Occlusal adjustment for treating and preventing temporomandibular ...
Strategies for preventing and treating IFALD
Dr Sue Beath The Liver Unit (including small bowel transplantation) [email protected]
Birmingham Children’s Hospital
Strategies for preventing and treating IFALD
Intestinal failure associated liver disease IFALD in children is a manifestation of a systemic inflammatory response syndrome (SIRS) often triggered by sepsis
Scenarios which increase the intensity of SIRS • surgery • invasive care NICU/PICU
Also known as Parenteral Nutrition Associated Cholestastis (PNAC), but IFALD is to be preferred as it focuses attention on the whole context of intestinal failure and not just the PN infusions
Strategies for preventing and treating IFALD
Why worry about intestinal failure associated liver disease • over 1000 children on PN per year and at risk of IFALD • about half have abnormal liver function • of those who are referred for small bowel transplant half
have advanced liver disease (type 3 IFALD; bilirubin >100 micromol/L)
• IFALD (esp type 3) increases the risk of mortality • neonates and children are more susceptible to IFALD than adults • liver transplantation is an option but v. high risk in context of IF
Strategies for preventing and treating IFALD
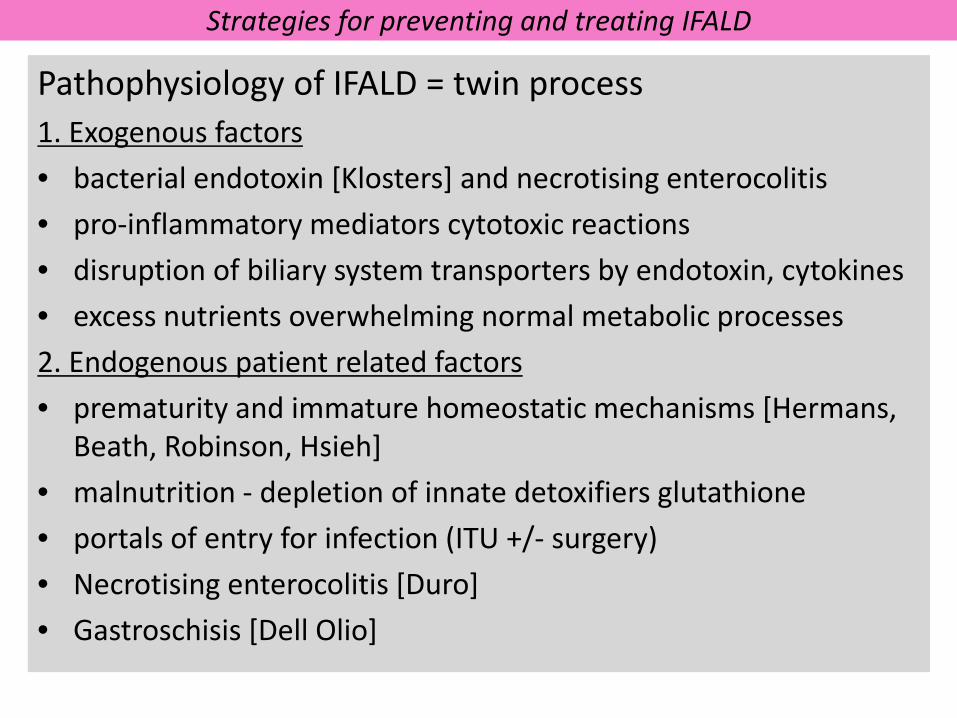
