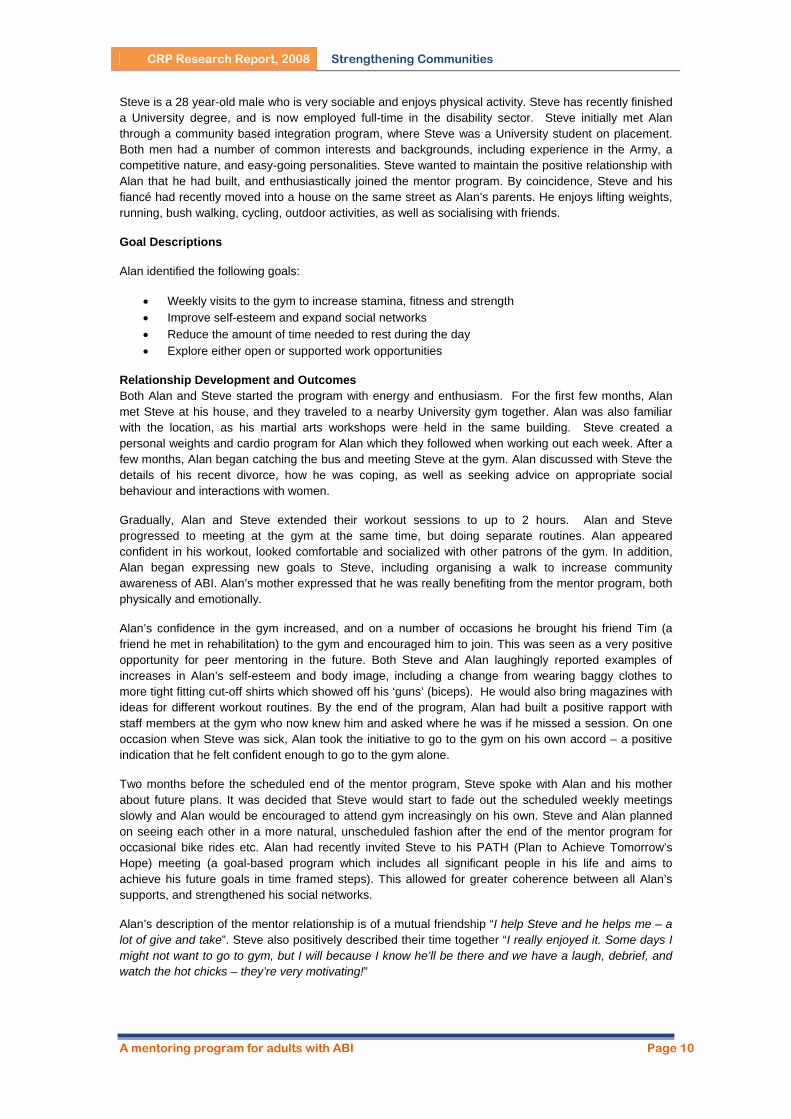
The graphs below illustrate Julia’s CIQ sub-score results from baseline to follow-up. By the end of the mentor program, there was a slight improvement in home integration scores due to Julia’s increased involvement in everyday housework, and a noticeable improvement in social integration scores reflecting an increase in leisure activities and visits to friends and family. No change was recorded in productivity as she did not commence study, voluntary or paid employment over this period. Julia’s total CIQ score moved from 15 to 19 by the end of the program. Unfortunately these reported improvements were not maintained by the follow-up, and returned to near baseline levels in all areas. This reflects the increased assistance her parents now provide by living with her.
A mentoring program for adults with ABI Page 13
CRP Research Report, 2008 Strengthening Communities
Jim & Philip Jim is a 60 year-old man who was involved in a car accident at the age of 52 (GCS = 7). This resulted in difficulties with short term memory, initiation, motivation, aggression, and balance. Prior to the accident, Jim worked in the navy, and he now enjoys recalling vivid memories of his travels. He carries with him a list of dates and ports he was stationed in to prompt his memory and provide conversation starters. Jim finds it difficult to suggest activities he would like to do, but when given a choice, he happily selects from available options.
Jim is sociable and easy-going, and lives with his wife who plays a significant role in organizing his schedule and daily activities. His week is highly structured, and involves weekly woodworking in a community shed, attending writing and computing workshops twice a week, and a social group every second Friday night with the community integration program. Weekends are often spent looking after his grandchildren with his wife.
Philip is a 47 year-old man who works full time as a train driver. Philip heard about the mentor program through his wife, who was studying at University and informed him of the program. A number of years previously, Philip had an aneurism, resulting in a mild brain injury and short period of rehabilitation. This has left him feeling extremely aware of how lucky he was to survive and escape serious disability. Philip was very keen to participate in the program, as he felt the need to help others with severe brain injury in whatever way he could. Philip mentioned that he could relate very well to the frustration of short-term memory loss, as he experienced similar difficulties shortly after his aneurism.
Goal Descriptions:
Jim identified the following goals:
• Expand social activities (e.g. walking, attending sporting events, learning how to sail, sharing computer interests)
• Maintaining anger management techniques, including deep breathing and relaxation • Revisit the possibility of regaining driving license (eg organizing an assessment to determine if
this is possible)
Relationship Development and Outcomes:
As Philip worked alternating afternoon and night shifts, they both decided that it would be best to approach the relationship flexibly, and arrange when to meet week by week. This was reviewed periodically to make sure it was meeting both their needs. They started by meeting in a local shopping complex for coffee to get to know each other better and find common interests. They both reported feeling a bit apprehensive at this time, and Philip gradually became aware of the extent of Jim’s memory difficulties.
One area that Philip reported finding challenging was Jim’s inability to generate new ideas for future activities. He first asked Jim to think about it for the next week, however Jim didn’t have any suggestions, and was happy to do whatever Philip suggested.
Jim’s wife quickly remarked that she didn’t want Jim going to coffee shops too often as he was putting on weight, and that previous carers had done only that activity with him. Philip was concerned that she
A mentoring program for adults with ABI Page 14
CRP Research Report, 2008 Strengthening Communities
saw him in that role. Instead, she suggested that they check out some walking trails, which is an activity Jim enjoys. Bush and beach walking soon became a regular activity and desired exercise for them both.
Philip sought to expand Jim’s interests, and brought him to a local soccer game, which he seemed to enjoy (even if he didn’t agree with the rules), went to the movies, museums and art galleries. On a couple of occasions, Philip encouraged Jim to be less reliant on his wife, and meet him across town by taking the bus. This was a successful experience, and increased Jim’s confidence and feeling of independence. Due to Philip’s shift work schedule, they only met on average once per fortnight, however this didn’t bother either of them, and Jim understood Philip’s time constraints.
Jim’s goal of regaining his driver’s license was not addressed in this period. Although he was still interested, this was not a high priority for their time together, and a medical assessment is still required.
Both men reported that they enjoyed the time they spent together, and developed a strong friendship. They were successful in identifying and engaging in a range of social and physical activities that they both enjoyed. There was no need to address any anger management issues, as these did not occur. Jim enjoyed the phone calls and social interaction with another man close to his age. Philip also described “We’re both simple guys, we have a leisurely stroke. We understand each other better now… Spending time with Jim helped me to look at things differently – appreciating what I’ve got.”
When the program had ended, they both planned to go out to dinner together with their wives. As Philip was about to start a new job interstate, they anticipated that their relationship would change, but they both planned to “keep the friendship going” and have a meal “now and then”. At 6-month follow-up, occasional phone contact was maintained.
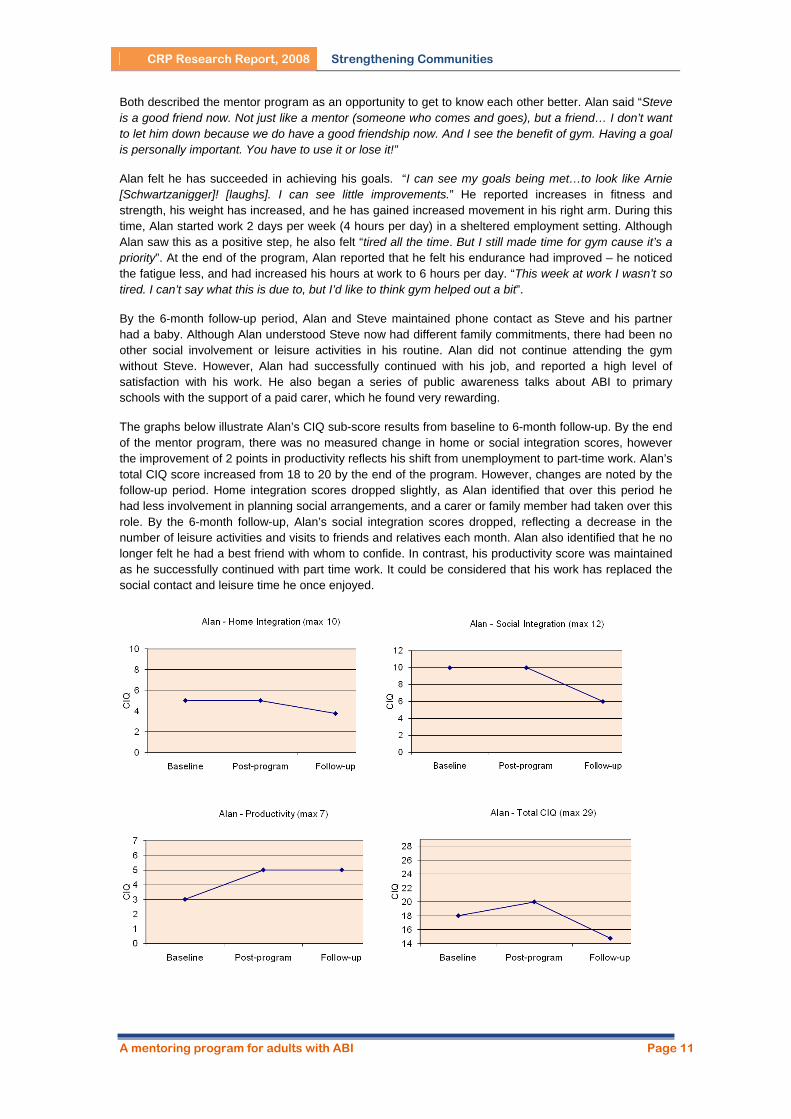
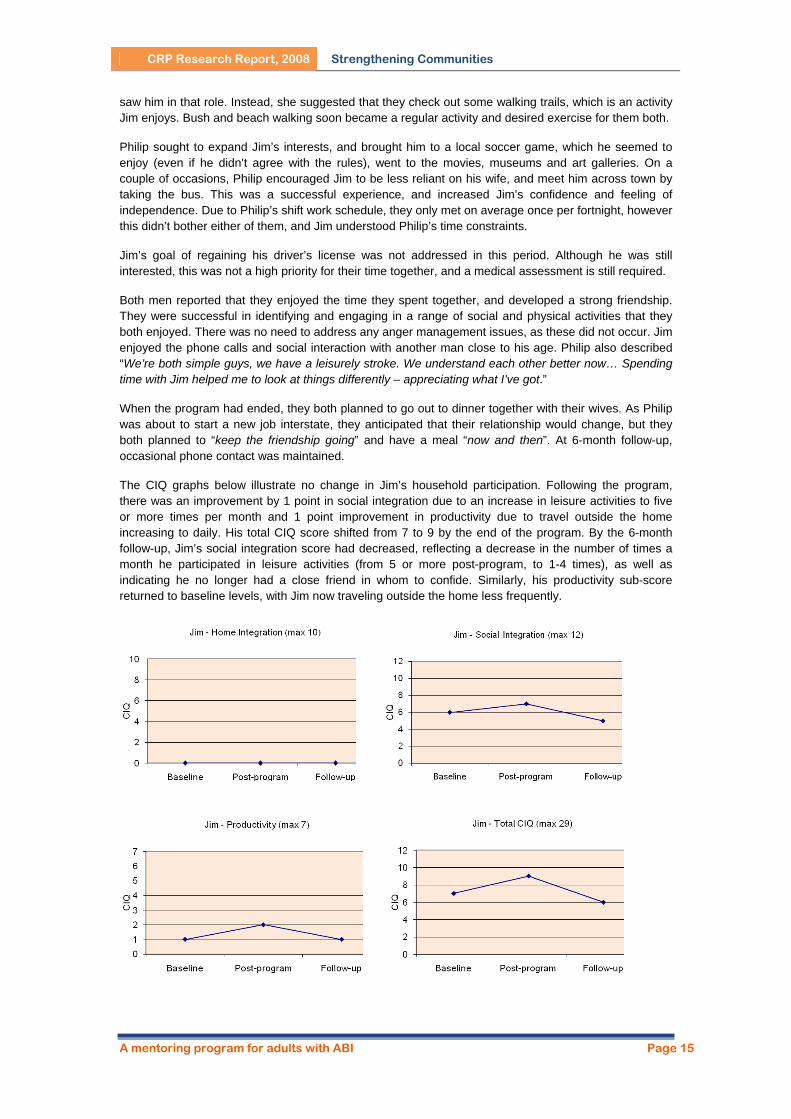
The CIQ graphs below illustrate no change in Jim’s household participation. Following the program, there was an improvement by 1 point in social integration due to an increase in leisure activities to five or more times per month and 1 point improvement in productivity due to travel outside the home increasing to daily. His total CIQ score shifted from 7 to 9 by the end of the program. By the 6-month follow-up, Jim’s social integration score had decreased, reflecting a decrease in the number of times a month he participated in leisure activities (from 5 or more post-program, to 1-4 times), as well as indicating he no longer had a close friend in whom to confide. Similarly, his productivity sub-score returned to baseline levels, with Jim now traveling outside the home less frequently.
