Stopping Sepsis in Virginia Hospitals and Nursing Homes · 2017-10-10 · Stopping Sepsis in...
81
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #5- Thursday, September 21, 2017
Transcript of Stopping Sepsis in Virginia Hospitals and Nursing Homes · 2017-10-10 · Stopping Sepsis in...

Stopping Sepsis in Virginia Hospitals and Nursing Homes
Hospital Webinar #5- Thursday, September 21, 2017

Welcome and Introductions
Today’s Objectives:
• Discuss Post Sepsis Syndrome and Post ICU Syndrome
• Address Handouts and Improving Communications (verbal and written)
• Stopping Sepsis Project Updates• Next Steps
2

John Lawrence, RN, BSNStroke & Sepsis Coordinator
INOVA Mount Vernon HospitalAlexandria, VA
Collaboration Spotlight
3

Your Sepsis Support Team
Deborah Smith, MTL(ASCP),
BSN,CIC, CPHQImprovement
Consultant
Candy Hamner,RN, BA, MA
Improvement Consultant
Betsy Cole Archer ,MS, ASCP
Sr. Director, Performance Improvement
Joyce Dayvault, RN, BBA
Director, Performance Improvement
4
Lisa Mark,RN, BSN
Improvement Consultant

Your Sepsis Content Expert
5
Kathleen M. Vollman RN, MSN, CCNS, FCCM, FAAN
Clinical Nurse Specialist/Educator/ConsultantADVANCING NURSING LLC
Sepsis Solutions International LLC [email protected]
Northville, Michiganwww.vollman.com
Disclosures for Kathleen Vollman
• Consultant-Michigan Hospital Association Keystone Center
• Consultant/Faculty for CUSP for MVP—AHRQ funded national study
• Subject matter expert for CAUTI and CLABSI for CMS/HEN 1.0 & 2.0
• Consultant and speaker bureau for Sage Products, LLC
• Consultant and speaker bureau for Hill-Rom, Inc.
• Consultant and speaker bureau for Eloquest Healthcare
6

Let’s Get Started
Post Sepsis Syndrome(PSS) and Post ICU Syndrome (PICS) What You Need to Know to Impact Outcomes
Starts with Your ABC’s…
7
• Define Post Sepsis Syndrome (PSS) and Post ICU Syndrome (PICS) in the patients.
• Identify current practice and begin to build the will to reduce cognitive and physical dysfunction harm that occurs as a result of sepsis or in patients with an ICU stay.
• Discussion current evidence based practice that can help reduce PICS
Learning Objectives
8

Describes physical and/or long-term effects that affects up to 50% of people who survive sepsis.Longer term effects of sepsis include:• Sleep disturbance including insomnia• Experiencing nightmares, hallucinations,
flashbacks and panic attacks• Muscle and joint pains which can be severe
and disabling• Extreme tiredness and fatigue• Inability to concentrate• Impaired mental (cognitive) functioning• Loss of confidence and self-belief
Post-Sepsis Syndrome
Iwashyna, T. JAMA 2010; Mukherjee, S SHOCK 20129

Post Sepsis Syndrome
• People who have suffered from severe sepsis and especially those treated in an intensive care unit are at greatest risk of suffering post-sepsis syndrome.
• “60 percent of hospitalizations for severe sepsis were associated with worsened cognitive and physical function among surviving older adults. The odds of acquiring moderate to severe cognitive impairment were 3.3 times higher following an episode of sepsis than for other hospitalizations.”
• Sepsis survivors may be more at risk for developing other infections both viral and bacterial
Iwashyna, T. JAMA 2010; Mukherjee, S SHOCK 201210

Mild Cognitive Impairment
Moderate/Severe Cog Impairment
20
15
10
5
0
% survivors cognitively impaired
-3 years -1 year +1 year + 3 years
25
p<0.001After SepsisBefore Sepsis
Iwashyna T, JAMA 2010;304:1787-1794
Cognitive Impairment: Sepsis
11

Functional Trajectories by Baseline Functioning
ADL: walking, dressing, bathing, eating, getting into and out of bed and toiletingIADL: preparing a hot meal, shopping for groceries, making telephone calls, taking medicines, and managing money
Iwashyna T, JAMA 2010;304:1787-1794
1.57 new limitations among patients who had no limitations
before
12

Cause of Post Sepsis Syndrome
• Response to systemic inflammation• Brain, muscle and nerve injury from
inflammation, ischemia and ischemia-reperfusion
• Poor perfusion, blood clots• End organ damage
13

Quote from Husband of 32 year Old Sepsis Survivor
“Doctor, she’s not all there. The wit, the comprehension, the concentration. It’s all haphazard at best. To most, it is unrecognizable. The best way to describe it is mental disorganization, like there is a connection missing or a synapse not firing. It has been 10 months, and I just keep waiting for it to straighten itself out. Is this it?”
http://www.icudelirium.org/testimonials.html
14

Post Intensive Care Syndrome
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-38515

Definition
PICS is defined as new or worsening impairment in physical, cognitive, or mental health status arising and persisting after hospitalization for critical illness
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-38516