Pathophysiology of IFALD = twin process 1. Exogenous factors • bacterial endotoxin [Klosters] and necrotising enterocolitis • pro-inflammatory mediators cytotoxic reactions • disruption of biliary system transporters by endotoxin, cytokines • excess nutrients overwhelming normal metabolic processes 2. Endogenous patient related factors • prematurity and immature homeostatic mechanisms [Hermans,
Beath, Robinson, Hsieh] • malnutrition - depletion of innate detoxifiers glutathione • portals of entry for infection (ITU +/- surgery) • Necrotising enterocolitis [Duro] • Gastroschisis [Dell Olio]
Strategies for preventing and treating IFALD
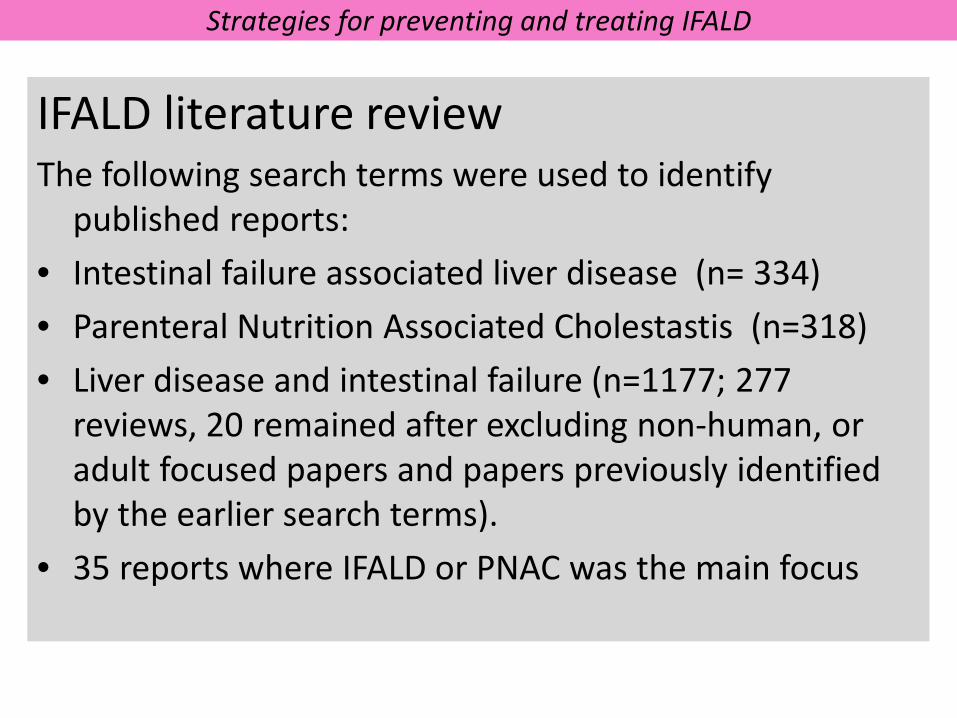
IFALD literature review The following search terms were used to identify
published reports: • Intestinal failure associated liver disease (n= 334) • Parenteral Nutrition Associated Cholestastis (n=318) • Liver disease and intestinal failure (n=1177; 277
reviews, 20 remained after excluding non-human, or adult focused papers and papers previously identified by the earlier search terms).
• 35 reports where IFALD or PNAC was the main focus
Strategies for preventing and treating IFALD
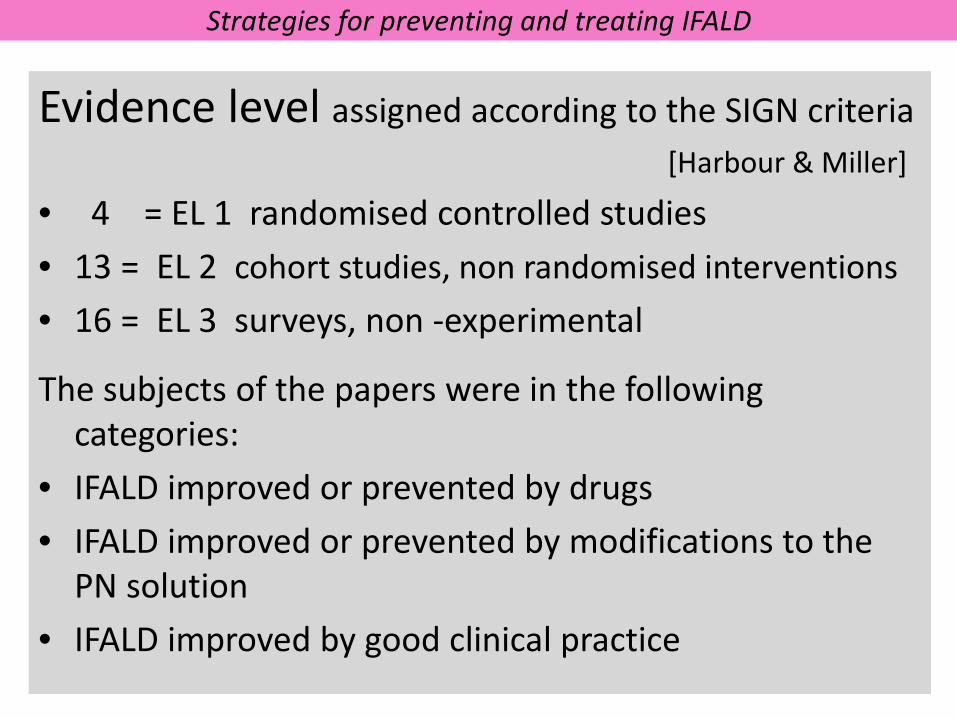
Evidence level assigned according to the SIGN criteria [Harbour & Miller]
• 4 = EL 1 randomised controlled studies • 13 = EL 2 cohort studies, non randomised interventions • 16 = EL 3 surveys, non -experimental
The subjects of the papers were in the following categories:
• IFALD improved or prevented by drugs • IFALD improved or prevented by modifications to the
