Strategies for Recruiting Middle Eastern-American Young Adults for Physical Activity Research: A...
11
ORIGINAL PAPER Strategies for Recruiting Middle Eastern-American Young Adults for Physical Activity Research: A Case of Snowballs and Salaam David Kahan Alia Al-Tamimi Published online: 23 January 2008 Ó Springer Science+Business Media, LLC 2008 Abstract Recruitment of minorities into health studies is a process that has been the subject of recent research effort. The prevalence of hypokinetic disease in the fast growing Middle Eastern-American community is higher than whites and some minority groups and descriptive research is needed to further quantify morbidity status and antecedent behavior. To date, we know of no study that reports recruitment methods of Middle Eastern-American young adults, a demographic group that is transitioning into an at- risk stratum for ethnically associated morbidity. We report and analyze a multi-method approach used in recruiting 240 young adults of this ethnic group into a 1-week study of physical activity utilizing activity logs and pedometers. Participants were primarily recruited through snowball sampling (48.3%), flyers (15.8%), presentations to uni- versity campus organizations (15.4%), and graduate research assistants (10.8%). Access was facilitated by assistants who were community insiders; active recruit- ment was more successful than passive recruitment; and different techniques appealed to different group segments based on gender and religion. Keywords Recruitment methods Á Arab Americans Á Young adults Á Snowball sampling Introduction In the United States, over the last 20 years the influx of immigrants and growth of all autochthonous racial minority populations have outpaced that of the nation’s white majority [1, 2]. These peoples’ health behaviors and beliefs frequently differ within and between identity groups and compared to whites [3–5]. As a result, immigrants and minority groups are uniquely and differentially afflicted with certain morbidities. For example, Black Americans’ death rates from stroke and heart disease are between 1.2 and 1.4 times higher, respectively than whites [6]; yet when blacks are differentiated by birthplace, it is African-born blacks, but not US-born blacks, who report significantly better health and fewer activity limitations when compared to whites [7]. Often, minority and immigrant health is influenced by socio-cultural factors and manifest in dis- parate conditions related to food sufficiency and safety, access to health care and insurance, childcare, affordable housing, and educational and occupational attainment, which can create or reinforce a tiered status relative to health and mortality [8–11]. The resultant burden on American society cannot be underestimated. Morbidities directly contribute to financial burden associated with lost wages and productivity [12, 13], strain social medicine services and their funding [14], and induce ethical dilemmas over failed health care ini- tiatives and services [15–17]. Disparities between populations and ethnic groups have been noted for many morbid conditions, including heart disease, overweight/ obesity, diabetes, and certain forms of cancer [18]. A prophylaxis for these and other morbidities is engagement in health-enhancing and abatement in health-damaging behavior. Toward this end, in the Healthy People 2010 initiative [18] there are many objectives aimed toward D. Kahan (&) Á A. Al-Tamimi School of Exercise and Nutritional Sciences, San Diego State University, 5500 Campanile Drive, San Diego, CA 92182-7251, USA e-mail: [email protected] 123 J Immigrant Minority Health (2009) 11:380–390 DOI 10.1007/s10903-008-9117-7
-
Upload
david-kahan -
Category
Documents
-
view
213 -
download
1
Transcript of Strategies for Recruiting Middle Eastern-American Young Adults for Physical Activity Research: A...

ORIGINAL PAPER
Strategies for Recruiting Middle Eastern-American Young Adultsfor Physical Activity Research: A Case of Snowballs and Salaam
David Kahan Æ Alia Al-Tamimi
Published online: 23 January 2008
� Springer Science+Business Media, LLC 2008
Abstract Recruitment of minorities into health studies is
a process that has been the subject of recent research effort.
The prevalence of hypokinetic disease in the fast growing
Middle Eastern-American community is higher than whites
and some minority groups and descriptive research is
needed to further quantify morbidity status and antecedent
behavior. To date, we know of no study that reports
recruitment methods of Middle Eastern-American young
adults, a demographic group that is transitioning into an at-
risk stratum for ethnically associated morbidity. We report
and analyze a multi-method approach used in recruiting
240 young adults of this ethnic group into a 1-week study
of physical activity utilizing activity logs and pedometers.
Participants were primarily recruited through snowball
sampling (48.3%), flyers (15.8%), presentations to uni-
versity campus organizations (15.4%), and graduate
research assistants (10.8%). Access was facilitated by
assistants who were community insiders; active recruit-
ment was more successful than passive recruitment; and
different techniques appealed to different group segments
based on gender and religion.
Keywords Recruitment methods � Arab Americans �Young adults � Snowball sampling
Introduction
In the United States, over the last 20 years the influx of
immigrants and growth of all autochthonous racial
minority populations have outpaced that of the nation’s
white majority [1, 2]. These peoples’ health behaviors and
beliefs frequently differ within and between identity groups
and compared to whites [3–5]. As a result, immigrants and
minority groups are uniquely and differentially afflicted
with certain morbidities. For example, Black Americans’
death rates from stroke and heart disease are between 1.2
and 1.4 times higher, respectively than whites [6]; yet when
blacks are differentiated by birthplace, it is African-born
blacks, but not US-born blacks, who report significantly
better health and fewer activity limitations when compared
to whites [7]. Often, minority and immigrant health is
influenced by socio-cultural factors and manifest in dis-
parate conditions related to food sufficiency and safety,
access to health care and insurance, childcare, affordable
housing, and educational and occupational attainment,
which can create or reinforce a tiered status relative to
health and mortality [8–11].
The resultant burden on American society cannot be
underestimated. Morbidities directly contribute to financial
burden associated with lost wages and productivity [12,
13], strain social medicine services and their funding [14],
and induce ethical dilemmas over failed health care ini-
tiatives and services [15–17]. Disparities between
populations and ethnic groups have been noted for many
morbid conditions, including heart disease, overweight/
obesity, diabetes, and certain forms of cancer [18]. A
prophylaxis for these and other morbidities is engagement
in health-enhancing and abatement in health-damaging
behavior. Toward this end, in the Healthy People 2010
initiative [18] there are many objectives aimed toward
D. Kahan (&) � A. Al-Tamimi
School of Exercise and Nutritional Sciences,
San Diego State University, 5500 Campanile Drive,
San Diego, CA 92182-7251, USA
e-mail: [email protected]
123
J Immigrant Minority Health (2009) 11:380–390
DOI 10.1007/s10903-008-9117-7

narrowing the disparities between population groups for a
variety of health behaviors such as physical activity, oral
health behavior, tobacco use and immunization.