PICS-Physical Dysfunction
• Less than 10% of patients on mechanical ventilation • for >4 d are alive and fully independent 1 yr later• Caregiver assistance ranging from assistance with activities
of daily living to full care is required by patients 1 yr later• Half of patients with adult respiratory distress syndrome
have not returned to work 1 yr later• ICU-acquired weakness that can persist for years can
develop in 25–80% of those with sepsis or on mechanical ventilation for > 4 d
Desai SV, Law TJ, Needham DM:. Crit Care Med 2011; 39:371–379Brummel NE, Balas MC, Morandi A, et al: Crit Care Med 2015; 43:1265–1275Briegel I, Dolch M, Irlbeck M, et al:Anaesthesist 2013; 62:261–270
17

PICS: Cognition & Mental Illness
• Cognitive impairment that can persist for years develops in 30–80% of patients
• Symptoms of depression occur 1/3 of patient and persist for a year
• Symptoms of anxiety occur in 23–48% have symptoms of anxiety
• Symptoms of posttraumatic distress syndrome occur in 10–50% of patients and may persist for years
Desai SV, Law TJ, Needham DM:. Crit Care Med 2011; 39:371–379Brummel NE, Balas MC, Morandi A, et al: Crit Care Med 2015; 43:1265–1275Briegel I, Dolch M, Irlbeck M, et al:Anaesthesist 2013; 62:261–270Rabiee A, et al. Crit Care Med, 2016, May 5th online
18

Epidemiology of ICU Delirium• 20 - 80% of ICU patients have delirium during ICU• Frequently unrecognized or misdiagnosed by
clinicians• Subtypes
o Hyperactive (agitated, increased motor activity) 1%o Hypoactive (sleepy, inattentive, decreased motor
activity) 44%o Mixed 55%
• Onset: ICU Day 2 (+/- 2)• Duration: 4 (+/- 2) days• 50% & 10% of ARDS pts delirious at ICU &
hospital d/cEly, EW, et al. JAMA 2001; 286, 2703-2710Ely, EW, et al. CCM 2001; 9:1370-1379Peterson, et al JAGS 2006: 54:479-484 McNicoll L, JAGS 2003;51:591-98;Fan, et al CCM 2008:94-99.
19

Brain-ICU Study
• Multicenter RCT- medical-surgical ICU’s• 821 patients with ARF or Shock• Evaluated in-hospital delirium and cognitive
impact 3-12 months post d/c
Results:• 74% of patients developed
delirium during hospital stay• 1/3 & 1/4 had cognitive scores at
1 year follow-up c/w moderate TBI & mild Alzheimers, respectively
• Affected both older and younger
Pandharipande, PP. et al. N Engl J Med;369:1306:1316
1 out of 4 cognitive
Impairment at 12
months
20

Delirium and Patient Outcomes
• Independently associated with increased risk of death: Each day of delirium increase 1 yr mortality by 10%
• Duration assoc. with short & long term cognitive impairment
• 1 out of 4 patients had cognitive impairment at 12 months• Mech Vent duration• ICU & Hospital Length of Stay• Estimated national costs $4 to $16 Billion• ?Post-d/c anxiety/ PTSD symptom from delirious memory
Klouwenberg BMJ 2014;349:g6652; Ely. ICM 2001; 27, 1892-1900 Ely, JAMA 2004; 291: 1753-1762 ; Lin, SM CCM 2004; 32: 2254-2259Girard CCM 38(7):1513-1520; Milbrandt E.,CCM 2004; 32:955-962. Jackson. Neuropsychology Review 2004; 14: 87-98.Oimet ICM 2007; 33:1007-1013; Davydow Gen. Hosp. Psych 2008;30:421-434Pandharipande, PP. et al. N Engl J Med;369:1306:1316
21

Patient Risk Factors
• Immobility• Number of days on mechanical ventilation• Length of stay in the ICU• Heavy sedation• Delirium• Hypoglycemia• Hypoxia• Sepsis• ARDS
Desai SV, Law TJ, Needham DM:. Crit Care Med 2011; 39:371–379Brummel NE, Balas MC, Morandi A, et al: Crit Care Med 2015; 43:1265–1275Briegel I, Dolch M, Irlbeck M, et al:Anaesthesist 2013; 62:261–27022

Prevention is Key
Minimizing Risk Factors23
Reduction of Risk Factors for PICS
• ABCDEF bundle• Early psychological intervention• ICU diaries• Healing environments of care• Post-discharge follow-up programs
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-38524

“Four Cornerstones for Success”
Evidence Based
Practice
Inter-Professional
Teams
System Collaboration
Reduction of Practice Variation