PN solution • IFALD improved by good clinical practice
Strategies for preventing and treating IFALD
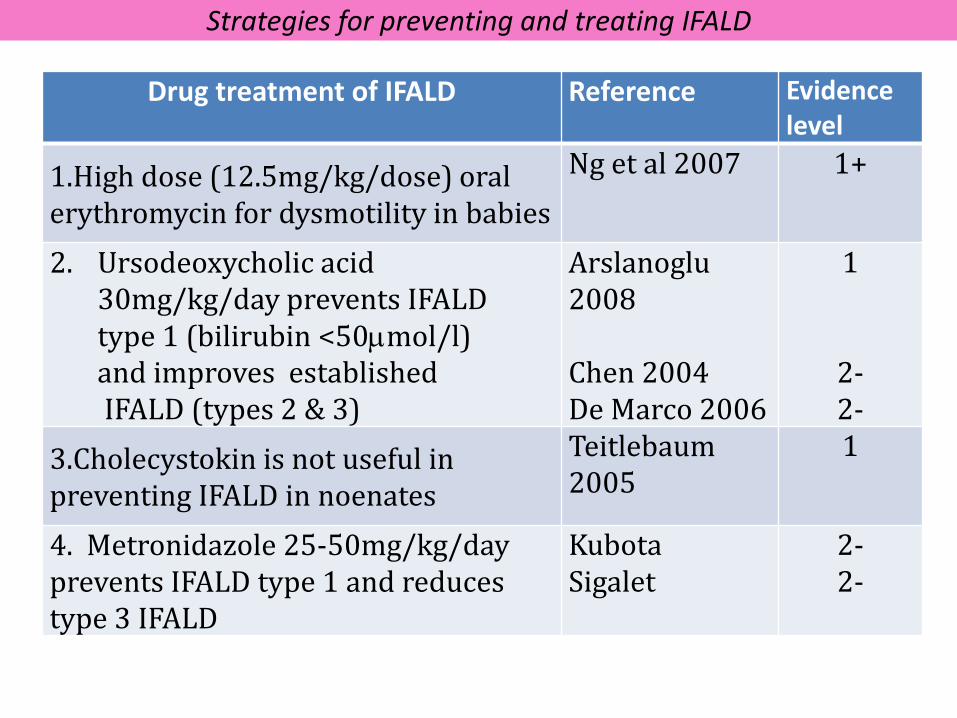
Drug treatment of IFALD Reference Evidence level
1.High dose (12.5mg/kg/dose) oral erythromycin for dysmotility in babies
Ng et al 2007 1+
2. Ursodeoxycholic acid 30mg/kg/day prevents IFALD type 1 (bilirubin <50µmol/l)
and improves established IFALD (types 2 & 3)
Arslanoglu 2008 Chen 2004 De Marco 2006
1
2- 2-
3.Cholecystokin is not useful in preventing IFALD in noenates
Teitlebaum 2005
1
4. Metronidazole 25-50mg/kg/day prevents IFALD type 1 and reduces type 3 IFALD
Kubota Sigalet
2- 2-
Strategies for preventing and treating IFALD
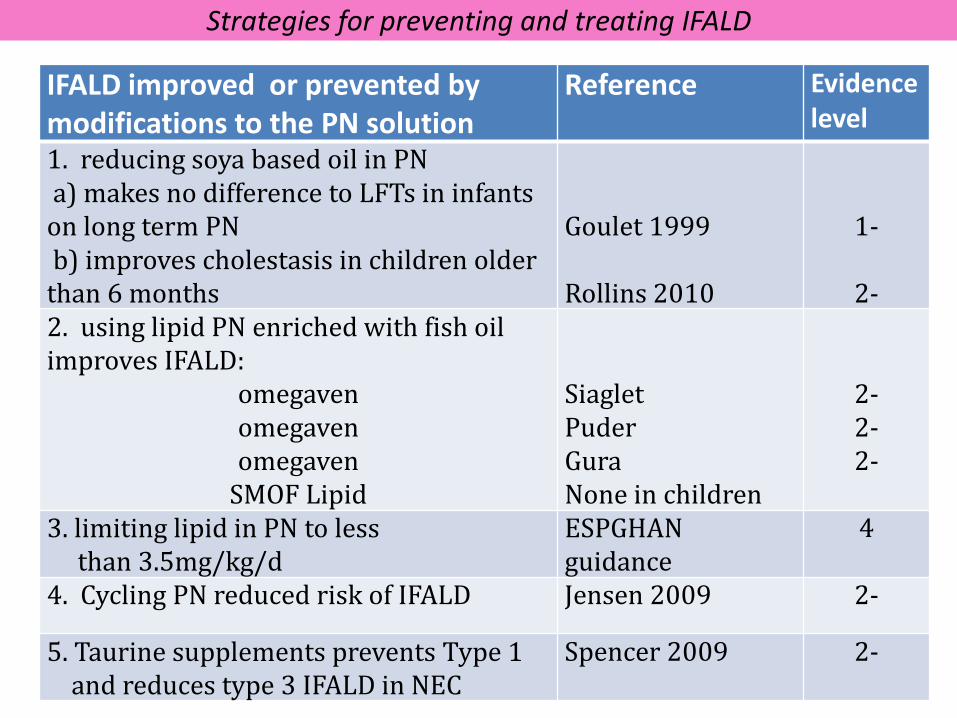
IFALD improved or prevented by modifications to the PN solution
Reference Evidence level
1. reducing soya based oil in PN a) makes no difference to LFTs in infants on long term PN b) improves cholestasis in children older than 6 months
Goulet 1999 Rollins 2010
1-
2- 2. using lipid PN enriched with fish oil improves IFALD:
omegaven omegaven omegaven
SMOF Lipid
Siaglet Puder Gura None in children
2- 2- 2-
3. limiting lipid in PN to less than 3.5mg/kg/d
ESPGHAN guidance
4
4. Cycling PN reduced risk of IFALD Jensen 2009 2-
5. Taurine supplements prevents Type 1 and reduces type 3 IFALD in NEC
Spencer 2009 2-
Strategies for preventing and treating IFALD
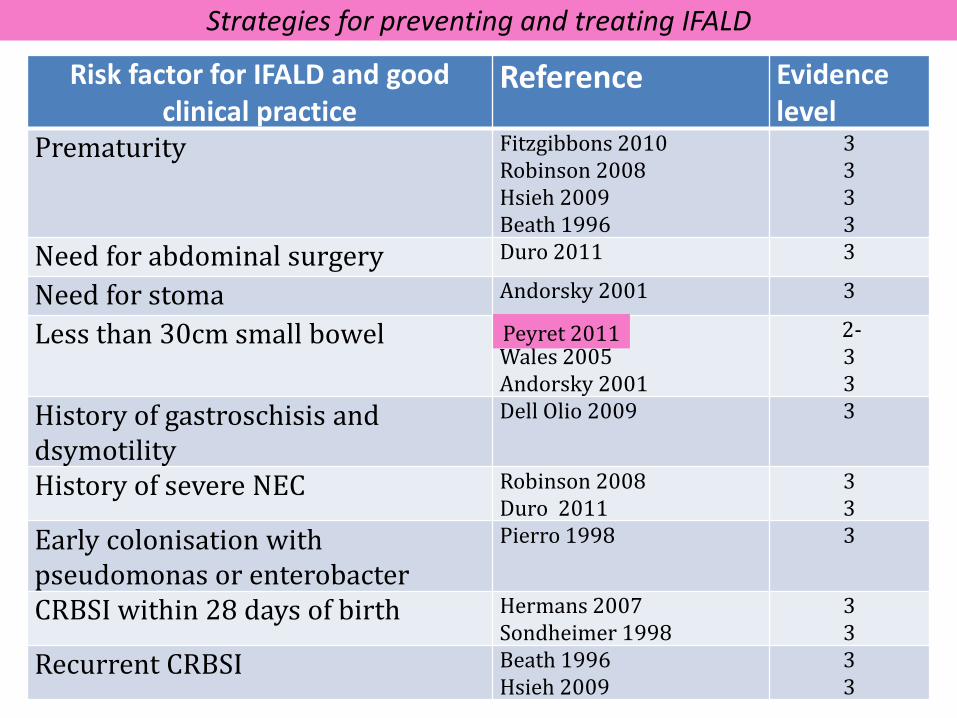
Risk factor for IFALD and good clinical practice
Reference Evidence level