A mentoring program for adults with ABI Page 15

CRP Research Report, 2008 Strengthening Communities
Simon & Bill Simon is a 29 year-old man who, at the age of 20, was hit by a car while riding his bicycle on his way to University. This resulted in right frontal and left temporal lobe damage, with a GCS of 5. Prior to the accident, Simon was an achieving young man with a high school scholarship and completing a University degree. Six months following the injury, Simon re-enrolled at University in an attempt to complete his second year. However, after two years of intermittent attempts, it became clear that Simon was unable to “think fast enough” and keep up with the demands of University.
Other reported changes subsequent to the brain injury included personality changes, loss of confidence and difficulty with decision-making. Simon also developed bipolar mood disorder post-trauma. Over the years, he has had a number of “severe bouts” which have resulted in periods of psychiatric admission. These mood changes were noticed in the first few months following the accident, and became worse 6 months later. He began to see a psychiatrist and began various anti-psychotic medications including Carbamazepine and Lithium. His mother reports “For some days, for 10 days he’d be dreadfully depressed and snap out of it like that, on top of the world and then it could change quite quickly again.” Simon can be very eloquent, and at such times describes his situation in the following terms “My brain is like swiss cheese – parts are unaffected and others are damaged” and “I’m on ice so thin you can barely even see it.” Since changing medications recently, Simon reports that these bouts have been less severe, with no psychiatric admissions for 2 years. Simon has been living independently in his own home across the street from his parents, working 3 days per week (5 hours per day) at a local supermarket stocking shelves and organizing the trolleys, participating in a mixed social tennis team, attending church services and maintaining a personal exercise regimen (running and swimming 3 days per week). Simon joined the mentor program by stating “I don’t have much on at the moment. I’d mainly like someone to talk to, do stuff with, and eat!”
Bill is a single 24 year-old man who has recently finished his University degree in Psychology with honours. Bill heard about the program through the University advertisements, and volunteered as a mentor to gain experience in community integration for people with brain injury. As he had little experience in spending time with people with brain injury, Bill sought to extend his theoretical knowledge by meeting and developing a relationship with a participant in the program. Both men had a number of common interests in how the brain and body works, scientific and psychological theories, and an easy-going nature.
Goal Descriptions
Simon identified the following goals:
• To get to know each other and develop a natural friendship • Weekly social contact to expand range of social activities and networks. • Develop strategies to assist with difficulties in perceiving and interpreting others responses at
work and socially.
Relationship Development and Outcomes
Simon and Bill started by meeting each other weekly and engaging in activities such as tennis and walking Simon’s dogs. After one month, Bill started his first graduate job in a rural town 5 hours drive from Adelaide, which changed the nature of their contact to weekly phone calls and e-mails. Once a month, Bill would return to Adelaide and catch up with Simon for a drink and meals with each other’s friends and family members. Although Simon was not concerned with this change, Bill would have preferred to have a more stable routine, and a set day when they ‘caught-up’. “We would organize to catch up on the fly. It would have been more satisfying and meaningful if we met in person. It wasn’t as personal, as easy to get invested over the phone.”
Simon described the relationship as “Just having a friend, going to town, someone to call and catch-up with. It was a friendship like any other – you meet when you can. It was fairly natural.” Simon and Bill frequently talked about girls, sharing advice and ‘consoling each other’ over ‘girl problems’. A frequent issue they would problem solve together was Simon’s feelings of paranoia concerning social interactions at work. For example, Simon would become consumed with concern whether he should say hello to a colleague at work, or wait for them to say something first. These dilemmas would take on enormous
A mentoring program for adults with ABI Page 16
CRP Research Report, 2008 Strengthening Communities
proportions, and result in Simon worrying and analyzing for days whether he did the right/wrong thing. Bill sought feedback and advice from the mentor coordinator on how to help Simon through these periods of stress, as well as his periods of depression. One lesson which Bill learned through this experience was the importance of active listening rather than providing advice and solving Simon’s problems. “A lot of the things Simon faces are beyond me. Whenever I felt that I had to give Simon advice, I felt uptight. The best time was when I opened up and said ‘I can’t fix your problems’, and Simon said ‘That’s fine! You talk to someone and there’s value in that’. I didn’t see that at first – it took a while for me to see that was a significant process”.
Both men describe the relationship as very reciprocal and mutual. Simon stated “I don’t think I need a ‘mentor’, Bill and I just help each other out. He’s a friend, someone to call up and talk to”. Bill similarly described the experience as “having someone extra to talk to. We share experiences and provide other opinions.” When Bill moved to the remote rural location for work, he shared his perceptions and difficulties fitting in with Simon, who offered reciprocal support. They had developed a very natural friendship centered on sharing experiences, new ideas, and supporting each other through personal difficulties and issues, which they both intended to continue beyond the program. Bill stated “We're getting on really well and I have come to value him in my life”. At the 6-month follow-up period, the two men had maintained phone and e-mail contact.
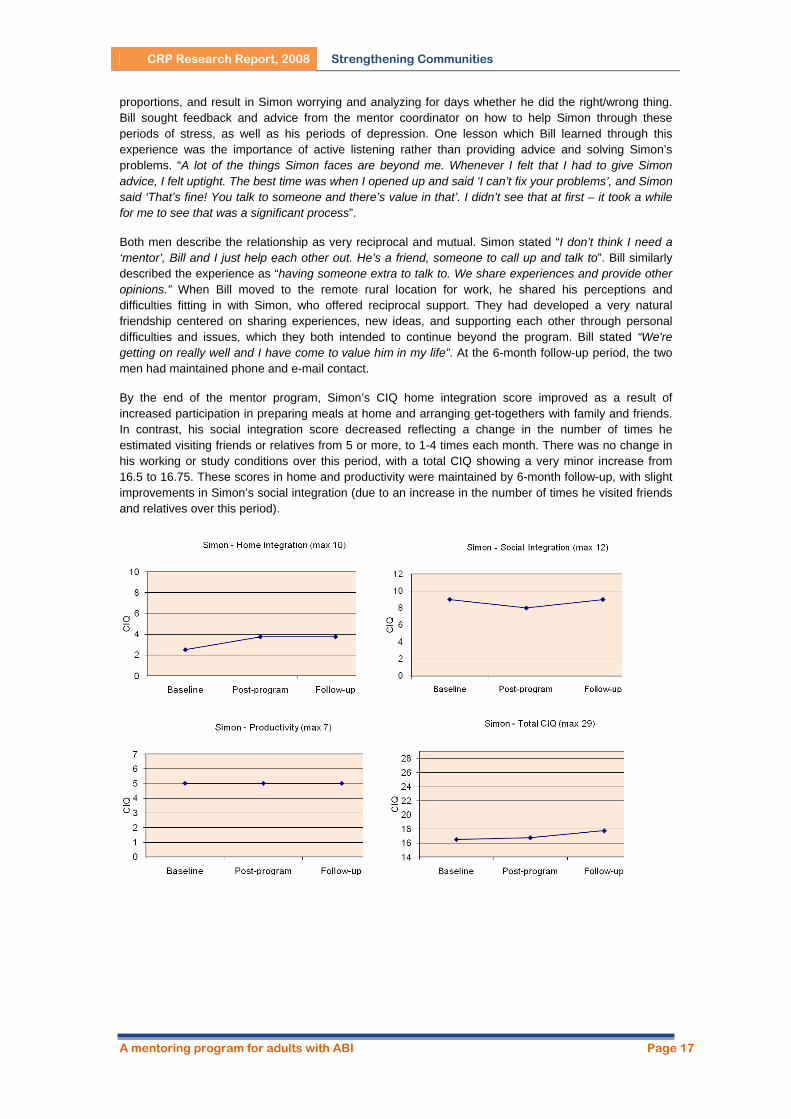
By the end of the mentor program, Simon’s CIQ home integration score improved as a result of increased participation in preparing meals at home and arranging get-togethers with family and friends. In contrast, his social integration score decreased reflecting a change in the number of times he estimated visiting friends or relatives from 5 or more, to 1-4 times each month. There was no change in his working or study conditions over this period, with a total CIQ showing a very minor increase from 16.5 to 16.75. These scores in home and productivity were maintained by 6-month follow-up, with slight improvements in Simon’s social integration (due to an increase in the number of times he visited friends and relatives over this period).
A mentoring program for adults with ABI Page 17

CRP Research Report, 2008 Strengthening Communities
Bonnie & Kay Bonnie is a fit and active 47 year-old woman. At the age of 26, she was involved in a motor vehicle accident, resulting in coma for 7 months (GCS = 3), loss of balance, uncoordinated gait and dysarthria. Prior to the accident, Bonnie was a nurse and lived with her husband. Tragically, her husband committed suicide three months into her coma. Bonnie has been living independently in her own unit for the past 9 years, and only visits her family who live in a rural town a few times each year. She is fiercely independent, and since the accident, has preferred to spend time by herself, refusing “companions who were sent” to spend time with her. At the time, she felt that she wanted to learn how to do tasks herself and not have someone who would do them for her.