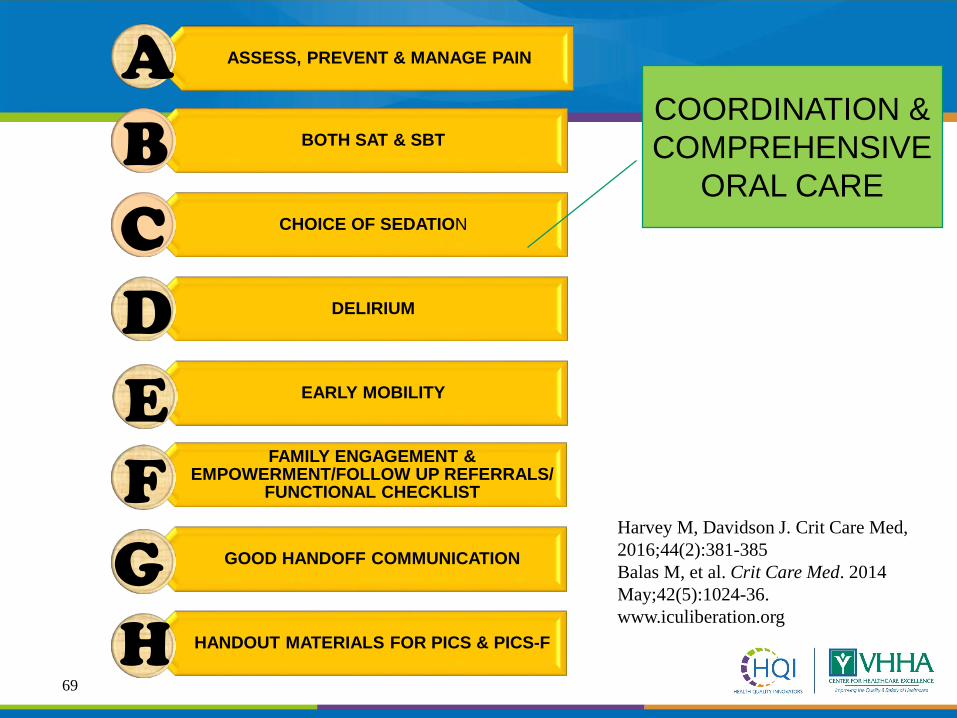
ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
26

Pain, Agitation and Delirium (PAD)
• Agitation in critically ill patients may result from inadequately treated pain, anxiety, delirium, and/or ventilator desynchrony
• Detection and treatment of pain, agitation, and delirium should be reassessed often in these patients
• Patients should be awake and able to purposely follow commands in order to participate in their care unless a clinical indication for deeper sedation exists
Website to help organizations implement the PAD guidelines and reverse immobility:www.iculiberation.org; www.icudelirium.org
Barr J. Crit Care Med. 2013;41:263-30627

ASSESS, PREVENT & MANAGE PAIN
28
Society of Critical Care Medicine PAD Guidelines 2013
CPOT and BPS most valid and reliable
The American Society of Pain Management Nursing July 2011
CPOT is acceptable for the critically ill/unconscious