Prior to developing health behavior interventions tai-
lored toward specific populations, descriptive
epidemiological studies must be conducted with each
toward identifying the scope and severity of morbidity and
quantifying and qualifying the health behaviors that con-
tribute to or prevent the development of morbidity. One
ethnic group that has recently received attention in this
regard is the Middle Eastern population of the United
States, particularly Arab Americans, a group that has
grown by 38.3% between the 1990 and 2000 US Censuses
[19].
Results of morbidity research within this population
indicate high prevalence of hypokinetic diseases, such as
diabetes, cardiovascular disease, hypertension, and certain
cancers [20–23], which in turn may be influenced by
insalubrious changes in lifestyle and diet while living in the
US [24, 25]. Results of physical activity research con-
ducted in Canada and Sweden suggest that Arabs are: (1)
40–50% less likely of being moderately physically active
compared to whites and that these differences considerably
narrow according to time since immigration [26, 27]; and
(2) between 4.4 and 12.5 times likelier than whites to
engage in sedentary leisure time activities [28]. To our
knowledge, researchers have ignored objective assessment
of physical activity behavior within the Arab American and
American Middle Eastern communities. Additionally, there
is comparatively less research on these communities’
young adults’ (ages 18–29) health behavior. With calls to
focus on young adults’ physical activity [29] coupled with
the observation that within Arab culture children still
strongly affiliate with the family at this age [30], it is
important that we study this transition age group within this
vulnerable minority.
To conduct descriptive research of this type, adequate
recruitment of participants is necessary, which may prove
difficult with an under-researched population because the
size of the group is unknown, group members may be
reluctant to acknowledge their membership, and may dis-
trust nonmembers [31]. Additionally, at the community
level, participation may be compromised if a group has
been previously patronized or stigmatized, or is skeptical
regarding how research outcomes might be used and how it
stands to benefit [31]. Observational studies that utilize
non-probabilistic sampling appear to pose the fewest bar-
riers to the recruitment of minorities [32]. Nevertheless,
recruitment of some minority’s members can be further
expedited by snowball sampling; making face-to-face
contact with prospective participants; establishing rapport
and building trust with individuals and their community;
prioritizing participants’ convenience over that of the
research team’s; effectively conveying a study’s purpose,
tasks, and benefits to the individual and community;
including meaningful incentives; and utilizing cultural
adaptation strategies [32, 33]. Kreuter and colleagues [34]
qualified cultural adaptation strategies by category: (1)
peripheral (i.e., producing study materials that visually
appeal to a specific culture); (2) evidential (i.e., presenting
data concerning relevant health issues); (3) linguistic (i.e.,
responding to language preferences of minority group
members); (4) constituent involving (i.e., seeking group
members for input or staffing); and (5) sociocultural (i.e.,
imbuing a study’s methods with normative group beliefs
and values).
Several of the aforementioned strategies and cultural
adaptations have been used with varying degrees of success
in recruiting within the Arab American community [20,
35–38]; however, to our knowledge only two papers
explicitly and centrally focus on recruitment strategies for
health-related research within this population.
First, Aroian and colleagues [38] found that: (1) a panel
of advisory experts’ assumptions and recommendations
were not always accurate and fruitful; (2) cultural and
religious community gatekeepers were not helpful in
recruitment efforts; (3) personal contact was the only
means of advertising that was successful; (4) ample bud-
geting of money and time was required to provide adequate
incentives and opportunity for rapport building; and (5)
having a community insider on the research team facili-
tated access to community members.
Second, Barry [39] studied the acculturation experiences
of male Arab immigrant university students. He discovered
that traditional recruitment methods (e.g., canvassing
undergraduate psychology classes, flyers, networking with
local Arab groups, personal contacts) were inadequate. He
resorted to Internet solicitation of Arabs affiliated with
campus and community organizations. Interested persons
replied by e-mail and were sent questionnaires by mail. Of
the 700 persons solicited, 17% replied and 11% of the
original total participated. Feedback about using the
Internet included: (1) Concerns about the rationale of the
study and potential injurious findings about Arabs were
alleviated by receiving quick one-on-one e-mail replies; (2)
comfort using the medium motivated their participation;
(3) usage of the Internet was linked to participants feeling
actively involved in the fine-tuning of recruitment methods
as well as casting the Internet as a medium that was less
biased toward Arabs than standard media; and (4) interest
in participating was heightened by participants’ sense of
novelty and creativity associated with the Internet.
In our study, we aim to broaden the focus of previous
work [38, 39] to include a broader segment of the Middle
Eastern American population and an unreported health
behavior. We descriptively report recruitment methods
J Immigrant Minority Health (2009) 11:380–390 381
123

used to recruit Middle Eastern-American young adults for a
physical activity behavior study as well as analytic results
of those methods. Results of this study may be used to
verify or refute recruitment methods of Arab- and Middle
Eastern Americans for health research in general while
adding an unreported demographic to the literature.
Methods
Setting
A majority (92.1%) of participants were living in San
Diego County, California at the time of the study with
remaining participants residing in adjacent or nearby
counties. According to US 2000 Census data [40], there
were a combined *24,000 (0.85% of San Diego County
population) persons reporting Arab or Assyrian/Chaldean/
Syriac (ACS) ancestry. It is possible that this estimate
underreports the true county population, as a discrepancy
of nearly 13,000 Chaldeans is noted between Census 2000
and local [41] estimates. These figures exclude the county’s
Kurdish population—estimated at greater than 8,000
[41]—whose members were eligible for the present study if
their or their family members’ birthplace was an Arab
League nation (typically the Kurdistan region of Iraq).
Characteristics of the combined Arab and ACS population
of San Diego County include: 55.5% foreign-born; 53.4%
male; 41.3% younger than 25; 21.2% living below the
poverty level; and 20.9% of those 25 years of age and older
having at least a bachelor’s degree [40].
Project SALAAM-E
Before making local inquiries, the lead author, who is a
cultural, religious, and linguistic outsider to the commu-
nity, undertook a sustained period of inquiry into the
history, beliefs, and customs of Arabs and Muslims with
particular focus paid to Arab- and Muslim Americans and
their health behaviors. Additionally, the lead author con-
tacted The Arab Community Center for Economic and
Social Services (ACCESS; Dearborn, MI), a community
health service agency, and was advised that participation in
health research among this demographic required contact-
ing prospective participants actively and directly (i.e., face-
to-face) and working in schools as opposed to houses of
worship (D. Rabiah, personal communication, November
20, 2003).