Bonnie confidently uses public transport, enjoys shopping and chatting with friendly shop assistants in the city, and engages in volunteer work one day per week. She has a long-term relationship with a male friend who she visits weekly, and with whom she goes on holidays. Eighteen months ago, she started seeing a psychologist weekly and since this time feels her life has taken a turn for the better. “Even though I have always wanted to do something more with my life, now I feel a bit more impatient for something to happen… Now I feel ready to learn, I am ready to have a companion. As I still don’t feel confident to learn by myself, I am looking forward to having someone with me who will give me the confidence that I lack by myself.” Bonnie confides that she doesn’t feel very competent. She is not confident that she is able to retain what she is taught, and is very hesitant about undertaking new activities that require her to demonstrate that she is learning. Bonnie is often overwhelmed by feelings of self-doubt and loathing of her disability, however is hopeful that this can change. “I used to feel very proud of being able to do anything. Because I am less able, I feel less of a person. I would like to feel that I’m able to feel proud of being able to do something again.”
Kay is a 47 year-old full-time University student who has recently emigrated to Australia with her husband and adult children. Kay’s previous career was also as a nurse, and she shares an interest in sewing and craft. Kay was eager to learn more about how people live with a brain injury, beyond her acute care knowledge.
Goal Descriptions
Bonnie identified the following goals:
• Develop confidence and motivation with sewing and mending tasks • Complete a First Aid course • Explore and expand interests and participation in activities/groups in the community
Relationship Development and Outcomes
Bonnie and Kay joined the program with enthusiasm and optimism. At the start, Bonnie confronted Kay by questioning how much she was paid a week to spend time with her. It was explained that it was not a paid role, but a voluntary commitment. Due to their shared interests and background, the two developed a strong and reciprocal rapport very quickly. After their first meeting, Bonnie sent Kay an email, writing “for the first time I felt that someone was actually interested to find out what I wanted to do. This whole idea is so new to me, as I never felt that I was that important before". They began by meeting regularly each week for 5 hours at Bonnie’s home to attend to Bonnie’s pile of sewing and mending tasks. The five hour time commitment was soon too difficult for Kay to continue, and she negotiated with Bonnie to bring this back to 2-3 hours per week.
As a new immigrant, one of Kay’s own goals was to be integrated into the Adelaide community. Together, they participated in a variety of community activities, starting with Bonnie teaching Kay how to use the Adelaide public transport system. Over the 9-month period, they went shopping, visited Adelaide landmarks, Bonnie took Kay to her manicurist, and held dinners at each others’ house.
Kay expressed concern about Bonnie’s strongly negative self-perception and self-esteem. A few months into the program, Kay attended a session with Kay and her psychologist, where Kay was given strategies to counteract her negative self-talk. Kay also acted as an impartial sounding board for Bonnie by listening and helping her sort through and problem solve issues.
A mentoring program for adults with ABI Page 18
CRP Research Report, 2008 Strengthening Communities
Bonnie asked Kay to research first aid courses in Adelaide to determine which would suit her and make her feel welcome. Together they completed the preparation material and successfully completed the 2-day training sessions. Despite acute anxiety prior to the course, Bonnie asked questions freely, contributed well and appeared to be comfortable in the company of the group. After being briefed by Kay in advance, the instructor asked Bonnie when they arrived whether she was comfortable to do the assessment with the other members of the group or whether she would be more comfortable doing the assessment during the lunch break. Bonnie and Kay both did their assessment during the lunch break, which they independently passed. The afternoon session ended with a 40 mark multiple choice question sheet which Bonnie completed alongside Kay and other members of the course. Bonnie took a little longer to complete the questions but she passed the course – a positive affirmation of her capabilities.
Although the first two goals were achieved, attempts to encourage Bonnie to join new groups and social activities were met with resistance. She stopped her volunteer work part way through the year, and did not replace this activity.
Bonnie reported that she felt that she had gained a new friendship, which she would like to continue after the program came to an end. This was of enormous value to her and she enjoyed the “warmth” that this relationship had brought her. Bonnie also felt that she had gained the confidence to feel more “capable” and motivated to undertake activities like sewing, mending and knitting. With Kay’s encouragement, she had made a Duvet cover, quilt and a red jumper, which she was proud and pleased with.
Bonnie also admitted that she was now “less reluctant and less frightened about opening my mouth to speak to others”. She reported no longer feeling as frightened that strangers will be unable to understand her. After a few months, she developed confidence to leave messages and speak with Kay’s son on the phone. She also initiated a conversation with a stranger on the bus which she acknowledged was a significant positive step and that she will certainly consider doing this again, “I feel in control of the situation”.
According to Bonnie, a mentor is “someone who I can get advice from, someone who gives you options to consider when making up your own mind about something… they are someone who makes you feel like you have a purpose in life… a mentor is like a sister relationship”.
Bonnie shared that she wanted to “find a purpose for my life… I want to know that I can make a difference and contribute to society”. Future goals she identified were to talk to the community about ABI, join a bushwalking group, and to audit a University subject in the following year. Together with Kay, she brainstormed ways to achieve these goals. Although the formal relationship had ended, the two decided to continue their friendship in a less structured way, and continue to work towards achieving these goals.
At the 6-month follow-up, Bonnie had been introduced to a new mentor, and had begun to audit a first year University topic. They also identified a walking group, however the pace was too fast, and Bonnie felt uncomfortable in continuing with the group. Kay and Bonnie had continued their social contact on a monthly basis, with reciprocated phone calls and coffee dates.
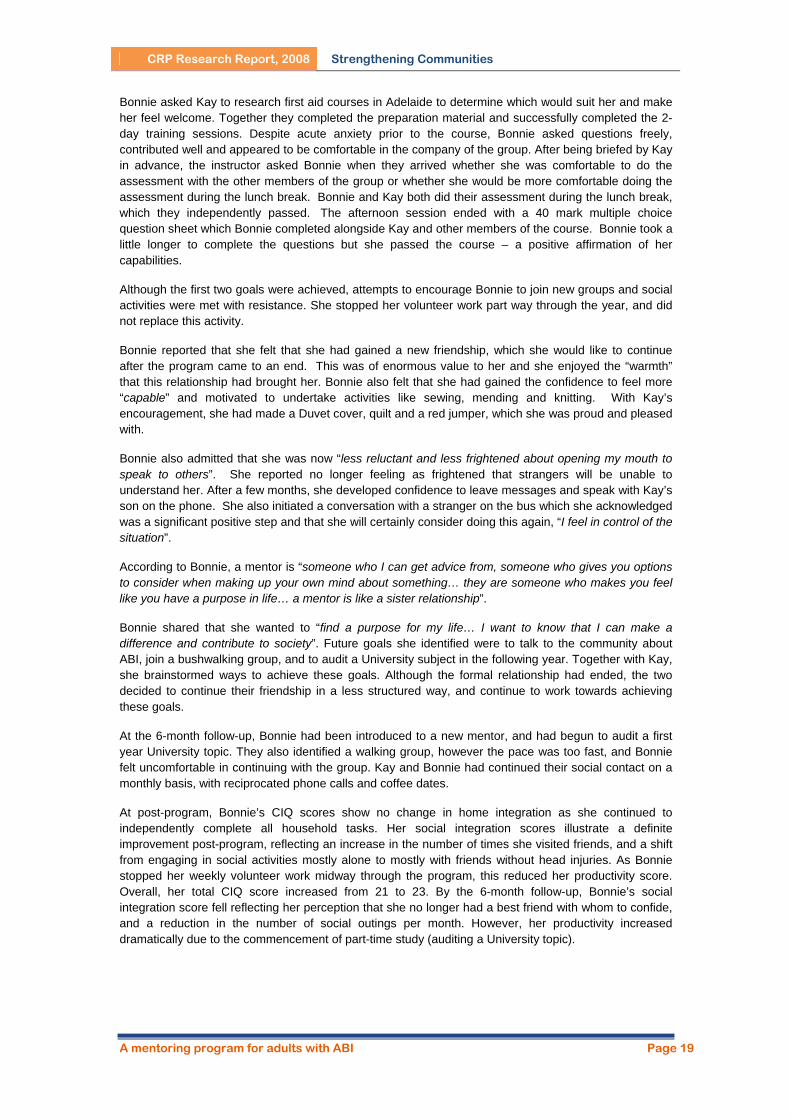
At post-program, Bonnie’s CIQ scores show no change in home integration as she continued to independently complete all household tasks. Her social integration scores illustrate a definite improvement post-program, reflecting an increase in the number of times she visited friends, and a shift from engaging in social activities mostly alone to mostly with friends without head injuries. As Bonnie stopped her weekly volunteer work midway through the program, this reduced her productivity score. Overall, her total CIQ score increased from 21 to 23. By the 6-month follow-up, Bonnie’s social integration score fell reflecting her perception that she no longer had a best friend with whom to confide, and a reduction in the number of social outings per month. However, her productivity increased dramatically due to the commencement of part-time study (auditing a University topic).
A mentoring program for adults with ABI Page 19
CRP Research Report, 2008 Strengthening Communities
Leon & Trevor Leon is a 34 year-old man who is interested in the arts, film, movies, music and writing. Prior to his brain injury, Leon studied film at university, and made short films which were positively received and of which he speaks of fondly. Leon experienced a hypoxic brain injury as a result of a drug overdose at the age of 29 (GCS = 14). This resulted in severe cognitive difficulties, disorientation, behavioural difficulties and significant difficulty with short-term memory. Leon finds it difficult to follow conversations, instructions and tasks. He has often forgotten what task he is engaged in before he completes it. Consequently, he needs assistance, encouragement and prompts constantly. Leon has great difficulty with his perception of time. He doesn’t know how long ago an event happened and will often talk about events in the present when they happened some ten years ago. This can be confusing and information he gives is often unintentionally misleading. Further assistance is required with positioning as Leon is often disoriented and unaware of his environment. Even though Leon experiences a number of difficulties, he is articulate and fluent, and has developed strategies to hide his confusion and engage with others socially. He has demonstrated evidence of implicit learning during drama rehearsals where he follows stage directions and incorporates feedback in his delivery of lines over time.
Leon has a very supportive family, who he frequently visits. Although his parents are not his official guardians, they control his finances. Leon is single and lives in shared and supported accommodation with 16 hours of social and recreational support each week. Leon is a solitary individual, who has expressed enjoyment in creative writing, going to coffee shops, visiting libraries and bookshops and viewing films. Leon is involved in few community-based activities, but manages to attend writing and creative arts workshops weekly, at a community based integration program.
Trevor is a 23 year-old male who volunteered for the mentor program through the University because he wanted to expand his experience working with people and learn to apply skills. Trevor has completed a Psychology degree with Honours, about which he is passionate. Trevor is single, lives with his family, and uses public transport. Trevor is interested in concerts of Australian bands, art, cartoon and real-life drawing, clay and materials, sculpture and story writing. Trevor expressed an interest in the program because it sounded fun and rewarding, and he wanted to gain broader work experience.