Critical Care Pain Observation Tool (CPOT)
29

ICU Liberation Program Based on PAD Guidelines
www.iculiberation.org30

ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
31

Agitation
• Avoid deep sedation/coma: • Sedative medications should be titrated to maintain lighter
levels of sedation, unless clinically contraindicated. (+1B)• Use daily awakening or a titrated sedation strategy to
maintain patient wakefulness. (1B)• Choice of sedative:
• Non-benzodiazepines may be preferred over benzodiazepines to improve clinical outcomes in mechanically ventilated ICU patients. (+2B)
• Reduction in sedation requirements:• Use of an analgesia-first (i.e., analog-sedation) strategy is
recommended in mechanically ventilated patients. (+ 2B)Barr J. Crit Care Med. 2013;41:263-306.
32
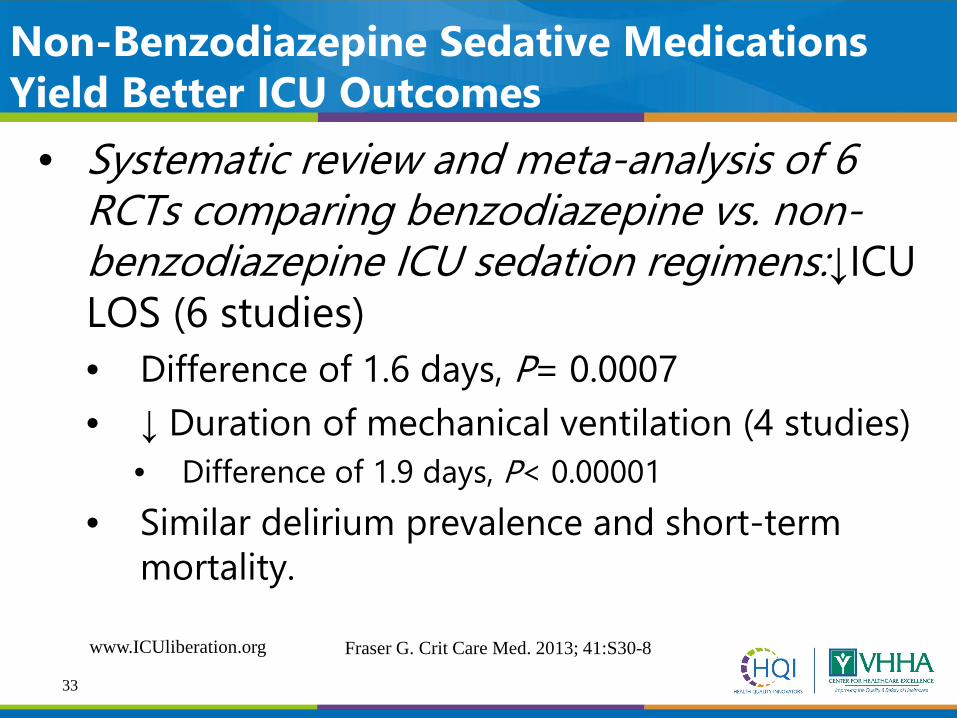
Non-Benzodiazepine Sedative Medications Yield Better ICU Outcomes
• Systematic review and meta-analysis of 6 RCTs comparing benzodiazepine vs. non-benzodiazepine ICU sedation regimens:↓ICU LOS (6 studies)• Difference of 1.6 days, P= 0.0007• ↓ Duration of mechanical ventilation (4 studies)
• Difference of 1.9 days, P< 0.00001• Similar delirium prevalence and short-term
mortality.
Fraser G. Crit Care Med. 2013; 41:S30-8www.ICUliberation.org
33
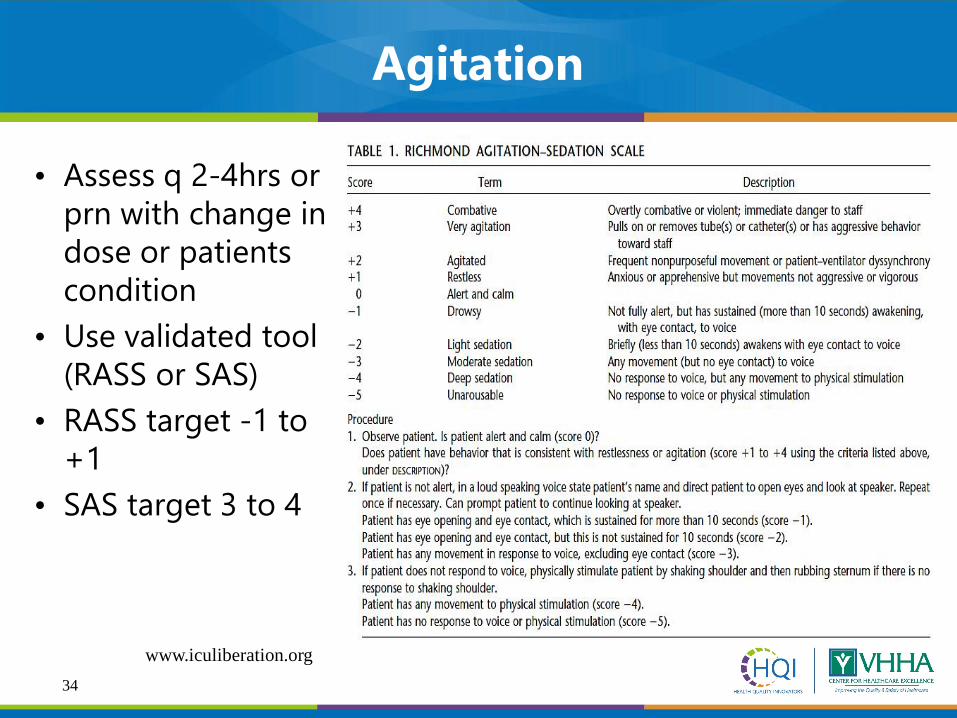
Agitation
• Assess q 2-4hrs or prn with change in dose or patients condition
• Use validated tool (RASS or SAS)
• RASS target -1 to +1
• SAS target 3 to 4
www.iculiberation.org34

35

ABC Trial (RCT Paired Sedation & Vent Weaning Protocols)
Girard, et al, Lancet. 2008;371:126-3436

ABC Trail: Mortality at 1 Year
Girard, et al, Lancet. 2008;371:126-3437

Perform the Safety Screen
• Pass safety screen? Turn off all sedatives• Observe for 5 min, continuously for up to 4 hrs.• If patient awakens: follow 3 out of 4 commands
(open eyes, look at you, squeeze hand, push out tongue)
• Leave sedation off! Tell RT so SBT can be completed.
• The patient fails based on:Try
intermittent dosing or
restart at ½ rate
38

DAILY SBT Process
• Coordinate timing with RT• Conduct safety screen
• Is the patient on vasopressors? This is not automatic exclusion. Must be a discussion with the medical team.
• Pass the safety screen? RT will perform and document SBT and results of SBT.
• RT will notify team if patient passes.• Failure of SBT is based on:
39