Prematurity Fitzgibbons 2010 Robinson 2008 Hsieh 2009 Beath 1996
3 3 3 3
Need for abdominal surgery Duro 2011 3
Need for stoma Andorsky 2001 3
Less than 30cm small bowel Wales 2005 Andorsky 2001
2- 3 3
History of gastroschisis and dsymotility
Dell Olio 2009 3
History of severe NEC Robinson 2008 Duro 2011
3 3
Early colonisation with pseudomonas or enterobacter
Pierro 1998 3
CRBSI within 28 days of birth Hermans 2007 Sondheimer 1998
3 3
Recurrent CRBSI Beath 1996 Hsieh 2009
3 3
Peyret 2011
Strategies for preventing and treating IFALD
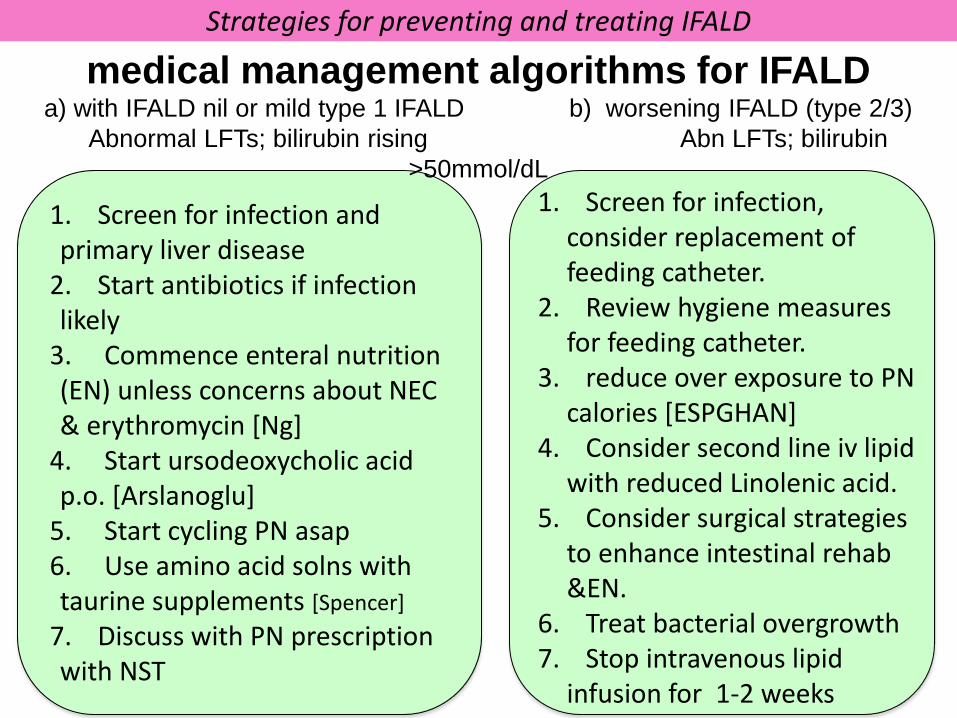
1. Screen for infection and primary liver disease
2. Start antibiotics if infection likely
3. Commence enteral nutrition (EN) unless concerns about NEC & erythromycin [Ng]
4. Start ursodeoxycholic acid p.o. [Arslanoglu]
5. Start cycling PN asap 6. Use amino acid solns with taurine supplements [Spencer]
7. Discuss with PN prescription with NST
1. Screen for infection, consider replacement of feeding catheter.
2. Review hygiene measures for feeding catheter.
3. reduce over exposure to PN calories [ESPGHAN]
4. Consider second line iv lipid with reduced Linolenic acid.
5. Consider surgical strategies to enhance intestinal rehab &EN.
6. Treat bacterial overgrowth 7. Stop intravenous lipid
infusion for 1-2 weeks
medical management algorithms for IFALD a) with IFALD nil or mild type 1 IFALD b) worsening IFALD (type 2/3)
Abnormal LFTs; bilirubin rising Abn LFTs; bilirubin >50mmol/dL