Preparatory to the study’s inception, the lead author
contacted the Center for Islamic and Arabic Studies on
campus to solicit input as to how to conduct a study of
physical activity in San Diego. The center’s founder
assembled a panel of colleagues and graduate students
none of whom had a background in physical activity or
epidemiological research. After several meetings, between
which they solicited community feedback, they made the
following key recommendations: (1) Expand the popula-
tion focus of the study to include all persons whose native
origins were in Arab League countries regardless of reli-
gion or ethnicity; (2) conduct the study on college
campuses, where students would be more open to such a
study and would spread word back to their communities;
and (3) be willing to go out to meet students in groups and
at times and locations convenient to them.
Conducted in 2005, the Survey of Activity and Leisure
among Adult Middle Easterners (SALAAM-E) quantified
the amount and qualified the type of activity engaged in by
young adults of Middle Eastern origin living primarily in
San Diego. Eligibility for the study included age (18–29),
pregnancy status (not in 3rd trimester), and origin (oneself,
a parent, or a grandparent born in any of the Arab League
countries). The latter criterion opened up the study to non-
Arabs as well as persons who might not identify as Arab
American. (We subsequently used the more encompassing
term Middle Eastern in advertisements, questionnaires, and
conversations with participants but interchangeably use
Arab American and Middle Eastern American in this
paper).
Our initial recruitment plan was localized to our home
campus. We relied on flyer advertisements, classroom
presentations, colleague referrals, presentations at student
organization meetings, and snowball sampling through
participants who had completed the study protocol. After
the recruitment process slowed, we turned our attention
toward other campuses, community businesses and agen-
cies, and research assistant contacts.
Participants1 (N = 240; 50% male; 50% Muslim, 50%
non-Muslim) completed a 27-item questionnaire, which
included scales measuring religiosity and acculturation,2
and standard types of demographic questions (e.g., gender,
age, height, weight).
Participants wore an unsealed pedometer (Yamax Digi-
Walker SW-200) during waking hours for 7 days and
maintained a daily physical activity log, in which they
recorded step count, time wearing the pedometer, and
checked off which of 22 activities they engaged in on a
particular day and for how long. In all cases, participants
1 For analyses purposes, an adequate power of 0.80 was associated
with a minimum sample size of 180; an additional 60 participants
were recruited in case of missing or poor quality data.2 Acculturation was measured with the Acculturative Index [47],
which represents a composite score equal to [(length of residence
proportion 9 4) + (generation score - 1) + (self-identification
value - 1)]. Scores B5 were labeled low acculturation and scores
[5 were labeled high acculturation.
382 J Immigrant Minority Health (2009) 11:380–390
123

met with data collectors at times and locations convenient
for them and were compensated $25 upon completion of
the study. The study was approved by the Institutional
Review Board.
Analysis
Data for evaluating recruitment methods came from vari-
ous sources. Selected demographic data were derived from
questionnaire responses and analyzed descriptively using
SPSS 13.0 (Table 1). A participant file was maintained and
identified each participant by number, gender, age, reli-
gion, and recruitment source. When recruited through
snowballing, the participant referee was noted by number
in the recruitment source column for the new participant.
These data were analyzed descriptively through manual
calculations of frequency counts (Table 2) and percentages
(text).
An event log was also maintained and contained meet-
ing minutes, results of weekly surveillance of flyer status,
contact information of organizations and results of con-
tacts, and communication related to reasons for non-
participation as reported by the five data collectors through
Table 1 Select demographics (N = 240)
Frequency Percentage
Age
18–19 70 29.2
20–21 70 29.2
22–25 69 28.7
26–29 31 12.9
Residence
Outside parental home 128 53.3
With parents 112 46.7
Employment
Unemployed 98 40.8
Part-time 110 45.8
Full-time 32 13.3
Self-identity
More/Very ME 102 42.5
ME-American 83 34.6
More/Very American 55 23.0
Social circle
Mainly/Almost exclusively ME 84 35.0
Even mix of ME and non-ME 87 36.3
Mainly/Almost exclusively non-ME 69 28.7
Language preference with family and friends
Mostly/Only Arabic or other ME
language
66 27.5
Table 1 continued
Frequency Percentage
Equal amounts English and Arabic/Other 64 26.7
Mostly/Only English 110 45.9
Parental education
Mother
Did not graduate high school 47 19.6
High school graduate 39 16.3
Some college/college graduate 107 44.6
Graduate work or degree 47 19.6
Father
Did not graduate high school 38 15.8
High school graduate 21 8.8
Some college/college graduate 95 39.6
Graduate work or degree 86 35.8
Birthplacea
Participant
North Africa 15 6.3
Other Africa 21 8.8
Arabian Peninsula 22 9.2
The Levant 66 27.6
United States 103 43.1
Other 12 5.0
Mother
North Africa 41 17.1
Other Africa 22 9.2
Arabian Peninsula 8 3.3
The Levant 118 49.2
United States 36 15.0
Other 15 6.3
Father
North Africa 45 18.8
Other Africa 20 8.3
Arabian Peninsula 10 4.2
The Levant 129 53.8
United States 24 10.0
Other 12 5.0
Acculturation indexa
Not born in the United States
Low (B5) 104 76.5
High ([5) 32 23.5
Born in the United States
Low (B5) 9 8.7
High ([5) 94 91.3
Note: ME = Middle Eastern. North Africa includes Algeria, Egypt,
Libya, Morocco, Tunisia, and Western Sahara. Other Africa includes
Comoros, Djibouti, Mauritania, Somalia, and Sudan. Arabian Pen-insula includes Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, UAE,
and Yemen. The Levant includes Iraq, Jordan, Lebanon, Palestine,
and Syriaa Based on n = 239 (i.e., missing datum)
J Immigrant Minority Health (2009) 11:380–390 383
123

regular debriefings and e-mails. Lastly, e-mail sent to the
lead author by participants and prospective participants
related to the study were retained; those pertaining to
recruitment were filtered and content analyzed for verbiage
that explained successful or failed referrals. The authors
independently reviewed these materials and discussed to
consensus the critical events that facilitated and deterred
participation, which are found in this report.
Results
A demographic profile of study participants is found in
Table 1. Pluralities of participants were either 18–19 or
20–21 years of age (29.2% each), were employed part time
(45.8%), identified as more or very Middle Eastern
(42.5%), reported an even mix of Middle Eastern and non-
Middle Eastern friends (36.3%), spoke mostly or only
English with family and friends (45.9%), had parents who
attended some college or had a college degree (44.6%,
mother; 39.6%, father), were born in the United States
(43.1%), and had mothers who were born in Levantine
countries (49.2%). A slight majority of participants lived
outside the parental home (53.3%), had fathers who were
born in Levantine countries (53.8%), and were highly
acculturated (52.7%).