A mentoring program for adults with ABI Page 20
CRP Research Report, 2008 Strengthening Communities
Goal descriptions
Leon’s parents identified the following goals:
• Fortnightly visits to films/performances, internet cafes etc to practice communication and social skills and increase the number of activities Leon participates in the community to decrease social isolation
• Publish Leon’s writing in an online forum
Relationship Development and Outcomes
Despite a positive beginning, there were a number of challenges that led to the relationship stalling. Shortly after Leon and Trevor had been matched, Trevor commenced a full time graduate job, resulting in difficulty coordinating schedules. Due to Trevor’s changing shift work schedule, it was not until four weeks into the program that Trevor could visit Leon as arranged. On the first visit to Leon’s home, Leon was not home, as another support worker was uninformed of Trevor and Leon’s plans. It became apparent that there was little cohesiveness between many people in Leon’s life. Trevor debriefed with the Mentor Coordinator about this, and decided that meeting Leon’s parents may help. The Mentor Coordinator and Trevor met with Leon’s parents and discussed possible activity suggestions for Trevor and Leon. Some of these included publishing Leon’s writing online as Leon has previously expressed the desire to do this, taking up photography, making some short films and/or becoming part of a group who publish their work or discuss film.
Leon’s parents discussed Leon’s current social networks and supports. In their opinion Leon’s current accommodation situation was successful, and in recent days Leon had been more motivated than he has been in the past. They felt this may be due to Leon’s involvement in the aforementioned drama production. Leon’s parents explained that although Leon has severe short-term memory difficulties, it was apparent that consequent to the production, there was some improvement to Leon’s performance over time, and felt that Leon was the happiest they had seen him after the production. Leon’s parents explained that pre-injury Leon was a solitary individual with few friends, and expressed that they would not be surprised if Leon did not want to meet new people and be part of numerous social activities (such as playing pool etc).
It was seven weeks into the program when Leon and Trevor went for coffee and spoke about activity ideas. Due to Leon’s short-term memory loss, he had no idea who Trevor was (although they had spoken on the phone the previous night). However when Trevor mentioned to Leon that he was part of the same community based integration program that Leon attends, he appeared to remember the positive relationship he has with this program, and said “Well, let’s go!” During their coffee, Trevor mentioned to Leon the possibility of having work published online and Leon expressed that he would love to explore this further.
Ten weeks into the program Trevor and Leon met again. Trevor explained that Leon was less personable than the first time they met and appeared to be tired. They didn’t meet again for another six weeks. The Mentor Coordinator was in constant communication with both Leon and Trevor. Even though Trevor was finding it difficult to commit time to meeting Leon he still wished to be part of the program, and would continue to attempt to meet with Leon. It was evident that they were not meeting because of logistical reasons.
Trevor attended the Mentor Debriefing meetings as well as keeping in contact with the Mentor Coordinator fortnightly. The relationship was formally called to an end after 7 months. The final interviews were conducted separately. In this meeting, Leon did not remember Trevor at all. Leon has one significant support worker who has been a constant in his life over the past five years. Rob sees Leon three times a week to facilitate a range of social activities. A deep mutual respect between the two is evident. Rob explained that he saw effective mentoring as expanding Leon’s real interests. Rob explained that the challenges for Leon were not seeing Trevor very frequently and not hearing much from him. No major changes have occurred in Leon’s life over the last seven months, apart from minor changes in support workers.
Trevor explained that his relationship with Leon had very much a ‘living for the moment’ mentality. Although the goal of publishing Leon’s writing was articulated by Leon and his parents, Trevor found that
A mentoring program for adults with ABI Page 21
CRP Research Report, 2008 Strengthening Communities
Leon’s motivation would shift from moment to moment, and he did not want to ‘coerce’ Leon into doing an activity that he didn’t want to do at the time. The few occasions they met were spent having coffee and going to a bookshop. The goal of putting his poetry on-line was not achieved, primarily due to infrequent contact. It was clear that it was difficult for Trevor to establish a relationship with Leon, both due to work commitments, as well as the difficulty in coming to terms with Leon’s memory difficulties resulting in missed opportunities to enrich and extend Leon’s writing and related activities.
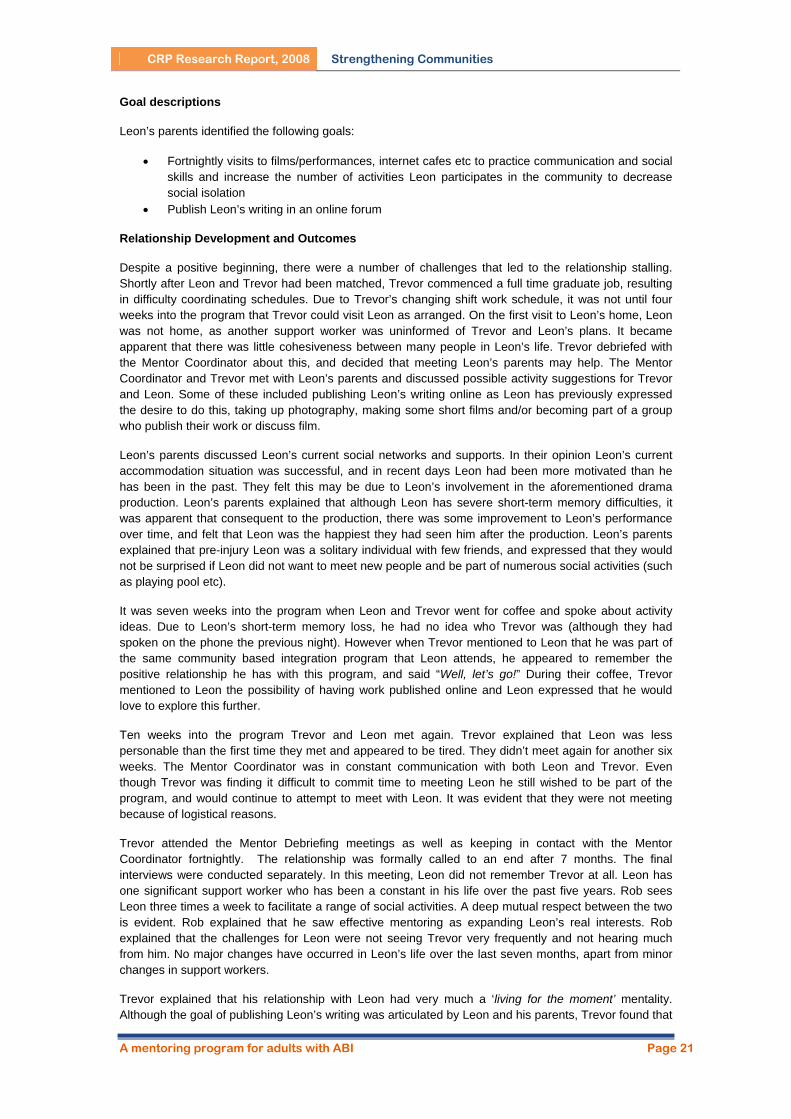
There were no changes in Leon’s home, social or volunteer/study/work life over this period, which is reflected in the unchanged scores on his CIQ. By 6-month follow-up the only change which was reflected in the CIQ was a decrease in the number of times he traveled outside the home, from almost every day, to almost every week.
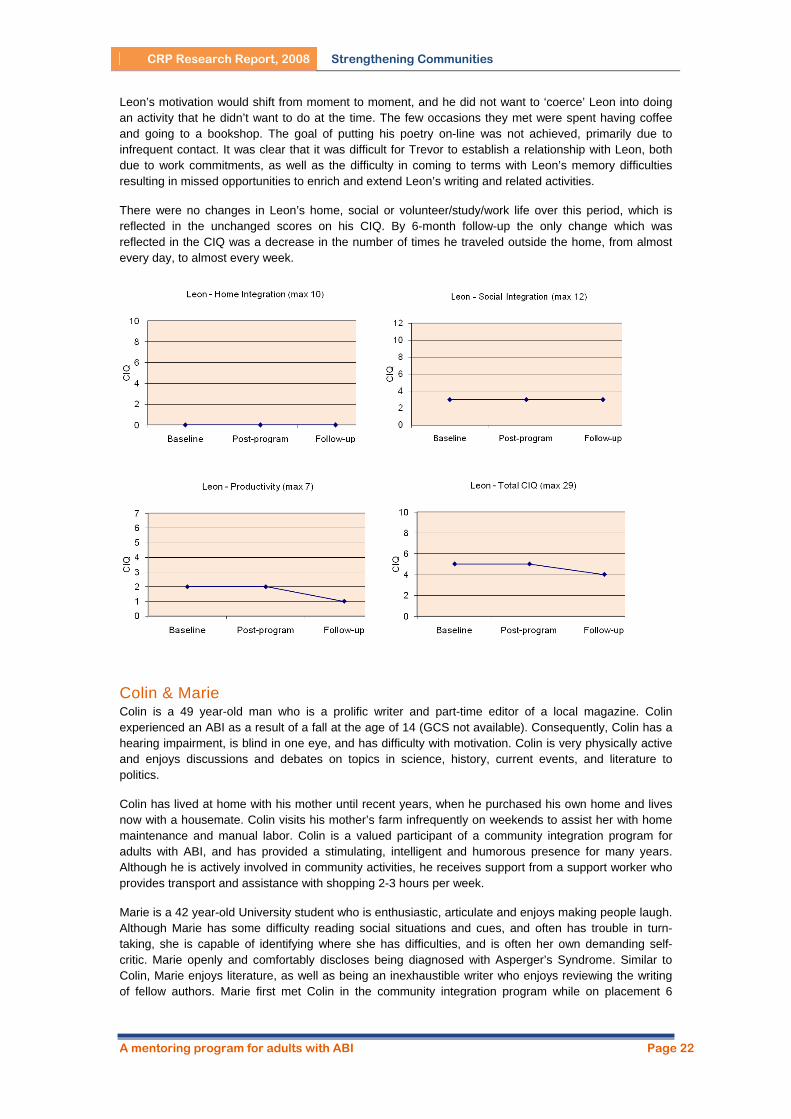
Colin & Marie Colin is a 49 year-old man who is a prolific writer and part-time editor of a local magazine. Colin experienced an ABI as a result of a fall at the age of 14 (GCS not available). Consequently, Colin has a hearing impairment, is blind in one eye, and has difficulty with motivation. Colin is very physically active and enjoys discussions and debates on topics in science, history, current events, and literature to politics.
Colin has lived at home with his mother until recent years, when he purchased his own home and lives now with a housemate. Colin visits his mother’s farm infrequently on weekends to assist her with home maintenance and manual labor. Colin is a valued participant of a community integration program for adults with ABI, and has provided a stimulating, intelligent and humorous presence for many years. Although he is actively involved in community activities, he receives support from a support worker who provides transport and assistance with shopping 2-3 hours per week.