Strategies for preventing and treating IFALD
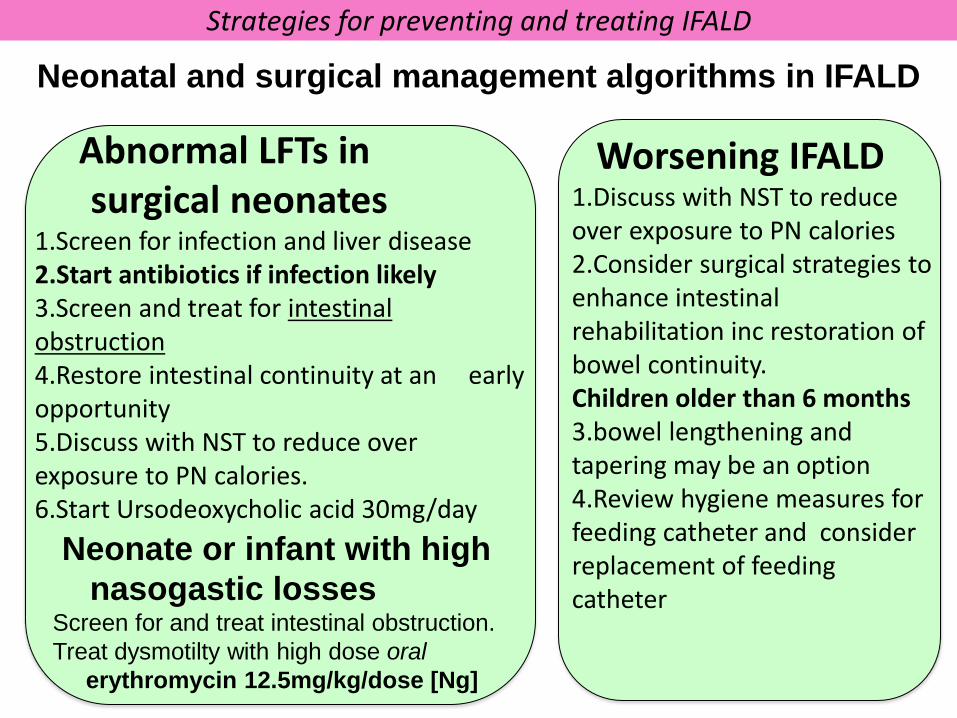
Neonatal and surgical management algorithms in IFALD
Neonate or infant with high nasogastic losses Screen for and treat intestinal obstruction. Treat dysmotilty with high dose oral erythromycin 12.5mg/kg/dose [Ng]
Abnormal LFTs in surgical neonates 1.Screen for infection and liver disease 2.Start antibiotics if infection likely 3.Screen and treat for intestinal obstruction 4.Restore intestinal continuity at an early opportunity 5.Discuss with NST to reduce over exposure to PN calories. 6.Start Ursodeoxycholic acid 30mg/day
Worsening IFALD 1.Discuss with NST to reduce over exposure to PN calories 2.Consider surgical strategies to enhance intestinal rehabilitation inc restoration of bowel continuity. Children older than 6 months 3.bowel lengthening and tapering may be an option 4.Review hygiene measures for feeding catheter and consider replacement of feeding catheter
Strategies for preventing and treating IFALD
IFALD in setting of long term intestinal failure
1. Discharge to home with NST supporting care of Home PN [Puntis, Hess]
2. Review prescription to reduce over exposure to PN calories [ESPGHAN]
3. Introduce lipid free days / Consider alternative type of PN lipid
4. Screen for infection and treat as indicated, consider replacement of feeding catheter.
5. Consider alternative type of PN lipid If IFALD worsens or does not resolve Consult specialist centre for suitability of liver +/- small bowel transplant