The types and results of recruitment methods that yiel-
ded participants appear in Table 2. Snowball sampling
yielded 48.3% of all participants, and for this study was
defined as a participant who successfully recruited one or
more additional participants into the study or provided
information that led to successful recruitment. In snowball
sampling, the researcher ‘‘asks each participant to suggest
others with similar ability to address the issues…[and] can
be a valuable one when the researcher does not know the
field…[or] when individuals with the knowledge or expe-
rience to provide rich data are difficult to reach’’ ([42],
p. 58). Flyer advertisement (15.8% overall, three cam-
puses) was the second most successful strategy followed by
contact with campus religious/cultural organizations and
attendance at their events (15.4% overall, three campuses).
Graduate research assistants’ (GRA) outreach efforts
directly contributed an additional 26 participants (10.8%).
The remaining 23 participants (9.6%) were recruited
through class presentations, departmental colleague refer-
rals, and other techniques.
We did not systematically ask participants why they
elected to participate. However, frequently and on an
informal level, participants voluntarily expressed reasons
for their participation: (1) The monetary incentive was
sufficiently appealing; (2) friends participated in the study;
(3) they were interested in learning about their physical
activity levels vis-a-vis pedometers; (4) they perceived the
study was for the community’s greater good; (5) they were
intrigued by the novelty of a research study focused on
Middle Easterners; or (6) some combination of factors.
Analysis of Recruitment Strategies
For succinctness, only recruitment strategies that yielded
10% or more of the total number of participants are pre-
sented: snowball sampling, flyer advertisement,
presentations at organizations’ meetings, and GRA outreach.
Snowball Sampling
To stimulate the snowball effect, participants were
informed at the intake appointment of the target number of
participants and of the researchers’ reliance on them
Table 2 Types and results of participant-yielding recruitment
methods
Type n # $ >/A ;AI :AI
Snowball 116 69 47 41 75 47 69
Flyer
Campus 1 19 7 12 6 13 6 13
Campus 2 16 10 6 4 12 5 11
Campus 3 3 1 2 0 3 1 2
Class presentations 5 2 3 2 3 2 3
Departmental colleagues 5 2 3 0 5 1 4
Organizations
Campus 1
ASU 12 2 10 8 4 8 4
MSA 3 3 0 3 0 3 0
Campus 2
MSA 16 9 7 16 0 7 9
Hillel 1 0 1 0 1 0 1
Campus 4
MSA 5 1 4 5 0 5 0
Graduate research assistants
Male Muslim 6 4 2 6 0 6 0
Female Muslim 20 7 13 17 3 11 9
Other
Librarian 9 0 9 9 0 8 1
Health fair 1 1 0 1 0 1 0
ISA social function 1 1 0 1 0 1 0
Personal acquaintance 1 0 1 0 1 1 0
Chance encounter 1 1 0 1 0 1 0
Total 240 120 120 120 120 114 126
Note: AI = acculturative index (;, low; :, high); ASU = Arab
Student Union; MSA = Muslim Student Association; ISA = Inter-
national Student Association
384 J Immigrant Minority Health (2009) 11:380–390
123

spreading word of the study to friends and relatives. They
were encouraged to share their participation experience
with anyone who fit eligibility criteria and encourage their
subsequent participation. An e-mail prompt concerning
sharing any potential contacts at the outtake meeting was
sent on Day 6 of the 7-day protocol. At the conclusion of
the outtake meeting, data collectors asked for any referrals
who agreed to be contacted about the study and e-mail or
phone information was provided with potential partici-
pants’ consent.
During the course of data collection, 22 distinct snow-
balls formed as a result of the outlined methodology—17
were initiated by females and 5 by males. Of 15 secondary
referees (i.e., referees within a snowball cascade), 12 were
male and 3 were female. A majority (81.8%) of snowball
events were two-generation in nature (i.e., a participant was
responsible for bringing in one additional participant and
then the chain stopped). Additionally, there were 1 three-, 2
four-, and 1 eight-generation snowballs, respectively. With
116 participants recruited through snowball methodology,
the mean snowball size, excluding the initial referee, was
5.6 (SD = 12.4) participants. The majorities recruited
through this technique were highly acculturated (67.2%),
non-Muslim (64.6%), and male (59.5%), respectively
(Table 2).
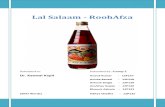
Figure 1 depicts an eight-generation cascade that rep-
resents the single largest snowball event. The scrolls on the
left numerically represent successive generations with the
cumulative number of participants recruited denoted by
subscript. The ovals on the right identify referees by
participant number when more than one participant from a
previous generation referred someone else. The numbers
within the rectangular boxes identify all participants
enveloped by the snowball by participant number. Lastly,
letter subscripts indicate the gender of the referee.
Within this particular snowball, nine males and two
females were responsible for initiating or perpetuating the
chain, which resulted in 60 participants (25.0% of the total
sample). A breakdown of the snowball provides insight
into the nature and complexity of the snowball recruitment
method. (For succinctness a participant will be referred to
by the letter ‘P’ followed by his or her participant number).
A collegial referral led the author to P83 who partici-
pated and also identified her brother (P94) as a potential
participant who was well connected within the Campus 2
Middle Eastern community. Besides participating, P94
indicated interest in assisting with recruitment along with
his friend (P110). Both were Christian males of Jordanian
and Syrian heritage, respectively. After their pool of on-
campus referrals dwindled, they were hired and trained as
recruiters and protocol administrators in order to reach
persons beyond the campus. Toward this end, both
attempted to establish contact with his respective church
and were unsuccessful: The priests indicated initial interest
in assisting but upon learning of the lead author’s last name
refused their church’s involvement because of political-
ideological differences. P94 shifted focus to soliciting
faculty teaching Arabic classes at two campuses to allow
him to make class presentations. Very few responded to his
repeated phone and e-mail queries and the few classes he
38 F
49 M
,111-106 ,69 671-571 ,131-031
,731 ,821 ,621 ,421 ,221042-532 ,132-622 ,422-212
021 M
251 ,831 ,721
471251 F
741 M831 M
871 M
981-881 ,581-381
781-681 591-391
69 M
011 M
581 M
12
2 31
3 44
4 74
5 94
6 05
7 55
8 06
981 M
Fig. 1 Schematic diagram of
largest snowball event across
generations
J Immigrant Minority Health (2009) 11:380–390 385
123

did address yielded no additional participants. P110 spent
vacation time in his hometown near Los Angeles and met
friends and family at their homes and on- and off-campus
residences, which resulted in an additional 25 participants.