CDC Prevention Epicenters’Wake Up and Breathe Collaborative• Prospective quality improvement collaborative• Goal: prevent VAEs through less sedation and
earlier liberation from mechanical ventilation• Mechanism: increase performance of paired daily
spontaneous awakening trials and breathing trials (SATs and SBTs)
• 12 ICUs affiliated with 7 hospitals
Klompas M. (CDC ABCDE Collaborative), Am J Respir Crit Care Med. 2015;191:292-301.
40

CDC Prevention Epicenters’Wake Up and Breathe Collaborative
a. 63% in SATs
b. 16% in SBTs
c. 81% in SBTs done with sedatives off
a. 37% in VACs
b. 65% in IVACs
SATs / SBTs VAEs
Klompas M. (CDC ABCDE Collaborative) Am J Respir Crit Care Med. 2015;191:292-301.
41

Outcome of SAT/SBT
• Decreased days of mechanical ventilation• Reduced weaning time• Reduced re-intubation rates• Fewer days with delirium• Decreased length of ICU stay• Decreased length of hospital stay
Ely E. N Engl J Med.1999;335:1864-9.Girard T. Lancet.2008;371:126-34.Esteban A. Am J Respir Crit Care Med.1997;156:459-65.Esteban A. Am J Respir Crit Care Med.1999;159:512-8www.ICUliberation.org
42
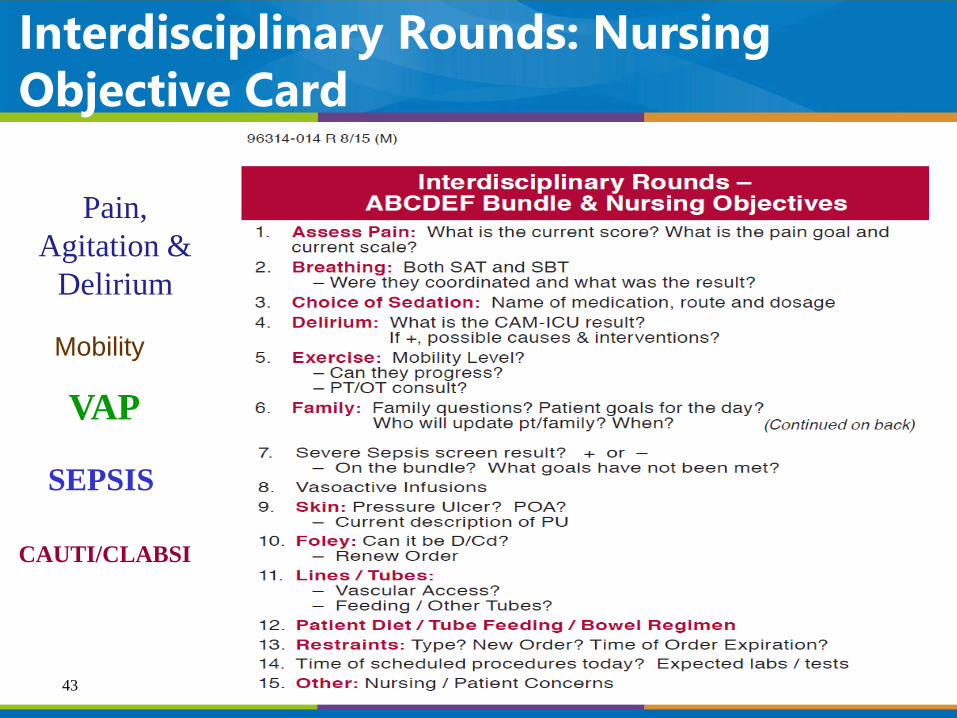
Interdisciplinary Rounds: Nursing Objective Card
VAP
SEPSIS
Pain, Agitation &
Delirium
CAUTI/CLABSI
Mobility
43

ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
44

Delirium: First Focus on Prevention
• Pain and sedation scores• Analgesia and Sedative Algorithm
• Control pain first, then anxiety
• Use intermittent meds first before continuous
• Target RASS + 1 to -1• Daily SAT (spontaneous awakening trial)• Daily SBT (spontaneous breathing trial)• Screen for Delirium---minimum q12hrs; can do it more
frequently• Implement non-pharmacological strategies
45

For Nursing Home Participants:
Polling Question #1
46
Are you screening for delirium at a minimum of every 12 hours using a validated tool?

Check if the lights are on
Is anyone home?
47
48

Non-Pharmacological Strategies
a. Appropriate Medicationsb. Bath during dayc. Chair positiond. Lightinge. Televisionf. Hearing/Vision Aids/Denturesg. Control Noiseh. Ear plugs/eye maski. Minimizing care related disruptions
j. Cognitive Stimulation/Musick. Reorientationl. Familiar objects in room/pictures
Sleep Promotion Mobility Promotiona. Evaluate for Physical Therapyb. Range of Motionc. Sleepd. Work with PTe. Spontaneous Awakening Trial
Sedation Awakening
Other
• Sleep Promotion• Mobility
Pandharipande P et al. (Lorazepam) Anesthesiology 2006;104:21–26;Oimet ICM 2007; 33:1007-1013;Pandharipande P et al. (Midazolam) J Trauma 2008Dubois MJ et al., (Morphine) Intensive Care Med 2001; 27:1297Abraha I, et al. Plos One. 2015;DOI:10.1371/journal.pone.0123090Gathecha E, et al. J of Hosp Med, 2016 online
49