Strategies for preventing and treating IFALD
Currently the only EL 1 studies in IFALD are: High-dose oral erythromycin (12.5 mg/kg/dose) to be used as a rescue
measure for VLBW infants who fail to establish adequate EN and in whom intestinal obstruction has been excluded
EL1+ Ng 2007
UDCA p.o. should be routinely administered to infants who are receiving minimal oral/enteral feeding
EL1+ Arslanoglu 2008
Cholecystokin is not useful in preventing IFALD in neonates EL1++ Teitlebaum 2005
Reducing soya based oil in lipid component of PN makes no difference to LFTs in infants on long term PN
EL1- Goulet 1999
Strategies for preventing and treating IFALD
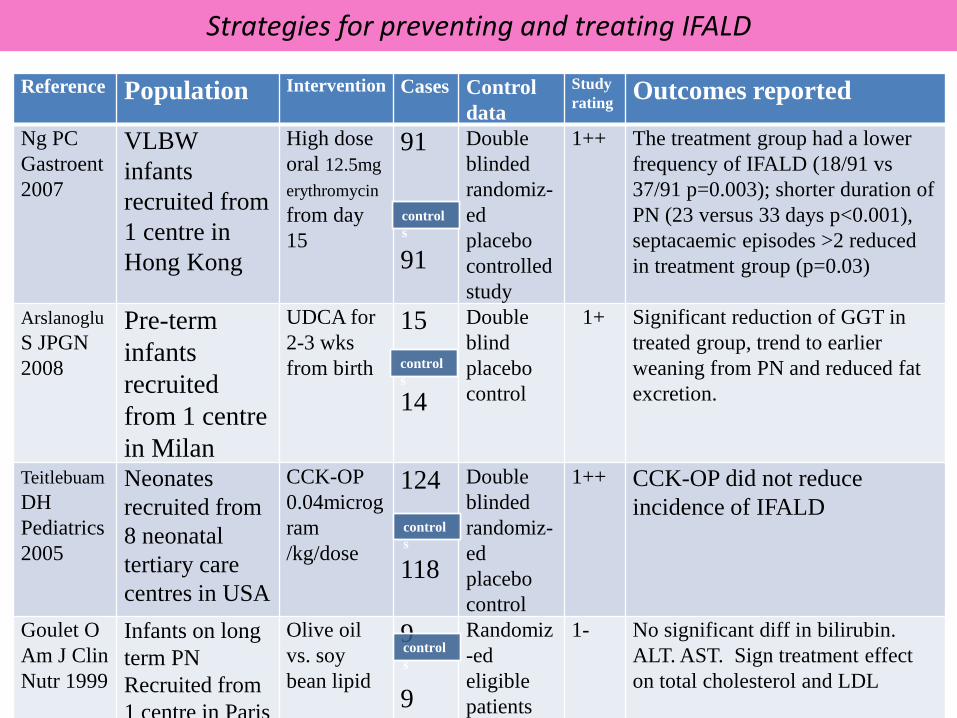
Reference Population Intervention Cases Control data
Study rating Outcomes reported
Ng PC Gastroent 2007
VLBW infants recruited from 1 centre in Hong Kong
High dose oral 12.5mg erythromycin from day 15
91 91
Double blinded randomiz-ed placebo controlled study
1++ The treatment group had a lower frequency of IFALD (18/91 vs 37/91 p=0.003); shorter duration of PN (23 versus 33 days p<0.001), septacaemic episodes >2 reduced in treatment group (p=0.03)
Arslanoglu S JPGN 2008
Pre-term infants recruited from 1 centre in Milan
UDCA for 2-3 wks from birth
15
14
Double blind placebo control
1+ Significant reduction of GGT in treated group, trend to earlier weaning from PN and reduced fat excretion.