Later in the cascade, a student (Fig. 1, Generation 6,
dashed line) who had seen a flyer advertisement contacted
us. Although ineligible because the target number of
female Muslim participants had already been reached, she
referred us to P178 who referred his sister and cousins to
the study (Fig. 1, Generation 7), who in turn referred their
friends to the study (Fig. 1, Generation 8).
The preceding vignette demonstrates the snowball
method’s potential for generating a critical mass of par-
ticipants. The success of the method in this study was the
product of tenacious querying of participants for procuring
referrals; dedication to following up these referrals and
establishing an initial rapport partly based on the referral’s
trust in the referee; and a large measure of serendipity.
Identifying key members of the participant pool who could
formally assist in recruitment on a for-compensation basis
was an additional mitigating factor.
Flyers
Bold colored flyers that briefly described the study, eligi-
bility criteria, and compensation; and had detachable tabs
containing contact information were posted on three cam-
puses. The majority recruited through flyers was non-
Muslim (73.7%), highly acculturated (68.4%), and female
(52.6%) (Table 2).
On Campus 1 (authors’ home campus), flyers were
posted at 42 different locations in 20 buildings and their
status regularly monitored during the spring semester. Only
40 (1.7%) tabs were taken of the possible 2,412 total during
the monitoring period with six tabs total being the most
removed from any venue over the course of inspection.
On Campus 2, posting flyers was a less laborious pro-
cess. University policy allowed unrestricted posting at the
main campus commons area where hundreds of adver-
tisements for research studies were regularly posted.
Although official monitoring was not conducted, nearly as
many participants as Campus 1 were recruited through
flyer advertisement under less difficult conditions.
Organizations
The general approach toward identifying campus organi-
zations was to initially access university web sites and
phone campus student services offices in order to deter-
mine whether a student club or organization by its name,
description, or purpose might have a Middle Eastern con-
stituency. Follow-up phone calls, e-mail, or both to an
organization’s listed contacts were made. When the contact
person or affiliated individual was reached, the lead author
introduced himself and briefly identified the study and its
purpose. Occasionally, a follow-up e-mail was required,
which included a summary of what the study was about and
why we wanted access to their members and study mate-
rials such as consent forms and questionnaire were
attached. When agreeable, organization leaders granted
permission to us to attend meetings to announce the study,
distribute flyers, recruit participants, and in some cases
administer the intake protocol. We realized the potential
efficiency and efficacy of recruiting participants in this
manner and were aware of the collective social affiliations
that are characteristic of many Middle Easterners; there-
fore, in order to improve the likelihood of cooperation, an
incentive of $10 per affiliated participant or any non-
member that participated as a result of an affiliated par-
ticipant’s referral (snowball technique) was offered to an
organization to be used in any manner deemed appropriate.
(This offer was also made to P189 and P204, who identified
themselves as members of non-campus-based Lebanese
and Somali church and social groups, respectively).
Table 2 shows the number of organization members
(excluding non-members who were ‘‘snowballed’’ into the
study) recruited in this manner.
Being in the right place at the right time: Arab Student
Union. On Campus 1, the Arab Student Union (ASU) was
only active during spring semester 2005. After consider-
able explanation and reassurance by the coauthor, the ASU
president allowed us to present at upcoming meetings.
Typically, most attendees were female and saturation was
quickly reached. However, the ASU set out weekly infor-
mation tables in the university commons, and we were
welcomed to table with them. Additionally, one member
recruited friends and family into the study, whom the lead
author met at the family’s residence.
A case of contrasts: two Muslim Student Associations.
Unlike the ASU, the Muslim Student Associations’ (MSA)
memberships were partially composed of students who
were ineligible for the study based on nationality, which
posed an impediment on Campus 1, where the president
and vice-president of the MSA were Iranian and Afghan,
respectively. We made repeated attempts to contact them
and once formal contact was established ensuing commu-
nication demonstrated lengthy response latency. These
gatekeepers were cordial and respectful but not overly
enthusiastic toward the study and questioned why the focus
was on Arabs, thereby excluding their own participation.
Nevertheless, they permitted us to make several presenta-
tions at meetings throughout the semester, but in our
presence did not overtly encourage members. (There was
some overlap of the ASU and MSA membership that may
have contributed to a relatively weaker response by the
386 J Immigrant Minority Health (2009) 11:380–390
123

MSA considering the organization was contacted later than
the ASU. Additionally, the ASU was headed by an eligible
participant).
In contrast, the response of the MSA on Campus 2 was
much different. The vice president’s (P64) mother was a
close friend and colleague of the coauthor’s and encour-
aged her son to participate and help publicize the study. We
were invited to present at MSA’s regular Thursday night
Islamic Studies meeting. The MSA president and P64 (vice
president) were grateful for the group monetary contin-
gency that was offered and this aspect was reframed and
presented as sadaqah, the Islamic concept of extra charity
(beyond obligatory zakat). In addition to this meeting, the
lead author was welcomed to Friday afternoon Jummah
prayers, when the largest gathering of the organization’s
members and non-affiliates came to pray and listen to a
sermon. The lead author was given time during
announcements to announce the study, after which mem-
bers voluntarily approached him while P64 brought over
shier members.
Graduate Research Assistants (GRA)
Two GRAs (one is the coauthor)—both religious Muslims,
fluent speakers of Arabic, and ineligible for the study due
to their age—assisted in recruitment and protocol admin-
istration. Both were passionate about the study’s premise
and through assisting earned independent study credit
toward their respective Masters degrees in Exercise and
Nutritional Sciences.
Of the 26 participants they recruited, 88.5% were
Muslim, 65.4% were less acculturated, and 57.7% were
female (Table 2). Work associations, and random and
planned social encounters were channels by which they
independently recruited participants. Both were reticent of
approaching unknown members of the opposite sex, in
accordance with Islamic values. However, the male GRA’s
wife, a more acculturated and noticeably outgoing librarian
at Campus 4 (Table 2, Other), approached female Middle
Eastern-looking students in the library, and this approach
yielded nine female Muslim participants. The coauthor was
particularly effective in recruiting less acculturated par-
ticipants, particularly religious females who trusted her as a
co-religionist. She was adept at transparently explaining
the study and its purpose to participants and tying in Arab
and Muslim community ethos during personal encounters.
