STREAM TRUNCATE trials Andrew Nunn MRC Clinical Trials Unit at UCL Institute of Clinical Trials and...
18
STREAM & TRUNCATE trials Andrew Nunn MRC Clinical Trials Unit at UCL Institute of Clinical Trials and Methodology University College, London, UK
-
Upload
roderick-benson -
Category
Documents
-
view
222 -
download
0
description
Results of the 9-month regimen in Bangladesh Introdion ObjectifMéthodes Conclusion Published cohort (206 pts) Cure82.5% Completion 5.3% Default 5.8% Death 5.3% Failure 0.5% Relapse 0.5% Overall success rate: 87.9% (95% CI 82.7, 92.6) Am J Respir Crit Care Med Vol –692, 2010 Cohort update (515 pts) 81.2% 3.3% 7.8% 5.6% 1.4% 0.8% Overall success rate: 84.5% (95% CI 0.81, 0.88) Aung et all, IJTLD 18(10):1180–1187, 2014
Transcript of STREAM TRUNCATE trials Andrew Nunn MRC Clinical Trials Unit at UCL Institute of Clinical Trials and...

STREAM & TRUNCATE trialsAndrew NunnMRC Clinical Trials Unit at UCLInstitute of Clinical Trials and MethodologyUniversity College, London, UK

Why STREAM?
• Results from the last of six successive cohorts of patients with MDR-TB in Bangladesh treated with a 9-month regimen suggested there are better options even without the introduction of new drugs
– Van Deun A, Maug AKJ, Salim MAH, Das PK, Sarker MR, Daru P, et al. Short, Highly Effective, and Inexpensive Standardized Treatment of Multidrug-resistant Tuberculosis. Am J Respir Crit Care Med. 2010; 182(5): 684-92.

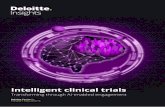
Results of the 9-month regimen in Bangladesh
Introdion Objectif Méthodes Conclusion
Published cohort (206 pts)
Cure 82.5%
Completion 5.3%
Default 5.8%
Death 5.3%
Failure 0.5%
Relapse 0.5%
Overall success rate:
87.9% (95% CI 82.7, 92.6)
Am J Respir Crit Care Med Vol 182. 684–692, 2010
Cohort update (515 pts)
81.2%
3.3%
7.8%
5.6%
1.4%
0.8%
Overall success rate:
84.5% (95% CI 0.81, 0.88)
Aung et all, IJTLD 18(10):1180–1187, 2014

4
Why is a randomised controlled trial needed?
• To eliminate risk that patient selection biased results obtained from cohort studies
• To assess the 9-month regimen in a variety of settings including high levels of HIV-coinfection
• To develop a better evidence base for MDR-TB treatment
• If successful, to provide a new standard of care for comparison with potentially better regimens

A parallel approach to assessing the effectiveness of the Bangladesh regimen
Cohort studies
African countries including:• Cameroon• Benin• Niger• Swaziland
• Afghanistan• Uzbekistan
Randomised trial
• STREAM

STREAM Stage 1 study design
• STREAM is a randomised controlled trial of non-inferiority design currently being conducted in Ethiopia, South Africa, Vietnam and Mongolia
• The control regimen (A) is the locally used WHO recommended regimen in the participating countries
• The study regimen (B) is closely similar to the regimen used in Bangladesh with the exception that high dose moxifloxacin replaces high dose gatifloxacin

7
The 9-month regimen (B)
Weeks Drug doses by weight group
Drug < 33 kg 33 - 50 kg > 50 kg Kanamycin* 1 - 16 15 mg per kilogramme body weight Isoniazid (H) 1 - 16 300 mg 400 mg 600 mgProthionamide 1 - 16 250 mg 500 mg 750 mg Clofazimine 1 - 40 50 mg 100 mg 100 mg Moxifloxacin 1 - 40 400 mg 600 mg 800 mg Ethambutol 1 - 40 800 mg 800 mg 1200 mg Pyrazinamide 1 - 40 1000 mg 1500 mg 2000 mg
• Kanamycin 3 times/week after week 12
The intensive phase may be extended by 4 or 8 weeks if smear conversion has not occurred by 16 or 20 weeks

8
STREAM Study Population • Adults (18 years or older) who has given consent for
treatment and follow-up • Smear-positive pulmonary tuberculosis, or if HIV positive may
be smear negative• Evidence of initial resistance to rifampicin on line-probe assay,
GeneXpert or other DST• No evidence of initial resistance to fluoroquinolone or
2nd-line injectables on line-probe assay• No pre-existent QT prolongation >500msec • If pre-menopausal woman, not pregnant or breast feeding and
agrees to use effective barrier contraception/IUCD during treatment