For Hospital & Nursing Home Participants:
Polling Question #2
50
Do your ICUs and nursing care units have a sleep protocol?
PAD Treatment of Delirium Recommendations
• There is no published evidence that treatment with haloperidol reduces the duration of delirium in adult ICU patients (No Evidence).
• Atypical antipsychotics may reduce the duration of delirium in adult ICU patients (C).
• We do not recommend administering rivastigmine to reduce the duration of delirium in ICU patients (–1B).
Barr J, et al. Crit Care Med 2013; 41:263–306 51

Perceptions and Practices Regarding Sleep in the ICU*1
• 1223 surveys of providers• 59% nurses• 39% physicians
• 24 countries• 75% indicate ICU
patients sleep poor or very poor
• 83% to 97% felt poor sleep was associated with negative ICU outcomes
• 32% had sleep promoting protocols
1.Kamdar BB, et al. Ann Am Thorac Soc. 2016 Apr 22,The Sleep in the ICU Task Force2. Presented at Euroanaesthia 2016 accessed 07/14/2016 http://www.medicaldaily.com/noise-levels-icu-who-recommendations-388073
ICU noise at 45dBA & ½ the time at 54 dBA2
52

Perceptions and Practices Regarding Sleep in the ICU
Kamdar BB, et al. Ann Am Thorac Soc. 2016 Apr 22, The Sleep in the ICU Task Force53

ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
54

Outcomes of Early Mobility Programs
• incidence of VAP• time on the ventilator• days of sedation• incidence of skin injury• delirium• ambulatory distance• Improved function• in hospital readmissions• ICU & Hospital LOS
Staudinger t, et al. Crit Care Med, 2010;38.Abroung F, et al. Critical Care, 2011;15:R6Morris PE, et al. Crit Care Med, 2008;36:2238-2243 Pohlman MC, et al. Crit Care Med, 2010;38:2089-2094Schweickert WD, et al. Lancet, 373(9678):1874-82. Thomsen GE, et al. CCM 2008;36;1119-1124Winkelman C et al, CCN,2010;30:36-60Azuh O, et al. The American Journal of Medicine, 2016, doi:10.106/jmjmed.2016.03.032Corcoran JR, et al. PMR J, 2016 in press
55

Systematic Review of Early Rehabilitation in the ICU
• 14 studies/1753 patients
• 880 patients in intervention group
• 873 patient in control group
• Varying methodologies
• Results• No difference in
short or long term mortality
Tipping CJ, et al. ICM, 2017;43:171-18356
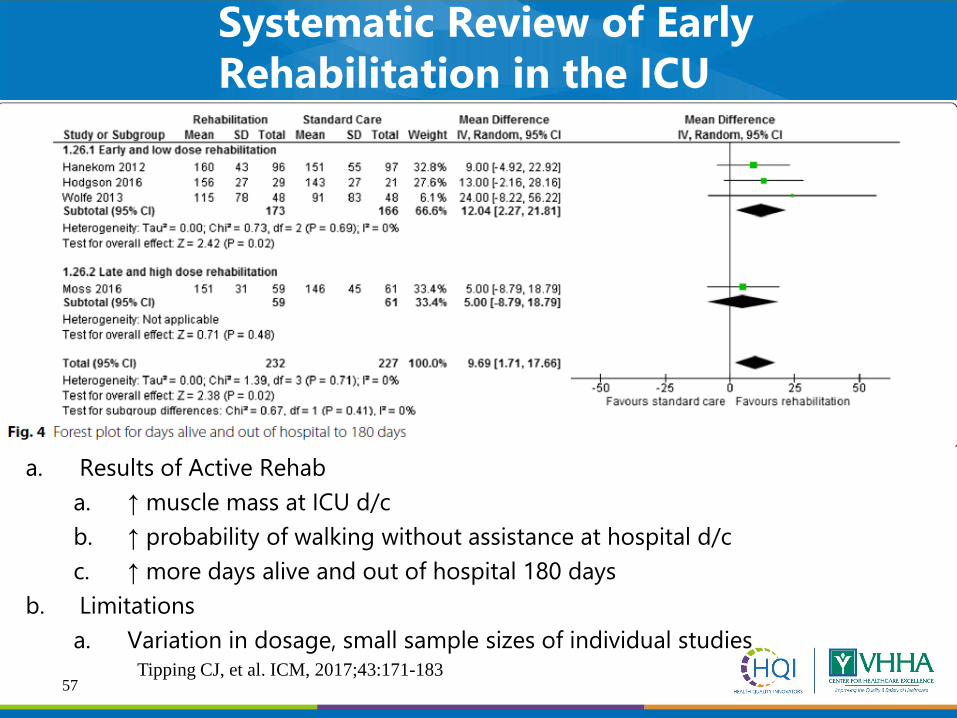
a. Results of Active Rehaba. ↑ muscle mass at ICU d/cb. ↑ probability of walking without assistance at hospital d/cc. ↑ more days alive and out of hospital 180 days
b. Limitationsa. Variation in dosage, small sample sizes of individual studies
Tipping CJ, et al. ICM, 2017;43:171-183
Systematic Review of Early Rehabilitation in the ICU
57