Teitlebuam DH Pediatrics 2005
Neonates recruited from 8 neonatal tertiary care centres in USA
CCK-OP 0.04microgram /kg/dose
124 118
Double blinded randomiz-ed placebo control
1++ CCK-OP did not reduce incidence of IFALD
Goulet O Am J Clin Nutr 1999
Infants on long term PN Recruited from 1 centre in Paris
Olive oil vs. soy bean lipid
9
9
Randomiz-ed eligible patients
1- No significant diff in bilirubin. ALT. AST. Sign treatment effect on total cholesterol and LDL
controls
controls
controls
controls
1. Ng PC, et al High-dose oral erythromycin decreased the incidence of parenteral nutrition-
associated cholestasis in preterm infants. Gastroenterology. 2007;132:1726-39. 2. Arslanoglu S et al Ursodeoxycholic acid treatment in preterm infants: a pilot study for the
prevention of cholestasis associated with total parenteral nutrition. J Pediatr Gastroenterol Nutr. 2008;46:228-31.
3. Guidelines on paediatric parenteral nutrition J Pediatr Gastroenterol Nutr 2005;41;suppl 4. Sigalet D et Improvd outcomes in paediatric intestinal failure with aggressive prevention of
liver disease. Eur J Pedaitr Surg 2009; 19: 348-53.
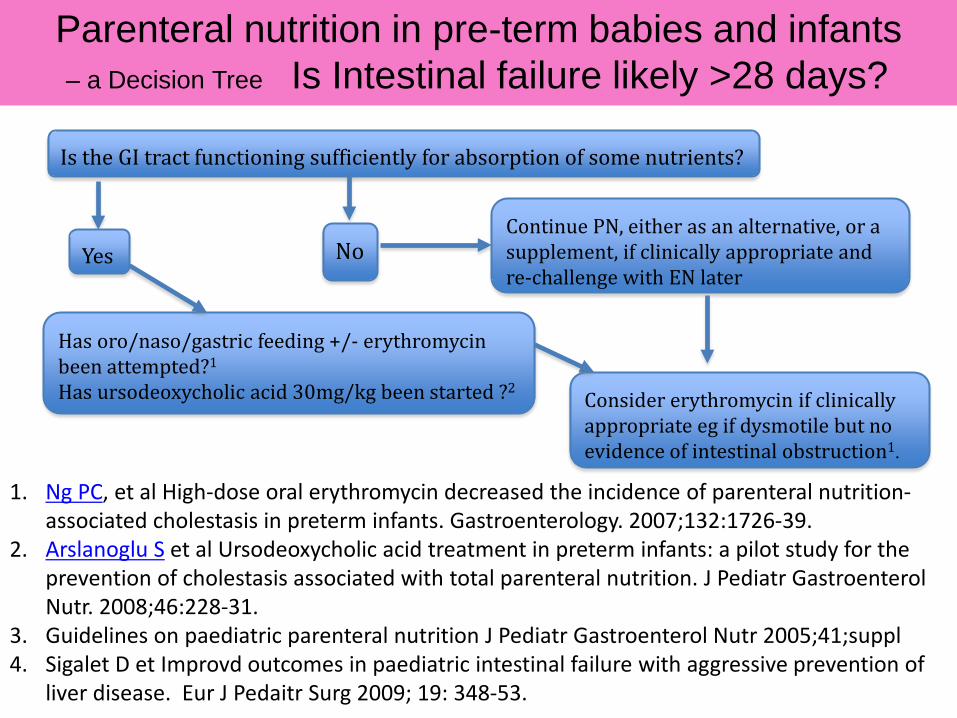
Is the GI tract functioning sufficiently for absorption of some nutrients?