Problems Encountered
Despite it taking only 255 days to recruit all 240 partici-
pants, there were a number of events and factors that
prevented earlier completion of the study. First, the most
neutral term we could think of using to describe the par-
ticipants we were looking for was ‘‘Middle Eastern.’’
However, to avoid excessive inquiries from persons who
would have been ineligible, a list of countries of origin was
included on flyers and in presentations with a disclaimer
that persons of any religious faith with origins from one of
those countries were eligible. Nevertheless, we occasion-
ally experienced resentment from persons not of those
countries who may have known eligible persons but would
not refer them to us or vice versa; and by including Pal-
estine, there was one documented instance where a female
student voiced anger during a presentation as to the
exclusion of Israel and inclusion of Palestine and how she
would never participate even though she was eligible
through her grandparents’ birthplace.
Second, on our home campus, we could not get past
bureaucratic hurdles designed to limit synchronous access
to the entire student body in accordance with university
regulations. We were rebuffed or made to follow lengthy
due process to electronically advertise through various
large-scale channels and decided to abandon the effort.
Third, on Campuses 1 and 2, a number of operating
student organizations were splinter advocacy groups for
larger organizations that we had already contacted and thus
turned out to be dead ends. Other organizations that were
cultural in nature (e.g., Somali Student Union, Horn of
Africa, ASU, Coptic Club) either dragged their feet for such
time as to make us abandon our outreach attempts, flatly
denied our request, or deferred by stating that their orga-
nization was loosely organized and not meeting regularly.
Fourth, in the community, even when some extant
connection was tapped, the resultant product was nil. A
recent immigrant from Egypt, working at a local super-
market and referred by a coworker, would not participate
for fear of his immigrant status being used against him. An
Arab restaurant and supermarket were contacted and
seemingly positive meetings were held with the proprietors
who knew the coauthor, yet we were unsure if flyers given
to them were ever hung as we did not feel comfortable
following up with or pressing these persons further. The
health and welfare representative at one community out-
reach organization—which served Iraqi Kurds, Shiites, and
Chaldeans—met with the lead author, was supportive of
the study, and took flyers for distribution, but again our
instinct was not to follow up and no referrals came from
this source. The House of Palestine cultural group met with
us at its monthly business meeting and was supportive in
principle but only informally offered to disseminate the
existence of the study to its members. Unreturned phone
messages categorized our one attempt at contacting a
Sephardic Jewish rabbi with knowledge of eligible students
through his campus ministry.
J Immigrant Minority Health (2009) 11:380–390 387
123

Fifth, access to the ACS community was closely guar-
ded by one clergy member who on the community web site
indicated a distrust of Muslims; and a Chaldean graduate
student declined to assist in recruiting because it was his
belief that Chaldeans would be weary of wearing a
pedometer. Of the participants who were ACS, some made
attempts to speak with the head priest on our behalf, but
subsequently expressed discomfort doing so. (The authors
were advised not to cold call the church). During one
outtake meeting, over the course of several extra hours of
conversation, a Chaldean participant (P201) asked the lead
author to teach her about his religion. At various junctures
during the conversation, P201 volunteered that she was
taught differently about his faith and people by her parents,
family, and church and felt that many of her friends’ atti-
tudes were similar to hers, which bore tinges of
stereotypical thinking. These events in concert suggest that
targeting the ACS community directly without a respected
inside contact in support of the study was misinformed and
ACS participation was chiefly the result of snowball and
flyer methods used on campuses.
Sixth, medical doctors expressed interest in assisting
with recruitment in their communities. In one case, a
Somali doctor, who had practiced in the UAE initiated
contact with the lead author having heard about the study
from a Somali student. However, he was looking for
employment and expected to be compensated beyond the
lead author’s means. In a second case, P113’s father ran a
pediatric and young adult medicine clinic that catered to
Middle Eastern persons and was also on the Board of
Directors of the city’s Islamic Center. P113’s intent was to
recruit participants at his father’s practice over the summer;
however, he received late notice of acceptance into medical
school and relocated.
We did not systematically query non-participants as to
their reasons for declination. However, recruiters identified
the following reasons for non-participation based on
informal conversations with non-participants: (1) They did
not know of anyone who was eligible; (2) did not have the
time or resolve to participate or contact others; (3) claimed
their own or acquaintances’ lack of interest in the study; (4)
found it to be too involved or require too much effort; (5)
were reluctant to wear the pedometer due to inconvenience,
discomfort, fear of being under surveillance, or the device
being construed by others as threatening or a weapon; (6)
were concerned about repercussions from responding to
portions of the questionnaire regarding citizenship status,
language use, and religiosity; (7) felt that their answers
would result in them being branded as radical or too liberal;
(8) claimed that the compensation for participation was
insufficient; (9) felt the study’s purpose was a pretense for
some underlying negative motive directed at Middle
Eastern persons; or (10) some combination.
Discussion and Lessons Learned
A purposeful mixed-method recruitment strategy was used
to obtain an adequately sized sample of Middle Eastern
American young adults, similar to procedures used in other
studies recruiting ethnic minority groups with heteroge-
neous membership [43, 44]. Relying on one or two
methods would have proved insufficient for ample
recruitment or would have extended the time required to
recruit 240 persons, similar to what Barry encountered
[39]. While recruitment methods need to be planned in
advance, methods need to be adjusted in response to events
at hand, particularized for specific venues and subgroups,
and be implemented at multiple sites.
Peripheral, evidential, linguistic, constituent involving
and sociocultural adaptations recommended by Kreuter and
colleagues [34] were all incorporated in the study with the
latter two being most prominent.
To address constituent involvement, we recommend the
inclusion of input from those who perform research and are
also members of the community of interest (i.e., academic
colleagues from the Center for Islamic and Arab Studies)
during the planning stages of a study. Without their unique
knowledge, it is quite possible that a major error in judg-
ment may have been made that would negatively impact
recruitment. Staffing with members of the community,
particularly in roles that interface directly with participants,
is another important piece of constituent involvement. We
employed male/female and Muslim/non-Muslim Arabs,
which helped in gaining access to individuals and groups.
We were not as effective recruiting from the large East
African community in San Diego, which may have
reflected the absence of a Somali research assistant or
someone who spoke the language or knew the customs
(i.e., Somalis are typically not Arab).
To address sociocultural adaptations, we recommend
that researchers be versed in the social dynamics, cus-
toms, language, and beliefs of the target population. For
example, incentives were reframed in Islamic terms as
charity when interacting with Muslim organizations.