Marie is a 42 year-old University student who is enthusiastic, articulate and enjoys making people laugh. Although Marie has some difficulty reading social situations and cues, and often has trouble in turn-taking, she is capable of identifying where she has difficulties, and is often her own demanding self-critic. Marie openly and comfortably discloses being diagnosed with Asperger’s Syndrome. Similar to Colin, Marie enjoys literature, as well as being an inexhaustible writer who enjoys reviewing the writing of fellow authors. Marie first met Colin in the community integration program while on placement 6
A mentoring program for adults with ABI Page 22

CRP Research Report, 2008 Strengthening Communities
months before the mentor program began. Due to a busy schedule, Marie was not able to attend the mentor training session, or the first mentor debrief meeting with other mentors.
Goal Descriptions Colin and Marie identified the following goals:
• to meet weekly to discuss and read/review each other’s writing, and explore social activities (eg golf, ten pin bowling and lawn bowls)
• improve Colin’s motivation, including home maintenance, clearing the garden and mowing the lawn
• complete a first aid course • provide moral support and motivation with University study.
Relationship Development and Outcomes
Both Colin and Marie were enthusiastic about starting the program. In the initial meeting, they engaged in witty and clever conversations, bouncing off the other’s word play and shared humor. They arranged to meet each week to review their writing, then go out and have coffee.
Although they tried to maintain flexibility in their regular contact, this was unsuccessful. Colin and Marie spent their second meeting at a local marketplace. A fortnight later, they managed to meet again to play golf and have lunch. Both Colin and Marie reported that they enjoyed the time spent together, but further contact did not proceed as planned. It was at this time that Colin was starting to experience the effects of pressure from increasing work hours and the possibility of starting a University degree, with scholarship support from his place of employment. Colin had experienced periods of depression for some twenty years. His experience of depression intensified during this period of increasing workload, conflict with his housemate, and the delicate balance of juggling numerous schedules. Despite the positive start there were challenges that led to the relationship ending after four months.
Colin stopped meeting Marie and did not answer phone calls. A number of meetings were held with Marie and Colin separately and together to identify and problem solve these difficulties. The goals were reviewed, and Colin described that he felt the mentor program was an academic and social opportunity and did not want to cease his involvement. Colin said he wanted Marie to help with motivation with study, bounce his ideas off, and discuss the content of the lectures. Marie planned to attend lectures with Colin to provide support.
Due to a miscommunication, Marie missed Colin’s first lecture. Colin stopped attending classes, and for the next month did not return the messages which Marie left for him. Once Colin could be contacted by the Mentor Coordinator, another meeting was held to help clarify and address the issues. It was unclear whether Colin’s withdrawal was due to his desire to discontinue involvement with Marie, or mounting pressures and the introduction of new significant expectations and responsibility. During this meeting Colin explained that he had decided to defer his studies until the following year, due to his work pressure and the feeling of trying to stay afloat. He was highly apologetic for the lack of communication, they wished each other well and ended the mentor relationship. Colin explained that he was beginning to seek professional help in managing his depressive behaviors and that he was looking for avenues to change his housing situation, which was a major cause of stress in his life. They both accepted the end of the relationship amicably and appeared to have a positive emotional response to the closure.
It appeared from initial meetings that Colin and Marie had similar definitions of mentoring. However, by the 4-month closure there were noticeable differences in role expectations. Colin felt there was confusion regarding who was the mentor, and what role they had. In the past, Colin perceived his involvement in social and community activities as that of a mentor. He expressed that the assumption that Marie was the mentor may have led to failure of the relationship. Colin felt that the relationship should not involve any member feeling superior, consequently leading to different expectations of each other. Marie stated a power imbalance was present due to the relationship beginning as fabricated akin to a client/worker relationship. Marie felt that if this relationship continued, it might have developed closer to a mentor/friend-like relationship.
Marie reflected she felt frustrated because she did not understand why Colin was avoidant and distant, as he did not disclose what he was experiencing at the time. She shared that she felt the relationship
A mentoring program for adults with ABI Page 23
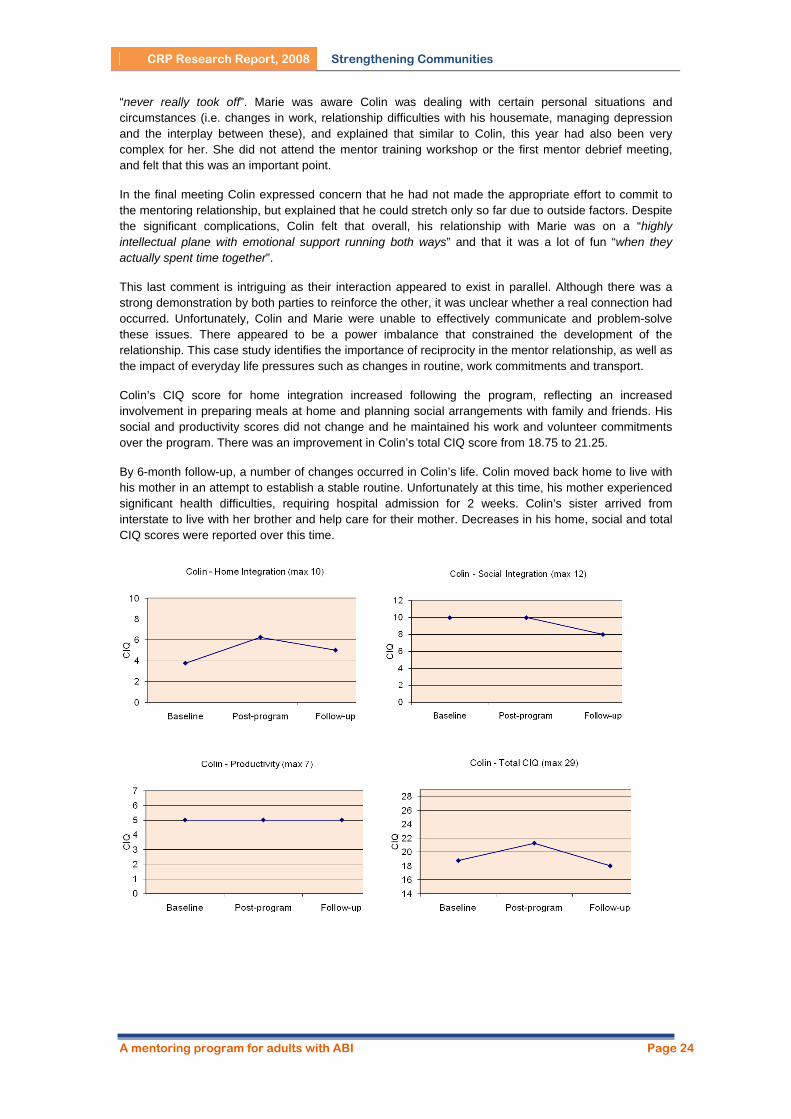
CRP Research Report, 2008 Strengthening Communities
“never really took off”. Marie was aware Colin was dealing with certain personal situations and circumstances (i.e. changes in work, relationship difficulties with his housemate, managing depression and the interplay between these), and explained that similar to Colin, this year had also been very complex for her. She did not attend the mentor training workshop or the first mentor debrief meeting, and felt that this was an important point.
In the final meeting Colin expressed concern that he had not made the appropriate effort to commit to the mentoring relationship, but explained that he could stretch only so far due to outside factors. Despite the significant complications, Colin felt that overall, his relationship with Marie was on a “highly intellectual plane with emotional support running both ways” and that it was a lot of fun “when they actually spent time together”.
This last comment is intriguing as their interaction appeared to exist in parallel. Although there was a strong demonstration by both parties to reinforce the other, it was unclear whether a real connection had occurred. Unfortunately, Colin and Marie were unable to effectively communicate and problem-solve these issues. There appeared to be a power imbalance that constrained the development of the relationship. This case study identifies the importance of reciprocity in the mentor relationship, as well as the impact of everyday life pressures such as changes in routine, work commitments and transport.
Colin’s CIQ score for home integration increased following the program, reflecting an increased involvement in preparing meals at home and planning social arrangements with family and friends. His social and productivity scores did not change and he maintained his work and volunteer commitments over the program. There was an improvement in Colin’s total CIQ score from 18.75 to 21.25.
By 6-month follow-up, a number of changes occurred in Colin’s life. Colin moved back home to live with his mother in an attempt to establish a stable routine. Unfortunately at this time, his mother experienced significant health difficulties, requiring hospital admission for 2 weeks. Colin’s sister arrived from interstate to live with her brother and help care for their mother. Decreases in his home, social and total CIQ scores were reported over this time.
A mentoring program for adults with ABI Page 24
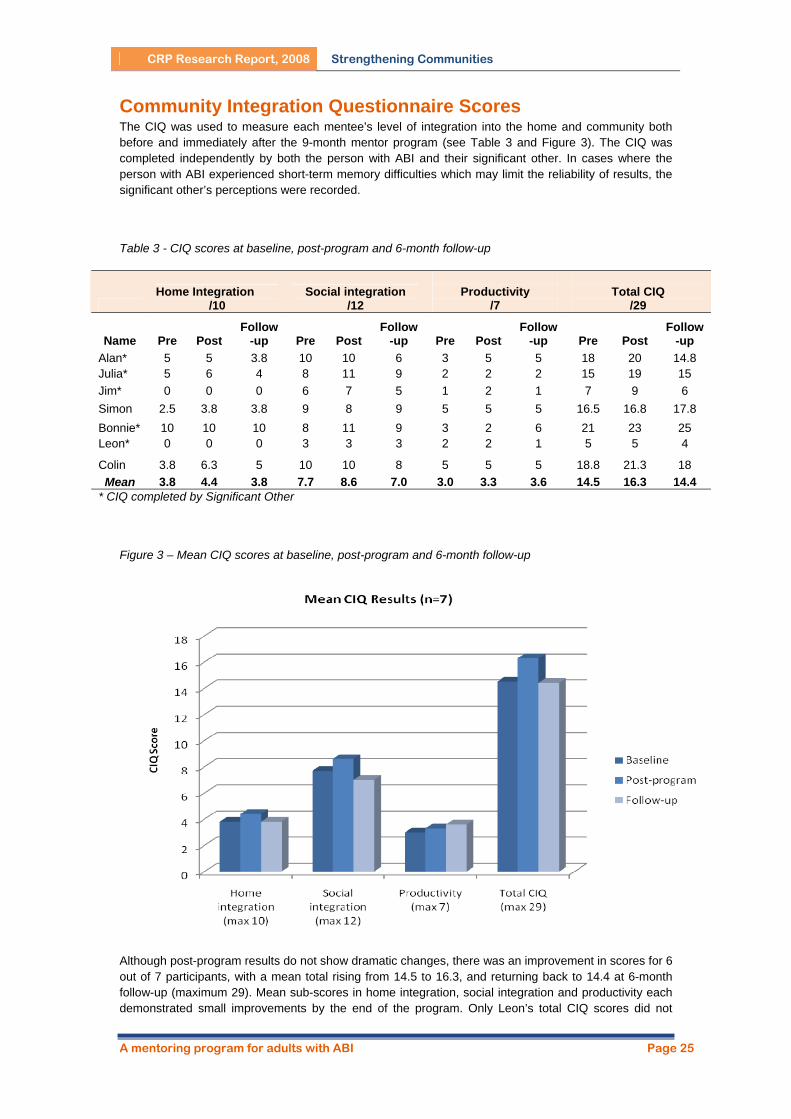
CRP Research Report, 2008 Strengthening Communities
Community Integration Questionnaire Scores The CIQ was used to measure each mentee’s level of integration into the home and community both before and immediately after the 9-month mentor program (see Table 3 and Figure 3). The CIQ was completed independently by both the person with ABI and their significant other. In cases where the person with ABI experienced short-term memory difficulties which may limit the reliability of results, the significant other’s perceptions were recorded.