9
Stage 1: current status
• Enrolment to Stage 1 commenced: July 2012• Sites: Ethiopia (2), South Africa (3), Vietnam and Mongolia• 424 of initial target of 400 patients enrolled• Intake closed: June 30th 2015• Primary endpoint at 30 months • Last patient visit: Q4 2017• Results from Stage 1 expected: Q1/2 2018

STREAM Stage 1 Partners
MONGOLIA
· NCCD, Ulaanbataar
Funder: USAID
SOUTH AFRICA
· Sizwe Tropical Diseases Hospital
· King Dinuzulu Hospital, Durban
· Doris Goodwin Hospital, Pietermaritzburg/THINK
Design, Management, Analysis
ETHIOPIA
· Armaeur Hansen Research Institute (AHRI)
· St. Peter’s Tuberculosis Specialised Hosp./ Global Health Committee
Impact Assessment: Liverpool School of Tropical Medicine
Microbiology: Institute of Tropical Medicine,Antwerp
VIETNAM
· Ho Chi Minh City Hospital
Sponsor: The Union

11
STREAM Stage 2• Following the provisional licensing of bedaquiline we were
asked to consider:– is it possible to include additional regimens to the
STREAM trial in its present form? – if so, what would be the appropriate regimen(s) to
evaluate?
• After extensive discussions between the study partners and other experts it was agreed that the primary interest to patients and programmes would be:– a fully oral regimen (no kanamycin) and/or– a shorter and simpler regimen

Regimens for Stage 2

13
STREAM Stage 2Collaboration• Funding : USAID and Janssen; Sponsor: The Union• Including as many of the Stage 1 sites as possible, with additional sites
(inc. Eastern Europe)
Primary objectives:• To assess whether the proportion of patients with a favourable efficacy
outcome on Regimen C, the fully oral regimen, is as effective as Regimen B at 76 weeks (18 months)
• To assess whether the proportion of patients with a favourable efficacy outcome on Regimen D, the 6-month regimen, is as effective as Regimen B at 76 weeks (18 months)

14
STREAM Stage 2 design
• Because it is possible that Regimen B might not be found to be non-inferior to Regimen A it was decided to continue to enrol patients to Regimen A
• Secondary objectives include the comparisons of Regimen C and Regimen D to Regimen A; these will be particularly important if Regimen B is found to be inferior to Regimen A
• Sample size for Stage 2 = 1155

15
TRUNCATE
Two-month Regimens Using Novel Combinations to Augment Treatment Effectiveness for drug-sensitive Tuberculosis (TB): a randomised controlled non-inferiority trial with a multi-arm multi-stage design
led by National University of Singapore, and run in collaboration with MRC CTU at UCL

16
TRUNCATE: why so short?
• In 1981 Wallace Fox reviewed the current status of short course chemotherapy; he noted that even in regimens of only 3 or 4 months duration using standard drugs over 80% of patients had a relapse-free cure.
• What if new drugs were added and treatment was given for only 2 months? Equally good or better results might be achieved.
• If relapsing patients could be successfully retreated such a strategy might be very attractive both the patients and TB programmes.

17
TRUNCATE – a strategy trial• Objective: To test whether the TRUNCATE-TB strategy is non-
inferior to the standard 6-monthTB strategy • TRUNCATE treatment strategyo Treatment can be extended from 8 to 12 weeks for patients
responding slowlyo Patients smear positive at 12 weeks or missing more than 2
weeks treatment to be given 6 months’ treatmento Regimens behaving badly stopped early (MAMS design)o Close monitoring for relapse
• Primary outcome: assessed by the proportion of patients with unsatisfactory outcome 2 years after randomisation

ChinaBeijing Chest HospitalWuhan Center for TB ControlTianjin Haihe Hospital
IndonesiaFMUI, Jakarta University of Padjadjaran, BandungHasanuddin University, Makassar
Philippines Philippine Tuberculosis SocietyLung Centre of the Philippines
Singapore National University HospitalSingapore General Hospital Changi General Hospital
ThailandSiriraj Hospital – Mahidol UniversityChulalongkorn Hospital Bamrasnaradura Hospital VietnamHanoi Lung HospitalThanh Hoa TB and Lung Hospital
TB REGIONAL CLINICAL TRIALS NETWORK