Findings and recommendations specific to Arab American
recruitment [38, 39] were corroborated in this study:
Experts’ recommendations were not always accurate;
some non-participants were concerned about the study
casting Arabs in a bad light; community gatekeepers were
not particularly nor uniformly helpful; personal contact
was a successful means of recruitment; ample budgeting
of time but not money (only $10,000 was available) was
required; and access was facilitated by assistants who
were also community insiders.
Strategies aimed at the community (e.g., houses of
worship, businesses, community outreach organizations)
were only tepidly pursued per expert recommendation and
388 J Immigrant Minority Health (2009) 11:380–390
123

in most cases failed. In hindsight, we see the need for
establishing connections early with off-campus community
leaders who have connections with the young adult
demographic we were seeking. Clearly presenting our
objectives and connecting the study to the entire commu-
nity’s welfare while identifying suitable reinforcement for
cooperation may have resulted in additional recruits.
At the organizational level (e.g., social- and religious-
oriented clubs), a more focused approach was aggressively
pursued, which included organizational incentives and
results were more positive, yet still inconsistent. While
extremely convenient for the researchers, presentations
took away from regularly scheduled agenda items and were
sometimes not made known to members beforehand. We
recommend getting in touch with campus organizations
very early in a semester so they can commit to a presen-
tation without it interfering with other business. Providing
refreshments and prizes in addition to the monetary
incentives may increase positive response.
At the individualistic level, a combination of active (i.e.,
personal contacts with the authors, assistants, and previous
participants) and passive (i.e., flyers) recruitment strategies
yielded the most successful response. Personal face-to-face
contact also characterizes the most successful recruitment
method of other studies of Arab Americans’ health behavior
[36, 38], whereas the less successful passive methods of this
study were utilized with more success in studies conducted
by research teams composed of at least one community
insider who was not a graduate student, in denser Arab
American communities, and with older community
members [22, 35, 37]. We recommend active recruitment
strategies that engage participants convivially and not
clinically (i.e., establishing a respectful and personal rela-
tionship with participants that extends beyond labeling them
as P1, P2, etc.).
Combined, the success of individualistic and organi-
zational methods employed in the present study may be
attributable to several explanations singularly or in
combination: (1) a desire to educate an outsider (lead
author) so he could realize the value or truth of Islam
[45] and clear up misperceptions associated with Arab
Americans; (2) a good fit of snowball methods for this
sample, whose self-identity and social circle were pre-
dominantly skewed toward Middle Easterners (Table 1);
(3) a sample that was more educated and more receptive
to research (i.e., 54.2 and 75.4% of participants’ mothers
and fathers, respectively had at least some college edu-
cation); (4) a sample that was linguistically comfortable
with English (Table 1); (5) data collectors who were
willing to meet with participants at times and places
convenient to the latter; and (6) energetic assistants who
were community insiders and who were diverse reli-
giously and culturally.
Limitations and Key Suggestions
We acknowledge the limitations of this study as being
context specific to demographic (young adults who pri-
marily were attending college), region (southern
California), time (4 years after the events of September
11, 2001) and purpose (observational study of physical
activity behavior). We were also somewhat unsystematic
from a methodological standpoint, as we used multiple
strategies and shifted between them based on their effi-
cacy with a certain subgroup; however, such an approach
is noted in the literature [39, 43, 46]. Similar to other
studies [38, 46], it is impossible to disentangle the effect
of any one strategy from others because in some cases
multiple methods acted synergistically but in unquantifi-
able ways. For example, when a faculty member
announced the study on Campus 2, he was told by his
students that they had already participated or knew of the
study through flyers or friends.
Key suggestions for recruiting from this demographic
include outsiders learning about the target group as a
gesture of respect and goodwill, foregrounding active
recruitment strategies, stimulating the snowballing effect
through systematic follow up of participants, allocating an
additional monetary incentive for every successful referral,
including insiders in the planning and recruitment stages,
budgeting large chunks of time for travel, as well as being
flexible to accommodate the contingencies for participation
posed by the prospective participant. Additional accounts
and analyses of methodology employed in studying
minority health are welcomed, whether they are particu-
laristic or reinforce findings obtained under different
conditions.
References
1. Malone N, Baluja T, Costanzo JM, Davis CJ. The foreign-born
population: 2000. Census 2000 brief. (on-line). 2003.
http://www.census.gov/prod/2003pubs/c2kbr-34.pdf. Accessed
Feb 2007.
2. U.S. Census Bureau: Race and Hispanic Origin in 2004. (Internet
Release Dynamic Version). (on-line). http://www.census.gov/
population/pop-profile/2000/chap16.pdf. Accessed Feb 2007.
3. Zsembik BA, Fennell D. Ethnic variation in health and deter-
minants of health among Latinos. Soc Sci Med 2005;61:53–63.
4. Woodward LD, Hernandez MT, Lees E, Petersen LA. Racial
differences in attitudes regarding cardiovascular disease preven-
tion and treatment: a qualitative study. Patient Educ Couns
2005;57:225–31.
5. Paskett ED, Tatum C, Rushing J, Michielutte R, Bell R, Foley
KL, Bittoni M, Dickinson S. Racial differences in knowledge,
attitudes, and cancer screnning practices among a triracial rural
population. Cancer 2004;101:2650–9.
6. Mensah GA, Mokdad AH, Ford ES, Greenlund KJ, Croft JB.
State of disparities in cardiovascular health in the United States.
Circulation 2005;111:1233–41.
J Immigrant Minority Health (2009) 11:380–390 389
123

7. Read JG, Emerson MO, Tarlov A. Implications of black immi-
grant health for U.S. racial disparities in health. J Immigr Health
2005;7:205–12.
8. Shavers VL, Shavers BS. Racism and health inequity among
Americans. J Natl Med Assoc 2006;98:386–96.
9. Winkleby MA, Cubbin C. Influence of individual and neigh-
bourhood socioeconomic status on mortality among black,
Mexican-American, and white women and men in the United
States. J Epidemiol Community Health 2003;57:444–52.
10. Robert SA, Reither EN. A multilevel analysis of race, community
disadvantage, and body mass index among adults in the US. Soc
Sci Med 2004;59:2421–34.
11. Kirby JB, Taliaferro G, Zuvekas SH. Explaining racial and ethnic
disparities in health care. Med Care 2006;44 Suppl:I64–72.
12. Brown ML, Lipscomb J, Snyder C. The burden of illness of
cancer: economic cost and quality of life. Annu Rev Public
Health 2001;22:91–113.