Table 3 - CIQ scores at baseline, post-program and 6-month follow-up
Home Integration
/10 Social integration
/12
Productivity
/7
Total CIQ
/29
Name Pre Post Follow
-up Pre Post Follow
-up Pre Post Follow
-up Pre Post Follow
-up Alan* 5 5 3.8 10 10 6 3 5 5 18 20 14.8 Julia* 5 6 4 8 11 9 2 2 2 15 19 15 Jim* 0 0 0 6 7 5 1 2 1 7 9 6 Simon 2.5 3.8 3.8 9 8 9 5 5 5 16.5 16.8 17.8 Bonnie* 10 10 10 8 11 9 3 2 6 21 23 25 Leon* 0 0 0 3 3 3 2 2 1 5 5 4
Colin 3.8 6.3 5 10 10 8 5 5 5 18.8 21.3 18 Mean 3.8 4.4 3.8 7.7 8.6 7.0 3.0 3.3 3.6 14.5 16.3 14.4
* CIQ completed by Significant Other
Figure 3 – Mean CIQ scores at baseline, post-program and 6-month follow-up
Although post-program results do not show dramatic changes, there was an improvement in scores for 6 out of 7 participants, with a mean total rising from 14.5 to 16.3, and returning back to 14.4 at 6-month follow-up (maximum 29). Mean sub-scores in home integration, social integration and productivity each demonstrated small improvements by the end of the program. Only Leon’s total CIQ scores did not
A mentoring program for adults with ABI Page 25
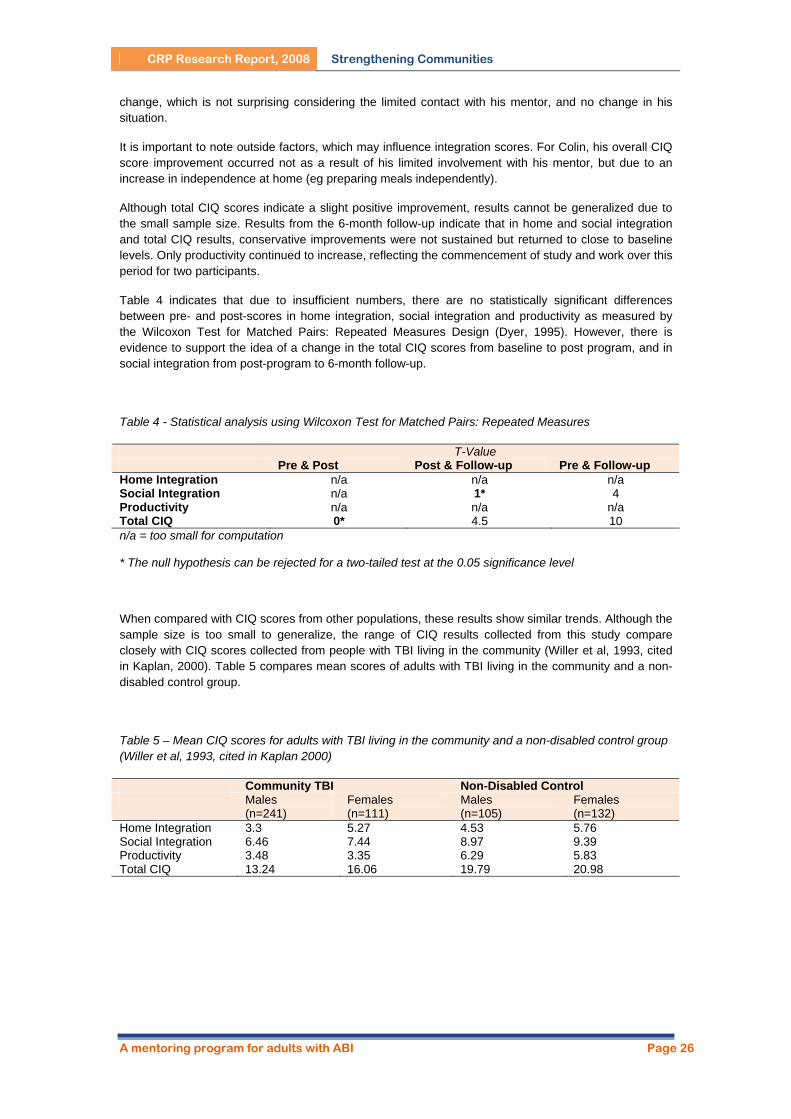
CRP Research Report, 2008 Strengthening Communities
change, which is not surprising considering the limited contact with his mentor, and no change in his situation.
It is important to note outside factors, which may influence integration scores. For Colin, his overall CIQ score improvement occurred not as a result of his limited involvement with his mentor, but due to an increase in independence at home (eg preparing meals independently).
Although total CIQ scores indicate a slight positive improvement, results cannot be generalized due to the small sample size. Results from the 6-month follow-up indicate that in home and social integration and total CIQ results, conservative improvements were not sustained but returned to close to baseline levels. Only productivity continued to increase, reflecting the commencement of study and work over this period for two participants.
Table 4 indicates that due to insufficient numbers, there are no statistically significant differences between pre- and post-scores in home integration, social integration and productivity as measured by the Wilcoxon Test for Matched Pairs: Repeated Measures Design (Dyer, 1995). However, there is evidence to support the idea of a change in the total CIQ scores from baseline to post program, and in social integration from post-program to 6-month follow-up.
Table 4 - Statistical analysis using Wilcoxon Test for Matched Pairs: Repeated Measures
T-Value Pre & Post Post & Follow-up Pre & Follow-up Home Integration n/a n/a n/a Social Integration n/a 1* 4 Productivity n/a n/a n/a Total CIQ 0* 4.5 10 n/a = too small for computation
* The null hypothesis can be rejected for a two-tailed test at the 0.05 significance level
When compared with CIQ scores from other populations, these results show similar trends. Although the sample size is too small to generalize, the range of CIQ results collected from this study compare closely with CIQ scores collected from people with TBI living in the community (Willer et al, 1993, cited in Kaplan, 2000). Table 5 compares mean scores of adults with TBI living in the community and a non-disabled control group.
Table 5 – Mean CIQ scores for adults with TBI living in the community and a non-disabled control group (Willer et al, 1993, cited in Kaplan 2000)
Community TBI Non-Disabled Control Males
(n=241) Females (n=111)
Males (n=105)
Females (n=132)
Home Integration 3.3 5.27 4.53 5.76 Social Integration 6.46 7.44 8.97 9.39 Productivity 3.48 3.35 6.29 5.83 Total CIQ 13.24 16.06 19.79 20.98
A mentoring program for adults with ABI Page 26

CRP Research Report, 2008 Strengthening Communities
DISCUSSION
What Factors Influence the Success of the Mentor Relationship? Effective matching An important factor in successful mentoring relationships appears to be the extent to which both partners feel they have common interests and backgrounds (e.g. ages, careers, hobbies etc). Where mentors and mentees shared similar goals and motivation (e.g. improving fitness, attending first aid training etc), the relationship was maintained and goals achieved.
However, this was not necessarily the case in all partnerships. Despite shared interests in film for Leon and Trevor, and writing for Colin and Maree, other factors such as time availability and expectations reduced the opportunity for these interests to be explored and form a solid foundation for the relationship. Even though similar life experiences assist in developing rapport, they do not guarantee the success of the partnership. Cox (2005) shares similar results, however recommends matching should primarily consider geographical location and time availability, and underplays the importance of other matching criteria.
Trust, communication and reciprocity A high level of mutual trust, effective communication, and reciprocity characterized successful mentor relationships. Over time, effective partnerships were those which developed reciprocal relationships, with both partners acting in the supporting and educating role. In cases where this was not developed, the relationship ended prematurely.
According to a study by Rhodes, Reddy, Roffman & Grossman (2005), the damaging effects of disappointment and distrust in mentoring relationships have the potential to outweigh any positive features. Effective communication is an essential component of a mentor program, and support and feedback from a supervisor can assist minimizing unrealistic expectations and miscommunication.
Figure 4 demonstrates a step-wise approach to developing strong relationships with people with ABI, with a focus on facilitating participation in chosen activities, and acquisition of skills and increased independence (Rees, 1999). The model is characterised by; sensitivity to the person with ABI, developing a sense of trust based on sustained and guaranteed support, respect, facilitating his/her choice of activities, developing a range of options via strong professional and social networks, and having as a goal a perception and belief in the independence of the person with ABI (Rees & Bellon, 2002). This model is recommended as an effective teaching tool for mentors, which can form the basis for reflection and discussion during debriefing sessions.
A mentoring program for adults with ABI Page 27
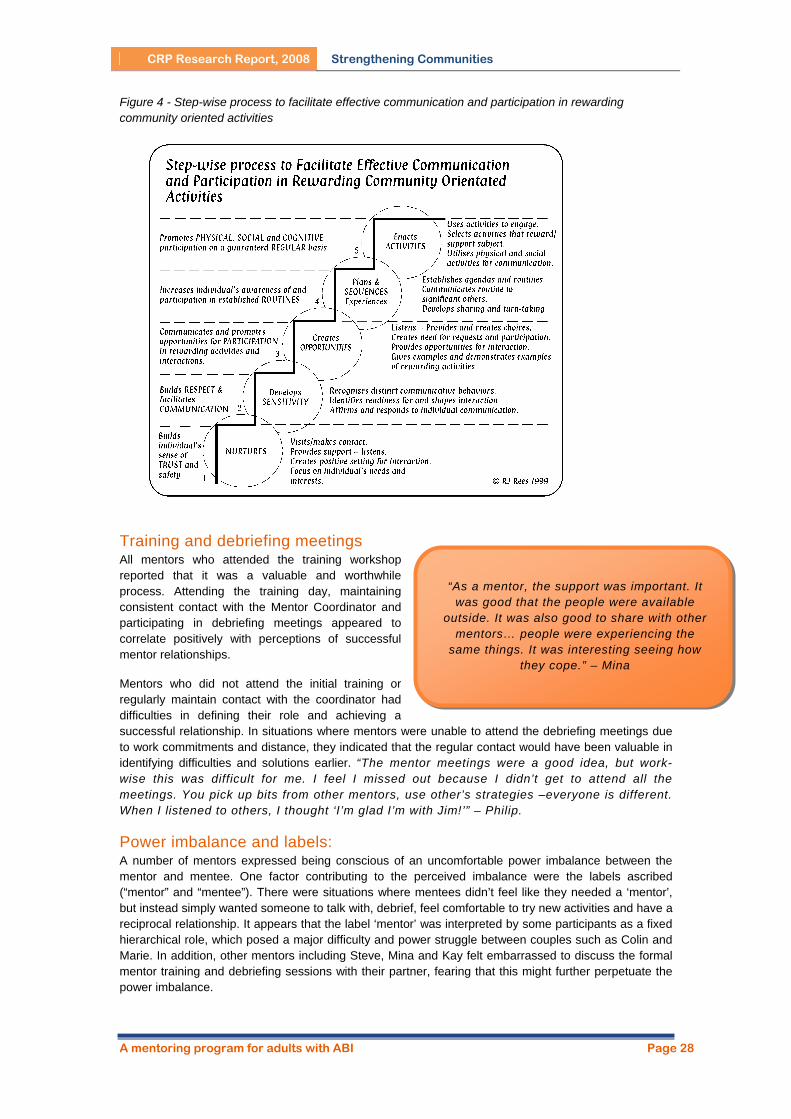
CRP Research Report, 2008 Strengthening Communities
Figure 4 - Step-wise process to facilitate effective communication and participation in rewarding community oriented activities
Training and debriefing meetings All mentors who attended the training workshop reported that it was a valuable and worthwhile process. Attending the training day, maintaining consistent contact with the Mentor Coordinator and participating in debriefing meetings appeared to correlate positively with perceptions of successful mentor relationships.