Consensus on Safe Criteria for Active MobilizationSystematic review performed than 23 international experts gather to reach consensus
• Respiratory• Cardiovascular• Neurological• Other Considerations
Categories: Consensus reach on all criteria. If no other contraindications; vasoactives, endotracheal tube, FIO2 < 60% with SaO2 90% & RR < 30/min were considered safe criteriaHodgson CL, et. al Critical Care, 2014;18:658
58

Can We Do It?Is it Safe?
Early Mobility
59
• 7,546 patients with 583 potential safety events occurring in 22,351 mobilization/rehabilitation sessions (2.6%)
• Meta-analysis: hemodynamic changes, 3.8 (1.3–11.4) and desaturation 1.9 (0.9–4.3) per 1000 mobilization sessions
• Events that could not be meta-analyzed-• 11 falls , 2 removals of ETT, 35 removal or dysfunctions of
intravascular catheters, 15 removals of other tube/catheter, 4 cardiac arrest in a single study (not during mobilization).
• Consequences of Potential Safety Events Were reported in23 publications, with 3,329 patients & 13,974 mobilization sessions, 308 potential safety events, for incidence of 2% with consequences 0.6% (78 events)
Safety of Patient Mobilization & Rehab in ICU: Systematic Review & Meta-Analysis
Nydahl P, et al. Annals ATS, 2017;14(5):766-77660

ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
61

FGood communication with the family is critical at every step of a patient’s clinical course, and empowering the family to be part of the team to ensure best care is adhered to diligently will improve many aspects of the patient’s experience. The F was recently added to help to keep patients and families as the center and focus of care.
www.icudelirium.org
Family Engagement and Empowerment
62

Families are the heart of
patient-centered
63
Families are the Heart of Patient-Centered

“I have learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.” Maya Angelou
64

ICU Diaries
• Used routinely in Europe• Diaries are kept by families and
staff to describe the patients experience during the ICU stay
• Pictures are sometimes included• When read post discharge diaries
can fill in memory gaps, replace false memories and delusions
Ullman AJ, et al. Cochrane Database Syst Rev, 2014;12:CD010468Garrouste-Orgeas M, et al. Crit Care Med, 2012;40:2033-2040Jones C, et al. Am J Crit Care, 2012;21:172-176
Outcomes of ICU Diaries:• Decrease anxiety, depression and PTSD symptoms• Decrease PTSD symptoms in families
65

Early Psychologic Intervention
• Psychologists as members of the critical care team
• Early patient & family support, counseling and education on stress management and coping skills
• Psychologist involvement has shown to cut the prevalence of anxiety, depression and PTSD in half
Peris A , et al. Crit Care, 2011;15:R41Czerwonka Al, et al. J Crit Care 2015;30:242-249Petrinec AM, et al. Crit Care Med, 2015;43:1205-1212
66

ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
67

Functional Reconciliation Checklist
• Communication throughout the continuum of care—each transfer to ensure all areas are aware of the patients current physical function• ROM• Bed mobility• Chair• Ambulation• ADL
68
ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
69

Good Handoff Communication
Each Phase Requires Different Levels of Support & Effective Handoff Communication
Czerwonka AI, et al. J of Crit Care, 2015;30:242-249
Major Theme: Survivors do not experience continuity of medical care during recovery after critical illness
• Informational needs change across the care continuum• Fear and worry persist when families don’t know what to expect• Survivors transition from dependence to independence
70

ASSESS, PREVENT & MANAGE PAIN
BOTH SAT & SBT
CHOICE OF SEDATION
DELIRIUM
EARLY MOBILITY
FAMILY ENGAGEMENT & EMPOWERMENT/FOLLOW UP REFERRALS/
FUNCTIONAL CHECKLIST
GOOD HANDOFF COMMUNICATION
HANDOUT MATERIALS FOR PICS & PICS-F
A
DEF
BC
COORDINATION & COMPREHENSIVE
ORAL CARE
GH
Harvey M, Davidson J. Crit Care Med, 2016;44(2):381-385Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36. www.iculiberation.org
71

PICS Resources
Self help rehabilitation manual showed ↓ In PTSD symptoms. Jones C, et al. Crit Care Med, 2003;31:2456-2461
72

ResourcesWebsite Selected information available at the site
www.sepsisalliance.org • signs/symptoms of sepsis• description of common sequelae• over 400 “Faces of Sepsis” – written tributes to lost loved ones and stories of
survivors
www.myicucare.org/thrive • several white-board videos for patient an families, including videos on preparing for hospital discharge after critical illness, post-intensive care syndrome, and wellness after critical illness
• information on virtual and in-person peer support groups for critical illness survivors
www.icusteps.org • information on in-person support groups in the United Kingdom• informational pamphlets for patients and families, including a guide to the ICU
www.healthtalk.org • video interviews describing patient and family experiences of the ICU
www.icudelirium.org/patients • information about common sequelae of critical illness, including patient testimonials
• information about the Vanderbilt ICU recovery center
http://www.aftertheicu.org • Site for information to help patients and families after their ICU stay• Blog to share journeys
73