13. Wang G, Zhi-Jie Z, Heath G, Macera C, Pratt MD, Buchner D.
Economic burden of cardiovascular disease associated with
excess body weight in US adults. Am J Prev Med 2002;23:1–6.
14. Bach PB. Costs of cancer care: a view from the centers of
Medicare and Medicaid services. J Clin Oncol 2007;25:187–90.
15. McManus SM, Pohl CM. Ethics and financing: overview of the
U.S. health care system. J Health Hum Resour Adm
1994;16:332–49.
16. Francis CK. The medical ethos and social responsibility in clin-
ical medicine. J Natl Med Assoc 2001;93:157–69.
17. Betancourt JR. Eliminating racial and ethnic disparities in
healthcare: what is the role of academic medicine? Acad Med
2006;81:788–92.
18. U.S. Department of Health and Human Services. Healthy people
2010. 2nd ed. Washington, DC: U.S. Government Printing Office;
2000.
19. de la Cruz PG, Brittingham A. The Arab population. 2000.
Census 2000 brief. (on-line). 2003. http://www.census.gov/prod/
2003pubs/c2kbr-23.pdf. Accessed Feb 2007.
20. Jaber LA, Brown MB, Hammad A, Nowak SN, Zhu Q, Ghafoor
A, Herman WH. Epidemiology of diabetes among Arab Ameri-
cans. Diabetes Care 2003;26:308–13.
21. Hatahet W, Khosla P, Fungwe TV. Prevalence of risk factors to
coronary heart disease in an Arab-American population of
Southeast Michigan. Int J Food Sci Nutr 2002;53:325–35.
22. Dallo FJ, James SA. Acculturation and blood pressure in a com-
munity-based sample of Chaldean-American women. J Immigr
Health 2000;2:145–53.
23. Darwish-Yassine M, Wing D. Cancer epidemiology in Arab
Americans and Arabs outside the Middle East. Ethn Dis 2005;15
Suppl 1:S5–8.
24. Hassoun R. Arab American health and the process of coming to
America: lessons from the metropolitan Detroit area. In: Sulei-
man M, editor. Arabs in America building a new future.
Philadelphia: Temple University Press; 2000. p. 157–76.
25. Aswad M. Health survey of the Arab, Muslim, Chaldean Amer-
ican communities in Michigan. Dearborn, MI: ACCESS
Community Health and Research Center; 2001.
26. Bryan SN, Tremblay MS, Perez CE, Ardern CI, Katzmarzyk PT.
Physical activity and ethnicity: evidence from the Canadian
Community Health Survey. Can J Public Health 2006;97:271–6.
27. Tremblay MS, Bryan SN, Perez CE, Ardern CI, Katzmarzyk PT.
Physical activity and immigrant status: evidence from the
Canadian Community Health Survey. Can J Public Health
2006;97:277–82.
28. Lindstrom ML, Sundquist J. Immigration and leisure-time phys-
ical inactivity: a population-based study. Ethn Health 2001;6:77–
85.
29. Sparling PB. College physical education: an unrecognized agent
of change in combating inactivity-related diseases. Perspect Biol
Med 2003;46:579–87.
30. Abudabbeh N. Arab families: an overview. In: McGoldrick M,
Giordano J, Garcia-Preto N, editors. Ethnicity and family therapy.
3rd ed. New York: Guilford Press; 2005. p. 423–36.
31. Benoit C, Jansson M, Millar A, Phillips R. Community-academic
research on hard-to-reach populations: benefits and challenges.
Qual Health Res 2005;15:263–82.
32. Yancey AK, Ortega AN, Kumanyika SK. Effective recruitment
and retention of minority research participants. Annu Rev Public
Health 2006;27:1–28.
33. Alvarez RA, Vasquez E, Mayorga CC, Feaster DJ, Mitrani VB.
Increasing minority research participation through community
organization outreach. West J Nurs Res 2006;28:541–60.
34. Kreuter MW, Lukwago SN, Bucholtz RD, Clark EM, Thompson
V. Achieving cultural appropriateness in health promotion pro-
grams: targeted and tailored approaches. Health Educ Behav
2003;30:133–46.
35. Barry DT. Measuring acculturation among male Arab immigrants
in the United States: an exploratory study. J Immigr Health
2005;7:179–84.
36. Johnson M, Nriagu J, Hammad A, Savoie K, Jamil H. Asthma
prevalence and severity in Arab American communities in the
Detroit Area, Michigan. J Immigr Health 2005;7:165–78.
37. Hatahet W, Fungwe TV. Obesity and cardiovascular disease risk
factors are ethnicity based: a study of women of different ethnic
backgrounds in southeastern Michigan. Ethn Dis 2005;15 Suppl
1:S23–5.
38. Aroian KJ, Katz A, Kulwicki A. Recruiting and retaining Arab
Muslim mothers and children for research. J Nurs Scholarsh
2006;38:255–61.
39. Barry DT. Assessing culture via the Internet: methods and tech-
niques for psychological research. Cyberpsychol Behav
2001;4:17–21.
40. U.S. Census Bureau. American Fact Finder. Fact Sheet for a
Race, Ethnic, or Ancestry Group. (on-line). http://factfinder.
census.gov/servlet/
SAFFFactsCharIteration?_submenuId=factsheet_2&_sse=on.Accessed Jan 2007.
41. Kurdish Human Rights Watch. Communities in San Diego. (on-
line). http://www.khrw.com/sandiego/community.html. Accessed
Jan 2007.
42. Ulin PR, Robinson ET, Tolley EE. Qualitative methods in public
health: a field guide for applied research. San Francisco: Jossey-
Bass; 2005.
43. Hughes AO, Fenton S, Hine CE. Strategies for sampling black
and minority populations. J Public Health Med 1995;17:187–92.
44. Lee SK, Cheng YY. Reaching Asian Americans: sampling
strategies and incentives. J Immigr Minor Health 2006;8:245–50.
45. Walseth K, Fasting K. Islam’s view on physical activity and
sport. Int Rev Sociol Sport 2003;38:45–60.
46. Han HR, Kang J, Kim KB, Ryu JP, Kim MT. Barriers to and
strategies for recruiting Korean Americans for community-part-
nered health promotion research. J Immigr Minor Health
2007;9:137–46.
47. Marin G, Sabogal F, Marin BV, Otero-Sabogal R, Perez-Stable
EJ. Development of a short acculturation scale for Hispanics.
Hisp J Behav Sci 1987;9:183–205.
390 J Immigrant Minority Health (2009) 11:380–390
123