Mentors who did not attend the initial training or regularly maintain contact with the coordinator had difficulties in defining their role and achieving a successful relationship. In situations where mentors were unable to attend the debriefing meetings due to work commitments and distance, they indicated that the regular contact would have been valuable in identifying difficulties and solutions earlier. “The mentor meetings were a good idea, but work-wise this was difficult for me. I feel I missed out because I didn’t get to attend all the meetings. You pick up bits from other mentors, use other’s strategies –everyone is different. When I listened to others, I thought ‘I’m glad I’m with Jim!’” – Philip.
“As a mentor, the support was important. It was good that the people were available
outside. It was also good to share with other mentors… people were experiencing the
same things. It was interesting seeing how they cope.” – Mina
Power imbalance and labels: A number of mentors expressed being conscious of an uncomfortable power imbalance between the mentor and mentee. One factor contributing to the perceived imbalance were the labels ascribed (“mentor” and “mentee”). There were situations where mentees didn’t feel like they needed a ‘mentor’, but instead simply wanted someone to talk with, debrief, feel comfortable to try new activities and have a reciprocal relationship. It appears that the label ‘mentor’ was interpreted by some participants as a fixed hierarchical role, which posed a major difficulty and power struggle between couples such as Colin and Marie. In addition, other mentors including Steve, Mina and Kay felt embarrassed to discuss the formal mentor training and debriefing sessions with their partner, fearing that this might further perpetuate the power imbalance.
A mentoring program for adults with ABI Page 28

CRP Research Report, 2008 Strengthening Communities
Facilitating communication on these issues is important in clarifying roles and expectations. In addition, sensitivity to perceptions of labels is necessary, and finding an appropriate ‘fit’ is an essential part of a person-centered approach.
Life events Changes in life circumstances had a significant impact on the development of the mentor relationship. Life events in this study included increased employment hours and change in shifts, starting a new job or course, moving interstate, holidays, and moving house. It is acknowledged that these situations can’t be avoided, but it is important to note their impact on potential goal achievement and relationship development.
Time commitment The frequency and consistency of contact between the mentor and mentee determined the success of the relationship. Time to develop the relationship was identified by a number of mentors as a key factor.
Having a guide to contact time each week which both parties anticipated and planned for was an important feature of a successful mentor relationship.
Two mentors commenced full-time work shortly after beginning the mentor program, affecting their availability. For Trevor, this adversely affected his relationship with Leon, resulting in the two only meeting a few times, and the relationship ending. However, for Bill, this resulted in a change of contact mode to phone, SMS and email. Although Bill reported that losing face to face interaction
after one month made maintaining the rapport they had developed difficult, by this stage, the two felt that they had achieved a natural friendship which wasn’t negatively impacted by the distance. Bill stated “We are getting into some deeper conversations on the phone about feelings re: family and how others relate to him and he them. It was a breakthrough to get comfortable bringing up feelings, and I think he values talking about the doubts he often has of how he's related to people.” However, touching base regularly in person was important for both men to reconnect. Where phone and e-mail contact were the only means of contact between partners, the relationship still appeared to be successful. This may be due to the consistent, regular contact and not the form of communication.
“Time has a big impact on the relationship... Time influences the way
you interact with that person. 1-2 hours per week was not enough – a
day was more likely.” - Kay
In addition, having a regular day and time where contact was made was helpful in maintaining the relationship. The routine and structure this introduced seemed to make meeting goals more achievable, and minimized the risk of long periods of time stretching between contacts. Jones (1998, p.60) supports this factor by stating “whatever form of contact takes place, it should be regular and continuous”.
Avoiding ‘over-supporting’ Support and feedback was provided to mentors to minimise behavious such as controlling rather than guiding, and making decisions rather than facilitating problem solving. Mentors were aware of trying to avoid disempowering their partner by offering short-term solutions to problems. It was emphasized that effective support is achieved when mentors facilitate problem solving skills, rather than trying to fix the problem for their partner. This is positively demonstrated in Kay’s relationship with Bonnie, where Kay was supported to act as a sounding-board and help facilitate Bonnie to arrive at her own conclusions and solutions.
Effective closure Preparing for closure is an important phase in a time-limited program. Effective management of this issue involved the following steps:
Clearly identifying the length of the program (9 months) from the start. Reminding the partner of the approaching end of the mentor program in advance (eg 2
months). Encouraging discussion on feelings or thoughts about ending the relationship Discussing what has been accomplished and what has been missed Talking about future plans
A mentoring program for adults with ABI Page 29

CRP Research Report, 2008 Strengthening Communities
The ending phase provides opportunities to focus on the benefits of the relationship, and decide how the change process can continue with more natural supports. Ending should not come as a shock or surprise. Some relationships naturally ended at this point. Others continued after the program had ended. This decision was entirely dependent on the mentor and mentee, with no expectations that all relationships would evolve in the same way. Indeed, most mentors and their partners indicated that they intended to continue (often in a modified, less structured way) in each other’s life. In circumstances where mentors moved interstate (Bill and Philip), they both indicated a desire to maintain contact and support with their partner. The two mentor relationships that terminated revealed differences in commitment and rapport, with all members clearly stating the expectation that the relationship would end and not continue.
Extending social networks One of the mentor roles in community integration is to assist their partner enhance their range of social networks. This is opposed to fostering reliance on the mentor, but seeking other natural supports in the person’s community and life. The overall aim of the mentor relationship is to increase the mentee’s skills and networks in order to expand the range of supports in their community (Rees, 1999). Successful strategies included mentors involving and recruiting others already existing in their partner’s social network to help achieve goals, introducing their partner to their own friends, and actively looking at natural supports in their partner’s community (eg gym workers, librarians, and other community members) to create a cohesive support system.
Despite some successes, extending natural social networks was not well achieved. Mentee social integration scores fell back to baseline levels by 6-month follow-up, indicating that sustained natural supports were limited in nature. For most mentees, participation in a range of social activities in which they engaged during the mentor program did not continue. This highlights the importance of sustained support and cueing for many people with ABI. Focus on building natural supports in an individual’s community is an essential skill for mentors, and further development is needed.
What Impact does the Mentor Relationship have on Achievement of Mentee Goals? Each mentee and their mentor identified specific personal, social, vocational and educational goals at the start of the program. Many of these goals were achieved, however a number were also adapted, discarded, and others were ongoing. Individual goals successfully achieved by mentees in this program included:
• weekly gym sessions at local sports centre, • increase stamina, fitness, strength and self-esteem, • complete an accredited first aid course, • increase weekly social and recreational activities (e.g. regular walks, attending local soccer
games, shopping at markets), • expand interests and experiences (e.g. plan and facilitate a beauty workshop), • increase number of people in social network, • improve motivation and confidence to complete tasks (e.g. sewing and mending), • identify and practice strategies which help in adapting to life after brain injury, and • increased structure and routine.
Clearly identifying specific goals at the start of the program appeared to be influential in achieving positive and measurable outcomes. Flexibility was also important, playing a critical role in adjusting to the individual’s life and events. When goals were clearly articulated, joint motivation and direction was maintained.
Some mentors felt that it was difficult to remain goal focused when their partner did not remember their identified goal. They did not want to coerce their partner into doing something they did not want to do at that present moment. Strategies to routinely refocus on the goal and encourage participation can be
A mentoring program for adults with ABI Page 30

CRP Research Report, 2008 Strengthening Communities
helpful in shaping motivation and achievement for people with short-term memory difficulties (Rees, 2005).
What are the Benefits of a Mentor Program for People with ABI and Mentors? Development of new friendships was an outcome identified by most pairs. The mentor relationship evolved into a strong friendship for many couples, with five out of seven couples continuing their relationship at the end of the program. “I formed a new friendship. That, I think, was the most important.”- Bonnie.
Regular weekly or fortnightly contact helped establish a strong rapport between partners. This relationship provided valued support, encouragement and counsel, with the most effective involving reciprocal support. Role reversal and mutual support is an important component of effective mentoring partnerships, which empowers and eliminates any power imbalance.
“Steve is a good friend now. Not just like a mentor
(someone who comes and goes), but a friend.” - Adam
For partners who were at risk for social isolation, contact with their mentor provided an opportunity to expand their repertoire of social skills and activities. Difficulties with memory and executive functions including planning, goal setting, initiation, self-monitoring, self-regulation, responding to and incorporating feedback, persisting at and completing tasks were issues for many people with ABI in this program. Mentors were able to assist in formulating specific goals, provide structure and motivation, prompt, shape and encourage achievement, and in doing so, help mentees become part of an inclusive community culture (Bellon & Rees, 2006). “For the first time I felt that someone was actually interested to find out what I wanted to do. This whole idea is so new to me, as I never felt that I was that important before". – Bonnie
Mentors also identified a number of personal benefits. These included:
• improved knowledge and understanding of ABI, • opportunities to think creatively and ‘outside the square’, • improved listening skills, • new friendships, • learning to respect others choices, and • learning about drawing boundaries in a relationship.
Despite the positive intentions reported by mentors and mentee partners to maintain contact after the end of the program, the frequency and nature of contact changed for most couples by 6-month follow-up. Without the sustained momentum, prompting and focus of the program, contact was only maintained irregularly for the 5 couples. This may highlight the benefit of an arranged time-limited program, which reduces the risk of the relationship loosing direction and momentum. Similarly, a focus should be placed on strengthening more natural social networks that will continue after the end of the arranged mentor program.
The length of the program may also play a role. In one study by Grossman & Rhodes (2002), youth mentoring relationships which lasted one year or more corresponded with improvements in academic, psychosocial and behavioural outcomes. In contrast, partnerships which ended between three and six months reported increasingly fewer positive effects. The length of this ABI mentoring program was limited to 9 months to reflect the availability of University student mentors who are typically on-campus during this period (March to November). Increasing the duration of the program may assist in developing trust and rapport in the mentoring relationship (Rhodes et al, 2005), however realistic time availability is an issue which should be discussed with interested volunteers from the outset.
A mentoring program for adults with ABI Page 31
CRP Research Report, 2008 Strengthening Communities
Recommendations
Mentor training should be provided for all mentors to ensure roles and responsibilities are clearly understood. This can be provided in either a face-to-face group session as demonstrated in this program or an online environment for distance mentors.