First US Post ICU Clinics- Indiana University & Vanderbilt
• Critical Care Recovery Center at Indiana University (2011)• ICU recovery Center at Vanderbilt (2012)
• Team consists of medical ICU nurse practitioner, a pharmacist, pulmonary intensivists, a case manager and neurocognitive psychologist
• Any member of the ICU teams can make a referral for patients to the clinic• Screening for inclusion and exclusion criteria are performed• Exclusion criteria
• Pre-existing dementia or cognitive defect, life limiting illness, manage primarily by different subspecialty service/eg. liver/renal transplant, already have specialty resources (eg. Stroke or cardiac rehab, long-term resident of a skilled nursing facility
• Initial visit: completes spirometry & a 6 minute walk test• Nurse practitioner completes a detailed history and physical exam• Neuropsychologist meets with the patient to evaluate and screen for
cognitive impairment and PTSD, anxiety and depression• Only anecdotal data to date
Huggins EL, AACN Advances in Critical Care. 2016;27(2):204-21174

SCCM ProgramEvery year, millions of Americans survive critical illness; but despite the efforts of their ICU, many are left with ongoing problems. The current health care system often does not meet the needs of these survivors, or their families, during their weeks to years of recovery. SCCM seeks to improve patient and family support after critical illness through the THRIVE Initiative.
Network of In-Person Support Groups
Survivors as partners in
Professional Societies
Advancing Research &
Improving our Own Practice
Online Support Groups
Educating non-ICU
Clinicians RE Survivorship
TJ Iwashya presented at SCCM Congress 2016 Orlando Fl
https://www.youtube.com/watch?v=aMn8Yd2JInIhttps://www.youtube.com/watch?v=DU7Ax-xaDiwhttps://www.youtube.com/watch?v=Rwch2_9mSQA&index=1&list=PLsb8sp1zaJWoeZ2qY2L_ymyinpn671HS8
75

THE OUTCOME
The Outcome
76

ABCDEF Bundle: Improving Survival & Reducing Brain Dysfunction
• Ventilated and non-ventilated medical and surgical ICU patients enrolled between January 1, 2014, and December 31, 2014
• Determine association between ABCDEF bundle compliance/total & partial & outcomes of hospital survival and delirium-free and coma-free days/ adjusting for age, severity of illness, and presence of mechanical ventilation
• Patients experienced more days alive and free of delirium and coma with both total bundle compliance (incident rate ratio, 1.02; 95% CI, 1.01–1.04; p = 0.004) and partial bundle compliance (incident rate ratio, 1.15; 95% CI, 1.09–1.22; p < 0.001).
10% ↑ in total bundle compliance, patients had a 7% higher odds of hospital survival
Barnes-Daly, CCM 201777

Opportunities Identified in our 1st Cross Setting Meeting between Sepsis Project Hospitals and their Nursing Home Partners:
What have we learned?
78
• Improve communication and education of caregivers, patients and families on early signs of Sepsis
• Improve staff communication during handoffs of transfers and discharges
• Arranging for early discharges from acute care to nursing homes so that medical orders and medications can be obtained in a timely manner to eliminate disruption in care especially need for continuation of antibiotic therapy
• Ensure discharge documentation is accurate, timely and complete for continued appropriate plan of post acute care

Save The Date
Friday, September 29, 2017, 10:00AM-12:00NCross Setting Meeting – Richmond/Petersburg SIP Participating Hospitals & Nursing Homes: Friday, September 29, 2017, 10:00AM-12:00N @ VHHA
Thursday, October 26th Webinar 11:00AM-12:00N“Exploring the Long Term Care Regulatory Process”
Regulatory expert Mary Chiles will take our hospital partners on a journey of nursing home state & federal regulatory processes affecting admissions, transfers, discharges and reimbursement. Nursing Homes are welcomed to attend.
79

Q and A
80
This material was prepared by Health Quality Innovators (HQI), the Medicare Quality Innovation Network-Quality Improvement Organization for Maryland and Virginia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. HQI|11SOW|20170919-144111

81
Contact Information
Joyce Dayvault, RN, BBADirector of Performance Improvement, VHHASepsis Innovation Project Lead for Hospitals
Office: (804)297-3402email: [email protected]
Kathleen M. Vollman RN, MSN, CCNS, FCCM, FAAN
Clinical Nurse Specialist/Educator/ConsultantVA Sepsis Innovation Project Content Expert
ADVANCING NURSING LLCSepsis Solutions International LLC
email: [email protected]
Lisa Mark, RN, BSNImprovement Consultant, HQI
Sepsis Innovation Project Lead for Nursing HomesOffice: (804)-289-5331
email: [email protected]