Continue PN, either as an alternative, or a supplement, if clinically appropriate and re-challenge with EN later
Has oro/naso/gastric feeding +/- erythromycin been attempted?1
Has ursodeoxycholic acid 30mg/kg been started ?2 Consider erythromycin if clinically appropriate eg if dysmotile but no evidence of intestinal obstruction1.
Parenteral nutrition in pre-term babies and infants – a Decision Tree Is Intestinal failure likely >28 days?
No Yes
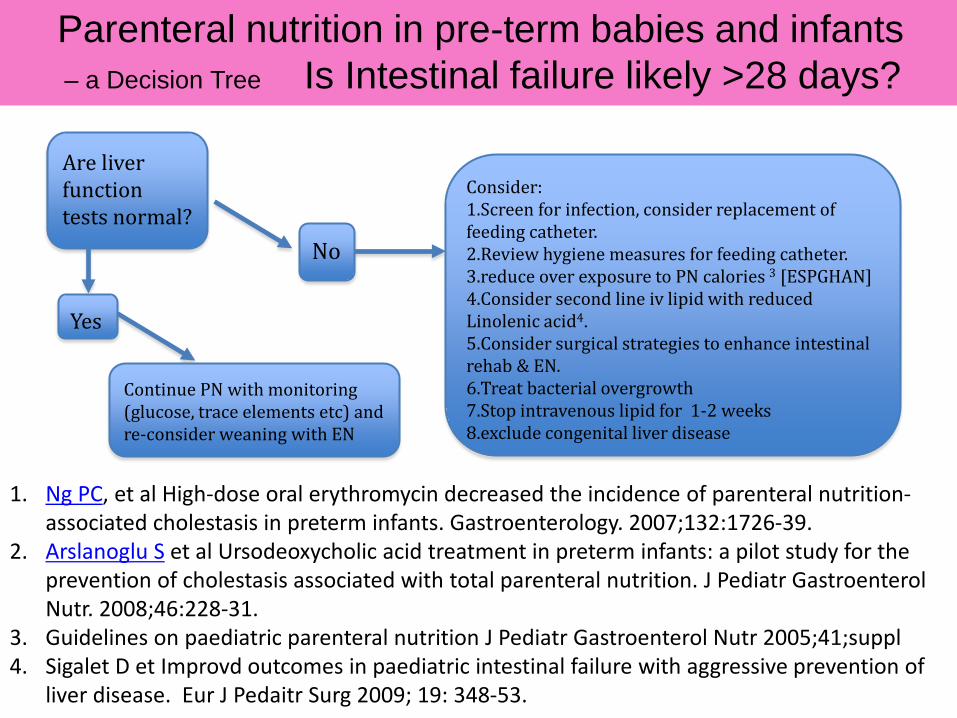
1. Ng PC, et al High-dose oral erythromycin decreased the incidence of parenteral nutrition-
associated cholestasis in preterm infants. Gastroenterology. 2007;132:1726-39. 2. Arslanoglu S et al Ursodeoxycholic acid treatment in preterm infants: a pilot study for the
prevention of cholestasis associated with total parenteral nutrition. J Pediatr Gastroenterol Nutr. 2008;46:228-31.
3. Guidelines on paediatric parenteral nutrition J Pediatr Gastroenterol Nutr 2005;41;suppl 4. Sigalet D et Improvd outcomes in paediatric intestinal failure with aggressive prevention of
liver disease. Eur J Pedaitr Surg 2009; 19: 348-53.
Consider: 1.Screen for infection, consider replacement of feeding catheter. 2.Review hygiene measures for feeding catheter. 3.reduce over exposure to PN calories 3 [ESPGHAN] 4.Consider second line iv lipid with reduced Linolenic acid4. 5.Consider surgical strategies to enhance intestinal rehab & EN. 6.Treat bacterial overgrowth 7.Stop intravenous lipid for 1-2 weeks 8.exclude congenital liver disease
Are liver function tests normal?
No
Yes
Continue PN with monitoring (glucose, trace elements etc) and re-consider weaning with EN
Parenteral nutrition in pre-term babies and infants – a Decision Tree Is Intestinal failure likely >28 days?
Strategies for preventing and treating IFALD
Research Recommendations in IFALD Multicentre studies needed to achieve recruitment of 50+
subjects for: • Multi-source lipids in cognitive and hepatic outcomes • Erythromycin as a treatment for dysmotility in term
infants and high risk groups eg in gastroschisis • Biochemical markers of liver fibrosis • Treatments which reduce CRBSI which is an important
factor in IFALD (eg line locks) in hospitalized and home PN patients