The matching process is an important component of the program. This should carefully consider age, gender, life experience, interests, geographical location, transport mode, time availability and similar expectations of the mentor relationship. However, careful matching does not guarantee successful relationships.
Level of commitment, expectations and boundaries need to be explicitly discussed with all parties at
start of relationship.
Minimum weekly time commitments should be clearly articulated to help ensure routine and focus on goals. Regular scheduled contact times should be arranged in advance, however flexibility is also necessary to adjust to changes in schedules and life events.
Mentors are to be encouraged to maintain regular weekly or fortnightly contact with a designated
Mentor Coordinator with updates of progress and to receive feedback and support.
The Mentor Coordinator should have effective counseling skills and be closely affiliated with the program from which mentees are sourced. This role is time intensive, and required a minimum of one day per week to adequately support 7 couples.
Successful outcomes can be facilitated when mentor and mentee partners clearly describe the goals
they wish to achieve together. Use of the Goal Attainment Scale (Malec, 1999) can assist in measuring progress towards highly individualized goals, developing ownership of and commitment to goals, self-awareness, and capacity for goal-setting. Evaluating goal achievement should be done regularly to keep on track.
Mentors should be supported to involve the mentee’s existing support network in identifying and
achieving goals (eg family, friends, professionals, local community members etc). This will assist in improving communication and coherence, and minimize duplication of support.
The mentor and mentee should receive an individualized booklet which describes the purpose and
definition of the mentor relationship, identifies their goals (with flexibility to change and add new goals), and includes relevant contact numbers. This aims to remind each party of the purpose and goals for the mentor program.
Meetings should be conducted between the Mentor Coordinator, mentor and mentee at regular
intervals to facilitate communication, increase ownership and involvement in the program, and address any issues or concerns as they arise.
Mentors need appropriate skills, regular information and support. Mentor debriefing meetings can be
extremely supportive and helpful, and should occur monthly. These are best facilitated in-person, but may include conference calls and on-line forums to include distance and rural mentors.
Debriefing sessions for mentee partners at the end of the program would provide opportunities for
mentees to reflect on the process and provide feedback.
A time-limited program may assist in maintaining focus, momentum and commitment by both parties. Nine months is considered the minimum length for the development of strong, reciprocal, trusting and effective relationships. Preparation for closure should occur at least two months prior to the pre-arranged end-date.
Emphasis should be placed on supporting mentors to help mentees expand their natural social
networks. As the mentor relationship is often time limited, planning for long-term supports which can assist the person with ABI to maintain social, vocational, educational and community participation is crucial if improvements are to be sustained and developed.
A mentoring program for adults with ABI Page 32
CRP Research Report, 2008 Strengthening Communities
CONCLUSION
All seven case studies illustrate the psychosocial, cognitive and integration difficulties that many people continue to experience long-term following ABI. Limited personal relationships and social isolation are common, restricting social, educational and vocational opportunities. Mentors can play a positive role in helping individuals to identify personal goals, work collaboratively to achieve these goals, and develop and strengthen social networks. Significant outcomes of this program have included the development of reciprocal and enduring friendships, achievement of identified goals, and improved community understanding of ABI and the support required for effective inclusion. Small but significant improvements were noted on the Community Integration Questionnaire post-program, suggesting improvements in home integration, social integration, productivity, and total CIQ scores, with further research required to determine if these results generalize to a larger sample. These improvements were not sustained by 6-month follow-up, with scores falling back to baseline levels in all areas except productivity. It is anticipated that the results from this study will provide a foundation for future effective mentor programs for adults with ABI, in the quest to expand natural supports and create an inclusive community for all.
REFERENCES AIHW. (2007). Disability in Australia: acquired brain injury. Australian Institute of Health and Welfare, 55.
Canberra: AIHW.
Allen, T.D., Eby, L.T., & Lentz, E. (2006). The Relationship between formal mentoring program characteristics and perceived program effectiveness. Personnel Psychology, 59(1), 125-154.
Barker, E.R. (2006). Mentoring – a complex relationship. Journal of the American Academy of Nurse Practitioners, 18(2), 56-61.
Barnett, B. (1995). Developing reflection and expertise: can mentors make the difference? Journal of Educational Administration, 33(5), 45-59.
Bellon, M.L., & Rees, R.J. (2006). The effect of context on communication: a study of the language and communication skills of adults with acquired brain injury. Brain Injury, 20(10), 1069-1078.
Bush, T., Coleman, M. (1995). Professional development for heads: the role of mentoring. Journal of Educational Administration, 33(5), 60-74.
Campbell, J. (1988). The hero with a thousand faces. London: Collins.
Clutterbuck, D. (1992). Mentoring. Henley: Henley Distance Learning.
Conway, K. (2006). Mentoring: back to basics. Training: Helping People and Business Succeed, 42(8), 42.
Cox, E. (2005). For better, for worse: the matching process in formal mentoring schemes. Mentoring & Tutoring, 13(3), 403-415.
DeVito, J. (2006). Human communication: the basic course. 10th Edition. New York: Pearson Education, Inc.
Duck, S. (1991). Understanding relationships. New York: The Guilford Press.
A mentoring program for adults with ABI Page 33
CRP Research Report, 2008 Strengthening Communities
Duffy, M., & Forgan, J. (2005). Mentoring new special education teachers: a guide for mentors and
program developers. Thousand Oaks: Corwin.
Dunn, K.A. (2005). Mentoring new special education teachers: a guide for mentors and program developers. Choice, 43(2), 342-344.
Dyer, C. (1995). Beginning research in psychology. Oxford: Blackwell Publishing.
Eddy, E.R., Tannenbaum, S.I., Lorenzet, S.J., & Smith-Jentsch, K.A. (2005). The influence of a continuous learning environment on peer mentoring behaviours. Journal of Managerial Issues, 17(3), 383-397.
Finn, R. (1993). Mentoring – the effective route to school-based development. In H. Green (Ed.) The School Management Handbook. London: Kogan Page.
Graziano, A.M, & Raulin, M.L. (2004). Research methods: a process of inquiry (5th Ed). Sydney: Pearson Education Group Inc.
Green, F., Schleien, S. J., Mactavish, J., & Benepe, S. (1995). Non-disabled adults’ perceptions of relationshiops in the early stages of arranged partnerships with peers with mental retardation. Education and training in mental retardation and developmental disabilities, June, 91-108.
Grossman, J.B., & Rhodes, J.E. (2002). The test of time: Predictors and effects of duration in youth mentoring programs. American Journal of Community Psychology, 30, 199-219.
Heart, T., & Evans, J. (2006). Self-regulation and goal theories in brain injury rehabilitation. The Journal of Head Trauma Rehabilitation, 21(2), 142-156.
Heartfield, M., Gibson, T., & Nasel, D. (2005). Mentoring fact sheets for nursing in general practice. Adelaide: University of South Australia.
Heffernan, M. and Joni, S-N. (2005). Of protégés and pitfalls: a complete plan for getting the mentoring you need. Fast Company: How Smart People Work, 97, 81-83.
Hibbard, M., Cantor, J., Gundersen, N., Charatz, H., Ashman, T., Gordon, W., Brown, M., Avner, J., Ireland Knight, L., Gartner, A., Lowenstein, J., Berk, W., Quick, S., & Weinberger, J. (2005). Mentoring partnership program: mentor training workbook. New York: Research & Training Center on Community Integration of Individuals with Traumatic Brain Injury, Mount Sinai School of Medicine.
Hunt, D., & Michael, C. (1983). Mentorship: a career training and development tool. Academy of Management Review, 8(8), 475-785.
Jones, S. (1998). Mentors for adults with acquired brain injury. Community Rehabilitation following Acquired Brain Injury, 2(1), 55-64.
Jucovy, L. (2002). Measuring the quality of mentor-youth relationships: a tool for mentoring programs. Northwest Regional Educational Laboratory.
Kuipers, P., Foster, M., Carlson, G., & Moy, J. (2003). Classifying client goals in community-based rehabilitation: a taxonomy for profiling services delivery and conceptualizing outcomes. Disability Rehabilitation, 25(3), 154-162.
Kram (1983). Phases of the mentor relationship. Academy of Management Journal, 26(4), 608-625.
Lawler, J., Dowswell, G., Hearn, J., Forster, A., & Young, J. (1999). Recovering from stroke: a qualitative investigation of the role of goal setting in late stroke recovery. Journal of Advanced Nursing, 30, 401-409.
A mentoring program for adults with ABI Page 34
CRP Research Report, 2008 Strengthening Communities
Lee, S-H., Theoharis, M.F., Kyeong-Hwa, K., Liss, J.M., Nix-Williams, T., Griswold, D.E., & Walther-
Thomas, C. (2006). Create effective mentoring relationships: strategies for mentor and mentee success. Intervention in School and Clinic, 41(4), 233-241.
Luckhaupt SE, Chin MH, Mangione CM et al. (2005). Mentorship in academic internal medicine. Journal of Genera/Internal Medicine. 20(11), 1014-1018.
Malec, J (1999). Goal attainment scaling in rehabilitation. Neuropsychological Rehabilitation, 9(3/4), 253-275.
Rees, R.J., (1999). Rewriting the script: demonstrating skills and talents of people with brain injury. Adelaide: ISLD (Institute for the Study of Learning Difficulties).
Rees, R.J., (2005). Interrupted lives: rehabilitation and learning following brain injury. Melbourne: IP Communications.
Rees, R.J., & Bellon, M.L. (2002). The acquisition of communication skills by people with brain injury: Some comparisons with children with autism. International Journal of Disability, Development and Education, 49(2), 175-189.
Rhodes, J.E., Reddy, R., Roffman, J., & Grossman, J.B. (2005). Promoting successful youth mentoring relationships: a preliminary screening questionnaire. The Journal of Primary Prevention, 26(2), 147-167.
Seritan, A. (2005). The development of a mentoring relationship. Psychiatric Times, March 1, 54.
Sohlberg, M. M., & Mateer, C. A. (2001). Cognitive rehabilitation: an integrative neuropsychological approach. New York: The Guilford Press.
Stuss, D., Gow, C., & Hetherington, C. (1992). No longer Gage: frontal lobe dysfunction and emotional changes. Journal of Consulting and Clinical Psychology, 60, 349-359.
Tracey, C., & Nicholl, H. (2006). Mentoring and networking: Caroline Tracey and Honor Nicholl consider the value to nursing leadership development of mentorship and networking. Nursing Management, 12(10), 28-33.
Tyerman, A. (1997). Social bases of community rehabilitation: a review. Community Rehabilitation following Acquired Brain Injury, 1(1), 29-46.
Wade, D.T. (1998). Evidence relating to goal planning in rehabilitation [Editorial]. Clinical Rehabilitation, 1(4), 273-275.
Willer, B., Rosenthal, M., Kruetzer, J., Gordon, W., Rempel, R. (1993). Assessment of community integration following rehabilitation for traumatic brain injury. Journal of Head Trauma Rehabilitation, 8(2), 75-87.
Ylvisaker, M., & Feeney, T. (1998). Collaborative brain injury intervention: positive everyday routines. College of Saint Rose: Albany.
A mentoring program for adults with ABI Page 35